You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Scientific Report 19993
4Patron HM The Queen Beatrix
Scientific Report 19995The Netherlands Cancer InstituteCANCER RESEARCH LABORATORY AND CANCER HOSPITAL
6Scientific Report 1999Illustrations and unpublished data in these reportsshould not be used without permission of the author.Copyright ©;The Netherlands Cancer InstituteAntoni van Leeuwenhoek HuisPlesmanlaan 1211066 CX AmsterdamThe NetherlandsPhone 31.20.512 9111Fax 31.20.617 2625ISSN 1387-8611
Contents7Board Members 8Research Divisions 9Introduction 12Education in Oncology 19I Division of Cell Biology 22II Division of Molecular Carcinogenesis 32III Division of Cellular Biochemistry 41IV Division of Immunology 51V Division of Molecular Biology 61VI Division of Tumor Biology 69VII Division of Molecular Genetics 76VIII Division of Experimental Therapy 86IX Division of Radiotherapy 98X Division of Medical Oncology 111XI Division of Surgical Oncology 126XII Division of Psychosocial Research andEpidemiology 136XIII Division of Diagnostic Oncology 145Biometrics Department 155Research Facilities 159Cancer Hospital 164Ongoing Trials 167Invited Speakers 177Projects 179Personnel-Project Index 187
8Board MembersWF Duisenberg, President ofBoard of GovernorsInternational Scientific Advisory BoardJR Bertino, American Cancer Society Professor ofMedicine and Pharmacology, Yale University School ofMedicine, New Haven, USARA Flavell, Professor of Immunobiology, Yale University,New Haven, USAS Hellman, AN Pritzker Distinguished Service Professor,The University of Chicago, Chicago, USAWGJ Hol, Professor of Molecular Biology University ofWashington, Biomolecular Structure Center, School ofMedicine University of Washington, Seattle, USAJ Mendelsohn, President, MD Anderson Cancer Center,The University of Texas, Houston, USAP Nurse, Professor of Microbiology, Director-General ofImperial Cancer Research Fund, London, UKR Nusse, Professor of Developmental Biology StanfordUniversity; Investigator, Howard Hughes MedicalInstitute, Stanford, USAHL Ploegh, Edward Mallinckrodt, Jr. Professor ofImmunopathology, Harvard Medical School, Boston,USARA Weinberg, Professor of Biology MassachusettsInstitute of Technology, Whitehead Institute, Cambridge,USAC Weissmann, Professor of Molecular Biology Universityof Zürich, Institut für Molekularbiologie Zürich,SwitzerlandNational Scientific Advisory BoardLA Aarden, Professor of Molecular Immunology,AmsterdamD Bootsma, Professor of Cell Biology and Genetics,RotterdamSWJ Lamberts, Professor of Internal Medicine,RotterdamB Löwenberg, Professor of Hematology, RotterdamCJLM Meijer, Professor of Pathological Anatomy,AmsterdamCJM Melief, Professor of Immunohematology, LeidenHM Pinedo, Professor of Clinical Oncology, AmsterdamFH Schröder, Professor of Urology, RotterdamGNJ Tytgat, Professor of Gastroenterology, AmsterdamAJ Van der Eb, Professor of Fundamental TumorVirology, LeidenPC Van der Vliet, Professor of Physiological Chemistry,UtrechtBoard of DirectorsP Borst, chairman and director of research(until 01.12.1999)AJM Berns, chairman and director of research(from 01.12.1999)L Neeleman, director organization and managementS Rodenhuis, director clinical research and developmentBoard of GovernorsWF Duisenberg, presidentML Frohn-De Winter, vice-president (until 27.09.1999)HCJ Van der Wielen, vice-president (from 13.12.1999)JF Visser, treasurerR HazelhoffJHM TemminkGNJ TytgatPF Van der HeydenS Van der KooijJ Van der MeerMWM Vos-Van GortelScientific Advisory CouncilP Borst, president (until 01.12.1999)AJM Berns, secretary (until 01.12.1999),president (from 01.12.1999)AM Kruisbeek, secretary (from 01.12.1999)R BernardsS RodenhuisA SonnenbergFE Van Leeuwen
Research Divisions9I Cell BiologyE Roos (head)J CalafatJG CollardK JalinkA SonnenbergII Molecular CarcinogenesisR Bernards (head)E Kriek (honorary staff member)TK SixmaH Te RieleM Van LohuizenIII Cellular BiochemistryWH Moolenaar (head)J BorstN DivechaP Ten Dijke (from 01.10.1999)WJ Van BlitterswijkLN Vernie (until 01.07.1999)IV ImmunologyAM Kruisbeek (head)MJ KerstenTNM SchumacherH SpitsCJM Vennegoor (stationed at the Free University)FA Vyth-DreeseK WeijerV Molecular BiologyRHA Plasterk (head)P BorstAPM Jongsma (stationed at the Free University)HGAM Van LuenenVI Tumor BiologyJ Neefjes (head)PC Hageman (honorary staff member)J HilkensRJAM MichalidesA Tulp (deceased 18.01.1999)AA Van der GugtenAA Verstraeten (stationed at the Free University)VII Molecular GeneticsAJM Berns (head until 01.12.1999)P Demant (head from 01.12.1999)D BarlowR Beijersbergen (from 01.04.1999)P KrimpenfortM SnoekMA Van der ValkVIII Experimental TherapyAC Begg (head)KMG HaustermansJHM SchellensAH SchinkelFA StewartMJ Van de VijverLJ Van ’t VeerIX RadiotherapyH Bartelink (head)BMP AlemanJSA BelderbosJ BorgerIAD BruinvisEMF DamenRW De BoerLGH DewitRLM HaasAAM HartKMG HaustermansRB KeusJV LebesqueEAH MasselinkBJ MijnheerLMF MoonenNS RussellJG SalverdaBNFM Van BunningenM Van HerkFW Wittkämper
10RESEARCH DIVISIONSX Medical OncologyS Rodenhuis (head)JW BaarsP BaasEM BaisJH BeijnenW BoogerdH BootPF BruningGC De GastSP IsraëlsMJ KerstenH NeeringJFM Pruijt (until 01.09.1999)JHM SchellensJH SchornagelBG TaalWW Ten Bokkel HuininkJJ Van der SandeM Van der WeideAMC Witte (from 01.07.1999)N Van ZandwijkAPE Vielvoye-KerkmeerResearch NursesD BatchelorAC DubbelmanMMJ HoltkampGAM LinthorstME SchotM SwartW UyterlindeXI Surgical OncologyBBR Kroon (head)AJM BalmCL BlackburnKE BosD BuitelaarJB De Boer (until 01.05.1999)FJM HilgersS HorenblasMM KaagW MeinhardtOE NiewegRP Noordanus (until 01.10.1999)EJTh RutgersPFE SchutteIB TanM Van BeurdenF Van CoevordenN Van der VangeACM Van LindertJ VisscherLAE Woerdeman (from 01.12.1999)FAN ZoetmulderXII Psychosocial Research and EpidemiologyNK Aaronson (head)MA RookusFSAM Van DamFE Van LeeuwenXIII Diagnostic OncologyMJ Van de Vijver (head)APE BesnardJMG BonfrerD De JongMPW GalleeK GilhuisCA HoefnagelFBL HogervorstW KoopsR KrögerSH MullerPM NederlofWJ NooijenFA PameijerJL PeterseL Schultze KoolM Smid-GeirnaerdRA Valdes OlmosO Van TellingenLJ Van ’t VeerMLF Van VelthuysenBiometrics DepartmentOB Dalesio (head)H Van Tinteren
Heads of General Research ServicesAudiovisual ServiceJM LomeckyBiophysicsGJF Blommestijn11RESEARCH DIVISIONSCentral Cancer LibraryS BakkerFinancial AdministrationB SimmelinkGeneral FacilitiesR ClementLaboratory Animal DepartmentRGM Ten BergResearch CoordinationAJM Berns, laboratory research coordinator(until 01.12.1999)AM Kruisbeek, laboratory research coordinator(from 01.12.1999)H Van Luenen, laboratory research managerEJ Vos, clinical research manager
12IntroductionDirector of ResearchA. BernsThe Netherlands Cancer Institute/Antoni vanLeeuwenhoek Hospital (<strong>NKI</strong>/<strong>AvL</strong>) is an integrated cancerinstitute, combining a hospital and research laboratoriesunder one roof in a single independent organization. Thehospital comprises 180 beds, a large RadiotherapyDepartment and outpatient clinics. Facilities for patientresearch include a large patient database, clinical datamanagement and active research groups in epidemiologyand psychosocial oncology. The laboratory covers allmajor areas of cancer research, with special emphasis onmouse tumor models, mouse (reverse) genetics, cellbiology, immunology and translational research requiringclose collaboration between clinical and basic scientists.This Scientific Report deals mainly with the clinical andbasic science in the <strong>NKI</strong>/<strong>AvL</strong>. Information on patient carecan be found in our General Report.1999 will be primarily remembered as the year thatPiet Borst stepped down as Director of Research afterholding this position for almost 17 years. During hisdirectorship the <strong>NKI</strong>/<strong>AvL</strong> metamorphosed from an organizationthat had lost contact with the fast developing areaof molecular and cellular biology into a high profileresearch institute with cutting edge research in basic andclinical disciplines. The institute now hosts many strongresearch groups, often headed by young group leaders.They constitute a vibrant faculty with the ambition tofurther build on the solid foundation laid in the lastdecade. In recognition of Piet Borst’s excellentleadership, a two-day symposium ‘Killing Cancer Cells’was held in Amsterdam. This well-attended meeting, withprestigious speakers, was a dignified and fitting tribute toPiet Borst. During the festivities Piet Borst received theRoyal honor ‘Commander in the Order of the DutchLion’. The Mayor of the City of Amsterdam, ScheltoPatijn presented the decoration. We are privileged thatPiet Borst will remain at the Cancer Institute as a groupleader for at least another 5 years, continuing his ownresearch.At the turn of the MillenniumAt the turn of the millennium we look back on a fascinatingperiod in biomedical research. The last fifty yearshave yielded fabulous insights in how nature works. Wenow know in some detail how cancer arises, and haveidentified many of the genetic lesions instrumental incausing cancer. However, there are still many unknowns.I want to mention some that are particularly relevant forcancer as they pose a challenge for us in the future. 1)We still have little understanding of most of the genetictraits that determine the level of susceptibility orresistance of individuals to the development of malignancies.2) We do not know how these genetic traitsinteract with environmental factors, such as lifestyle andenvironmental exposure, giving us little background forpreventive measures. 3) Although we have identifiedmany of the lesions frequently occurring in specifictumors, this information is still insufficient for a reliableprognosis and prediction of response to treatment. 4)Our knowledge of the precise effects of the geneticlesions on tumor cell biochemistry is still sketchy. A moredetailed insight is required for effective interventionstrategies.There is, however, also ample reason for optimism. Ina number of instances our understanding is beginning toreach the level that permits the design of new, highlyspecific drugs that will selectively attack cancer cellswhile leaving normal cells untouched. New treatmentsusing these designer drugs are expected to differprofoundly from the conventional chemotherapies in thatthey are more specific and therefore cause fewer sideeffects. They will complement and may eventually replacethe current chemotherapies, providing a much moreacceptable supplement to surgery and radiotherapy, themost effective treatments for localized and operabletumors.Such a detailed insight has to come both from highquality basic research and the thorough analysis ofclinical tumor samples. This will lead to markers for betterdiagnosis and to new targets for intervention. To achievethis, it is important to obtain a catalog of molecularfeatures of human tumors, using array technologies forDNA, RNA and proteins. The <strong>NKI</strong>/<strong>AvL</strong> is well positionedto contribute to these areas, some of which arementioned below.1) Understanding the details of how a cell works, howit divides and how it migrates. We have invested heavilyin cell biology research and this discipline will be ofcritical importance understanding how genetic instruc-
tions translate into specific cell characteristics. This informationis also indispensable for designing and testingintervention strategies as they can define new targets fordrug treatment or lead to strategies to effectively mobilizethe immune system against tumor cells.2) Understanding the heritable traits which controlresistance and susceptibility to cancers. We havedeveloped unique animal model systems, fully in thetradition of the <strong>NKI</strong>/<strong>AvL</strong>, that allow us to mimic and studytumor development as it occurs in man but under wellcontrolledlaboratory conditions. These models will alsobe invaluable to test existing and new interventionstrategies.3) We have unique expertise with the formulation ofdrugs, and with pharmacokinetic, and pharmacodynamicmeasurements in patients and model systems. Inaddition, there are strong groups within the institutestudying drug resistance mechanisms of cancer cells andhow to circumvent these. All this expertise is pivotal forclinical research purposes and it is also invaluable forpreclinical testing of new therapies.4) Over the decades we have collected the recordsand stored tumor samples of thousands of cancerpatients. Pairing the information from these records withthousands of molecular parameters of each patientsample using high throughput micro-array technologiesshould lead to the identification of molecular markers thatcan accurately classify tumors. This should lead to betterdiagnosis, more rational selection of therapies and,eventually, to the design of new therapies and early interventionstrategies.These projects need the participation of both cliniciansand basic researchers. They present unique opportunitiesfor exciting research. While expressing this optimism forthe future, we have to realize that current successfulcancer treatments depend almost entirely on surgery,radiotherapy, and chemotherapy. These treatmentmodalities will remain the backbone for the treatment ofcancer for quite some time and therefore furtheroptimizing and careful pairing of these existing treatmentmodalities remain important objectives of our research.Figure 1Quality of researchThe quality of research is monitored in several ways.Our scientific productivity as based on bibliometricparameters (citations and impact of scientific articlespublished by the <strong>NKI</strong> staff) has shown a steady increasesince the beginning of the eighties. In the last years thenumber of citations and impact are leveling off (Tables Iand 2) with yearly fluctuations suggesting that we havereached a steady state.Our competitiveness for obtaining grants is anothermeasure of quality. We have been quite successful duringthe last five years in obtaining grant support, scoring onaverage 2-3 fold better than our competitors. This translatesin funding of the vast majority of our grant applications.In 1999 our success rate was somewhatdiminished but still almost twofold higher than theaverage. The first impression for 2000 indicates that thescore is up again.The third measure of quality is based upon externalsite visits, in which international leaders in a particularfield of research review the work of a division or researchgroups with a similar theme on a quinquennial basis. InFebruary 1999 the work of two divisions was reviewed.The Division of Diagnostic Oncology was visited byD Sidransky (Director Head and Neck Cancer Research,Table 1Short-term citations and impact of scientific articlespublished by the <strong>NKI</strong> research staff 1982 - 1998Publication year Citations* Impact**1982 560 2951983 779 3651984 1340 6161985 1286 5491986 1366 6501987 1839 7651988 1775 7421989 1273 7641990 2127 8541991 2199 9101992 2074 9111993 2221 9581994 3455 12921995 2896 14151996 3324 15201997 17831998 135913INTRODUCTION* In the two years after publication, excluding self citations.Starting with 1989, the citation analysis has been carried outon-line. This allows detection (and elimination) of all selfcitations. Before 1989 this pruning was limited to first authors.** The impact factor is the average number of citations per yearof an article in a given journal. The total impact is the sum ofthe impact of all articles published that year.
14INTRODUCTIONTable 2Number of <strong>NKI</strong> publications in journals with an impactfactor 10 and higher in the period 1989 to 1998. SeeTable 1 for definition of impact factor.IF97 Journal ’89 ’96 ’97 ’98 Total1989-9839 Nat Genet 4 3 1 937 Cell 6 3 2 2628 Nat Med 1 128 N Engl J Med 1 727 Nature 4 2 2 3 2725 Science 3 1 1421 Immunity 2 2 1 519 Genes Dev 2 3 4 1418 Curr Opin Cell Biol 1 0 116 Immunol Today 1 116 Lancet 1 2 3 3 2114 J Exp Med 4 1 7 3 3113 EMBO J 4 7 7 5 4812 Ann Intern Med 1 212 J Cell Biol 3 5 4 5 3211 J Natl Cancer Inst 1 3 3 3 2611 Trends Cell Biol 1 210 Mol Cell Biol 1 2 1 3 13Total 24 37 43 31 280Johns Hopkins, Baltimore, USA), P Selby (Director ofClinical Research for ICRF, Leeds, UK), and M Stratton(Section Chairman of Cancer Genetics, Institute ofCancer Research, Surrey, UK). The site report waspositive with suggestions to further augment the researchof this still young division. The Division of PsychosocialResearch and Epidemiology was reviewed by P Ganz(University of California, Los Angeles, USA), P Patrick(University of Washington, Seattle, USA) and L Bernstein(USC-Norris Comprehensive Cancer center, University ofSouth California, Los Angeles, USA). Again, the reviewwas favorable, with part of the research identified asworld-class. A number of constructive suggestions weremade for improvement.This year we also received the results of a completelyindependent evaluation of biomedical sciences in theNetherlands conducted by the Dutch Academy of Artand Sciences. The mostly excellent rating of the <strong>NKI</strong>/<strong>AvL</strong>could now be put in the perspective of the evaluation ofbiomedical research elsewhere in the Netherlands. Theevaluation showed that overall biomedical research in theNetherlands is of good to very good quality. Twelvepercent of the programs’ score was excellent and 30%very good. Four of the five <strong>NKI</strong> programs’ scores wereexcellent and one very good. While it is pleasing thatoutside reviewers give us such a high rating, there isalways room for improvement. That will be the challengefor the coming five years.Research HighlightsIt is always difficult for a research director to selectresearch highlights to mention in the introduction. Ratherthan give an overview of highlights of all the divisions, Ihave decided to focus on a few discoveries by mostlyyoung investigators of the institute.The availability of the complete sequence of a range ofgenomes will revolutionize the way we do research. Nowwe have to make sense of this information using reverseand forward genetics in combination with cell biologicaland biochemical analyses. Work in many of the researchdivisions relies on a combination of these approaches. Anexciting example of this is represented by a discovery inthe group of Ronald Plasterk (Division V). While all knownnatural isolates of the worm C. elegans contain multiplecopies of the Tc1 transposon, which are active in thesoma, Tc1 transposition is fully silenced in the germline ofmany strains. Plasterk and colleagues mutagenized onesuch silenced strain and isolated mutants in which Tc1had been activated in the germline (‘mutators’).Interestingly, many other transposons of unrelatedsequence had also become active. Most of thesemutants appeared resistant to RNA interference (RNAi)(Ketting et al. Cell 1999; 99: 133-41). They found one ofthe mutated genes, mut-7, to encode a protein withhomology to RNaseD. This provided support for thenotion that RNAi works by dsRNA-directed, enzymaticRNA degradation. This led them to propose a model inwhich MUT-7, guided by transposon-derived dsRNA,represses transposition by degrading transposon-specificmessengers, thus preventing transposase production andtransposition. This represents an intriguing mechanism ofgene regulation and gene expression ‘inheritance’.Whether similar mechanisms of gene regulation areemployed in mammalian cells remains to be seen.Genetic screens can also be very rewarding in cells inculture, especially with the increasing availability ofprimary cells of knockout mice. The group of MaartenVan Lohuizen (Division II) showed that the oncogeneBMI1 silences the tumor suppressor genes Ink4a andP19Arf in mouse embryo fibroblasts in vitro and in micein vivo. The absence of BMI1 in Bmi1 knockout fibroblastsresulted in higher levels of INK4A and P19ARFleading to premature senescence of the cells (Jacobs etal. Nature 1999; 397: 164-68). His group has now usedthe poor growth of these fibroblasts to perform a rescuescreen with a retroviral cDNA library. CDNAs wereidentified which could restore growth of these fibroblastsin the absence of BMI1. At least some of the cDNA’sappeared to specifically impair the level of p19ARF butnot INK4A, thereby adding new regulatory componentsto this cell cycle regulatory network. Furthermore, VanLohuizen and colleagues have shown that downregulationof Ink4a-Arf by BMI1 underlies its ability tocooperate with MYC in tumorigenesis (Jacobs et al.Genes & Dev 1999; 13: 2678-90). Heterozygosity forBmi1 inhibits lymphomagenesis in Eµ-Myc mice by
enhancing c-MYC-induced apoptosis. They observeincreased apoptosis in Bmi1(-/-) lymphoid organs, whichcan be rescued by deletion of Ink4a-Arf or overexpressionof BCL2. Furthermore, BMI1 collaborates withMYC in enhancing proliferation and transformation ofprimary embryo fibroblasts (MEFs) in an INK4a-ARFdependentmanner, by prohibiting MYC-mediatedinduction of p19ARF and apoptosis. Strong collaborationwas observed between the Eµ-Myc transgene andheterozygosity for Ink4a-Arf, with the concomitant loss ofthe wild-type ink4a-ARF allele and formation of highlyaggressive B-cell lymphomas. Together, these resultsreinforce the critical role of BMI1 as a dose-dependentregulator of INK4A-ARF. It is expected that unraveling ofthe pathway in which BMI1 acts will uncover additionalgenes that will be critical for tumorigenesis in man.Hein Te Riele and colleagues demonstrated that micecarrying a disruption in MutS homolog Msh5 show ameiotic defect, leading to male and female sterility (DeVries et al. Genes & Dev 1999; 13:523-31). Histologicaland cytological examination of prophase I stages in bothsexes revealed an extended zygotene stage, characterizedby impaired and aberrant chromosome synapsis,that was followed by apoptotic cell death. Thus, murineMSH5 promotes synapsis of homologous chromosomesin meiotic prophase I. They also found that mice carryinga partial defect in mismatch repair by ablation of themismatch recognition protein MSH6, are highly cancerprone, but that intestinal cancer is suppressed byredundant functions of MSH3. This observation predictsthat families segregating a defect in MSH6 show a highincidence of cancer but are often not recognized asHNPCC families due to suppression of intestinal tumorigenesisby residual MMR activity.Ed Roos and colleagues (Division I) showed that thechemokine SDF-1 is essential for T lymphoma metastasisto many tissues. This indicates that lymphoma disseminationis, at least in part, determined by chemokinespresent in those tissues (Soede et al. J Immunol 1999;163: 4253-61). Stromal cell-Derived Factor 1 (SDF-1)acts by inducing migration but, in addition, by activatingintegrin adhesion molecules through heterotrimeric G-protein G q. LFA-1 dependence is only seen at low SDF-1concentrations. The LFA-1 signal can be propagated in aZAP70 dependent fashion to other LFA-1 molecules onthe same cell, which then bind to ICAM-2 on other cells.This causes cell aggregation that was also blocked bydominant-negative ZAP-70. Thus, an LFA-1 signalinvolving ZAP-70 activates other LFA-1 molecules,suggesting that the chemokine signal can be amplified bymultiple cycles of LFA-1 activation. This represents animportant step forward in our understanding of themolecular mechanisms and tissue specificities observedin metastatic growth.Kees Jalink (Division I) found, using a GFP-boundsensor, that the lipid PIP2, an important signalingmolecule, is localized in patches near the plasmamembrane. He generated a membrane-bound constructto detect PIP2 by intramolecular FRET (FluorescentResonance Energy Transfer). This should permit thehighly sensitive detection of local and transient changesin PIP2 levels during dynamic processes such as cellmigration. The possibility to measure protein-protein andprotein-substrate interaction in real time and space offersunique opportunities for following molecular signalingevents within a single cell upon exposure to externalsignals.The group of Ton Schumacher (Division IV) examinedthe role of cytotoxic T –cell memory in the subsequentresponse against mutant epitopes in vivo (Haanen et al.J Exp Med 1999; 190: 1319-28). Applying soluble tetramericpeptide-MHC complexes, these experiments showthat the CD8 T-cell mediated response against a largeseries of random mutants of a viral antigen is completelydominated by cross-reactive CD8 cells that recognizeboth the wild-type and the mutant epitopes. As thesecross-reactive T cells can also differentiate into cytotoxiceffector cells, these findings suggest that epitopemutations in TCR-exposed residues will not readilypromote CTL escape. In future studies, the group willdissect the molecular requirements that lead to selectiveexpansion of cross-reactive T cells.The groups of Jannie Borst and Wim Van Blitterswijk(Division III) studied the role of sphingolipid ceramide inapoptosis signaling. They examined ceramide formationinduced by CD95, etoposide, or gamma-radiation (IR) inrelation to caspase activation and mitochondrial changesin Jurkat T cells (Tepper et al. J Clin Invest 1999; 103:971-8). They demonstrated that ceramide, contrary tocommon belief, does not play a triggering role inapoptosis. Instead, ceramide production appears toresult from loss of plasma membrane symmetry duringthe effector phase of apoptosis; such lipid scramblingmay facilitate membrane blebbing, vesicle shedding andapoptotic body formation.Alfred Schinkel and colleagues (Division VIII) haveshown that P-glycoprotein (P-gp) inhibitors could potentiallybe used to increase the fetal penetration of P-gpsubstrate drugs (Smit et al. J Clin Invest 1999; 10: 1441-47). They used mice with a targeted disruption of theMdr1a and Mdr1b genes. Mdr1a(+/-)/1b(+/-) femaleswere mated with Mdr1a(+/-)/1b(+/-) males to obtainfetuses of 3 genotypes (Mdr1a(+/+)/1b(+/+), Mdr1a(+/-)/1b(+/-), and Mdr1a(-/-)/1b(-/-)) in a single mother.Intravenous administration of the P-gp substrate drugpaclitaxel to pregnant dams revealed that 16-fold moredrug entered the Mdr1a(-/-)/1b(-/-) fetuses than enteredwild-type fetuses. Furthermore, placental P-gp activitycould be completely inhibited by oral administration ofthe P-gp blockers PSC833 or GG918 to heterozygousmothers. This finding implies that the placental drugtransportingP-gp is of great importance in limiting thefetal penetration of various potentially harmful or therapeuticcompounds and demonstrates that this P-gpfunction can be abolished by pharmacological means.The latter principle could be applied clinically to improve15INTRODUCTION
16INTRODUCTIONpharmacotherapy of the unborn child. Other studies bythe Schinkel group showed that even low levels of P-gpand Mrp1 contribute considerably to tumor drugresistance, suggesting that multidrug transporterinhibitors may also increase the sensitivity of previouslyuntreated (naïve) tumors to chemotherapy.The group of Marcel Van Herk (Division IX) developeda generic method for 3-D evaluation of target volumedelineation in multiple imaging modalities to assistaccurate high-dose radiotherapy (Remeijer et al. MedPhys 1999; 26: 931-40). The evaluation includes geometricaland statistical methods to estimate observer differencesand variability in defining the Gross Tumor Volumein relation to the diagnostic CT and MRI modalities. Thestatistical method distinguishes observer and modalityrelated uncertainties, which are expressed in terms ofvarious error components: random observer deviations,systematic observer differences and systematic modalitydifferences. The method was successfully applied to agroup of prostate cancer patients, where it was demonstratedthat delineation variability is non-homogeneous,with the largest variations occurring near the seminalvesicles and the apex. This permits reliable treatmentplans for a three- field technique giving a dose of 78 Gyto the target volume (prostate). This approach isexpected to have a direct impact on both local cure andsurvival of the patients.Floor van Leeuwen and coworkers (Division XII) foundthat physically active women had a 30% lower risk ofbreast cancer than inactive women. This suggests thatphysical activity might be one of the first life-style riskfactors for breast cancer amenable to preventivemeasures.The clinical pharmacology group (Division X) hasinvested in facilitating the oral availability of taxanes byinhibition of the P-glycoprotein multi-drug transporter thatis responsible for the fact that orally administered taxaneshave a very low bioavailability. The group has beensuccessful in increasing the bioavailability of both paclitaxeland docetaxel by prior administration of cyclosporinA. These findings in phase I studies have led to a phaseII study of oral Docetaxel in advanced breast cancer. Oraladministration is not only of practical advantage, it alsocircumvents the adverse reactions of patients againstCremophor EL used for the formulation of paclitaxel forintravenous injection.One of the unique features of the institute is thenatural interaction between disciplines and divisions. Thishas led to the integration of a unit for chemoradiationtherapy in one of the hospital wards. The institute hasplayed a prominent role in the relatively recent recognitionthat concurrent chemo- and radiotherapy has curativepotential in a large number of epithelial tumors, whereasthe sequential application of these treatment modalitiesshows no advantage. Examples include treatments ofstage III NSLC with concurrent cisplatin and radiationand, more recently, intra-arterial cisplatin and radiotherapyin advanced head-and-neck cancers. The newclinical unit will make it possible to perform clinicalstudies in a range of tumor types.A boost for translational research in 2000The expression profile of many thousands of genes ina single tumor by micro-array technologies is expected tocontain important parameters for diagnosis and mightpredict response to treatment and clinical outcome. Inorder to establish correlations between expressionprofiles and biological characteristics of tumors, retrospectivestudies have to be conducted in which theprofiles of thousands of tumors are compared with theclinical records. The <strong>NKI</strong>/<strong>AvL</strong> has collected tumorsamples for many decades and has, in recent years,extracted RNA and DNA from several hundreds ofsamples. We are currently investigating several options toanalyze a substantial number of these tumor samples.For this we will establish collaborations with expertcenters elsewhere. In this way we hope to acquire thenecessary expertise for data collection and bioinformaticsin the course of 2000. Once reliable correlations betweenexpression profiles and prognostic parameters have beenestablished, array analyses can be introduced as aroutine screening methodology. Patients will immediatelyprofit, as this information will permit a more rationalchoice in the treatment options.Mouse models for cancer become more and moresophisticated. Switching genes on and off in a tissuespecific and time controlled fashion permits the inductionof specific tumors at high incidence within a narrow timeframe in these mice. Since multiple mutations can beintroduced simultaneously, these models permit moreaccurate determination of genotype-phenotyperelationships. Moreover, since we can introduce in thesemodels the same genetic lesions as found in humantumors, they probably will more closely mimic the humancondition and therefore be better suited to the initialtesting of intervention protocols. In that way they canhelp to bridge the gap between basic and clinicalresearch. A number of clinicians have shown interest inthese models and in the course of 2000 several cliniciansare expected to start working with them.HonorsPiet Borst received the Royal decoration of‘Commander in the Order of the Dutch Lion’ and thegolden ‘Van Leeuwenhoek Microscope’ of theNetherlands Cancer Institute during the festivities in honorof his retirement as Director of Research.Ronald Plasterk (Division V) received the prestigiousSpinoza Award of the Netherlands Organization forResearch, worth fl 3,000,000 Dutch guilders to be spenton research of his choice. In the spring of 2000, Plasterkwill become Director of the Hubrecht Laboratory, a highly
egarded research institute of The Netherlands Academyof the Arts and Sciences, fully devoted to developmentalbiology. Maarten Van Lohuizen (Division II) received thePioneer Stipendium of the Netherlands Organization forResearch, a high profile research career grant of theNetherlands Organization for Research. Ada Kruisbeekbecame member of EMBO and Anton Berns was electedas member of the Academia Europeana. JaquelineJacobs, a graduate student in the group of Maarten VanLohuizen, received the Antoni van Leeuwenhoek Prize1999, for elucidating the role of the oncogene BMI1 inthe cell cycle. She showed that BMI1 exerts its effect bysuppressing the expression of the tumor suppressorgenes Ink4a and p19Arf, thereby preventing cell cyclearrest and senescence.New <strong>NKI</strong> professorsThe <strong>NKI</strong>/<strong>AvL</strong> cannot award university degrees.However, many of our staff members hold special parttimechairs in one of the Dutch Universities. This facilitatesthe supervision and awarding of degrees tograduate students receiving their training at theNetherlands Cancer Institute. A particularly large numberof staff became professors in 1999. Jan Schellens wasappointed as ‘Professor of Drug Toxicology’ at theUniversity of Utrecht. Piet Borst was re-appointed as‘Professor of Clinical Chemistry’ at the University ofAmsterdam. Jacques Neefjes became ‘Professor of TheBiology of Antigen Processing and Presentation’ at theUniversity of Leiden, Bin Kroon ‘Professor of SurgicalOncology’ at the University of Amsterdam, Jannie Borst‘Professor of Experimental Oncology’ at the University ofAmsterdam, and Peter Peters ‘Professor of Cell Biology’at the Free University of Amsterdam.Changes in <strong>NKI</strong>/<strong>AvL</strong> academic staffIn January we were notified of the sudden death of AbTulp, a dedicated, if idiosyncratic biochemist who specializedin cell separation techniques. He was on the staff ofthe Netherlands Cancer Institute (Division of TumorBiology) from 1971. Besides his originality as a scientist,he was renowned for his artistic and humorous drawingsexplaining biochemical processes or exposing politicalcontroversies within the research community at the<strong>NKI</strong>/<strong>AvL</strong>. We have lost in him a loyal and fine colleague.A number of staff members retired in 1999. In additionto Piet Borst as Director of Research, Lou Smets,Professor of Experimental Oncology, also retired. Loujoined the <strong>NKI</strong>/<strong>AvL</strong> as head of Experimental Cytology in1970 and served the institute for almost 30 years. Hewas committed to leukemia research and studied druginduced apoptosis of tumor cells. Lou was a rigorousand original scientist. He was not easily convinced, andwas known for his critical reviews. He pointed out thediscrepancies between the outcome of short-termapoptosis assays and long-term clonogenic survival ofcells defective in regulation of cell cycle control. Lou wasalways keen to see his scientific findings applied in theclinic. The concept of lowering the pH in tumors wasexplored under his supervision, for the treatment ofcarcinoid tumors by MIBG. He was also a devotedteacher and served as chair of the teaching committee ofthe institute for over 15 years, including coordinating therotation of students. A postdoctoral course andsymposium of the European School of Oncology and theInternational Society of Pediatric Oncology, of which Louwas an organizer for many years, was held in Amsterdamto honor Lou’s contribution to cancer research.Leen Vernie (Division of Cellular Biochemistry) retired asstaff member after having served the institute for morethan 30 years. Leen investigated the anti-carcinogenicproperties of selenium in the early seventies. His interesthas remained with this early work although he was willingto take on many other tasks. In the eighties he becameinvolved in the purification of G-proteins and subsequentlyin the synthesis of custom peptides and specialderivatives. He has served the <strong>NKI</strong>/<strong>AvL</strong> as a dedicated,helpful and pleasant colleague.Ton Van der Gugten also said farewell to the <strong>NKI</strong>/<strong>AvL</strong>after being a staff member for more than 30 years. Heworked in the area of tumor virology and hormonedependence of tumors. In the last 10 years he becameinvolved in the mathematical modeling of biochemicalprocesses.New staff joining the <strong>NKI</strong>/<strong>AvL</strong> includes Peter Ten Dijkewho was recruited from the Ludwig Institute for CancerResearch in Uppsala, Sweden. He is well known for hiswork on TGF-β signaling and SMAD tumor suppressorproteins. He is a senior staff member of the Division ofCellular Biochemistry. Roderick Beijersbergen wasrecruited to the institute as an <strong>AvL</strong> fellow. He did hispost-doctoral work in the laboratory of Bob Weinberg(Whitehead, Cambridge, USA) and has now joined theDivision of Molecular Genetics where he will focus on theregulation of expression of human telomerase.Internal and external appointmentsWith my appointment as Director of Research, myprevious positions (head of the Division of MolecularGenetics and Laboratory Research Coordinator) becamevacant. We are pleased that Ada Kruisbeek, head of theDivision of Immunology, has accepted the position ofLaboratory Research Coordinator. Peter Demant willsucceed me as head of the Division of MolecularGenetics. I will continue to supervise my own researchgroup within that division. Jannie Borst has taken overthe chair of the teaching committee from Lou Smets.17INTRODUCTION
18INTRODUCTIONNational and international activitiesStaff of the <strong>NKI</strong>/<strong>AvL</strong> fulfilled numerous functions innational and international organizations, on the scientificboards of scientific journals, as members of studysections, as organizer or co-organizer of scientificmeetings, workshops and congresses. Internationalorganizations included: AACR, CIBA, EACR, EBCTCG,EMBO, EORTC, ESSO, ESTRO, ICRU, MRC, OECI,WFSOS, WHO. Staff members also served on boards oforganizations such as EORTC cooperative groups,International Association for Breast Cancer Research,Mesotheliomenwerkgroep van de Nederlandse Verenigingvan Artsen voor Longziekten en Tuberculose, LandsteinStichting voor Bloedtransfusie Research, NederlandseCommissie voor Stralingsdosimetrie, Dutch Head andNeck Cancer Cooperation Group, Oog en Orbita Commissie,The Netherlands Working Party on Melanoma,International Psycho-oncology Society, European CommunityCommittee on Palliative Cancer Care, ComprehensiveCancer Center Amsterdam, European Societyfor Therapeutic and Radiation Oncology, the WHO Qualityof Life Group, The International Academy of Pathology,the Gezondheidsraad, The European Cancer Center,National Advisory Board on AIDS, Netherlands HealthCouncil Committee on Home Care for Cancer Patients,Scientific Council on Social Oncology (WRSO) of theDutch Cancer Society, KNAW committee Disciplineadviesplan Medisch Onderzoek, KNAW selectiecommissieKNAW fellows, Walree Fonds, Heineken Prijsselection committee, the General Motors Awardcommittee for Cancer research, KEMO, CCMO, ScientificCommittee for the Cancer Research Campaign (UK),EMMA (European mouse repository), Education andPsychosocial Research Committee of the CancerResearch Campaign, the Dutch and European Societiesof Surgical Oncolgy, the World Federation of SurgicalOncological Societies, Wetenschappelijke Kommissie vanhet Fonds voor Wetenschappelijk Onderzoek België,Deutsche Forschungsgemeinschaft. Staff members alsoserved as editors or on editorial boards of scientificbooks or journals such as Genes & Development, BBAreviews in cancer, European Journal of SurgicalOncology, Genes to Cells, Experimental Cell Research,Mammalian Genome, Carcinogenesis, Immunogenetics,Quality of Life Research, European Journal Immunology,International Immunology, Journal of Biological Chemistry.Other activities included organizing national and internationaloncology meetings, workshops and congressesincluding: Killing Cancer Cells (Amsterdam, 17&18November, 1999), Thymus Workshop Rolduc (Kerkrade,May, 1999), INSERM Meeting on the T Cell Receptor/CD3 Complex (Aix-les-Bains, October, 1999), FirstInternational Congress on the Sentinel Node in Diagnosisand Treatment of Cancer (Amsterdam, 1999), Symposiumon neck node metastasis of an unknown primary(1999) and STATs and SMADs (Seoul, 10-13 October,1999). Finally, staff members participated in teaching forthe European School of Oncology and the ESTROteaching course on Radiation Physics for ClinicalRadiotherapy and Basic Clinical Radiobiology.Outlook and acknowledgementsWe are making steady progress in our plans for a newhospital building and renovation of the old premises. Wereceived a positive review from several governmentalagencies, including the Ministry of Health, regarding ourplans for the new hospital building. We expect that wecan now proceed expeditiously and lay the foundation forthe new building in the course of the year 2000. This willat least temporarily solve the ever increasing need foradditional space to accommodate our expanding basicand clinical research activities.For all our research we depend on the financialsupport of the government, the Dutch Cancer Societyand of many individuals. Only with their help can wecontinue to develop new ideas that should lead toprevention, early detection, and more effective treatment.Ton BernsDirector of Research
Education in Oncology19Education in fundamental and clinical research andtraining in patient care are regular activities of theinstitute. Several senior staff members have joint appointmentsas professors at Dutch universities and contributeto the regular curriculum at these universities. In addition,many staff members teach in courses for graduatestudents, either within the institute or at universities. Theresearch departments attract many undergraduatestudents from universities throughout the country, whocontribute practically to ongoing scientific projects andreceive in house theoretical training. The <strong>NKI</strong> has a formalliaison with the Biology Faculty of the University ofAmsterdam and is committed to present a course inExperimental Oncology to the third year students inMedical Biology of this university. The institute participatesin the Oncology Graduate School Amsterdam,together with of the University of Amsterdam and theFree University. A large body of PhD students areassigned to this graduate school, all for a four-yearperiod. These graduate students generally make significantcontributions to the scientific program. They receiveadditional practical and theoretical training within theinstitute. Post-doctoral teaching and training in clinicaloncology and patient care is the major educational taskof the cancer hospital. Collaboration with the localmedical faculties and hospitals has increased continuouslyby shared activities of their graduate schools andjoint projects in clinical and fundamental research.Table 1Lecture course in Experimental Oncology, Fall 1999Cancer, diagnostics, treatmentEpidemiologyPsychosocial researchPathologySurgeryChemotherapyPharmacokineticsDrug resistanceRadiotherapyDNA damage and repairApoptosisAntigen presentationImmunologyIntracellular transportClinical immunologyGenetic predisposition for cancerGenome projectCell cycleTranscriptionDevelopmental biologyCell senescenceCell adhesionSignal transductionTumor progressionMedical geneticsS RodenhuisF Van LeeuwenF Van DamD De JongO NiewegJ SchellensJ BeijnenA SchinkelR HaasH Te RieleJ BorstJ NeefjesH SpitsP PetersJ HaanenP DemantR PlasterkR MichalidesR BernardsM Van LohuizenR BeijersbergenE RoosW MoolenaarA BernsL Van ’t VeerUndergraduate studentsThe undergraduate program in Experimental Oncologyattracts students of all national universities in partial fulfillmentof the obligations of their curriculum. Studentsusually have a background in Medical Biology/HealthSciences, Biology, Chemistry or Medicine. The undergraduateprogram offers combined practical and theoreticaltraining in various aspects of experimental oncology.Practical training includes participation in ongoingresearch projects for a minimum period of 4 months,after which the students deliver oral and written accountsof the results obtained. In 1999 about 35 undergraduatestudents did a 4-9 month placement at the basicresearch divisions of the <strong>NKI</strong>. The majority of thesestudents came from either of the two universities inAmsterdam or from Utrecht University, in equal distribution.There were three students from Leiden University,one from Wageningen and one from Nijmegen. Moststudied either Medical Biology or Biology. The coreelement of theoretical training is the lecture course inexperimental oncology, given twice yearly by staffmembers of the institute. This course is also part of theregular curriculum of third year students in MedicalBiology of the University of Amsterdam. It is much appreciatedfor giving an accurate account of recent developmentsin basic oncology (Table 1). This year, the coursewas supplemented by visits to the clinical departments ofRadiotherapy, Radiobiology and Pathology, under supervisionof department staff.All teaching activities are supervised by a TeachingCommittee. Specialized tasks are assigned to individual
20EDUCATIONmembers of the scientific staff. These tasks include theorganization of lecture courses, guidance of scientificvisits and the distribution of information regarding undergraduatestudies at the <strong>NKI</strong>.Information undergraduate school: TeachingCommittee <strong>NKI</strong>; secretariat H3, phone 020-5121970.Dean: Prof. J BorstGraduate studentsAbout 75 PhD students of the Netherlands CancerInstitute are members of our Graduate School: the OOA(Onderzoekschool Oncologie Amsterdam: OncologyGraduate School Amsterdam). These are scientists-intraining,who receive complementary theoretical andpractical training covered by a 4-year contract. At theend of this period, the student can acquire the PhDdegree from any national university. The tutorship forthese graduate students is covered by the graduateschool, headed by Prof. R Plasterk. The OncologyGraduate School Amsterdam is a joint activity with themedical schools of the Free University and the Universityof Amsterdam. All OOA graduate students participate inthe yearly meeting of graduate students, a 3-days retreatduring which they present the highlights of their ongoinginvestigations. This year’s retreat was held in themonastery of Rolduc in Kerkrade.In 1999 several combined practical and theoreticalcourses were organized (Table 2). Scientists of internationalreputation in the respective areas were invited toteach at these courses. We have introduced a newelement to the programme of the <strong>NKI</strong> part of OOA: aSpecial Seminar Program and Semester Courses. For theSpecial Seminar Program leading scientists were invitedto the institute. We take full advantage of the visit byadvanced preparation for the visit and by organizing adiscussion session after the seminar. In the preparationsessions the graduate students discuss an articleselected by the guest; the lecture itself is open to theTable 2general public, it is advertized like all seminars, but thediscussion sessions afterwards are only open to the <strong>NKI</strong>OOA students. In 1999, 50 special seminars have beenorganized.We have continued the experiment with a series ofsemester courses. These courses consist of 10 sessionsin which the two course organizers and participantsdiscuss in great depth key publications that have had amajor impact on the field. The students prepare eachsession by writing a three page synopsis of the publication,and these synopses are corrected in detail (forstyle as well as content) by the course instructors beforethe discussion session. The following course were given:1. Cell biology (instructors: R Bernards and M VanLohuizen fall 1998); 2. Genetics (instructors: A Berns andR Plasterk, spring 1999); 3. Immunology (instructors: AKruisbeek and T Schumacher, fall 1999).Information graduate school: secretariat H8, phone020-5122081. Dean: Prof. RHA PlasterkPostdoctoral trainingThe <strong>NKI</strong> research department continually hosts anumber of postdoc fellows and trainees from the DutchCancer Foundation, The European Cancer Center,Amsterdam or abroad. Staff members lecture on variouspostdoctoral training courses such as the ‘ElementaryCourse in Oncology of the Dutch Oncology Society’ andvarious courses and seminars organized by the EuropeanSchool of Oncology. Moreover, the <strong>NKI</strong> is co-organizer ofnational, postdoctoral ‘Oncology Days’ for clinical oncologists.Teaching for medical students and doctors in trainingAt the medical schools of the University of Amsterdamand Free University, staff members lecture on fundamentaland clinical oncology in the undergraduate studyprograms. Two groups of 15 undergraduate medicalstudents of the University of Amsterdam participated in aCourses at the OOA Graduate School - 1999January Pathogenesis of malignant lymphomas C Meijer, S PalsJanuary-Feb Determinants of tumor behavior and G Peterstherapeutic effectsApril Translational research in pediatric oncology P Voûte, L SmetsSeptember Fluorescence microscopy:new developments in genetic analysis P Van Diest, G Meijer, M HermsenOctober The anatomy and histology of the house W Lamers, C Van NoordenmouseOctober Detection, treatment and biology of minimalresidual disease in human solid tumors R Brakenhoff, G Van DongenOctober Annual graduate student retreat R Plasterk, I DeltrapOct-Dec Immunology (semester course) T Schumacher, A KruisbeekNovember Immunotherapy R Scheper, A Van den Eertwegh, B De GastNovember Killing Cancer Cells (symposium) A Berns, S Rodenhuis
three week institutional training course with lectures givenby staff physicians covering the whole scope of clinicaloncology. As a spin off medical students apply for a 3months senior internship being actively involved in dailyclinical practice and retrospective analyses of patientsseries. Clinical oncology courses were given to theresidents of the institute and trainees in radiotherapy(<strong>NKI</strong>/<strong>AvL</strong>), general surgery (Academic Medical Center),plastic & reconstructive surgery (Academic MedicalCenter) and urology (Free University). Medical specialistsparticipated in the <strong>NKI</strong>/<strong>AvL</strong> postgraduate oncologyfellowship programs of medical oncology, surgicaloncology and head & neck oncology- and surgery.Cancer Nursing EducationThe educational department of the <strong>NKI</strong>/<strong>AvL</strong> organizeda post-basic, core curriculum course in cancer nursingfor internal and external candidates. This coursepromotes the development of cognitive, psycho-motorial,interactive and reactive skills to practice oncology nursingwith confidence and professionalism. The theoreticalprogram consists of 175 hours of classroom instruction,including the the following compulsory modules: 1) introductionof the educational system and instruments; 2)professional quality and quality of care; 3) continuity ofcare; 4) communication and collaborative skills; 5) introductionto oncology; 6) cancer nursing and medicaltreatment. In addition to these modules, the studentsmake a choice out of two non-compulsory modules.The ‘on-site’ practical training consists of 15 monthsinternship which takes place on both medical andsurgical wards. During this period the student willencounter various aspects of oncology nursing, includingdiagnosis, treatment, palliative and terminal care as wellas participation in clinical research trials.Further developments within the educationaldepartment include regular nursing grand-rounds whichinvolve the participation of all nursing departments.Themes directed to development in cancer nursing care,cancer nursing practice and new developments arediscussed. The educational department also organizedvarious post-graduate refresher courses in the treatmentand care of cancer patients.Clinical post-graduate coursesThe Department of Radiotherapy has a full trainingprogram for radiotherapists and radiographers. Foreignradiotherapists are regular guests at the department, aswell as residents of other hospitals. The Departments ofMedical Oncology and Surgery offer 6-12 months electiveresidencies for internists and surgeons in training, incooperation with various universities and training clinics.Both departments have 1-3 year training programs forqualified surgeons and internists to specialize inoncology. The Department of Plastic and ReconstructiveSurgery participates in the training program of theAcademic Medical Center and has a full time position fora resident. The Department of Pathology has a 3 monthtraining program for residents in diagnostic cytopathology,including fine-needle aspiration cytology, incooperation with the universities of Amsterdam, Utrechtand Rotterdam. In addition, postdoctoral courses indiagnostic cytology and histopathology are regularlyorganized by the department. The Department of Surgeryorganized the yearly ‘Surgeon’s Week’. The programinvolves multidisciplinary teaching lectures, demonstrationsof surgical techniques, demonstration of patientsand discussion of new modalities in diagnosis andtreatment. A cyclic program for continuing education inMedical Oncology has been developed by theDepartment of Medical Oncology. It consists of a 2-yearcourse of 10 meetings concluded by a symposium andmeets the requirements of the European Examination inMedical Oncology.21EDUCATION
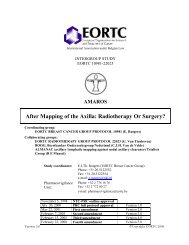
22I Division of Cell BiologyDivision head Ed RoosIntroductionThe major cause of cancer deaths is metastasis, i.e.the dissemination of cells throughout the body, leading totumor growth in distant, often vital organs. Metastasis isdue, at least in part, to defective regulation of celladhesion and motility, the main research theme in thisdivision. We study adhesion to the extracellular matrix,mainly mediated by integrins, and between cells,mediated by cadherins. Examples are the assembly ofhemidesmosomes, which are structures required forstable adhesion of epithelial cells to the basementmembrane, and the loss of intercellular adhesion inducedby oncogenes and by integrin signals. In addition, wefocus on the transient activation of adhesion moleculesas required for movement of cells, and essential forinvasion into tissues during metastasis formation.Adhesion and motility are regulated by signalstriggered by chemokines and growth factors that bind tocell surface receptors. In addition, integrins themselvesact as such receptors and elicit signals upon binding totheir ligands. These signals not only lead to immediateresponses such as the further activation of other integrinsduring invasion, but also have long-term effects on genetranscription, cell proliferation and cell morphology.Elucidation of the latter effects is crucial for the understandingof loss of anchorage-dependence for proliferationand loss of intercellular adhesion in cancer cells,and this goal is pursued in the groups of both ASonnenberg and J Collard. Rho-like GTPases, whichcontrol the activities of the cytoskeleton, have anessential role in metastasis. The group of J Collard wasamongst the first to demonstrate this. These GTPasesalso affect gene transcription, and feature in virtually allsignal pathways that regulate adhesion or are triggeredby adhesion molecules. These GTPases are thereforestudied in all three main research groups.Relevant signals for invasion, such as triggered bychemokines acting on G-protein-coupled receptors,studied in the group of E Roos, are elicited locally andquite transiently and therefore hard to detect withstandard biochemical assays. This problem should beovercome by real-time imaging of signaling events inliving cells as they move. Development of the requiredmethodology is a major aim of K Jalink. One of thecrucial regulators of cytoskeletal activity is the lipid PIP2,but its role is poorly understood. Jalink devised a methodfor real-time imaging of PIP2 in the plasma membrane,which should be of great help in elucidating this role inthe near future.Adhesion mechanisms in metastasisE Roos PhDRDM Soede PhD 1PJM Stroeken MSc 2IS Zeelenberg MSc 3MK Kamp 1EMF Ruuls-Van Stalle 3EAM Van Rijthoven 2YM Wijnands 1S LigthartN Van PoppelM BoterJ KamphorstGroup leaderPost-docGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentTrainee technicianTrainee technicianRole of the chemokine SDF-1 in lymphoma metastasisWe showed previously that the pertussis toxin catalyticsubunit, expressed in a T-cell hybridoma, blockedmetastasis to all tissues. We have now observed thesame for a B-lymphoma and a myeloid leukemia exceptthat, remarkably, colonization of the bone marrow by themyeloid cells was not affected. The toxin blocks G iprotein-transduced signals from certain receptors,including those for chemokines. A prominent candidatechemokine for being involved was SDF-1 because it isconstitutively expressed in many of the invaded tissues.To study this, we made cells that no longer displayed theSDF-1 receptor CXCR4 on the cell surface. This wasachieved by transfecting SDF-1 with an attached KDELsequence that binds to the KDEL-receptor, which retainsendoplasmic reticulum (ER) proteins in the ER. Newlysynthesized CXCR4 binds to SDF-1-KDEL, it is alsoretained in the ER and transport of CXCR4 to the surfaceis thus prevented. This is illustrated in Figure I.1.Chemotaxis towards SDF-1, but not towards thechemokine TARC, was abrogated. Invasion into fibroblastmonolayers was blocked but was restored when fibroblastswere pretreated with TARC, demonstrating thespecificity for SDF-1. Most importantly, metastasis tomany tissues was prevented. The cells grew normally
upon i.p. injection showing that the lack of metastasis isnot due to immune rejection. The dissemination of the B-lymphoma and myeloid leukemia cells probably involvesother chemokines. This is being investigated. Thus,dissemination of hematopoietic malignancies may bedetermined in part by expression of appropriatechemokine receptors. However, the signaling pathwaystriggered by these receptors should also be intact, asdemonstrated by BW5147 T-lymphoma cells which arenot invasive and do not metastasize. These cells expressCXCR4 but do not respond to SDF-1 in a chemotaxisassay.Figure I.1Generation of cells without the CXCR4 receptor for thechemokine SDF-1. Transfected SDF-1 with an attached KDELsequence binds to the KDEL-receptor, which retainsendoplasmic reticulum (ER) proteins in the ER, and to CXCR4and thus blocks the transport of CXCR4 to the surface. As aresult, the cells no longer respond to SDF-1.G i and G q proteins and Rho family GTPases: role inchemokine-induced LFA-1 activationChemotaxis towards low concentrations of SDF-1 (1ng/ml) through a filter coated with ICAM-1, a ligand forthe integrin adhesion molecule LFA-1, was dependent onLFA-1 function, as was invasion. We studied the involvedsignaling pathways using pharmacological inhibitors aswell as retroviral transduction of toxins or dominantnegativemutants of signaling molecules. Wheneverinvasion was blocked, this low SDF-1 chemotaxis wasalso affected. In contrast, chemotaxis towards high levels(100 ng/ml) of SDF-1, which is not dependent on LFA-1,was often not affected. In both cases, i.e. high and lowSDF-1 levels, G i proteins were required as well as theRHO-like GTPase CDC42. However, LFA-1-dependentchemotaxis (low SDF-1) as well as invasion required inaddition G q proteins, the RHOA GTPase and myosinactivity. Remarkably, this shows that high SDF-1-inducedchemotaxis proceeds without contraction of actin filamentnetworks by myosin.Metastasis of T-cell hybridoma cells expressingdominant-negative mutants of CDC42, RHOA and G qwas much reduced. In vivo growth upon i.p. injectionwas normal, showing that this was not due to immunerejection or an inherent inability to grow in vivo. The retroviralvector contained an intra-ribosomal entry site andGFP, to monitor expression levels and select cells withhigh expression. Cells expressing similar GFP levels froman empty vector metastasized normally, excluding aneffect of a possible immune response against GFP. Wehave also introduced a dominant-negative mutant of G qinto the myeloid leukemia cells. This blocked metastasisto liver and spleen as well as the bone marrow. Thus,whereas G i protein signals are only required for liver andspleen metastasis of these cells (see above), G q appearsto be required for invasion of the myeloid cells into alltissues, including the bone marrow.LFA-1 on lymphoid cells needs to be activated.Inhibition of T-cell hybridoma invasion by pertussis toxincan be overcome by direct LFA-1 activation, indicatingthat the chemokine signal activates LFA-1. This signal istoo weak and transient to be assessed in standardadhesion assays, but it can be mimicked by AlF 4 whichactivates heterotrimeric G-proteins including G i and G q.Indeed, similarly to low SDF-1 chemotaxis and invasion,AlF 4-induced adhesion to ICAM-1-coated substrates wasdependent on CDC42, RHOA and myosin activity. Theexistence of a G q-RHOA-myosin pathway was furthersupported by the effect of a constitutively active G qmutant which caused the constitutive activation of a largeproportion of RHOA. The transfectants aggregated extensively,due to activation of LFA-1 that binds to ICAM-2expressed by these cells, and this was blocked bymyosin inhibitors.LFA-1-induced LFA-1 activation: the role of ZAP-70We showed previously that invasiveness of T-cellhybridoma cells was blocked by the ZAP-70 inhibitorpiceatannol and by a truncated dominant-negative ZAP-70 mutant. ZAP-70 is probably not involved in thechemokine-triggered LFA-1 activation, described above,since neither the inhibitor nor the mutant affected AlF 4-induced adhesion. We propose that ZAP-70 actsdownstream of LFA-1, based on its involvement in LFA-1mAb-induced aggregation. At subsaturating concentrations,certain LFA-1 blocking mAbs induce aggregation,mediated by the unoccupied LFA-1 molecules that bindto ICAM-2. Cross-linking of LFA-1 by the mAbs isrequired. This phenomenon can be explained if thetriggering of LFA-1 elicits a signal that leads to theactivation of other LFA-1 molecules. This LFA-1-to-LFA-1signal appears to involve ZAP-70 since aggregation isblocked by piceatannol and dominant-negative ZAP-70.CDC42, RHOA and myosin contraction were not requiredfor this aggregation, in contrast to the chemokineinducedLFA-1 activation. We therefore propose a modelfor invasion, involving two different modes of LFA-1activation.ZAP-70 is essential in T-cell receptor (TCR) signaling.The ZAP-70 tandem SH2 domains bind to ITAMsequences in the TCR-CD3 complex, that have beenphosphorylated on tyrosine by Src-like kinases. UsingSH2 mutants, we found that both SH2 domains arerequired for ZAP-70 activity in invasion, suggesting that23CELL BIOLOGY
24CELL BIOLOGYbinding to a phosphorylated ITAM is required. However,the T-cell hybridoma we used does not express the TCR-CD3 complex. Furthermore, the lack of effects of specificinhibitors and dominant-negative mutants indicate thatSrc-like kinases are not involved. Identification of theprotein that binds to the ZAP-70 SH2 domains, as wellas the kinase that phosphorylates this protein, is now amain aim.Role of the ß1 integrin cytoplasmic domain inmetastasis of ESb lymphoma cellsESb lymphoma cells metastasize to liver and spleen,as do T-cell hybridoma cells, but they use the α4β1integrin instead of LFA-1 (αLβ2). We previously made β1-deficient double knock-out (DKO) mutants by targeteddeletion of both β1 genes. DKO cells had greatly reducedmetastatic capacity, which was regained upon restorationof β1 expression by retroviral transduction. ESb cellsinvade into monolayers of the BMS2 murine bonemarrow stromal cell line, and this invasion wascompletely blocked by α4 and β1 mAbs. In agreementwith this, DKO cells did not invade. We introduced aseries of β1 cytoplasmic domain mutants into DKO cellsand found that invasiveness into BMS2 monolayerscorrelated with metastatic capacity. Deletion of the C-terminal five residues, as well as conservative replacements(T>A) of the threonines between the two NPXYdomains, blocked invasiveness and metastasis. The twomutants have in common that they can not bind to therecently identified ICAP-1 protein that interacts specificallywith the β1 cytoplasmic domain. For the threoninemutant we demonstrated this by yeast two-hybridanalysis. We are presently investigating the possible roleof this protein.Remarkably, conservative replacement (Y>F) of the twoNPXY tyrosines had no effect on invasion and metastasisbut abrogated α4β1-mediated adhesion to fibronectin,induced by the integrin activator Mn 2+ . The same wasobserved with a β1β2 chimera, containing a β2cytoplasmic domain with NPXF domains instead of NPXYas in β1. This shows that the requirements for invasionand adhesion are not the same. Conceivably, α4β1 hasmainly a signaling function in invasion which may notrequire interactions with all proteins that are essential forstable adhesion.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-969.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1467.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1679.Publications: Adhesion mechanisms inmetastasisSoede RDM, Driessens MHE, Ruuls-Van Stalle L, Van HultenPEM, Brink A, Roos E. LFA-1 to LFA-1 signals involve the ζ-associatedprotein-70 (ZAP-70) tyrosine kinase: relevance for invasionand migration of a T-cell hybridoma. J Immunol 1999; 163:4253-61.Stroeken PJM, Van Rijthoven EAM, De Boer E, Geerts D, Roos E.Cytoplasmic domain mutants of β1 integrin, expressed in β1-knockout lymphoma cells, have distinct effects on adhesion, invasionand metastasis. Oncogene (in press).JG Collard PhDLCJM OomenPhD 4A Malliri PhD 3L Price PhD 5,2T Reid PhD 6EE Sander PhD 7S Van Delft PhD 2G Zondag PhD 8A Bathoorn 2L Janssen 9JP Ten Klooster 8RA Van der KammenMR Ahmadian PhD 1C Olivio PhDGenetic controlof invasion andmetastasisGroup leaderAcademic staffPost-docPost-docPost-docPost-docPost-docPost-docTechnicianTechnicianTechnicianTechnicianGuestGuestRHO family proteins control dynamic cytoskeletalchangesRho-like GTPases, which include CDC42, RAC, andRHOA, have been implicated in the control of a widerange of biological processes. In particular, RHO-likeproteins act as key control molecules in signalingpathways that determine the reorganization of the actincytoskeleton in response to receptor stimulation. Similarto RAS proteins, RHO-like proteins cycle between theactive GTP-bound state and the inactive GDP-boundstate. The dynamic cytoskeletal changes regulated byRHO-like GTPases determine the morphology, adhesionand motility of cells, processes required for themetastatic spread of tumor cells.The invasion-inducing Tiam1 gene encodes an activatorof RacTo identify genes involved in invasion and metastasis,we employed retroviral insertional mutagenesis in combinationwith in vitro selection of invasive T-lymphomavariants. This led to the identification of the invasioninducingTiam1 gene which encodes an activator (GEF)of the RHO-like GTPase RAC. TIAM1 is highly expressedin brain and testis and at moderate levels in most otherorgans. The gene is also expressed in almost all tumor
cell lines that we have analyzed, such as B- and T-celllymphomas, melanomas, neuroblastomas and carcinomas.Overexpression of TIAM1 in NIH3T3 fibroblastscauses a flat, pancake-shaped morphology withextensive membrane ruffling and many pinocytoticvesicles, similar to V12Rac1. We have developed pulldown assays using GST-PAK- and GST-Rhotekin fusionproteins, to determine the activity state of CDC42, RACand RHO in cells, in response to receptor stimulation orectopic expression of genes. Using these assays, weconfirmed that TIAM1 predominantly regulates the activityof RAC and demonstrated an unexpected cross-talkbetween RHO family proteins, as discussed below.Moreover, we have searched for other GEF proteinscapable of activating RAC. One of the known GEFs,hPEM-2, showed a very high homology to TIAM1 withinthe catalytic DH domain. HPEM-2 is a 70 kDa proteinand features an SH3 domain followed by a DH-PHdomain combination. The gene is highly expressed in thebrain but turned out to encode a specific activator ofCDC42 instead of RAC.RHO-like GTPases and invasion of T-lymphoma cellsSimilar to TIAM1, constitutively active V12RAC inducesan invasive phenotype in T-lymphoma cells. ActivatedV12CDC42 also induces invasion of T-lymphoma cellswhich is not caused by CDC42-mediated activation ofRAC, suggesting that one of the many commondownstream signaling pathways of CDC42 and RAC isinstrumental in the induction of invasion. ActivatedV14RHOA potentiates invasion but fails, by itself, to mimicRAC and CDC42. However, C3-transferase treatmentinhibits invasion of Tiam1- and V12Rac1-transduced cells,indicating that RHOA function is required, but not sufficient.We found that TIAM1/RAC-mediated effects on theactin cytoskeleton and on cell adhesion play a major rolein T-lymphoma invasion. Expression of TIAM1 andV12RAC1 promotes integrin-mediated adhesion to varioussubstrates and correlates with invasive capacity, suggestingthat enhancing cell-substrate adhesion of lymphoidtumor cells promotes their invasion.TIAM1-RAC signaling inhibits invasion of epithelial cellsIn epithelial carcinoma cells, invasion and metastasis isoften associated with reduced E-cadherin-mediated cellcelladhesion. Ectopic expression of TIAM1 in epithelialcells inhibits HGF-induced cell scattering and cellmigration by increasing these cell-cell adhesions. Inaddition, TIAM1-RAC signaling inhibits invasion andmigration of fibroblastoid Ras-transformed MDCK(-f3)cells by restoring E-cadherin-mediated adhesion and theepithelial phenotype. Interestingly, these TIAM1/RACinducedcellular responses are dependent on integrinmediatedcell substrate interactions. On fibronectin andlaminin-1, TIAM1/RAC signaling inhibits migration ofMDCK-f3 cells by restoring E-cadherin-mediated cell-celladhesion, whereas on collagen, RAC activation promotesmotile behavior. Invasion and migration of epithelial cellsare thus determined by a balance between invasioninhibitorycell-cell interactions and invasion-promotingcell-substrate interactions, both mediated by TIAM1-RACsignaling.Antagonistic role of RAC and RHOEarlier findings suggested that TIAM1 is involved inregulating cytoskeletal reorganization required duringneuronal cell migration and/or neurite extension. Indeed,overexpression of TIAM1 induces cell spreading andaffects neurite outgrowth in N1E-115 neuroblastomacells. Cells overexpressing TIAM1 no longer respond toLPA-induced neurite retraction and cell rounding,processes mediated by RHO. We found that RAC- andRHO-mediated pathways oppose each other duringneurite formation, and that a balance between thesepathways determines neuronal morphology. We showthat RAC antagonizes RHO by regulating threoninephosphorylation of the myosin II heavy chain (MHC).This RAC-mediated phosphorylation of MHC is Ca 2+ -dependent and accompanied by cell spreading and lossof cortical myosin II. The antagonistic role of RAC andRHO in the dynamic changes of the actin-myosincytoskeleton may thus be regulated by RAC-inducedphosphorylation of the myosin II heavy chain and RHOinducedphosphorylation of the myosin II light chain.Recently we found that RAC can also antagonize RHOdirectly by downregulation of RHO activity at the level ofthe GTPase.Cross-talk between RHO family proteinsA linear activation cascade has been proposed forCDC42, RAC, and RHO as deduced from cytoskeletalchanges induced by these GTPases. By determining theactual activation state we found, however, that bothtransient PDGF-induced and sustained RAC activation byTIAM1 or V12RAC downregulate RHO activity. Activationof CDC42 can also lead to downregulation of RHOactivity. Neither V14RHO nor N19RHO affects RACactivity, suggesting unidirectional signaling from RACtowards RHO. Downregulation of RHO activity occursindependently of RAC-induced cytoskeletal changes andcell spreading. Moreover, RAC effector mutants which aredefective in inducing cytoskeletal changes or Jun-kinaseactivation both downregulate RHO activity, suggestingthat neither of these RAC signaling pathways are involvedin the regulation of RHO activity. A model on the crosstalkbetween RHO family proteins is given in Figure I.2.RHO GTPases and epithelial-mesenchymal transitionIn fibroblasts, activation of RAC by TIAM1 induces anepithelial-like morphology. TIAM1/RAC signaling promotesfunctional cadherin-based adhesions (P-cadherin and N-cadherin) and inhibits migration of fibroblasts, as demonstratedin epithelial cells. This epithelial-like phenotype ischaracterized by RAC-mediated downregulation of RHOactivity. Restoration of RHO activity in TIAM1-expressingcells by expression of V14RHO results in reversion of the25CELL BIOLOGY
26CELL BIOLOGYPublications: Genetic control of invasionGeijsen N, Van Delft S, Raaijmakers JA, Lammers JW, Collard JG,Koenderman L, Coffer PJ. Regulation of P21Rac activation inhuman neutrophils. Blood 1999; 94: 1121-30.Gimond C, Van der Flier A, Van Delft S, Brakebusch C, KuikmanI, Collard JG, Fässler R, Sonnenberg, A. Induction of cell scatteringand activation of Rho-like GTPases by expression of β1integrins in β1-deficient epithelial cells. J Cell Biol, (in press).Michiels F, Collard JG. Rho-like GTPases: their role in cell adhesionand invasion. In: Cell behaviour: control and mechanism ofmotility, Portland Press, Biochem Soc Symp 1999; 65: 125-146.Figure I.2Model showing the crosstalk of RHO-like GTPases regulating cellspreading and cell migration. For explanation see text.epithelioid phenotype towards a migratory, fibroblastoidmorphology. The reciprocal balance between RAC andRHO activity determines cellular morphology andmigratory behavior in NIH3T3 fibroblasts.The proto-oncogene Ras is frequently mutated inepithelial tumors resulting in uncontrolled growth andtransition towards an invasive, mesenchymal phenotype.In epithelial cells, we found that sustained oncogenicRAS signaling permanently downregulates RAC andupregulates RHO activity which is accompanied byepithelial-mesenchymal transition. Oncogenic RASprovokes changes in RAC and RHO activity throughsustained activation of the RAF/MAP-kinase pathway,which causes transcriptional downregulation of Tiam1.Reconstitution of RAC activity by exogenous expressionof TIAM1 decreases RHO activity and restores theepithelial phenotype in mesenchymal V12RAS- or RAF-CAAX-transformed cells. These findings reveal a novelmechanism by which oncogenic RAS regulates RAC andRHO activity to achieve epithelial mesenchymal transition.Reid T, Bathoorn A, Ahmadian MR, Collard JG. Identification andcharacterization of hPEM-2, a Guanine Nucleotide ExchangeFactor specific for Cdc42. J Biol Chem 1999; 274:33587-93.Sander EE, Collard JG. Rho-like GTPases: Their role in epithelialcell-cell adhesion and invasion. Eur J Cancer 1999; 35: 1302-8.Sander EE, Ten Klooster J-P, Van Delft S, Van der Kammen RA,Collard JG. Rac downregulates Rho activity: reciprocal balancebetween both GTPases determines cellular morphology andmigratory behavior. J Cell Biol 1999; 147: 1009-21.Stam JC, Collard JG. The DH protein family, Exchange Factors forRho-Like GTPases. In: Progress in Mol and Subcell BiolCytoskeleton and Small G proteins. Springer Verlag, 1999; 22:51-83.Van Leeuwen FN, Van Delft S, Kain HE, Van der Kammen RA,Collard JG. Rac regulates phosphorylation of the Myosin-II heavychain, actinomyosin disassembly and cell spreading. Nature CellBiol 1999; 1: 242-8.Notes1 Funding: Dr Mildred Scheel Foundation for CancerResearch, Project 683 400001.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1267.3 Funding: EEC-Bio-CT98-5060.4 Department of Biophysics.5 Funding: Netherlands Organization for ScientificResearch, Project 900-501-165.6 Funding: EEC Project ERBFMBICT971964.7 Funding: Deutsche Forschungs Gemeinschaft (DFG),SA 763/1-1.8 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1839.9 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1443
27A Sonnenberg PhDE Danen PhD 1L Fontao PhD 2HAM Geerts PhD 3C Gimond PhD 4M Nievers PhD 5,11H De Jonge MSc 6J Koster MSc 7LMTh Sterk MSc 6A Van der Flier MSc 4S Van Leeuwen MSc 9MR Van Leusden MSc 8D Kramer 4M Kreft 10I Kuikman 5P Sonneveld 1Receptors formatrix adhesionGroup leaderPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianproteins that interact with the β1D splice variant. One ofthe interacting clones, isolated from a human skeletallibrary, encodes FHL1/SLIM1, a four and a half LIM-onlyprotein. The zinc finger-like LIM motif is present in manyproteins, including homeodomain-containing transcriptionfactors, cytoskeletal proteins (e.g. paxillin and zyxin) andkinases (e.g. LIM-kinase) and mediates protein-proteininteractions. FHL1/SLIM1 is expressed at high levels inskeletal and cardiac muscle and other tissues.Immunohistochemical analysis revealed that the protein islocalized mainly at the Z-lines in striated muscle fibersand in the nuclei of myoblasts and various other celltypes. This nuclear staining probably represents anuclear-targeted FHL1/SLIM1 splice variant, as recentlyreported by others. GFP-tagged FHL1/SLIM1 is localizedin focal contacts of a subpopulation of transfected cells.Unfortunately, we could neither reproduce the binding ofβ1D to FHL1/SLIM1 nor demonstrate this interaction inbiochemical assays. In collaboration with Dr V Wixler andM Aumailley (Institute for Biochemistry, Cologne,Germany), we studied the interaction of integrins withanother member of the LIM-only protein family. We foundthat FHL2/DRAL binds to the cytoplasmic domains ofdifferent α and β subunits and is colocalized withintegrins in focal contacts.CELL BIOLOGYRole of the ß1 integrin splice variants inmechanotransductionWe generated a mouse strain in which the β1D integrinsubunit splice variant in skeletal and cardiac muscle wasreplaced by β1A. This had no effect on the histology orultrastructure of these tissues, but the mice displayedmild functional abnormalities of the heart. The levels ofatrial natriuretic peptide (ANP) and the β myosin heavychain (β-MHC) were significantly increased in theventricles. Increased expression of these proteins is alsoinduced by high blood pressure in normal mice and ispart of the physiological response to mechanical stress.There is increasing evidence that integrins are mediatorsof this response. Our findings with the β1D knockoutmice suggest that β1A is more efficient than β1D in transducingmechanical stress into biochemical signals. Toinvestigate whether the presence of β1A (instead of β1D)in combination with a high blood pressure would lead toa pathological condition of the heart, we crossed ourβ1D -/- mice with transgenic mice carrying the rat angiotensingene (collaboration with M Bader, Max-DelbrückCentrum for Molecular Medicine, Berlin, Germany).Several mice were obtained that expressed β1A insteadof β1D in skeletal and cardiac muscle and were positivefor the transgene. However, despite high blood pressure,none of these mice developed a pathological defect ofthe heart. Thus, replacement of β1D by β1A and highblood pressure do not seem to have a cumulative effect.Identification of proteins involved in integrin-mediatedsignal transductionWe used the yeast two-hybrid system to search forRole of the β4 cytoplasmic domain in hemidesmosomeformationHemidesmosomes are multiprotein complexes thatmediate adhesion of epithelial cells to the basementmembrane. The transmembrane components includeBP180 and the integrin α6β4, which connect, viaHD1/plectin and BP230, to the keratin filaments. Theα6β4 integrin, which is a receptor for laminin-5, has acentral role in hemidesmosome assembly. In patients withFigure I.3Schematic representation of a hemidesmosome, indicating themolecular interactions potentially involved in its assembly. Theα6ß4 integrin interacts extracellularly with laminin-5 and intracellularlywith plectin to form a core to which BP180 and BP230attach. The hemidesmosome is then stabilized by multipleprotein-protein interactions.
adhesion and cell scattering. In addition, we found thatexpression of β1A, β1D or IL2R-β1A in GE11 or GD25cells triggers activation of both RHOA and RAC1, but notof CDC42. Moreover, dominant-negative RAC1(N17RAC1), RHOA (N19RHOA) or CDC42 (N17CDC42)inhibited disruption of cell-cell adhesion and scatteringwhen expressed prior to β1. All three GTPases may beinvolved since expression of either N19RHOA, N17RAC1or N17CDC42 reversed cell scattering and partiallyrestored cadherin-based adhesion in GE11-β1A cells.Our results indicate that β1 integrins regulate the polarityand motility of epithelial cells, by inducing RAC- andRHO-mediated reorganization of both intercellular andECM adhesion.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2117.2 Funding: Fondation pour la Recherche Médicale (FRM).3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-979.4 Funding: Netherlands Heart Foundation, Project 96.006.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1305.6 Funding: Dutch Kidney Foundation, Project C96.1581.7 Funding: Dystrophic Bullosa Research Association.8 Funding: Netherlands Organization for Scientific Research(NWO), Project 902-11-060.9 Funding: Netherlands Heart Foundation, Project 98.044.10 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2039.11 Funding: EEC, Project CHRX-CT97-2062.Publications: Receptors for matrixadhesionBorradori L, Sonnenberg A. Structure and function of hemidesmosomes:more than simple adhesion complexes. J InvestDermatol 1999; 112:411-8.Cohn RD, Mayer U, Saher G, Herrmann R, Van der Flier A,Sonnenberg A, Sorokin L, Voit T. Secondary reduction of a7Bintegrin in laminin α2-deficient congenital muscular dystrophysupports an additional transmembrane link in skeletal muscle. JNeurological Sci 1999; 163: 140-52.De Melker AA, Sonnenberg A. Integrins: alternative splicing as amechanism to regulate ligand binding and integrin signalingevents. BioEssays 1999; 21:499-509.Geerts D, Fontao L, Nievers MG, Schaapveld RQJ, Purkis T,Wheeler GN, Lane EB, Leigh IM, Sonnenberg A. Binding of integrinα6β4 to plectin prevents plectin association with F-actin butdoes not interfere with intermediate filament binding. J Cell Biol1999; 147: 417-34.Gimond C, Van der Flier A, Van Delft S, Brakebusch C, KuikmanI, Collard JG, Fässler R, Sonnenberg, A. Induction of cell scatteringand activation of Rho-like GTPases by expression of β1integrins in β1-deficient epithelial cells. J Cell Biol, (in press).Nievers M, Schaapveld RQJ, Sonnenberg A. Biology and functionof hemidesmosomes. Matrix Biol 1999; 18:#5-17.Sonnenberg A, Nievers M, Schaapveld RQJ, Geerts D, NiessenC, Borradori L. Interaction of BP180 and α6β4. J Invest Dermatol1999; 112: 830-2.Van der Neut R, CachaHo AS, Thorsteinsd\ttir S, Gimond C,Janssen H, Prins D, Bulthuis, J Van der Valk M, Calafat J,Sonnenberg A. Partial rescue of epithelial phenotype in integrin β4null mice by a keratin-5 driven human integrin β4 transgene. J CellScience 1999; 112: 3911-22.Wixler V, Laplantine E, Geerts D, Sonnenberg A, Petersohn D,Eckes B, Paulsson M, Aumailley M. Identification of novel interactionpartners for the conserved membrane proximal region ofintegrin a cytoplasmic domains. FEBS Lett 1999; 445: 351-5.K Jalink PhDJ Van der WalR HabetsBiophysicsin cell signalingGroup leaderTechnicianUndergraduate studentCellular signals that are either very local or short-livedcan easily escape detection by conventional biochemistry.A detailed understanding of these signals requirestechniques to study cellular processes with high spatiotemporalresolution in single living cells. Biophysicaltechniques (electrophysiology, microspectrometry, flashphotolysis) offer this high resolution, but were, until recently,limited to parameters such as membrane potential andintracellular ion concentrations. The introduction of GreenFluorescent Protein (GFP) has rapidly increased the numberof parameters that can be monitored, by protein tagging. Inaddition, spectral GFP mutants allow direct imaging ofmolecular interactions in the cell by Fluorescent ResonanceEnergy Transfer (FRET). FRET occurs when suitable donorand acceptor fluorophores come into close proximity, andserves as a cellular ‘ruler’ with Ångström resolution. Wehave established a biophysical laboratory with the sensitiveequipment to study these phenomena, and have characterizedthe physicochemical behavior of FRET between twowavelength-shifted GFP mutants (the Cyan-FP/Yellow-FPFRET pair).Detection of membrane phosphatidylinositolbisphosphate (PIP2) levels in vivo in single cellsInositolphospholipids in the plasma membrane playimportant roles in many signaling events. Upon activation,29CELL BIOLOGY
30CELL BIOLOGYphospholipase C cleaves PIP2 to yield the secondmessengers diacylglycerol (DAG) and inositol-trisphosphate(IP3). PIP2 itself also has a signaling role, inparticular in the regulation of the cytoskeleton. In vitro, itbinds to a number of cytoskeletal proteins, includinggelsolin, ezrin, cortactin and profilin. In the dynamiccytoskeleton, signals are short-lived and localized, andthus need to be investigated with high resolutiontechniques in living cells.We have adapted a strategy that uses a fusionconstruct of GFP with the PIP2-binding pleckstrinhomology (PH) domain from PLC-γ1 (GFP-PH). Upontransfection with this construct, cells are imaged usingconfocal microscopy. At rest, the construct binds toPIP2, and cells show a brightly fluorescent plasmamembrane. Following stimulation with agonists, PIP2 ishydrolyzed and GFP fluorescence rapidly translocates tothe cytosol. Translocation is complete within 10 seconds.Subsequently, the majority of GFP-PH gradually returnsto the membrane in 2-5 minutes.In line with a localized signaling role, GFP-PH fluorescencedoes not appear to be distributed uniformly overthe membrane. We observed enhanced fluorescence inlamellipodia, filopodia and growth cones, as well as brightisolated patches throughout the membrane. PIP2 spotsare dynamic, showing slow changes in size and location.When cells are stimulated with bradykinin, the spotsdisappear from the membrane. Remarkably, after desensitizationof the signaling cascade, PIP2 reappears at thesame ‘hot spots’. These spots thus reflect the existenceof functionally specialized ‘lipid patches’ in the membrane(opposing a view in which PIP2 is distributed uniformly inthe membrane by passive diffusion). Origin and cellularfunction of these patches are currently under study.Improved PIP2 sensing using FRETBefore PH-domain sensing can be routinely used toimage PIP2 in vivo, a number of potential pitfalls have tobe addressed. First, local enrichment in GFP-PH conceivablyreflects local differences in PIP2 accessibility ratherthan concentration. Second, on and off rates depend, atleast in part, on diffusion of GFP-PH, limiting the timeresolution to seconds. Third, the specificity for PIP2 overother cellular molecules has to be rigorously demonstrated.We are currently addressing the first two issuesby exploiting the FRET principle. We constructed a novelsensor that remains attached to the plasma membrane atall time and exhibits intramolecular FRET as a function ofmembrane PIP2 content. This sensor is distributeduniform over the PM and reports local PIP2 concentrationas a shift in emission wavelength, thus demonstrating theexistence of PIP2 patches. This construct will function asa template for the development of other lipid sensors bysubstituting the PH domain with protein motives withdifferent specificity. FRET sensing also exhibits superiortime resolution (Figure I.4). The potential of this approachto increase throughput of in vitro lipid biochemistry is alsobeing investigated.Publication: Biophysics in cell signalingMiyawaki A, Llopis J, Mizuno H, Jalink K, Tsien RY. Cameleons ascytosolic and intra-organellar calcium probes. In: CalciumSignalling: A Practical Approach, Oxford University Press (in press).Immuno EM facilityFigure I.4FRET-based PIP2 sensing. A. A single cell expresses both CFP-PH and YFP-PH. Initially, both chimeras are bound to membranePIP2 and thus located within FRET range. During PIP2 hydrolysis,the constructs dilute out into the cytosol and FRET ceases.B. Simultaneous emission recording at 475 nm and at 530 nmfrom a N1E-115 neuroblastoma cell, excited at 430 nm. Theratio between these two signals (lower trace) depicts PIP2content.J Calafat PhDJWRM JanssenAcademic staffTechnicianImmuno-EM study on ARF6 and RAC1-mediated rufflingin macrophages 1Activation of RAC1, a member of the RHO family ofGTPases, is associated with multiple cellular responses,
35animals (31/19). In contrast to Msh2-deficient animals,post-replicative DNA mismatch repair (MMR). This systemMsh6 -/- animals (9/12) was as high as that in Msh2 -/- single unpaired nucleotides are preferentially targeted byrecognizes and restores mismatched nucleotides that canarise by erroneous DNA replication, bypass replication ofdamaged DNA or incorporation of modified nucleotides.In addition, mismatches can arise in heteroduplex regionsMsh6-deficient mice only rarely developed intestinaltumors: two were found among 22 animals at a meanage of 52 weeks. Msh3 deficiency did not predispose tocancer, nor did it accelerate lymphomagenesis in Msh6-that are formed at initial stages of recombination between deficient animals. However, combined Msh3/Msh6-homologous but non-identical DNA molecules. Mismatch deficiency strongly predisposed to development ofrecognition activity in mammalian cells is attributed to twoheterodimeric protein complexes composed of differentMutS homologs (referring to the paradigmatic Escherichiacoli mutS,L postreplicative MMR system): MutSα, a dimerof MSH2 and MSH6, and MutSβ, a dimer of MSH2 andMSH3. These complexes have specific and redundantintestinal tumors, which were found in eight out ofthirteen Msh3-/-Msh6-/- animals at a mean age of 30weeks (Figure II. 2).In addition to mutation avoidance, we have previouslydemonstrated two additional functions of MMR in EScells. 1) Msh2 deficiency caused tolerance to methylatingmismatch recognition capacity. Thus, while MSH2 agents; 2) In wild-type ES cells, but not in Msh2-deficientdeficiency ablates the activity of both dimers, leading to cells, homologous recombination was stronglystrong cancer predisposition in mice and men, loss ofeither MSH3 or MSH6 function only causes a partialMMR defect with possibly less severe consequences.This may explain the rarity of MSH6 and absence ofMSH3 germline mutations in HNPCC families. To test thishypothesis, we have studied the phenotypic consequencessuppressed by base sequence divergence as small as0.6%. We now observed that Msh6 deficiency alsocaused loss of mismatch-dependent anti-recombination,whereas Msh3-deficient cells behaved identically to wildtypecells. Furthermore, we found that Msh6 deficiency,but not Msh3 deficiency, caused tolerance to N-methylmouseof single and combined homozygous defects in N'-nitro-N-nitrosoguanidine. Thus, besides redundantMsh3 and Msh6 genes. Msh6-deficient micewere highly cancer prone, the majority of animalsdeveloping lymphomas or epithelial tumors originatingfunctions, Msh6 also has specific functions that are notshared with Msh3.Previous studies by others have addressed thefrom the skin and uterus. Most lymphomas appeared mismatch recognition capacity of Msh2/Msh3 andwithin 30 weeks; in this period the tumor incidence in Msh2/Msh6 complexes: base/base mismatches andMutSα, while MutSa and MutSβ are redundant in looprepair with possibly some specificity of MutSb for larger(four/five nucleotides) loops. The activity of MutSβtowards single nucleotide loops is controversial, withsome assays contradicting and others supporting MutSbdependentrepair capacity. Moreover, we observed inMsh6 -/- cells residual binding activity to DNA oligonucleotidesequences carrying a G/T mismatch or an unpaireddinucleotide, which completely disappeared on concomitantinactivation of Msh3. Thus, both MutSa andMutSβ can bind to G/T and extrahelical dinucleotidemismatches, whereas free Msh2 can not. AlthoughMutSa activity exceeds that of MutSβ, on an equimolarbasis the two complexes appear to have similar affinitiesfor both types of mismatches. This may be indicative ofat least some base/base mismatch repair capacity ofMutSβ. Our data demonstrate two MMR functions to bespecific for Msh6: mismatch-dependent anti-recombinationand mediation of toxicity of methylating agents.Since lack of MutSα alone is sufficient to cause strongpredisposition to development of lymphoid tumors andepithelial tumors of the uterus and skin, these tumorsapparently ensue from genetic alterations that are specificallysuppressed by MutSα function. These may includepoint mutations, or perhaps frameshifts in runs ofFigure II. 2Tumor susceptibility of mismatch repair deficient mice. Msh6-deficient mice are highly cancer prone; however, intestinaltumorigenesis in these animals requires simultaneous loss ofMsh3.mononucleotides, but also methylation-damage-inducedpoint mutations and mitotic recombination events. On theother hand, the redundancy of MutSa and MutSβfunctions was hypothesized to account for the rarity ofMSH6 and lack of MSH3 germ line mutations in HNPCCMOLECULAR CARCINOGENESIS
36MOLECULAR CARCINOGENESISfamilies. This view is supported by our studies in mice:simultaneous loss of MutSα and MutSβ activity isrequired to induce intestinal tumors. Thus, specificmutations, presumably frameshifts that are suppressedby MutSβ, are rate limiting in intestinal carcinogenesis.Based on these observations, we speculate that familiessegregating a defect in MSH6 are cancer-prone but oftennot recognized as HNPCC families due to suppression ofintestinal tumorigenesis by MutSβ activity.The retinoblastoma gene family 3Loss of function of the retinoblastoma suppressor pRBis a common event in the development of many tumortypes in humans. pRB belongs to the family of so-called‘pocket proteins’ which also includes p107 and p130.These proteins may functionally overlap in blockingprogression through the cell cycle in response toexogenous factors. Indeed, we found evidence forfunctional overlap of tumor suppression functions of pRband p107 in mice: development of retinoblastomarequired simultaneous ablation of both proteins. Sinceearly embryonic lethality associated with pRb deficiencyin mice precluded a study of the consequences of pRbdeficiency at later developmental stages and adulthood,we choose an alternative approach. We generatedembryonic stem (ES) cell lines carrying inactivatingmutations in Rb alone and in both Rb and p107, andstudied of their developmental and tumorigenic capacityin chimeric mice. While Rb -/- chimeras developednormally into adulthood, most Rb -/- ;p107 -/- chimericembryos died in utero. Surviving chimeras, however,developed retinoblastoma. This result shows that in mice,p107 acts as a suppressor of oncogenic transformationof pRb-deficient retinoblasts and is the first demonstrationthat p107 can act as a tumor suppressor. Thisresult also demonstrates that the chimera approachprovides a powerful tool to study the consequences ofcombinations of mutations, which in normal crossingswould cause embryonic lethality. To further optimize thisapproach, genetically modified ES cells were labeled witha ubiquitously expressed LacZ marker gene, whichallows their descendants to be precisely traced inchimeric mice. This refinement allowed us to demonstratethat the vast majority of Rb/p107-deficient retinoblastsdisappeared from the developing retina throughapoptosis. We speculate that retinoblastomadevelopment requires at least one additional event thatcounteracts apoptotic cell death.We have now generated an isogenic panel of LacZlabeledES cell lines with the following genotypes: wildtype, Rb-/-; double knockouts Rb -/- ;p107 -/- , Rb -/- ;p130 -/-and p130 -/- ;p107 -/- and triple knockout Rb -/- ;p107 -/- ;p130 -/- . None of these genotypes affected the growthpotential or characteristics of ES cells. Unlike wild-typeES cells, the triple knockout cells failed to arrest upon invitro induction of differentiation, yielding a cell line withhigh growth potential. Also, unlike ES cells, these cellshad lost the capacity to grow in nude mice, suggestingthat some sort of acquired tumor suppressor functionsubstituted for the absence of pRb family members.We are currently studying the interplay between pRb,p107 and p130 control pathways in development andoncogenic transformation by following the fate of mutantES cells in chimeric embryos. The proliferative capacity ofthese cells will be assessed by combining LacZ stainingwith BrdU incorporation and apoptosis assays on histologicalsections. Specific antibodies will be used to identifyspecific cell types. In addition, we have used mutant EScells to derive primary mouse embryonic fibroblasts(MEFs) from mid-gestation chimeric embryos, takingadvantage of the presence selectable marker genes inmutant but not blastocyst-derived cells. MEFs could beobtained from all genotypes including the triple knockout.Thus far, we observed that all single and doubleknockouts underwent replicative senescence uponprolonged passaging which, like in wild-type cells, wasassociated with increased levels of p19. Interestingly, inlate passage Rb -/- ;p107 -/- MEFs foci developed withenhanced growth capacity apparently as a result of anadditional mutagenic event. This phenomenon was notobserved in any of the other double knockout combinations.Triple knockout cells, however, appeared to beimmortal from the beginning and grew to high density,despite abnormally high levels of p19. Thus, ablation ofall three pocket proteins causes resistance to replicativesenescence. We will use mutant MEFs to determine theeffect of each genotype on the response of cells to alarge number of growth inhibiting conditions and theirsensitivity to oncogenic transformation.Detailed knowledge of the function of each of thepocket proteins in cellular growth control will provideinsight into the question why abrogation of this pathwayis a mandatory step in the development of human cancer.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-958.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1838.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-956.Publications: Mouse models forhereditary cancerClaij N, Te Riele H. Microsatellite instability in human cancer: aprognostic marker for chemotherapy? Exp Cell Res 1999; 246: 1-10.Claij N, Van Klink Y, Dekker M, Jansen L, Beijnen J, Te Riele H.Interactions of DNA mismatch repair and DNA damage: implicationsfor the etiology and treatment of cancer. Mutat Res (inpress).De Vries SS, Baart EB, Dekker M, Siezen A, De Rooij DG, De BoerP, Te Riele H. Mouse MutS-like protein Msh5 is required for properchromosome synapsis in male and female meiosis. Genes &Dev. 1999; 13: 523-31.
De Wind N, Dekker M, Claij N, Van Klink Y, Radman M, RigginsG, Van der Valk M, Van ‘t Wout K, Te Riele H. HNPCC-like cancerpredisposition in mice through simultaneous loss of Msh3 andMsh6 mismatch-repair protein functions. Nat Genet 1999: 23;359-62.Jansen L, Claij N, Dekker M, Van Klink Y, Van der Valk M,Van ’t Wout K, Te Riele H. Acceleration of lymphomagenesis inmismatch-repair deficient mice by exposure to genotoxic agents.Toxicology Letters (in press).Toft NJ, Winton DJ, Kelly J, Howard LA, Dekker M, Te Riele H,Arends MJ, Wyllie AH, Margison GP, Clarke AR. Msh2 statusmodulates both apoptosis and mutation frequency in the murinesmall intestine. Proc Natl Acad Sci USA 1999; 96: 3911-15.Bmi1, M33, Ring1b and Mll, respectively. We havepreviously shown that BMI1 interacts with M33, MPH1,RING1b and other Pc-G proteins in large complexes.More recently, we identified a separate Pc-G complex,containing ENX1, ENX2 and EED, that is required duringearly development when Pc-G repression is initiated. Werecently investigated the subnuclear distribution andchromatin association of BMI1-containing Pc-G complexesin detail, using a combination of sensitive immunohistochemicalmethods and biochemistry. In primary humancells, BMI1 shows a fine-grain distribution over chromatin,whereas additional large subnuclear domains are observedin tumor cell lines. These were identified as associationswith distinct heterochromatic regions of certain chromo-37MOLECULAR CARCINOGENESISRole of mousePolycomb-groupgenes intranscriptionalrepression andtumorigenesisM Van Lohuizen PhDP Keblusek PhD 1A Lund PhD 2M C Motta PhD 3J W Voncken PhD 4JJL Jacobs MSc 5K Kieboom 5, 6E VerhoevenM Verlaan 1E WientjensGroup leaderPost-docPost-docPost-docPost-docGraduate studentTechnicianTechnicianTechnicianTechnicianWe are studying the mechanism of stably inheritedtranscriptional repressed- or activated states of individualtarget genes by respectively the Polycomb-group (Pc-G)and Trithorax-group (Trx-G) protein complexes in themouse, and the effects of deregulation of Pc-G andTrx-G genes on Homeobox (Hox) gene expression,development, cell cycle control and tumorigenesis.Functional and Biochemical characterization of Bmi1 andassociated Pc-G protein complexes 4, 5Bmi-1was found as an oncogene that synergizes withc-Myc in mouse B and T cell lymphomagenesis. Bmi1 isthe first example of the expanding mouse Polycomb-grouptranscriptional repressor family. Pc-G proteins and thecounteracting Trithorax-group (Trx-G) of nucleosomeremodeling factors are involved in maintenance of propergene expression patterns during development at the levelof chromatin structure. Important targets include the Hoxgene clusters and critical cell cycle regulatory genes (seebelow and Figure II. 3). To study Pc-G and Trx-G functionwe focus on representative members of these groups:Figure II. 3How Polycomb-group proteins connect to cell cycle regulation.Pc-G complexes recognize specific binding sites (PREs,Polycomb-responsive elements) and form, through an as yetpoorly understood mechanism, a stable, repressive chromatinstructure on specific target genes. Our recent results identifiedthe tumor suppressors p16 and p19Arf as critical cell cycletargets for Pc-G. Unbalanced mitogenic signaling mediated bythe activation of oncogenes such as cMYC and H-RAS activateas a fail-safe mechanism these cell cycle repressors in normalcells, leading to senescence or apoptosis, rather than immortalization.In contrast, Pc-G complexes act to repress this tumorsuppressor locus. Overexpression of the Pc-G protein Bmi1leads to inadvertant downregulation of p16 and p19Arf, leadingto immortalization and powerful cooperation with cMYC and H-RAS in tumorigenesis, whereas inhibition of Pc-G function bydeleting Bmi1 leads to overexpression of p16 and p19Arf andinduces premature senescence.
38MOLECULAR CARCINOGENESISsomes. We recently discovered a marked cell cycleregulation of Pc-G-chromatin interaction: nuclear Pc-Gstaining dissipates in late S-phase and is rapidly reestablishedin early G1 phase. Chromatin association ofBMI1 and MPH1 inversely correlates with their phosphorylationstatus: at G1/S hypophosphorylated BMI1 andMPH1 is present in chromatin-associated nuclear proteinfractions, whereas during G2/M, hyperphosphorylatedBMI1 and MPH1 complexes dissociate from chromatin,although a small but significant fraction of BMI1 remainsassociated with specific sites on mitotic chromosomes.These results provide new insights in the dynamicregulation of Pc-G complex-chromatin association, andsuggest that extra-cellular cues may influence thisprocess through kinase/phosphatase pathways (collaborationwith D Schweizer, University of Vienna).Generation and phenotypic analysis of new Polycomb-groupmutant mice and genetic interactions of Pc-G and Trx-G4, 5, 6We and others recently identified RING1b as a novelPc-G member. RING1b interacts with a number of Pc-Gproteins, including BMI1. For this interaction, the RINGfinger domains of both proteins are essential. To investigatethe function of Ring1b null mutant mice have beengenerated (collaboration with P Krimpenfort and A Berns,Division VII). Unlike other single Pc-G gene knockout mice(which display various defects but are viable, see below),Ring1b null mutant mice die shortly after gastrulation (day8-9). This may relate to the central positioning of theRING1b protein in the Pc-G complex, and in additionsuggests that the closely related Ring1a gene cannotcompensate for loss of Ring1b. This severe phenotyperesembles that of the Eed null mutant mice (the only Pc-Ghomolog known so far to be represented by a single gene),and suggests that loss of Ring1b results in complete lossof Pc-G function. This phenotype is being studied in detailby in situ hybridization with early developmental markers(In collaboration with J Deschamps, Hubrecht laboratory,Utrecht). In addition, we are generating Ring1b-conditionalknockout mice, which will be a valuable tool tostudy Pc-G function in relation to differentiation anddevelopment in a timed and cell type specific manner.To address the opposing roles of Pc-G and Trx-G invivo, we collaborate with S Korsmeyer (Dana Farber,Boston). Recent results of this study, investigating theeffects of combining Bmi1 and Mll (a Trx-G gene)mutations in mice, showed that Bmi1/Mll doubleknockout mice display a partial restoration of some of theHox gene expression boundaries. This confirms thenotion that also in mammals, Trx-G and Pc-G complexesact in opposition on specific (Hox) target genes.Pc-G genes and cell cycle regulation1, 5, 6Bmi1 transgenic mice have expanded pro-B andpro-T cell compartments, culminating in a high incidenceof B and T cell lymphomas. In contrast, Bmi1 knockoutmice show severe proliferative defects of lymphoidand myeloid cells, resulting in severe lymphopenia.Proliferation defects are not restricted to lymphoid cells:primary embryo fibroblasts (MEFs) and neurons in thecerebellum of Bmi1 knockouts also show such defects,resulting in neurological disorders. We recently found thatthese defects are due to increased levels of the INK4aencodedtumor suppressors p16 and p19Arf, that arecritical regulators of the Cyc.D/CDK4,6;pRB and the p53tumor suppressor pathways (see Figure II. 3). Conversely,overexpression of Bmi1 facilitates immortalization, andneoplastic transformation by repressing p16 and p19Arf.The dramatic rescue of defects and proliferative capacityin INK4a/Bmi1 double knockout mice proved that p16and p19Arf are prime targets of BMI1. This connects Pc-G repression to cell cycle control and control of the replicativesenescence checkpoint governed by these tumorsuppressors. We have shown that loss of cellularity inBmi1 knockouts is caused by INK4a/Arf-inducedapoptosis. Moreover, we found that the basis for strongco-operativety between Bmi1 and cMyc in tumorigenesisis the capacity of Bmi1 to repress p19Arf-mediatedapoptosis. In addition, we found clear dosage effects ofp16/p19Arf in controlling proliferation and apoptosis, andshowed that loss of p16/p19Arf prevents apoptosis uponmatrix-detachment of Myc+Ras transformed MEFs. Toelucidate the molecular mechanism of Pc-G repression,we are studying the INK4a locus as a relevant in vivotarget, for the presence of Pc-G responsive elements andPc-G-associated alterations in chromatin structure.Genetic screens to identify new regulators of cellularsenescenceWe have made use of the tight premature senescencearrestof Bmi1 knockout MEFs, to screen for mutations oroverexpressed cDNAs that can bypass the p16/p19Arfmediatedarrest. Application of MuLV proviral-insertionalmutagenesis resulted in immortalized cell clones; these arecurrently being screened for common insertion sites. In aseparate approach using tumor-derived retroviral cDNAlibrary transductions, we identified at least five cDNAs otherthan Bmi1 that are capable of potently immortalizing Bmi1-null mutant MEFs (collaboration with G Daley, WhiteheadInstitute, Cambridge, USA). The first of these cDNAsanalyzed in detail, revealed a potent transcriptionalrepressor of p19Arf. The role and mechanism of action ofthese putative oncogenes, and their interference with thecellular senescence/anti-immortalization ‘fail-safe’ in mouseand human cells, is the topic of intensive study.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2056.2 Funding: Danish Medical Research Council.3 Funding: EC-Marie Curie training fellowship, ProjectMCFI-1999-01131.4 Funding: Netherlands Organization for ScientificResearch (NWO-ALW), Project 805-17.541.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-970.6 Funding: Netherlands Organization for Scientific Research(NWO-MW) PIONIER, Project 0705/906-99-001.
Publications: Polycomb-group genesin transcriptional repression andtumorigenesisHanson RD, Hess JL, Yu BD, Ernst P, Van Lohuizen M, Berns A,Van der Lugt NMT, Shashikant CS, Ruddle FH, Seto M,Korsmeyer J. Mammalian Trithorax and Polycomb-group homologsare antagonistic regulators of homeotic development. ProcNatl Acad Sci 1999; 96: 14372-8.Jacobs JLJ, Kieboom K, Marino S, DePinho RA, Van Lohuizen M.The oncogene and Polycomb-group gene Bmi1 regulates cellproliferation and senescence through the INK4a locus. Nature1999; 397: 164-8.Jacobs JLJ, Van Lohuizen M. Cellular memory of transcriptionalstates by Polycomb-group proteins. Cell & Dev Biol 1999; 10:227-35.Jacobs JLJ, Scheijen B, Voncken J-W, Kieboom K, Berns A, VanLohuizen M. Bmi-1 collaborates with c-Myc in tumorigenesis byinhibiting c-Myc induced apoptosis via INK4a/ARF. Genes & Dev1999; 13: 2678-90.Lessard J, Schumacher A, Thorsteinsdottir U, Van Lohuizen M,Magnuson T, Sauvageau G. Functional antagonism of thePolycomb-Group genes Eed and Bmi1 in hemopoietic cell proliferation.Genes & Dev 1999; 13: 2691-703.Van Lohuizen M. The trithorax-group and Polycomb-group chromatinmodifiers: implications for disease. Curr Opin Genet Dev1999; 9: 355-61.Voncken JW, Schweizer D, Aagaard L, Sattler L, Jantsch MF, VanLohuizen M. Chromatin-association of the Polycomb group proteinBMI1 is cell cycle regulated and correlates with its phosphorylationstatus. J Cell Science 1999; 112: 4627-39.TK Sixma PhDK Brejc PhD 1L Jovine PhD 2P Knipscheer MSc 3M Lamers MSc 4J Enzlin 4D Van der Riet 2WJ Van DijkH WinterwerpProteinCrystallographyGroup leaderPost-docPost-docGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianDevelopment of cancer is generally due to errors inmolecular pathways. Structural biology can help tounderstand these errors at the atomic level, by studyingthe proteins and the DNA involved. We use X-ray crystallographyas a tool to provide three-dimensional structures.These will provide more insight in the molecularprocesses, but they can also be of great help indesigning new drugs. In our group we focus mainly onproteins involved in DNA stability (transposition, mismatchrepair) and in cell cycle control.Structure of proteins in cell cycle control 2, 3Cyclin D1 is an important regulator of the cell cyclebecause of its effect on cyclin dependent kinases (CDKs).Recently, however, R Zwijsen in this institute showed thatcyclin D1 can also positively regulate the estrogenreceptor in a CDK-independent fashion and may thushave an additional role in regulating growth of breastepithelial cells. Up-regulation of estrogen receptor activityis a consequence of the direct physical interaction ofcyclin D1 with the ligand-binding domain of the estrogenreceptor. This binding and activation is seen both in thepresence and absence of estrogens and anti-estrogens.Interestingly, cyclin D1 can also bind directly to theestrogen receptor coactivator SRC1. This suggests thatcyclin D1 can act as a bridging factor between theestrogen receptor and its coactivators in the absence ofhormone. This mechanism of estrogen receptor activationcould contribute to growth of cyclin D1 amplified breastcancers, especially those that are refractory to the antiestrogen tamoxifen The interaction between cyclin D1and the estrogen receptor and its coactivators aretherefore attractive drug targets. We initiated the crystalstructure determination of the cyclin D1/estrogenreceptor ligand-binding domain in the presence offragments of coactivator. Since cyclin D1 is a very labileprotein it is difficult to produce it in sufficient quantities.Therefore we have resorted to coexpression of the threepartners that we want to co-crystallize.Ubiquitin-mediated targeting is a mechanism for transmittingvarious signals in the cell, such as controlledbreakdown of short-lived cellular proteins and targeting tothe nucleus. Ubiquitin attachment is regulated through aubiquitin-activating enzyme E1, a ubiquitin conjugatingenzyme E2 (or Ubc) and a ubiquitin ligase E3. We havesolved the structure of Ubc9, an E2 protein. Despite thefact that several E2 structures are known, the precisedetails of the regulation are not understood at the atomiclevel. The G1/S transition in the cell cycle is regulated bybreakdown via the ubiquitin conjugating enzyme Ubc3(Cdc34) and an E3 ligase, consisting of Skp1, a Cullinhomolog (Cdc53) and an F-box protein (e.g., Cdc4, Grr1,Skp2). In this E3-ligase complex or SCF, the F-boxprotein is thought to mediate the target specificity. Inhumans cyclin A/CDK2 is part of this complex. We aimto determine the structures of the proteins in thisubiquitin-mediated pathway, in order to understandubiquitin transfer in atomic detail.39MOLECULAR CARCINOGENESIS
40MOLECULAR CARCINOGENESISStructure determination of mismatch repair proteins 4Mutations in DNA mismatch repair genes predisposefor the most prevalent type of familial cancers, hereditarynon-polyposis colon carcinoma (HNPCC). This type ofDNA repair is specific for a single mismatch or a smallstretch of unpaired bases in DNA. It involves a cascadeof proteins that is highly conserved from bacteria tohumans. The initial step of the repair is the recognitionand binding of mismatched DNA by the MutS protein (E.coli) or its homologs (eukaryotes). This complex is thenrecognized by the MutL protein or its homologs.Although the proteins involved are known, it is unclearhow even subtle mutations, as they are found in someHNPCC tumors, which involve the change of a singleconserved amino acid in MSH2, can cause a deficiencyin mismatch repair resulting in cancer.We study the structure/function relation of MutS, MutLand the eukaryotic homologs in detail by determining theX-ray structure of the proteins, alone and in complex withmismatched DNA. We have obtained crystals of MutS incomplex to a mismatched DNA oligomer, diffracting to2.7 Å. Initial problems in reproduction of the crystals havebeen overcome and an extensive derivative search hastaken place, using both MIR and MAD derivatives. Nonisomorphism,pseudo-symmetry and twinning as well asthe size of the complex (~230 kDa or 460 kDa in theasymmetric unit) are complicating the structure determination.Currently, systematic variation of crystallizationconditions is used to improve the isomorphism of thecrystals for solving the phase problem. Meanwhile we arestudying the ATPase activity by mutations of the activesite.Crystal structure of the DNA binding domain of Tc3transposase in complex with DNATransposable elements are small stretches of DNA thatcan move from one position in the genome to another.Excision and insertion of the transposon DNA into thegenome is performed by the transposase protein, whichis encoded by the transposon. The initial step in theprocess is recognition and binding of the transposase tothe transposon DNA. In collaboration with the group of RPlasterk (Division V), we are extending our studies intothe DNA binding domain of the Tc3 transposase (FigureII. 4). Crystals have been obtained of the bipartite DNAbinding domain complexed to a 25-mer fragment oftransposon DNA. Meanwhile we are studying the crystalstructure of full-length Tc1.Notes1 Funding: Technology Foundation STW VBI.4568.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2052.3 Funding: Netherlands Organization for ScientificResearch (NWO-MW): Project 901-02-223.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1279.Secretary Molecular CarcinogenesisM SonneResearch staff positions (full time equivalents)Scientific permanent 4.0Scientific project 23.0Technical permanent 4.8Technical project 11.0Figure II. 4Dimer of DNA binding domains of transposase Tc3A bound totransposon DNA, as seen in the crystal structure. Further analsisis required for determining the biological relevance of this dimerization.
III Division of CellularBiochemistry41Division head Wouter MoolenaarIntroductionMajor research topics in the Division of CellularBiochemistry concern the mechanisms of signal transductionvia cell surface receptors, particularly in thecontext of cell proliferation, differentiation and survival,and the role of lipid messengers, nuclear phosphoinositidesand Smad transcription factors in determining cellbehavior. The division comprises five research groups,each headed by a permanent staff member: J Borst,N Divecha, P Ten Dijke, W Moolenaar and W VanBlitterswijk.The group of Moolenaar investigates the multipleactions of the serum-borne mitogen lysophosphatidicacid (LPA). LPA acts through specific G protein-linkedreceptors belonging to the so-called Edg receptor family,which couple to activation of the Ras and Rho GTPasesto stimulate cell proliferation and changes in cellmorphology, respectively. Mitogenic signaling by LPA andother growth factors was shown to depend on dynamin,a key regulator of endocytosis. Dynamin function wasfound to be critical during the last step in the Ras-MAPkinase cascade. LPA signals through at least threedistinct Edg receptors. Interestingly, the Edg-2 receptorwas found to couple to activation of the Rac GTPase,thereby promoting cell spreading, whereas other LPAreceptors preferentially couple to the Rho GTPase tostimulate cell contraction. Rho/Rac signaling is thought tobe fundamental to tumor cell invasion. Newly identifiedRho-binding proteins include a Rho-specific GDP/GTPexchange factor (p190RhoGEF) which binds to activatedGα q, and a ‘scaffold’ protein (p116Rip) that binds f-actinand probably participates in cytoskeletal responses toLPA. Furthermore, LPA receptors couple to activation ofrapid conductance changes, notably an increase inchloride conductance that was found to be mediated bythe G 13 protein. LPA also inhibits connexin-based gapjunctional communication between adjacent cells,apparently via a Gαq signaling pathway involving bothprotein tyrosine kinase and phosphatase activity. Sinceimpaired cell-cell communication is a hallmark of transformedcells, elucidation of how LPA regulates connexinfunction is of obvious importance.The group of J Borst studies the regulation oflymphocyte activation and survival. Central is the analysisof antigen receptor signaling and its interplay with signalingby members of the tumor necrosis factor (TNF) receptorfamily. With the discovery of c-Cbl as an antigen receptorsubstrate, the group has entered the field of receptorubiquitination and endocytosis. This line will be pursued,since it is becoming evident that regulated protein degradationis an important regulatory principle in signal transduction.Within the TNF receptor family, there are bothdeath and survival promoting receptors such as CD95 andCD27, respectively. Variant T cells have been identified thatfail to undergo CD95-mediated apoptosis. These cells areinhibited in the apoptosis signaling pathway at a newlydefined control point, upstream from the mitochondria. It isthe aim to identify both facilitating and inhibitory componentsin the trajectory leading to mitochondrial activation.In collaboration with the Van Blitterswijk group, it wasestablished that ceramide does not play a secondmessenger role in this pathway. Instead, ceramideproduction was found to be secondary to redistribution ofplasma membrane sphingolipids during the apoptoticeffector phase. Finally, analysis of CD27-deficient mice hasrevealed that CD27 does not promote antigen receptorinducedcell cycle progression but mediates T cell survival.The molecular basis of this effect is currently under study.Van Blitterswijk and coworkers established that a newlycloned diacylglycerol kinase is a downstream target ofRhoA and, furthermore, is found in both the cytosol andthe nucleus. The latter finding raises the interesting possibilitythat diacylglycerol metabolism may play a role innuclear signaling. Furthermore, in a collaborative projectwith M Verheij (Division IX), it was found that certain alkyllysophospholipids,used in the clinic as anti-canceragents, trigger stress pathways and apoptosis in tumorcell lines, apparently by interfering with phosphoinositidemetabolism at the plasma membrane.Other aspects of lipid signaling are explored by NDivecha and coworkers. This group studies phosphoinositidemetabolism in the nucleus, particularly the role ofinositol lipid kinases therein. While the exact function ofinositol lipids in the nucleus is not yet clear, it seemslikely they play an important role in transmitting signalsfrom the cytosol to the nucleus.In September 1999, we welcomed our new staffmember P Ten Dijke (formerly the Ludwig Institute forCancer Research, Uppsala, Sweden). Research in the
42CELLULAR BIOCHEMISTRYTen Dijke group will focus on TGF-β serine/threoninekinase receptors and their intracellular effectors, termedSmad proteins. Now that so many new and excitingaspects of receptor-to-nucleus signaling pathways arebeing studied in the division, we trust that our sciencewill flourish in the coming years.Signal transduction by G protein-coupledreceptorsWH Moolenaar PhDO Kranenburg PhD 1H Lacerda PhD 2FR Postma PhD 4F Van Leeuwen PhD 3BNG Giepmans MSc 4J Mulder MSc 3FPG Van Horck MSc 5GM HengeveldL Ran 6I VerlaanI Van EttenGroup leaderPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianLysophosphatidic acid (LPA) and sphingosine-1-phosphate (S1P) are serum-borne lysophospholipids thatact on their cognate G protein-coupled receptors totrigger a host of cellular responses, ranging from rapidcytoskeletal changes and ionic conductance changes tostimulation of cell proliferation and survival. LPA and S1Psignal through the so-called Edg family of receptors,comprising at least seven members (Figure III.1).Edg-2 receptor signalingThe properties of the various Edg receptors are onlyjust beginning to be characterized. We have obtainedcDNAs for three different LPA receptors (Edg-2, Edg-4and Edg-7) and are now exploring their signalingproperties in more detail, using selected cell lines whichFigure III.1The Edg family of G protein-coupled receptors. Edg2, Edg4 andEdg7 are specific LPA receptors, whereas Edg1, Edg3, Edg5and Edg6 are receptors for S1P.are devoid of endogenous LPA receptors. Reorganizationof the actin cytoskeleton is one of the earliest responsesto Edg receptor activation and underlies changes in cellshape, adhesion and motility. LPA/S1P-induced cytoskeletalremodeling is mediated by the small GTPase RhoA. Inneuronal cells, LPA induces RhoA-mediated cell roundingand neurite retraction. We have found that, in addition toRhoA, both the small GTPase Rac and calcium entry mayplay an important role in LPA-induced cytoskeletalremodeling. Ectopic expression of the Edg-2 receptor inB103 neuroblastoma cells restores calcium signaling andMAP kinase activation in response to LPA. LPA stimulationleads to prominent activation of Rac and subsequent cellspreading and increased motility. These effects appear tobe G i/o-mediated. We conclude that LPA stimulation caneither induce Rho-dependent cell rounding or Racmediatedcell spreading, and that these differences reflectactivation of different Edg family members.Rho signalingIn neuronal cells, LPA and S1P induce rapid withdrawalof developing neurites and rounding of the cellbody. In other cell types, LPA induces the formation ofactin stress fibers. These effects are mediated by theRhoA GTPase which stimulates the so-called ROCK/ROKfamily kinases. These cause enhanced phosphorylation ofthe myosin light chain leading to contraction of thecortical actin cytoskeleton. Using transfection studies inboth COS and neuroblastoma cells, we found that LPAsignals RhoA activation and cytoskeletal contraction viathe G 12/13 subfamily of heterotrimeric G proteins. RhoA,like other Ras-related small GTPases, is activated byguanine nucleotide exchange factors (GEF’s) thatstimulate the exchange of GDP for GTP. We haveisolated a Rho-specific GEF (p190RhoGEF) that binds toand activates RhoA but not the related Rac or Cdc42GTPases. In contrast to the isolated catalytic DH/PHdomain, full length RhoGEF is inactive when tested invitro. By deletion mutant analysis we are currently testingthe nature of this intrinsic inhibitory activity.Interestingly, we observed that activated Gα q, but notGα 12 or Gα 13, binds to the catalytic DH/PH domain ofRhoGEF. We are currently testing the effect of thisbinding on RhoGEF activity (collaboration with MRAhmadian, Dortmund). Activated Gα q does not promoteRho-like cytoskeletal rearrangements but, instead, exertsa destabilizing effect on actin stress fibers and promotesthe neurite outgrowth. This raises the possibility that Gα qbinding may serve to inhibit rather than stimulateRhoGEF activity. In neuronal cells RhoGEF localized tothe cytoplasm, but also to discrete regions underneaththe plasma membrane. In addition, we find a fraction ofRhoGEF localized to microtubules. Of note, Rho activityis regulated by microtubule (de)polymerization. Thus,p190RhoGEF activity may be regulated by the polymerizationstate of microtubules. We will test the possibilitythat p190RhoGEF may serve a role in interconnecting thetubulin- and actin-based cytoskeletons.
Rho-regulated re-arrangement of the actin cytoskeletoninvolves not only the generation of force throughthe activation of myosin, it may also involve alteredfunctioning of actin-binding proteins. We have identified aputative ‘scaffold’ protein, termed p116Rip, that directlyinteracts with both RhoA and actin filaments and, hence,is an attractive candidate to mediate changes in actindynamics. The actin-binding domain of p116Rip issubject to protein kinase C (PKC)-mediated phosphorylationwith no apparent contribution of the ROCK/ROKkinases. PKC-activating phorbol ester has a dramaticeffect on cytoskeletal architecture and receptor-mediatedPKC activation has been implicated in the control of actindynamics. A major goal in these studies is to assess therole of p116Rip in the control of f-actin dynamics. We arecurrently testing the effects of purified full-length p116Ripon microfilament behavior and the consequences ofPKC-mediated phosphorylation of the actin-bindingdomain. Intriguingly, p116Rip is not only localized tof-actin networks, it also resides in the nucleus. We areexploring a possible role for p116Rip in nuclear signaling.Rac signaling: identification of myosin II heavy-chain kinaseMyosin IIA is the major motor protein in non-musclecells and associates with f-actin to regulate cellcontraction. We have recently identified a Myosin II heavychain kinase activity in rat PC12 cells and mouse NIE-115 cells, which is transiently activated by agonists suchas bradykinin and LPA. Activity of this kinase appears tobe regulated by the small GTPase Rac and is dependenton calcium entry. Activation of this kinase correlates withenhanced cell spreading. Although the kinase involvedhas not been identified, current evidence suggests thatMyosin II heavy chain phosphorylation serves to promoteMyosin II filament disassembly and the breakdown ofcortical actin/myosin, which leads to a loss of contractilityand cell spreading. We are in the process of testing thishypothesis, with emphasis on investigating the regulatoryrole of calcium. Moreover, we assembled a partial cDNArepresenting a putative human Myosin II heavy chainkinase. This cDNA clone, which contains the completecatalytic domain of this kinase, was obtained from ahuman ‘expressed sequence tag’ (EST) database. Weare currently trying to acquire a full-length cDNA and toexpress the kinase domain in E. coli. This should allowus to perform in vitro kinase assays using purified orrecombinant Myosin IIA as a substrate.Ras-MAP kinase signaling: a role for dynamin-regulatedendocytosisMitogen-activated protein kinases (MAPKs) are keyregulators of fundamental cellular processes like proliferationand differentiation. Ligands for tyrosine kinasereceptors and G protein-coupled receptors, but alsophorbol ester which bypasses cell-surface receptors, allstimulate MAPK activity. We have found that the signaltransduction cascade from activated LPA receptors toMAPK activation involves the tyrosine phosphorylation ofdynamin, a GTPase that regulates receptor endocytosis.At present it is unclear how tyrosine phosphorylationaffects dynamin function. Yet, it appears that MAPKactivation critically depends on the function of dynamin,as evidenced by the use of a dominant-negativedynamin-mutant (K44A) that interferes with clathrinmediatedendocytosis. We find that dynamin is requiredfor the activation of MAPK, but not for the activation ofupstream elements including Ras, Raf and MEK. Indeed,we find that MEK is activated at the plasma membrane,even though the majority of MEK is cytosolic. It thusappears that internalization of activated MEK is a ratelimitingstep in the MAPK activation cascade. We arecurrently examining the precise intracellular sites ofactivation of MEK and MAPK as well as the traffickingroutes of these activated signaling intermediates.The G13 protein couples LPA and S1P receptors tochloride-mediated membrane depolarizationLPA and S1P induce rapid neurite retraction and cellrounding in neuronal N1E-115 cells through G 12/13-mediated activation of the RhoA GTPase. We havediscovered that LPA- and S1P-induced RhoA activationis accompanied by a prominent, long-lasting membranedepolarization (inward current) due to an increase inchloride conductance. As a result, action potentialgeneration is suppressed for many minutes. The heterologouslyexpressed Edg-2 receptor can mediate the effect ofLPA. Ca 2+ -mobilizing agonists that do not activate RhoA,such as bradykinin and neurotransmitters, fail to activatethe chloride current. Activation of the chloride current canbe dissociated from RhoA activation and changes in cellshape, and requires neither inositol lipid hydrolysis nor Ca 2+mobilization. Microinjected antibody against Gα 13 subunitsprevents activation of the chloride current, whereasantibodies to Gα 12 and Gα i do not. Thus, the G 13 proteincouples LPA and S1P receptors to a bifurcating signalingpathway leading to: 1) RhoA activation; 2) activation ofchloride channels (Ca 2+ - and volume-insensitive) withconsequent membrane depolarization. We propose thatG 13-mediated membrane depolarization may serve tomodulate neuronal activity and stimulate Ca 2+ entry duringRho-regulated neurite remodeling under both physiologicalan pathological conditions.Inhibition of gap junctional communication by LPALPA rapidly disrupts connexin43 (Cx43)-based gapjunctional communication in normal fibroblasts, through apathway that involves the c-Src tyrosine kinase butotherwise is poorly understood. Expression of anactivated mutant of Gα q minics this effect of LPA. Thedownstream effector of Gα q is phospholipase C (PLC),which hydrolyses PtdIns(4,5)P2. We found that the Cx43C-terminus can bind PtdIns(4,5)P2 in vitro. This suggestsa model in which PtdIns(4,5)P2 levels modulate theaccessibility of the Cx43 C-terminus to signalling proteins.Furthermore, we found that Cx43 co-precipitates with thereceptor tyrosine phosphatase RPTPµ. Pervanadate43CELLULAR BIOCHEMISTRY
44CELLULAR BIOCHEMISTRYtreatment results in tyrosine phosphorylation of Cx43 anddecreased cell-cell communication. How RPTPµ may affectconnexin function remains to be elucidated. To search foradditional binding partners of Cx43, cytosolic proteins werepulled down using a GST-fusion protein containing theCx43 C-terminal tail from metabolically labeled cell lysates.A major Cx43-binding protein of around 55 kDa waspurified and, through microsequencing, identified astubulin. How tubulin binding may affect Cx43 function inintact cells is currently under investigation.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-978.2 Funding: EMBO.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1795.4 Funding: Dutch cancer Society, Project <strong>NKI</strong> 95-954.5 Funding: Netherlands Organization for ScientificResearch (NWO/SLW), Project 805-05.103.6 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2042.J Borst PhDA De Melker PhD 4L Smit PhD 4J Hendriks MSc 2AD Tepper MSc 5A Werner MSc 1I Bontjer 1E De VriesG Van der HorstR Kikkert MSc 3Regulation oflymphocyte activationGroup leaderPost-docPost-docGraduate studentGraduate studentGraduate studentTechnicianTechnicianTechnicianGuestPublications: Signal transduction byG protein-coupled receptorsFeiken E, Van Etten I, Gebbink MFBG, Moolenaar WH, ZondagGCM. Intramolecular interactions between the juxtamembranedomain and the phosphatase domains of receptor protein tyrosinephosphatase RPTPµ: regulation of catalytic activity. J BiolChem 1999 (in press).Kranenburg O, Verlaan I, Moolenaar WH. Gi-mediated tyrosinephosphorylation of Grb2-bound protein 2)-bound dynamin-II bylysophosphatidic acid. Biochem J. 1999; 339: 11-4.Kranenburg O, Poland M, Van Horck FPG, Drechsel D, Hall A,Moolenaar WH. Activation of RhoA by lysophosphatidic acid andGα 12/13 subunits in neuronal cells: induction of neurite retraction.Mol Biol Cell 1999; 10: 1851-7.Kranenburg O, Verlaan I, Moolenaar WH. Dynamin is required forthe activation of mitogen-activated protein (MAP) kinase by MAPkinase kinase. J Biol Chem 1999; 274: 35301-4.Moolenaar WH. Bioactive lysophospholipids and their G proteincoupled-receptors.Exp Cell Res 1999; 253: 230-8.Moolenaar WH. Development of our current understanding of lysophospholipids.In: Annals NY Acad Sci, Goetzl EJ, Lynch KR,editors. Lysophospholipids and eicosanoids in cancer and in cardiovascularand neurodegenerative diseases. New York: NY AcadSci 1999 (in press).Postma FR [Dissertation]. Cellular responses to lysophosphatidicacid and sphingosine-1-phosphate. Leiden: Leiden University, 1999.Zondag GCM, Reynolds AB, Moolenaar WH. Receptor tyrosinephosphatase RPTPmu binds to and dephosphorylates the cateninp120 ctn. J Biol Chem (in press).Lymphocyte activation is initiated by triggering of theT- or B- cell antigen receptors, which signal according tothe protein tyrosine kinase (PTK) principle. We haveestablished that the adaptor protein Grb2 links antigenreceptors to the Ras-MAP kinase pathway, but alsointeracts with proteins that perform other functions.Among these, we have focused on c-Cbl and theWiskott-Aldrich syndrome protein (WASP). c-Cbl is amajor target for tyrosine phosphorylation as induced byantigen receptors and receptor PTKs. Cbl associateswith these receptors and negatively regulates theirfunction, in part by promoting receptor ubiquitination.Cbl’s negative regulatory function impinges on an intactRing finger domain; deletion mutations in this region turnc-Cbl oncogenic. We set out to identify proteins interactingwith the Ring finger. Three proteins were found,including an E2-type ubiquitin conjugating enzyme(UbcH7). This is consistent with c-Cbl acting as an E3-type ubiquitin ligase, the component in the ubiquitinationreaction that interacts with the substrate. Using the EGFreceptor as a model, we are now monitoring receptorubiquitination and endocytosis in transfected cells, itspromotion by c-Cbl and mutants, as well as by the newlyidentified Ring finger-interacting proteins.Patients with WASP mutations show defects in plateletand lymphocyte function. WASP regulates the actincytoskeleton, but the receptor-linked pathways thatcontrol WASP function remain ill-defined. We haveestablished that WASP associates with the EGF receptorvia Grb2 in an EGF-dependent manner, and haveidentified a novel WW-domain protein that interacts withWASP. T-cell clones were generated from patients andreconstituted with WASP using retroviral gene transduction.In these clones, we will study the role of WASPand its binding partners in T cell receptor-induced cellpolarization.
Regulation of lymphocyte survivalWhile antigen receptors can prime lymphocytes forproliferation and differentiation, these same receptors canalso induce apoptosis during repertoire selection andafter antigenic challenge. We are examining the interactionbetween antigen receptor signaling and signalsinduced by members of the Tumor Necrosis Factor (TNF)receptor family. We have selected Jurkat cells forresistance to apoptosis induced by CD95, a deathinducingmember of the TNF receptor family. Thesevariant cells overexpress an, as yet, unknown moleculethat inhibits CD95 signaling. By various approaches,including representational difference analysis of cDNA(RDA), we are trying to clone this putative inhibitor. Weare particularly interested in this regulation, since theCD95-resistant Jurkat cells are cross-resistant to DNAdamaging anti-cancer regimens. Using isolatedmitochondria, we have established that signaling to themitochondria is blocked downstream from caspase-8 inthese cells. This defines a novel control point inapoptosis signaling upstream from the mitochondria. Weare in the process of identifying components of the deathreceptor- and DNA damage-induced pathways thatevoke mitochondrial activation.Synthetic ceramide (Cer) can overcome apoptosisresistance in the variant Jurkat cells. Using cells overexpressinginhibitors of death receptor and mitochondrialfunction, we found that the endogenous Cer response,contrary to popular belief, has no causal role in theactivation of inducer caspases or mitochondria but,rather, is a consequence of it. Cer was found to begenerated from plasma membrane sphingomyelin by ana neutral sphingomyelinase. Since sphingomyelin islocalized to the outer leaflet of the plasma membrane,the question arose of how it can serve as a substrate fora cytosolic enzyme. We found that Cer production correlatesperfectly with the alterations in plasma membranelipid distribution that occur in the effector phase ofapoptosis as illustrated by phosphatidylserine exposure.With regards to the relevance of sphingomyelin to Cerconversion, we are examining the possibility thatdepletion of sphingomyelin alters the structural propertiesof the bilayer, which may have consequences for theultimate generation of the apoptotic morphology.CD27 is a member of the TNF receptor family thatlacks a death domain and associates with Traf-2. In vitro,CD27 costimulates TCR-induced responses of naive Tcells. We are interested to define the exact nature of thiscostimulatory effect. In particular, we want to knowwhether CD27 affects cell survival and/or proliferation.We have generated a CD27-deficient mouse strain, inwhich lymphocyte development and thymic T-cellselection appear normal. Challenge of these mice withinfluenza virus has revealed a reduced responsiveness. Invitro, CD27-deficient T cells show decreased TCRinducedproliferative responses. Further analysis of cellcycle progression versus cell survival should reveal whichpathways are regulated by CD27.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1680.2 Funding: Netherlands Organization for ScientificResearch (NWO) program grant.3 Guest, graduate from University of Amsterdam.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1441.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1266.Publications: Regulation of lymphocyteactivationBoesen-de Cock JGR, Tepper AD, De Vries E, Van BlitterswijkWJ, Borst J. Common regulation of apoptosis signaling inducedCD95 and the by DNA damaging regimens etoposide and gammaradiation downstream from caspase-8. J Biol Chem 1999; 274:14255-61.Borst J, Cope A. Turning the immune system on. Immunol Today1999; 20: 156-8.Medema,J-P, Borst J. T cell signaling: a decision of life and death.Human Immunol 1999; 60: 403-11.Tepper AD, De Vries E, Van Blitterswijk WJ, Borst J. Orderingof ceramide formation, caspase activation, and mitochondrialchanges during CD95- and DNA-damage-induced apoptosis.J Clin Invest 1999; 103: 971-8.WJ Van Blitterswijk PhDPCJ Van der Hoeven PhDB Houssa MSc 1GA Ruiter MSc 2AD Tepper MSc 3S Diks 4A Los 4JJM De WidtP RuursSF Zerp 2Lipid metabolism insignal transductionGroup leaderPost-docGraduate studentGraduate studentGraduate studentUndergraduate studentUndergraduate studentTechnicianTechnicianTechnicianFunction of diacylglycerol kinase 1Diacylglycerol kinase (DGK) phosphorylates diacylglycerol(DAG) to yield phosphatidic acid (PA). Since DAGactivates protein kinase C (PKC), DGK may regulate PKCactivity. We have identified the DGKθ isotype which ishighly expressed in brain. In collaboration with WMoolenaar, we found that DGKθ binds specifically to theeffector loop of activated RhoA, in both COS and neuro-45CELLULAR BIOCHEMISTRY
46CELLULAR BIOCHEMISTRYFigure III.2Subcellular localization of DGKθ at different stages of celldivision. A. MelJuso cells were microinjected with DGKθ cDNA.Two microinjected cells show enhanced DGKθ staining innuclear speckels, while surrounding non-injected cells showendogenous DGKθ. B. Cell in metaphase. DGKθ is located atthe spindle pole bodies. Chromosomes at the metaphaseplaque were stained with propidium iodine. C. Cells at latetelophase. DGKθ clusters start to reform in the cytoplasm beforereentering the nuclei of daughter cells. DGKq is also seen at themidbody. DGKθ was stained with a specific polyclonal antobody.blastoma cells. Strikingly, the binding of activated RhoAto DGKθ inhibits DGK catalytic activity. These resultssuggest that that DGKθ is a downstream effector ofRhoA and that its activity is negatively regulated byRhoA. Through accumulation of newly produced DAG,RhoA-mediated inhibition of DGKθ may lead to enhancedPKC activity in response to external stimuli. DGKθ ispresent in the cytosol and the nucleus. Immunofluorescenceanalysis revealed that DGKθ in the nucleusclusters into so-called speckles (Figure III.2) where it colocalizeswith splicing factors, suggesting a possible rolefor DGKθ in mRNA processing. Phosphoinositide kinasesand phospholipase C are also detected in such speckels,suggesting that these structures contain preassembledsignaling complexes of a nuclear phosphoinositide cycle.DGKθ localization alters dramatically during cell division:in prophase and metaphase, DGKθ staining disappearsand concentrates at the spindle pole bodies. At lateanaphase and early telophase, DGKθ clusters reassemblein the cytosol and enter the nuclei of daughtercells. In addition, DGKθ acumulates at the midbody ofcells undergoing cytokinesis, suggesting that DGKθ alsoacts in this process.PKC-ζ signalingIn growth factor-stimulated Rat-1 cells, protein kinaseC-ζ (PKC-ζ) phosphorylates and activates the Raf-1kinase in a signaling complex. Formation of this complexis mediated by the scaffold protein 14-3-3. Complexformation was much stronger with a kinase-inactive PKCζmutant than with the wild-type enzyme, supporting theidea that kinase activation causes complex dissociation.Certain 14-3-3 proteins could serve as substrates forPKC-ζ. Phosphorylation of 14-3-3 by PKC-ζ negativelyregulated their physical association. Our findings suggestthat 14-3-3 facilitates coupling of PKC-ζ to RAF-1 in aternary complex, in an isotype-specific and phosphorylation-dependentmanner. We propose that 14-3-3 is atransient mediator of RAF-1 phosphorylation andactivation by PKC-ζ.PKC-ζ can also associate with protein kinase B (PKBor AKT) in a 14-3-3-mediated and phosphorylationdependentfashion (collaboration with P Van Bergen andHenegouwen, Utrecht University). Growth factor stimulationof COS cells decreased this association. Ourresults suggest that, contrary to its stimulatory activity onRAF-1 signaling, PKC-ζ may act as a negative regulatorof the PKB/AKT survival pathway.Sphingomyelinase-mediated ceramide formation inapoptosis 3(collaboration with J Borst)Apoptosis induction is generally accompanied withceramide (Cer) production but cause-effect relationshipsremain unclear. As mentioned above, Cer formation inJurkat cells by CD95 or DNA-damaging regimensappears to be associated with the effector phase ofapoptosis. CD95-induced Cer production in Jurkat cellswas temporally associated with sphingomyelin (SM)hydrolysis, phosphatidylserine (PS) exposure and thehydrolysis of the exogenously supplied fluorescent SManalog (NBD-SM), which intially inserts into the outerleaflet of the plasma membrane, to NBD-Cer. Bycontrast, NBD-phosphatidylcholine was not metabolized.Raji cells defective in calcium-induced phospholipidscrambling did not show CD95-induced PS externali-
zation nor Cer production, yet underwent apoptosis asassessed by loss of mitochondrial depolarization andnuclear fragmentation. These results support a causal linkbetween two plasma membrane events, i.e. loss ofphospholipid asymmetry and Cer formation. Moreover, itappears that Cer has no role in the induction ofmitochondrial and nuclear changes. Direct induction oflipid scrambling by Ca 2+ ionophore resulted in concomitantPS exposure and NBD-SM hydrolysis in Jurkatcells but not in Raji cells, indicating that loss of phospholipidasymmetry is necessary and sufficient togenerate a Cer response. We propose a novelmechanism of Cer formation, in which SM in the outerleaflet of the plasma membrane flips to the inner leaflet,where it becomes accessible to cytosolic neutral sphingomyelinase.SM has a high affinity for cholesterol, which isimportant for stability of the plasma membrane and thesignaling function of specialized domains (rafts/caveolae)therein. Using methyl-cyclodextrin as a strong cholesterol-bindingagent, we observed an enhanced cholesterolefflux from the plasma membrane upon exposure ofJurkat cells to bacterial sphingomyelinase, anti-CD95mAb or ionomycin. We postulate that lipid scramblingresults in SM hydrolysis, loss of SM/cholesterol interactionand altered bilayer properties, which may facilitatemembrane blebbing, vesicle shedding and apoptoticbody formation. Accordingly, Raji cells defective in lipidscrambling did not show membrane blebbing, whereasexogenous NBD-SM prevented blebbing in CD95-stimulatedJurkat cells. This suggests that the breakdown ofSM, rather than the production of Cer, is the determiningfactor for these morphological changes in apoptotic cells.Publications: Lipid metabolism in signaltransductionBoesen-de Cock JGR, Tepper AD, De Vries E, Van BlitterswijkWJ, Borst J. Common regulation of apoptosis signaling inducedby CD95 and the DNA-damaging stimuli etoposide and γ-radiationdownstream from caspase-8 activation. J Biol Chem 1999;274: 14255-61.Doornbos RP, Theelen M, Van der Hoeven PCJ, Van BlitterswijkWJ, Verkleij AJ, Van Bergen en Henegouwen PMP. Protein kinaseC-ζ is a negative regulator of protein kinase B activity. J Biol Chem1999; 174: 8589-96.Houssa B, De Widt J, Kranenburg O, Moolenaar WH, VanBlitterswijk WJ. Diacylglycerol kinase θ binds to and is negativelyregulated by active RhoA. J Biol Chem 1999; 274: 6820-2.Ruiter GA, Zerp SF, Bartelink H, Van Blitterswijk WJ, Verheij M.Alkyl-lysophospholipids activate the SAPK/JNK pathway andenhance radiation-induced apoptosis. Cancer Res 1999; 59:2457-63.Tepper AD, De Vries E, Van Blitterswijk WJ, Borst J. Orderingof ceramide formation, caspase activation, and mitochondrialchanges during CD95- and DNA damage-induced apoptosis.J Clin Invest 1999; 103: 971-8.Tepper AD, Van Blitterswijk WJ. Ceramide mass analysis by normalphase HPLC. Methods Enzymol 1999 (in press).Van Blitterswijk WJ, Houssa B. Diacylglycerol kinases in signaltransduction. Chem Phys Lipids 1999; 98: 95-108.47CELLULAR BIOCHEMISTRYApoptosis induced by alkyl-lysophospholipids (ALPs) 2(collaboration with M Verheij, Division IX)Synthetic alkyl-lysophospholipids (ALPs) such as 1-Ooctadecyl-2-O-methylglycero-3-phosphocholine(ET-18-OCH 3) readily incorporate into the plasma membrane andinduce apoptosis in various tumor cells by an unknownmechanism. ALPs act synergistically with ionizingradiation in inducing apoptosis in leukemic cells. ALPsrapidly activate the stress-activated protein kinase(SAPK/JNK) signaling pathway and inhibit two antiapoptoticpathways, i.e. the MAP kinase pathway andthe PKB/AKT survival pathway. ALPs prevent ERKsignaling in a RAS-independent manner, by interferingwith phospholipase C and PKB signaling. Thus, ALPsmay act by interfering with inositol lipid metabolism at theplasma membrane and possibly in intracellular organelles.Notes1 Funding: Netherlands Organization for ScientificResearch (NWO/SON 330-210).2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1435.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1266.4 University of Utrecht.Van der Hoeven PCJ, Van der Wal J, Ruurs P, Van Dijk MCM, VanBlitterswijk WJ. 14-3-3 isotypes facilitate coupling of protein kinaseC-ζ to Raf-1; negative regulation by 14-3-3 phosphorylation.Biochem J 1999; 345: 297-306.N Divecha PhDJ Clarke PhDC D’Santos PhD 1J Halstead PhD 2M RoefsSignaling throughinositol phospholipidsGroup leaderPost-docPost-docPost-docTechnicianThe inositol phospholipid pathway is an intracellularsignaling cascade which, in response to growth factorsand other stimuli, can generate a number of second
48CELLULAR BIOCHEMISTRYmessengers. Our research is focused on the regulation ofthe synthesis and cellular functions of phosphatidylinositol-4,5-bisphosphate(PtdIns(4,5)P2) and, in particular,the role of phosphatidyl-inositol-phosphate kinases(PIPkins) therein. Cloning has revealed that there arethree sub-families of PIPkins able to phosphorylatedifferent phosphatidylinositol phosphates at variouspositions. The type I PIPkin will phosphorylate PtdIns(4)Pon the 5 position of the inositol ring, while the type IIenzymes (or PIPkin C) have a specificity for PtdIns(5)Pwhich they phosphorylate on the 4 position. These datademonstrate that eukaryotic cells have developed at leasttwo distinct pathways for regulating the synthesis ofPtdIns(4,5)P2. This highly regulated process probablyreflects the cellular requirements for PtdIns(4,5)P2 in anumber of diverse functions in discrete subcellularcompartments. For example, it is the substrate forreceptor-mediated generation of inositol(1,4,5)trisphosphate,which regulates cellular calcium, and diacylglycerol(DAG) which regulates the activity of proteinkinase C. Genetic evidence suggests that PtdIns(4,5)P2is important in membrane trafficking through therecruitment of coat proteins required for vesicleformation. PtdIns(4,5)P2 is also the substrate for agrowth factor-stimulated PtdIns-3-kinase which leadsto the formation of PtdIns(3,4,5)P3. AlthoughPtdIns(3,4,5)P3 has pleiotropic effects, the demonstrationthat an enzyme (PTEN), which dephosphorylates this lipidis a tumour suppressor and is mutated in a number oftumors, suggests it is physiologically important in cellgrowth and survival. Finally, the phosphoinositidepathway is also present within the nucleus where thefunctions of PtdIns(4,5)P2 appear to be involved in theproduction of second messengers as outlined above, butalso has a potential role in the regulation of other nuclearfunctions such as chromatin structure and nucleartransport. To better understand the regulation of thesepools of PtdIns(4,5)P2 we are currently analyzing thesubcellular localization and mode of activation of PIPkinsas well as the regulation of the intranuclear pool ofPtdIns(4,5)P2.Type I PIPkinThere are three family members of the type I PIPkinsidentified to date and we have concentrated on theregulation of the type Iα. Our data suggest that it isregulated by interaction with at least two differentproteins leading to its involvement in two importantsignaling pathways. The Rac GTPase regulates diversecellular processes such as cytoskeletal and endocyticdynamics. We have demonstrated that RAC interactswith type I PIPkin. This interaction not only leads to theenhanced synthesis of PtdIns(4,5)P2, but also to anincrease in the cellular PtdIns(3,4,5)P3 pool. Previousdata have demonstrated that PtdIns(3,4,5)P3 is importantin the regulation of protein kinase B (PKB), a cell survivalfactor. However, our data demonstrate thatPtdIns(3,4,5)P3, derived from the interaction of RAC andFigure III.3Porcine endothelial cells were microinjected with the type IαPIPkin together with GFP-labeled PLD2. Three hours later, thecells were fixed and the type Iα was visualized after staining witha specific antibody. The figure shows the same cells viewed byconfocal microscopy.the type Iα. PIPkin, is unable to activate PKB. This mayreflect the intracellular location of this PtdIns(3,4,5)P3,which we are currently investigating in collaboration withK Jalink (Division I) using new fluorescent probes specificfor this lipid.Phospholipase D (PLD) is important in the regulation ofsecretion and membrane trafficking. This enzyme haspreviously been shown to have an absolute requirementfor PtdIns(4,5)P2. Using cloned PLDs (obtained in a collaborationwith M Wakelam, Birmingham, UK), we haveshown that the type Iα PIPkin interacts with, activatesand co-localizes with PLD2. Interestingly, the coexpressionof PLD2 appears to recruit the type Iα. PIPkinto vesicles (Figure III.3). The role of this interaction interms of the regulation of membrane flow is currentlyunder investigation (collaboration with J Neefjes, DivisionIV).Type II PIPkinIn collaboration with R Irvine (University of Cambridge,UK) we have investigated the potential regulation of thetype II PIPkins. This family is composed of at least threemembers. We have demonstrated that the α isoform isregulated by phosphorylation, by casein kinase 2, whichleads to the translocation of the normally cytosolic proteinto the plasma membrane. Whether this opens a crypticFigure III.4Hela cells were transfected with cDNA encoding either GFP-typeIIα or β. After 12 hours the cells were fixed and viewed byconfocal microscopy.
membrane binding site or a protein interaction site iscurrently under investigation.We have previously demonstrated that a type II PIPkinis also present in the nucleus. Using GFP-taggedproteins we have shown that the β isoform is nuclearwhile the a isoform is cytosolic (Figure III.4). Chimerasbetween these proteins has allowed us to identify thatthe α helix-7 domain of the type IIβ. is important in thislocalization. This domain may be involved in the processof nuclear translocation or in binding to specific nuclearsites.The nuclear inositide pathwayWe have previously shown that the inositol phospholipidpathway also operates in the nucleus and thatnuclear inositol lipids and the enzymes required tosynthesize and metabolize them are regulated distinctlyfrom those found at the plasma membrane. DAG is a keysecond messenger within the nucleus and its removal byoverexpression of a DAG kinase leads to cell cycle arrest.By exploiting the differences in the fatty acid compositionof PtdIns and PtdCho lipids, we have demonstrated thatthere exists within MEL (murine erythroleukemia) cellnuclei two discrete pools of DAG derived from theendogenous pools of PtdIns and phosphatidylcholine,respectively. By the use of specific inhibitors, we haveshown that these pools are differentially regulated withrespect to either cell differentiation or proliferation. Wehave shown changes in the levels of nuclear PtdInsP,PtdInsP 2 and phosphatidic acid which are consistent withthese nuclear lipids having a function as cells move intothe replicative phase of the cell cyle. To visualize this inreal time, we have constructed cell lines which overexpressa fluorescent probe which is targeted to thenucleus and binds specifically to nuclear PtdIns(4,5)P2.Interestingly, we demonstrate that the mass levels of thislipid increases specifically at this time point and that thepresence of the probe, which specifically binds toPtdIns(4,5)P2, appears to lead to a cell cycle arrestwhich does not occur if the probe is targeted toPtdIns(4,5)P2 present at the plasma membrane. Thesedata suggest a important physiological function fornuclear PtdIns(4,5)P2 as cells progress through the cellcycle.We have characterized a pathway of nuclearPtdIns(4,5)P2 synthesis and now are able to pharmacologicallyinhibit this pathway resulting in a specificdecrease in the nuclear PtdIns(4,5)P2 levels. This shouldshed light on the physiological functions of this pathway.Notes1 Funding: EEC.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2055.Publications: Signaling through inositolphospholipidsDivecha N, Clarke JH, Roefs M, Halstead JR, D’Santos C.Nuclear inositides; inconsistent consistencies. Cell Mol Life Sci1999 (in press).D’Santos CS, Clarke JH, Irvine RF, Divecha N. Nuclei contain twodifferentially regulated pools of diacylglycerol. Curr Biol 1999; 9:437-40.Fernandez-Borja M, Wubbolts R, Calafat J, Janssen H, DivechaN, Dusseljee S, Neefjes J Multivesicular body morphogenesisrequires phosphatidyl-inositol 3-kinase activity. Curr Biol 1999; 9:55-8.Hinchliffe KA, Ciruela A, Letcher AJ, Divecha N, Irvine RF.Regulation of type IIalpha phosphatidylinositol phosphate kinaselocalization by the protein kinase CK2. Curr Biol 1999; 9: 983-6.Smith GC, Divecha N, Lakin ND, Jackson SP. DNA-dependentprotein kinase and related proteins. Biochem Soc Symp 1999; 64:91-104.P Ten Dijke PhDM-J Goumans PhDS Itoh PhDF Itoh MScG Valdimarsdottir MSc 1M ThorikayTGF-β/Smad signaltransductionGroup leaderPost-docPost-docGraduate studentGraduate studentTechnicianTransforming growth factor-β (TGF-β) is the prototypeof a large family of multifunctional cytokines, whichinclude TGF-βs, activins and bone morphogeneticproteins. Many of them have important functions duringembryonic development and in adults they are involved inmaintaining tissue homeostasis. Our research 2 is aimedat elucidating the signaling mechanisms by which TGF-βfamily members elicit their wide range of biological effectson many different cell types, including modulation of cellproliferation, differentiation, apoptosis and migration. Anincreased understanding in TGF-β signaling processesand in vivo function of the signaling components isessential for the treatment of various clinical disorders,including cancer, fibrosis, vascular and auto-immunediseases, that are caused by deregulated TGF-β activity.Our work focuses on the activation and regulation ofthe TGF-β serine/threonine kinase receptors and their49CELLULAR BIOCHEMISTRY
50CELLULAR BIOCHEMISTRYintracellular effectors, termed Smad proteins. Uponbinding to their specific receptors, each TGF-β familymember activates a particular subset of Smad proteins,which form heteromeric complexes that translocate tothe nucleus where they regulate gene transcription. Wewill study the role of Smads as transcriptional regulatorsof various TGF-β-induced responses by identifying transcriptionfactors, co-activators and co-repressors withwhich Smads make functional interactions and identifyand characterize Smad target genes. To elucidate howsubversion of TGF-β signaling contributes to cancer, wewill search for molecules that, when misexpressed or (inactivated)perturb TGF-β-induced growth arrest. To investigatethe patho-physiological role of TGF-β in vasculogenesis,we will use mice lacking TGF-β receptors inendothelial cells and cells from patients with TGF-βreceptor-associated vascular diseases, i.e. hereditaryhemorrhagic telangiectasia 1 .Notes1 Funding: Netherlands Heart Foundation, Project99.046.2 Supported in part by EEC TMR grant(ERBFMRXCT980216) and Netherlands Organizationfor Scientific Research, Project ALW 809.67.024.Publications: TGFβ/Smad signaltransductionHeldin C-H, Ten Dijke P. SMAD destruction turns off signaling.Nature Cell Biol 1999; 1: E195-7.Ten Dijke P, Miyazono K, Heldin C-H. Signaling inputs convergeon nuclear effectors in TGF-β signaling. Trends Biochem 1999 (inpress).Secretary Cellular BiochemistryJM OverwaterResearch staff positions (full time equivalents)Scientific permanent: 5.0Scientific project: 18.5Technical permanent: 8.2Technical project: 4.6
IV Division of Immunology51Division head Ada KruisbeekIntroductionThis division spans a broad range of topics related toT-cell-mediated immune responses and T-celldevelopment. Not all the research lines can behighlighted in this short introduction, but a few of thecommon interests should be mentioned. Since the groupof T Schumacher introduced the technology for use ofsoluble tetrameric peptide-MHC complexes, essentially allprojects related to tumor immunity and auto-immunityapply this technology to follow the fate of T cells in vivoand in vitro. As soluble tetrameric complexes bind to thevariable portion of the antigen receptors on T cells, theycan be applied to study the anatomy of the tumorspecificT-cell response, to study how T cells withreceptors specific for self-proteins behave in vivo, and tostudy how variations in antigenic epitopes may affectescape from T-cell immunity. This year, T Schumacherand his co-workers discovered that the immune responseto naturally arising variants of a dominant T-cell epitope ininfluenza A virus consists mainly of rare cross-reactivekiller T cells, originating in the T-cell memory population.Another technology that is applied in virtually allprojects in the division is retrovirus-mediated genetransfer, introduced here by the laboratory of H Spitssome years ago. Lymphocytes are notoriously difficult totransfect through means that work well with most othercell types and, as lymphocytes are the mainstay of thedivision, it used to be difficult to perform signaling studiesand gene complementation experiments ex vivo. Now,however, most of the T-cell development studies of boththe Kruisbeek and the Spits laboratory rely heavily onectopic expression of signaling molecules or transcriptionfactors and their mutants for identification of crucial stepsin the developmental pathway of T cells. H Spits reportson some exciting insights about the survival and proliferationversus differentiation signals in early T cells. Inanother recent discovery, the life span of human killer Tcells could be extended tremendously through ectopicexpression of the catalytically active component oftelomerase.Ever since the finding that a self-antigen on humanmelanomas, tyrosinase, represents a tumor rejectionantigen recognized by killer T cells, the ground rules oftumor immunology have changed. Rather than focusingon tumor-specific antigens, many laboratories nowexplore tissue-specific self-antigens as promising targetsfor T-cell mediated anti-tumor therapy. This has fosteredan interest in defining conditions that can overcome the(naturally occurring) tolerance to self-antigens.Fortunately, tolerance is inherently imperfect, and apopulation of low avidity self-antigen specific T cellscould easily be detected in the normal T-cell repertoire(Kruisbeek laboratory). The challenge for the future will beto define how we can make such cells work for us: it isclear that they have severe defects in their ability toproduce IL-2 and proliferate in response to an antigenicchallenge, and we are now in a good position to dissectthe basis for these defects. Being able to correct them,however, may be another matter. In preparation of analternative approach, the Schumacher laboratory hasdeveloped a very promising strategy for retroviral TCRdisplay that allows selection of high affinity TCRs with adesirable fine-specificity. Application of this strategy mayprovide a way to circumvent the limitations of the lowavidity self-specific T-cell repertoire.Tuning TCR signaling in T-celldevelopment and tumor immunityAM Kruisbeek, PhDF Bischof MD 1M Haks PhD 2W Marissen PhD 3E Pépin PhD 4Q Valent PhD 5Y Zevering PhD 6T Cordaro MScK De Visser MSc 7I Klitsie 5F Tirion 7J Van den BrakelP WederE Wijnands 5A BinsS SmeeleGroup leaderPost-docPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentThis laboratory studies how T-cell receptor (TCR)signaling determines T-cell fate, both early indevelopment, and in the mature T-cell pool. Our work
52IMMUNOLOGYcenters around 2 major lines of investigation: 1) the roleof the TCR and the pre-TCR in the development of Tcells; and 2) the regulation of mature T-cell responsivenessin the context of tumorimmunity and autoimmunity.Recent results in these areas include thediscovery that receptor triggering of CD8 T cells with lowavidity TCRs results in an aborted immune response. Wealso found that pre-T cells with a dysfunctional pre-TCRfail to complete their differentiation program, even whentheir survival defect is restored.Pre-TCR and TCR controlled checkpoints of T-celldevelopmentProgression of T-cell development is monitored byantigen receptors at two checkpoints. The first is at thetransition from the double negative (DN) to the doublepositive (DP) stage; this process is termed TCRβselection and is regulated by the pre-TCR. The secondcheckpoint is at the DP to the SP stage and is driven bythe mature TCR complex.Regulation of early T-cell development by the pre-TCRis one of the topics of our research, with specialemphasis on the identification of molecular eventsmodulated by signals from the pre-TCR. Our studieswere the first to establish genetic evidence for the crucialrole of the CD3γ chain in the pre-TCR (Haks et al. EMBOJ 1998; 17: 1871-82). These findings were surprising, asthey suggest that CD3γ is not functionally redundant inthe pre-TCR complex. We also demonstrated a role forthe p53 protein at the TCRβ selection checkpoint: introductionof p53 deficiency into CD3γ-deficient micecompletely reverses the survival defect in the DNcompartment and the DP compartment eventuallyreaches its normal size. Nevertheless, such rescuedCD3γ-deficient thymocytes are unable to undergo certainsubsequent developmental steps in αβ T-celldevelopment. Proliferative and survival signals can thusbe separated from the pre-TCR driven signaling eventsthat regulate further differentiation at this stage ofdevelopment.Given the previously established roles for theCD3δ and CD3ζ chains in the TCR complex at thepositive selection checkpoint, our subsequent findingswere even more surprising. When CD3γ-deficient miceare crossed to mice expressing a transgenic TCR, thethymus increases in size and forms a large DPcompartment, but positive selection does not occur.Although DP cells lacking CD3γ do have the ability toinitiate the first steps in positive selection, they are unableto progress through the entire differentiation program.The data further suggest that CD3γ-deficient TCRs areunable to deliver the prerequisite signals that DP thymocytesneed to be rescued from programmed cell death.These findings underscore the complex relationshipbetween TCR signaling and positive selection.Identification of crucial signaling events downstream ofthe TCR will be required to further dissect the multi-stepprogram of positive selection.T-cell tolerance and antitumor immunityQuestions such as how self-reactive T cells cansurvive, expand and differentiate into effector andmemory populations are central to our understanding ofboth autoimmunity and antitumor immunity. Self-reactiveT cells can cause both undesirable autoimmunepathology and desirable tumor rejection. We are thereforestudying how such cells are generated and which conditionsdetermine their in vivo response.In collaboration with the group of T Schumacher, weemploy tetramer technology to determine the phenotypicaland functional characteristics and in vivo fate of aself-reactive CD8 T-cell population specific for an ubiquitouslyexpressed T-cell epitope. Contrary to expectationsbased on TCR transgenic studies, we find that a sizablepopulation of self-reactive CD8 + T cells can be triggeredto expand and differentiate into effector cells. These cellsare not deleted, do not downregulate their antigen or CD8receptors, are not inactivated, and can differentiate intomemory cells. The main hallmark of the self-reactive CD8 +T-cell population that can be elicited from the polyclonalrepertoire is its diminished avidity for the pertinent tetramericMHC/peptide complex. The ability to identify andisolate these cells is then applied to compare theactivation, survival, expansion and differentiation requirementsof low versus high avidity CD8 + T cells. The resultsobtained so far show that, although low avidity T cellscan be triggered to differentiate into effector CTL andIFNγ secreting cells, they differ from high affinity CD8 +cells in a number of ways. Low avidity cells display adramatically reduced susceptibility to antigenic peptide,and cannot produce IL-2, regardless of the antigen doseused. In addition, their ability to be expanded after stimulationin exogenous IL-2 is severely limited. These studiesillustrate that responsiveness is not dictated by signalstrength alone. Future studies will be directed at acquiringa better molecular understanding of how binding characteristicsof the TCR translate into different responses.Connected to this line of research are efforts to dissecthow the CTLA-4 receptor regulates T-cell responsiveness,and how antigen processing pathways affect T-celltolerance. It is clear that engagement of the CTLA-4receptor on T cells is critically involved in terminatingclonal expansion, but little is known about the underlyingmechanisms. We have used biotinylated peptides of theinactive and active (i.e., phosphorylated) CTLA-4cytoplasmic tail, in combination with chemical crosslinkingreagents to search for CTLA-4 interacting proteinsin T-cell lysates. This approach enabled us to confirm thedocumented CTLA-4 LCK interaction and to pick up twoyet to be identified CTLA-4 interacting proteins. Apartfrom ongoing work on the identification of these proteins,a second major focus of this project is on the consequencesof CTLA-4 engagement for TCR, CD28 andcytokine receptor signaling.In addition, we continue to study how self-antigenexpression in different cellular and intracellular compartmentsaffects T-cell repertoire development. In very
exciting recent experiments, we established that transgenicexpression of a given (model) self-protein in the B-cell compartment, through use of an Ig-promotor, dramaticallyskews the repertoire towards generation ofTh1-only responses. We shall investigate the molecularbasis for this observation, plus its consequences for thesusceptibility to the autoimmune pathology normallyassociated with responses to this protein.Notes1 Funding: German Research Association, Germany.2 Funding: Human Frontier Science ProgramOrganization, Project RG0335/1998-M.3 Funding: NWO (Netherlands Organization for ScientificResearch), Program grant 901-07-096.4 Funding: Association pour la Recherche sur le Cancer,France.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1796.6 Funding: American Multiple Sclerosis Society, ProjectRG 2940-A-1.7 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1276.Publications: TCR signalingAmsen D, Kruisbeek AM. Thymocyte selection: not by TCR alone.Immunol Rev 1999; 165: 209-29.Amsen D, Osborne B, Kruisbeek AM. Costimulatory signals arerequired for induction of Nur77 during negative selection ofCD4 + CD8 + thymocytes. Proc Natl Acad Sci USA 1998; 96: 622-7.Haanen JBAG, Toebes M, Cordaro TA, Wolkers MC, KruisbeekAM, Schumacher TNM. Systemic T-cell expansion during localizedviral infection. Eur J Immunol 1999; 29: 1168-74.Haanen JBAG, Wolkers MC, Kruisbeek AM, Schumacher TNM.Selective expansion of cross-reactive CD8 + memory T cells byviral variants. J Exp Med 1999; 190: 1319-28.Haks MC, Oosterwegel MA, Blom B, Spits H, Kruisbeek AM. Cellfatedecisions in early T-cell development: regulation by cytokinereceptors and the pre-TCR. Semin Immunol 1999; 11: 23-37.Haks MC, Krimpenfort P, Van Den Brakel JHN, Kruisbeek AM.Pre-TCR signaling and inactivation of p53 induces crucial cell survivalpathways in pre-T cells. Immunity 1999; 11: 91-101.Jacobs H, Krimpenfort P, Haks MC, Blom B, DÈmolliËre C,Kruisbeek AM, Spits H, Berns AM. PIM1 reconstitutes thymuscellularity in interleukin-7- and common γ chain-mutant mice andpermits thymocyte maturation in Rag- but not in CD3γ-deficientmice. J Exp Med 1999; 190: 1059-68.ThesisHaks MC. Regulation of T-cell development by cytokine and antigenreceptors. Amsterdam: Free University, 1999.H Spits PhDK Weijer DVM PhDD Clark PhD 1E Hooijberg PhD 2M Naspetti PhD 3Y Yasuda PhD 4W Wiegant MSc 5AQ BakkerF Couwenberg 6E Kueter 7J Ruizendaal 2A VoordouwB VisserD OverdijkLymphoid cell development in humansDevelopment andfunction of humanT cellsGroup leaderAcademic staffPost-docPost-docPost-docPost-docGraduate studentTechnicianTechnicianTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentThis research program focuses on two topics: 1) therole of cytokines, in particular of IL-7, in T-celldevelopment; 2) investigation of the transcriptional controlof human lymphoid development mediated by basic helixloop helix proteins.The role of the IL-7Rα chain in T-cell developmentThe interleukin (IL)-7 receptor plays an essential role inT-cell development and IL-7 binding to the IL-7Ractivates PKB and STAT5 in precursor T cells. We introducedchimeric receptors into such precursors with acytoplasmic domain of the IL-7R that is no longer able toactivate PI-3K/PKB and STAT5 and tested the transducedcells in a fetal thymic organ culture. We alsoexamined the T-cell precursor activity of progenitorsexpressing dominant negative forms of PI-3K (DNp85) orSTAT5B. Ectopic expression of DNp85 in T-cellprecursors strongly blocked proliferation and survival ofthese cells but did not affect their differentiation, as thefew surviving DNp85 expressing cells developed normallyinto both TCRαβ and TCRγδ cells in fetal thymic organcultures. These experiments revealed that PI-3K/PKBactivation is essential for the survival and proliferation ofT-cell precursors and suggest that STAT5 activated by IL-7 mediates T-cell differentiation.Analysis of T-cell development in a normal thymicenvironmentWe have optimized methods to study the role oftranscription factors and signaling molecules ondevelopment of human T cells in the natural thymicenvironment. Progenitors are transduced with dominant53IMMUNOLOGY
54IMMUNOLOGYnegative mutants of transcription factors or signalingcomponents tagged with GFP and with a control taggedwith a truncated form of the nerve growth factor receptor(DNGFR). These transduced cells are then mixed andinjected into an established thymus graft in mice deficientfor RAG1 and the common IL-2/IL7γ chain. By takingbiopsies of the injected thymus and analyzing the NGFRand GFP expression, we can follow the kinetics of T-celldevelopment. We applied this method to analyze theeffect of dominant negative STAT5B on thymic T-celldevelopment. This experiment revealed that DNSTAT5Bstrongly delayed T-cell development. In addition, in collaborationwith N Taylor and N Noraz (University ofMontpellier, France), we analyzed the effect of adominant negative mutant of ZAP-70 and found that thismutant inhibits positive selection as assessed by evaluatingexpression of certain hallmarks of positive selectionon TCR expressing thymocytes.A lymphoid origin of precursors of dendritic cell 2 (pDC2)/natural interferon producing cells (NIPC)We have characterized (in collaboration with F Vyth-Dreese from the Immunotherapy group, and C Uittenbogaart,UCLA, USA) a DC precursor in the thymus whichexpresses CD4, CD45RA and high levels of IL-3Rα(CD123). The phenotype of this rare cell type is identicalto the recently described pDC2 and NIPC, and is thereforereferred to as pDC2/NIPC. Importantly, these cells lack thesurface markers characteristic for the myeloid lineage ofDC, but express a number of markers typical for thelymphoid lineage. Strikingly, these cells also express highlevels of pre T-cell receptor alpha (pTα) transcripts,suggesting a close relationship between these cells andcells of the T-cell lineage. A novel assay was developed inwhich we can determine the pDC2/NIPC precursor activityof CD34 + populations. Using this assay we found thatthymic precursors which mostly lack myeloid developingpotential, have the ability to develop onto pDC2. Thesedata indicate a lymphoid origin of pDC2/NIPC.Control of human lymphoid cell development by bHLHtranscription factorsBasic helix loop helix (bHLH) transcription factorscontrol cell fate decisions in a wide range of organisms,ranging from yeast to mammals. They act in concert withinhibitors of DNA binding (Id) proteins. These proteinspossess the HLH motif and can form dimers with bHLHfactors but, because they lack a basic DNA-bindingdomain, complexes with Id and bHLH proteins are transcriptionallyinactive. We previously reported that ectopicexpression of Id3 in hematopoietic progenitor cellsinhibits the development of these cells into T and B cellsat a very early stage. In contrast, development into NKcells was not affected. We now analyzed the effect of ID3expression on development of hemopoietic progenitorsinto pDC2/NIPC, and observed that development ofthese cells from both uncommitted stem cells and fromearly thymic precursors was completely inhibited by ID3.Ectopic expression of ID3 in progenitor cells thus inhibitsnot only development of T and B cells, but also of thelymphoid dendritic lineage. These data are consistentwith a model in which Id proteins consolidate NK-celldevelopment by limiting the developmental options oflymphoid precursors.Tumor immunologyIsolation of antigen-specific T-cell clones from antigenactivatedT-cell blasts infected with a self inactivating viruscontaining GFP under control of multiple NFAT binding sitesRecent work in our tumor immunology group includesthe development of a novel method for detection andisolation of antigen specific human T cells from aheterogeneous pool of T cells. We engineered into a selfinactivating retroviral (SIN) vector DNA constructs carryingmultiple NFAT binding sites, followed by the minimal IL-2promoter and the reporter gene GFP. Jurkat cells, T-cellblasts and T-cell clones could be transduced with highefficiency with this vector (20-40%). Activation of transducedT-cell blasts with the superantigen SEB or oftransduced antigen specific T-cell clones with cognateantigen, induced GFP expression which could beblocked by Cyclosporin-A and FK506. Following stimulationof a heterogeneous T-cell bulk culture with an HLAmismatched stimulator cell (JY), the GFP expressing cellswere cloned. As expected, the cloning frequency of theantigen-specific GFP + cells was considerably higher thanthat of the total T-cell population. Most of the T-cellclones were either cytolytic, or proliferative towards JYstimulator cells. Interestingly, we also isolated T-cellclones which were non-cytolytic and non-proliferativetowards JY cells, but specifically upregulated GFP afteran overnight stimulation with JY. In future experiments,we will apply this technology towards the isolation andenrichment of tumor-specific T cells.Immortalization of antigen-specific T-cell clonesReplicative senescence of T cells is correlated witherosion of telomere ends. As telomerase plays a key rolein maintaining telomere length, it is thought thattelomerase regulates the life span of T cells. To test thishypothesis we have (in collaboration with the group of JWalboomers, Free University, Amsterdam) ectopicallyexpressed the catalytically active component oftelomerase, telomerase end reverse transcriptase (TERT)tagged with GFP, into a Mart-1/HLA-A2 specific T-cellclone obtained from a melanoma patient. The transductionefficiency was low (5%), but the proportion ofGFP-TERT + cells increased strongly upon furtherexpansion of the cells by weekly stimulations in thepresence of IL-2. After 5 weeks >95% of the cells wereTERT + , indicating a strong growth advantage of thetransduced cells. The telomere lengths of the TERT-transducedcells were longer than those of the untransducedcells, confirming the biological activity of the introducedTERT. In contrast to untransduced T cells, the TERT +
cells could be subcloned at least two times. After morethan 120 population doublings, the subclones have so farmaintained GFP expression, and they are still growingwell, indicating the stability of the introduced gene. Thephenotype of the TERT-transduced cells was virtuallyindistinguishable from that of the untransduced cells and,importantly, the specificity and the cytotoxic activity of thecells (determined by MART1/HLA-A2 tetramer stainingand cytotoxicity assays) were not altered by introductionof TERT. In addition, the cells remained dependent onantigen-stimulation and cytokines for their expansion andsurvival, indicating that the cells retained their normalphysiology and were not transformed. These observationsprove that TERT directly regulates the replicative lifespan of human CD8+ T cells.Heemskerk MHM, Hooijberg E, Ruizendaal JJ, Van Der WeideMMC, Kueter E, Bakker AQ, Schumacher TNM, Spits H.Enrichment of an antigen-specific T-cell response by retrovirallytransduced human dendritic cells. Cell Immunol 1999; 195: 10-7.Jacobs H, Krimpenfort P, Haks MC, Blom B, Démoliere C,Kruisbeek AM, Spits H, Berns AM. PIM-1 reconstitutes thymuscellularity in interleukin-7 and common γ chain mutant mice andpermits thymocyte maturation in Rag- but not in CD3γ-deficientmice. J Exp Med 1999; 190: 1059-68.Jaleco A-C, Stegmann APA, Heemskerk MHM, Couwenberg F,Bakker AQ, Weijer K, Spits H. Genetic modification of human B-cell development. B-cell development is inhibited by the dominantnegative helix loop helix factor Id3. Blood 1999; 94: 2637-46.55IMMUNOLOGYNotes1 Funding: NWO (Netherlands Organization for ScientificResearch), Project 901-03-317.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1275.3 Funding: ARC, France.4 Funding: Ciba-Geigy, Japan (till 11/99); Dutch CancerSociety, Project <strong>NKI</strong> 99-2051 (from 11/99).5 Funding: NWO (Netherlands Organization for ScientificResearch), Project 901-03-317.6 Funding: Netherlands Cancer Society, Project <strong>NKI</strong> 96-1248.7 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2051.Publications: Development and functionof human T cellsPallard C, Stegmann APA, Van Kleffens T, Smart F, VenkitaramenA, Spits H. Distinct roles of the phosphatidylinositol 3-kinase andSTAT5 pathways in IL-7-mediated development of human thymocyteprecursors. Immunity 1999; 10: 525-35.Res PCM, Couwenberg F, Vyth-Dreese FA, Spits H. Expression ofpre-Tα mRNA in a committed DC precursor in the human thymus.Blood 1999; 94: 2647-57.Res PCM, Spits H. Developmental stages in the human thymusSemin Immunol 1999; 11: 39-46.In vitro and in vivoanalysis of T-cellfunctionBlom B, Heemskerk MHM, Verschuren MCM, Van Dongen JJM,Stegmann APA, Bakker AQ, Couwenberg F, Res PCM, Spits H.Overexpression of the helix-loop-helix factor Id3 in committed Tcell progenitors blocks TCR αβ but not TCR γδ development.EMBO J 1999; 18: 2793-802.Blom B, Verschuren MCM, Heemskerk MHM, Bakker AQ, VanGastel-Mol E, Wolvers-Tettero ILM, Van Dongen JJM, Spits H.TCR rearrangements and expression of the pre-T cell receptorcomplex during human T cell differentiation. Blood 1999; 93:3033-43.Dardalhon V, Noraz N, Pollok K, Rebouissou C, Boyer M, BakkerAQ, Spits H, Taylor N. Green fluorescent protein as a selectablemarker of fibronectin-facilitated retroviral gene transfer in primaryhuman T lymphocytes Human Gene Ther 1999; 10: 5-14.Galy A, Christopherson I, Ferlazzo G, Wesa A, Spits H,Georgopoulos K. Human lymphoid-related DC: A distinct populationof antigen presenting cells requiring Ikaros for hematopoiesis.Blood (in press).Haks MC, Oosterwegel MA, Blom B, Spits H, Kruisbeek AM. Cellfatedecisions in early T-cell development: regulation by cytokinereceptors and the pre-TCR Semin Immunol 1999; 11: 23-37.TNM Schumacher PhDJBAG Haanen MD PhDHH Kessels MSc 1K Schepers MSc 2G Stötter MSc 3M Wolkers MScM Toebes 2M Van Den Boom 1D FontijnM CoccorisGroup leaderAcademic staffGraduate studentGraduate studentGraduate studentGraduate studentTechnicianTechnicianUndergraduate studentUndergraduate studentThe aim of our research is two-fold: 1) thedevelopment of novel strategies that can be used toexamine protein interactions which should be of generalvalue for biological and pharmaceutical research; 2) theuse of such tools to unravel and manipulate themolecular processes underlying immune recognition by Tlymphocytes. Amongst other things, in the past year thiscombination of technology development and biologicalresearch has resulted in a strategy for retroviral T-cell
56IMMUNOLOGYFigure IV.1A retroviral TCR display library, based on an influenza A-specificT-cell receptor (F5) was screened for variant T-cell receptorsspecific for the CTL epitopes from influenza strains A/NT/60/68(NT-1) and A/PR8/34 (PR-1). Biological function of the selectedT-cell receptors was assessed by monitoring ligand-inducedT-cell activation, using a YFP reporter construct. Note that thein vitro selected TCRs display absolute ligand specificity for theT-cell epitope.receptor display that may be used to select TCRs withdesirable specificities in vitro, and has led to an understandingof the role of memory T cells during theencounter of random antigenic variants in vivo.Molecular recognitionSpecificity and affinity in SH2-ligand interactionsProtein-protein interactions are often mediated by therecognition of short continuous amino acid stretches byprotein domains. Affinity-based selection strategies havesuccessfully been used to define recognition motifs for alarge series of protein domains, such as SH2, SH3 andPTB domains. However, it is unclear whether in vivoligands do evolve towards an optimal affinity and, indeed,many physiological ligands only partially conform to themotifs that have been identified. We have developed anovel library screening technology that can be used todirectly define ligands for protein domains based not onlyon affinity but also on specificity of binding. We havedocumented the value of this approach by the selectionof peptide ligands that are either highly specific for theGRB2 SH2 domain, or that are cross-reactive betweendistantly related SH2 domains. Comparison of theseselected ligands with previously identified physiologicalligands for the GRB2 SH2 domain suggests that formany of these ligands, specificity of binding may be animportant factor in ligand selection in vivo.Isolation of low affinity ligandsThe development of technologies that allow theassembly and screening of synthetic libraries of smallmolecules holds promise for the identification of novelligands for target molecules of therapeutical interest.However, for most target molecules no high affinityligands are represented in these molecular libraries. Inaddition, the available strategies for the identification ofligands from these libraries are ill-suited for the detectionof low affinity ligands. The identification of such lowaffinity ligands would be of significant value, since thedefinition of these ligands would greatly facilitate thesubsequent identification of high affinity ligands, bypermitting a non-random walk through sequence space.We have developed a strategy that can be used toenhance the affinity of the interaction between librarymembers and target molecules in an artificial mannerusing disulphide chemistry. This approach rests on simplethermodynamic principles and requires no priorknowledge about the binding site or ligand preference ofthe target molecule. We have demonstrated the value ofthis strategy for the identification of low affinity ligands fortarget molecules by the selection of peptide ligands forthe N-SH3 domain of the adaptor protein c-Crk. The lowaffinity ligands identified using this strategy should proveuseful substrates for approaches for affinity optimization.Retroviral TCR displayThe diversity of the T-cell receptor (TCR) repertoire islimited due to the processes of positive and negative T-cell selection. In order to obtain T cells with specificitiesbeyond the immune system’s capacity, we havedeveloped a strategy for retroviral TCR display. Using thisapproach, an in vitro T-cell library of variants of aninfluenza A-specific T-cell receptor was generated andscreened for the occurrence of TCRs with a desiredspecificity. We have documented the value of TCRdisplay by selection of variant T-cell receptors that eitherrecognize the parental T-cell epitope, or that haveacquired a novel specificity for a different influenza Astrain. In collaboration with the group of H Spits we haveshown that these manipulated TCRs initiate full T-cellactivation upon ligand recognition in vitro (Figure IV.1).Retroviral TCR display opens the possibility for thegeneration of high affinity tumor specific TCRs, bycircumventing T-cell self tolerance. This potentiallyimportant application of retroviral TCR display will be thesubject of further studies.
Dissecting cytotoxic T-cell responsesIn situ detection of antigen specific T-cell immunityOver the past years, the development of novelstrategies that can be used to visualize antigen specificT-cell responses by flow cytometry has radically changedour understanding of the dynamics and magnitude ofantigen-specific T-cell immunity. Through the use of tetramericMHC complexes, massive expansions of antigenspecificCD8 + T cells have been demonstrated andcharacterized for a variety of pathogens. However, theinability to use these reagents for the detection ofantigen-specific T-cell responses in tissue sections hasprecluded a parallel anatomical dissection of T-cellimmunity. In collaboration with F Vyth-Dreese from theImmunotherapy group, L Oomen from the Department ofBiophysics, and the group of A Kruisbeek, we haverecently developed a strategy that permits the use ofMHC tetramers for the direct in situ visualization ofantigen specific T-cell responses. The combined use ofMHC tetramer technology and confocal laser scanningmicroscopy allows detection of both virus- and tumorspecificCD8 + T cells in lymphoid organs, peripheraltissues and tumor infiltrates. The value of this techniquefor the study of the anatomy of tumor-reactive T-cellimmunity, in particular in melanoma patients, will be thesubject of future studies.T-cell responses against antigenic variantsThe role of memory T cells during the immuneresponse against random antigenic variants has not beenresolved. In collaboration with the group of AdaKruisbeek we have used a strategy employing the simultaneousstaining of polyclonal T-cell populations with twotetrameric MHC-peptide molecules to address this issue.These experiments demonstrate that the polyclonal CD8 +T-cell response against a series of natural variants of theinfluenza A CTL epitope is completely dominated byinfrequent cross-reactive T cells that expand from anoriginal memory T-cell population. Based on both biochemicaland functional criteria, these cross-reactivecytotoxic T cells productively recognize both the parentaland the mutant epitopes in vitro and in vivo. Theseresults provide direct evidence that polyclonal memory T-cell populations can provide protection against a range ofantigenic variants, and suggest that random mutations ofTCR-exposed residues of CTL epitopes are unlikely toresult in efficient CTL escape.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1442.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2036.3 Funding: NWO (Netherlands Organization for ScientificResearch), Project 901-02-215.Publications: Analysis of T-cell functionHaanen JBAG, Toebes M, Cordaro TA, Wolkers MC, KruisbeekAM, Schumacher TNM. Systemic T-cell expansion during localizedviral infection. Eur J Immunol 1999; 29: 1168-74.Schumacher TNM. Accessory to murder. Nature 1999; 398: 26-7.Heemskerk M, Hooijberg E, Ruizendaal JJ, Van Der Weide MC,Kueter E, Bakker AQ, Schumacher TNM, Spits H. Enrichment ofan antigen specific T-cell response by retrovirally transducedhuman dendritic cells. Cell Immunol 1999; 195: 10-7.Diehl L, Den Boer ATh, Schoenberger SP, Van der Voort EIH,Schumacher TNM, Melief CJM, Offringa R, Toes R. CD40 activationin vivo overcomes peptide-induced peripheral cytotoxic T-lymphocyte tolerance and augments anti-tumor vaccine efficacy.Nature Med 1999; 5: 774-9.Haanen JBAG, Wolkers MC, Kruisbeek AM, Schumacher TNM.Selective expansion of cross-reactive CD8 + memory T cells byviral variants. J Exp Med 1999; 190: 1319-28.Smyth Reynolds LA, Tyrrell R, Williams O, Norton T, Tybulewicz V,Schumacher TNM, Ley SC, Kioussis D. Altered peptide ligandsand signalling in primary thymocytes. In: Cold Spring HarborSymposia on Quantitative Biology, Vol LXIII. Signaling & GeneExpression in the Immune System, Cold Spring Harbor: CSHPress, 1999 (in press).GC De Gast 1 MD PhDD De Jong MD PhD 2FA Vyth-Dreese PhDM Van Oijen PhDA Van Puijenbroek PhDW Vooys PhDN Verra MSc 2TAM DellemijnJ Sein 3WF Van de KasteeleCJC Van den Bogaard 3S EliasImmunotherapyGroup leaderAcademic staffAcademic staffPost-docPost-docPost-docGraduate studentTechnicianTechnicianTechnicianTechnicianUndergraduate studentThe role of T-cell co-stimulation in low grade B-cell nonHodgkin’s lymphoma (B-NHL)In a previous study, immunohistochemical analysis ofB-cell non Hodgkin’s lymphomas (B-NHL) showed the57IMMUNOLOGY
58IMMUNOLOGYpresence of co-stimulatory receptors on the tumor Bcells and their ligands on intermingled T lymphocytes.The preferential expression of these molecules, as well ascytokines, in low grade follicular lymphomas and extranodal mucosa-associated lymphoid tissue (MALT) NHLsuggested that these tumors are most optimallyequipped for, and possibly dependent on, functionalinteractions with T cells (Vyth-Dreese et al, Immunology1998; 94: 580-6). To test this hypothesis, patients withlow grade, gastric MALT NHL, who were treated withantibiotics to eradicate Helicobacter pylori as anti-cancertherapy (in collaboration with H Boot, Department ofGastro-enterology, Division X), were studied. The H. pylorieradication treatment is known to result in remissions inabout 70% of low grade MALT NHL patients, supportinga relative dependence of this B-cell lymphoma on H.pylori antigenic stimulation. A correlation was observedbetween the immunohistologically determined expressionof co-stimulatory receptors CD80 and CD86, the histopathologicalgrading of blast-like cells of type 2 and aclinical response to H. pylori eradication therapy. Theimplications of these observations are that in situ demonstrationof co-stimulatory molecules in MALT NHL tumortissues 1) indeed reflects a physiological process; 2) maypredict whether patients will respond to subsequent H.pylori eradication treatment. Further analysis of tumortissues from responding patients may reveal whetherqualitative and/or quantitative alterations of intermingled Tcells play a role in this response.Immunohistochemical analysis of renal cell carcinomas(RCC) from patients treated with immunotherapyIn a dose-toxicity pilot-study (in collaboration with SHorenblas, Division XI), triple cytokine immunotherapyconsisting of interleukin-2, interferon-α and granulocytemacrophage-colony-stimulatingfactor, has been given tometastatic RCC patients. From 8 out of 35 treatedpatients, tumor material was obtained after treatment.These tumor samples were compared to a control panelof 10 non-treated RCC for a large set of markers relatedto immunological reactions. In half of the treated patients,a more pronounced infiltrate was found compared to thecontrol RCC. Furthermore, in 5 out of 8 patients, infiltratingT cells were partly located between the tumorcells, whereas in the control RCC, T cells were predominantlyfound in the stroma. Moreover, several markerswere found to be expressed differentially in the treatedtumors compared to the control RCC. An increase wasfound in treated RCC for dendritic cells and an adhesionmarker. A decreased expression was found for restingmacrophages/dendritic cells, an activation marker andseveral co-stimulation markers on T cells. These datasuggest that triple cytokine immunotherapy induces ashift in the activation state of the tumor associatedinfiltrate, and increases the number of dendritic cellsneeded to initiate a specific immune response.Detection of dendritic cells of different subtypes andmaturation stages in tumor tissuesIn collaboration with the group of H Spits, wedescribed precursor lymphoid dendritic cells (DC) in thehuman thymus that have been suggested to have afunction in the survival of activated T cells. We thereforesearched for cells with the phenotype of precursorlymphoid DC in tumor tissues of patients with renal cellcarcinoma (RCC) and head and neck squamous cellcarcinoma (HNSCC), using immunohistochemistry andconfocal laser scanning microscopy (CLSM) analysis.Cells expressing typical lymphoid DC markers wereidentified in 5/6 tumor samples from HNSCC patients, 4of which also expressed the mature DC marker DCLAMP. Lymphoid DC were also identified in tissues from5/8 RCC patients treated with combined immunotherapywith IL-2, GM-CSF and IFNα, but in 0/6 untreatedpatients. RCC patients did not show expression ofmature myeloid DC markers regardless of whether theywere treated or not. Further confirmation on the presenceof precursor lymphoid DC in tumor tissues from treatedRCC patients was obtained using 3-color immunofluorescenceand CLSM analysis; myeloid origin could beexcluded. This surprising presence of precursors oflymphoid DC in tumor infiltrates warrants further investigationof their functional role.Detection of antigen specific T lymphocytes in tumortissues and bloodIn collaboration with the group of T Schumacher, anew strategy has been developed to visualize antigenspecificT cells in tissues through the use of tetramericpeptide/MHC complexes. This approach, when appliedto patients, will provide a useful tool for further detailedstudies on T-cell/tumor cell interactions in tumor infiltrates,and will also be applied in the monitoring ofimmunotherapy trials.Tetramer technology using HLA A2/melanosomalpeptides is also used for the detection of CTLs in peripheralblood of melanoma patients before and after nonspecificimmunotherapy with GM-CSF, low dose IL-2 andIFNα. In several patients, a ten-fold increase in thepercentage of Mart-1 specific CTLs has been observed.This creates a good basis for following the fate of tumorspecificCD8 T cells in melanoma patients enrolled indifferent immunotherapy trials.ImmunotoxinsReed-Sternberg (R-S) cells, the putative tumor cells ofHodgkin’s disease, consistently express the antigensCD80 and CD86. The cells are very sensitive forimmunotoxins directed to these antigens. Efficacy ofimmunotoxins is highly dependent on internalization ofthe complex by the target cell. Internalization experimentswith iodinated anti-CD80 and anti-CD86 mAbs indeedshow that both antigens are internalized upon binding ofthe mAb. Some R-S cell lines exhibit a strong inductionof aggregation in the presence of anti-CD86 mAb, but
not of anti-CD80. This aggregation does not match otherpreviously described types of homotypic aggregation, asit is not inhibited by blocking mAb to LFA-1 and ICAM-1,and is only partly dependent on Ca and Mg. A numberof different anti-CD86 mAb recognizing different epitopes,is capable of inducing aggregation and we speculate thatthis reflects CD86-mediated signaling. Indeed, Westernblot analysis of cells treated with anti-CD86 mAbrevealed activation of the ERK1/2 pathway only in the celllines that show aggregation. Since the CD86 moleculeitself does not become phosphorylated on its serineresidues in the intracytoplasmic tail, another moleculemight be involved which is associated with the CD86molecule. Such association has already been reported forCD80.Immunotoxins are also explored for treatment ofmultiple myeloma. The effect of an anti-CD138 plasmacell-specific immunotoxin (B-B4-SO6) in combination withthe chemotherapeutic drug doxorubicin was evaluated invitro on drug-sensitive and drug-resistant variants of themultiple-myeloma (MM)-derived cell line RPMI8226 andfreshly isolated malignant myeloma cells. Drug-resistantRPMI8226 cells were still sensitive to the immunotoxin,although to a lesser extent than drug-sensitive cells. Inthe clonogenic assay, drug-sensitive RPMI8226 cells areseveral logs more susceptible to immunotoxin induceddeath than the drug-resistant RPMI8226 cells. When asub-optimal dose of immunotoxin was combined withdoxorubicin, an additive effect was found for drugsensitiveRPMI8226 cells. The immunotoxin did notinfluence the sensitivity of resistant cells for doxorubicin.Both drug-sensitive and drug-resistant cells from MMpatients were also sensitive to the immunotoxin.Doxorubicin was effective only on sensitive MM cells, andthere was a tendency for an additive effect in the combinationof immunotoxin and doxorubicin on these cells.These studies will form the basis for further dissectingthe parameters dictating immunotoxin-sensitivity.Notes1 Division X.2 Division XIII.3 Laboratory of Clinical Chemistry / Hematology-Immunotherapy Laboratory.Publications: ImmunotherapyPost J, Vooijs WC, Bast BJEG, De Gast GC. Efficacy of an anti-CD138 immunotoxin and doxorubicin on drug resistant and drugsensitivemyeloma cells. Int J Cancer 1999; 83: 571-6.Res PCM, Couwenberg F, Vyth-Dreese FA, Spits H. Expression ofpTα mRNA in a Committed Dendritic Cell Precursor in the HumanThymus. Blood 1999; 94: 2647-57.MJ Kersten MD PhDM Schreurs PhD 1P Van den BerkImmunotherapy ofB cell non-Hodgkin’slymphomaGroup leaderPost-docTechnicianAdvanced follicular non-Hodgkin’s lymphoma (FL) is atpresent an incurable disease, with a median survival of 8years. FL forms an attractive target for immunotherapybecause it represents a well-defined clinico-pathologicalentity with an indolent disease course, and because itpossesses a tumor- and even patient-unique tumorantigen, the idiotype. Research of this recently formedgroup will focus on two projects (in collaboration with thegroup of H Spits, and with R van Oers, Department ofHematology, AMC, Amsterdam).Development of a novel lymphoma mouse modelCurrent lymphoma mouse models using transplantedlymphoma cell lines or lymphomas that are virally orchemically induced, resemble acute leukemia oraggressive lymphoma more than FL. Major disadvantagesof existing transgenic mouse models are that the introducedoncogene is present in the whole B-cellcompartment, and that they often lead to aggressivelymphomas, which are more often of T-cell than of B-cellphenotype. In collaboration with P Krimpenfort (DivisionVII), we aim to develop a novel mouse model with anincreased incidence of ‘spontaneous’ lymphomas, with aknown idiotype. For this purpose, anti-HEL-Ig transgenicmice will be crossed with bcl2 transgenic and/or p16conditional knockout mice. Cre/Lox switching for the p16tumor suppressor gene will take place either in vitro or invivo. Other combinations of transgenes are currentlybeing explored.Idiotype DNA vaccinationDue to its flexibility, DNA vaccination offers an idealmodel to study idiotype vaccination. Thusfar, idiotypevaccination has been shown to mediate tumor protectionmostly through a humoral anti-idiotype response. In botha transplantation lymphoma mouse model, and in thetransgenic mouse model, we aim at developing a DNAvaccine which will (through either targeting to antigenpresenting cells, or targeting into the MHC class Ipathway, or through combination with different cyto- orchemokines) elicit a protective CD8 + cytotoxic T-cellresponse directed against the lymphoma idiotype.Note1 Funding: Academic Medical Center, Amsterdam.59IMMUNOLOGY
60IMMUNOLOGYPublications: Immunotherapy of NHLBerger C, Van Baarle D, Kersten MJ, Klein MR, Samer Al-HomsiA, McQuain C, Van Oers MHJ, Knecht H. Carboxy terminalvariants of Epstein-Barr virus encoded LMP1 during longtermHIV-infection: reliable markers for individual strain identification. JInfect Dis 1999; 179: 240-4.Van Baarle D, Hovenkamp E, Kersten MJ, Klein MR, Miedema F,Van Oers MHJ. Direct Epstein-Barr virus typing on peripheralblood mononuclear cells: no association between EBV type 2infection or superinfection and the development of acquiredimmunodeficiency syndrome-related non-Hodgkinís lymphoma.Blood 1999; 93: 3949-55.Secretary Division of ImmunologyMA Van HalemResearch staff positions (full time equivalents)Scientific permanent: 5.0Scientific project: 18.0Technical permanent: 6.1Technical project: 7.0
V Division of Molecular Biology61Division head Ronald PlasterkIntroductionMajor research themes in the division are generearrangements, gene expression and signal transduction,functional genomics and drug resistance oftumor cells.The Borst group is working on two topics, antigenicvariation in African trypanosomes, and multidrugresistance in tumor cells. The goal of the trypanosomeproject is to determine how trypanosomes manage torepeatedly change their surface molecules allowing themto escape immune destruction in the bloodstream of thehost. Recent work focuses on the role of base J, β-glucosylhydroxymethylU, a new minor base discoveredby the Borst group in trypanosomes. In 1999 the Borstgroup identified a protein that specifically binds to J inDNA. Disruption of the gene for this J-binding protein(JBP1) was found to have no gross effect on growth orgene expression, but reduced the level of J in the T.brucei genome 10-to 30-fold. It therefore appears that J-binding protein can set up a chromatin structure resultingin additional conversion of thymine into J. A second J-binding protein was identified and this JBP2 is beingcharacterized.In the Borst multidrug resistance (MDR) group theemphasis is on MRPs (multidrug resistance proteins), afamily of 6 related membrane proteins. Two of these,MRP1 and 2, have been shown to be organic anionpumps able to transport drugs conjugated to glutathioneout of the cell. In 1999, the Borst group showed thatcells overexpressing MRP3 can become resistant toetoposide and methotrexate, whereas overexpression ofMRP5 results in resistance to purine base analogs,probably because MRP5 is an organic anion pump ableto transport nucleotide analogs. This is an interestingnew addition to the range of drug classes affected bydrug pumps of the MRP family.The Plasterk group studies the nematodeCaenorhabditis elegans as a model system, in particularthe mechanism and regulation of DNA transposition andof signal transduction in the nervous system. This yearthe group identified a gene that is required for silencingof transposable elements in the germline of the animal;loss of function mutants of this gene (mut-7) showfrequent mutations in progeny animals, as a result ofjumping of Tc1, Tc3 and other transposons into genes.Surprisingly this gene, as well as many other similar‘mutator’ genes are also required for the effect of RNAinterference (RNAi), the silencing of gene expression afterexperimental introduction of double stranded RNA. Thissuggests that the function of the RNA interferencesystem may be to silence repetitive elements, such astransposons and viruses. Using the available completesequence of the C. elegans genome, the group identifiedmany SNPs (single nucleotide polymorphisms), anddeveloped a method to use these SNPs for quick genemapping (using so-called snip-SNPs, polymorphisms thatcan be scored because they change a restriction enzymecleavage site). This method is now being used to identifygenes involved in perception. A complete inventory wasmade of all G protein genes of the animal: for each of the25 genes the expression pattern was studied, as well asthe phenotype of knock out mutants; this showed thatmost G protein genes are specifically expressed insensory neurons and are involved in perception.The division is undergoing major changes. P Borstgave up his directorship of the <strong>NKI</strong>/<strong>AvL</strong>, and will be ableto focus his attention on his own research projects.Having reached the age of mandatory retirement byDutch law, he will continue his own research group for atleast five more years, as an honorary staff member andmember of the division. R Plasterk will become the newdirector of the Hubrecht Laboratory in Utrecht and heand his research group will move to Utrecht early nextyear. In the coming year the division will thereforeundergo major changes, and see new research groupsmove in.
MOLECULAR BIOLOGY62Caenorhabditis elegansRHA Plasterk PhDHGAM Van Luenen PhD 1E Cuppen PhD 2I Garcia-Saez PhD 3Z Iszvak PhD 3Z Ivics PhDG Jansen PhD 4M Tijsterman PhD 5C Van den Berg PhD 6M Verheijen PhD 7S Wicks PhD 8E BerezikovSEJ Fischer 9M HilliardR Ketting 10R Koch 11C Moorman 8F Simmer 12S Van der Linden 2E HazendonkK Thijssen 2M Van der Horst 8T HaverkampJ PothofE WienholdsGroup leaderAcademic staffPost-docPost-docPost-docPost-docPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentUndergraduate studentTransposons in Caenorhabditis elegans and otherorganismsThe Tc1/mariner superfamily of transposons is found indiverse species, from fungi to human, and seems to havespread by horizontal as well as vertical transfer. Theelements are in essence single genes that encode thetransposase protein, flanked by inverted repeats that thetransposase protein recognizes to initiate the transpositionprocess.The most active transposon in C. elegans is Tc1. Overthe years the group has studied the mechanism andregulation of jumping of this element (plus the related Tc3transposon). This year we finished a study to define theminimal cis-requirements for transposition; it turns outthat approximately 100 base pairs of the termini of Tc1and of Tc3 are sufficient for jumping. We compared thefrequency of jumping of Tc1 and Tc3 in heterologoushosts (mouse NIH 3T3 cells and human HeLa cells) tothat of the mariner element from Drosophila and theSleeping Beauty transposon (reconstructed from severaldead transposons in the fish genome). We found thatSleeping Beauty is 40 times more active. Most probablythis indicates that Tc1 and Tc3, as naturally occurringelements, have been selected for sub-optimal activity (tokeep their hosts alive), while the Sleeping Beauty elementwas a reconstructed element in its most aggressive state.The genome of the second isolate of C. elegans(Bristol N2) contains 33 copies of Tc1. We analyzed theirsequences in detail, and found that virtually all have adistinctive set of SNPs (Single NucleotidePolymorphisms). These can be used to identify andfollow individual elements in the genome. Surprisinglythere are three cases of elements with exactly the sameSNP types; these are all within 2 map units of a siblingelement, suggesting they once jumped to a neigbouringposition in the genome.The Bristol N2 strain itself is not permissive for transposition:the pattern of Tc1 and other transposonsremains exactly identical in consecutive generations. Wepreviously described the isolation of an EMS-inducedmutant derivative of Bristol N2 in which Tc1 and othertransposons had become mobile (also see below). In thisstrain we see new Tc1 insertions appear, and weinspected their SNP patterns. One conclusion is thatthere is some preference for local jumping, so that newTc1 insertions often have SNP types similar to that of adonor locus nearby in the genome. However, in somecase we see new SNP types, that are combinations ofSNPs of elements originally present in the N2 isolate.Apparently recombination has occurred between Tc1types. Interestingly some of the resident Tc1 copies, stillpresent at the position in the genome where they were inthe starting strain, had also switched SNP type. Thissuggests that recombination may not occur to elementsthat are excising and reintegrating into new loci, but thatit occurs during the DNA double strand break repair ofthe donor site after Tc1 excision. We refer to this phenomenonas ‘transposon type switching’, which seemsmechanistically related to mating type switching in yeast.As mentioned above, we isolated multiple mutantFigure V.1A model for MUT-7 action. A complex of proteins, indicated byX,Y, and MUT-7, binds a dsRNA molecule. The dsRNA specificallytargets the complex to homologous mRNA by an yetunknown mechanism, which needs at some level base pairingbetween the dsRNA and the target mRNA. This leads to degradationof the bound mRNA by the Rnase function of MUT-7.Because of the homology to RNaseD, this is expected toproceed in a 3’-5’ direction. The dsRNA could survive thisprocess and target the nuclease complex to the next mRNAmolecule.
derivatives of N2 in which repression of transposition waslost. We now identified one of the genes, mut-7, at themolecular level. It encodes a putative nuclease, homologof RNaseD, a 3’ to 5’ exonuclease. This may explain theintriguing observation that mut-7 mutants, as well 20other mutator mutants we isolated, are resistant to theexperimental silencing of gene expression by introductionof double stranded RNA, referred to as RNAi or RNAinterference. We postulate that the MUT-7 protein,probably complexed to other proteins, and to a ‘guideRNA’ which is double stranded, targets mRNA molecules(based on homology to the dsRNA), and degrades themenzymatically (see Figure V.1). This effect is lost in mut-7mutants. The relation to transposon silencing may be thattransposons, as soon as they occur in multiple copies inthe genome, are bound to be transcribed by fortuitousread-through transcription from flanking promoters; theresult would be RNA made from each of the transposonstrands, allowing formation of dsRNA. In this model theRNAi machinery is a surveillance system that recognizesrepetitive sequences in the genome, sees them aspotential threats, molecular parasites, and repressesexpression of their transposase.Signal transduction in the C. elegans nervous systemWe studied the entire family of G proteins, which arethe connectors between membrane spanning receptorsthat recognize the outside world of cells and intra-cellularsignal transduction cascades. The family consists of twogenes encoding the beta subunits, two (recognized thusfar) for the gamma subunits, and twenty for the alphasubunits. As reported before, we analyzed the expressionpatterns of all these genes, and their phenotypes, andwe conclude that most G protein genes are (almost)exclusively expressed in sensory neurons of the amphidorgans, and that their mutation (loss or gain of function)in several cases affect chemotactic responses.We performed mutant screens to search for genesspecifically involved in chemo-perception of solubletastants, and found several such mutants. These arecurrently being mapped, as well as a mutation previouslyidentified by the lab of C Bargmann (University ofCalifornia, San Francisco), adp-1, which affectsadaptation to chemical tastants.Functional genomics of C. elegansWe screened wild type isolates for Single NucleotidePolymorphisms (SNPs) by shotgun sequencing ofgenomic DNA and comparison to the canonicalsequence of the Bristol N2 isolate. We found an overrepresentationof SNPs in non-coding regions, and withincoding regions in silent third-base positions. Lessexpected was that we found a strong clustering of SNPsin the ‘arms’ of the chromosomes compared to thecentral regions. This fits with the observation that thecenters contain a higher proportion of conserved genes(as scored by matches to yeast genes), and suggeststhat there are higher rates of evolutionary changes ofgenes in the chromosome arms.SNPs are ideal markers for gene mapping. Weselected a set of what we call ‘snip-SNPs’, these areSNPs that change the restriction pattern of a DNAregion, and can thus be recognized by PCR followed bya restriction enzyme snip. In collaboration with the groupof R Waterston (Washington University, St. Louis) weselected a set of snip-SNPs that cover the entiregenome, so that genes can now be mapped in a quick,easy and cheap fashion. These data are being madeavailable to the research community via the world wideweb, in an easily searchable fashion.Notes1 Funding: Fellowship Human Frontier Science ProgramOrganization (HFSPO).2 Funding: Netherlands Organization for ScientificResearch (NWO 940-70-008).3 Funding: EMBO fellowship.4 Funding: Netherlands Organization for ScientificResearch (NWO 805-48-009).5 Funding: SmitKline Beecham.6 Funding: Netherlands Organization for ScientificResearch (NWO 901-04-209).7 University of Utrecht, Utrecht.8 Funding: Netherlands Organization for ScientificResearch (NWO 901-04-094).9 Funding: Netherlands Organization for ScientificResearch (NWO/Stichting Scheikundig Onderzoek:SON 335-210).10 Funding: Netherlands Organization for ScientificResearch (NWO 940-70-008).11 Funding: Center for Biomedical Genetics.12 Funding: Netherlands Organization for ScientificResearch (NWO/Stichting Scheikundig Onderzoek:SON 97-045).Publications: C. elegansEijkelenboom APAM, Sprangers R, Hard K, Puras Lutzke RA,Plasterk RHA, Boelens R, Kaptein R. Refined solution structure ofthe C-terminal DNA-binding domain of HIV-1 integrase. Proteins1999; 36: 556-64.Fischer SEJ, Van Luenen HGAM, Plasterk RHA. Cis requirementsfor tramsposition of Tc1-like transposons in C. elegans. Mol GenGenet 1999; 262: 268-74.Jansen G, Thijssen KL, Werner P, Van der Horst M, Hazendonk E,Plasterk RHA. The complete family of genes encoding G proteinsof Caenorhabditis elegans. Nature Genetics 1999; 21: 414-419.Ketting RF, Haverkamp THA, Van Luenen HGAM, Plasterk RHA.mut-7 of C. elegans, required for transposon silencing and RNAinterference, is a homolog of Werner syndrome helicase andRNaseD. Cell 1999; 99: 133-41.Korswagen HC, Van der Linden AM, Plasterk RHA. G-protein63MOLECULAR BIOLOGY
64MOLECULAR BIOLOGYhyperactivation of the Caenorhabditis elegans adenylyl cyclaseSGA-1 induces neuronal degeneration. EMBO J. 1998; 17: 5059-65.Plasterk RHA. Hershey heaven and Caenorhabditis elegans.Nature Genetics 1999; 21: 63-4.Plasterk RHA. The year of the worm. BioEssays 1999; 21: 105-9.Plasterk RHA, Izsvak Z, Ivics Z. Resident aliens, the Tc1/marinersuperfamily of transposable elements. Trends in Genetics 1999;15: 326-32.Plasterk RHA, Van Luenen HGAM, Vos C, Ivics Z, Isvak Z, FischerS. Elements transposables: des outils permettant la mutageneseet la transgenese chez les vertebres. Pathologie Biologie 1998;46: 661-732.Van den Ent FMI, Vos A, Plasterk RHA. Dissecting the role of theN-terminal domain of human immunodeficiency virus integrase bytrans-complementation analysis. J of Virology 1999; 73: 3176-83.P Borst PhDF Baas PhD 1R Evers PhD 2Z Hollo PhD 3M Kool PhD 2T Saeki PhD 4A Van Helvoort PhD 5P Wielinga PhD 2J Wijnholds PhD 2J Guo 6N Zelcer 2M De Haas 2C Mol 2L Van Deemter 2Multidrug resistanceGroup leaderAcademic staffPost-docPost-docPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentTechnicianTechnicianTechnicianMultidrug resistance (MDR) of cancer cells is usuallycaused by drug pumps that lower the intra-cellular drugconcentration by actively extruding drug from the cell.These pumps are large glycosylated plasma membraneproteins and of two types: P-glycoproteins (Pgps) andMultidrug Resistance (associated) Proteins (MRPs; seeFigure V.2). Whereas Pgps extrude unmodified hydrophobicdrugs, MRPs are also able to extrude drugs conjugatedto glutathione (GSH), glucuronic acid, or sulphate.Carriers with this property are known as GS-X pumps.To study the physiological function of Pgps and MRPswe have disrupted the genes for these proteins in mice.In this way we have shown that these transporters havean important function in protecting mammals againsthydrophobic drugs, but that they are not required for thewell-being of mice in the protected environment of the<strong>NKI</strong>/<strong>AvL</strong>. The work on drug-transporting Pgps is beingcontinued by the group of AH Schinkel (Division VIII). Weare concentrating on the further characterization of theMRP gene family.The Multidrug Resistance (associated) Protein 1To elucidate the physiological role of MRP1, we havegenerated mice lacking a functional Mrp1 gene, as wellas mice with disrupted Mrp1, Mdr1a, and Mdr1b genes,in collaboration with P Krimpenfort and AJM Berns(Division VII). Mice homozygous for disrupted Mrp1, orMrp1/Mdr1a/1b genes, are viable and fertile underlaboratory conditions, but the Mrp1 -/- mice are hypersensitiveto etoposide and the Mdr1a/1b -/- , Mrp1 -/- evenmore so.The hypersensitivity of Mrp1 -/- mice to etoposide isespecially manifest in cells which contain substantialamounts of Mrp1 in wild-type mice. In collaboration withL De Lange and D Breimer (Pharmacology, University ofLeiden) we have shown that the high Mrp1 concentrationin the basolateral membrane of the epithelial cells of thechoroid plexus protects the cerebrospinal fluid (CSF)against etoposide. In Mdr1a/1b -/- , Mrp1 -/- mice theetoposide level in the CSF rises 10-fold higher after i.v.administration than in the Mdr1a/1b -/- control mice. Wehave previously shown that P-glycoprotein in brain capillariesis important to protect the brain from amphipathicdrugs. MRP1 appears to play a similar role for drugs thatattempt to reach the brain via the choroid plexus andCSF.MRP3In addition to MRP1, we identified 5 other members ofthe human MRP family, cMOAT or MRP2, and MRP3-6.One of these, MRP2, has been characterized as anorganic anion transporter responsible for secretion ofbilirubin glucuronides and other organic anions from theliver into bile. For a more detailed analysis of MRP3, weisolated monoclonal antibodies specific for this protein (incollaboration with the group of R Scheper, FreeUniversity, Amsterdam) and constructed DNAs complementaryto full-length mRNA. These cDNAs were stablyintroduced into various non-polarized and polarized cellsby retroviral transduction. The only phenotype observedin transfected non-polarized cells is low-level resistanceto etoposide and teniposide (2-to 4-fold) and high levelresistance to brief (4 hour) incubations with high methotrexate(MTX) concentrations, but no resistance to lowMTX during continuous exposure. In collaboration with GJansen and coworkers (Medical Oncology, FreeUniversity, Amsterdam) we previously demonstratedsimilar results for cells overexpressing MRP1 and 2. Ithad long been known that mammalian cells containseveral transporters able to export MTX. It now seems
Figure V.2:Membrane topology model of full-length MRP1 and MRP5.MRP1 consists of a MDR1-like core region containing two ATPbinding sites (circles), two membrane-bound domains, and anN-terminal polypeptide region of about 280 amino acids, forminga membrane-bound domain and a cytoplasmic loop (TMD 0 andL 0, respectively). MRP5 lacks TMD 0.MRP1-3, but all our attempts to demonstrate MRP5-mediated resistance to MDR drugs have remainedunsuccessful. However, we found low level resistance tosulphur-containing purine base analogs, 6-mercaptopurine(6-MP) and 6-thioguanine. When MRP5 transfectantsare loaded with radioactive 6-MP, they export theradioactivity more rapidly than untransfected control cells.In the course of 1999 Schuetz and coworkers discoveredthat MRP4 is associated with resistance to nucleotideanalogs, such as PMEA, 9-(2-phosphonylmethoxyethyl)adenine.We tested this drug on ourMRP5-transfected cells and found low-level resistance. Itis therefore possible that MRP5 is an organic anion pumpwith a preference for nucleotide analogs, resistance to 6-MP being due to the conversion of this base into itsnucleotide analog, 6-thio-IMP.We have generated knock-out mice lacking MRP5.These mice are healthy and fertile showing that MRP5has no essential function in mice in a protectiveenvironment. Whether these mice are hypersensitive tobase/nucleoside/nucleotide analogs is under investigation.65MOLECULAR BIOLOGYlikely that these transporters are the MRPs. Within thecell MTX is slowly polyglutamylated. We have found thatthe polyglutamylated forms are not transported by MRPs.The difference between short- and long-term MTXexposure is therefore probably due to competitionbetween export by MRP and polyglutamylation by folylpolyglutatamatesynthetase (FPGS), as illustrated inFigure V.3. During long-term MTX incubations enoughMTX polyglutamates can accumulate to inhibit cell multiplication.In polarized cells overexpression of MRP3 gives rise toincreased export of dinitrophenyl-glutathione at thebasolateral side, but not of GSH itself (unlike MRP1 and2). To study the substrate specificity of MRP3 in moredetail we have expressed the protein in insect cells usinga baculovirus MRP3 construct. Vesicles isolated fromthese cells transport estradiol-17-β-glucuronide in anATP-dependent fashion. MRP3 levels are relatively high insmall bile canaliculi and in the gut epithelium, and the lowMRP3 level normally found in the liver is highly upregulatedin liver disease. It is therefore possible that MRP3plays a role in bile salt metabolism. We are generatingmice with disrupted MRP3 genes to get more informationabout the physiological function of MRP3 and itspotential for causing drug resistance.MRP5MRP5 differs from MRP1, 2, 3 and 6 in that it lacksthe TMD0 part of the protein (Figure V.2). We havecloned full-length MRP5 cDNA and expressed this intransfected cells. In polarized cells MRP5 is routed to thebasolateral membrane where it can mediate export of S-glutathionyl 2,4-dinitrobenzene and glutathione itself.MRP5 is also inhibited by benzbromarone, an inhibitor ofother MRPs. MRP5 is therefore a GS-X pump, likeFigure V.3MRPs and folylpoly-γ-glutamate synthetase (FPGS) compete forMTX. MTX is taken up by the cells via the reduced folate carrier(RFC) and overexpression of MRP results in transport ofunmodified MTX. Polyglutamylated MTX is formed in a relativelyslow reaction by FPGS and this results in the efficient inhibitionof dihydrofolate reductase (DHFR).Notes1 Staff member Academic Medical Center, Amsterdamand honorary staff member <strong>NKI</strong>/<strong>AvL</strong>.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1794.
66MOLECULAR BIOLOGY3 Funding: Netherlands Organization for ScientificResearch, NWO-OTKA 048-011-021.4 Funding: Japan Society for the Promotion of Science.5 Funding: Netherlands Organization for ScientificResearch, NWO 902-23-097.6 Funding: Ministry of Education & Science of TheNetherlands (O C & W).Publications: Multidrug resistanceAllen JD, Brinkhuis RF, Wijnholds J, Schinkel AH. The mouseBcrps/Mxr/Abcp gene: amplification and overexpression in celllines selected for resistance to topotecan, mitoxantrone, or doxorubicin.Cancer Res 1999; 59: 4237-41.Arts HJ, Katsaros D, De Vries EG, Massobrio M, Genta F, DaneseS, Arisio R, Scheper RJ, Kool M, Scheffer GL, Willemse PH, Vander Zee AG, Suurmeijer AJ. Drug resistance-associated markersP-glycoprotein, multidrug resistance-associated protein 1, multidrugresistance-associated protein 2, and lung resistance proteinas prognostic factors in ovarian carcinoma. Clin Cancer Res1999; 5: 2798-805.Borst P, Van Blitterswijk WJ, Borst J, Tepper AD, Schinkel AH.New physiological functions for drug-transporting P-glycoproteins?Drug Resistance Updates 1998; 1: 337-9.Borst P. Multidrug resistance - A solvable problem? ECC:Biliopancreatic Malignancy: From Gene to Cure, Febr 4-6, 1999.Annals of Oncol. 1999; 10 S4: 162-4.Borst P, Evers R, Kool M, Wijnholds J. The multidrug resistanceprotein family. Biochim Biophys Acta: special issue ‘Structure andfunction of ABC transporters’ 1999; 1461: 347-57.Borst P, Zelcer N, Van Helvoort A. ABC-Transporters in lipid transport.Biochim Biophys Acta; special issue on Intracellular LipidTransport. 1999 (in press).Van Helvoort A, De Brouwer A, Ottenhoff R, Brouwers JFHM,Wijnholds J, Beijnen JH, Rijneveld A, Van der Poll T, Van der ValkMA, Majoor D, Voorhout W, Wirtz KWA, Oude Elferink RPJ, BorstP. Mice without phosphatidylcholine transfer protein have nodefects in the secretion of phosphatidylcholine into bile or into thelung airspaces. Proc Natl Acad Sci USA 1999; 96: 11501-6.Antigenic variation in TrypanosomesP BorstM Cross PhD 1D Dooijes PhD 2R Mussmann PhD 3B Sabatini PhD 2I Chaves 4H Gerrits 2S Ulbert 5A Dirks 2R Kieft 2Group leaderPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentTechnicianTechnicianTrypanosoma brucei, the causative agent of AfricanSleeping Sickness in humans, is a unicellular parasitetransmitted to the mammalian host by the tsetse fly. Inthe bloodstream of the mammal, the trypanosome avoidsimmune destruction by repeatedly changing its VariantSurface Glycoprotein (VSG) coat. A given coat isencoded by a single gene from a repertoire of up to athousand different VSG genes. To be expressed, thesegenes have to move to one of several expression sites,containing additional Expression Site Associated Genes(ESAGs) and located adjacent to a telomere (see FigureV.4). Antigenic variation occurs by replacing the VSGgene in the active expression site or by switching toanother site.Hooijberg JH, Broxterman HJ, Kool M, Assaraf YG, Peters GJ,Noordhuis P, Scheper RJ, Borst P, Pinedo HM, Jansen G.Antifolate resistance mediated by the multidrug resistance proteinsMRP1 and MRP2. Cancer Res 1999; 59: 2532-5.Kool M, Van der Linden M, De Haas M, Baas F, Borst P.Expression of human MRP6, a homologue of the multidrug resistanceprotein gene MRP1, in tissues and cancer cells. CancerRes 1999; 59: 175-82.Kool M, Van der Linden M, De Haas M, Scheffer GL, De Vree ML,Smith AJ, Jansen G, Peters GJ, Ponne N, Scheper RJ, OudeElferink RPJ, Baas F, Borst P. MRP3, a new organic anion transporterable to transport anti-cancer drugs. Proc Natl Acad SciUSA 1999; 96: 6914-9.Paulusma CC, Van Geer MA, Evers R, Heijn M, Ottenhoff R, BorstP, Oude Elferink RPJ. The canalicular multispecific organic aniontransporter (cMOAT/MRP2) mediates low-affinity transport ofreduced glutathione. Biochem J 1999; 338: 393-401.Figure V.4J in expression site. Schematic representation of an active andan inactive VSG gene expression site. The flag indicates thepromoter, The modified DNA base J is present in the 50 bprepeat and telomeric repeat arrays flanking both active andinactive sites. In silent expression sites the VSG gene, 70 bprepeats and ESAGs are also modified.Control of VSG expression sitesA central question in antigenic variation is how thebloodstream form trypanosome can silence all VSGexpression sites but one, even though there are some 20expression sites that look alike. Our earlier worksuggested a model for expression site control involvingthree states: off, pre-active and active. Whereas thetransition from off to pre-active or active is infrequent
(about 10-6), the transition from pre-active to active issufficiently frequent to allow the selection of unstabledouble expressors. Such unstable double expressorsmight be intermediates in normal switching from oneexpression site to the next.To test this mechanism further we have marked a thirdexpression site with a new resistance marker, blasticidinresistance. We have also succeeded in visualizing anexpression site in living trypanosomes using the systemdeveloped by Belmont and coworkers (University ofIllinois, Urbana, USA). This involves the insertion of a LACoperator gene array upstream of an expression site.When a construct encoding green fluorescent proteinfused to a LAC repressor is introduced in the trypanosomesthe operator gene array becomes a greenfluorescent dot dancing in the microscope field in theliving trypanosome. This system should allow us to keeptrack of expression sites when they are activated andinactivated.DNA modification and antigenic variationWe have previously shown that bloodstream formT.brucei contains a novel DNA base b-D-glucosyl-hydroxymethyluracil,called J. To determine the location of J inthe genome, we have generated J-specific antiseraraised against JMP. By immunoprecipitation of J-containing DNA fragments, we showed that J is presentin and around VSG genes in inactive expression sites,and never in transcribed VSG genes (see Figure V.3).Nevertheless, we have also found J in other repetitivesequences, which suggests that J might have a widerfunction and is not just involved in silencing of expressionsites. This is supported by our identification of J in otherkinetoplastids, including Leishmania, T.cruzi, and Crithidia,which do not undergo antigenic variation, and in Euglena.We did not find J in mammals, Drosophila, C.elegans, oryeast (Figure V.5).Figure V.5Evolution tree. J is present in all kinetoplastida, in Diplonemaand Euglena gracilis, but not elsewhere in nature.A J-binding proteinThe presence of J in DNA must somehow be translatedinto nuclear action (altered chromatinstructure/transcription, etc.) and we expect this translationto be mediated by J-binding protein(s). We havefound such a protein in nuclear extracts using a specificband shift assay of labeled oligonucleotides in acrylamidegels. The collaboration with J Van Boom’s group inLeiden University, gave us access to a range of oligodeoxynucleotidescontaining either J, hydroxymethyluracilor thymine in defined sequences. We have purified the J-binding protein from Crithidia extracts and cloned thecorresponding gene. J-binding protein is a novel proteinwith a predicted mass of 90.4 kDa. By homology we alsocloned the J-binding protein genes of T.brucei andLeishmania.To study the function of J-binding protein we havedisrupted the two alleles of the gene in T.brucei.Remarkably, this has no effect on the multiplication of thetrypanosomes, on their ability to keep silent VSG geneexpression sites repressed, or on the rate of switchingfrom one expression site to another. We find, however,that the J level of trypanosomes without J-binding proteinis 10- to 30- fold lower than of wild-type trypanosomes.The difference is not due to turn-over of J. A possibleexplanation for this unusual result is that J-bindingprotein can change chromatin structure resulting in anadditional conversion of Thy into J. As the effect of J-binding protein appears to be subtle, we are alsodisrupting the gene for J-binding protein in Leishmaniamajor. This should allow us to test the effect of theabsence of this protein in a complex competitive biologicalsystem, i.e. chronic infections in macrophages ormouse foot pads.By database search we identified a protein with significanthomology to J-binding protein. We have cloned thegene for this large putative J-binding protein 2 and aretesting its functions by gene disruption.The variant transferrin receptor of T. bruceiEach VSG gene expression site contains a set ofESAG 6 and 7 genes (see Figure V.4) specifying a heterodimerictransferein (Tf) receptor (Tf-r), and the receptorsencoded by different expression sites are similar but notidentical. These small differences have dramatic effectson the ability to bind Tfs from different hosts. Forinstance, the Tf-R encoded by the 221 expression sitedoes not detectably bind canine Tf, whereas the V02 siteTf-R does bind this Tf. Hence, we conclude that multipleVSG gene expression sites may primarily exist to allowthe trypanosome to use a diversity of mammalian hosts.The ability to make multiple Tf-Rs binding the same hostTf may also help the trypanosome to evade the effects ofaccumulating antibodies in a chronic infection. To testthis we have raised polyclonal antibodies against Tf-Rsencoded by different expression sites. We find that suchantibodies inhibit Tf uptake by the homologous Tf-Rmore than by a heterologous Tf-R. This suggests that the67MOLECULAR BIOLOGY
68MOLECULAR BIOLOGYability to make multiple Tf-Rs may not only serve as anadaption to a diverse range of mammalian hosts, butalso to allow antigenic variation of receptor duringchronic infection in a single host.Notes1 Funding: The Netherlands Cancer Institute.2 Funding: Netherlands Organization for ScientificResearch (NWO-Gebied Chemische Wetenschappen(CW 331-026; CW 97-046).3 Funding: Fellowship Human Frontier Science ProgramOrganization (HFSPO).4 Funding: Gulbenkian PhD Program in Biology andMedicine.5 Funding: Fellowship Boehringer Ingelheim.Publications: Antigenic variationBorst P, Chaves I. Mono-allelic expression of genes in simpleeukaryotes. (Letter to) Trends in Genetics 1999; 15: 95-6.Chaves I, Rudenko G, Dirks-Mulder A, Cross M, Borst P. Controlof variant surface glycoprotein gene expression sites inTrypanosoma brucei. EMBO J 1999; 18: 4846-55.Cross M, Kieft R, Sabatini R, Wilm M, De Kort M, Van der MarelGA, Van Boom JH, Van Leeuwen F, Borst P. The modified base Jis the target for a novel DNA-binding protein in kinetoplastid protozoans.EMBO J 1999; 18: 6573-81.McCulloch R, Barry D. A role for RAD51 and homologous recombinationin T. brucei antigenic variation. Genes & Dev 1999; 13:2875-88.Secretary Molecular BiologyC Smit (until September)I Deltrap (from August)Secretary Director of ResearchI Van Lieverloo (till October )B Van HoutenResearch staff positions (full time equivalents)Scientific permanent: 4.0Scientific project: 31.0Technical permanent: 4.5Technical project: 2.8
68MOLECULAR BIOLOGYability to make multiple Tf-Rs may not only serve as anadaption to a diverse range of mammalian hosts, butalso to allow antigenic variation of receptor duringchronic infection in a single host.Notes1 Funding: The Netherlands Cancer Institute.2 Funding: Netherlands Organization for ScientificResearch (NWO-Gebied Chemische Wetenschappen(CW 331-026; CW 97-046).3 Funding: Fellowship Human Frontier Science ProgramOrganization (HFSPO).4 Funding: Gulbenkian PhD Program in Biology andMedicine.5 Funding: Fellowship Boehringer Ingelheim.Publications: Antigenic variationBorst P, Chaves I. Mono-allelic expression of genes in simpleeukaryotes. (Letter to) Trends in Genetics 1999; 15: 95-6.Chaves I, Rudenko G, Dirks-Mulder A, Cross M, Borst P. Controlof variant surface glycoprotein gene expression sites inTrypanosoma brucei. EMBO J 1999; 18: 4846-55.Cross M, Kieft R, Sabatini R, Wilm M, De Kort M, Van der MarelGA, Van Boom JH, Van Leeuwen F, Borst P. The modified base Jis the target for a novel DNA-binding protein in kinetoplastid protozoans.EMBO J 1999; 18: 6573-81.McCulloch R, Barry D. A role for RAD51 and homologous recombinationin T. brucei antigenic variation. Genes & Dev 1999; 13:2875-88.Secretary Molecular BiologyC Smit (until September)I Deltrap (from August)Secretary Director of ResearchI Van Lieverloo (till October )B Van HoutenResearch staff positions (full time equivalents)Scientific permanent: 4.0Scientific project: 31.0Technical permanent: 4.5Technical project: 2.8
VI Division of Tumor Biology69Division head Jacques NeefjesIntroductionWithin the Division of Tumor Biology, we use cellbiology to understand intracellular transport processes,cell division, tumor progression and metastasis.Technologies to follow and manipulate these processesat virtually any level of resolution are operational in thedivision. These include molecular biological, biochemicaland various morphological techniques such as confocallaser microscopy and electron microscopy. Active collaborationsexist with various clinicians and scientists withinand outside the <strong>NKI</strong>/<strong>AvL</strong>.1999 had a sad start because of the death of Ab Tulp,a loss that is still felt in the division. A Van der Gugtenleft because of early retirement.Three new projects were started this year. One on theregulation of transport of MHC class II molecules, one onthe connection between the cytoskeleton andendo/phagosomes (both in the Neefjes group) and oneon the routing of antigen uptake and presentation by the4 different CD1 molecules that have recently beenidentified as antigen presenting molecules (Peters).Peters has now set up a lab for cryosectioning forimmunoelectronmicroscopy. State-of-the-art technology isbeing introduced for this purpose. This already allows theproduction of top quality electronmicrographs which isrecognized by many collaborating cell biologists. Realtime confocal microscopy combined with micromanipulationof cells is a technique now operational in the lab ofNeefjes. This allows the visualization of conformationalchanges and protein interactions in living cells. Forexample, Neefjes and collaborators have thus visualizedconformational alterations in an ABC transporter, thepeptide transporter TAP which is crucial for feeding MHCclass I molecules with antigenic peptides. This ‘single cellbiochemistry’ approach is further used to study vesiclecytoskeletoninteractions and the regulation of motorproteins that are essential in timing vesicle transport andDNA-segregation during mitosis (a process studied byMichalides). The combination of ‘single cell biochemistry’with electronmicroscopy will bring this type of research ina unique position.Antigen processing and presentationby MHC moleculesJ Neefjes PhDM Fernandez-Borja PhD 1A Neisig PhD 2SM Van Ham PhD 3JC Vos PhD 4RW Wubbolts PhD 5I Jordens MSc 3M Marsman MSc 6EAJ Reits MSc 3PJL Spee MSc 7MJTM Van Lith MSc 3S DusseljeeD VerwoerdGroup leaderPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentGraduate studentGraduate studentTechnicianTechnicianAntigen Presentation by MHC class I molecules and theaction of the ABC transporter TAPMHC class I molecules present antigenic fragments thatare mainly derived from degraded nuclear and cytosolicproteins. The fragments are subsequently translocated intothe ER lumen for binding to MHC class I molecules. TheABC transporter TAP pumps the peptides into the ER. Wehad previously determined the peptide substrate specificityof TAP from human, mice and rat. We have now started alarge series of biochemical experiments to determine thetopology, subunit interactions and relative orientation of thetwo subunits of TAP. TAP has a head-head topology andthree domains can be distinguished; a pore domainfollowed by a peptide-binding domain and, at the end, thetwo nucleotide-binding segments. ER-retention signals arefound in the first trans-membrane segments of both TAP1and 2 but other retention signals should be present aswell in the pore segment. To follow the conformationalchanges in TAP during translocation, cells were madeexpressing GFP-labelled TAP. FRAP (FluorescenceRecovery After Photobleaching) experiments on living cellswere performed to follow the activity of TAP (Figure VI.1).The lateral mobility of TAP was reduced by introduction ofpeptide and increased by inhibition of proteasomal activityas well as by ATP depletion. Experiments using the viralprotein US6 or peptides with long side chains suggest thatthe alterations in mobility are the result of pore opening.These alterations were subsequently used to monitor the
70TUMOR BIOLOGYFigure VI.1Confocal analysis of GFP-labelled TAP molecules expressed inthe endoplasmic reticulum of living cells. These cells were usedto measure the lateral mobility of TAP in the presence orabsence of peptides using bleaching protocol.peptide pool in living cells. We thus note a large increasein the intracellular peptide content upon an acute influenzainfection. This is the result of additional degradation by theproteasome of influenza-encoded proteins. More notably,we then showed that a large content of peptides isderived from (endogenous and viral) proteins degradedvery shortly after synthesis. The peptides that enter the ERcan subsequently bind to a large set of chaperones, oneof which is being used in vaccination trials. Using peptideswith a photoaffinity label, we have identified other chaperonesthat are also tested in vaccination studies.The current dogma is that MHC class I moleculespresent peptides that are captured in the ER. In contrastto this we observed that a fraction of MHC class Imolecules appears to enter endo/lysosomes and torecycle to the plasma membrane. Biochemical analysisshowed that these were class I complexes that were ableto exchange peptide at pH 5.0. Recycling class Imolecules can thus exchange peptides and present novelpeptides from endocytosed antigens.Antigen presentation by MHC class II molecules and theaction of HLA-DOUnlike MHC class I molecules, MHC class II moleculespresent peptides derived from endocytosed antigens.Class II molecules are transported to early lysosomalstructures termed MIIC where, with the help of adedicated chaperone HLA-DM, they are loaded withpeptide. HLA-DO binds to HLA-DM and is highlyexpressed in primary B cells. HLA-DO expression nowappears to act as a pH sensor restricting the activity ofHLA-DM to more acidic compartments and thus affectingthe peptide repertoire associated to MHC class IIFigure VI.2Cytoplasmic tail of DOB contains internalizaition signal CD8 andCD8 DOB transfected into Meljuso stably transfected withDOαβGFP.molecules. HLA-DO is recycling along with HLA-DMbetween MIIC and the plasma membrane and rapid internalizationfrom the plasma membrane is due to the tail ofDMB as well as DOB (Figure VI.2).We have previously shown that retention and transportof MIIC is controlled by the counteracting activity of themotor proteins kinesin and dynein. We have now isolateda novel protein that induces the recruitment of thedynein-dynactin complex to MIIC and causes retention.We are currently studying the molecular basis for this.In order to present antigen, vesicles are internalized tomeet the lysosome. These processes are criticallydependent on the actin and microtubule network. We arestudying the effect of a small GTPase called Rho B,which appears to inhibit an early step in endocytosis.Notes1 Funding: EEC, Project TMR ERB FMRXCT960069.2 Funding: The Alfred Benzon Foundation.3 Funding: NWO, Project 901-09-227.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-982.5 Funding: EEC, Project B104-97-0505.6 Funding: NWO, Pioneer Project 900-90-157.7 Funding: NWO, Project 901-09-228.Publications: Antigen processingBeekman NJ, Van Veelen PA, Van Hall T, Neisig A, Sijts A, CampsM, Kloetzel P-M, Neefjes JJ, Melief CJ, Ossendorp F. Abrogationof CTL epitope processing by single amino acid substitution flankingthe C-terminal proteasome cleavage site. J Immunol 1999 (inpress).
Fernandez-Borja M, Wubbolts R, Calafat J, Janssen H, DivechaN, Dusseljee S, Neefjes J. Multivesicular body morphogenesisrequires phosphatidylinositol 3-kinase activity. Curr Biol 1999; 9:55-8.Grommé M, Uytdehaag FG, Van Binnendijk RS, Kenter MJ, TulpA, Verwoerd D, Neefjes J. Endosomal Antigen Presentation byRecycling MHC Class I Molecules. PNAS 1999; 96: 103326-31.Ultrastructuralstudies on membranetraffic in cytotoxicT lymphocytes andtarget cells71TUMOR BIOLOGYHaurum JS, Bjerring Hoier I, Arsequell G, Neisig A, Stevanovic S,Valencia G, Zeuthen J, Neefjes J, Rammensee H-G, Elliott T.Presentation of cytosolic glycosylated peptides by Human Class IMajor Histocompatibility Complex Molecules in vivo. J Exp Med1999; 190: 145-50.Neefjes, J. CIIV, MIIC and other compartments for MHC class IIloading. Eur J Immunol 1999; 29: 1421-5.PJ Peters 1A Engering PhD 2N Van der Wel PhD 3E Tjin MSc 4E BosY De Jong 3D Fluitsma 5E Van DonselaarGroup leaderPost-docPost-docGraduate studentTechnicianTechnicianTechnicianTechnicianNeefjes J. Determining Protein Transport to the PlasmaMembrane. Curr Prot Cell Biol 1999 (in press).Spee P, Subjeck J, Neefjes J. Identification of novel peptide bindingproteins in the endoplasmic reticulum: Erp72, calnexin andGRp170. Biochem J 1999; 38: 19558-66.Tulp A, Verwoerd D, Neefjes J. Electromigration for separations ofprotein complexes. J Chromatogr B 1999; 722: 141-51.Tulp A, Verwoerd D, Neefjes J. Lectin induced retardation of subcellularorganelles during preparative density gradient electrophoresis:selective purification of plasma membranes. Electrophoresis1999; 20: 438-44.Vos JC, Reits EAJ, Wojcik-Jacobs E, J Neefjes. Subunit interactionsvisualized by ER-mobility and post-translational translocationdefine a head-head/tail-tail topology for the pore of the ABCtransporter TAP. Current Biol. 1999 (in press).Vos JC, Spee PJL, Momburg F, Neefjes J. The topology anddimerization of the two subunits of the Transporter associatedwith Antigen Processing reveal a three domain structure. JImmunol 1999; 163: 6679-85.Wubbolts R, Fernandez-Borja M, Jordens I, Reits E, Dusseljee S,Echeverri C, Vallee RB, Neefjes J. Opposing motor activities ofdynein and kinesin determine retention and transport of MHCclass II-containing compartments. J Cell Sci 1999; 112: 785-95.ThesesGrommé M. Aspects of conventional and alternative MHC Class Iantigen processing and presentation, Leiden: State University,1999.Wubbolts R. Dynamics in the intracellular transport of MajorHistocompatibility Complex class II molecules, Leiden: StateUniversity, 1999.Cytotoxic T Lymphocytes (CTLs) are essential componentsof our immunological defense against tumor cellsand virus infected cells. CTLs rapidly kill target cells via atleast two distinct effector pathways: 1) the secretorypathway involving the polarized exocytosis of cytolyticgranules; 2) the Fas pathway in which the Fas ligand onthe CTL interacts with the Fas receptor on the target cell.Both these processes appear to work in concert andinduce apoptotic changes in the target cell nuclei thatculminates in the destruction of the target cell.Conceivably, regulated exocytosis will be pivotal to thecytolytic function of CTLs, however, the molecularmachinery involved in this process is poorly characterized.We have previously shown, by use of the highresolutiontechnique of cryo-immunogold electron microscopy,that CTL granules are secretory lysosomes thatcontain the lytic molecules perforin and granzymes andthat their formation is coupled to the endocytic pathway.Mechanism of CTL degranulation 2It is now well documented that members of the Rassuperfamily of GTPases (Ras, ARF, Rho, Rab, Ran)control a wide range of biological processes includingmembrane trafficking and cytoskeletal remodeling. Weare investigating the role of the GTPases of the ARF andRho subfamilies in CTLs, since they are likely candidatesto regulate various stages of the granule exocytosispathway. Specifically, we are in collaboration with CD’Souza Schorey, University of Notre Dame, IN, USA, VHsu, Harvard Medical School, Boston, USA and H Spits(Division IV) investigating the role of ARF6 in CTL-TCadhesion and ARF6, Rac and Rho in granule exocytosis.SCAMP (secretory carrier membrane protein)compartment in CTL 4,5In other systems such as the nerve termini of neurons,rapid advances have been made in understanding theprocess of synaptic vesicle exocytosis, vesicle-membranefusion and in the identification of key components of themembrane fusion process. Preliminary investigations in
72TUMOR BIOLOGYFigure VI.3The prion disease is manifested when the prion protein,designated PrP, is converted from a benign cellular form to adisease causing form by a change in conformation. Thus, it hasbecome increasingly important to establish the site(s) ofconversion of PrP c (cellular prion protein) into PrP Sc (scrapieprion protein) and the subsequent site of accumulation. A betterunderstanding of the subcellular trafficking routes of PrP c is aprerequisite for establishing the precise location where theconformational changes of PrP Sc takes place. To this end, wehave analyzed the intracellular localization of PrP c in a ChineseHamster ovary cell line that stably expresses PrP c , by using thetechnique of cryoimmunogold electron microscopy. This figureshows that PrP c (small dots) is enriched in caveolae labeled forcaveolin (large dots). (A collaborative study with Stanley Prusiner,University of California, San Francisco, Medical School, SanFrancisco CA.)collaboration with D Castle, University of Virginia HealthSciences Center, Charlottesville, USA and with J Neefjes,have suggested that a comparable mechanism ofmembrane exocytosis may exist in CTLs. PCR cloningand Western Blot analysis using antibodies directedagainst Rab3, VAMP2, syntaxin 4, SCAMP (secretorycarrier membrane protein) and SNAP-23 have indicatedthat these proteins or their T-cell homologs are present inactivated CTLs. We have therefore begun to unravel themolecular components of the exocytic process in CTLs.An exciting finding is the observation that SCAMP redistributesfrom a non-granule membrane to the plasmamembrane on encountering a target cell. We will investigatethe role of SCAMP in CTL granule exocytosis andtarget cell lysis.The CD1 family of lipid antigen-presenting molecules inTarget Cells 3Four CD1 isoforms (CD1a,b,c and d) have beenidentified in humans as type 1 integral membraneproteins structurally related to MHC class I molecules.Functional studies revealed that CD1b presentedmycobacterial antigens, either added exogenously orderived from endosome-resident live bacteria.Mycobacterial antigens presented in this way are knownto enter the endocytic (phagocytic) pathways, previouslyappreciated to result in binding to MHC class IImolecules. In collaboration with M Sugita, S Porcelli andM Brenner, Harvard Medical School, Boston, MA, USAwe have demonstrated that CD1b was internalized fromthe cell surface via clathrin-coated pits/vesicles andtransported to endosomes, eventually reaching lateendosomal/lysosomal compartments where sampling ofmycobacterial-derived lipid antigens occurred. Theendosomal localization of CD1b, which is essential for itsantigen presenting function, is directed by its shortcytoplasmic domain containing a YXXZ sequence (Y,tyrosine; X, any amino acid; Z, a hydrophobic aminoacid), as demonstrated by our studies showing thatdeletion of this cytoplasmic tail alters endosomal localization.This motif is found in other proteins localized toendosomes and is known to interact with adaptor protein(AP) complexes of clathrin-coated vesicles. WhereasCD1c and CD1d contain a similar motif and distribute toendosomes, CD1a is the only molecule of the humanCD1 family that lacks this tyrosine-based endosomaltargeting motif. Thus, CD1a is likely to follow an intracellularpathway distinct from that by the other CD1isoforms. We hypothesize that the intracellular pathwaysfollowed by CD1a and CD1b are different. Such differencesare likely to be of critical functional importancesince they determine the compartments in which antigenloading can occur. By comparison, the differentialintracellular trafficking patterns of MHC class I and classII molecules are central in determining their ability to bindendogenous or exogenous antigens, respectively. Thesedifferences also correlate with distinct effector functionsof T cells activated by MHC class I (CD8+, cytotoxic) andclass II (CD4+, Th1 and Th2). We are now trying toelucidate the pathway for antigen presentation mediatedby the different CD1 molecules.Teaching at the Medical School, Free UniversityThis year PJ Peters started teaching at the MedicalSchool of the Free University in Amsterdam. In additionto lecturing the Cell Biology class the task as semesterchair for first year students is to co-ordinate the semesterprogram ‘From Molecule to Cell’.Notes1 PJ Peters has a joint appointment (20%) at theMedical School of the Free University Amsterdam.2 Funding: Dutch Cancer Society, Project: UU 95-1098.3 Funding: Netherlands Leprosy Relief.4 Funding: NWO, Project: 901-09-261.5 Free University, Medical School, Amsterdam.
Publications: Ultrastructural studiesAoe T, Lee AJ, Van Donselaar E, Peters PJ, Hsu VW. Modulationof intracellular transport by transported proteins: insight fromregulation of COPI-mediated transport. Proc Natl Acad Sci U S A1998; 95: 1624-9.Cell cycle controlgenes and tumorprogression73TUMOR BIOLOGYD’Souza-Schorey C, Van Donselaar E, Hsu VW, Yang C, Stahl PD,Peters PJ. ARF6 targets recycling vesicles to the plasma membrane:insights from an ultrastructural investigation. J Cell Biol1998; 140: 603-16.Franco M, Peters PJ, Boretto J, Van Donselaar E, Neri A,D’Souza-Schorey C and Chavrier P. EFA6, a sec7 domaincontainingexchange factor for ARF6, coordinates membranerecycling and actin cytoskeleton organization. EMBO J 1999; 18:1480-91.Hochstenbach F, Klis FM, Van den Ende H, Van Donselaar E,Peters PJ, Klausner RD. Identification of a putative alpha-glucansynthase essential for cell wall construction and morphogenesis infission yeast. Proc Natl Acad Sci U S A 1998; 95: 9161-6.Hsu VW, Peters PJ. Current views in intracellular transport: insightsfrom studies in immunology. Adv Immunol 1998; 70: 369-415.Hunziker W, Peters PJ. Rab17 localizes to recycling endosomesand regulates receptor-mediated transcytosis in epithelial cells. JBiol Chem 1998; 273: 15734-41.Jackman RM, Stenger S, Lee A, Moody DB, Rogers RA, Niazi KR,Sugita M, Modlin RL, Peters PJ, Porcelli SA. The tyrosine-containingcytoplasmic tail of CD1b is essential for its efficient presentationof bacterial lipid antigens. Immunity 1998; 8: 341-51.Korinek V, Barker N, Moerer P, Van Donselaar E, Huls G, Peters PJ,Clevers H, Depletion of epithelial stem-cell compartments in thesmall intestine of mice lacking Tcf-4. Nat Genet 1998; 19: 379-83.Peters PJ. Cryo-Immunogold Electron Microscopy. In: BonifacinoJS, Dasso M, Harford JB, Lippincott-Schwartz J and YamadaKM, editors. Current Protocols in Cell Biology. New York, JohnWiley & Sons, 1999: 4.7.1-12.Spada FM, Grant EP, Peters PJ, Sugita M, Melián A, Leslie DS,Van Donselaar E, Lee HK, Hanson DA, Krensky AM, Majdic O,Porcelli SO, Morita CT, Brenner MB. Self Recognition of CD1 bygamma delta T cells: Implications for Innate Immunity. J of ExpMed 1999 (in press).Sugita M, Grant EP, Van Donselaar E, Hsu VW, Rogers RA, PetersPJ, Brenner MB. Separate pathways for antigen presentation byCD1 molecules. Immunity 1999 (in press).Sugita M, Moody DB, Jackman RM, Grant EP, Rosat JP, BeharSM, Peters PJ, Porcelli SA, Brenner MB. CD1—a new paradigmfor antigen presentation and T cell activation. Clin ImmunolImmunopathol 1998; 87: 8-14.R Michalides PhDGroup leaderA BalkenendeTechnicianT Verschoor 1 Technician 1W SilvisUndergraduate studentTumor progressionThe proliferative effect of overexpression of cyclin D1 indifferentiated cells of squamous cell carcinomas iscounterbalanced by the induction of cyclin kinaseinhibitor p21. In squamous cell carcinomas, proliferationmarker Ki-67 was present in the basal layer of the tumorand absent in the more differentiated layers where cyclinD1 was co-expressed with p21 (a collaborative studywith P Van Diest, Free University Amsterdam). Inducedoverexpression of cyclin D1 resulted in upregulation ofp21 in MCF7 breast cancer cells. The balance betweencyclin D1 expression and p21 may therefore, beassociated with the differentiation status of tumor cells.In a collaborative study with M Barbareschi (Trento,Italy) we found that the prognostic value of cyclin kinaseinhibitor p27 as described in the literature, is stronglyinfluenced by a selective partitioning of breast cancercases. p27 should therefore be used with caution as amarker for prognosis.Indicators for therapyDisturbed regulation of the G1 phase of the cell cyclein the Rb/cyclin D1/p16/cdk4 pathway alters chemo- andradiosensitivity of tumor cells (Figure VI.4). In MCF7 cells(wild type for Rb, cyclin D1, p53, p19ARF, but with amutated p16), we observed that induced overexpressionof cyclin D1 increased sensitivity to γ-radiation by anenhanced transit through G2/M before a subsequententry into apoptosis. Sensitivity towards paclitaxel inMCF7 cells is also enhanced by cyclin D1.Cyclin D1 also affected sensitivity of MCF7 cellstowards simvastatin, a farnesyltransferase-inhibitorpreventing activation of Ras and Rho (a collaborativestudy with A Weisz, Napoli, Italy). Overexpression ofcyclin D1 resulted in a transient release of the simvastatininduced cell cycle block. This was also observed whenMCF7 cells were treated with anti-estrogens ICI 182.780or tamoxifen.These findings indicate that overexpression of cyclinD1 affects the therapeutic window of treatment with antiestrogens,farnesyltransferase-inhibitors, γ-radiation andpaclitaxel, which may well be of clinical relevance.
74TUMOR BIOLOGYSchuuring E, Van Damme H, Schuuring-Scholtes E, Verhoeven E,Michalides R, Geelen E, De Boer C, Brok H, Van Buuren V, KluinPh. Characterization of the EMS1 gene and its product, humancortactin. Cell Adhesion and Communication 1998; 6: 185-209.Genes involved inbreast cancermetastasisFigure VI.4Effects of overexpression of cyclin D1 on some therapeuticmodalities.Adhesion-dependent proliferationAdhesion of cells onto extracellular matrix componentsactivates the Rho-like GTPases Rac and CDC42.Constitutive activation of the Rho-like GTPases in porcineaortic endothelial PAE cells resulted in ‘mitotic slippage’,where nuclear replication becomes dissociated fromcytokinesis. This results in polyploid, multinucleated cells,which ultimately succumb to apoptosis. The mechanismbehind the prevention of cytokinesis by constitutive activeRac or CDC42 is under study.Note1 Funding: Dutch Cancer Society, Project 97-1431.Publications: Cell cycle controlBarbareshi M, Peterse H, Mauri FA, Veronese S, Van Tinteren H,Maisonneuve P, Scaioli M, Caffo O, Galligioni E, Doglioni C, DallaPalma P, Michalides R. P27 KIP-1 expression in breast carcinomas:an immunohistochemical study on 512 patients with longfollow-up. Int J Cancer 1999 (in press).Coco-Martin J, Verschoor T, Lallemand F, Michalides R.Overexpression of cyclin D1 increases sensitivity to g-irradiation inMCF7 cells. Cancer Research 1999; 59: 1134-40.De Jong JS, Van Diest P, Michalides R, Baak J. Concerted overexpressionof p21 and cyclin D1 is associated with growth inhibitionand differentiation in various carcinomas. J Clin Pathology:Mol Pathol 1999; 52: 78-83.Germano D, Pacillio C, Cancemi M, Cicatiello L, Altucci L, BelsitoV, Salzano S, Michalides R, Taya Y, Bresciani F, Weisz A. Cyclin D1overexpression does not interfere with inhibition of human breastcancer growth by blockade of the mevalonate-protein prenylationpathway. Br J Cancer 1999 (in press).Michalides R. Cell cycle regulators: mechanisms and their role inetiology, prognosis and treatment of cancer. J Clinical Pathology(review) 1999; 52: 555-68.Michalides R. Prognosis for cell cycle regulators: useful to predictcourse of disease and for assessment of therapy in cancer. J Path1999; 188: 341-3.J Hilkens PhDI Gaemers PhD 1T Thingstad MSc 2M Van der Velden MScM BoerH Volders 1J HendriksenP SchneiderGroup leaderPost-docGraduate studentGraduate studentTechnicianTechnicianUndergraduate studentUndergraduate studentOverexpression of membrane-associated mucins in breastcancerEpisialin (also designated EMA, CA 15-3 antigen)encoded by the MUC1 gene, and epiglycanin belong tothe class of membrane-associated mucins which arecharacterized by a heavily O-glycosylated mucin domain.Both are frequently highly overexpressed on carcinomacells compared with normal epithelial cells. Biochemicaland electronmicroscopy studies revealed that the mucindomains of both molecules project more than 200 nmabove the plasma membrane. When these elongated andrelatively rigid molecules are overexpressed they maskother much shorter cell surface molecules, thus impedingcell-cell and cell-matrix interactions and contributing tothe invasive and metastatic potential of tumor cells.Epiglycanin has thus far only been identified in mousemammary tumor cells. An antiserum against the nonglycosylatedprecursor of mouse epiglycanin crossreactedwith human epiglycanin precursor, showing thatepiglycanin is also present in carcinoma cell lines. Theexpression of epiglycanin in carcinoma cells appears tobe sensitive to a component present in mouse andhuman cancer ascites fluids. The normal function and themechanism of overexpression of both membraneassociatedmucins are presently being studied.Episialin overexpression and metastasisWe have previously shown that the formation ofexperimental metastases in the lung is strongly affectedby overexpression of episialin. The effect of episialinoverexpression on tumor progression has been furtherinvestigated in episialin transgenic FVB mice. N-ethyl-Nnitroso-urea(ENU) induced lung tumors in these miceexpress high levels of episialin. Histological examination
of the lungs of the ENU treated mice revealed more andlarger tumors in the transgenic mice than in the FVBcontrol animals, indicating that episialin indeed affects theprogression of lung tumors in this animal model.Regulation of episialin gene expressionExamination of the episialin promoter revealed severalputative regulatory elements, including a STAT-responsiveelement (STAT: Signal Transducer and Activator ofTranscription) and several glucocorticoid binding sites.Luciferase reporter gene assays and electrophoreticmobility shift assays (EMSA) revealed that STAT1, STAT3and STAT5 are binding to the STAT element. Interestingly,in some breast carcinoma cell lines STAT3 is constitutivelyactivated, which may contribute to the overexpressionof episialin in these carcinomas.Hydrocortisone also stimulated the episialin promoter.Mutation analysis of two putative glucocorticoid bindingelements (GRE) just upstream of the STAT bindingelement revealed that both sites are involved in hydrocortisonemediated regulation of the episialin promoter.Addition of hydrocortisone and IL-6 together synergisticallystimulated episialin expression. We have elucidatedthe mechanism responsible for this synergism: supershiftEMSA and co-immunoprecipitation using antibodiesagainst the glucocorticoid receptor (GR) revealed a directinteraction between STAT3 and the GR. Moreover,mutations in the STAT binding element abolished thesynergism and negatively affected the stimulation byhydrocortisone and visa versa, suggesting that DNAbinding of both transcription factors stabilized the interactions.Identification of novel genes involved in mammary tumormetastasisWe have developed a model system that can be usedto identify novel metastasis genes in a BALB/c substrainthat acquired mouse mammary tumor virus (MMTV) byfoster-nursing (denoted BALB/c+ strain). Subcutaneous(s.c.) transplantation of lungs from tumor bearing animalsprovided a source of metastatic mammary tumor cells forgenetic analysis which was not previously available. Aseries of independent sets of primary tumors and s.c.lung metastases has been collected and analyzed forMMTV proviral integrations. In about 1/3 of the subcutaneouslyexpanded metastatic tumors extra MMTV copieswere present that were not present in the primary tumor.These MMTV copies might be involved in activatingmetastasis genes by promoter or enhancer insertion. Wehave adapted the splinkerette PCR to specifically amplifythe MMTV flanking sequences. Several of these flanksare currently being analyzed to detect metastasis relatedcommon integration sites.Publication: Genes in breast cancermetastasisHilkens J, Bonfrer H Diagnosis and monitoring of bone metastasesusing serum tumor markers. In: Body JJ editor. Tumor BoneDisease and Osteoporosis in Cancer Patients, Pathophysiology,Diagnosis and Therapy. New York, Marcel Dekker, 1999: 197-207.Secretary Tumor BiologyMK Van der VeldeResearch staff positionsScientific permanent: 4.1Scientific project: 16.0Technical permanent: 6.0Technical project: 3.075TUMOR BIOLOGYNotes1 Funding: NIH grant 1R01-CA79580-01.2 Funding: Biotag.
76VII Division of MolecularGeneticsDivision head Anton BernsIntroductionThe Division of Molecular genetics currently comprisesfour research groups, headed by D Barlow, RBeijersbergen, A Berns and P Demant, respectively. Inaddition, our animal pathologist, M Van der Valk, isformally part of the division.Focus of the group of Barlow is on the mechanisms ofimprinting using the Igf2 receptor gene locus as aparadigm. In addition, her group concentrates on theidentification of genes involved in invasive growthproperties of placental tissues and their possible role intumorigenesis. R Beijersbergen joined the division in1999 as an <strong>AvL</strong> fellow after having spent a post-doctoralperiod in the lab of R Weinberg at MIT, Boston, USA. Hisfocus is on the regulation of telomerase activation duringimmortalization and tumorigenic transformation of humancells. In the group of P Demant the main emphasis is onthe identification of Tumor Susceptibility Genes forintestinal and lung tumors. To this end, the group hasdeveloped the Recombinant Congenic Strains in which12.5% of the genome of a susceptible donor strain isintroduced onto a resistant background strain. The groupis closing in on one of the susceptibility genes that wasfirst identified (Scc1). Within this group M Snoek focuseson the identification of genes within the MHC thatpredispose to lung cancer. The group of A Bernsconcentrates on the generation and study of conditionaltumor suppressor (TS) gene knockout mice with the aimto identify the contribution of distinct genetic lesions tospecific tumor characteristics. Finally, there is an ongoingeffort to improve current mouse model systems. Activitiesin this area include exploring strategies to mark cells afterCre/Lox switching, generation of better inducible Cre/Flptransgenes, the use of somatic gene transfer to achieveswitching, development of reliable cell markers, and thegeneration of better insertional mutagens to disrupt andmark genes of interest.In the coming years emphasis in the division will be onthe identification of new genes directly involved in orpredisposed to tumorigenesis, unraveling of theregulation of telomerase, and on the development of anew generation of mouse models for human cancer.Molecular geneticsA Berns PhDP Krimpenfort PhD*M Van der Valk MSc**J Jonkers PhD 1S Lyons PhD 4S Marino PhD 2P Merel PhD 4R Meuwissen PhD 1K Quon PhD 3M Vooijs PhD 5A Loonstra MSc 1C Martins MSc 6H Mikkers MSc 8R Van Amerongen MSc 7D Hoogervorst 5F Matthesius8H Van der GuldenJ Vink 1F BleekerP KnipscheerF MicelliGroup leaderAcademic staffAcademic staffPost-docPost-docPost-docPost-docPost-docPost-docPost-docGraduate studentGraduate studentGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentUndergraduate studentWe have embarked on developing better mousemodels for cancer using techniques that permit theconditional activation of oncogenes and inactivation oftumor suppressor genes in a tissue-specific fashion. Fourdifferent sets of mice have been generated with: 1)Conditional tumor suppressor gene alleles through theintroduction of LoxP sites in the locus by gene targetingtechniques (Rb, p53, Brca1, Brca2, Dcc, Nf2, Apc, Pten,E-cadherin, Ink4a, Atr, VHL). 2) Conditional and inducible(Tet-on/Tet-off) oncogenes permitting regulatableoncogene activation in a tissue-specific fashion. 3) Cretransgenic lines, some with hormone inducible Cre, eitherproduced by conventional transgenesis or knockinstrategies (POMC-Cre. K14-Cre, Actin-Cre, GFAP-Cre,IRBP-Cre, P0-Cre, Rosa26-Cre-MER, WAP-Cre). 4)Reporter lines permitting the monitoring of Cre activity bya LacZ reporter gene. These systems are used toproduce compound mutant strains in which multiplealleles can be switched in a tissue-specific fashion. Thiswill allow us to somatically induce, at will, a complex setof oncogenic mutations. In this way we expect to
eproduce more faithfully the mutations found in tumorsin man. We can then study the correlation betweentumor genotype and phenotype in a highly controlledexperimental setting. These systems will be used tostudy tumor progression events, to test the effects oftherapeutic intervention protocols, and to serve as asource of cells to study the effects of these mutations oncell cycle and differentiation in vitro. Many of theseanalyses are ongoing, utilizing various combinations ofmutant alleles.Conditional tumor suppressor gene knockout miceRetinoblastomaA number of years ago, in collaboration with M Hooperin Edinburgh, we embarked on the targeted disruption ofthe retinoblastoma gene. Rb deficiency resulted in earlyembryonic lethality. Surprisingly, chimeric mice generatedfrom injection of Rb -/- ES cells into blastocysts wererelatively normal with significant contribution of Rb -/- cellsto most tissues and no propensity to develop retinoblastoma.However, we did observe extensive apoptosis inthe retinal layer explaining the low contribution of theRb -/- ES cells to the adult retina. In collaboration with TeRiele (Division II), a series of compound chimeric micewas generated carrying various combinations of mutantalleles for Rb, p107. Loss of Rb and p107, but not p53was required for retinoblastoma formation in the mouse.Tumors originated from the inner nuclear layer rather thanthe outer nuclear layer and exhibited markers of amacrinecells.Subsequently, we have generated conditional Rbmutants to better explore the role of Rb loss in tumors inmice. The Rb gene was fitted with either frt or loxP sitesflanking exon 19. Crossing of Rbfrt/frt mice with POMC-Flp transgenic mice, which express the Flp recombinasein the intermediate lobe of the pituitary gland, resulted ininactivation of the Rb gene specifically in these cellsleading to pituitary tumors at high incidence. Next, wegenerated compound mutant mice with the floxed Rballeles on a p107 and/or p53 null background. A photoreceptorcell-specific Cre transgene was crossed intothese mice. No retinoblastomas developed indicating thatinactivation of Rb, p107 and p53 in photoreceptor cells isnot sufficient to give rise to retinal tumors in mice.However, pineal gland tumors, tumors of the anterior lobeof the pituitary, and choroid plexus tumors werefrequently found. Interestingly, some of these tumor pronetissues arise from the same neuroblastic precursor as thephotoreceptors suggesting that this lineage is not indifferentto Rb loss. p53 loss was found to contribute onlyto a subset of these tumors (e.g. to anterior lobe tumorsbut not to intermediate lobe tumors). Epithelial switchingof Rb in the presence or absence of a functional p107allele resulted in hyperplasia of the skin. Basal layer cellsshowed increased proliferation and retained proliferativecapacity during differentiation into the more differentiatedcell types of the skin. Absence of p107 aggravated thisphenotype considerably, leading to early death of theK14-Cre;Rbflox/flox;P107 -/- mice. Currently, the effects ofadditional mutations on a Rb conditional background areassessed in vivo and in vitro using cultured keratinocytesof these mice.Schwann cell tumorsWe have generated conditional Nf2 knockout mice incollaboration with the group of G Thomas, Institut Curie,in Paris. In view of the involvement of Nf2 in the inductionof schwannomas, we have produced P0 transgenic micethat express the Cre recombinase in Schwann cells.P0Cre;Nf2flox/flox mice develop schwannomas after along latency period. Tumorigenesis is greatly acceleratedby the introduction of a mutant p53 allele. p53 and Nf2are on the same chromosome. When a single conditionalNf2 allele is combined with a single p53 allele no tumorsare found when both mutant alleles are in trans, while alow incidence of tumors do form when they are in cis.The much earlier tumor onset in Nf2flox/flox;p53 +/- micesuggests that Cre-mediated loss of Nf2 is critical for thedevelopment of schwannomas and accelerates loss ofthe wt p53 allele.MesotheliomasScreening of human mesotheliomas for tumorsuppressor gene mutations has shown the relativelyfrequent mutation/deletion of NF2 and INK4a. SinceINK4a acts in the RB pathway, we have generatedcompound Nf2flox/flox;Rb/flox/flox mice and inactivatedthe Nf2 and Rb alleles in the mesothelial lining of thethoracic and peritoneal cavity by a single injection withAdenoCre virus. Tumors with the characteristics ofmesotheliomas arose after a latency of 8-12 months.Most of the tumors showed a spindle cell morphologyand the tumors are currently further characterized using apanel of antibodies. We will test a series of additionalcombinations of conditional tumor suppressor genes inorder to determine how the different lesions affect thephenotypic characteristics of the tumors. Furthermore,we will derive cell lines from the mesothelial lining of thevarious mutant strains and study their growth and differentiationin vitro, with and without switching. In addition,we will accelerate tumorigenesis by carcinogen treatment(both ENU and asbestos fibers) and search for chromosomalabnormalities using RDA and LOH analyses.Epithelial tumorsEmphasis is on the role of Rb, p107, Brca1, Brca2,p53, Ras, and E-cadherin in tumorigenesis in skin andmammary epithelium. Conditional alleles of Brca2 werecombined with a conditional allele of p53 yieldingBrca2flox/flox;P53flox/flox mice. In this background aK14-Cre transgene was introduced. The double conditionalscarrying the K14-Cre transgene developed skinabnormalities in a subset of the mice. The penetrance ofthis phenotype appears to correlate with the level ofswitching of Brca2 and p53. None of the mice of the77MOLECULAR GENETICS
78MOLECULAR GENETICSBrain tumorsWe have generated a mouse model for medulloblastomaby the Cre-mediated inactivation of both p53 andRb in the cerebellar external granular layer (EGL). Usingthe promoter of the gene encoding glial fibrillary acidicprotein (GFAP), Cre expression was directed to astrocytesand immature precursor cells of the EGL in thedeveloping cerebellum. GFAP-Cre;Rbflox/flox;P53flox/floxmice developed aggressive embryonal tumors with typicalfeatures of the medulloblastoma, a malignant humanchildhood tumor. Neoplastic lesions were identified at theage of seven weeks on the outer surface of themolecular layer, corresponding to the location of the EGLduring development. Interestingly, complete P53deficiency was required for the development of thistumor. In GFAP-Cre;Rbflox/flox;p53 +/- animals thesetumors were not found, whereas in GFAP-Cre;Rbflox/+;P53 -/- mice the tumors developed after aprolonged latency period with the concomitant loss of thewt Rb allele.Figure VII.14’-OHT regulated Cre recombination in vivo.I.p. administration of 4’OHT Tamoxifen to Rosa-Rep/Rosa-CreMer double transgenic mice results in Cre-mediated recombinationin vivo. Whole mount beta-galactosidase staining ofperitoneum of a single rosa-rep (A) and double rosa-rep/rosacremerwithout tamoxifen (B) and rosa-rep/rosacremer withtamoxifen (C & D).Rosa-rep and Rosa-CreMer mice weregenerated through a knockin of floxed lacZ reporter construct inthe rosa-26 locus (Rosa-reporter, P. Soriano) and a knockin of aCre gene fused to the mutated estrogen receptor (Mer) bindingdomain (CreMer) into the rosa-26 locus (Marc Vooijs)K14-Cre;Brca2flox/flox or K14-Cre;p53flox/flox genotypedeveloped this condition (Figure VII.1). Subsequently,papillomas and mammary tumors developed in thecompound mutants. These are currently being analyzedin more detail. Similar compound conditionals are beingproduced with conditional alleles of Brca1 and p53. AsBrca1 and Brca2 are implicated in DNA repair, the effectsof DNA damage inflicted by carcinogens and radiationwill be tested in these mice. When the K14-Cretransgene was combined with conditional Rb alleleswidespread hyperplasia of the skin was observed. Thisphenotype was further aggravated in a p107 deficientbackground. Proliferating cells, expressing both basal andsuprabasal markers were found in the suprabasal layersuggesting that Rb plays a role in cell cycle exit ratherthan in differentiation. This system will be used to furtherdefine the role of Rb and p107 in differentiation andproliferation of basal cells. We are defining conditions toswitch conditional alleles in a number of cells types invitro. Special attention has been given to mitigate theinhibitory effects that Cre expression appears to exert oncell growth.Identification of tumor suppressor genesWe have obtained a highly metastatic human cell lineC8161 (Welsch et al. Oncogene 1994; 9: 255-62) whosemetastatic capacity is suppressed by introduction of asingle copy of a Neo-tagged human chromosome 6. Wehave shown that the spontaneous reversion of this cellline to the highly metastatic phenotype is sufficiently lowto permit inactivation and subsequent identification of theresponsible tumor suppressor gene by insertionalmutagenesis with a replication-defective gene trap vector.We are currently in the stage of identifying the integrationsites of proviruses in cells that regained enhanced growthproperties upon transplantation into syngeneic hosts.Identification and characterization of collaboratingoncogenesTransgenic mice expressing (putative) oncogenes canprovide insight into the oncogenic potential of genes,disclose their tissue-specific activity and reveal their rolesin transformation. Genetic crosses between transgenicmice carrying different oncogenes allow assessment oftheir cooperative activity and, when used in combinationwith proviral tagging, permit identification of genes whosegain- or loss-of-function synergizes with the transgene(s).Furthermore, by transplanting primary tumors induced inthis fashion, genes contributing to tumor progression canbe identified. Finally, by applying proviral tagging incompound mutant mice, we can mark genes acting inspecific signal transduction pathways. Emphasis in thisprogram is on the identification of oncogenes, on theunraveling of the biochemical function of the encodedproteins, their physiological role, and their contribution tothe tumorigenic process. We have set up a highthroughput screen for proviral insertion sites with the aimof achieving saturation tagging of genes contributing totumorigenesis. In the coming years we expect toaccumulate flanking sequences of thousands of insertionsites which will give access to the genes deregulated bythese insertions. In this way we expect to identify thesignaling networks critical for transformation of lymphoidcells in mice. This will facilitate the search for alterationsin the corresponding pathways/genes in tumors in man.
Pim oncogenesMyc and Pim oncogenes strongly collaborate intumorigenesis. However, it remains unclear what themechanism is underlying this synergy. In search of thefunctions of PIM proteins, we have generated Pimdeficient mice (Pim1, Pim2, and Pim3). Single Pim1 orPim2 knockout mice show a rather subtle phenotype.The same holds for the Pim1;Pim2 double KO mice. Theother pairs of double mutants and the triple compoundmutant mice are currently being generated. There is goodevidence that Pim1 and Pim2 act downstream of anumber of interleukin receptors as these induce Pim1and Pim2 transcription upon ligand binding, probablythrough the jak/stat pathway. Overexpression of Pim canpartly counteract defective receptor signaling.Introduction of a Pim1 transgene into IL2Rgammaknockout mice, which have a very small thymus due todefective interleukin signaling, restores thymic cellularity.Interestingly, overexpression of Pim1 also leads to theformation of a CD4+8+ double positive compartment ofnormal size in a RAG1-deficient background whereasPim1 is unable to rescue the strongly reduced cellularityof thymi in CD3gamma knockout mice, suggesting thatPIM proteins might act as ‘gain setters’ of signalingcascades.To uncover components in the PIM signal transductionpathway we have set up a genetic screen. Takingadvantage of the strong collaboration between PIM andMYC we generated mice carrying the Eµ-myc transgeneor a Pim1/Pim2-deficient background. In these micelymphomas were induced by retroviral insertional mutagenesis.The concept explored here is that we expect topreferentially activate genes that can substitute for thefunction of PIM. Genes that have been found includePim3, c-kit, tpl2, and cyclinD2. None of these geneswere found to be provirally activated in a Pim1/2 proficientbackground. We are currently assessing whetherPim proteins can suppress the phenotypic abnormalitiesseen in c-kit mutant mice.To determine the potential role of the human PIMgenes in tumorigenesis we have analyzed a series oflymphoid tumors for aberrant expression of PIM genes. Ina substantial fraction of these tumors, particularly largecell B lymphomas, high levels of either PIM1, PIM2 orboth were found. However, so far we have no evidencefor chromosomal alterations linked to one of the PIMgenes.Frat1Frat1 has been cloned as a tumor progression geneusing retroviral tagging. Frat1 is a small intronless gene.The encoded protein does not exhibit obvious sequencemotifs that suggest a function or points to specific interactions.Transgenic mice overexpressing Frat1 are nottumor prone but show an accelerated tumorigenesis ratewhen infected with MuLV or when crossed with Pim1transgenic mice. This is in accordance with the contributionof Frat1 to later steps in tumorigenesis as wasFigure VII.2Frat funtion in the ß-catenin signaling pathwayfurther substantiated by retroviral transduction of Frat1into cell lines derived from primary tumors arising spontaneouslyin Pim1 transgenic mice. Tumor cells expressingFrat1 expanded preferentially upon subcutaneous inoculation.Interestingly, at older age Frat1 transgenic miceexhibit epithelial hyperplasia in their mammary glands.This is in agreement with the recent finding by the groupof Kimelman et al. Cell 1998; 93: 1031-41 that FRATbinds to GSK3beta and thereby modulates the betacateninpathway. We failed to detect this interaction, inspite of exhaustive two hybrid screens in which we dididentify a number of other binders. We have confirmedthat the mouse FRAT1 can confer beta-catenin signalingactivity in Xenopus (Figure VII.2). In addition, co-immuneprecipitations show its binding to GSK3beta and Axin.We are currently testing the functionality of these interactions.Frat1 knockout mice do not show phenotypicalaberrations, possibly due to the widely overlappingexpression pattern of the related Frat2, and Frat3. Weare currently generating Frat2 and Frat3 knockout miceto test this.Proviral tagging in Cdk inhibitor knockout miceWe have started proviral tagging experiments in p21,p27, p15, p16, p19Arf single and compound knockoutmice to determine which proto-oncogene activationssynergize with the Cdk mutants. In this way we expect toidentify the complementation groups in transformation towhich the CDK inhibitors belong. This will permit us toestablish functional relationships between these differentgroups of genes. Proviral tagging in a p21 and p15 KObackground resulted in the activation of genes belongingto the standard complementation groups (Pim, Myc, Gfi1)without a significant difference in tumor latency.Interestingly, in p27 and p21;p27 deficient mice, MuLVinfection resulted in accelerated tumor inductioncompared to control mice; p27 +/- showed an intermediatelatency period. Remarkably, proviral tagging in the p27 -/-mice showed in a much higher frequency of activation ofMyc, whereas integrations near Pim and cyclinD 2 werestrongly reduced. This reduction was most pronounced inp21 -/- ;p27 -/- tumors, suggesting that PIM might, directly79MOLECULAR GENETICS
80MOLECULAR GENETICSor indirectly, act to relieve the inhibitory function of p21and p27 proteins. We are currently sequencing the flanksof the proviruses in this tumor panel.Further refinement of insertional mutagenesisTissue-specific expression of L1 retrotransposons toachieve insertional mutagenesis was investigated. For thispurpose, we have generated transgenic mice carryingthis retrotransposon. None of these mice expressed thetransposon. A knockin of the retrotransposon into theROSA26 locus yielded a low level of expression. Micecarrying this insertion were crossed with tumor pronePim1 transgenic mice to determine whether the transposonwould accelerate tumorigenesis but this did notappear to be the case. We are also exploring the utilityof the Sleeping Beauty (SB) DNA transposon for mutagenesisof somatic cells. This project is in collaboration withthe Plasterk group (Division V). Transposition in tissueculture cells is found at an appreciable level. However,insertion of the transposon into an adenoviral vector andinfection of cells with this vector did not give rise to ahigh frequency of transposition.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1447.2 Funding: EEC training grant ERBFMBICT 972620.3 Funding: EMBO fellowship.4 Funding: EEC BMH4-CT96-1518.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2058.6 Funding: Portugese PhD fellowship.7 Funding: Centre of Biomedical Genetics.8 STW royalties.* Head of transgenic/knockout service facility.** Animal Pathology Laboratory.Publications: Molecular geneticsBerns A. Mouse models for cancer at center stage.Trends Genet1999 15: 177.Berns A. Turning on tumors to study cancer progression. Nat Med1999; 5: 989-90.Hanson RD, Hess JH, Yu BD, Ernst P, Van Lohuizen M, Berns A,Van der Lugt N, Shashikant CS, Ruddle F, Seto M, Korsmeyer SJ. Mammalian Trithorax and Polycomb-group homologues areantagonistic regulators of homeotic development. Proc Natl AcadSci USA 1999; 96: 14372-7.Jacobs H, Krimpenfort P, Haks M, Allen J, Blom B, Démollière C,Kruisbeek A, Spits H, Berns A. PIM1 reconstitutes thymus cellularityin interleukin 7- and common gamma chain-mutant miceand permits thymocyte maturation in rag- but not CD3gammadeficientmice. J Exp Med 1999; 190: 1059-68.Jacobs JJ, Kieboom K, Marino S, Depinho RA, Van Lohuizen M.The oncogene and Polycomb-group gene Bmi1 regulates cellproliferation and senescence through the Ink4a locus. Nature1999;397: 164-8.Jacobs J, Scheijen B, Voncken J-W, Kieboom K, Berns A, VanLohuizen M Bmi-1 collaborates with c-Myc in tumorigenesis byinhibiting c-Myc induced apoptosis via INK4a/ARF. Genes &Development 1999;13: 2687-90.Jonkers J[Dissertation]. Identification and characterization of theFrat1 proto-oncogene. University of Amsterdam.1999.Jonkers J, Van Amerongen R, Van der Valk M, Robanus-MaandagE, Molenaar M, Destrée O, Berns A. Mechan of Devel 1999;88:183-94.Jonkers J, Weening JJ, Van der Valk M, Bobeldijk RC, Berns A..Overexpression of Frat1 in transgenic mice leads to glomerulosclerosesand nephrotic syndrome, and provides direct evidencefor involvement of Frat1 in lymphoma progresssion. Oncogene1999;18: 5982-90.Konietzko U, Kauselmann G, Scafidi J, Staubli U, Mikkers H,Berns A, Schweizer M, Waltereit R, Kuhl D. Pim kinase expressionis induced by LTP stimulation and required for the consolidation ofenduring LTP. EMBO J 1999;8: 3359-69.Li L, Yuan H, Weaver CD, Mao J, Farr GH, Sussman DJ, JonkersJ, Kimelman D, Wu D. Axin and Frat1 interact with dvl and GSK,bridging Dvl to GSK in Wnt- mediated regulation of LEF-1. EMBOJ 1999;18: 4233-40.Berns A, Mikkers H, Krimpenfort P, Scheijen B, Jonkers J.Identification and characterization of collaborating oncogenes incompound mutant mice. Cancer Res 1999;59: 1773s-1777s.Giovannini M, Robanus-Maandag E, Niwa-Kawakita M, Van derValk M, Woodruff J, Berns A, Thomas G. Schwann cell hyperplasiaand tumors in transgenic mice expressing a naturally occurringmutant NF2 protein. Genes Dev 1999; 13: 978-86.Quon K, Berns A. Biochim Biophys Acta 1999; 1423(2): 53-61Robanus Maandag E [Dissertation]. Mouse models for the humanhereditary cancer syndromes retinoblastoma and neurofibromatosistype 2. University of Amsterdam, 1999.Vooijs M, Berns A. Developmental defects and tumor predispositionin Rb mutant mice. Oncogene 1999; 18: 5293-303.Haks MC, Krimpenfort P, Van den Brakel JH, Kruisbeek AM. Pre-TCR signaling and inactivation of p53 induces crucial cell survivalpathways in pre-T cells. Immunity 1999;11: 91-101.
D Barlow PhDR Lyle PhD 1R Zwart PhD 2F Sleutels MSc 1S Verhaagh MSc 2I Van der BorchM Cuadrado LopezMammaliandevelopment andcancer geneticsGroup leaderPost-docPost-docGraduate studentGraduate studentTechnicianUndergraduate studentThe mechanism regulating imprinted gene expression 1Imprinted genes are epigenetically silenced on one ofthe two parental chromosomes. Since both the activeand inactive parental allele are retained in the nucleus,imprinting offers a particularly useful model to identify theepigenetic modifications that lead to gene silencing. Lossof imprinting (known as LOI) and parental-specific LOH(loss of heterozygosity) that indicates the presence ofimprinted loci, are features of tumor progression indiverse tumors types, suggesting that imprinted genescan function as growth regulators in adult tissues. Ourlaboratory has studied gene imprinting for several yearswith the aim of understanding more about its biologicalfunction and epigenetic mechanism. We have identifiedand analyzed the imprinted maternal-specific expressionof the Igf2r gene (Insulin-like growth factor type 2receptor, also known as the cation independent mannose6-phosphate receptor). This work has shown that theprimary function of Igf2r is to reduce extracellular levels ofthe growth hormone IGF2 in the embryo and, thus, todecrease embryonic size. Other laboratories have shownthat in humans, IGF2R is a tumor suppressor gene inliver and breast tumors. In an attempt to dissect theepigenetic mechanism imprinting this gene we haveinitially followed a transgenic approach in mice. Ourprevious work has demonstrated that the paternal alleleof Igf2r is repressed by a 3.7 kb DNA element containedin intron 2 (Wutz et al. Nature 1997; 389: 745-9). Thisintron 2 element contains the promoter of an unusualantisense RNA that has the reciprocal imprintedexpression compared to Igf2r. These results have allowedus to propose that expression-competition betweenneighboring promoters may be a common feature of theimprinting mechanism (Barlow, EMBO J 1997; 16: 6899-905).Work in progress on Igf2r imprintingTransgenic studies have demonstrated that imprintingof the Igf2r gene could be maintained in ectopic chromosomalpositions on a 300 kb genomic fragment.However, this work also demonstrated that shortfragments (1-14 kb) could not maintain imprinting of theantisense RNA promoter. We have continued to investigatethe minimum elements required for Igf2r imprintingusing transgenes. This work is still in progress but resultsindicate that multiple elements may be required for fullimprinted expression. This year we have mainly focusedon defining the extent of the antisense RNA. This hasbeen done by generating a 130 kb sequence contigspanning from Igf2r intron 7 to the upstream flankinggene. This sequence was used to identify EST cDNAclones from the database and this and other analysesshows that the antisense RNA is an exceptionally longand stable RNA that appears to lack an open readingframe. Whatever the final answer, the existing analysis ofgene imprinting has already demonstrated the involvementof several key epigenetic players including DNAmethylation and cis-repressor elements. The exactfunction of each of these is being actively investigated.Embryonic implantation as model of tumor metastases 2Establishing a vascular connection to host tissue isessential for further growth and development ofmammalian embryos. It is also a requirement of tumors.The mammalian embryo makes a vascular connection byinitiating a tightly controlled invasion of the maternaluterus using a specialized invasive cell type (the trophoblast),and subsequently forms a direct connection withthe maternal circulation through a specialized organ (theplacenta). Several genes have already been identified bytargeted inactivation as essential for implantation,however, many are cell lethals or not directly informativeabout the implantation process itself. In this project weare using a naturally-occurring mouse mutant namedtw 73 , to isolate a gene that appears to play a direct rolein trophoblast differentiation. Embryos homozygous forthe tw 73 gene fail to form a competent maternal-fetalconnection and die in the peri-implantation period. Thetw 73 gene will be used as a starting point to analyzeimplantation and to test our hypothesis that genes specificallyregulating implantation are candidate oncogenes ortumor suppressor genes.Work in progress in isolating the tw 73 geneA ‘positional cloning’ strategy is being used to isolatethe tw 73 gene that we have previously mapped to a 500kb critical region on mouse chromosome 17. Last yearwe described the identification of a novel cluster of threeorganic cation transporter genes (named Slc22 a1, a2,a3) spanning 150 kb of the 500 kb critical region. Thisyear, in an attempt to further reduce the minimal criticalregion we have applied genetic tests to this gene clusterto determine if any were equivalent to tw 73 . Slc22 a2 anda3 fulfill several of the criteria demanded for a candidatetw 73 gene. Both are expressed in implanting embryosand, in addition, Slc22a3 contains a tw 73 specific DNApolymorphism. Genetic rescue using a 300 kb YACtransgene (for Slc22 a1 & a2) and genetic complementationusing a targeted-inactive locus (for Slc22a3) are81MOLECULAR GENETICS
82MOLECULAR GENETICSnow being performed. The Slc22a3 gene is exclusivelyexpressed in placental tissue during embryonicdevelopment and is down regulated prior to birth. Otherlaboratories have suggested that Slc22a3 is a nonneuronalcatecholamine transporter that limits catecholamineavailability during embryonic development. Otherlaboratories have also shown that the catecholaminesadrenaline and nor-adrenaline are essential for embryonicdevelopment and mice deficient for these neurotransmittersdie shortly after mid-gestation. We are using ourSlc22 a3 ‘knockout’ mouse to examine the function ofthis gene in the embryonic placenta and in particular totest its role in placental catecholamine clearance(FigureVII.3).Our final goal with this project is to use the isolated tw 73gene as a molecular entry point to study the invasivephase of embryonic implantation. In addition, the humanhomolog of the tw 73 gene is expected to reside in thesyntenic region on human chromosome 6q26-27. Thisregion shows frequent LOH in liver, breast and ovariantumors. The human tw 73 gene will provide a usefulmarker to define more accurately the physical maps ofthe minimum LOH region. It is also anticipated thatidentification of the human tw 73 gene may provide amolecular entry point into genes involved in cancermetastases.Notes1 Funding: Dutch Cancer Society, Project 97-1561.2 Funding: Dutch Cancer Society, Project 96-128.Publications: Mammalian developmentSleutels F, Barlow DP. One more imprinting review? BookReview. Nat Genetics 1999; 23: 23.Verhaagh S, Schweifer N, Barlow DP, Zwart R. Cloning of themouse and human solute carrier 22a3 (Slc22a3/SLC22A3)identifies a conserved cluster of three organic cation transporterson mouse chromosome 17 and human 6q26-27. Genomics1999; 55: 209-18.Control of telomeraseactivationR Beijersbergen PhDL Carlee MScW NijkampS CillessenGroup leaderGraduate studentTechnicianUndergraduate studentFigure VII.3Expression of the Slc22a3 gene is restricted to the labyrinth (L)layer of the embryonic placenta. Top panel: general organizationof the day 13.5 placenta. Middle, RNA in situ analysis ofSlc22a3 (10x magnification), bottom panel 20X magnification. S,spongiotrophoblast layer.Research in our group is primarily focused on theactivation of telomerase in human cells. Normal humansomatic cells, which generally lack telomerase activity,exhibit progressively shortened telomeres with repeatedcell divisions and enter senescence after a limitednumber of cell divisions. When the life span of normalcells is extended beyond senescence, life span terminatesat crisis, a point at which telomere loss results in
chromosome instability and cell death. However, telomereshortening is stopped by the expression of hTERT, thecatalytic subunit of the telomerase enzyme, in those cellsthat have become immortal. hTERT mRNA cannot bedetected in most normal cell lineages but is present in avariety of tumor cell lines and is detectable in 90% ofhuman tumors. The ectopic expression of hTERT is sufficientto restore telomerase activity and maintain orextend telomeres. The introduction of hTERT in severalprimary human cells prevented senescence, allowedthem to bypass crisis and become immortal. The introductionof hTERT together with collaborating oncogenes,such as Large T and Ras, is sufficient for tumorigenictransformation of primary human cells. In contrast, inactivationof telomerase in immortal cells results in telomereshortening and cell death. Together these results indicatethat hTERT expression represents the rate-limiting determinantthat regulates the levels of telomerase enzymeactivity in tumor cells and that the process of cell immortalizationis closely or completely linked to the expressionof hTERT.We are studying the molecular mechanisms responsiblefor derepression of the hTERT gene that occursupon immortalization. We have isolated, sequenced, andanalyzed genomic fragments containing the promoter andpotentially upstream regulatory elements of the humanhTERT gene. Our detailed analysis has revealed severalcandidate transcription factor-binding sites. We haveidentified the promoter region required for activation intelomerase positive cells. This region is currently beingused to identify transcriptional activators and/orrepressors of the hTERT gene. Through comparison ofhTERT promoter regulation in telomerase positive andnegative cells by deletion analysis, genomic footprinting,and electromobility bandshift analysis, we will identifyelements involved in the regulation of hTERT expression.These elements will then be used to identify interactingproteins that can elucidate the regulation of the hTERTgene. Furthermore we have set up a hTERT-reportersystem that allows for the identification of proteins orpathways that can either repress or activate hTERTexpression through cDNA expression library screens.The result of these studies may allow us to elucidatethe molecular mechanism that enables cancer cells toovercome two barriers, senescence and crisis, beforethey become immortal. The identification of the proteinsor pathways that are involved in regulation of telomeraseexpression may have implications for interference with theprocess of immortalization and provide us with amolecular event, specific in the generation of tumor cells.Publications: Control of telomeraseactivationHahn W C, Counter C M, Lundberg A S, Beijersbergen R L,Brooks M W, Weinberg R A. Creation of human tumour cells withdefined genetic elements. Nature 1999; 400: 464-68.Hahn W C, Stewart S A, Brooks M W, York S G, Eaton E, KurachiA, Beijersbergen R L, Knoll J H, Meyerson M, Weinberg R A.Inhibition of telomerase limits the growth of human cancer cells.Nat Med 1999; 10: 1164-70.P Demant PhDM Snoek PhDT Csikos PhD 5N Tripodis PhD 1M Van Kooy PhD 4C Ruivenkamp MSc 2T Van Wezel MSc 3K De Groot 4E Delzenne-GoetteJ De MoesE Dijsselbloem 5A Klous 5M Treur-MulderH Van Vugt 2M GajewskaH HavelkovaI SchultzCancer geneticsGroup leaderAcademic staffPost-docPost-docPost-docGraduate studentGraduate studentTechnicianTechnicianTechnicianTechnicianTechnicianTechnicianTechnicianGuestGuestUndergraduate studentThe outcome of the processes initiated by theexposure to carcinogenic agents (chemical, physical, viral)is strongly modified by numerous genes of the host. Thisoften results in large differences in cancer susceptibilitybetween individuals. The identification of the modifiergenes and the elucidation of their functions is the aim ofthis group. As the number of these genes is large, theirdetection in humans is virtually impossible and they haveto be identified first in animal models. This effort startswith the establishment of linkage of the modifier genes tospecific chromosomes. For this purpose we developed aspecific genetic tool, the recombinant congenic strains(RCS) of mice which exhibit reduced genetic variabilityand therefore facilitate detection of modifier genes, eventhose with relatively small effects. In the next steps themodifier genes are mapped to a very short chromosomalsegment (less than 0.5 centiMorgan long), encompassingless than 1 Mb DNA. Subsequently, the candidate genesin the region are identified and the correlation of theirpolymorphism with their cancer-modifying effects has tobe established and their function demonstrated infunctional assays or by genetic modification. In additionto identifying the modifier genes we are also studying thenature of their effects in the segregating populations, aswell as their impact on tumor phenotype.83MOLECULAR GENETICS
84MOLECULAR GENETICSOur main interest resides in the study of colon andlung cancer, the two major causes of cancer morbidityand mortality. In collaborative projects genes modifyingsusceptibility to radiation-induced leukemias and genesinvolved in control of various stages of immuneresponses have also been mapped.MHC class III region and tumorigenesisWe have mapped a tumor susceptibility gene forchemically induced alveolar lung cancer to an interval of27 kb within the Major Histocompatibility Complex of themouse. Detailed analysis of this segment has revealedthe presence of three genes G7e, G7a and G7c, forwhich we have determined the complete genomic organization.The G7e encodes a viral envelop protein, G7aencodes valy-tRNA synthetase, while the G7c gene hasno homologs in the database that could predict itsfunction. We are currently studying the expressionpatterns and expression levels of the genes in the criticalregion.We generated genomic DNA lambda phage librariesand built contigs spanning the interval derived from DNAfrom the resistant B10.A(1R) and the susceptibleB10.A(2R). Using shot gun subcloning of lambda insertsand in conjunction with automatic sequencing, we aredetermining the sequence of the complete interval ofboth strains. Comparison of the critical region betweenthe susceptible and the resistant strain will lead to thefinding of disease associated differences.Analysis of the genetic differences and study of thesusceptibility gene involved might lead to the understandingof the possible mechanism underlying thephenomenon of predisposition to tumorigenesis. Sincethe class III region of the MHC is highly conservedbetween species, the assignment of a mouse tumorsusceptibility gene might be of importance for the evaluationof human predisposition to lung cancer.Susceptibility to lung tumorsThe strain O20/A is susceptible and the strainB10.O20/Dem is relatively resistant to carcinogeninduced tumors. Moreover, they differ in the histologicaltype and rate of progression of the lung tumors.Previously, using crosses of several OcB recombinantcongenic strains (containing 88% of genes from the strainO20 and the remainder from the strain B10.O20) wemapped 14 novel Sluc (Susceptibility to lung cancer) lociand demonstrated that they frequently engage in mutualinter-locus interaction. We proceeded with the finemapping of these loci, as a step towards their positionalcloning. Mice with recombinations at various sites of theregions bearing the Sluc loci 1,3,4,6, and 8 wereproduced for testing their susceptibility phenotype.Analysis of the genetic differences in the histological typeof the lung tumors is ongoing. Morphometric systemsand methods of statistical analysis were developed whichallow recognition of strain specific patterns of variousaspects of the tumor phenotype, as well as the study oftheir inheritance in segregating populations. This studyled to mapping of several novel loci controlling the qualitativeaspects of lung tumorigenesis.Susceptibility to colon tumorsThe analysis of genetics of susceptibility to colontumors in the recombinant congenic strains led to thedetection of 9 novel Scc (Susceptibility to colon cancer)loci (Scc1 - Scc9) located on chromosomes 1, 2, 3, 8,10, 11, 17, and 18. Two pairs of loci were found tointeract with each other: Scc4 - Scc5 and Scc7 - Scc8(Van Wezel et al. Nature Genetics 1996; 14: 468-70 andVan Wezel et al. Cancer Res 1999; 59: 4216-18). Apositional cloning approach is being used to identify theScc1 gene on chromosome 2. Previously, Scc1 has beenmapped to an interval of less than 200 kb using recombinanthaplotypes. The DNA from the BACs covering thisinterval was subcloned and shot-gun sequenced. Theavailable sequence covers almost the whole region andits analysis revealed several genes and ESTs. Theexon/intron organization of the genes has been partlyunraveled and several polymorphisms between susceptibleand resistant allele were defined. This resulted in themapping of the Scc1 locus to less than 70 kb.An analogous strategy is being applied to thepositional cloning of the interacting pair of the loci Scc4(chromosome 17) and Scc5 (chromosome 18). A novelmapping cross between the strains CcS19 and BALB/chas been started, to confirm and further improve theoriginal mapping result and a number of recombinanthaplotypes in the chromosomal regions containing thetwo loci has been produced. The susceptibility testing ofthese recombinants will be performed in the comingperiod and may localize each of the loci to a 2 - 3centiMorgan interval, which will provide a starting pointfor fine mapping and positional cloning.Notes1 Funding: NWO Project <strong>NKI</strong> 925-01-001.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1436.3 Funding: European Commission, Contract CT 98-0445.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1837.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1832.Publications: Cancer geneticsHavelkova H, Kosarova M, Krulova M, Demant P, Lipoldova M. T cellproliferative response is controlled by loci Tria4 and Tria5 on mousechromosomes 7 and 9. Mammalian Genome 1999; 10: 670-4.Kosarova M, Havelkova H, Krulova M, Demant P, Lipoldova M.Production of two Th2 cytokines, IL-4 and IL-10 is independentlycontrolled by a locus Cypr1 and by loci Cypr2 and Cypr3, respectively.Immunogenetics 1999; 49: 134-41.Mori N, Okumoto M, Yamate J, Stassen APM, Tsubura A,Akamatus T, Sakuma S, Demant P. Enhancement of glucocorti-
85coid-induced apoptosis of thymocytes linked to the p53-deletionand interaction between the chromosomal segments containingRapop1 and p53. Oncogene 1999; 18: 4282-5.Snoek M, Van Kooij M, De Groot K, Van Vugt H. The mouse p52subunit of the transcription/DNA repair factor TFIIH is not locatedin the MHC class III region of the H2 complex, but resides next toa G7a/Bat6 homologue in the telomeric part of the MHC.Immunogenetics 1999 (in press).MOLECULAR GENETICSSnoek M, Van Vugt H. The sequence and organization of themouse valyl-tRNA synthetase gene G7a/Bat6 located in the MHCclass III region. Immunogenetics 1999; 49: 468-70.Szymanska H, Sitarz M, Krysiak E, Piskorowska J, CzarnomskaA, Skurzak H, Hart AAM, De Jong D, Demant P. Genetics ofsusceptibility to radiation-induced lymphomas, leukemias andlung tumors studied in recombinant congenic strains. Int J Cancer1999; 83: 674-8.Van Wezel T, Ruivenkamp C A L, Stassen APM, Moen CJA,Demant P. Four new colon cancer susceptibility loci, Sscc6 toScc9 in the mouse. Cancer Research 1999; 59: 4216-18.SecretariesG De Jong-MeijerinkS HeussenK Van den BergResearch staff positions (full time equivalents)Scientific permanent: 5.1Scientific project: 20.0Technical permanent: 2.5Technical project: 7.5
86VIII Division of ExperimentalTherapyDivision head Adrian BeggIntroductionThe goals of the Division of Experimental Therapy areto optimize and refine existing cancer therapies, developand test new ones, and improve diagnosis and responseprediction by cellular and molecular characterization oftumors. The division consists of three subdivisions:Experimental Chemotherapy, Experimental Radiotherapyand Molecular Pathology. Clinical links are emphasized inall projects, with active collaboration of scientists andclinicians.One new project was started this year; a collaborationbetween the Schellens and Schinkel groups on mechanismsof reduced cellular accumulation of topoisomeraseI inhibitors. Lou Smets retired this year, bringing to anend an illustrious career in experimental chemotherapy.His scientific and social input will be missed.Highlights and future plansIn studies on hypoxia (Begg group), an image analysismethod was developed and validated in which IdUrdlabeling around individual vessels was used to monitorvascular perfusion. Analysis of vasculature alone wasfound to be insufficient to accurately assess tumor hypoxia(comparison with the bioreductive marker pimonidazole).Projects to develop assays for predicting radiotherapyoutcome will continue to concentrate on ways to measurechronic and acute hypoxia in human tumors, focusing onthe combined use of bioreductive marker drugs, vascularderived parameters and vascular perfusion using IUdRbasedand other techniques. Clinical studies will continuein head and neck cancer patients, which will include thesehypoxia measurement methods. A recently started projecthas shown that transduction with a retroviral vectorexpressing a dominant negative of DNA polymerase betatogether with EGFP (green fluorescent protein) markedlysensitized human tumor cells to radiation. These studieswill continue, concentrating on DNA polymerase beta, forwhich significant effects have already been observed, andon ku80, with the eventual aim of testing the potential fortherapeutic intervention.The Stewart group has shown a significant increase inglomerular vWF and leukocytes in the renal cortex afterirradiation, although the increased glomerular vWF didnot quantitatively predict renal dysfunction. Plateletaggregation could be inhibited with acetylsalicylic acid orClopidogrel, but with only small effects on kidneyfunction. Studies will continue on the role of endothelialcell and vascular damage in kidney pathogenesis afterradiation, with emphasis on mechanisms and ways toameliorate damage. Emphasis will be on anti-thromboticagents which block the GPIIb/IIIa and ADP plateletreceptors. In the photodynamic therapy (PDT) program,carbogen breathing ± nicotinamide improved pO2 leadingto significantly improved PDT response. In addition,preclinical and clinical studies have demonstrated greaterPDT responses for illuminations at 1 to 2 days aftersensitization than at 3 to 5 days. Future research willfocus on the relationship between photosensitizerpharmacokinetics in tissues and plasma and PDT efficacyin animal and clinical studies. In a new preclinical studywith Division XII, attempts to improve peritoneal lavageregimes will be made to increase cytotoxicity and reducetumor re-seeding.The Schinkel Experimental Chemotherapy group hasshown that placental P-gp limits the passage of varioustoxins and drugs into developing fetuses. It was alsoshown that P-gp inhibitors could potentially be used toincrease the fetal penetration of P-gp substrate drugs.Other studies showed that even low levels of P-gp andMrp1 contribute considerably to tumor drug resistance,suggesting that multidrug transporter inhibitors may alsoincrease the sensitivity of previously untreated (naïve)tumors to chemotherapy. Further investigations will becarried out into the functional role of Bcrp1 in drugresistance, e.g. by trying to elucidate why Bcrp1 overexpressionsometimes correlates with efficient resistanceagainst anthracyclines, whereas othertimes only very lowresistance is observed. Conditional and constitutiveBcrp1 knockout mice will be generated in order to studythe physiological and possible pharmacological roles ofBcrp1. In addition, knockout mice for several otherpharmacologically relevant proteins, including the Orct1and Orct2 organic cation transporters and various drugmetabolizingenzymes, will be generated to better understandand predict the overall pharmacological behavior ofdrugs in an intact organism. The behavior and interactionsof HIV protease inhibitor drugs will be furtheranalyzed in Mdr1a/1b knockout mice, and possibly inadditional knockout mouse strains.
The Schellens Experimental Chemotherapy groupfound that drug resistant human ovarian tumor cellsexpressed the Breast Cancer Resistance Protein (BCRP),which could efficiently transport Topotecan and mitoxantrone.One of several potential inhibitors for BCRP wascapable of completely blocking outward transport oftopotecan, completely resensitizing these cells to drug.Studies will continue on mechanisms of resistance totopoisomerase I inhibitors and mitoxantrone, in particularinvestigating the nature of the implicated novel BCRPefflux system present at the plasma membrane ofresistant cells. In addition, studies on the interactionbetween platinum drugs and topoisomerase I inhibitorswill continue, focusing on yeast as a model systems inwhich a variety of mutants will be employed, havingdefects in various aspects of DNA repair and enzymetopoisomerase levels. These studies have alreadyindicated a role for rad52 but not rad4 in synergy. Finally,platinum-DNA adducts, and topoisomerase I levels inWBC and tumor tissue, will be measured as pharmacodynamicendpoints in ongoing clinical studies withcisplatin, carboplatin and topoisomerase I inhibitors.Research in the Molecular Pathology group (Van ’tVeer, Van de Vijver) will remain focused on breast cancerpathogenesis and treatment. In studies on multidrugresistance proteins in breast cancer, MDR1/P-Gp involvementwas shown to be unlikely. Preliminary experimentsinvolving comparative genomic hybridization (CGH)showed that the number of genetic alterations involved inbreast tumor progression (in situ to invasive) is low.These studies will continue in the coming year.Completing the case-control study on the involvement ofradiotherapy in breast cancer susceptibility will enable usto assess the contribution of ATM heterozygosity to therisk of radiation-induced breast cancer. Marker genes forbreast cancer cells, determined by the method of SerialAnalysis of Gene Expression (SAGE), will be tested fortheir validity in minimal residual disease detection. SAGEprofiles of a breast cell line transfected with either anormal or a dominant-active estrogen receptor willelucidate downstream effector genes of normal andvariant receptors.Publications Smets group (now disbanded)Kuin A, Aalders M, Lamfers M, Van Zuidam DJ, Essers M, BeijnenJH, Smets LA. Potentiation of anticancer drugs at low intratumoralpH induced by the mitochondrial inhibitor m-iodobenzylguanidine(MIBG) and its analogue benzylguanidine (BG). Br J Cancer1999, 79: 793-801.Kuin A, Van der Valk M, Rutgers M, Beijnen JH, Smets LA.Bioavailability and toxicity of oral administration of m-iodobenzylguanidine(MIBG). Br J Cancer 1999, 79: 802-6.Taal BG, Hoefnagel C, Rutgers M. Carcinoid tumors. N Engl JMed 1999, 341: 454-5.Salomons GS, Smets LA, Verwijs-Janssen M, Hart AAM,Haarman EG, Kaspers GJL, Van Wering ER, Van der Does-Vanden Berg A, Kamps WA. Bcl-2 family members in childhood acutelymphoblastic leukemia: relationships with features at presentation,in vitro and in vivo drug response and long-term clinical outcome.Leukemia 1999; 13: 1574-80.Prediction and manipulation of treatmentoutcomeAC Begg PhDH Bartelink MD PhD 1KMG Haustermans MD PhDNS Russell MD 1JM Coco Martin PhD 2C Vens PhDE DahmenA GrummelsI HoflandD SprongI Van de Pavert 3M VerwijsW BlyweertB Van der SchuerenGroup leaderAcademic staffAcademic staffAcademic staffPost-docPost-docTechnicianTechnicianTechnicianTechnicianTechnicianTechnicianUndergraduate studentUndergraduate studentPrediction of tumor radiosensitivityAttempts to measure chromosome damage in cellsextracted from human tumor biopsies have continued.Separating fibroblasts from tumor cells is a majorconcern, and we previously reported on the use of ananti-human-fibroblast antibody and FACS sorting. We arenow using an improved antibody together with magneticbead separation (MACS). MACS was shown to have littleor no negative effect on plating efficiencies and toproduce purity of over 95% tumor cells and yields ofaround 70%. It appeared to be less toxic than FACSsorting and is now our method of choice. Prematurechromosome condensation (PCC) using the phosphataseinhibitor calyculin A (CA) has proved feasible in cells frombiopsies, although PCCs indices are lower than in celllines. We showed that the majority of scorable PCCswere from G2 cells and few from G1, although this couldbe improved slightly by addition of activated cdc2. Wecompared 5h colcemid, which should collect all G2 cellsin mitosis, with 1h CA in cells from biopsies.Approximately 4 times more scorable PCCs were foundthan metaphases, showing the superiority of chemicalPCCs over conventional metaphase collection. Theoptimum culture time of biopsy cells for maximum PCCyield was found to be 1 week. Good growth of cells froma large fraction of tumor cells remains the most difficultand limiting factor.Prediction of tumor hypoxiaThere is strong evidence that tumor hypoxia limits thesuccess of cancer therapy, including radiotherapy.Indirect evidence suggests acute hypoxia, caused by87EXPERIMENTAL THERAPY
88EXPERIMENTAL THERAPYblood perfusion changes, can be equally important aschronic hypoxia, caused by diffusion limitations. Ourimmediate goal is to define the relative importance ofacute and chronic hypoxia in human tumors in limitingsuccess of radiotherapy. We developed an imageanalysis protocol to measure the Diffusion LimitedFraction (DLF), being the fraction of tumor area in a histologicalsection greater than 120µ from the nearest bloodvessel; a measure of diffusion limited hypoxia.Comparisons were made with pimonidazole staining (abioreductive hypoxic marker drug) in 10 cervix tumors.The area stained by pimonidazole was significantlysmaller than DLF for all tumors. When images from alltumors (n=123) were analyzed together, the correlationwas highly significant (r=0.36, p
Notes1 Division IX.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1265.3 Biophysics.Publications: Prediction andmanipulation of treatment outcomeBartelink H, Begg A, Coco J Martin, Van Dijk M, Van ‘t Veer L, Vande Vaart P, Verheij M. Towards prediction and modulation of treatmentresponse. Radiother Oncol 1999; 50: 1-11.Begg AC, Haustermans K, Hart AA, Dische S, Saunders M,Zackrisson B, Gustaffson H, Coucke P, Paschoud N, Hoyer M,Overgaard J, Antognoni P, Richetti A, Bourhis J, Bartelink H,Horiot JC, Corvo R, Giaretti W, Awwad H, Shouman T, Jouffroy T,Maciorowski Z, Dobrowsky W, Struikmans H, Wilson GD. Thevalue of pretreatment cell kinetic parameters as predictors forradiotherapy outcome in head and neck cancer: a multicenteranalysis. Radiother Oncol 1999; 50: 13-23.Begg AC, Hofland I, Van de Pavert I, Van der Schueren B,Haustermans K. The use of thymidine analogs to indicate vascularperfusion in tumours. Br J Cancer (in press).Bergstrom C, Begg A, Palmqvist R, Waites A, Denekamp J.Labelling indices in human tumours: to apply corrections or not -that is the question. Br J Cancer 1999; 80:1635-43.Coco Martin JM, Mooren E, Ottenheim C, Burrill W, Nunez MI,Sprong D, Bartelink H and Begg AC. Potential of radiation-inducedchromosome aberrations to predict radiosensitivity in humantumor cells. Int J Radiat Biol 1999; 75: 1161-8.Dittmann KH, Gueven N, Mayer C, Ohneseit P, Zell R, Begg AC,Rodemann HP. The presence of wild-type TP53 is necessary forthe radioprotective effect of the Bowman-Birk proteinase inhibitorin normal fibroblasts. Radiat Res 1998; 150: 648-55.Haustermans K, Fowler J, Geboes K, Lerut A, Van Cutsem E,Begg A. Cell kinetic measurements: principles, guidelines for treatment?Hepatogastroenterology 1999; 46: 670-8.Van de Vaart PJM, Belderbos J, De Jong D, Sneeuw KCA, MajorD, Bartelink H, Begg AC. DNA-adduct levels as a predictor of outcomefor NSCLC patients receiving daily cisplatin and radiotherapy.Int J Cancer (in press).Van de Vaart PJM [Dissertation]. Interaction of platinum coordinationcompounds with radiation or hyperthermia: from laboratory toclinic. Amsterdam: Free University, 1999.FA Stewart PhDP Baas MD PhD 1LGH Dewit MD PhD 2N Van der Vange MD PhD 3S Bapat PhD 4A Kuin PhDEM Van Kleef PhD 5BGJ FlootH Oppelaar 4MC RuevekampJAM Te PoeleA Van der Wal 5RLP Van Veen 4, 6JH Schouwink MD 7Vascular mediatedtherapy and tissuedamageGroup leaderAcademic staffAcademic staffAcademic staffPost-docPost-docPost-docTechnicianTechnicianTechnicianTechnicianTechnicianTechnicianGuestRadiation induced renal injury 5Irradiation has been shown to induce changes inendothelial cell (EC) function which initiates thromboticand inflammatory cascades. We are investigating the roleof EC and vascular damage in the development of laterenal radiation injury with the aim of identifying possiblemechanisms for pharmacological intervention. Markers ofEC damage under investigation include von WillebrandFactor (vWF) and ADPase (mediators of plateletadhesion), and leukocyte accumulation, which occurs atsites of platelet activation. Quantitative immunohistochemistryof mouse kidneys demonstrated a significantincrease in glomerular vWF and leukocytes in the renalcortex from 12 weeks after high single dose irradiation.Smaller increases were seen after more clinically relevantfractionated irradiation. The leukocyte accumulation wassignificantly related to both time and dose but increasedglomerular vWF was independent of dose and did notquantitatively predict for the extent of renal dysfunction.Increased glomerular vWF could be due to upregulationof vWF synthesis in irradiated EC’s, or to the presence ofan increased number of glomerular EC’s as a result ofradiation induced compensatory proliferation. Increasedglomerular proliferation was seen from 10 weeks afterirradiation but the total cell number actually decreased(cell loss exceeded proliferation). This suggests that theobserved increase in glomerular vWF was due toincreased production of the protein in surviving EC’srather than proliferation.We have investigated the potential of anti-platelettherapy for ameliorating late radiation nephropathy inmice. Daily oral administration of the cyclooxygenaseinhibitor acetylsalicylic acid (ASA) inhibited production ofthromboxane and effectively inhibited platelet aggre-89EXPERIMENTAL THERAPY
90EXPERIMENTAL THERAPYgation. ASA given continuously from the time ofirradiation lead to a small (non-significant) protectiveeffect and delayed the onset of renal functional damageby 2 to 6 weeks. The ADP receptor blocker Clopidogrelalso provided effective inhibition of platelet aggregationbut studies to date have not demonstrated anyprotection against radiation nephropathy.Proteinurea is an early sign of progressive renaldamage. The increased vascular permeability may be dueto inflammatory responses or increased expression ofVEGF. We are currently studying these phenomena tosee how they relate to the dramatic changes seen inrenal vascular structure after irradiation. Major vessels inirradiated kidneys become enlarge and tortuous, whereasthe fine vascular network is lost leading to underperfusionof large areas of the tissue. Oxygen radicalscavengers are being evaluated as possible modifiers ofproteinuria resulting from the inflammatory response.Short term administration of catalase and superoxidedismutase could not reduce existing proteinurea. Longterm administration of n-actyl-cysteine is currently underinvestigation.of photosensitized rats did demonstrate increasedcardiac muscle degeneration and myocardial hemorrhagefor illumination at 1 day. Short illumination intervals,although effective, are probably only suitable for smallvolume PDT.In the clinical application of PDT for treatment of MM,integral illumination of the entire thoracic cavity isrequired. Real time fluence rate measurements made atvarious positions within the cavity have demonstratedthat sinuses which form near the diaphragm aresometimes under-illuminated. To overcome this problem,a wedge shaped light delivery/detector applicator hasbeen developed to give additional illumination in thesinuses and provide a more homogeneous dose distributionover the thorax (Figure VIII.2).One possibility for improving the selectivity of PDT is totarget photosensitizer specifically to the tumor. In collaborationwith M Vrouenraets and G van Dongen (FreeUniversity, Amsterdam), we have tested photoimmunoconjugatesof Foscan ® coupled to mAb’s specific forPhotodynamic Therapy 4PDT is being evaluated in our clinic for the treatmentof malignant mesothelioma (MM), head and neck cancerand basal cell skin cancer (BCC). The goal of this projectis to identify optimal parameters for Foscan ® -mediatedPDT.Oxygen is a necessary substrate for the photochemicalreaction and deficits can arise during illumination,rendering the reaction inefficient. This is more likely tooccur for illumination at high fluence rates and in poorlyvascularized tumors. In situ measurements of pO 2 andimmunohistochemical staining of hypoxic areas, demonstratedhypoxia developing during PDT in some murineRIF1 tumors but not in human MM xenografts. Carbogenbreathing ± nicotinamide (a vasodilator) improved pO 2 inall tumors and lead to significantly improved PDTresponse (tumor growth delay and cure). Reducing thefluence rate also improved response for RIF1 tumors butnot for MM xenografts.Our preclinical experiments have consistently demonstratedgreater PDT responses for tumor illumination at 1day after sensitization than at 3 to 5 days, despite thefact that tumor drug levels remained high throughout thisperiod. PDT of patients with multiple BCC was also moreeffective for illumination at 1 to 2 days (70 to 85% CR)than at 3 to 4 days (
head and neck carcinoma (HNSCC). Biodistributionstudies in mice bearing HNSCC xenografts demonstratedimproved tumor selectivity (by >5x) of the conjugates,despite their rapid elimination from the blood. Preliminaryresults on in vitro efficacy of PDT showed that Foscan ®coupled to an internalizing Ab exhibited more phototoxicitythan when coupled to a non-internalizing Ab.Intra-abdominal perfusion for treatment of minimal residualdisease (MRD)Since 1995 an experimental treatment modality(OV)HIPEC is being investigated in our clinic for intraabdominallymetastasized colorectal and ovarian cancer(see Division XII). In this new preclinical study we areusing rat models to determine whether lavage regimes asused in the (OV)HIPEC procedure could be improved to1) increase cytotoxicity against MRD; 2) reduce the riskof tumor re-seeding and growth at sites of surgicallyinduced peritoneal defects. Peritoneal perfusion regimesto be investigated include hyperthermic cisplatinum, withthe addition of compounds that inhibit cell adhesion (e.g.RGD-peptides) or cell infiltration (e.g. metalloproteinaseinhibitors).Notes1 Division X.2 Division IX.3 Division XI.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1446.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1444.6 Dr. Daniel den Hoed Cancer Clinic, Rotterdam.7 Medisch Spectrum Twente, Enschede.Publications: Vascular mediated therapyAalders MCG, Van der Vange N, Stewart FA, Klein MG, Van deVijver MJ, Sterenborg HJCM. White light toxicity resulting fromsystemically administered 5-ALA under normal operating conditions.J Photochem Photobiol B 1999; 50: 88-93.Stewart FA. Retreatment after full course radiotherapy: is it a viableoption? Acta Oncol 1999; 38: 855-62.Tan IB, Oppelaar H, Ruevekamp MC, Veenhuizen RB, Timmers A,Stewart FA. The importance of in situ light dosimetry for photodynamictherapy of oral cavity tumors. Head Neck 1999; 21: 434-41.Van Kleef EM, Zurcher C, Oussoren YG, Te Poele JAM, Van derValk MA, Niemer Tucker MMB, Van der Hage MH, Broerse JJ,Robbins MEC, Johnston DA, Stewart FA. Long-term effects oftotal body irradiation on the kidney of Rhesus monkeys. Int JRadiat Biol (in press).Vrouenraets MB, Visser GWM, Stewart FA, Oppelaar H, Stigter M,Postmus PE, Snow GB, Van Dongen GAMS. Development ofmTHPC-monoclonal antibody conjugates for photoimmunotherapy.Cancer Res 1999; 59: 1505-13.AH Schinkel PhDJD Allen PhD 1JW Smit PhD 2MT Huisman MSc 3JW Jonker MSc 2RF Brinkhuis 1E WagenaarGenes and proteinsinvolved in anticancerdrug resistance andpharmacokineticsGroup leaderPost-docPost-docGraduate studentGraduate studentTechnicianTechnicianOur research focuses on genes and proteins that can:1) cause (multi-)drug resistance in tumors; 2) determinethe pharmacological behavior of anticancer drugs. Insightinto these systems may help improve current chemotherapystrategies used to treat cancer, as well aspharmacotherapy in a broader sense. To study thephysiological and pharmacological roles of the relevantgenes we generate knockout mice that lack one or moreof the encoded proteins, and analyze the mice forresulting alterations. In addition, we are using cell linesobtained from such knockout mice as tools to search fornew drug resistance genes.Mice lacking Mdr1-type P-glycoproteinsPharmacological experiments using the Mdr1a/1bknockout mouse model have taught us that the drugtransportingP-glycoproteins (P-gps) have an importantrole in protecting an organism against exogenous toxins.We previously found that P-gp in the blood-brain barrierand blood-testis barrier prevents accumulation of transporteddrugs in these organs, while in liver, kidney andintestine P-gp contributes to the total body clearance ofthese drugs. We recently found that, analogous to therole of P-gp in the blood-brain barrier, placental P-gplimits the passage of various toxins and drugs intodeveloping fetuses (Figure VIII.3). We have further shownthat the P-gp inhibitors PSC833 or GG918 can enhancethe trans-placental movement of substrate drugs into thefetus by complete inhibition of placental P-gp. Thesefindings imply that P-gp inhibitors should be usedcautiously in pregnant women but that they may potentiallybe used to increase the fetal penetration of P-gpsubstrate drugs when this is therapeutically desirable.Since the fetal penetration of the HIV protease inhibitorssaquinavir and indinavir was clearly diminished byplacental P-gp, this principle could potentially be used todiminish the chance of vertical transmission of HIV.Characterization of new anticancer drug resistance genesCharacterization of mouse fibroblast cell lines deficientfor the multidrug transporters P-gp and Mrp1 demon-91EXPERIMENTAL THERAPY
92EXPERIMENTAL THERAPYAmsterdam). The goal is to identify an analog that is bothless toxic and more easily synthesized than the nativecompound. Bcrp1-mediated resistance in the mouse celllines could also be effectively reversed by the known P-gp inhibitor GG918. The existence of this effectiveBCRP/Bcrp1 inhibitor, which also has a low toxicity, mayallow us to quickly test possible in vivo roles of Bcrp1 inmice.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1433.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1434.3 Funding: AIDS fonds, Netherlands, Project 4011.Publications: Drug resistance andpharmacokineticsFigure VIII.3Effect of placental P-glycoprotein (Mdr1a/1b) genotype on thedistribution of the anticancer drug paclitaxel (inset) to fetuses.Heterozygous females were crossed to heterozygous males toobtain embryos of all three genotypes in one mother. The ratioof total fetal paclitaxel concentration and maternal plasmaconcentration of paclitaxel, 1 hour after an i.v. administration ofpaclitaxel, is plotted. P-glycoprotein-deficient fetuses accumulate16-fold more paclitaxel than wild-type fetuses.strated that normal expression of these proteins contributessubstantially to basal drug resistance. Thissuggests that even low levels of P-gp and Mrp1 couldcontribute to tumor drug resistance and that inhibitors ofmultidrug transporters, currently tested in clinical trials asdrug resistance reversal agents, may also increase thesensitivity of previously untreated (naïve) tumors tochemotherapy.Selection of the P-gp/Mrp1 deficient cell lines forresistance to the drugs mitoxantrone, topotecan ordoxorubicin resulted in amplification and consequentoverexpression of the murine homolog (Bcrp1) of therecently identified human multidrug transporter BCRP(Breast Cancer Resistance Protein). Cloning and characterizationof the mouse Bcrp1 cDNA indicated that Bcrp1closely resembles its human counterpart, and that mousemodels will therefore be useful for investigating thenormal physiological and possible pharmacological rolesof BCRP.Inhibitors of drug transporters are valuable as reagentsfor analyzing drug resistance mechanisms in thelaboratory, and potentially for reversal of clinical drugresistance in tumors. We are currently evaluating analogsof fumitremorgin C, a known inhibitor of BCRP, aspotential inhibitors of Bcrp1 and BCRP. Compounds areproduced by combinatorial synthesis in a collaborationwith A Van Loevezijn and GJ Koomen (University ofAllen JD, Brinkhuis RF, Wijnholds J, Schinkel AH. The mouseBcrp1/Mxr/Abcp gene: amplification and overexpression in celllines selected for resistance to topotecan, mitoxantrone or doxorubicin.Cancer Res 1999; 59: 4237-41.Huisman MT, Smit JW, Schinkel AH. Significance of P-glycoproteinfor the pharmacology and clinical use of HIV protease inhibitors.AIDS (in press).Jonker JW, Wagenaar E, Van Deemter L, Gottschlich R, BenderHM, Dasenbrock J, Schinkel AH. Role of blood-brain barrier P-glycoprotein in limiting brain accumulation and sedative sideeffectsof asimadoline, a peripherally acting analgaesic drug. Br JPharmacol 1999; 127: 43-50.Schuetz EG, Umbenhauer DR, Yasuda K, Brimer C, Relling MV,Schuetz JD, Schinkel AH. Altered expression of hepatic cytochromesP450 in mice deficient in one or more mdr1 genes. MolPharmacol 2000; 57: 188-97.Smit JW, Huisman MT, Van Tellingen O, Wiltshire HR, Schinkel AH.Absence or pharmacological blocking of placental P-glycoproteinprofoundly increases fetal drug exposure. J Clin Invest 1999; 104:1441-7.Van Asperen J, Van Tellingen O, Schinkel AH, Beijnen JH.Comparative pharmacokinetics of vinblastine after a 96-hour continuousinfusion in wild-type mice and mice lacking mdr1a P-glycoprotein.J Pharmacol Exp Ther 1999; 289: 329-33.Van Asperen J, Van Tellingen O, Tijssen F, Schinkel AH, BeijnenJH. Increased accumulation of doxorubicin and doxorubicinol incardiac tissue of mice lacking mdr1a P-glycoprotein. Br J Cancer1999; 79: 108-13.
Pharmacodynamicsof anticancer agentsJHM Schellens MD PhD Group leaderJH Beijnen PhD 1Academic staffAH Schinkel PhDAcademic staffM Maliepaard PhD 2Post-docRCAM Van Waardenburg PhD 3 Post-docLA De Jong 3TechnicianD Pluim 5TechnicianMA Van Gastelen 2TechnicianM BohlanderUndergraduate studentResistance to topoisomerase I inhibitors and mitoxantroneInvestigations into the mechanism of resistance in thehuman ovarian tumor cell lines IGROV1, T8 and MX3have revealed the presence of the Breast CancerResistance Protein (BCRP, also known as MXR andABCP). Topotecan and mitoxantrone were shown to betransported out of the cells very efficiently by this transporter.The level of resistance in a series of partiallyFigure VIII.4Northern blot of BCRP mRNA in parent IGROV1 and in resistantT8 and MX3 cell lines, including T8 revertant cell lines (upperpanel). Lower panel shows levels of resistance to SN-38 (▲),TPT (✚) and MX (●) in T8 lines passaged without drug (left), andin revertants re-exposed to drug (right). mRNA was isolated frompassages indicated with an arrow.reverted T8 cells correlated with the expression level ofBCRP (Figure VIII.4), strongly suggesting that BCRP hasa pivotal role in the development of resistance totopotecan and mitoxantrone in these tumor cells. Inattempts to circumvent this resistance, several potentialinhibitors for BCRP were tested. One of them,GF120918, a compound originally developed as aninhibitor of P-glycoprotein, was capable of completelyblocking the BCRP-mediated outward transport oftopotecan in the T8 and MX3 cells. By doing this, cellswere almost completely resensitized to topotecan andmitoxantrone. The resistance factor for topotecan in theT8 cell line decreased from 110 to 4.2 in the presence ofGF120918 and in the MX3 cells from 30 to 1.5.GF120918 appeared to be a very potent inhibitor ofBCRP, with maximum inhibition of topotecan cytotoxicityand transport present at concentrations as low as 100nM. This means that GF120918 is equally efficient ininhibiting P-gp and BCRP. Furthermore, we haveassessed the substrate characteristics of BCRP in detail.Several other registered topoisomerase I inhibitors appearto be transported by BCRP. However, a couple of experimentaltopoisomerase I drugs are hardly transported byBCRP, and could therefore be potentially useful incircumventing BCRP-related resistance. In collaborationwith Professor Scheper (Free University, Amsterdam), amonoclonal antibody was raised against BCRP. Furtherstudies focus on cellular distribution of BCRP andexpression in normal and tumor tissues.Interactions between platinum drugs and topoisomerase Iinhibitors 4Our laboratory previously reported a scheduledependent synergistic cytotoxicity of cisplatin (cDDP)followed by topoisomerase I (topI) inhibitors in varioushuman cancer cell lines (Ma et al., Cancer Chem.Pharmacol. 1998; 41: 307-16). The most active schedulewas addition of cDDP followed by the topI inhibitor. Thisschedule dependent synergistic cytotoxicity was alsofound for other platinum derivatives such as transplatin,carboplatin, oxaliplatin, lobaplatin and JM-216 in combinationwith various topI inhibitors (camptothecin (CPT),topotecan (TPT) and SN-28). In contrast, BCNU ormitomycin C (also DNA-adduct forming agents) in combinationwith CPT and TPT showed no synergy. The synergisticeffect appears to be platinum dependent. Thekinetics of the major intra-strand (AG- and GG-) adductswere only slightly affected by the topI inhibitor and couldnot explain the observed synergistic cytotoxicity. Usingthe ICT (in vivo complex of topoisomerase I)-assay weobserved that the amount of topI cleavable complexesincreases after incubation with cDDP, which could meanthat Pt-DNA damage facilitates topI interaction with DNA.The significance of this observation in relation to thesynergistic effect is currently investigated.To further investigate synergy between cDDP and CPT,we have used the yeast S. cerevisiae as a model. Wildtype, W303, (wt, repair proficient) cells and isogenic93EXPERIMENTAL THERAPY
94EXPERIMENTAL THERAPYmutants defective in nucleotide excision repair (rad4),mismatch correction (msh2) and double strand breakrepair (rad52) were used. All strains contain a plasmid foroverexpression of the topI gene to increase sensitivity forCPT, apart from the rad52 strain which was already 10times more sensitive for CPT than the topI overexpressingstrains. The cDDP survival curve showed theexpected pattern, i.e. the msh2 mutant was less sensitivefor cDDP compared to the wt, while the rad52 and therad4 mutants were highly cDDP sensitive.Combination experiments with cDDP followed by CPTshowed a synergistic effect at high doses in rad4 and wtstrains, indicating no involvement of the rad4 pathway insynergy. In contrast, the rad52 mutant showed a highlyantagonistic to additive effect, which was confirmed inthe rad4,rad52 double mutant. We conclude that therad52 pathway is required for synergy, while the nucleotideexcision and mismatch repair pathways are not.This indicates that homologous recombination plays animportant role, and its involvement is currently beinginvestigated.Pharmacodynamic endpoints in clinical studiesWe initiated a randomized phase I study in patients withadvanced non-small cell lung cancer to explore thetoxicities and maximum tolerated dose (MTD) of cisplatinplus gemcitabine given weekly or every two weeks.Gemcitabine is administered on day one and cisplatin onday two. The study has not yet reached its definedendpoints. The total number of patients entered is 35. Thebioanalytical, pharmacokinetic and pharmacodynamicresults reveal that there is a significant interaction betweengemcitabine and cisplatin. The clearance of unboundplatinum is significantly reduced with increasing doses ofgemcitabine. In addition, there appears to be a reductionof formation of platinum DNA-adducts in leukocytes bygemcitabine. The mechanism of the interaction and clinicalimplications are the subject of current investigations. TheDNA-adducts are being measured by a sensitive 32Ppostlabelingassay that we have developed and validated.Another phase I and pharmacologic study is ongoingto explore the maximum tolerated dose, dose-limitingtoxicities, pharmacokinetics and pharmacodynamics ofthe combination of carboplatin and topotecan. In thisstudy tumor biopsies are also taken during course one toquantitate the formation of platinum DNA adducts andtopo I activity and expression, by a catalytic activity assayand by Western blotting respectively. Levels will be correlatedwith levels in leukocytes and pharmacokineticparameters of both drugs as well as with toxicityendpoints.In another phase I and pharmacologic study a novelruthenium organic compound NAMI-A is being investigatedfor its toxicity and MTD. In this study the postlabelingassay is being used to quantitate ruthenium-DNAcomplexes in leukocytes. Preliminary results indicate thatruthenium forms DNA adducts, but to a much lowerextent than cisplatin and carboplatin.An HPLC assay with online radioisotope detection isbeing employed to support a recently initiated massbalance study with the novel disulphonamide anticanceragent E7070.Notes1 Also University Utrecht, Faculty of Pharmacy.2 Funding Dutch Cancer Society, Project <strong>NKI</strong> 99-2060.3 Funding Dutch Cancer Society, Project <strong>NKI</strong> 97-1440.4 Collaboration with J Brouwer, Department ofMolecular Genetics, University Leiden.5 Funding Dutch Cancer Society, Project <strong>NKI</strong> 95-1059.Publications: PharmacodynamicsDe Graaff M, Maliepaard M, Pluim D, Floot BGJ, Slaper-Cortenbach IC, Schellens JHM. In vitro antagonistic cytotoxicinteractions between platinum drugs and taxanes on bone marrowprogenitor cell CFU-GM. Anti-Cancer Drugs 1999; 10: 213-8.Maliepaard M, Van Gastelen MA, De Jong LA, Pluim D, VanWaardenburg RCAM, Ruevekamp-Helmers MC, Floot BGJ,Schellens JHM. Overexpression of the BCRP/MXR/ABCP gene ina topotecan-selected ovarian tumor cell line. Cancer Res 1999;59: 4559-63.Pluim D, Maliepaard M, Van Waardenburg RCAM, Beijnen JH,Schellens JHM. 32P-postlabeling assay for the quantification ofthe major platinum-DNA adducts. Anal Biochem 1999; 275: 30-8.LJ van ’t Veer PhDH Bartelink MD PhD 2, 5BR Pieters MDS Rodenhuis MD PhD 3, 6NS Russell MDFE Van Leeuwen PhD 1, 4A Broeks PhD 4AC Lambrechts PhD 6MAJ Van Dijk MSc 5AJ Bosma 6AN FlooreJN Ridderbos 5JHM Urbanus 4E Dahler 1, 4Molecular Pathology:Molecular markers ofbreast cancergroup leaderAcademic staffAcademic staffAcademic staffAcademic staffAcademic staffPost-docPost-docGraduate studentTechnicianTechnicianTechnicianTechnicianResearch assistent
ATM heterozygous germline mutations contribute to breastcancer susceptibility 4Approximately 0.5-1% of the general population hasbeen estimated to be heterozygous for a germlinemutation in the ataxia-telangiectasia mutated gene (ATM)and epidemiological studies have indicated that femaleheterozygous carriers have an excess risk of breastcancer (RR 3.9). The purpose of our study is todetermine the contribution of ATM heterozygosity to therisk of (radiation-induced) breast cancer. The frequency ofATM germline mutations is examined in high-risk breastcancer families, and in three case-control studies ofwomen who developed breast cancer subsequent toexposure to various levels of ionizing radiation: 1) breastcancer (n=250); 2) Hodgkin’s disease (n=200); 3)mammography (n=300). Using the protein truncation test(PTT) as the mutation detection method, followed bygenomic sequencing, we expect to have a mutationdetection sensitivity of approximately 75%. At present,material of more than half of our selected study participantshas been collected and analyzed.The results so far in our first case-control studyindicate that ATM heterozygotes have an increased riskof developing a type of breast cancer characterized byfrequent bilateral occurrence, early age at onset andlong-term survival (approximate RR 9). In addition, allpatients had received radiation for their first breast tumorand a trend was noted towards a higher incidence ofATM mutations for women with bilateral breast cancer(5/58 bilateral versus 4/175 unilateral breast cancerpatients). This suggests that radiation might indeed be aninduction trigger and warrants further investigation intothe role of ATM heterozygosity in the pathogenesis ofradiogenic cancers.Long-term survivors of Hodgkin’s disease whoreceived mantle-field irradiation at a young age have astrong increased risk of developing breast cancer. In thesecond case-control study we concluded that ‘diseasecausing’ ATM germline mutations, however, are not amajor component underlying this increased risk (32 casestested). We did detect several alternative splicing eventswhich might influence protein expression levels.Functional activity of the human estrogen receptor inprimary breast cancer and normal breast tissue 5The positive immunohistochemical staining of theestrogen receptor alpha (hER) in fifty to sixty percent ofall breast cancers correlates with a better prognosiswhen patients are treated with anti-estrogens (e.g.tamoxifen). However, a substantial proportion (40%) ofthese patients does not respond to tamoxifen therapy.Variant estrogen receptors (non-functional, dominantactiveor dominant-negative receptors) cannot be discriminatedwith the routinely used immunohistochemicalmethods and might be responsible for this phenomenon.The aim of this project is to evaluate the functionalactivity of hER in breast carcinogenesis and to correlatethe functional activity of hER with clinical response andrecurrence-free/overall survival of patients treated withtamoxifen.We developed a functional assay in yeast (hER-FASAY)that can quantitatively detect the presence of hERvariants with an aberrant functional activity amongnormal, wild-type hER in a tissue specimen. We foundthat the presence of wild-type hER, relative to the totalamount of hER present, differs markedly (P
96EXPERIMENTAL THERAPYcancer tissues, from blood of healthy volunteers and frombone marrow of control individuals. Comparison of thesethree expression profiles resulted in the identification of arange of genes that were expressed in breast cancer, butwere absent in the profiles of blood or bone marrow cells.The relative expression levels of 30 of these genes werestudied by semi-quantitative RT-PCR. For twelve of thesepotential marker genes higher mRNA expression levelswere found in peripheral blood mononuclear cells (PBMC)of patients with metastatic breast cancer than in PBMCsof healthy volunteers. As an example, one of these genes(pS2) was subsequently tested by real-time quantitativePCR on 50 PBMCs of patients with metastatic breastcancer and on 50 PBMCs of healthy volunteers. The pS2expression was significantly higher in PBMCs of patientswith breast cancer than in PBMCs of healthy volunteers(p=0.038). The results indicate that SAGE analysis has theability to identify suitable genes for detection of minimalresidual disease in breast cancer patients. pS2 is the firstexample resulting from this selection process.Notes1 Division XII.2 Division IX.3 Division X.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1430.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1268.6 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1468.Publications: Molecular markers of breastcancerBartelink H, Begg AC, Coco Martin J, Van Dijk M, Van ‘t Veer L,Van de Vaart P, Verheij M. Towards prediction and modulation oftreatment response. Radiotherapy and Oncology 1999; 50, 1-11.Broeks A, Russell NS, Urbanus JHM, Dahler EC, Van ‘t Veer MB,Hagenbeek A, Noordijk EM, Crommelin MA, Van Leeuwen FE.Van ‘t Veer LJ. Increased risk of breast cancer following irradiationof Hodgkin’s disease is not a result of ATM germline mutations. IntJ Rad Biol 1999 (in press).Broeks A, Urbanus JHM, Floore AN, Dahler EC, Klijn JGM,Rutgers EJTh, Devilee P, Russell NS, Van Leeuwen FE, Van ‘t VeerLJ. ATM heterozygous germline mutations contribute to breastcancer susceptibility. Am J Hum Genet 1999 (in press).Laake K, Launonen V, Niederacher D, Gudlaugsdottir S, Seitz S,Rio P, Champème MH, Bièche I, Birnbaum D, White G, Sztan M,Sever N, Plummer S, Osorio A, Broeks A, Huusko P, Spurr N,Borg A, Cleton-Jansen AM, Van ‘t Veer L, Benitez J, Casey G,Peterlin B, Olah E, Varley J, Bignon YJ, Scherneck S,Sigurdardottir V, Lidereau R, Eyfjord J, Beckmann MW, WinqvistR, Skovlund E, Børresen-Dale AL and the Breast Cancer SomaticGenetics Consortium. Loss of heterozygosity at 11q23.1 and survivalin breast cancer; Results of a large European study. Gen ChrCancer 1999; 25: 212-21.Lambrechts AC, Bosma AJ, Klaver SG, Top B, Perebolte L, Van ‘tVeer LJ, Rodenhuis S. Comparison of immunocytochemistry,reverse transcriptase polymerase chain reaction and nucleic acidsequence-based amplification for the detection of circulating breastcancer cells. Breast Cancer Res Tr 1999; 56: 219-31.Van Dijk MAJ, Hart AAM, Van ’t Veer LJ. Differences in estrogenreceptor alpha variant messenger RNAs between normal humanbreast tissue and primary breast carcinomas. Cancer Res (in press).MJ Van de Vijver MD PhDH Bartelink MD PhD 1JL Peterse MD 2E Robanus Maandag PhD 3I Faneyte MDC BoschP KristelMolecular analysis ofbreast cancerGroup leaderAcademic staffAcademic staffPost-docGraduate studentTechnicianTechnicianMultidrug resistance related proteins in breast cancerMany breast cancer patients die of metastasizeddisease that is unresponsive to cytotoxic treatment. Themechanisms causing drug resistance are unknown, andno good parameters are available to predict success oftreatment. In vitro studies have shown the involvement ofATP binding cassette proteins in multidrug resistance.ABC proteins are over-expressed in MDR cells and theirencoding genes, transfected into drug sensitive cells,confer the same MDR phenotype. Although it is clear thatABC proteins play a role in the physiologic defense againsttoxic compounds, it is as yet unresolved whether they arealso involved in clinical drug resistance of breast cancer.To answer this question we have first validated a methodto measure the ABC expression. With several RNA basedtechniques (RNase protection, semi-quantitative RT-PCR,Northern blot) we detected varying levels of expression ofMultidrug Resisitance (associated) Protein (MRP)1, MRP2and MRP3 in breast cancer cell lines and tumor samples.Immunohistochemical detection of these proteins waspossible in the cell lines and samples that over-expressedthe encoding RNA at least two-fold, relative to that of ahousekeeping gene. The P-glycoprotein gene MDR1 wasnot detected in breast cancer cell lines, whereas theexpression in tumor samples could be attributed tolymphocytes and macrophages. We conclude that it isunlikely that MDR1/P-Gp is involved in drug resistance inbreast cancer. The possible role of the other ABC proteinswill be investigated by comparing the expression of theseproteins with response to chemotherapy.
97Genetic alterations in ductal carcinoma in situ and invasivecarcinoma of the breastIn a previous project (see Division XIII) we haveanalyzed the genetic alterations in ductal and lobularcarcinoma in situ of the breast. This study revealed thatthe spectrum of genetic alterations in the in situ tumorsis comparable to that of the invasive carcinomas.However, the frequencies of the individual genetic alterationsdiffered significantly between the two tumorcategories. As most invasive carcinomas also contain anin situ component, we want to compare the geneticalterations in both components of the same tumor and,in this way, identify the genetic alterations that areinvolved in the progression from the in situ to the invasivestage. Of two invasive breast carcinomas with a relativelylarge in situ component, we have microdissected theinvasive and adjacent in situ component, isolated DNAand performed comparative genomic hybridization. Thesepilot experiments showed only minor differences betweenthe two components, suggesting that the number ofgenetic alterations involved in breast tumor progression islow. A larger group of invasive breast carcinomas with anin situ component is now being analyzed.EXPERIMENTAL THERAPYNotes1 Division IX.2 Division XIII.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 1998-1798.Secretary Division of Experimental TherapyTEA EggenhuizenResearch staff positions (full time equivalents)Scientific permanent: 4.0Scientific project: 15.2Technical permanent: 10.5Technical project: 13.0
98IX Division of RadiotherapyDivision head H BartelinkHeadH Bartelink MD PhDPermanent academic staffBMP Aleman MD, JSA Belderbos MD,JH Borger MD PhD, IAD Bruinvis PhD, EMF Damen PhD,RW De Boer PhD, LGH Dewit MD PhD, RLM Haas MD,AAM Hart MSc, RB Keus MD, JV Lebesque MD PhD,EAH Masselink MD, BJ Mijnheer PhD, AWH Minken PhD,LMF Moonen MD PhD, NS Russell MD, JG Salverda MD,BNFM Van Bunningen MD, M Van Herk PhD,FW Wittkämper PhDOther academic staffLJ Boersma MD PhD, L Bos PhD,K De Jaeger MD MSc, N Dekker MSc,M Engelsman MSc, W Heemsbergen MSc,FJP Hoebers MD, M Hoogeman PhD,CW Hurkmans MSc, EPM Jansen MD, R Louwe PhD,GJ Meijer MSc, F Ong MD PhD, BR Pieters MD,LAJ Ploeger MSc, CRN Rasch MD, P Remeijer PhD,A Saarnak PhD, Y Seppenwoolde MSc, CJA Tissing MD,JF Ubbels MD, M Verheij MD PhD, C Vrieling MDPermanent technical staffTJ Minderhoud, PJH Van de VenOther technical staffJ De Goede, P Filius, C Goedbloed, E Kalkman, P Muller,MHP Smitsmans, B Smulders, H Uiterwaal, L ZijpGuestsA OlszewskaO TörzsökSecretaryD BrandwijkE HofmannResearch funded positions (full time equivalents)Clinical permanent: 3.5Clinical project: 14.3Technical permanent: 4.4Technical project: 6.3IntroductionDuring 1999 progress has been made in the implementationof research findings in the clinic. At the sametime, fundamental research inspired by clinical observationsof staff members is carried out in close cooperationwith other research divisions. A typical example of applicationof research activities in clinical studies is a phaseIII randomized clinical trial in prostate cancer patients. Inthis trial sophisticated conformal radiation techniques areused to escalate the radiation dose to the prostate inorder to improve both local cure and survival in thesepatients. This approach became possible through theinput of the different research groups and by applyingsophisticated image registration techniques. Thetreatment plan for individual patients is designed byapplying treatment optimization procedures. This plan isexecuted by meticulous irradiation procedures, with amultileaf collimator on the linear accelerator, and accompaniedby intensive quality assurance with dosimetry andmegavoltage imaging. The results of this work have alsomade the application of this approach possible inpatients with head and neck or lung cancer.Other studies in patients with breast cancer have ledto a better insight into possibilities of reducing the sideeffects of irradiation and have led to the development ofimproved treatment approaches.This year was also characterized by an increasedintegration of the research activities into multidisciplinaryprojects. Epidemiological studies are ongoing to assessthe risk of second cancers after radiotherapy and thepossible contribution of ATM germ line mutations in theinduction of breast cancer (see Division XII). Preliminaryresults of the investigation of genetic alterations involvedin local recurrence and progression of invasive breastcancer and in situ ductal cancer after breast conservingtherapy are reported by Division XIII. The observedimproved local cure from adjuvant hormonotherapy withradiotherapy for patients with locally advanced breastcancer has lead to a joint investigation with Division VIIIinto the link between estrogen receptor b and tumorprogression under tamoxifen treatment.Previous results have demonstrated improved localcure and survival in lung cancer patients treated withconcomitant cisplatin and irradiation (Schaake Koning et
al. NEJM 1992; 327: 432-3). Our results have now beenconfirmed in various USA trials for patients with cervicalcancer. More optimal use of this combined chemo-radiotherapyapproach seems to be possible since our resultsshow that cisplatin-sensitive patients can be identifiedusing specific markers. Another successful approachappears to be increasing the tumor concentration ofcisplatin by giving this drug intra-arterially (i.a.). Animpressive local cure rate has been observed for patientswith advanced tumors of the head and neck regiontreated with i.a. cisplatin plus radiotherapy.Studies are on going in cooperation with Division VIIIon the role of endothelial cell and vascular damage inkidney pathogenesis after radiation, with emphasis onmechanisms and possible ways to ameliorate damage.Further collaboration with Division VIII can be seen inprojects on the use of fluorescence in situ hybridization(FISH) for detecting radiation-induced chromosomedamage, both for estimating intrinsic radiosensitivity oftumor cells (using human tumor biopsies) and inpredicting normal tissue morbidity (using peripheral bloodlymphocytes).Interesting results emerged from our work on influencingapoptosis by inhibiting the MAPK pathway whileinitiating pro-apoptotic signals through the SAPK/JNKcascade. The experiments show that alkyl-lysophospholipidsincreased apoptosis in a wide variety of tumor cellswhile normal tissue cells remain unaffected. In patientswith bladder cancer, it was found that low base-lineapoptotic index and over-expression of cyclin D1 wascorrelated with a poor local cure after irradiation.Three co-workers of the division successfully defendedtheir theses this year and the ESTRO Varian Award for1999 was presented to Conny Vrieling for her investigationinto the dose-effect relationships in patients withearly breast cancer with regard to the cosmetic result.Joos Lebesque was presented with the Glyn Evans Medalat the Annual Scientific Meeting of the Royal College ofRadiologists, London for his lecture on conformal radiotherapyof prostate cancer in clinical practice. HarryBartelink received the Marion Burgers Memorial Award for1999 from the Egyptian Cancer Society.Future directionsThe clinical research is directed towards escalation ofthe radiation dose in patients with prostate or lungcancer. This will involve newly designed radiotherapytechniques with radiation dose-intensity modulation.Optimal use will be made of the increasing knowledge ofnormal tissue tolerance, for example lung tolerance,movement of organs during radiotherapy and improvedtumor delineation. Reduction of the impact of organmovement which can enlarge the irradiated volume willbe attempted by the so called ABC machine, whichcontrols the breathing of the patient during radiotherapy.Some of these treatments will be carried out in combinationwith systemic treatment in order to increase thelocal tumor cell killing effect of radiotherapy. In closecollaboration with the Radiology Department, newmethods of 3-dimensional delineation of the tumor will betested in breast cancer patients who underwent MRIexamination and will undergo tumorectomy followed bybreast conserving therapy.The physics research is directed at providing newmethods of target volume delineation, new approaches indelivering intensity-modulated beams to patients andimproving accurate dose delivery. Both static anddynamic methods of modifying beam intensity will beexplored using various methods of verifying both patientposition and beam intensity. Better knowledge of thetarget volume position during treatment and the incorporationof geometrical uncertainties into the treatmentmargin will further enhance the potential advantages ofthese intensity-modulated beams in the clinic. Dosecalculations will be improved and verified to assureadequate target coverage with these high dose-highprecision treatment techniques.Image acquisition and processingR De Boer, N Dekker, P Filius, S Muller 1 , BJ Mijnheer,AR Peters, LS Ploeger, C Rasch 2 , P Remeijer 2 ,MHP Smitsmans, AJ Van Dalen, PJH Van de Ven,RE Vijlbrief, L Zijp, H Bartelink, KGA Gilhuijs 1 ,JV Lebesque, M Van HerkEPID application for intensity modulated radiotherapy(IMRT)A first version of a field shape verification system fordynamic therapy was completed. In the matrix ionizationchamber electronic portal imaging device (EPID), eachscan line is recorded at a slightly different time due to thescanning readout. This means that the position of, forinstance, a moving diaphragm, will appear in differentpositions for each line of the image. To verify the positionof irradiated objects, the percentage integrated monitorunit (IMU) signal available from the accelerator is digitizedonce for each scan line and stored with the image. Afilter was developed to compensate for the lag and theslow update rate of the IMU signal. Rendering softwarewas developed to obtain the expected (reference) shapeof the field outline on the EPID images. The dynamicMLC prescriptions are accepted both in Elekta andDICOM formats. Comparing the reference and measuredfield outlines demonstrated both random leaf positionerrors (about 1 mm standard deviation at 6 mm/s at theisocenter) and a significant lag in the position of theleaves. The lag corresponds with a delay of about 0.6 s,and it is partly explained by the lag of the IMU signalwhich is used to drive the collimator. In cooperation withthe Royal Marsden Hospital, London, the feasibility of anumber of commercial EPID systems was compared forverification of intensity modulated beam delivery. Thepreliminary results showed that the accuracy was similarfor all systems.99RADIOTHERAPY
100RADIOTHERAPYPatient setup errors: 3-D setup analysis for parotid glandtumorsTwenty-eight patients were treated for parotid glandtumors with two oblique beams. Orthogonal localizationimages were used to determine setup deviations. Theimages were analyzed with a conventional 2-D registrationtechnique and a true 3-D technique which usesCT data to determine patient displacement. For bothtechniques, standard deviations of the systematic andrandom translations along the three principal axes (leftright,cranial-caudal and anterior-posterior) were determined.The 3-D technique also quantified the rotationsaround the three axes. To determine the accuracy of the2-D registration technique for various rotation angles, thedifferences between translations determined using 2-Dand 3-D registration techniques were analyzed as afunction of 3-D rotations. The standard deviations of thesystematic and random translations along the threeprincipal axes varied between 1.5 and 2.3 mm. Theoverall mean translations deviated significantly from zeroin the left-right direction (0.8 mm) and the anteriorposteriordirection (-1.2 mm). The standard deviations ofthe systematic and random rotations were about 1degree. The overall rotations did not deviate significantlyfrom zero. Surprisingly, the rotations are larger than thosefound in an earlier study for prostate patients, eventhough we do not apply any fixation of the prostatepatients whereas this is the case for parotid glandpatients. No correlation was found between the 2-D - 3-D translational differences and the rotation magnitude,which indicates that rotations do not systematicallyinfluence the measurement of the translations in 2-D.However, the variability of the 2-D - 3-D translation differencesincreased with larger rotation magnitudes. Thisfinding demonstrates that the registration errors in 2-Dbecome larger for large rotations.directions), which is not taken into account in the TREequation. A simulation of marker matching with anisotropyin the errors confirmed this finding. With four re-appliedmarkers, the TRE is ≤ 6 mm in most regions of the head.Image registration methods and application: clinicalimplementationAn improved delineation tool has been developed forincorporation of two or more registered scans intotreatment planning. The tool is based on concurrentprocessing, which means, for example, that each manualdelineation of multiple image modalities on a CT displayoccurs simultaneously with the MRI display, and viceversa.A prototype of this system is shown in Fig IX.1.The tool can handle up to 10 scans simultaneously.There are two main challenges in this software. The firstone is to keep the 10 images synchronized, for whichspecial automated data management software wasdeveloped. The second challenge was to maintain thetransformation matrices involved with the differentcoordinate systems. For this purpose a softwarecomponent was developed that automatically maintains amatrix of NxN coordinate systems and all associatedtransformation parameters, thus simplifying the extensionof the number of scans. This system is in experimentaluse for clinical problems such as measurement of fasttumor growth (Fig IX.1) and the assessment of recur-Image registration methods and application: markermatchingWe investigated the accuracy of 3-D matching usingmarkers that are repeatedly applied to external anatomicallandmarks on the head. The purpose of this study is toestablish a lower limit of the errors that would occur in,for instance, MRI-SPECT matching, which can,sometimes, only be achieved using external landmarks.Marker matching was compared with (single modality)volume matching for 20 MRI scans using several markercombinations. The results were compared with apublished expression for the Target Registration Error(TRE), which gives the 3D distribution of the mismatchbetween both scans. The main error source was identifiedas reapplication of the markers on the anatomicallandmarks. The theoretical expressions describe therelative distribution of the TRE in space, but tend tounderestimate the actual registration error. This deviationis due to anisotropy of the marker position errors (theerror of the marker position in the direction perpendicularto the skin surface is much smaller than the error in otherFigure IX.1A prototype delineation tool, developed at the <strong>NKI</strong>, for multipleimage modalities. Scan 1 shows a zoomed part of a planningCT scan of a brain tumor patient. Scans 2 and 3 show matchedand resampled MRI scans. In this particular patient, fast tumorprogression was observed on a diagnostic CT scan (4). This toolallows instantaneous delineation on any of these scans. Actionsperformed on any display are reflected in real time in all otherdisplays: such as slicing, zooming and panning. In this particularcase, the planning CT delineated edema region (black) andtumor margins (white) are smaller than the corresponding regionon the diagnostic CT scan. On Scan 5 the high dose region ofthe planned dose distribution is the bright area. Since the edgeof the edema was closely approaching the edge of the highdose region, the treatment fields were enlarged. Scan 6 containsthe paint tool used to delineate the tumor.
ences, and also in an evaluation study in which helicalCT scans made in different phases of the breathing cycleare compared with each other and with PET data whichallows separation of active tumor tissue from othertissues (see also Division XIII).Notes1 Division XIII.2 Funding Dutch Cancer Society, Project <strong>NKI</strong> 96-1308.Dose calculationJ Venselaar 1 , BJ MijnheerNew formalisms, for monitor unit calculation for radiationtreatments with photon beams from accelerators and 60 Counits,have been developed by ESTRO and a workinggroup of the Netherlands Commission in RadiationDosimetry (NCS). Both formalisms apply a coherent systemfor the use of scatter correction factors for dose calculationson the central axis of arbitrarily-shaped photonbeams. The system is suitable for application in both thefixed source-surface distance (SSD) and in the isocentrictreatment setup. In order to derive the relations in theformalism, we introduced a separation of the phenomenarelated to the energy fluence in air and to the phantomscatter contributions to the dose. It was shown that dosecalculations can be performed with only one set of basicbeam data, obtained at the reference depth of 10 cm.Problems related to measurements performed at the depthof maximum absorbed dose, due to the electron contaminationof the beam, are avoided in this way. Dose calculationsin a fixed SSD treatment set-up are straightforward.Application in the isocentric treatment setup needs simpleconversion steps, while the inverse approach, fromisocentric to fixed SSD, is also described.The new formalism requires collimator and phantomscatter correction factors, S c and S p, defined at thereference depth of 10 cm. These data can be obtainedfrom measurements at that depth in a mini-phantom andin a full scatter phantom. Equations have been derived,giving the relation between these quantities and correspondingquantities obtained from measurements at thedepth of dose maximum. It was shown that conversionof S c and S p determined at 10 cm depth to quantitiesdefined at dose maximum such as (normalized) peakscatter factor, (N)PSF, (normalized) tissue-air ratio,(N)TAR, and vice versa is not possible without quantitativeknowledge of the electron contamination. The differencein S c at d max resulting from this electron contaminationcompared with S c values obtained at a depth of10 cm in a mini-phantom has been determined as amultiplication factor, S cel, for a number of photon beamsof different accelerator types. Figure IX.2 shows that S celmay vary up to 5%. In the new formalisms, outputfactors are defined at a reference depth of 10 cm,therefore they do not require S cel data. The use of S c andS p values, defined at 10 cm depth, in combination withrelative depth-dose data or tissue-phantom ratios istherefore recommended. For a transition period, the useof the new equations and S cel data might be required if,for instance, treatment planning systems apply S c datanormalized at d max.Note1 Dr Bernard Verbeeten Instituut, Tilburg.101RADIOTHERAPYExperimental dosimetryL Bos 1 , M Engelsman 2 , JH Lanson 3 , G Laureijs 1 ,R Louwe 4 , N Raaijmakers 5 , H Uiterwaal, K Van Ingen 2 ,FW Wittkämper, BJ Mijnheer, M Van HerkFigure IX.2Experimentally determined values of S cel(v c,d max) for fourdifferent photon beam qualities ranging from 60 Co to 25 MV.For measurements at d ref, S cel(v c,d ref) by definition equalsunity.In vivo dosimetryConformal radiotherapy requires accurate knowledgeof the actual dose delivered to a patient. The impact ofroutine in vivo dosimetry has been analyzed for threeconformal treatment techniques to evaluate its usefulnessin daily clinical practice. Based on pilot studies, routine invivo dosimetry quality control (QC) protocols were implementedin the clinic. Entrance and exit diode dosemeasurements have been performed during twotreatment sessions for 378 patients having prostate,bladder and parotid gland tumors. Dose calculationswere performed with a CT-based three-dimensionaltreatment planning system. In our QC-protocol weapplied action levels of 2.5% for the prostate and bladder
102RADIOTHERAPYtumor group and 4.0% for the parotid gland patients.When the difference between the measured dose at thedose specification point and the prescribed doseexceeded the action level, the deviation was investigatedand the number of monitor units (MUs) adjusted. For 34(9%) patients the difference between the measured andcalculated dose was larger than the action level.Systematic errors in the use of a new software release ofthe monitor unit calculation program, limitations of thedose calculation algorithms, errors in the planningprocedure and instability in the performance of theaccelerator have been detected. It can be concluded thataccurate in vivo dosimetry, using a diode measurementsystem, is a powerful tool to trace dosimetric errorsduring conformal radiotherapy in the range of 2.5-10%,provided that the system is carefully calibrated. Theimplementation of an intensive in vivo dosimetry programrequires additional staff for measurements and evaluation.The patient measurements add only a few minutes to thetotal treatment time per patient and guarantee anaccurate dose delivery, which is a prerequisite forconformal radiotherapy.Transmission dosimetrySeveral groups have presented procedures to useelectronic portal imaging devices for in vivo dosimetry.We developed methods to determine transmission, exitand mid-plane dose distributions from portal imagesacquired with a liquid-filled electronic portal imagingdevice (EPID). Recently, a PC-based software systemwas developed for bringing portal in vivo dosimetry intofull-scale clinical use. The implementation consists ofcomputation modules written in C and a user interfacewritten in Delphi. The following components have beenincorporated: database and treatment planning system(TPS) integration, acquisition software, dose reconstructionalgorithms and evaluation tools. The programwas tested for a variety of combinations of inputparameters and calibration data which resulted in anumber of modifications. The intercomparison of filmdosimetry and EPID dosimetry for phantoms has alsobeen made possible. One complication is that the filmsand the EPID measurements often refer to differentplanes in space. For this reason, the dose planes are firstmatched with the patient’s CT data in those planes andthen compared in a three-dimensional grid. Phantommeasurements are in progress and will be used tocompare EPID dose distributions with ionization chamberand film measurements. Recently, a start has been madewith the clinical use of the system for the measurementof midplane dose distributions during radiotherapy of thebreast. The purpose of this study is to evaluate theoccurrence and magnitude of dose inhomogeneities.Dosimetry of intensity-modulated beamsConformal radiotherapy of lung tumors can beperformed in various ways, including the use of intensitymodulatedbeams (IMRT). In order to assess the limitationsin the design of new techniques for IMRT of lungtumors, it is necessary to quantify the errors made bydose calculation algorithms currently available incommercial treatment planning systems (TPS). Both theabsolute dose at the ICRU dose specification point andrelative dose distributions were therefore assessed for asimple beam setup. Film and ionization chambermeasurements were performed in an inhomogeneouspolystyrene and cork layered phantom, with a sphericallyshaped polystyrene insertion simulating a tumor inside alung. Single non-wedged conformal beams of differentenergies, shaped by a multi-leaf collimator, were usedand measurements were compared with calculationsusing various treatment planning systems with differentinhomogeneity correction algorithms. For this specificconfiguration, the dose calculation at the dose specificationpoint, i.e. the monitor unit calculation, has a systematicuncertainty smaller than a few percent dependingon field size, beam energy and dose calculationsalgorithm. Underestimation of the penumbra width mayoccur, depending on the algorithm used in a particularTPS, leading to an underdosage of the Planning TargetVolume, PTV, up to about 20%. It can therefore beconcluded that algorithms used for monitor unit calculationsin lung cancer treatments have acceptable accuracyif the non-wedged fields are not too small. However,these algorithms do not yet take into account the lateralelectron transport in low density material like lung tissue.This limitation will lead to unaccepable errors whenchoosing field sizes for conformal treatments particularlyfor high photon energies.An important tool for the verification of newly designedIMRT techniques is film dosimetry using a stack of filmsin specific phantoms. In order to determine the accuracyof dose determinations using radiographic film, weevaluated the reproducibility of two types of dosimetricfilms, TVS (CEA) and X-Omat V (Kodak). For the formertype of film, we found a large intra-institutional variabilityof the sensitometric curve, in contrast to other studiesevaluating the same type of film. This large variability isprobably related to ageing of the film, in combination witha rather long period of analysis. The inter-institutionalvariability for the TVS (CEA) films was smaller than theintra-institutional variability, but markedly higher than theinter-institutional variability of the X-Omat V (Kodak) films.We concluded that the sensitometric curves of CEA filmsmust be determined regularly in order to performaccurate film dosimetry. The sensitometric curves ofKodak films show less variability, which reduces the needfor regular verification.Boron neutron capture therapyConsistent dosimetry is a requirement for themeaningful comparison of the results of treatment byboron neutron capture therapy (BNCT). Internationalrecommendations currently available for conventionalphoton and electron beam dosimetry and for fast neutrontherapy are not applicable to BNCT. An EC project was
therefore started to draft a Code of Practice for theDosimetry of BNCT. An important problem with thestandardization of dosimetric procedures is whichphantom material is most suitable for the dosimetryunder reference conditions of neutron beams for BNCT.For this purpose, phantoms of various dimensions,composed of water, tissue-equivalent (TE) liquid,polyethylene (PE), polymethyl-metacrylate (PMMA) andwater containing 10 B were irradiated using the PettenBNCT beam. Activation foils and a diode detector wereused for the determination of the thermal neutron fluencerate. The gamma-ray dose rate and the fast neutrondose rate were determined using paired ionizationchambers. In water, PMMA and TE-liquid, the absolutedose and fluence values agreed within 3% at thereference depth, with the exception of the gamma-raydose rate in PMMA which was 12% lower than in water.Due to a higher hydrogen concentration in PE comparedwith water, the dose and fluence values in PE differedmore than 30% from those in water. Only minor differenceswere observed between the percentage depthdose curves for the various dose components in water,PMMA and TE-liquid. The addition of clinically relevantamounts of 10 B to water resulted in a considerabledecrease in the absolute thermal neutron fluence and adecreased penetration of thermal neutrons. For referencedosimetry of an epithermal neutron beam for BNCT bothwater and TE-liquid are suitable phantom materials. Forpractical reasons, water is therefore proposed asreference phantom material. For measurements requiringa solid phantom, PMMA is recommended.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 96-1302.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1831.3 Medisch Centrum Alkmaar.4 Funding: Foundation for Technical Sciences, ProjectBGN 33.3240.5 University Medical Center, Utrecht.Treatment planningJSA Belderbos, JH Borger, K De Jaeger, BA Fraas 1 ,CW Hurkmans, JV Lebesque, DL McShan 1 ,TJ Minderhoud, BR Pieters, AE Saarnak, BS Smulders,MJ Steggerda, IAD Bruinvis, EMF Damen, BJ MijnheerDose and monitor unit calculationThe use of multi-segment techniques for irradiation ofadvanced head and neck cancer and prostate cancerinitiated the development of a more accurate beamdescription in the treatment planning system and of newmethods to calculate monitor units for highly asymmetricfields. For the 6 and 8 MV beams of our accelerators,the parameters of the photon beam model in thetreatment planning system have been refitted withemphasis on asymmetric fields. This procedure resultedin excellent agreement between measured and calculateddose profiles for wedged and open fields for bothsymmetric and asymmetric fields (including fields withoffsets larger than half the field size). To accuratelycalculate monitor units for asymmetric fields, correctionfactors depending on field size and offset were measuredand incorporated into the monitor unit calculationprogram. As a result of these modifications, the relativeand absolute dose calculation is accurate to within 2%for all open and wedged fields, including highlyasymmetric fields.Lung cancerTreatment planning for inoperable NSCLC patients wasconsiderably refined by allowing up to six beams and anon-coplanar beam set-up. In addition, small beamsegments are allowed to compensate the higher beamattenuation in the mediastinum. In the dose escalationstudy the patients are classified into five groupsaccording to the calculated mean lung dose. Thephysical 3-D dose distribution of the complete treatment(i.e. including the dose contribution of fields used forelectronic portal imaging) is converted to a biologicallyequivalent dose distribution given in fractions of 2 Gyusing the Normalized Total Dose (NTD) concept with anα/β-ratio of 3 Gy. The mean (biologically equivalent) lungdose, NTD mean, is subsequently calculated for the lungsas one organ. The final treatment plan should fulfill strictcriteria with respect to coverage of the Planning TargetVolume (PTV), and total biologically equivalent dose tospinal cord, heart, and esophagus.Breast cancerIn order to minimize the lung dose and to reduce thedose to the heart, a new irradiation technique for internalmammary node (IM) irradiation of breast cancer patientswas developed. In the improved technique, an obliqueelectron and an oblique asymmetric photon field arecombined to irradiate the IM lymph nodes. Three-dimensionaltreatment planning was performed for 8 patientsfor the standard and the new technique. Dose volumehistograms and normal tissue complication probabilitieswere compared. Better IM planning target coverage wasseen for the improved technique. The heart generallyreceived less dose with the improved technique and asmall, but acceptable, increase in lung dose wasoccasionally found. In order to determine the mostaccurate and efficient localization procedure of the IMnodes, lymphoscintigraphy, ultrasound, and CT-scan arebeing evaluated in a study group of 40 patients.Note1 University of Michigan, Ann Arbor, USA.103RADIOTHERAPY
104RADIOTHERAPYStudies of radiation response in normaltissueP Baas 1 , K De Jaeger 2 , C Goedbloed 2 , E Kalkman 3 ,SH Muller 4 , Y Seppenwoolde 2 , JCM Theuws 3 ,J Belderbos, LJ Boersma, JV LebesqueLocal dose-effect relations were determined by usingSingle Photon Emission Computed Tomography (SPECT)lung perfusion and ventilation scans matched with theaccompanying CT scans for patients with breast cancer,malignant lymphoma and non-small cell lung cancer(NSCLC). Normalized dose-effect relations for perfusionand air-filled fraction were calculated (at 3 months followup)for different patient subgroups and different regions inthe lung. The changes in perfusion as a function of dosewere less for all NSCLC-patients than the changes forpatients with healthy lungs, especially above 50 Gy.However, for the air-filled fraction, no deviation from thepreviously derived dose-effect relation for healthy lungtissue could be seen. When the group was divided intopatients with and without reduced perfusion adjacent tothe tumor, the group with homogeneous perfusion beforeradiotherapy showed greater changes in lung perfusionthan the group with reduced perfusion adjacent to thetumor. Average dose-effect relations for well and poorlyperfused regions of the lung (DE wp and DE pp) are shownin Figure IX.3. For the well-perfused lung regions therewas a steeper dose-effect relation than for the poorlyperfused areas; these last regions show a more chaoticdose response while in the lower dose bins somefunctional recovery could be observed (re-perfusion). Forthe reference group (lymphoma and breast cancerpatients), there was no difference in response for the welland poorly perfused lung regions. For the air-filled fractionno significant differences in dose response could beobserved between the patient subgroups and thedifferent regions of the lungs. To obtain a dose-effectrelation, valid up to 80 Gy, we extended the data of thereference group (lymphoma and breast cancer patients)with the data of the well-perfused parts of the lungs ofthe patients with NSCLC. This dose-effect relation couldbe described by a logistic fit with a D 50 of 63 ± 3 Gy anda steepness parameter k of 1.7 ± 0.2.For patients with breast cancer and malignantlymphoma we saw a recovery in local function (perfusionand ventilation) and air-filled fraction when we compareddose-effect relations measured at 3 and 18 months afterthe start of radiotherapy, with no further recovery from 18to 48 months. The recovery from radiation inducedchanges in ventilation and air-filled fraction was similar forbreast cancer and lymphoma patients, but lymphomapatients showed more recovery in perfusion. Regionaldifferences in radiosensitivity were not present, except forthe dorsal versus ventral region, which was attributed toa gravity-related effect in the measuring procedure.Notes1 Division X.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2043.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 94-819.4 Division XIII.Conformal radiotherapyJSA Belderbos, LJ Boersma, JJP De Goede,K De Jaeger 1 , WD Heemsbergen, M Hoogeman 2 ,P Koper 2 , EA Lamers, GJ Meijer, BJ Mijnheer, P Muller 2 ,C Rasch, Y Seppenwoolde 3 , BS Smulders, M Van Herk,HP Vijlbrief, D Yan 4 , IAD Bruinvis, JV LebesqueConformal radiation therapy (CRT) aims at increasingthe dose to the target volume and/or decreasing theirradiated volumes of normal tissue. CRT is being used inPhase II and III studies to investigate the impact ofdelivering higher tumor doses on local control andsurvival. In 1999, 90 prostate, 12 head and neck, 20parotid gland, 12 bladder and 38 lung CRT treatmentswere done.Figure IX.3The average dose-effect relation for well perfused lung regions,DEwp (triangles) and the average dose-effect relation for poorlyperfused lung regions, DEpp (open circles).The solid line (extrapolation is dashed) represents the doseeffectrelation (logistic fit) for lymphoma and breast cancerpatients (DEref.pat).Prostate cancerThe accrual of patients in the phase III dose escalationtrial was continued. Up to October 1999, 78 <strong>NKI</strong> and195 Daniel den Hoed Cancer Center patients had beenrandomized. To study the results of this trial, with respectto tumor control and normal tissue complications inrelation to the 3D dose distribution, a 3D–imagedatabase was developed to store all acquired patientdata. The database offers direct access to CT images,dose distributions, and delineated organs of all enteredpatients. Furthermore, the database is able to processthe various uncertainties in the delivery of CRT and apply
these uncertainties to the analysis of dose-effectrelationships for all patients in a uniform way.When all treatment data of a patient is available, thedata is transferred to the database, where it is stored ina CD-ROM jukebox. A sophisticated user interfaceprovides access to the different planning system anddata exchange formats. This interface is used to checkthe consistency of the treatment planning data and, ifnecessary, ‘fix’ the data. Altered and newly generateddata are stored in an additional, format-independentdatabase, whereas the user interface combines bothdatabases.The trial database has been designed to incorporateuncertainties in dose delivery for the analysis of therelationships between the actual delivered dose distributionand local tumor control and complications ofnormal tissue.A recently implemented model is a mechanical representationof the rectum, which has a different shape foreach delivered fraction. The model describes the shapesthat a rectum can obtain during the course of atreatment. In this model the rectum is divided into slices.For each slice we determine the area, the difference ofthe area with respect to its two neighboring slices, andits position. Different rectum configurations are generatedusing a Monte Carlo technique, in which the position andthe area of all rectum slices is randomly varied. Therandom variations are weighted by probability distributionsof the computed parameters. The probability distributionsare derived from a generic group of patients,which are provided by D. Yan 4 . Each patient of this groupreceived 1 planning CT scan and 17 repeat CT scansduring the treatment. All repeat CT scans are matchedon the planning CT scan using the bony anatomy. Foreach treatment fraction, a new rectum configuration willbe computed using the Monte Carlo technique. Theactual delivered ‘total’ dose will be estimated on thebasis of the obtained rectum configurations. The locationof the prostate is correlated with the position and theshape of the rectum. The target volume motion willtherefore also be included in the simulation.Lung cancerThe phase I/II dose escalation study for inoperableNSCLC patients was continued. Up to October 1999, 23patients had been entered in the study. In the threelowest risk groups for radiation pneumonitis, the nexthigher dose level of 81 Gy was attained.A collaboration with the AZVU was started to investigatethe impact of metabolic imaging on target volumedetermination. In a number of patients with inoperablenon-small cell lung cancer referred for radical radiotherapy,a thoracic transmission and emission 18 FDG-PETscan was performed. CT scans for radiotherapy planningwere matched with the PET-transmission scans, using anadjusted root mean square algorithm. 18 FDG activity inlymph nodes and primary tumor was anatomicallylocalized by overlaying the simultaneously registeredemission PET scan on the matched CT scan. Preliminaryanalysis indicates that additional information from PETscan changes the CT-based target volume in approximately30% of the patients.Correcting dose distributions distorted by set-upverification fieldsElectronic portal imaging is used to verify the set-upaccuracy. Since the treatment field images are generallynot suitable for matching purposes, additional orthogonalfields are used with a number of monitor units between16 and 34. Both the absolute dose and the dosehomogeneity over the planning target volume (PTV), aredistorted by these extra fields. A method was developedto adjust the beam weights and wedge angles of thetreatment plan in such a way that the dose homogeneityover the PTV is maintained. The method applies to threedimensions, which also allows application for noncoplanarbeam setups. The dose gradient of a singlebeam can be described by a vector, whose magnitude isproportional to the beam weight of the beam. Thisproblem can thus be solved using vector analysismethods using several coordinate transformations. Theformalism resulted in clinically acceptable solutions for allcoplanar and non-coplanar cases.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2043.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1830.3 Dr. Daniel den Hoed Cancer Center, ErasmusUniversity, Rotterdam.4 William Beaumont Hospital, Royal Oak, MI, USA.Breast CancerE Damen, AAM Hart, FJP Hoebers, CW Hurkmans,JV Lebesque, BJ Mijnheer, SH Muller1, JL Peterse 1 ,BR Pieters, AE Saarnak, L Van ’t Veer 1 , C Vrieling,H Bartelink, JH BorgerIn EORTC trial 22881/10882 a total of 5,569 breastcancer patients was randomized for boost versus noboost irradiation following whole-breast irradiation. Thecosmetic result was assessed for 731 patients after 3years of follow-up. A panel scored the qualitativeappearance of the breast using photographs. Quantitativedigitizer measurements of nipple displacement wereperformed using these photographs for breast retractionassessment (BRA). For the panel evaluation the intraobserveragreement for the global cosmetic score wasmoderate, the interobserver agreement was fair. Allspecific cosmetic items scored by the panel were significantlyrelated to the global cosmetic score; breast sizeand shape being the most important. For the digitizermeasurements, the standard deviation from the averagevalue of 30.0 mm was 2.3 mm (7.7%) for the intraobservervariability and 2.6 mm (8.7%) for the interob-105RADIOTHERAPY
106RADIOTHERAPYserver variability. The two methods moderately correlated.Both methods showed that the boost had a limited butsignificant adverse effect on the cosmetic result. Thedigitizer evaluation of cosmesis appears to be easier andmore accurate than the panel evaluation, however, thereare some treatment sequellae, such as disturbing scarsand skin changes, that can not be evaluated by BRAmeasurements.Three-dimensional treatment planning was performedfor 30 patients with left-sided breast cancer to assessthe dependence of cardiac and lung complications ontreatment technique and individual patient anatomy. Twolocoregional techniques (A and B) and a tangential fieldtechnique (C), were planned and evaluated for eachpatient. Dose-volume histograms (DVHs) and normaltissue complication probabilities (NTCPs) for the heartand lung were compared for the three techniques. In thebeam’s eye view of the medial tangential fields themaximum distance of the heart contour to the posteriorfield border (MHD) was measured. NTCP values forexcess cardiac mortality due to acute myocardialischaemia varied considerably between patients, withminimum and maximum values of 0.2% and 8.9% (A),0.3% and 7.2% (B) and 0.0% and 6.4% (C). NTCPvalues for radiation pneumonitis were very low for alltechniques. The NTCP values for technique C could verywell be described using the MHD concept. Therefore, theMHD is a simple and generally applicable method toestimate the risk for cardiac mortality, making it easy toestimate the cardiac risk using simulator films andthereby to modify the treatment technique.To evaluate the effectiveness and morbidity of primaryaxillary radiotherapy in breast conserving therapy inpostmenopausal clinically node negative patients withearly stage breast cancer, 105 patients were treatedbetween 1983 and 1997 by wide local excision, followedby radiotherapy to breast and axilla. Fifty-five patientswith no evidence of disease were evaluated for late sideeffects. Three patients had a local recurrence (3%). Noisolated axillary recurrences were seen. In 2 patientsaxillary recurrence was accompanied by distantmetastases (2%). Arm edema was reported subjectivelyby 4% of patients, objectively measured in 11%. Animpaired shoulder function was subjectively noticed in35%, objectively measured in 17%. No brachial plexusneuropathy was seen. It can be concluded that primaryaxillary radiotherapy can be considered as a safe alternativefor axillary lymph node dissection in selectedpatients.Note1 Division XIII.BrachytherapyM Boersma, JH Borger, AE Saarnak, MJ Steggerda,BNFM Van Bunningen, R Wolterink, BR PietersA method to reduce treated volumes of interstitial breastimplants using geometrically optimized stepping sourcetechniques and alternative dose normalizationThe standard breast implant of our clinic, consisting ofan uneven number of needles loaded with linear sourcesof equal lengths, was compared with an optimized implantapplying an even number of needles. In the optimizedsituation linear sources were replaced by a steppingsource with geometric volume optimization to the shape ofthe target volume. A cylindrical target volume of 48 cm 3was chosen. The V(100), V(125) and V(150) (= volumesencompassed by the reference isodose (CRI) of 100%,125% and 150%) were reduced by approximately 35% forthe optimized implant. Despite substantial reduction oftreated volumes, the target volume was completelycovered by the RI in the optimized situation.The effect of dose normalization on the dose distribution,i.e. 85% of the mean central dose (MCD) vs 91%MCD, was subsequently studied for the optimized implant.As an example four different target volumes (varying from15 cm 3 to 40 cm 3 ) were chosen. The average reduction ofV(125) and V(150) when the dose is normalized to 91%instead of 85% of the MCD was 21.2% and 12.7 %,respectively. The V(100) showed little variation.This study shows that by altering the geometry of animplant, performing geometric volume optimization with astepping source and improving the dose distribution bynormalizing to 91% of the MCD, a substantial reductioncan be achieved for treated volumes, whilst maintainingfull coverage of the target volume.This optimized technique was recently implemented inthe clinic using a high dose-rate stepping source.Inter-observer variation in bladder and rectum delineationon CT-images for brachytherapy of cervical cancerIntracavitary treatment of cervical cancer is planned usingpost-implant CT images. Bladder and rectum, which are theorgans at risk, are delineated in order to estimate theabsorbed dose using dose-volume histograms (DVHs). Inorder to determine the accuracy of the dose assessment inbladder and rectum, different aspects of the planningprocedure are investigated. One of the studies concernedthe inter-observer variation in delineation of bladder andrectum. Two dosimetrists and one radiation oncologistdelineated bladder and rectum on CT scans of 10 patients.The dose to bladder and rectum volumes in the high-doseregion was determined from DVHs of each delineatedorgan. In addition, the dose at points placed on thedelineated bladder and rectum walls was determined.Variation in the dose due to delineation differences wasabout 10% both in the high-dose region of the DVHs andin the dose points. Variation in delineation occurred particularlyin areas where organ borders are difficult to distinguish
on a CT image, such as between the bladder and cervixand the rectum and vagina. Since the filling of these organsinfluences the DVHs, we are now investigating whetherdose-wall histograms or dose-surface histograms wouldgive a better representation of the dose to these organs.Radiation-induced apoptosisL Moonen, GA Ruiter 1, 2 , SF Zerp 1, 2 , H Bartelink,WJ Van Blitterswijk 1 , M VerheijFigure IX.4T4 processus alveolaris carcinoma before treatment, tumorblush and 6 weeks after treatment. Tumor is in completeremission.Apoptosis is now recognized as a significant mode ofcell death by ionizing radiation. Split-dose fractionationexperiments in endothelial cells showed that the contributionof the second fraction to cell death increased withlonger time intervals up to 32 hours. These data are in linewith the concept of re-emergence of an apoptosissensitivesub-population between fractions. In order tofurther increase radiation-induced apoptosis, we usesynthetic membrane-permeable alkyl-lysophospholipids(ALPs; Et-18-OCH 3, HePC and D-21266). Thesecompounds have potent anti-tumor properties and someare currently undergoing clinical evaluation. ALPs primarilyact on cell membranes where they interfere with mitogenicsignaling pathways. We found that ALPs preventMAPK/ERK signaling in a Ras-independent manner byinterfering with the PLC/Ca 2+ /PKC pathway. Besides theinhibitory effect on MAPK/ERK, ALPs also suppress theanti-apoptotic Akt/PKB pathway and initiate pro-apoptoticsignals through the SAPK/JNK cascade. Whereas ALPswere found to induce apoptosis in a wide variety of tumorcell lines, normal fibroblasts and quiescent vascular endothelialcells remained unaffected. In combination withradiation, ALPs act synergistically in inducing an apoptoticresponse. Both radiation- and ALP-induced apoptosisproceed in a caspase-dependent fashion. Our currentinvestigations focus on identifying the upstream,membrane-associated, target(s) of ALP-induced apoptosis.In collaboration with M Gallee (Division XIII) we investigatedwhether pretreatment levels of apoptosis (AI), Ki-67index and expression of p53, cyclin D1 and pRbcorrelate with treatment outcome after radiotherapy inmuscle-invasive bladder carcinoma (n=88). In this retrospectiveanalysis, over-expression of cyclin D1 and, to alesser extent, a low baseline AI were found to correlatewith poor local control after external beam irradiation.Notes1 Division III.2 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1435.Combination of radiotherapy andchemotherapyAC Begg 1 , JSA Belderbos, R Keus, C Rasch,L Schultze Kool 2 , B Tan 3 , PJM Van de Vaart 4 ,H BartelinkAssessment of cisplatin DNA adducts as prognostic factorIn a study of 27 patients with non-small cell lung cancer(NSCLC) treated with concomitant daily cisplatin andradiotherapy, the tumor specimens were analyzed for p53and bcl-2 expression. Staining intensity with antibodiesagainst Ki-67 was also measured and the apoptotic indexwas estimated with the tunnel assay. Finally, in buccal cellscisplatin-induced DNA adducts were assessed immunohistochemically.The median follow-up was 41 months, and21 patients (78%) have died. In a univariate analysis, age,tumor stage and cisplatin-DNA adduct staining werethe only factors significantly associated with survival. P53,bcl-2, Ki-67 and apoptosis showed no relationship withoutcome. Multivariate analysis revealed that cisplatin-DNAadduct staining remained an independent prognosticfactor with shorter survival times for patients with a lowadduct staining. The determination of the extent ofplatinum-induced DNA modification in buccal cells couldprovide a simple way to predict treatment outcome inpatients with NSCLC treated with daily concomitantcisplatin and radiation.RADPLATFor inoperable advanced head and neck cancer thephase II study (RADPLAT) protocol of concomitant high107RADIOTHERAPY
108RADIOTHERAPYdose intra-arterial chemotherapy with systemic rescuewith sodiom thio-sulfate and conventional radiotherapywas continued. A total of 76 patients entered the study(67 T4, 9 T3 tumors, 3-10 cm). The majority of thepatients were node positive (51 patients). The medianfollow-up was 11 months (20–30), the median age was50 years (40-69).A complete remission (CR) of the primary tumor wasachieved in 84%, the lymph node CR-rate was 88%, theremainder had partial remission (PR) at the primary siteas well. Figure IX.4 shows an example. No stable orprogressive disease occurred. Grade IV hematologicaltoxicity (Common Toxicity Criteria) occurred in 17% butdid not result in treatment interruptions. Grade III (RTOG)pharyngeal mucositis, upper gastrointestinal and skintoxicity and hearing loss occurred in 43%, 60%, 24%and 10%, respectively. The mean hearing loss was 5 dB.At 20 months local and regional control was 73% and80% respectively. Three patients experienced osteoradionecrosis,all in previous tumor invaded areas.Notes1 Division VIII.2 Division XIII.3 Division XI.4 Daniel den Hoed Cancer Center.Borger JH, Kroon BBR. Low risk of locoregional recurrence of primarybreast carcinoma after treatment with a modification of theHalsted radical mastectomy and selective use of radiotherapy.Cancer 1999; 85: 1773-81.Brugmans M, Van der Horst A, Lebesque JV, Mijnheer BJ. Beamintensity modulation to reduce the field sizes for conformal irradiationof lung tumors: a dosimetric study. Int J Radiat Oncol BiolPhys 1999; 43: 893-904.Coco Martin J, Mooren E, Ottenheim C, Burril W, Nunez MI,Sprong D, Bartelink H, Begg AC. Potential of radiation-inducedchromosome aberrations to predict radiosensitivity in humantumour cells. Int J Radiat Biol 1999; 75: 1161-68.De Jong D, Aleman BMP, Taal BG, Boot H. Controversies andconsensus in the diagnosis, work-up and treatment of gastriclymphoma: an international study. Ann Oncol 1999; 10: 275-80.Dewit L, Verheij M, Valdés Olmos R. Regarding Maor, North,Cabanillas et al. in Int J Radiat Oncol Biol Phys 40, 7647-50, 1998[letter]. Int J Radiat Oncol Biol Phys 1999; 43: 939-41.Essers M, Mijnheer BJ. In vivo dosimetry during external photonbeam radiotherapy. Int J Radiat Oncol Biol Phys 1999; 43: 245-59.Publications: Division IXFull papersLanson JH, Essers M, Meijer G, Minken AWH, Uiterwaal H,Mijnheer BJ. In vivo dosimetry during conformal radiotherapy:requirements for and findings of a routine procedure. RadiotherOncol 1999; 52: 51-60.Bartelink H, Begg AC, Coco Martin J, Van Dijk M, Van ‘t Veer L,Van de Vaart PJ, Verheij M. Towards prediction and modulation oftreatment response. Radiother Oncol 1999; 50: 1-11.Bartelink H. Is neoadjuvant chemotherapy the answer for bladdercancer? [Commentary]. Lancet 1999; 354: 526-7.Bartelink H, Roelofsen F, Eschwege F, Rougier P, Bosset JF,Gonzalez Gonzalez D, Peiffert D, Van Glabbeke M, Pierart M.Concomitant radiotherapy and chemotherapy is superior to radiotherapyalone in the treatment of locally advanced anal cancer:results of a phase III randomized trial of the EuropeanOrganization for Research and Treatment of Cancer, Radiotherapyand Gastrointestinal Cooperative Groups. Classic Papers andCurrent Comments 1999; 3: 529-38.Mageras GS, Fuks Z, Leibel SA, Ling CC, Zelefsky MJ, Kooy HM,Van Herk M, Kutcher GJ. Computerized design of target marginsfor treatment uncertainties in conformal radiotherapy. Int J RadiatOncol Biol Phys 1999; 43: 437-45.Meijer G, Van den Brink M, Hoogeman MS, Meinders J, LebesqueJV. Dose wall histograms and normalized dose surface histogramsfor the rectum. Int J Radiat Oncol Biol Phys 1999; 45:1073-1080.Moonen L, Van der Voet H, De Nijs R, Hart G, Horenblas S,Bartelink H. Muscle-invasive bladder cancer treated with externalbeam radiotherapy: pretreatment prognostic factors and the predictivevalue of cystoscopic re-evaluation during treatment.Radiother Oncol 1998; 49: 149-155.Begg AC, Haustermans K, Hart G, Dische S, Saunders M,Zackrisson B, Gustaffson H, Coucke P, Paschoud N, Houer M,Overgaard J, Antognoni P, Richetti A, Bourhis J, Bartelink H,Horiot JC, Corvo R, Giaretti W, Awwad H, Shouman T, Jouffroy T,Maciorowski Z, Dobrowsky W, Struikmans H, Rutgers D, WilsonGD. The value of pretreatment cell kinetic parameters as predictorsfor radiotherapy outcome in head and neck cancer: a multicenteranalysis. Radiother Oncol 1999; 50: 13-23.Bijker N, Rutgers EJ, Peterse JL, Van Dongen JA, Hart AMM,Ptaszynski A, Van den Bogaert W, Horiot JC, Poortmans P,Fourquet A, Struikmans H, Bartelink H, Pierart M, Collette L, Vander Schueren E. Radiation dose homogeneity in an EORTC multicentretrial on breast irradiation. Acta Oncol 1999; 38 (suppl 13):19-27.Rasch CRN, Remeijer P, Koper PCM, Meijer G, Stroom JC, VanHerk M, Lebesque JV. Comparison of prostate cancer treatmentin two institutions, a quality control study. Int J Radiat Oncol BiolPhys 1999; 45: 1055-62.
Rasch CRN, Barillot I, Remeijer P, Touw A, Van Herk M, LebesqueJV. Definition of the prostate in CT and MRI: a multi-observerstudy. Int J Radiat Oncol Biol Phys 1999; 43: 57-66.Remeijer P, Rasch CRN, Lebesque JV, Van Herk M. A generalmethodology for three-dimensional analysis of variation in targetvolume delineation. Med Phys 1999; 26: 931-40.Roelofsen F, Bartelink H. Combined modality treatment of analcarcinoma. Oncologist 1998; 3: 413-18.Ruiter GA, Zerp SF, Bartelink H, Van Blitterswijk WJ, Verheij M.Alkyl-lysophospholipids activate the SAPK-JNK pathway andenhance radiation-induced apoptosis. Cancer Res 1999; 59:2457-63.Theuws JCM, Kwa SLS, Wagenaar A, Seppenwoolde Y, BoersmaLJ, Damen EMF, Muller SH, Baas P, Lebesque JV. Prediction ofoverall pulmonary function loss in relation to the 3-D dose distribution,for patients with breast cancer and malignant lymphoma.Radiother Oncol 1998; 49: 233-44.Theuws JCM, Muller SH, Seppenwoolde Y, Kwa SLS, BoersmaLJ, Hart G, Baas P, Lebesque JV. The effect of radiotherapy andchemotherapy on pulmonary function following treatment for breastcancer and lymphoma. J Clin Oncol 1999; 17: 3091-100.Van Tienhoven G, Voogd AC, Peterse JL, Nielsen M, AndersenKW, Mignolet F, Sylvester R, Fentiman IS, Van der Schueren E,Van Zijl K, Blichert-Toft M, Bartelink H, Van Dongen JA, on behalfof the EORTC Breast Cancer Cooperative Group and the DanishBreast Cancer Cooperative Group. Prognosis after treatment forloco-regional recurrence after mastectomy or breast conservingtherapy in two randomised trials (EORTC 10801 and DBCG-82TM). Eur J Cancer 1999; 35: 32-8.Multidimensional assessment of voice characteristics after radiotherapyfor early glottic cancer. Laryngoscope 1999; 109: 241-8.Verdonck-De Leeuw IM, Keus RB, Hilgers FJM, Koopmans-VanBeinum FJ, Greven AJ, De Jong JM, Vreeburg G, Bartelink H.Consequences of voice impairment in daily life for patients followingradiotherapy for early glottic cancer: voice quality, vocalfunction and vocal performance. Int J Radiat Oncol Biol Phys1999; 44: 1071-8.Verheij M, Van Blitterswijk WJ, Bartelink H. Radiation-inducedapoptosis: the ceramide-SAPK signaling pathway and clinicalaspects. Acta Oncol 1998; 37: 575-81.Vrieling C, Collette L, Fourquet A, Hoogenraad W, Horiot JC,Jager JJ, Pierart M, Poortmans P, Struikmans H, Van der Hulst M,Van der Schueren E, Bartelink H. The influence of the boost in breastconserving therapy on cosmetic outcome in the EORTC“boost versus no bost” trial. Int J Radiat Oncol Biol Phys 1999;45: 677-85.Vrieling C, Collette L, Bartelink E, Borger J, Brenninkmeyer SJ,Horiot JC, Pierart M, Poortmans P, Struikmans H, Van derSchueren E, Van Dongen J, Van Limbergen E, Bartelink H.Validation of the methods of cosmetic assessment after breastconserving therapy in the EORTC “boost versus no boost” trial. IntJ Radiat Oncol Biol Phys 1999; 45: 667-76.Zelefsky MJ, Crean D, Mageras GS, Lyass O, Happersett L, LingCC, Leibel SA, Fuks Z, Bull S, Kooy HM, Van Herk M, Kutcher GJ.Quantification and predictors of prostate position variability in 50patients evaluated with multiple CT scans during conformal radiotherapy.Radiother Oncol 1999; 50: 225-34.Full papers in press109RADIOTHERAPYVander Poorten VLM, Balm AJM, Hilgers FJM, Bing Tan I, Loftus-Coll BM, Keus RB, Van Leeuwen FE, Hart AMM. The developmentof a prognostic score for patients with parotid carcinoma.Cancer 1999; 85: 2057-67.Bartelink H, Begg AC, Coco Martin J, Van Dijk M, Moonen L, Van‘t Veer L, Van der Vaart PJ, Verheij M. Translational research offersindividually tailored treatments for cancer patients. Cancer J SciAm 1999 (in press).Vander Poorten VLM, Balm AJM, Hilgers FJM, Bing Tan I, Loftus-Coll BM, Keus RB, Hart AMM. Prognostic factors for long termresults of the treatment of patients with malignant submandibulargland tumors. Cancer 1999; 85: 2255-64.Venselaar JLM, Heukelom S, Jager HN, Mijnheer BJ, Van derLaarse R, Van Gasteren JJM, Van Kleffens HJ, Westermann CF.Effect of electron contamination on scatter correction factors forphoton beam dosimetry. Med Phys 1999; 26: 2099-106.Venselaar JLM, Van Gasteren JJM, Heukelom S, Jager HN,Mijnheer BJ, Van der Laarse R, Van Kleffens HJ, Westermann CF.A consistent formalism for the application of phantom and collimatorscatter factors. Phys Med Biol 1999; 44: 365-81.Verdonck-De Leeuw IM, Hilgers FJM, Keus RB, Koopmans-VanBeinum FJ, Greven AJ, De Jong JMA, Vreeburg G, Bartelink H.Bartelink H, Horiot JC. Factors in decision making in the treatmentof breast cancer [commentary]. Radiother Oncol 1999 (in press).Broeks A, Russell NS, Van ‘t Veer L. Increased risk of breast cancerfollowing irradiation for Hodgkin’s disease is not a result ofclassical ATM germline mutations. Int J Radiat Oncol Biol Phys1999 (in press).Meijer G, Bruinvis IAD, Mijnheer BJ, Lebesque JV. A treatmentplanning method to correct dose distributions distroted by setupverification fields. Int J Radiat Oncol Biol Phys 1999 (in press).Moonen L, Gallee M, Verheij M, Ong C, Hart G, Bartelink H.Apoptosis, proliferation and p53, cyclin D1 and retinoblastomagene expression in relation to radiation response in muscleinvasivebladder cancer. Int J Radiat Oncol Biol Phys 1999 (inpress).
110RADIOTHERAPYRemeijer P, Geerlof E, Ploeger L, Gilhuijs KGA, Van Herk M,Lebesque JV. 3-D portal image analysis in clinical practice: anevaluation of 2-D and 3-D analysis techniques as applied to 30prostate cancer patients. Int J Radiat Oncol Biol Phys 1999 (inpress).Russell NS, Bartelink H. Radiotherapy: the last 25 years. CancerTreat Rev 1999 (in press).Russell NS, Lara PC, Grummels A, Hart AMM, Coco Martin J,Bartelink H, Begg AC. In vitro differentiation characteristics ofhuman skin fibroblasts: correlations with radiotherapy-inducedbreast fibrosis in patients. Int J Radiat Biol 1999 (in press).Van de Vaart PJ, Belderbos J, De Jong D, Sneeuw KCA, Major D,Bartelink H, Begg AC. DNA-adduct levels as a predictor of outcomefor NSCLC patients receiving daily cisplatin and radiotherapy.Int J Cancer 1999 (in press).Van Leeuwen FE, Klokman WJ, Van ‘t Veer MB, Hagenbeek A,Krol ADG, Vetter UAO, Schaapveld M, Van Heerde P, BurgersJMV, Somers R, Aleman BMP. Second cancer risk in young survivorsof Hodgkin’s disease: a 25 year follow-up study. J Clin Oncol1999 (in press).Verheij M, Bartelink H. Radiation-induced apoptosis. Cell TissueRes 1999 (in press).Local papers and thesesJansen EPM, Valdés Olmos R, Dewit L, Hamburger HL, BartelinkH, Hoefnagel CA. Residual pituitary adenoma visualized by functional99mTc-HMPAO SPECT. Tijdschr Nucl Geneeskd 1999; 21:76-9.Koning C, Belderbos J, Van Zandwijk N. Radiotherapie. In:Demedts M, Dijkman J H, Hilvering C, Postma D S, redactie.Longziekten; Vol 1. Assen/Leuven: Van Gorcum/UniversitairePers, 1999: 531-5.Moonen L. Radiotherapy in bladder cancer [dissertation].Amsterdam: Free University, 1999.Struikmans H, Van Tienhoven G, Jobsen JJ, Jager JJ, Borger J,Scheijmans LJEE. Loco-regionale radiotherapie van het mammacarcinoomna mastectomie en chemotherapie, commentaarbij twee gerandomiseerde trials. Ned Tijdschr Geneeskd 1998;143: 71-3.Theuws JCM. Pulmonary effects of radiotherapy; a clinical analysis[dissertation]. Amsterdam: Free University, 1999.Van de Vaart PJM. Interaction of platinum coordination compoundswith radiation or hyperthermia: from laboratory to clinic[dissertation]. Amsterdam: Free University, 1999.
X Division of Medical Oncology111Division head Sjoerd RodenhuisHeadS Rodenhuis MD PhDPermanent academic staffJW Baars MD PhD, P Baas MD PhD, EM Bais MD,JH Beijnen PhD, W Boogerd MD PhD, H Boot MD PhD,PF Bruning MD PhD, GC De Gast MD PhD,SP Israëls MD, MJ Kersten MD PhD, H Neering MD PhD,JFM Pruijt MD (until September),JHM Schellens MD PhD, JH Schornagel MD PhD,BG Taal MD PhD, WW Ten Bokkel Huinink MD PhD,JJ Van der Sande MD PhD, M Van der Weide MD PhD,AMC Witte MD (from July), N Van Zandwijk MD PhD,APE Vielvoye-Kerkmeer MD PhDOther academic staffJP Baars MD, GM Bronner, F Custers MD,G De Klerk MD, B De Valk MD, JBAG Haanen,ALT Imholz MD PhD, CMF Kruijtzer MD,RAA Mathôt PhD, Y Oosterhoff MD PhD, J Schrama MD,J Wanders MD, C Weenink MDPermanent technical staffMJX Hillebrand, SE Jansen, FJ Koopman-Kroon,L Nan-OfferingaOther technical staffCGL Cleypool, M Ouwehand, M Profijt, M TibbenGraduate studentsADR Huitema, B Nuyen, M Bouma, Th Kerbusch,H Bardelmeijer, NE Schoemaker, MM Malingré,DHJG Van den Bongard, Ch Van KesterenUndergraduate studentsP QuadvliegResearch nursesD Batchelor, AC Dubbelman, M Holtkamp,GAM Linthorst, H Mallo, ME Schot, M Swart,W UijterlindeGuestJA BurgersSecretariesY Arts-Blom, MEG De KwantResearch funded positions (full time equivalents)Clinical permanent: 7.4Clinical project: 10.9Technical permanent: 9.9Technical project: 4.0IntroductionIn 1999, the clinical research program of the Divisionof Medical Oncology continued to concentrate on thedevelopment of innovative treatments and furtherstrengthened its ties with the fundamental sciencegroups in the institute. To increase the level of interactionbetween the laboratory and the clinic, several youngspecialists in internal medicine work for two years inbasic research under supervision of a non-clinicalscientist and than switch to the clinic for their formaltraining in Medical Oncology.Good clinical science is demanding in many respectsand the excellent infrastructure of the institute is essentialfor its expansion. As a national cancer institute, webelieve that interactions with research groups in universitiescan be beneficial to all parties and we haveestablished close links with university centers inside andoutside Amsterdam. In January 1999, JHM Schellens,the coordinator of our Clinical Pharmacology program,was appointed part-time Professor of Pharmacy at theUniversity of Utrecht. This appointment is a further naturallink in the Cancer Pharmacology network that has theNetherlands Cancer Institute at its core.A novelty for the clinical research program was theappointment of a Clinical Quality Assurance Officer tohelp in the implementation and execution of GoodClinical Practice (GCP) guidelines. The conduct of clinicalstudies is increasinly done under GCP and the ClinicalPharmacology Program is entirely done under GCPconditions.Clinical Pharmacology is the largest research groupwithin the division. One major research topic is the theoral administration of taxanes, facilitated by the inhibitionof P-glycoprotein, a drug transporter that is responsible
112MEDICAL ONCOLOGYfor the fact that orally administered taxanes have a verylow bioavailability. The Pharmacology Group has beensuccessful in increasing the bioavailabiltiy of bothPaclitaxel and Docetaxel by prior administration ofCyclosporin A. These findings from phase I studies haveled to a phase II study of oral Docetaxel in advancedbreast cancer. This study is now accruing patients.The autologous transplantation group has completedpatient accrual in the national study of high-dose chemotherapyin breast cancer patients with 4 or more tumorpositiveaxillary lymph nodes. A total of 885 patients havebeen randomized in this study, in 10 Dutch centers,making this the largest study internationally. It may wellbe that this trial will prove pivotal since it lacks a numberof major problems that other large studies have: it isessentially a population-based study rather than a trial inhighly selected patients, and there is hardly any toxicmortality. The first meaningful (progression-free) survivalanalysis can be done in 2002 and any advantage seenfor the high-dose therapy must be regarded as uncertainuntil that time.The Thoracic Oncology Group presented the firstanalysis of a large chemo-prevention trial initiated in1987. This ‘EUROSCAN study’ involved nearly 2,000patients at risk for a second primary tumor of the lung orin the head-and-neck area. The analysis showed nopreventive effect at all for interventions with either vitaminA, or N-acetylcysteine, or both. The disappointingoutcome of this very large and well-designed study is inline with several American chemo-prevention projects inaerodigestive tract cancers. Unsurprisingly, even in thenew millennium, there is no substitute for smokingcessation.One of the unique features of the institute is the rapidand natural interaction between disciplines and divisions.Among its consequences is the establishment of aclinical unit for chemo-radiation therapy integrated in oneof the two medical wards. The institute has played aprominent part in the relatively recent recognition thatconcurrent radiotherapy has curative potential in a largenumber of epithelial tumors, where the sequential applicationof these treatment modalities holds no specialadvantage. Examples include the treatment of stage IIInon-small cell lung cancer with concurrent cisplatin andradiation and, more recently, intra-arterial cisplatin andradiotherapy in advanced head-and neck cancers. Theconcurrent approach is demanding in terms of logisticsand an optimal clinical setup is obviously required forambitious clinical studies in a large number of tumortypes, including cervical, anal, esophageal and urothelialcancers. This will be provided by the novel clinical unit.The immediate future for the clinical research programof the division will not dramatically differ from theactivities in 1999. The growing emphasis on clinicalstudies that exploit the basic science progress will be acommon theme, greatly facilitated by the presence ofstrong fundamental biology in the institute. It is satisfyingthat at last the understanding of disease at a molecularlevel is beginning to benefit individual patients withcancer.Clinical PharmacologyP Baas, EM Bais, OB Dalesio, G De Klerk,AC Dubbelman, ADR Huitema 1 , Th Kerbusch,CMF Kruijtzer, J Lieverst 2 , JM Maaskant, M Mahn 2 ,M Maliepaard 3, 4, 5 , MM Malingré, H Mallo, R Mathôt,I Mandjes 2 , D Pluim 3 , S Rodenhuis, NE Schoemaker,JH Schornagel, M Schot, A Schrijvers 6 , M Swart,Ch Van Kesteren, RCAM Van Waardenburg 7 ,N Van Zandwijk, JH Beijnen, JHM Schellens,WW Ten Bokkel HuininkPhase I studies and drug schedulingIn 1999, the number of active studies has increasedeven beyond that of 1998. At present, 20 phase I andpharmacologic studies are being conducted, of which 15are open for accrual. The patient recruitment in thesestudies totals over 170 in 1999.One of the major translational research activitiescontinued to be the development of oral treatmentschedules for paclitaxel and docetaxel in combinationwith oral cyclosporin A (CsA). The bioavailability ofdocetaxel after oral administration plus one single oraldose of CsA was 88 ± 36% (Figure X.1 and X.2).Importantly, the interpatient variability in systemicexposure after oral and i.v. administration was almostidentical. The safety of the oral route was excellent. Todate, a phase II study of weekly oral docetaxel plus CsAin second line advanced breast cancer has recruited 7patients. All three patients currently evaluable forresponse had achieved at least a partial remission.A P-glycoprotein blocker GF120918 was combinedwith oral Taxol in 6 patients and the results reveal thatthe effect of this blocker on the systemic exposure topaclitaxel is at least as pronounced as that of CsA.Figure X.1Plasma concentration-time curve of docetaxel administeredorally at a dose of 75 mg/m 2 in combination with an oral doseof 15 mg/kg of the P-glycoprotein blocker cyclosporin A (CsA)and at a dose of 100 mg/m 2 intravenously to the same patient.
Figure X.2Mean (SD) dose-corrected area under the curve (AUC) values ofdocetaxel when administered intravenously, orally in combinationwith CsA (N=10) and orally without CsA (N=3).Another phase I study was initiated with a novel farnesyltransferaseinhibitor R115777. The maximum tolerateddose (MTD) was 300 mg twice daily without interruption.The dose limiting toxicity (DLT) was neutropenia. Two outof 30 patients developed significant primarily sensoryneuropathy after 2 months of treatment. A partialremission was documented in platinum resistant stage IVnon-small cell lung cancer (NSCLC) and activity was alsonoted in colon and pancreatic cancer. The area under thecurve (AUC) of R115777 proved to be significantly correlatedwith myelosuppression.Based on the results of our previous phase I studywith continuous i.v. CPT11, we are currently performing aphase I and pharmacologic study with oral CPT11 dailytimes 14. The regimen is well tolerated and the MTD hasnot been reached at 20 mg/m 2 /day.The oral miltefosine analog D21266 (perifosine) wasinvestigated in a dose-escalating study to determine theMTD, which was reached at 200 mg on a 21 day q 28day schedule. Gastro-intestinal toxicity was dose-limiting,in particular nausea and vomiting.The randomized phase I study with weekly or twoweeklygemcitabine and cisplatin in patients with NSCLCis ongoing. To date, 35 patients have been recruited. Thecurrent dose level in the weekly schedule is 55 mg/m 2 ofcisplatin plus 900 mg/m 2 of gemcitabine. The doseintensityis already over 50% higher than in the standardschedule of this combination. Activity has been noted inseveral patients. Pharmacokinetic and dynamic analysisrevealed that the total plasma clearance of unboundplatinum as well as the DNA-adduct formation in leukocytesis reduced by gemcitabine.E7070 is a novel disulphonamide anticancer agentinterfering with the G1-S cell cycle transition, which isinvestigated in phase I trials within the framework of theEarly Clinical Studies Group (ECSG). The schedule is aone hour i.v. infusion q 3 weeks. The dose-limitingtoxicity is neutropenia. The pharmacokinetics areprofoundly nonlinear. The AUC of E7070 is significantlycorrelated with neutropenia. Currently, a mass balancestudy with 14C-labeled E7070 is in progress.The food-drug interaction study with the 5FU oralprodrug S1 revealed that food significantly affected thepharmacokinetics of S1 and reduced the AUC of 5FU by16%.The combination of carboplatin and topotecan is beinginvestigated in a phase I and pharmacologic study. Inaddition to bioanalysis of topotecan and carboplatin,platinum-DNA adduct levels in leukocytes and tumor cellsas well as catalytic activity and expression of topoisomeraseI are determined in leukocytes and tumor biopsymaterial collected during the first course of treatment.Biopsies have been collected in all 5 patients.Another phase I study with a polymer MAG-camptothecinformulation is actively recruiting patients at thedaily times 3, q 4 weeks schedule at a dose level of68 mg/m 2 /day.A phase I study with a novel organic rutheniumcompound NAMI-A was recently initiated. The scheduleis daily times 5 q 3 weeks. In pharmacologic studies,concentrations of ruthenium in plasma and DNA-adductsin leukocytes are being monitored.Phase II and pharmacologic studiesWithin the framework of the ECSG, the activity of UFT(an oral prodrug of 5FU) plus leucovorin was determinedas the first chemotherapy for advanced gastric cancer.The drug was well tolerated. One out of 8 patientsremained stable for 2.5 years while on study. In anotherECSG study, the activity of S1 was investigated in thefirst line treatment of advanced colorectal and gastriccancer.Clinical phase II and III studies within the framework ofthe European Biomed 2 program are ongoing. The aim isto determine pharmacokinetic/tumor biologic-responserelationships and pharmacokinetic-toxicity relationshipswith the combination of doxorubicine-cyclophosphamidein the first line chemotherapy of advanced breast cancer,and with the carboplatin-Taxol regimen in the first linechemotherapy of advanced ovarian cancer. To date, 21patients with breast cancer and 12 patients with ovariancancer were included in our institute.Population pharmacokinetics (PK) and dynamics (PD)Population PK and PD is a subject of increasingimportance within the pharmacology group. TheNonlinear Mixed Effects Models software programNONMEM is extensively used. NONMEM is employed tosupport the outlined Biomed 2 program and NONMEM isalso used to explore the population PK and PD ofET743. This is a novel anticancer agent of marine sourceunder development in sarcoma.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1799.2 Biometrics.3 Division VIII.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-1059.113MEDICAL ONCOLOGY
114MEDICAL ONCOLOGY5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2060.6 Funding: Biomed 2, Project PL96.2333.7 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1440.PharmacyH Bardelmeijer 1 , I Bedeker 2 , M Bouma 2 ,CGJ Cleypool 3 , RMW Hoetelmans 2 , MJX Hillebrand,ADR Huitema 4 , SE Jansen 2 , Th Kerbusch,FJ Koopman-Kroon 2 , MM Malingré, RAA Mathôt,L Nan-Offeringa 2 , B Nuyen 2 , M Ouwehand 1 , M Profijt 2 ,H Rosing 2 , NE Schoemaker, RW Sparidans 2 ,WW Ten Bokkel Huinink, MM Tibben 4 ,DHJG Van den Bongard, R Van der Put 2 , R Van Gijn 2 ,RPG Van Heeswijk 2 , Ch Van Kesteren, O Van Tellingen 5 ,AI Veldkamp 2 , JH Beijnen, JHM SchellensThe research programs of the Department ofPharmacy and Pharmacology are focused onpharmaceutical formulation and drug level monitoring of(investigational) anticancer drugs to support preclinical(see Division VIII) and clinical pharmacologic research.The investigations are conducted in the setting of afoundation (NLADF), which is a collaboration between theNetherlands Cancer Institute and Slotervaart Hospital.1999 was a very important year for the department. Theministry of Health, Welfare and Sport has granted us theGMP (Good Manufacturing Practice) license which is theofficial qualification required to manufacture investigationalcytotoxic drugs for clinical trials, both on site andelsewhere. On June 25 1999, the laboratory received itsofficial recognition ‘in compliance with the OECDPrinciples of Good Laboratory Practice (GLP)’ in the fieldof Analytical Chemistry.FormulationCurrent formulation research is mainly focused oncytotoxic agents originating from marine organisms andheavy metals (platinum, ruthenium). The followingcompounds are currently investigated to find a suitableparenteral formulation to be used in clinical phase Iresearch: thiocoraline, spisulosine, isohomohallichondrin-B, kahalalide F and P-65. The formulation of aplidine(freeze-dried) was successfully transferred to thepharmaceutical industry with no problems of upscaling.We have designed and manufactured a freeze-driedproduct of the ruthenium-containing antitumor agentencoded NAMI-A. The drug is currently tested in a phaseI trial in our institute. A HPMA-polymer bound platinumcompound is now in its pre-formulation stage. Batches offreeze-dried products (MEN10755, BBR2778) weremanufactured for clinical phase I testing. In a collaborativenetwork with the EORTC, NCI and CRC weperform pre-formulation and quality control studies ofnovel chemical entities with in vitro anti-tumor activity tobe selected for further development.An oral tablet formulation for the tyrosine kinaseinhibitor BIBX1382BS has been designed and batcheshave been manufactured to support ECSG phase Iclinical trials.Further optimization of our validation programs of theFormulation Laboratory to maintain the GMP status is acontinuous process which significantly impacts on thework load.Bioanalysis and clinical pharmacologyBioanalytic and clinical pharmacologic researchcomprise the following compounds: topoisomerase-Iinhibitors, taxoids, platinum compounds, the drugs in the‘CTC’ high dose regimen (carboplatin-thiotepa-cyclophosphamide),ifosfamide, perifosine and novel cytotoxics(ET-743, aplidine, thiocoraline, KRN 7000) originatingfrom marine sources.We have developed HPLC assays to measurecamptothecin in plasma after administration of polymerbounddrug (MAG-CPT) to support an ongoing phase Itrial.A large program has been set up to track downmetabolites of ecteinascidin-743 (ET-743) by usingcoupled liquid chromatography and mass spectrometry.HPLC assays have been validated and implemented tomeasure 4-hydroxy- and nitrogen mustard metabolites ofcyclophosphamide and ifosfamide. Close pharmacokineticmonitoring in the CTC-program has revealed thatthioTEPA inhibits the activation route of cyclophosphamide.The clinical relevance of this observation,however, is not clear. A new alkylating metabolite ofthioTEPA, thioTEPA-mercapturate has been identified inthe urine of treated patients. Pharmacokinetic individualizationappear feasible in the CTC-scheme.A pharmacokinetic, population-based model has beendesigned to describe the ifosfamide auto-inductionphenomenon.The triple quadrupole, tandem mass spectrometer(LC/MS/MS; Sciex API 365) has greatly expanded ourFigure X.3Mass spectrum of spisulosine (ES-285), a novel anti-tumor drugfound in a North Atlantic clam, with selectivity against prostateand renal cancer and hepatomas. The compound is now in thedevelopmental, pre-formulation phase. Mass spectrum: m/z286.4 MH+, m/z 268.3 MH+ (-H2O), m/z 571.2 (2 x M)H+(dimer).
analytical capabilities (Figure X.3). We are now setting upLC/MS/MS assays for E7070, ET-743 metabolites andkahalalide-F to support clinical pharmacologic research.The equipment is also being used for quality controlpurposes of peptides synthesized in the institute.Notes1 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1779.2 NLADF/Slotervaart Hospital.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 99-2033.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1439.5 Division XIII.ImmunotherapyD Batchelor, JBAG Haanen, SP Israëls, MJ Kersten,H Mallo, WJ Nooijen 1 , JH Schornagel, J Sein 2 ,W Van de Kasteele 2 , N Verra 1 , FA Vyth-Dreese 2 ,GC De GastMetastatic melanomaA phase II single center study was performed ofchemo-immunotherapy consisting of temozolomide (150mg/m 2 for 5 days in 6 patients), escalated to 200 mg/m 2in 18 patients, and subsequently to 250 mg/m 2 in 18patients), followed by combined immunotherapy of GM-CSF, low dose IL-2 and IFNa. In one year, 42 patientswere included. Preliminary results show response, stabledisease and progressive disease, each in approximatelyone third of the patient population. Of interest is theabsence of brain metastases in patients with response orstable disease and the absence of lymphocytopenia, awell known toxicity of temozolomide. Half of the patientswith 250 mg/m 2 temozolomide showed thrombocytopeniaas dose limiting toxicity and some also had granulocytopenia.Patients with residual metastases underwentsurgical removal (two times lobectomy, two times adrenalectomy)with normalization of S100 afterwards.Monitoring with serum S100b levels showed a goodcorrelation with the clinical response. In patients withprogression after chemo-immunotherapy, a phase I trialof increasing doses of temozolomide with standardcisplatin (75 mg/m 2 ) followed by the same immunotherapywas performed. Stabilization of the disease wasachieved in the majority of patients.Renal cell carcinoma (RCC)A phase II multicenter study of combined non-specificimmunotherapy was started in which Maastricht, Utrechtand Nijmegen participate. At this time, 30 patients areevaluable with 5 x CR, 3 x PR (27%), 11 x SD, 11 x PD.Vaccination with a G250 peptide will start in HLA-A2+patients with progression after combined non-specificimmunotherapy.Perioperative immunomonitoringIn HLA-A2+ patients undergoing a lymphadenectomy formelanoma, the number of cytotoxic T lymphocytes (CTLs)with a T-cell receptor for melanocyte differentiation antigenswas determined by tetramer technology. In 2 patients Mart-1 specific CTLs were found in the CD8 population (0.5-2.0%) from the lymph nodes, that were not present in theblood. In patients with a nephrectomy after 2 cycles oftreatment with combined immunotherapy for RCC, therewas an increase of dendritic cells of several types andmaturation stages, as well as T cells in the tumor.Lymphocyte reinfusion after high dose chemotherapy inmetastasized breast cancerPatients with breast cancer receiving multiple coursesof high-dose chemotherapy (tCTC) with peripheral bloodprogenitor cell transplantation, continue to be immunosuppressedfor prolonged periods after treatment. Thisleads to an increased incidence of infections, such asHerpes zoster, and is an obstacle for the development ofimmunotherapy-based treatments to eradicate minimalresidual disease.To deal with this problem, the feasibility and efficacy oflymphocyte-reinfusions after second and third high-dosecourses was explored.Three patients who had not received a lymphocytereinfusion showed a profound lymphocytopenia of CD4+T cells (< 100/µL) and CD8+ T cells (< 200/µL) for morethan 6 months. In 9 patients in whom lymphocytes(≥ 2 x 10 10 ) were harvested after standard chemotherapy,lymphocytes were reinfused after the second tCTCcourse, which was followed by G-CSF, and after the thirdtCTC course, which was followed by both GM-CSF andIL-2. Lymphocyte recovery after re-infusion was significantlybetter than after the first high dose course or thanin the first 3 patients, with restoration of CD4 and CD8T- cell levels to pre-treatment levels after 1 month. Afterthe third tCTC course, CD4+ T cell recovery was better.There was, however, no apparent decrease in Herpeszoster reactivations.Notes1 Division XIII.2 Division IV.Autologous hematopoietic progenitor celltransplantation programJW Baars, JH Beijnen, GC De Gast, O Dalesio,M Holtkamp, ARD Huitema, MJ Kersten, G Linthorst,WJ Nooijen 1 , JFM Pruijt, JH Schornagel, J Schrama,ICM Slaper-Cortenbach 2 , AM Westermann, S RodenhuisMultiple courses of ‘tiny’-CTCIn the past few years, about sixty patients have beentreated in a series of clinical studies aiming to develop ahigh dose alkylating chemotherapy regimen that can beadministered safely within in a tight time frame. Thesestudies have led to the ‘tiny’-CTC regimen, which incor-115MEDICAL ONCOLOGY
116MEDICAL ONCOLOGYporates cyclophosphamide (4 g/m 2 ), thiotepa (320mg/m 2 ) and carboplatin (target AUC 13.3 mg.ml -1 .min).Three subsequent courses of tCTC can be administeredevery four to five weeks provided that autologous peripheralblood progenitor cells can be reinfused followingeach course.In 1999, a first relapse-free survival analysis could bedone of a phase II study 3 in which patients with disseminatedhormone refractory breast cancer receivedintensive chemotherapy (Figure X.4). A total of forty-onepatients were scheduled to receive two courses offluorouracil, epirubicin and cyclophosphamide.Responding patients went on to three subsequentcourses of tCTC. Twenty-nine patients either showedevidence of tumor regression as a result of FEC, or werenot evaluable. For this subgroup, the projected four yeardisease-free survival was 30% (confidence interval 14-49%). This finding confirms that long-term disease-freesurvival is achievable for a subgroup of chemotherapyresponsivepatients with breast cancer.The large majority of patients had achieved a completeremission at the end of the treatment sequence. The factthat most of them relapsed within the first year illustratesthat a treatment strategy is required to deal with minimalresidual disease. For this purpose, a feasibility study ofpost-transplantation immunotherapy was completed in1999. In this study, patients received an autologous invivo activated lymphocyte re-infusion, in addition to thestem cell transplantation. Although this led to rapid restorationof T-cell subsets, most patients developed herpeszoster infections in the first months after transplantion.Thus, it is questionable whether the enhanced immunoreconstitutionhas clinical significance. Alternativemethods to manage the minimal residual diseasesituation after high-dose chemotherapy are being considered,including maintenance low-dose chemotherapy oranti-angiogenesis agents.The repeated high-dose alkylating chemotherapy isalso the subject of detailed pharmacodynamic studies 4 .In 1999, analytic methods to determine the plasma levelsof cyclophosphamide and its many metabolites weredeveloped and validated, as were methods for thiotepaand tepa. These methods and the assays for carboplatindeveloped earlier were employed to adjust the dose ofthe four day tCTC-courses based on pharmacokineticparameters determined on the first day of the course.The efficacy of this strategy to decrease end-organtoxicity is now being studied.High-dose alkylating therapy is potentially curative ingerm cell cancer, as well as breast cancer. Patients withchemotherapy refractory testicular cancer do not usuallybenefit from high-dose therapy and are thereforeexcluded from the national high-dose study. Two of thesepatients received three closely spaced courses of tCTCas salvage therapy. Both achieved a complete remission.One of them has remained free of disease and ispossibly cured. A phase II study of triple tiny-CTC inrefractory germ cell cancer is being considered.Figure X.4Progression-free survival of 29 patients who responded to twoconventional doses of chemotherapy, and subsequentlyunderwent multiple courses of high-dose chemotherapy. All hadstage IV breast cancer and were hormone-unresponsive.Multicenter high-dose chemotherapy studies coordinatedby <strong>NKI</strong>/<strong>AvL</strong>By August 1, 1999 the national study of adjuvant highdosechemotherapy in high-risk breast cancer wasclosed 5 . This trial, designed in our institute and coordinatedin collaboration with Groningen University, hasrandomized a total of 885 patients and is thus the largeststudy of its kind. The relapse- free survival advantageseen for the patients who were randomized to the highdosechemotherapy arm could be the result of a statisticalfluctuation and should thus not be considered as arationale for high-dose therapy outside clinical studies.A second national study devised and led by ourinstitute is the high-dose chemotherapy study for patientswith germ cell cancer relapsing from a completeremission. A preliminary analysis was performed andpublished in 1999, showing that about 50% of thesepatients can be cured by high-dose therapy.Notes1 Division XIII.2 Central Laboratory of the Netherlands Red Cross forthe Blood Transfusion Service, Amsterdam.3 Supported in part by the Schumacher-KramerFoundation.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1439.5 Funding: Health Insurance Council Fund forInvestigative Medicine (Ziekenfondsraad)Ontwikkelingsgeneeskunde) 09-94-051.
GastroenterologyBMP Aleman 1 , D De Jong 2 , CA Hoefnagel 2 ,P Qaedvlieg, RA Valdés Olmos 2 , F Van Coevorden 3 ,L Van ’t Veer 2 , MLF Veldhuysen 2 , AMC Witte,FAN Zoetmulder 3 , H Boot, BG TaalGastric non-Hodgkin’s lymphomaTreatment decisions are mainly based on histologicalgrading and clinical staging (including endoscopic ultrasound).Helibacter pylori eradication is generally acceptedas a non-toxic and effective treatment in stage I lowgrade MALT lymphoma. In a series of 22 patients, acomplete remission was achieved in 13 (59%) and partialresponse in 2 (9%). Further histological grading wasrelated to response: complete remission was observed in12 of 15 purely low-grade tumors (type A), and in only 1of 7 lymphomas with some blasts (type B) (p < 0.01).The expression of co-stimulatory markers was alsopredictive: two or all of the three markers CD40, CD80and CD86 were expressed in 12 of 13 type Alymphomas, compared to 1 of 6 type B lymphomas(p < 0.001).Carcinoid tumorsCarcinoid tumors are rare and account for approximately300 new cases per year in the Netherlands. Theprognosis is relatively good: the 5 year survival for locoregionaldisease is 53-80% and for metastatic disease18%. Whether adequate palliative treatment has resultedin a survival benefit, will be studied in cooperation withthe Cancer Registry (IKA).A tracer dose of [131I]MIBG is frequently employed forimaging of neuroendocrine tumors, and results in apositive test in 70% of the carcinoid patients. RadiolabeledMIBG treatment was shown to be effective andresulted in (long-lasting) reduction of symptoms, but itwas not associated with a significant decrease in urinary5HIAA excretion (biochemical response). Improved tumortargeting by predosing with unlabeled MIBG could beachieved in 6 of 10 cases; the subsequently appliedcombined treatment dose induced symptomatic improvementin 5 patients and a biochemical response in 3 ofthem. These encouraging results have been confirmed inanimal models and will be built on in further studies.Hereditary cancerAmong the familial cancers, HNPCC (hereditary nonpolyposiscoli cancer) has received a great deal ofattention: DNA tests are available and guidelines forsurveillance have been developed. Less information isavailable regarding a genetic predisposition for gastriccancer. Using the same Amsterdam criteria that weredeveloped for HNPCC, the number of families withgastric cancer is increasing. Currently the clinical data of8 kindreds has been collected. The histological subtype(diffuse or intestinal type) may be correlated with DNAtests.Gastric metastasesIn 51 breast cancer patients, an endoscopic diagnosisof gastric involvement was made. Histology showed apredominance (72%) of the relatively infrequent subtypeof lobular carcinoma. Symptoms were non-specific; 12%of patients presented with hemorrhage. All patients alsohad other sites of metastatic disease, particularly bonemetastases (43%). Although gastric involvement is a latemanifestation of metastatic disease, its response tochemotherapy or endocrine treatment was fairly goodwith an objective response rate of 46%. The remaininglife-span was 10 months (median) and the 2 year survival23%.Esophageal cancerIn advanced disease with a short life expectancyseveral palliative treatment options have been explored(argon beam coagulation, alcohol injection and laser)among which the insertion of a stent is most frequentlyapplied. Since the introduction of the self expandablestents, various modified types have become available toindividualize the choice of stent per patient. The overallsuccess rate is 90%, leading to immediate improvementof dysphagia.In order to improve the treatment results in esophagealcancer, combined modality approaches have beendeveloped. In locally advanced disease, chemo-radiationseems to be superior to radiation therapy alone: currentlya phase I study is in progress that investigates increasingdoses of radiotherapy and concurrent low-dose cisplatinum.In patients with a local tumor amenable forsurgery, pre-operative chemo-radiation has been appliedin a pilot study of 8 patients. Full dose cisplatinum and5FU at the beginning and end of the radiation schemewas employed. This concurrent chemo-radiation schemehas induced several histologically confirmed completeremissions and is tolerable in fit patients; long-termresults have to be awaited.Notes1 Division IX.2 Division XIII.3 Division XI.Thoracic OncologyAJM Balm 1 , JSA Belderbos 2 , F Custers, OB Dalesio,Y Oosterhoff, JHM Schellens, FA Stewart 3 ,FJ Van Schooten 4 , LJ Van ’t Veer 5 , H Van Tinteren,C Weenink, P Baas, N Van ZandwijkNon-Small Cell Lung Cancer (NSCLC)Locally advanced NSCLC stage III disease involves asubset of patients without distant metastases. For manyyears, radiotherapy has been accepted as the standardof care. A revision of the therapeutic strategies in suchpatients came about in the early nineties when better117MEDICAL ONCOLOGY
118MEDICAL ONCOLOGYresults were obtained with cisplatin added to radiotherapyas a radiosensitizer. The recent favorable results(EORTC 08955) of the gemcitabine/cisplatin (G/C) combinationas a pre-operative and pre-radiotherapy regimensuggest that further improvement is possible. With anoverall response rate of 84%, leading to completesurgical resection in 71%, this regimen may well beconsidered as a standard in combined modalitytreatment. Although it is true that the population ofpatients who received G/C as induction treatment wassmall and selected, we conclude that surgery alone is nolonger an adequate standard for stage IIIA patients. Thequestion of whether induction therapy should be followedby surgery or radiotherapy is still under investigation inEORTC 08941. For medically inoperable patients, acomparison between concurrent and sequential chemoradiotherapyis being made in EORTC 08972. This trialwas activated in the beginning of 1999 and has nowbeen adopted by several centers in the Benelux.The use of incremental doses of cisplatin (day 1) andgemcitabine (day 2) on a weekly or a two-weekly basis inmainly stage IV NSCLC patients has revealed that thisintensive dose therapy is reasonably well-tolerated.Several objective responses have been documented afteronly 6 weeks of intensive therapy and these resultsencourage the further exploration of intensified therapy inpatients with early NSCLC.Chemoprevention and early detectionEuroscan 6 is a large scale clinical trial to assess thechemopreventive effects of Vitamin A and N-acetylcysteinein patients treated with curative intent for lung andhead and neck cancer. Disappointingly, the first fullanalysis of the results has not revealed any preventiveeffect of a 2-year intervention period with Vitamin A or N-acetylcysteine after a median follow-up of 49 months.Taking into account the latency period of lung cancer,assumed to be 10 years or more, additional follow-up isneeded before definite conclusions may be drawn. Inessence, Euroscan has yielded a similar outcome asseveral other large chemoprevention studies that wererecently published.Another project focused on premalignant epithelialchanges in smoking volunteers and revealed that p53mutations detected by FASAY may already be presentwhen white light bronchoscopy appears normal. Toexplore new methods for early detection, an endoscopyprogram studying autofluorescence and ALA (aminolevulinicacid) induced fluorescence in patients withelevated cancer risk (Euroscan population) was initiated.Malignant Mesothelioma 7The phase II study of intraoperative photodynamictherapy and pleuropneumonectomy in patients withlimited mesothelioma and favorable prognostic factorswas completed. The following conclusions can be drawnfrom the study: 1) This combined treatment is frequentlyaccompanied by a prolonged recovery period andrequires intensive postoperative care to prevent complicationswhich occur at a higher rate than seen afterstandard pneumonectomy. 2) Although efficient localcontrol could be obtained, some patients wereconfronted with isolated distant metastases. It is possiblethat in the past metastatic disease has been obscured byprogression of locoregional disease.Another novel technique combining pleurectomy withintraoperative hyperthermic chemotherapy has beenintroduced in the clinic, as described in the report ofDivision XI. This treatment approach was explored in 4patients and was shown to be feasible. Additionalexperience with this technique will be gained in 2000.Phase II studies employing new agents or combinationsof agents continued. Objective responses have beenrecorded with the gemcitabine/cisplatin combination.Notes1 Division XI.2 Division IX.3 Division VIII.4 University of Limburg, Maastricht.5 Division VIII and XIII.6 Funding: European Communities (EuropeanCommission DG V).7 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 97-1446.Publications: Division XFull papersBerger C, Van Baarle D, Kersten MJ, Klein MR, Samer Al-HomsiA, McQuain C, Van Oers MHJ, Knecht H. Carboxy terminalvariants of Epstein-Barr virus encoded LMP1 during longtermHIV-infection: reliable markers for individual strain identification. JInfect Dis 1999; 179: 240-4.Beijnen JH, Meenhorst PL. Follow-up of ectasy intoxication [letter].J Toxicol & Clin Toxicol 1999; 37: 343.Boven E, Jansen WJM, Hulscher TM, Beijnen JH, Van Tellingen O.The influence of P170-glycoprotein modulators on the efficacyand the distribution of vincristine as well as MDR1 expression inBRO/mdr1.1 human melanoma xenografts. Eur J Cancer 1999;35: 840-9.Cohen Stuart JW, Schuurman R, Burger DM, Koopmans PP,Sprenger HG, Juttmann JR, Richter C, Meenhorst PL,Hoetelmans RMW, Kroon FP, Bravenboer B, Hamann D, BoucherCA, Borleffs JC. Randomized trial comparing saquinavir soft felatincapsules versus indinavir as part of triple therapy (CHEESEstudy). AIDS 1999; 13: F53-8.Crommentuyn KML, Schellens JHM, Van den Berg JD, BeijnenJH. In-vitro metabolism of anti-cancer drugs, methods and applications:paclitaxel, docetaxel, tamoxifen and ifosfamide. CancerTreat Rev 1998; 24: 345-66.
De Graaff M, Maliepaard M, Pluim D, Floot BJ, Slaper-CortenbachIC, Schellens JHM. In vitro antagonistic cytotoxic interactionsbetween platinum drugs and taxanes on bone marrow progenitorcell CFU-GM. Anticancer Drugs 1999; 10: 213-8.De Vries N, Van Zandwijk N, Pastorino U. Chemoprevention ofhead and neck and lung (pre)cancer. Recent Results Cancer Res1999; 151: 13-25.De Wit R, Collette L, Sylvester R, De Mulder PH, Sleijfer DT, TenBokkel Huinink WW, Kaye SB, Van Oosterom AT, Boven E, StoterG. Serum alpha-fetoprotein surge after the initiation of chemotherapyfor non-seminomatous testicular cancer has an adverseprognostic significance. Br J Cancer 1998; 78: 1350-5.De Wit R, Van Dam FSAM, Vielvoye-Kerkmeer A, Mattern C,Huijer Abu-Saad H. The treatment of chronic cancer pain in a cancerhospital in the Netherlands. J Pain Symptom Manage 1999;17: 333-50.Enting RH, Hoetelmans RMW, Lange JMA, Burger DM, BeijnenJH, Portegies P. Antiretroviral drugs and the central nervous system.AIDS 1998; 12: 1941-55.Gerrits CJ, Schellens JHM, Burris H, Eckardt JR, Planting AS, Vander Burg ME, Rodriguez GI, Loos WJ, Van Beurden V, Hudson I,Von Hoff DD, Verweij J. A comparison of clinical pharmacodynamicsof different administration schedules of oral topotecan. ClinCancer Res 1999; 5: 69-75.Giaccone GC, Baas P. Mesotheliomas. In: Raghaven D, BrecherML, Johnson DH, Meropol NJ, Moots PL, Thigpen JT, editors.Textbook of uncommon cancer; second edition. West Sussex:John Wiley, 1999: 523-7.Herben VMM, Schellens JHM, Swart M, Gruia G, Vernillet L,Beijnen JH, Ten Bokkel Huinink WW. Phase I and pharmacokineticstudy of irinotecan administered as a low-dose, continuousintravenous infusion over 14 days in patients with malignant solidtumors. J Clin Oncol 1999; 17: 1897-905.Herben VMM, Van Gijn R, Schellens JHM, Schot M, Lieverst J,Hillebrand MJX, Schoemaker NE, Porro MG, Beijnen JH, TenBokkel Huinink WW. Phase I and pharmacokinetic study of a dailytimes 5 short intravenous infusion schedule of 9-aminocamptothecinin a colloidal dispersion formulation in patients with advancedsolid tumors. J Clin Oncol 1999; 17: 1906-14.Hoetelmans RMW, Profijt M, Meenhorst PL, Mulder JW, VanHeeswijk RPG, Beijnen JH. Co-trimoxazole and stavudine interferencein a high-performance liquid chromatographic analysis fordidanosine in human plasma. Ther Drug Monitor 1998; 20: 669-72.Hoetelmans RMW, Van Heeswijk RPG, Profijt M, Mulder JW,Meenhorst PL, Lange JMA, Reiss P, Beijnen JH. Comparison ofthe plasma pharmacokinetics and renal clearance of didanosine inonce and twice daily dosing in HIV-1 infected individuals. AIDS1998; 12: F211-6.Huitema ADR, Holtkamp M, Rodenhuis S, Beijnen JH. Samplingtechnique from central venous catheters proves critical for pharmacokineticstudies. Ther Drug Monitor 1999; 21: 102-4.Jansen G, Mauritz R, Drori S, Sprecher H, Kathmann I, Bunni M,Priest DG, Noordhuis P, Schornagel JH, Pinedo HM, Peters GJ,Assaraf YG. A structurally altered human reduced folate carrierwith increased folic acid transport mediates a novel mechanism ofantifolate resistance. J Biol Chem 1998; 273: 30189-98.119MEDICAL ONCOLOGYGodschalk RW, Maas LM, Van Zandwijk N, Van ‘t Veer LJ,Breedijk A, Borm PJ, Verhaert J, Kleinjans JC, Van Schooten FJ.Differences in aromatic-DNA adduct levels between alveolarmacrophages and subpopulations of white blood cells from smokers.Carcinogenesis 1998;19: 819-25.Kroep JR, Giaccone G, Voorn DA, Smit EF, Beijnen JH, Rosing H,Van Moorsel CJA, Van Groeningen CJ, Postmus PE, Pinedo HM,Peters GJ. Gemcitabine and paclitaxel: Pharmacokinetic andpharmacodynamic interactions in patients with non-small-cell lungcancer. J Clin Oncol 1999; 17: 2190-7.Groenewegen G, De Gast GC. GM-CSF can cause T-cell activation;Results of sequential chemo-immunotherapy. Eur J Cancer1999; 35: 23-4.Herben VMM, Nannan Panday VR, Richel DJ, Schellens JHM,Van der Vange N, Rosing H, Beusenberg FD, Hearn S, Doyle E,Beijnen JH, Ten Bokkel Huinink WW. Phase I and pharmacologicstudy of the combination of paclitaxel, cisplatin, and topotecanadministered intravenously every 21 days as first-line therapy inpatients with advanced ovarian cancer. J Clin Oncol 1999; 17:747-55.Herben VMM, Rosing H, Ten Bokkel Huinink WW, Van ZomerenDM, Batchelor D, Doyle E, Beusenberg FD, Beijnen JH, SchellensJHM. Oral topotecan: bioavailability and effect of food co-administration.Br J Cancer 1999; 80: 1380-6.Kuin A, Aalders M, Lamfers M, Van Zuidam DJ, Essers M, BeijnenJH, Smets LA. Potentiation of anti-cancer drugs at low intratumoralpH induced by the the mitochondrial inhibitor m-iodobenzylguanidine(MIBG) and its analog benzylguanidine (BG). Br JCancer 1999; 79: 793-801.Kuin A, Rutgers M, Van der Valk MA, Beijnen JH, Smets LA.Bioavailability and toxicity of oral administration of m-iodobenzylguanidine(MIBG). Br J Cancer 1999; 79: 802-6.Lambrechts AC, Bosma AJ, Klaver SG, Top B, Perebolte L, Van’t Veer LJ, Rodenhuis S. Comparison of immunocytochemistry,reverse transcriptase polymerase chain reaction and nucleicacid sequence-based amplification for the detection of circulatingbreast cancer cells. Breast Cancer Res Treat 1999; 56: 219-31.
120MEDICAL ONCOLOGYMaliepaard M, Van Gastelen MA, De Jong LA, Pluim D, VanWaardenburg RC, Ruevekamp-Helmers MC, Floot BG, SchellensJHM. Overexpression of the BCRP/MXR/ABCP gene in a topotecan-selectedovarian tumor cell line. Cancer Res 1999; 59: 4559-63.Meerum Terwogt JM, Mandjes IM, Sindermann H, Beijnen JH, TenBokkel Huinink WW. Phase II trial of topically applied miltefosinesolution in patients with skin-metastasized breast cancer. Br JCancer 1999; 79: 1158-61.Meerum Terwogt JM, Schellens JHM, Ten Bokkel Huinink WW,Beijnen JH. Clinical pharmacology of anticancer agents in relationto formulations and administration routes. Cancer Treat Rev 1999;25: 83-101.Nannan Panday VR, De Wit R, Schornagel JH, Schot M, RosingH, Lieverst J, Ten Bokkel Huinink WW, Schellens JHM, BeijnenJH. Pharmacokinetics of paclitaxel administered in combinationwith cisplatin, etoposide and bleomycin in patients with advancedsolid tumors. Cancer Chemother Pharmacol 1999; 44: 349-53.Post J, Vooijs WC, Bast BJEG, De Gast GC. Efficacy of an anti-CD138 immunotoxin and doxorubicin on drug-resistant and drugsensitivemyeloma cells. Int J Cancer 1999; 83: 571-6.Ravaud A, Borner M, Schellens JHM, Geoffrois L, Schoffski P,Wanders J, Hanauske AR. UFT and oral calcium folinate as firstlinechemotherapy for metastatic gastric cancer. Oncology(Huntington NY) 1999; 13: 61-3.Reiser M, Salzberger B, Stiepel A, Ivette A, Hoetelmans RMW,Fätkenheuer G. Virological efficacy and plasma drug concentrationsof nelfinavir plus saquinavir as salvage therapy in HIV-infectedpatients refractory to standard triple therapy. Eur J Med Res1999; 4: 54-8.Reubsaet JLE, Beijnen JH, Belshof EHM, Bouyakhrichan M, BultA, Hop E, Kellekule Y, Van Maanen RJ, Teeuwsen J, UnderbergWJM. Qualitative and quantitative aspects of the degradation ofseveral oligopeptides derived from the antitumour peptide antagonist[Arg 6 ,D-Trp 7,9 ,MePhe 8 ] substance P{6-11}. J PharmBiomed Anal 1999; 19: 277-84.Nannan Panday VR, Hoetelmans RMW, Van Heeswijk RPG,Meenhorst PL, Inghels M, Mulder J-W, Beijnen JH. Paclitaxel inthe treatment of human immunodeficiency virus 1-associatedKaposi’s sarcoma: drug-drug interactions with protease inhibitorsand nonnucleoside reverse transcriptase inhibitors: a case reportstudy. Cancer Chemother Pharmacol 1999; 43: 516-9.Nannan Panday VR, Huizing MT, Van Tellingen O, Hakvoort RA,Willemse PHB, De Graeff A, Vermorken JB, Beijnen JH.Pharmacologic study of Cremophor EL7 administered in cancerpatients with impaired hepatic function receiving paclitaxel. JOncol Pharm Pract 1999; 5: 83-6.Nannan Panday VR, Rosing H, Huizing MT, Koopman FJ, VanWarmerdam LJC, Ten Bokkel Huinink WW, Beijnen JH. Urinaryexcretion of paclitaxel and metabolites in a large series study. JOncol Pharm Pract 1998; 4: 159-64.Nannan Panday VR, Ten Bokkel Huinink WW, Vermorken JB,Rosing H, Koopman FJ, Swart M, Schellens JHM, Beijnen JH.Pharmacokinetics of paclitaxel administered as a 3-hour or 96-hour infusion. Pharmacol Res 1999; 40: 67-74.Nannan Panday VR, Van Warmerdam LJC, Huizing MT,Rodenhuis S, Schellens JHM, Beijnen JH. A single 24-hour plasmasample does not predict the carboplatin AUC from carboplatin-paclitaxelcombinations or from a high dose carboplatin-thiotepa-cyclophosphamideregimen. Cancer Chemother Pharmacol1999; 43: 435-8.Reubsaet JLE, Beijnen JH, Bult A, Van Maanen RJ, Marchal JAD,Underberg WJM. Analytical techniques used to study the degradationof proteins and peptides. Chemical instability. J PharmBiomed Anal 1998; 17: 955-78.Reubsaet JLE, Beijnen JH, Bult A, Van Maanen RJ, Marchal JAD,Underberg WJM. Analytical techniques used to study the degradationof proteins and peptides. Physical instability. J PharmBiomed Anal 1998; 17: 979-84.Reubsaet JLE, Beijnen JH, Van Bennekom WP, Bult A, HoekstraAJ, Hop E, Van Os PJHJ, Teeuwsen J, Underberg WJM.Reduction of Cys 36 -Cys 42 and Cys 64 -Cys 74 disulfide bonds inrecombinant human granulocyte colony stimulating factor. JPharm Biomed Anal 1999; 19: 837-45.Rodenhuis S, De Wit R, De Mulder PHM, Keizer HJ, Sleijfer DTh,Lalisang RI, Bakker P, Mandjes I, Kooi M, De Vries EGE. A multicenterprospective phase II study of high-dose chemotherapy ingerm cell cancer patients relapsing from complete remission. AnnOncol 1999; 12: 1267-74.Rodenhuis S, Huitema ADR, Baars JW, Westermann A, HoltkampMMJ, Schornagel JH, Beijnen JH. Multiple courses of cyclophosphamide,thiotepa and carboplatin: managing toxicity by dosereduction and pharmacokinetic monitoring. In: Dicke KA, KeatingA, editors. Autologous blood and marrow transplantation: proceedingsof the ninth international symposium; Arlington, Texas,1998: 422-34.Nannan Panday VR, Van Warmerdam LJC, Huizing MT, TenBokkel Huinink WW, Schellens JHM, Beijnen JH. A limited-samplingmodel for the pharmacokinetics of carboplatin administered incombination with paclitaxel. J Cancer Res Clin Oncol 1999; 125:615-20.Rosing H, Hillebrand MJX, Jimeno JM, Gomez A, Floriano P,Faircloth G, Henrar REC, Vermorken JB, Cvitkovic E, Bult A,Beijnen JH. Quantitative determination of ecteinascidin 743 inhuman plasma by miniaturized high-performance liquid chromatographycoupled with electrospray ionization tandem mass spectrometry.J Mass Spectrom 1998; 33: 1134-40.
Rosing H, Ten Bokkel Huinink WW, Van Gijn R, Rombouts RFM,Bult A, Beijnen JH. Comparative open, randomized, cross-overbioequivalence study of two intravenous dexrazoxane formulations(Cardioxane7 and ICRF-187) in patients with advanced breastcancer treated with 5-fluorouracil-doxorubicin-cyclophosphamide(FDC). Eur J Drug Metab Pharmacokinet 1999; 24:69-77.Straathof CS, Van den Bent MJ, Loos WJ, Vecht CJ, SchellensJHM. The accumulation of topotecan in 9L glioma and in brainparenchyma with and without dexamethasone administration. JNeuro-Oncol 1999; 42: 117-22.Taal BG, Hoefnagel C, Rutgers M. Carcinoid tumors. N Engl JMed 1999; 341: 454.121MEDICAL ONCOLOGYRosing H, Van Zomeren DM, Doyle E, Ten Bokkel Huinink WW,Schellens JHM, Bult A, Beijnen JH. Quantification of topotecanand its metabolite N-desmethyltopotecan in human plasma, urineand faeces by high-performance liquid chromatographicmethods. J Chromatogr B 1999; 727: 191-203.Schouwink JH, Baas P, Rutgers EJTh, Zoetmulder FAN.Malignant pleural mesothelioma. Eur Respir J 1999; 13: 706.Schouwink JH, Korse CM, Bonfrer JM, Hart AA, Baas P.Prognostic value of the serum tumour markers Cyfra 21-1 and tissuepolypeptide antigen in malignant mesothelioma. Lung Cancer1999; 25: 25-32.Schrama JG, Rodenhuis S. Dose-intense chemotherapy for locallyadvanced breast cancer. Curr Oncol Rep 1999; 1: 23-30.Sessa C, Ten Bokkel Huinink WW, Du Bois A. Oxaliplatin in ovariancancer. Ann Oncol 1999; 10 (suppl 1): 55-7.Sneeuw KC, Aaronson NK, Sprangers MA, Detmar SB, WeverLD, Schornagel JH. Evaluating the quality of life of cancerpatients: assessments by patients, significant others, physiciansand nurses. Br J Cancer 1999; 81: 87-94.Sparidans RW, Den Hartigh J, Cremers S, Beijnen JH, Vermeij P.Semi-automated liquid chromatographic analysis of pamidronatein urine after derivatization with 1-naphthylisothiocyanate. JChromatogr B 1999; 730: 95-9.Sparidans RW, Henrar REC, Jimeno JM, Faircloth G, Floriano P,Beijnen JH. Bioanalysis of thiocoraline, a new marine antitumoraldepsipeptide, in plasma by high-performance liquid chromatographywith fluorescence detection. J Chromatogr B 1999; 726: 255-60.Sparidans RW, Kettenes-van den Bosch JJ, VanTellingen O,Nuyen B, Henrar REC, Jimeno JM, Faircloth G, Floriano P,Rinehart KL, Beijnen JH. Bioanalysis of aplidine, a new marineantitumoral depsipeptide, in plasma by high-performance liquidchromatography after derivatization with trans-4’-hydrazino-2-stilbazole.J Chromatogr B 1999; 729: 43-53.Sparidans RW, Taal BG, Beijnen JH. Bioanalysis of meta-iodobenzylguanidinein plasma by high-performance liquid chromatographyafter derivatization with benzoin. J Chromatogr B 1999;730: 193-9.Taal BG, Westerman H, Boot H, Rankin E. Clinical and endoscopicfeatures of melanoma metastases in the upper GI tract.Gastrointest Endosc 1999; 50: 261-4.Ten Bokkel Huinink WW, De Swart CA, Van Toorn DW, Morack G,Breed WP, Hillen HF, Van der Hoeven JJ, Reed NS, Fairlamb DJ,Chan SY, Godfrey KA, Kristensen GB, Van Tinteren H, Ehmer B.Controlled multicentre study of the influence of subcutaneousrecombinant human erythropoietin on anaemia and transfusiondependency in patients with ovarian carcinoma treated with platinum-basedchemotherapy. Med Oncol 1998;15: 174-82.Theuws JC, Muller SH, Seppenwoolde Y, Kwa SL, Boersma LJ,Hart GA, Baas P, Lebesque JV. Effect of radiotherapy and chemotherapyon pulmonary function after treatment for breast cancerand lymphoma: a follow-up study. J Clin Oncol 1999; 17:3091-100.Van Asperen J, Van Tellingen O, Schinkel AH, Beijnen JH.Comparative pharmacokinetics of vinblastine after a 96-hour continuousinfusion in wild-type mice and mice lacking mdr1a P-glycoprotein.J Pharmacol Exp Ther 1999; 289: 329-33.Van Asperen J, Van Tellingen O, Tijssen F, Schinkel AH, BeijnenJH. Increased accumulation of doxorubicin and doxorubicinol incardiac tissue of mice lacking mdr1a P-glycoprotein. Br J Cancer1999; 79: 108-13.Van Baarle D, Hovenkamp E, Kersten MJ, Klein MR, Miedema F,Van Oers MHJ. Direct Epstein-Barr virus typing on peripheralblood mononuclear cells: no association between EBV type 2infection or superinfection and the development of acquiredimmunodeficiency syndrome-related non-Hodgkin’s lymphoma.Blood 1999; 93: 3949-55.Van Cutsem E, Cunningham D, Ten Bokkel Huinink WW, Punt CJ,Alexopoulos CG, Dirix L, Symann M, Blijham, GH, Cholet P, Fillet G,Van Groeningen C, Vannetzel JM, Levi F, Panagos G, Unger C, WilsJ, Cote C, Blanc C, Herait P, Bleiberg H. Clinical activity and benefitof irinotecan (CPT-11) in patients with colorectal cancer truly resistantto 5-fluorouracil (5-FU). Eur J Cancer 1999; 35: 54-9.Van Gijn R, Ten Bokkel Huinink WW, Rodenhuis S, Vermorken JB,Van Tellingen O, Rosing H, Van Warmerdam LJC, Beijnen JH.Topoisomerase I/II inhibitor intoplicine administered as a 24-hourinfusion: phase I and pharmacologic study. Anticancer Drugs1999; 10: 17-23.
122MEDICAL ONCOLOGYVan Gijn R, Van Tellingen O, Haverkate E, Kettenes-van denBosch JJ, Bult A, Beijnen JH. Pharmacokinetics and metabolismof the staurosporine analogue CGP 41 251 in mice. Invest NewDrugs 1999; 17: 29-41.Van Heeswijk RPG, Hoetelmans RMW, Harms R, Meenhorst PL,Mulder JW, Lange JMA, Beijnen JH. Simultaneous quantitativedetermination of the HIV protease inhibitors amprenavir, indinavir,nelfinavir, ritonavir, and saquinavir in human plasma by ion-pairhigh-performance liquid chromatography with ultraviolet detection.J Chromatogr B 1998; 719: 159-68.Van Heeswijk RPG, Veldkamp AI, Hoetelmans RMW, Mulder JW,Schreij G, Hsu A, Lange JMA, Beijnen JH, Meenhorst PL. The steady-stateplasma pharmacokinetics of indinavir alone and in combinationwith low dose of ritonavir in twice daily dosing regimensin HIV-1 infected individuals. AIDS 1999; 13: F95-9.Van Helvoort A, De Brouwer A, Ottenhof R, Brouwers JFHM,Wijnholds J, Beijnen JH, Rijneveld A, Van der Poll T, Van der ValkMA, Majoor D, Voorhout W, Witz KWA, Oude Elferink RPJ, BorstP. Mice without phosphatidylcholine transfer protein have nodefects in the secretion of phosphatidylcholine into bile or intolung airspaces. Proc Natl Acad Sci USA 1999; 96: 11501-6.Van Lent-Evers NA, Mathot RAA, Geus WP, Van Hout BA, VinksAATMM. Impact of goal-oriented and model-based clinical pharmacokineticdosing of aminoglycosides on clinical outcome: acost-effectiveness analysis. Ther Drug Monitor 1999; 21: 63-73.Van Maanen MJ, Beijnen JH. Liquid chromatographic—massspectrometric determination of the novel, recently identifiedthioTEPA metabolite, thioTEPA-mercapturate, in urine. JChromatogr B 1999; 732: 73-80.Van Maanen MJ, Brandt AC, Damen JMA, Beijnen JH.Degradation study of thiotepa in aqueous solutions. Int J Pharm1999; 179: 55-64.Van Maanen MJ, Thijhof IM, Damen JMA, Versluis C, Kettenesvanden Bosch JJ, Heck AJR, Rodenhuis S, Beijnen JH. A searchfor new metabolites of N',N'',N'''-triethylenethiophosphoramide.Cancer Res 1999; 59: 4720-4.Van Tellingen O, Beijnen JH, Verweij J, Scherrenberg EJ, NooijenWJ, Sparreboom A. Rapid esterase-sensitive breakdown ofpolysorbate 80 and its impact on the plasma pharmacokinetics ofdocetaxel and metabolites in mice. Clin Cancer Res 1999; 5:2918-24.Van Tellingen O, Huizing MT, Nannan Panday VR, Schellens JHM,Nooijen WJ, Beijnen JH. Cremophor EL causes (pseudo)-nonlinearpharmacokinetics of paclitaxel in patients. Br J Cancer 1999;81: 330-5.Van Tellingen O, Kemper M, Tijssen F, Van Asperen J, Nooijen WJ,Beijnen JH. High-performace liquid chromatographic bio-analysisof PSC 833 in human and murine plasma. J Chromatogr B 1998;719: 251-7.Van Zuylen L, Schellens JHM, Goey SH, Pronk LC, De Boer-Dennert MM, Loos WJ, Ma J, Stoter G, Verweij J. Phase I andpharmacologic study of the arotinoid Ro 40-8757 in combinationwith cisplatin and etoposide in patients with non-small cell lungcancer. Anticancer Drugs 1999; 10: 361-8.Veldkamp AI, Van Heeswijk RPG, Hoetelmans RMW, MeenhorstPL, Mulder JW, Lange JMA, Beijnen JH. Rapid quantification ofdelavirdine, a novel non-nucleoside reverse transcriptase inhibitor,in human plasma using isocratic reversed-phase high-performanceliquid chromatography with fluorescence detection. JChromatogr B 1999; 727: 151-7.Vermorken JB, Ten Bokkel Huinink WW, Kobierska A, Van derBurg ME, Forni M, Piccart MJ, Van der Putten E. Phase I study ofhigh-dose epirubicin in platinum-pretreated patients with ovariancarcinoma. Oncology (Basel) 1999; 57: 10-6.Verschraagen M, Koks CHW, Schellens JHM, Beijnen JH. P-glycoproteinsystem as a determinant of drug interactions. The caseof digoxin-verapamil. Pharmacol Res 1999; 40: 301-6.Westermann AM, Holtkamp MMJ, Linthorst GAM, Van LeeuwenL, Willemsen EJM, Van Dijk W, Nooijen WJ, Baars JW, SchornagelJH, Rodenhuis S. At home management of aplastic phase followinghigh-dose chemotherapy with stem cell rescue for hematologicand non-hematologic malignancies. Ann Oncol 1999; 10:511-7.Van Maanen MJ, Van Ooijen RD, Zwikker JW, Huitema ADR,Rodenhuis S, Beijnen JH. Determination of N,N’,N’’-triethylenthiophosphoramideand its active metabolite N,N’,N’’-triethylenphosphoramidein plasma and urine using capillary gas chromatography.J Chromatogr B 1998; 719: 103-12.Woll PJ, Judson I, Lee SM, Rodenhuis S, Nielsen OS, Buesa JM,Lorigan PC, Leyvraz S, Hermans C, Van Glabbeke M, Verweij J.Temozolomide in adult patients with advanced soft tissue sarcoma:a phase II study of the EORTC soft tissue and bone sarcomagroup. Eur J Cancer 1999; 35: 410-2.Van Meerbeeck JP, Baas P, Debruyne C, Groen HJ, Manegold C,Ardizzoni A, Gridelli C, Van Marck EA, Lentz M, Giaccone G. APhase II study of gemcitabine in patients with malignant pleuralmesothelioma. European Organization for Research andTreatment of Cancer Lung Cancer Cooperative Group. Cancer1999; 85: 2577-82.Zuetenhorst H, Taal BG, Boot H, Valdes Olmos R, Hoefnagel C.Longterm palliation in metastatic carcinoid tumours with variousapplications of meta-iodobenzylguanidin (MIBG): pharmacologicalMIBG, 131I labeled MIBG and the combination. Eur JGastroenterol Hepatol 1999; 11: 1157-64.
Full papers in pressAckerstaff AH, Hilgers FJM, Meeuwis C, Knegt P, Weenink C.Pulmonary function, pre and post total laryngectomy. ClinOtolaryngol 1999 (in press).Boogerd W, Beijnen JH. Methylphenidate for congenital cerebralpalsy with choreo-athetosis. Ann Intern Med 1999 (in press).Boogerd W, Tjahja IS, Van de Sandt MM, Beijnen JH. Penetrationof idarubicin into malignant brain tumor tissue. J Neuro-Oncol1999 (in press).De Gast GC, Klümpen H-J, Vyth-Dreese FA, Kersten MJ, VerraNCV, Sein J, Batchelor D, Nooijen WJ, Schornagel JH. Phase I/IItrial of combined immunotherapy with subcutaneous GM-CSF,low dose IL-2 and IFNa in progressive metastatic melanoma andrenal cell carcinoma. Clin Cancer Res 1999 (in press).Groenewegen GC, De Gast GC. Sequential chemo-immunotherapy(SCIT) for metastatic melanoma: outpatient treatment withdacarbazine, molgramostim, interleukin-2, and interferon-alpha.Clin Cancer Res 1999 (in press).Nuyen B, Bouma M, Henrar REC, Jimeno JM, Manada C, Bult A,Beijnen JH. Compatibility and stability of aplidine in infusion devicesand its hemolytic and precipitation potential upon intravenousadministration. Anti-Cancer Drugs 1999 (in press).Paridaens R, Biganzoli L, Bruning PF, Klijn JGM, Gamucci T,Houston S, Coleman R, Schachter J, Van Vreckem A, Sylvester R,Awada A, Wildiers J, Piccart M. Taxol ® versus doxorubicin as firstlinesingle agent chemotherapy for metastatic breast cancer - anEORTC randomized study with crossover. J Clin Oncol 1999 (inpress).Pluim D, Maliepaard M, Van Waardenburg RCAM, Beijnen JH,Schellens JHM. 32 P-postlabeling assay for the quantification ofthe major platinum-DNA adducts. Anal Biochem 1999 (in press).Reijers MHE, Weverling GJ, Hart AAM, Weigel HM, Ten Kate RW,Mulder JW, Reiss P, Schuitemaker H, Hoetelmans RMW, LangeJMA.Toxicity and drug exposure in a quadruple drug regimen inHIV–1 infected patients. AIDS 1999 (in press).Rodenhuis S. High-dose chemotherapy in solid tumors [editorial].Revista de Oncología 1999 (in press).123MEDICAL ONCOLOGYHoitink MA, Beijnen JH, Bult A, Damen MA, Van der HouwenOAGJ, Kruijtzer JAW, Tibben MM, Wiese G, Underberg WJM.Degradation of azaglycinamido residues in model tripeptides derivedfrom goserelin. J Pharm Sci 1999 (in press)..Koks CHW, van Heeswijk RPG, Veldkamp AI, Meenhorst PL,Mulder JW, Van der Meer JTM, Beijnen JH, Hoetelmans RMW.Itraconazole as an alternative for ritonavir liquid formulation whencombined with saquinavir. AIDS 1999 (in press).Rosing H, Man WY, Doyle E, Bult A, Beijnen JH. Bio-analyticalchromatographic method validation: a review of current practicesand procedures. J Liq Chromatogr Rel Techn 1999 (in press).Rosing H, Van Warmerdam LJC, Ten Bokkel Huinink WW,Dubbelman AC, Rodenhuis S, Beijnen JH. Pharmacokinetics andmetabolism of docetaxel administered as an one hour intravenousinfusion during a phase II clinical trial. Cancer ChemotherPharmacol 1999 (in press).Kuiper RAJ, Malingré MM, Beijnen JH, Schellens JHMS.Anaphylactic reaction after first ingestion of oral cyclosporin(Neoral ® ) capules. Ann Pharmacother 1999 (in press).Schellens JHM, Beijnen JH. Cisplatin. In: Ratain MJ, Tempero M,Skosey C, editors. Oncology therapeutics: a quick referenceguide. Orlando: Saunders, 1999 (in press).Malingré MM, Meerum Terwogt JM, Beijnen JH, Rosing H,Koopman FJ, Van Tellingen O, Duchin KKL, Ten Bokkel HuininkWW, Swart M, Schellens JHM. Clinical pharmacology of oralpaclitaxel in a dose escalating study. Clin Cancer Res 1999 (inpress).Meerum Terwogt JM, Tibben MM, Schellens JHM, McGahen L,Beijnen JH. Validated method for the determination of platinumfrom a liposomal source (SPI-77) in plasma using graphite furnaceatomic absorption spectrometry with Zeeman correction.Fresenius J Anal Chem 1999 (in press).Newell DR, McLeod H, Schellens JHM. The pharmacology of anticancerdrugs. In: Souhami RL, Tannock I, Hohenberger P, HoriotJC, editors. Oxford Textbook of Oncology. Oxford: OxfordUniversity Press, 1999 (in press).Nuyen B, Bouma M, Henrar REC, Bette P, Bult A, Beijnen JH. Invitro compatibility studies with the experimental anticancer agentBIBX1382BS. Int J Pharm 1999 (in press).Schellens JHM, Beijnen JH. Topotecan. In: Ratain MJ, TemperoM, Skosey C, editors. Oncology therapeutics: a quick referenceguide. Orlando: Saunders, 1999 (in press).Sparidans RW, Veldkamp AI, Hoetelmans RMW, Beijnen JH. Animproved and simplified liquid chromatographic assay for adefovirin plasma using derivatization with chloroacetaldehyde.J Chromatogr B 1999 (in press).Theuws JCM, Seppenwoolde Y, Kwa SLS, Boersma LJ, DamenEMF, Baas P, Muller SH, Lebesque JV. Recovery of local pulmonaryinjury 18 to 48 months after irradiation for lymphoma orbreast cancer. Int J Radiat Oncol Biol Phys 1999 (in press).Van Dijk AMC, Kessler FL, Stadhouders-Keet SAE, Verdonck LF,De Gast GC, Otten HG. Selective depletion of major and minorhistocompatibility antigen reactive T cells; Towards prevention ofacute graft-versus-host disease. Br J Hematol 1999 (in press).
124MEDICAL ONCOLOGYVeldkamp AI, Hoetelmans RMW, Lange JMA, Beijnen JH,Meenhorst PL. Ritonavir enables combined therapy with rifampinand saquinavir. Clin Infect Dis 1999 (in press).Veldkamp AI, Mulder JW, Meenhorst PL, Lange JMA, Beijnen JH,Hoetelmans RMW. Determination of the novel antiretroviral drugefavirenz in human plasma using high-performance liquid chromatographywith ultraviolet detection. J Chromatogr B 1999 (inpress).Rodenhuis S. Hoge dosis chemotherapie met stamcelondersteuningbij gemetastaseerd mammacarcinoom. Tijdschr Kanker1999; 23: 8-12.Schellens JHM, Meerum Terwogt JM, Malingré MM, Beijnen JH.Orale therapie met taxanen. In: Schellens JHM, Meinders AE,Vermeij P, redactie. Medicamenteuze therapie: condolidatie eninnovatie. Leiden: Boerhaave Commissie voor PostacademischOnderwijs in de Geneeskunde, 1999: 177-85.Veldkamp AI, Sparidans RW, Hoetelmans RMW, Beijnen JH.Rapid determination of abacavir in human plasma using high-performanceliquid chromatography with ultraviolet detection.J Chromatogr B 1999 (in press).Vielvoye-Kerkmeer APE, Bergman W. Letter to the editor. ThePain Clinic 1999 (in press).Vielvoye-Kerkmeer APE, Mattern C, Uiterdaal M. Transdermal fentanylin opioid-naive cancer patients. J Pain Symptom Manage1999 (in press).Vielvoye-Kerkmeer APE, Van der Weide M, Mattern C. Letter tothe Editor. J Pain Symptom Manage 1999 (in press).Vulcan TG, Zhu TC, Rodrigues C, His A, Fraker DL, Baas P,Murrer L, Star WM, Yodh AG, Hahn SM. In vivo light measurementduring intraperitoneal photodynamic therapy: a comparison oftwo dosimetry systems. Lasers Surg Med 1999 (in press).Schellens JHM. Variabiliteit in ‘gevoeligheid’ voor farmaca. In: VanRee JM, Breimer DD, redactie. Algemene farmacologie.Maarssen: Elsevier/Bunge, 1999: 113-30.Taal BG, Hoefnagel C, Boot H, De Jong D, Rutgers. Carcinoidetumoren van de darm: ontwikkelingen binnen Nederland in diagnostieken palliatieve behandeling. Ned Tijdschr Geneeskd 1999;143: 445-51.Taal BG, Van Loon HJ, Kahn N, De Jong D, Vasen HFA, Van ’tVeer. De rol van genetische factoren bij het ontstaan van maagcarcinoom.Ned Tijdschr Geneeskd 1999; 143: 342-6.Van der Weide M, Vielvoye-Kerkmeer APE. Pijnbestrijding bij terminalekankerpatiënten. Mod Med 1999; 5: 455-9.Van Dijk AMC. T cell reactivity against keratinocytes in acute graftversus-hostdisease after bone marrow transplantation [dissertation].Utrecht: University of Utrecht, 1999.Local papers and thesesBoogerd W. Neuro-oncologie: als de prognose nog maar eenpaar maanden bedraagt. Neurologie Actueel 1999; 2: 1-5.Van Zandwijk N, Smit EF, Vansteenkiste J. Oncogenese. In:Demedts M, Dijkman JH, Hilversing C, Postma DS, redactie.Longziekten. Assen: Van Gorcum/ Leuven: Universitaire Pers,1999: 208-14.Bronner GM, Koks CHW, Beijnen JH. Thalidomide opnieuw in debelangstelling. [ingezonden] Ned Tijdschr Geneeskd 1999; 143:122.Koning CCE, Belderbos JSA, Van Zandwijk N. Radiotherapie. In:Demedts M, Dijkman JH, Hilversing C, Postma DS, redactie.Longziekten. Assen/Leuven: Van Gorcum/Universitaire Pers,1999: 531-5.Kuiper RAJ, Schellens JHM, Beijnen JH, Blijham GH, Voest EE.Grote verwachtingen van nieuwe aanpak: tumorangiogenese alsdoelwit voor kankertherapie. Pharm Weekbl 1999; 134: 572-7.Meerum Terwogt JM. Clinical pharmacology of anticancer agentsin relation to formulations and administration routes [disseration].Utrecht: University of Utrecht, 1999.Rodenhuis S, De Vries EGE: Hoge dosis chemotherapie metstamcelondersteuning bij solide tumoren van volwassenen [capitaselecta]. Ned Tijdschr Geneeskd 1999; 143: 731-8.Van Zandwijk N, Vansteenkiste J, Festen J. Algemeen. In:Demedts M, Dijkman JH, Hilversing C, Postma DS, redactie.Longziekten. Assen: Van Gorcum/ Leuven:Universitaire Pers,1999: 755-73.Vanuytsel LJ, Van Zandwijk N. Longafwijkingen door ioniserendestraling. In: Demedts M, Dijkman JH, Hilversing C, Postma DS,redactie. Longziekten. Assen: Van Gorcum/ Leuven: UniversitairePers, 1999: 1262-9.Vasen HFA, Nagengast FM, Griffioen G, Kleibeuker JH, MenkoFH, Taal BG. Periodiek onderzoek bij personen met een belastefamilie anamnese voor colorectaal carcinoom. Ned TijdschrGeneeskd 1999; 143: 1211-4.Vielvoye-Kerkmeer APE, Meijler WJ. Praktische aspecten van depijnbestrijding. In: Wesseling H, Neef C, De Graeff PA, redactie.Algemene farmacotherapie. Houten/Diemen: Bohn Stafleu VanLoghum, 1999: 333-43.Vielvoye-Kerkmeer APE, Van der Weide M. Behandeling van pijndoor kanker. Tijdschr Kanker 1999; 23: 20-2.
125Vielvoye-Kerkmeer APE, Van Luyt PA. Zin en onzin over dystrofie.Mod Med 1999; 6: 558-61.Westermann AM. Novel applications of growth factors in solidtumors [dissertation]. Amsterdam: University of Amsterdam,1999.Zoetmulder FAN, Van der Vange N, Witkamp AJ, Kaag MM, BootH, Beijnen JH. Hypertherme intraperitoneale chemotherapie(HIPEC) bij patiënten met pseudomyxoma peritonei of peritoneummetastasenvan colorectaal carcinoom; gunstige eersteervaringen in het Nederlands Kanker Instituut. Ned TijdschrGeneeskd 1999; 143: 1863-8.MEDICAL ONCOLOGYLocal papers in pressJonkers DAP, Kerbusch T, Schellens JHM, Beijnen JH. Ifosfamideencephalopathie. Mechanisme, behandeling en preventie. PharmWeekbl 1999 (in press).Meijler WJ, Vielvoye-Kerkmeer APE. Farmacotherapie van benignepijn. Handboek Pijnbestrijding 1999 (in press).Rodenhuis S, Beijnen JH. Principes van medicamenteuze therapie.In: Voûte PA, Veenhof CHN, redactie. Behandeling van kanker.Houten: Bohn Stafleu Van Loghum, 1999 (in press).Vielvoye-Kerkmeer APE, Bergman W. Help, mijn benen doen zozeer; een patiënte met een idiopathische erythromelalgie. TijdschrHuisartsgeneeskd 1999 (in press).Vielvoye-Kerkmeer APE, Van Luijt PA. Complex regional pain syndrome.Tijdschr Huisartsgeneeskd 1999 (in press).
126SURGICAL ONCOLOGYXI Division of SurgicalOncologySurgical Oncology Board:Bin Kroon and Fons BalmBoardBBR Kroon MD PhD (Head)AJM Balm MD PhD FRCS FACSPermanent academic staffGeneral SurgeryBBR Kroon MD PhD (Head)OE Nieweg MD PhD, EJTh Rutgers MD PhD,F Van Coevorden MD PhD, FAN Zoetmulder MD PhDHead and Neck SurgeryFJM Hilgers MD PhD (Head)AJM Balm MD PhD FRCS FACS, S Gonggrijp DDS,FHM Kroon DDS PhD, IB Tan MD PhD, AP TimmersGynecologyACM Van Lindert MD PhD, (Head)M Van Beurden MD PhD, N Van der Vange MD PhDUrologyS Horenblas MD PhD (Head)W Meinhardt MD PhDPlastic and Reconstructive SurgeryKE Bos MD PhD (Head)JB De Boer MD (until May),RP Noordanus MD (until October)AnesthesiologyPFE Schutte MD (Head)CL Blackburn MMBS FRCA (until February),D Buitelaar MD, MM Kaag MD,JM Ronday MD (from February), J Visscher MDOther academic staff involved in research activitiesAH Ackerstaff PhD, N Bijker MD, RBJ De Bondt MD,IF Faneyte MD, M Govaert MD, M Heetveld MD,L Jansen MD, R Kaas MD, N Kimmings MD,WMC Klop MD, R Lewicz MD, M Piek-Den Hartog MD,TA Roeleveld MD, LJA Strobbe MD, PJ Tanis MD,CJ Van As MSc, SAJM Van der Veen MD,AJ Witkamp MD, CL Zuur MDUndergraduate studentsW Deenik, CMG Dekker BSc, JDH De Vries,ME Grunstra, E Hensen, RG Houtkamp, M Koppe,ELAR Mutsaerts, M Raming, GK Roozendaal, M Smit,D Van PollFellowsA Bex MD, MP Copper MD PhD, PHP Davids MD PhD,E De Bree MD, W IJzerman MD, JWS Merkus MD,KDHM Keuning MD DDS, HSA Oldenburg MD,IGM Tjakra MD, LAE Woerdeman MDSecretaryE Van Damme, GMM Van ZuilenResearch funded positions (full-time equivalents)Clinical permanent: 2.2Clinical project: 4.0IntroductionThe Division of Surgical Oncology focused on its mainthemes of preoperative staging, organ preservation andreconstructive surgery. The unique institutional experiencewith sexuality preserving cystectomy and neobladderreconstruction resulted in successful preservation ofcontinence and sexual function for 25 patients. The significantimprovement of disease-free survival in peritonealpseudomyxoma by HIPEC (Hyperthermic IntraperitonealChemotherapy) was consolidated and is now recognizedas the treatment of choice. The value of this method incolorectal cancer is being studied in the framework of aprospective randomized trial, supported by the HealthInsurance Council Fund for Investigative Medicine.Hyperthermic intrapleural chemotherapy (HIPLEC), avariant of this treatment modality, started in patients withpleural metastases of limited mesothelioma or thymoma.A major achievement in the development of newsurgical treatments is the sentinel node procedure whichhas now made the practice of elective axillary dissectionobsolete in patients with breast cancer. The division wasactively involved in organizing the First InternationalCongress on the Sentinel Node in Diagnosis andTreatment of Cancer, held in Amsterdam in cooperation
with the Free University. This successful event wasattended by more than 700 delegates.The organ preserving treatment of advanced stage IVhead and neck squamous cell carcinoma by RADPLAT(super-selective intra-arterial infusion of high dosecisplatin and concomitant radiotherapy) was successfullycontinued in close collaboration with Divisions IX(Radiotherapy), X (Medical Oncology) and XIII (DiagnosticOncology). A phase II study was completed in 76evaluable patients, demonstrating a high loco-regionalcomplete response rate of 88%. A randomized studycomparing intravenous (RADPLAT i.v.) and intra-arterialinfusion of cisplatin (RADPLAT i.a.) plus concomitantradiotherapy started at the end of 1999.In cooperation with Divisions IV (Immunology), X(Medical Oncology) and XIII (Diagnostic Oncology),perioperative immunotherapy and immuno-monitoringcommenced in renal cancer patients and head and neckcancer patients. Continued collaboration with theDivisions VIII (Experimental Therapy), IX (Radiotherapy)and Departments of Radiotherapy and Otolaryngology/Head and Neck Surgery of the Catholic University Leuvenresulted in the first hypoxia measurements in freshoperation specimens of head and neck cancer.In addition to their traditional clinical program of organpreservation and preoperative staging, the surgicaloncological specialties will concentrate on furtherdevelopment of translational research, with emphasis onprognostic markers and the development of experimentalanimal tumor model systems, in close collaboration withDivisions VI (Tumor Biology), VIII (Experimental Therapy)and XIII (Diagnostic Oncology).MelanomaAJM Balm, D Batchelor, JMG Bonfrer 2 , GC De Gast 1 ,JDH De Vries, CA Hoefnagel 2 , SP Israëls 1 , L Jansen,MJ Kersten 1 , SH Muller 2 , GK Roozendaal,LJA Strobbe 3 , PJ Tanis, RA Valdés Olmos 2 , D Van Poll,BBR Kroon, OE NiewegLymphatic mapping with selective lymphadenectomyLymphatic mapping with sentinel node biopsy can beused to stage the regional lymph node field and to selectpatients for therapeutic regional lymph node dissection.Lymphoscintigraphy is one of the three techniques usedto aid in the identification of a sentinel node. Theaccuracy of this technique to determine the number ofsentinel nodes was investigated in 199 patients and wasfound to be 77%. In 23% of the patients scintigraphysuggested too few or too many sentinel nodes. Theprinciple reasons for discrepancies were non-visualizationof a lymphatic duct on the dynamic (early) images andthe limited resolution of the gamma camera.Drainage from melanomas in the head and neck is themost difficult to map. The sentinel node could beidentified in 90% of the patients with a melanoma in thisregion. The need for a two-tracer ( 99m Tc-nanocolloid,Patent Blue Dye) approach was established because47% of the nodes were missed with one of the tracers.The sensitivity for finding lymph node metastases was80%.A study was undertaken to analyze sentinel nodesoutside regular lymphatic fields. In the 379 patientsstudied, this phenomenon was encountered 25 times(7% incidence). The majority of these nodes wasretrieved. A number of previously unknown drainagepatterns were discovered. In four patients, such anabnormally situated node was involved with metastaticdisease. The relevance of these findings extends to thefollow-up of melanoma patients in general. The latter twostudies were done in cooperation with the UniversityHospital Groningen.The division is one of the two European participants inthe international randomized trial to determine potentialbenefits of lymphatic mapping in local-regional controland survival. That trial has now accrued well over 1,400patients and will be closed in the year 2000. Analysis of551 patients in this trial revealed that lymphatic mappingperformed with lymphoscintigraphy, a gamma raydetection probe plus a blue dye, was more successful(99.1%) than lymphatic mapping performed with blue dyealone (95.2%) (p = 0.014). After a new participatingcenter had completed the 30-case learning phase, thesuccess of sentinel node identification was independentof the center’s case volume or experience in the trial.Notes1 Division X.2 Division XIII.3 Canisius Wilhelmina Hospital, Nijmegen.Isolated Limb Perfusion (ILP) for malignanttumors of the limbsJ Clarke, AMM Eggermont 1 , P Gustafson 6 ,JM Klausner 4 , FJ Lejeune 2 , D Liénard 2 , PM Schlag 5 ,H Schraffordt Koops 3 , G Steinmann 7 , GW Van Slooten,BBR Kroon, OE NiewegLimb salvage by ILP with Tumor Necrosis Factor alpha andMelphalan in patients with locally advanced soft tissuesarcomasLimb salvage in patients with ‘irresectable’ soft tissuesarcomas (STS) conventionally treated by anatomic orfunctional amputation was investigated in a large internationalmulti-institutional study. ILP with Tumor NecrosisFactor alpha (TNFα) + Melphalan (M) was given asinduction biochemotherapy to obtain local control and/ormake limb sparing surgery possible. A total of 246patients with locally advanced STS were offered an ILPwith TNF + M. There were 55% primary tumors, 45%recurrent tumors, 22% multiple tumors and 15%concurrent known metastatic disease. Thirteen percent of127SURGICAL ONCOLOGY
128SURGICAL ONCOLOGYthe patients had received previous radiotherapy and 15%chemotherapy. In 46% the diameter measured >10 cm.Grade III tumors were diagnosed in 66%. The majority ofpatients (222) underwent one ILP of 90 minutes at 39—400C with 2—4 mg TNF + Melphalan (10—13 mg/l limbvolume). The first 62 patients also received Interferon-γ.Two to four months later a delayed marginal resection ofthe tumor remnant was done in 75% of cases. All caseswere reviewed by two independent committees whichagreed that for 80% (196 patients) ILP offered the onlychance of limb salvage: 67% were otherwise clear cutamputation cases and 13% were resectable cases butwith severe loss of function. Major tumor responsesoccurred in 75%, rendering tumors resectable in mostcases. The following response rates were achieved:complete response in 28%, partial response in 47%, nochange (17%), progressive disease (6%), missing values(1%). At median follow up of >3 years, limb salvage wasachieved in 71% of the 196 patients considered justifiedILP-candidates by independent reviews. Regional toxicitywas limited. Systemic toxicity was minimal/moderate,easily managed with no toxic deaths. Matched-pairanalysis with cases from the Scandinavian STS-databaseshowed TNF-ILP had no negative effect on survival (p =0.96). This study demonstrates that TNF based ILP is anew and effective option for the limb sparingmanagement of locally advanced extremity STS. TNFdestroys tumor vessels and increases the Melphalanuptake by the tumor four-fold as has recently beenshown by the Rotterdam-perfusion program explainingthe synergistic anti-tumor effects. TNF is now approvedand registered in Europe for ILP of locally advancedgrade II—III extremity soft tissue sarcomas.Notes1 Dr Daniel den Hoed Cancer Center, Rotterdam.2 Centre Pluridisciplinaire d’Oncologie, Lausanne.3 University Hospital, Groningen.4 University Hospital, Tel-Aviv.5 Robert-Roessle University Clinic, Berlin.6 University Hospital, Lund.7 Boehringer Ingelheim Company, Germany.Figure XI.IThe nasal airflow inducing manoeuvre (NAIM) with watermanometer connected to one nostril through a tube with an‘olive’ and the other nostril closed with a finger, to demonstratethe negative pressure in the nasal cavity by displacement of thewater column towards the nose.Head & Neck OncologyAH Ackerstaff, AC Begg 1 , KE Bos, JM Coco Martin 1 ,MP Copper 2 , LDA Dorresteijn 3, 12 , S Gonggrijp,AAM Hart 4 , K Haustermans 5 , KDHM Keuning 2, 6 ,RB Keus 4 , S Keijzers 7 , WMC Klop, BBR Kroon,FHM Kroon 6 , RJAM Michalides 8 , RP Noordanus,BMR Op de Coul 9 , FA Pameijer 10 , CRN Rasch 4 ,JH Schornagel 3 , L Schultze Kool 10 , AP Timmers,RA Valdés Olmos 10 , CJ Van As, FSAM Van Dam 7 ,VLM Vander Poorten 11 , SAJM Van der Veen,MLF Van Velthuysen 10 , LAE Woerdeman 13 , CL Zuur,AJM Balm, FJM Hilgers, IB TanRehabilitationIn the ongoing research program on post-laryngectomyrehabilitation, several topics have beenexpanded. A high incidence of complete loss of olfactoryacuity is one of the disturbing consequences of totallaryngectomy due to the absence of a nasal airflow. Thekey to rehabilitation of olfaction appears to be thedevelopment of a Nasal Airflow Inducing Manoeuver(NAIM), which can be described as ‘polite yawning’, i.e.yawning with closed lips. This technique is based on ourearlier observations in a series of 63 patients and hasbeen refined during an intervention study. The effecti-Table XI.I.Objective measurement of the width of the neoglottis at rest and during phonation on digitized videofluoroscopic images.Measurement Near normal voice Abnormal voice DifferenceMaximal width at rest 4.2 mm 7.3 mm p = 0.018Minimal width during phonation 0.5 mm 2.7 mm p = 0.029
veness of the manoeuver could be demonstrated with awater- and/or digital manometer (Figure XI.I). The interventionconsisted of one half-hour training session in themajority of the patients. Using an odor detection test anda structured questionnaire in a series of 44 patients, thepercentage of patients with functional olfactory acuitycould be increased from 25% to 57% (p
130SURGICAL ONCOLOGY3 Division X.4 Division IX.5 Department of Radiotherapy, Catholic University,Leuven, Belgium.6 Department of Oral/Maxillofacial Surgery, AcademicMedical Center, Amsterdam.7 Division XIII.8 Divsion VI.9 Department of Otolaryngology/Head and NeckSurgery, University Hospital Nijmegen.10 Division XIII.11 Department of Otolaryngology/Head&Neck Surgery,Catholic University, Leuven, Belgium.12 Department of Neurology, University HospitalNijmegen.13 Department of Plastic and Reconstructive Sugery,Academic Medical Center, Amsterdam.Breast CancerH Bartelink 1 , APE Besnard 2 , N Bijker, JH Borger 1 ,JB De Boer, IF Faneyte, ME Grunstra, CA Hoefnagel 2 ,L Jansen, R Kaas, H Klaren 2 , BBR Kroon, OE Nieweg,JL Peterse 2 , BR Pieters 1 , R Valdes Olmos 2 ,MJ Van de Vijver 2 , FE Van Leeuwen 3 , EJTh RutgersProphylactic mastectomyFiles of 69 women who underwent prophylacticmastectomy between 1986 -1999 were analyzed. Thirtyeight women were asymptomatic (mean age 37, 29BRCA-1/2 mutations) and 31 underwent contralateralmastectomy after previous treatment for breast cancer(mean age 42, 20 BRCA-1/2 mutations). A total of 107breasts were surgically removed. Two patients werediagnosed with breast cancer by mammography/MRIscreening before surgery. At surgery, one patient had aT1N0 breast cancer and three had ductal carcinoma insitu (DCIS) /lobular carcinoma in situ (LCIS). Fifty-sixpatients underwent reconstruction of whom 50 werereconstructed in the same surgical session. There were58 tissue expanders (TE) placed, of which twelve werelost due to infection. All 13 transpositions of rectoabdominalmuscle (TRAM) were successful. Duringfollow-up (142 women years at risk), no breast cancerwas encountered. The clinical outcome seems to confirmthe estimated risk reduction by prophylactic mastectomy.Immediate TE reconstruction has a substantial failurerate.Ductal Carcinoma In SituThe effects of selection of patients for the EORTC10853 trial, investigating the role of radiotherapy in breastconserving therapy, were studied in five participatingcenters by analyzing all patients treated for DCIS.Reasons for non-entry were evaluated and treatmentresults of entered and non-entered patients werecompared. Of the eligible patients 64% were entered; themain reason for non-entry were doctors’ preference forone of the treatment arms, or patients’ refusal to trialparticipation (respectively 26% and 9%). These percentagesvaried significantly among the centers. At fouryears, non-entered patients treated with local excisionand radiotherapy had higher local recurrence rates thanrandomized patients (17% versus 2% respectively,p=0.003). Patients treated with local excision only hadequal recurrence rates (11% in both groups). Theseresults suggest that the trial results may not be applicableto all patients with DCIS.Clinical relevance of sentinel node outside the axillaUnexpected lymphatic drainage may be found duringthe sentinel node procedure. The relevance of sentinelnodes (SN) outside the lower axilla was studied in 113patients with breast cancer. In 21 (19%) SN’s outside thelower axilla were found using pre-operative lymphoscintigraphy,a gamma ray detection probe and intra-operativepatent blue dye. SN biopsy was performed in the internalmammary chain (17), the breast parenchyma (3), theinterpectoral fossa (2) and the infraclavicular fossa (2). Allbut 3 patients also had a SN in the lower axilla. Onepatient had a metastasis only in the SN outside the axilla.In three patients SN’s within the axilla and elsewherecontained tumor. In three patients the adjuvant treatmentpolicy was modified based on the extra-axillar SN statusonly. No postoperative complications were seen due tothe extra-axillar SN biopsies. Based on these results,biopsy of extra-axillar SN is recommended.Uptake of radiocolloid in sentinel nodesThe chance of intra-operatively SN retrieval with thegamma ray detection probe depends on the amount ofradioactivity in the node in relation to the uptake in thesurrounding normal tissue. In a series of 60 patients withbreast cancer and 22 patients with melanoma, uptake inSN’s was measured and compared to possibly relatedfactors in a multivariate analysis. Median uptake was 6.5kBq (0.16% of the injected dose; 95% range 0.03-102kBq) 24 hrs after injection of 64 MBq in breast cancerpatients, and 33 kBq (0.82%; 2.6-147 kBq) in patientswith melanoma. The radioactivity level depends mainly onthe time interval between injection and surgery, and noton age sex, nodal status, or dose.Notes1 Division IX.2 Division XIII.3 Division XII.Gastrointestinal Tract CancerJH Beijnen 1 , H Boot 2 , E De Bree, MM Kaag, SH Muller 3 ,N Van der Vange, GW Van Slooten, AJ Witkamp,F Van Coevorden, FAN Zoetmulder
Figure XI.2Actuarial survival curve (Kaplan-Meier) after intra-operativehyperthermic intraperitoneal chemotherapy (HIPEC) in patientswith carcinosis peritonei of colorectal origin.Colorectal cancerSince November 1995, patients with peritoneal carcinosisof colorectal origin without distant metastases aretreated by extensive surgical cytoreduction in combinationwith intra-operative hyperthermic intraperitoneal chemotherapy(HIPEC). Twenty-nine patients were included in aphase II study with a median follow-up of 28 months (19-39 months). At the time of evaluation, eleven patientswere still alive, six of them with proven recurrence (twolocal, four distant). The actuarial survival at one and twoyears is 79% and 48% respectively (Figure XI.2 ). A totalof fifty-three patients have now been accrued in theongoing randomized phase III trial (financed by the HealthInsurance Council Fund for Investigative Medicine),comparing extensive surgical cytoreduction + HIPEC andsystemic 5-FU to systemic 5-FU alone.Pseudomyxoma peritoneiForty patients with pseudomyxoma peritonei were treatedby HIPEC. In most patients the tumor was widely spreadthroughout the abdomen needing extensive surgical cytoreduction(mean operating time 11 hours). Consequently, asignificant postoperative morbidity was encountered. Fourpatients had long-term nutritional problems related to bowelfistula. Eleven patients needed a re-laparotomy. After amedian follow-up of 14 months, 34 patients are still alive(25 of them disease-free). Four patients died from treatmentrelated causes and one patient died from recurrent disease.These data are promising and support previously describedresults (Sugarbaker PH. Adv Surg 1996; 30: 233-80).Notes1 Department of Pharmacology, Slotervaart Hospital,Amsterdam.2 Division X.3 Division XIII.Urologic OncologyCA Hoefnagel 1 , D De Jong 1 , L Jansen, OE Nieweg,WW Ten Bokkel Huinink 2 , S Horenblas, W MeinhardtLymphatic mapping and sentinel node biopsy in penilecancerWith the aim of reducing the number of unnecessarylymph node dissections in penile cancer, we prospectivelyassessed the value of a dynamic sentinel nodeprocedure based on the individual drainage pattern of thetumor. From 1994 to 1998, 55 consecutive patients withsquamous cell carcinoma of the penis were prospectivelyentered in this study. A positive sentinel node was foundin 11 patients who underwent a subsequent regionallymph node dissection. To date, one false negativesentinel lymph node was observed. We conclude thatthis technique is minimally invasive and seems promisingin identifying patients with lymphatic metastases at anearly stage of the disease.Salvage prostatectomyFrom 1991-1998, 20 patients with residual prostatecancer after 125 I or external beam radiotherapy weretreated with a radical prostatectomy. This type of surgeryis seldom performed because of the assumed surgicalrisks and the presumed low potential for local control andcure. Analysis of our results shows an excellent localcontrol with an overall survival of 90% (median follow-up78 months) and a five-years disease-free survival of 72%(prostate specific antigen (PSA) progression-free survivaland/or absence of local recurrence). All patients sufferedfrom erectile dysfunction before surgery and the majorityof patients (70%) did not need to wear any externalappliance for incontinence. We conclude that in selectedcases salvage prostatectomy is a feasible procedure withan acceptable morbidity and excellent results regardinglocal control and overall survival.Non-seminomaFrom 1982-1994, 90 patients were entered in a waitand-see-protocolafter orchidectomy and 26% developeda recurrence. The eight years disease-specific survivalwas 98%. Prognostic factors for recurrence are: tumorsize, vascular invasion and percentage of embryonalcarcinoma (p< 0.03). By using these prognostic factors,a subgroup of patients with high risk for recurrence canbe identified for adjuvant treatment.Bladder cancerFrom 1994 to date, three females and 17 malesunderwent a modified sexuality- and continencepreservingcystectomy for removal of muscle invasivebladder cancer. One patient developed a urinary fistulawhich needed surgical closure. Storage function wasexcellent in 18 patients who are fully continent. Sixteenpatients empty their bladder without residual urine. Threepatients need to catheterize themselves and one patient131SURGICAL ONCOLOGY
132SURGICAL ONCOLOGYis not yet fully evaluable. In 19 patients, normal sexualfunction could be established. Maximum organ andtissue conservation is achieved through modifiedcystectomy, leaving a normal sexual function with goodurinary tract reconstruction.Testicular tissue preservationPatients with seminoma stage I treated with one-sidedorchidectomy and radiotherapy were studied prospectivelyfor serum testosterone levels (LH, FSH and SHBG).Within a normal spread of serum levels (grouped aroundP30), pathologically low testosterone levels were found in17% of the patients, indicating that hormonal recovery isat risk from one-sided orchidectomy. In selected casestesticular tissue preservation is therefore strongly recommended.Notes1 Division XIII.2 Division X.Gynecologic OncologyMCG Aalders 1 , MG Klein 2 , HJCM Sterenborg 3 ,FA Stewart 4 , WW Ten Bokkel Huinink 5 ,MJ Van de Vijver 6 , FAN Zoetmulder, M Van Beurden,N Van der Vange, ACM Van LindertPhotodetection with 5-aminolevulinic acid inducedprotoporphyrin IX in the rat abdominal cavity: Drug dosedependent fluorescence kineticsMacroscopically non-visible peritoneal metastases ofovarian tumors can be detected by fluorescencediagnostics as an aid to diagnostic laparoscopy orlaparotomy. The technique of photodetection of tumormetastases is based on differential concentration ofphotoactive dyes/fluorophores between tumor andnormal tissue. The higher the differential, the greater thesensitivity and specificty of photodetection. In this studywe performed fluorescence pharmacokinetics on 5-aminolevuline acid (ALA) induced protoporphyrin IX (PpIX)on abdominal organs and tumor metastases in theperitoneal cavity of rats. Three different drug doses (100,25 and 5 mg/kg) were used and PpIX fluorescenceprofiles were followed up to 24 hours after i.v. administration.Maximum tumor to normal tissue ratios werefound two to three hours after administration of ALAwith all drug doses. Three hours after administration of5 mg/kg, a significant tumor to normal tissue contrastratio was obtained with all included organs (Figure XI.3).This indicates that low dosages of ALA are optimal forphotodetection and are also safe with respect tounwanted white light phototoxicity.Notes1 Laser center, Academic Medical Center, Amsterdam.2 Department of Experimental Surgery, AcademicMedical Center, Amsterdam.3 Department of Radiotherapy, Daniel den Hoed CancerCenter, Rotterdam.4 Division VIII.5 Division X.6 Division XIII.Publications: Division XIFull papersAalders MCG, Van der Vange N, Stewart FA, Klein MG, Van deVijver MJ, Sterenborg HJCM. White-light toxicity, resulting fromsystemically administered 5-aminolevulinic acid, under normaloperating conditions. J Photochem Photobiol B Biol 1999; 50:88-93.Ackerstaff AH, Hilgers FJM, Meeuwis CA, Van der Velden LA, Vanden Hoogen FJA, Marres HAM, Manni JJ, Vreeburg GCM. Multiinstitutionalassessment of the Provox ® 2 voice prosthesis. ArchOtolaryngol Head Neck Surg 1999; 125: 167-73.Figure XI.3Tumor/normal ratio of fluorescence contrast as function of timeafter administration of 5mg/kg 5 - aminolevulinic acid (ALA)Bijker N, Rutgers EJT, Peterse JL, Van Dongen JA, Hart AAM,Borger JH, Kroon BBR. Low risk of loco-regional recurrence ofprimary breast carcinoma after treatment with a modification ofthe Halsted radical mastectomy and selective use of radiotherapy.Cancer 1999; 85: 1773-81.
De Gruijl TD, Bontkes HJ, Peccatori F, Gallee MP, Helmerhorst TJ,Verheijen RH, Aarbiou J, Mulder WM, Walboomers JM, Meijer CJ,Van de Vange N, Scheper RJ. Expression of CD3-zeta on T-cellsin primary cervical carcinoma and in metastasis-positive and–negative pelvic lymph nodes. Br J Cancer 1999; 79: 1127-32.De Gruijl TD, Bontkes HJ, Van den Muysenberg AJ, Van OostveenJW, Stukart MJ, Verheijen RH, Van der Vange N, Snijders PJ,Meijer CJ, Walboomers JM, Scheper RJ. Differences in cytokinemRNA profiles between premalignant and malignant lesions of theuterine cervix. Eur J Cancer 1999; 35: 490-7.Meinhardt W, Horenblas S. Time to normalisation of serumtestosteroneafter 3-months LHRH agonist administration [letter]. JUrol 1999; 162: 169-70.Morton DL, Thompson JF, Essner R, Elashoff R, Stern SL, NiewegOE, Roses DF, Karakousis CP, Mozillo N, Reintgen D, Wang H,Glass EC, Cochran AJ, and the Multicenter SelectiveLymphadenectomy Trial Group. Validation of the accuracy in amulticenter trial of intraoperative lymphatic mapping and sentinellymphadenectomy for early-stage melanoma. Ann Surg 1999;230: 453-63.133SURGICAL ONCOLOGYDeenik W, Mooi WJ, Rutgers EJT, Peterse JL, Hart AAM, KroonBBR. Clear cell sarcoma (malignant melanoma) of soft parts.Cancer 1999; 86: 696-75.Herben VM, Panday VR, Richel DJ, Schellens JH, Van der VangeN, Rosing H, Beusenberg FD, Hearn S, Doyle E, Beijnen JH, TenBokkel Huinink WW. Phase I and pharmocologic study of thecombination of paclitaxel, cisplatin, and topotecan administeredintravenously every 21 days as first-line therapy in patients withadvanced ovarian cancer. J Clin Oncol 1999; 17: 747-55.Nieweg OE, Jansen L, Valdés Olmos RA, Rutgers EJT, PeterseJL, Hoefnagel CA, Kroon BBR. Lymphatic mapping and sentinellymph node biopsy in breast cancer. Eur J Nucl Med 1999; 26(suppl): 11-6.Olieman AFT, Eggermont AMM, Lejeune FJ, Kroon BBR,Hoekstra HJ, Schraffordt Koops H. Hyperthermic isolated limbperfusion with tumor necrosis factor-alpha, interferon-gamma andmelphalan for locally advanced extremity non-melanoma skintumors; a multicenter study. Arch Surg 1999; 134: 303-7.Hilgers FJM, Ackerstaff AH. Comprehensive rehabilitation aftertotal laryngectomy is more than voice alone. Folia PhoniatricaLogopaedica 2000; 52: 65-73.Pameijer FA, Mukherji SK, Balm AJM, Van der Laan BFAM.Imaging of squamous cell carcinoma of the hypopharynx [review].Semin Ultrasound CT MRI 1998; 19: 476-491.Hilgers FJM, Ackerstaff AH, Van As CJ. Tracheoesophageal puncture:prosthetic voice management. Curr Opin Otolaryngol HeadNeck Surg 1999; 7: 112-8.Strobbe LJA, Jonk A, Hart AAM, Kroon BBR. Positive iliac andobturator nodes in melanoma: survival and prognostic factors.Ann Surg Oncol 1999; 6: 255-62.Hoefnagel CA, Moonen LMF, Haustermans KMG, Balm AJM.Imaging of tumour hypoxia in nuclear medicine. In: Oxygen and oncotherapy 98; Vol 3, Van der Kleij AJ, Voûte PA, Sminia P, editors.Archimedes Hyperbarmedizin und Verlags-GmbH, 1998: 79-87.Tan IB, Oppelaar H, Ruevekamp MC, Veenhuizen RB, TimmersAP, Stewart FA. The importance of in situ light dosimetry for photodynamictherapy of oral cavity tumors. Head Neck 1999; 21:434-41.Horenblas S. Surgical management, Carcinoma of the penis andscrotum. In: Petrovich Z, Baert L, Brady LW, editors. Medicalradiology: diagnostic imaging and radiation oncology; Volume:Carcinoma of the kidney, testis and uncommon tumors of thegenitourinary tract. Heidelberg: Springer, 1999: …Kerrebijn JDF, Balm AJM, Freeman JL, Dosch HM, Drexhage HA.Who is in control of the immune system in head and neck cancer?Crit Rev Oncol Hematol 1999; 31: 31-53.Tjiong MY, Van der Vange N, Ten Kate FJ, Tjong-A-Hung SP, TerSchegget J, Burger MP, Out TA. Increased IL-6 and IL-8 levels incervicovaginal secretions of patients with cervical cancer. GynecolOncol 1999; 73: 285-91.Valdés Olmos RA, Hoefnagel CA, Nieweg OE, Jansen L, RutgersEJT, Borger J, Horenblas S, Kroon BBR. Lymphoscintigraphy inoncology: a rediscovered challenge. Eur J Nucl Med 1999; 26(suppl): 2-10.Kroon BBR, Bergman W, Coebergh JWW, Ruiter DJ on behalf ofthe Dutch Melanoma Working Party. Consensus on the managementof malignant melanoma of the skin in the Netherlands: aconsensus report. Melanoma Res 1999; 9: 207-12.Valdés Olmos RA, Jansen L, Muller SA, Hoefnagel CA, NiewegOE. Contribution of nuclear medicine to lymphatic mapping andsentinel node identification in oncology. Rev Esp Med Nucl 1999;18: 111-21.Ligtenberg MJL, Hogervorst FBL, Willems HW, Arts PJW, Brink G,Hageman S, Bosgoed EAJ, Van der Looij E, Rookus MA, DevileeP, Vos EMAW, Wigbout G, Struycken PM, Menko FH, RutgersEJT, Hoefsloot EH, Mariman ECM, Brunner HG, Van ’t Veer LJ.Characteristics of small breast and/or ovarian cancer families withgermline mutations in BRCA1 and BRCA2. Br J Cancer 1999; 79:1475-8.Valdés Olmos RA, Koops W, Loftus BM, Liem IH, Gregor RT,Hoefnagel CA, Hilgers FJM, Balm AJM. Correlative 201 TI SPECT,MRI, and ex-vivo 201 TI uptake in detecting and characterizing cervicallymphadenopathy in head and neck squamous-cell carcinoma.J Nucl Med 1999; 40: 1414-9.
134SURGICAL ONCOLOGYVan As CJ, Tigges M, Wittenberg T, Op de Coul BMR, EysholdtU, Hilgers FJM. High-speed digital imaging of neoglottic vibrationafter total laryngectomy. Arch Otolaryngol Head Neck Surg 1999;125: 891-7.Van Dam FSAM, Hilgers FJM, Emsbroek G, Touw FI, Van As CJ,De Jong N. Deterioration of olfaction and gustation as a consequenceof total laryngectomy. Laryngoscope 1999; 109: 1150-55.Van der Poel HG, Roukema JA, Horenblas S, Van Geel AN,Debruyne FMJ. Metastasectomy in renal cell carcinoma: a multicenterretrospective analysis. Eur J Urol 1999: 197-203.Vander Poorten VLM, Balm AJM, Hilgers FJM, Tan IB, Loftus-CollBM, Keus RB, Hart AAM. Prognostic factors for long term resultsof the treatment of patients with malignant submandibular glandtumors. Cancer 1999; 85: 2255-64.Vrouenraets BC, Kroon BBR, Ogilvie AC, Van Geel AN, NiewegOE, Swaak AJG, Eggermont AMM. Absence of severe systemictoxicity after leakage-controlled isolated limb perfusion with tumornecrosis factor-alpha and melphalan. Ann Surg Oncol 1999; 6:405-12.Full papers in pressAckerstaff AH, Hilgers FJM, Meeuwis CA, Knegt PPM, WeeninkC. Pulmonary function pre and post total laryngectomy. ClinOtolaryngol 1999 (in press).Hilgers FJM, Van Dam FSAM, Keyzers S, Koster MN, Van As CJ,Muller MJ. Rehabilitation of olfaction in laryngectomized patientsby means of a nasal airflow inducing maneuver: the ‘polite yawning’technique. Arch Otolaryngol Head Neck Surg 1999 (inpress).Vander Poorten VLM, Balm AJM, Hilgers FJM, Tan IB, Loftus-CollBM, Van Leeuwen FE, Hart AAM. The development of a prognosticscore for patients with parotid carcinoma. Cancer 1999; 85:2057-67.Horenblas S. Dynamic sentinel node procedure in squamous cellcarcinoma of the penis. In: Nieweg OE, Reitgen DS, ThompsonFF, Essner R, editors. Lymphatic mapping in cancer. New York:Marcel Dekker, 1999 (in press).Van Ginkel RJ, Kole AC, Nieweg OE, Molenaar WM, Pruim J,Schraffordt Koops H, Vaalburg W, Hoekstra HJ. L-[1-11C]-tyrosinePET to evaluate response to hyperthermic isolated limb perfusionfor locally advanced soft-tissue sarcoma and skin cancer. JNucl Med 1999; 40: 262-7.Verdonck-de Leeuw IM, Hilgers FJM, Keus RB, Koopmans-VanBeinum FJ, Greven AJ, De Jong A, Bartelink H. Multidimensionalassessment of voice characteristics following radiotherapy forearly glottic cancer. Laryngoscope 1999; 109: 241-8.Verdonck-de Leeuw IM, Keus RB, Hilgers FJM, Koopmans-vanBeinum FJ, Greven AJ, De Jong A. Bartelink H. Consequences ofvoice impairment in daily-life for patients following radiotherapy forearly glottic cancer: voice quality, vocal function, and vocal performance.Int J Radiat Oncol Biol Phys 1999; 44: 1071-8.Voogd AC, Van Tienhoven G, Peterse JL, Crommelin MA, RutgersEJT, Van de Velde CJH, Van Geel AN, Slot A, Rodrigus PTR,Jobsen JJ, Von Meyenfeldt MF, Coebergh JWW, for the DutchStudy Group on Local Recurrence after Breast Conservation(BORST). Local recurrence after breast conservation therapy forearly breast cancer: detection, treatment and outcome in 266patients. Cancer 1999; 85: 437-46.Vrouenraets BC, Hart AAM, Eggermont AMM, Klaase JM, VanGeel BN, Nieweg OE, Kroon BBR. Relation between limb toxicityand treatment outcome after isolated limb perfusion for recurrentmelanoma. J Am Coll Surg 1999; 522-30.Horenblas S, Jansen L, Meinhardt W, Hoefnagel CA, De Jong D,Nieweg OE. Detection of occult metastasis in squamous cell carcinomaof the penis using a dynamic sentinel node procedure. JUrol 1999 (in press).Jansen L, Nieweg OE, Peterse JL, Hoefnagel CA, Valdés OlmosRA, Kroon BBR. Reliability of sentinel node biopsy for stagingmelanoma. Br J Surg 1999 (in press).Jansen L, Schraffordt Koops H, Nieweg OE, Doting MHE,Kapteijn BAE, Balm AJM, Vermey A, Plukker JT, Hoefnagel CA,Piers DA, Kroon BBR. Sentinel node biopsy for melanoma in thehead and neck region. Head Neck 1999 (in press).Kroon BBR, Jansen L, Rutgers EJT, Nieweg OE. Future of lymphaticmapping and sentinel node biopsy. In: Lymphatic mappingin cancer. Nieweg OE, Reintgen D, Thompson J, Essner R, editors.New York: Marcel Dekker, 1999 (in press).Liénard D, Eggermont AMM, Schraffordt Koops H, Kroon BBR,Towse G, Hiemstra S, Schmitz P, Clarke J, Steinmann G,Rosenkaimer F, Lejeune FJ. Isolated limb perfusion with TNFalphaand Melphalan with or without Interferon-y for treatment ofin-transit melanoma metastases: a multicenter randomised phaseII study. Melanoma Res 1999 (in press).Nieweg OE, Rutgers EJT, Jansen L, Valdés Olmos RA, PeterseJL, Hoefnagel CA, Kroon BBR. Is lymphatic mapping in breastcancer adequate and safe? World J Surg 1999 (in press).Vrouenraets BC, In ‘t Veld GJ, Nieweg OE, Van Slooten GW, VanDongen JA, Kroon BBR. Long-term functional morbidity after mildhyperthermic isolated limb perfusion with melphalan. Eur J SurgOncol 1999; 25: 503-8.
135Local papers and thesesHorenblas S, Efthymiou KM, Meinhardt W, Moonen LMF, VanTinteren H. Totale prostatectomie goede mogelijkheid na Jodium-125-behandeling of uitwendige radiotherapie. Ned TijdschrGeneeskd 1999; 143: 945-9.Nieweg OE, Sosef MN, Van Coevorden F. Wekedelensarcoom,diagnostiek: self assessment quiz. Ned Tijdschr Heelkd 1999; 8:26, 29.SURGICAL ONCOLOGYKroon BBR. Is een melanoom in de voorgeschiedenis een contraindicatievoor hormonale substitutie in verband met osteoporose?Vademecum 1998; 50.Kroon BBR, Bergman W, Coebergh JWW, Ruiter DJ. Consensusmelanoom van de huid. Tijdschr Huisartsgeneeskd 1999; 6: 334-8.Pameijer FA. Pre- and post-radiotherapy computed tomographyin laryngeal and hypopharyngeal cancer. Imaging-based predictionof local control [dissertation]. Utrecht: University of Utrecht,1999.Roeleveld T, Horenblas S, Meinhardt W, Van de Vijver M, De VriesF, Ten Bokkel Huinink WW. Wait-and-see-beleid bij non-seminomatestis stadium I. Ned Tijdschr Urol 1999; 7: 6-9.Rutgers EJT. Minder mutileren bij borstkanker: de schildwachtklier:de derde revolutie? In: Liber Amoricum M.A. Crommelin.Tilburg: Het inventief, 1999: 115-20.Sosef MN, Nieweg OE, Van Coevorden F. Wekedelensarcoom,therapie: self assessment quiz. Ned Tijdschr Heelkd 1999; 8: 26,29.Zoetmulder FAN. Wat te doen als de appendix bij onderzoek eencarcinoïd van 2 cm bevat? Vademecum 1999; 17: 2a.Zoetmulder FAN, Van der Vange N, Witkamp AJ, Kaag MM, BootH, Beijnen JH. Hypertherme intraperitoneale chemotherapie(HIPEC) bij patiënten met pseudomyxoma peritonei of peritoneummetastasenvan colorectaal carcinoom; gunstige eersteervaringen in het Nederlands Kanker Instituut. Ned TijdschrGeneeskd 1999; 143: 1863-8.Local papers in pressKroon BBR. Van Lanschot JJB. Principes van kankerchirurgie. In:Veenhof CHN, Voûte PA, redactie. Behandeling van kanker.Houten/Antwerpen: Bohn/Stafleu/Van Loghum,1999 (in press).Neering H, Kroon BBR. Huidtumoren. In: Van de Velde CHJBosman FT, Wagner DJT, redactie. Oncologie, 6e druk.Houten/Antwerpen: Bohn/Stafleu/Van Loghum, 1999 (in press).
136XII Division of PsychosocialResearch and EpidemiologyDivision head Neil AaronsonIntroductionThe psychosocial research group is pursuing threeprimary research lines: 1) the development, testing andapplication of quality of life (QL) measures in clinicaloncology research and practice; 2) assessment of thepsychosocial consequences of genetic counseling andtesting for hereditary forms of cancer; and 3) thedevelopment of methods for monitoring and managingsymptoms related to cancer and its treatment.Preliminary results of a prospective, randomized studyindicated that the routine provision of information derivedfrom standardized QL assessments increased significantly(by approximately 20%) the frequency with whichphysicians discussed their patients’ physical and psychosocialfunctioning, and their symptom experience duringoutpatient palliative chemotherapy visits. Additionally,physicians provided with the QL summary data weremore successful in identifying patients with moderate tosevere functional impairments and symptoms.Our on-going research into the feasibility of employingproxy respondents for assessing cancer patients’ QLindicated that the spouses of patients with metastaticcancer are able to evaluate, with a relatively high degreeof accuracy, patients’ physical and psychosocialfunctioning, symptom burden, and overall quality of life.Patient accrual continued for two companion studieson the impact of low-grade and high-grade glioma andits treatment on patients’ QL and neuropsychologicalfunctioning. Preliminary results indicated significant postsurgicalQL and neuropsychological deficits among highgradeglioma in almost all QL domains assessed. Moredisturbing were the preliminary findings indicating significantQL and neuropsychological deficits among themid-term to long-term survivors of low-grade glioma,compared with age- and gender-matched controls fromthe general population.In a retrospective, multicenter study we found thatapproximately 1 in 6 individuals at increased risk ofdeveloping colorectal cancer underwent preventivescreening (colonoscopy or sigmoidoscopy) less frequentlythan had been advised. The most important reasons fornon-adherence were the painful nature of the screening,and the belief that screening was not necessary due tothe absence of symptoms. Data collection is continuingfor a prospective, multicenter study of the effect ofgenetic counseling and testing for colorectal cancer onrisk perception, levels of distress, family relationships,work, family and financial planning, and preventive healthbehavior. We have also initiated a cross-sectional, multicenterstudy of the physical and psychosocial impact ofgynecological screening versus prophylactic oophorectomyamong women from hereditary breast/ovarian(HBOC) families.Finally, in the area of symptom management andcontrol, work continued on a prospective, multicenterstudy of the neuropsychological sequelae of high-dose,adjuvant chemotherapy in patients with high-risk breastcancer and high-grade lymphoma. Neurophysiological(qEEG) testing of a small sample of patients who hadreceived high-dose chemotherapy in the past, indicatedpathological asymmetry of the alpha rhythm. Finally, in alaboratory study carried out in collaboration with theUniversity of Groningen, mice injected with a single, highdoseof chemotherapy (CTC) were found to performsignificantly less well on a maze test than a non-treatedcontrol group. These results suggest a diminished consolidationof information, possibly indicative of long-termmemory deficits.The cancer epidemiology group is currently concentratingon two principal research lines: 1) the etiology ofhormone-related cancers; 2) the long-term health consequencesof cancer treatment, particularly in terms of therisk of developing a second cancer. Data collection isbeing carried out for a large case-control study whichcompares risk factors for ductal carcinoma in situ of thebreast and unilateral (invasive) breast cancer. Further, weare conducting a nation-wide cohort study to examinewhether women who underwent in vitro fertilization are atincreased risk of ovarian cancer and other hormonerelatedcancers. Using data from a large populationbasedcase-control study of breast cancer and oralcontraceptives, we examined the association betweenphysical activity and risk of breast cancer. We found thatphysically active women had a 30 percent lower risk ofbreast cancer than inactive women. In collaboration withthe Molecular Pathology laboratory (LJ Van ’t Veer) andthe Netherlands Collaborative Group on Hereditary BreastCancer, the epidemiology group is also conducting anation-wide prospective study of gene-environment inter-
actions in familial and hereditary breast and ovariancancer. Since penetrance and age at onset vary betweenand within BRCA1 and BRCA2 families, the developmentof cancer may also be influenced by hormonal or lifestylefactors or other distinct genetic loci.With the increased survival for several malignancies, ithas become exceedingly important to evaluate thepotential carcinogenic effects of cancer treatment. Theepidemiology group is therefore examining the long-termrisk of second cancers and cardiovascular diseasefollowing treatment of Hodgkin’s disease, breast cancerand testicular cancer. In 1999, analyses in a large groupof Hodgkin’s disease survivors demonstrated that therelative risk of solid tumors increased strongly withyounger age at first treatment of Hodgkin’s disease. Thiswas not only observed for breast cancer but also for allother solid tumors. Reassuringly, the strongly increasedsolid tumor risks in patients who were very young (≤20)at first treatment appeared to decrease as these patientsgrow older. We are also examining, in collaboration withthe Molecular Pathology laboratory (LJ Van ’t Veer),whether AT heterozygotes have an increased risk ofdeveloping radiation-induced second malignancies,especially breast cancer. In view of the large interest fortamoxifen as a chemopreventive agent, it is of greatimportance to better quantify its effect on endometrialcancer. In a series of 300 endometrial cancers followingbreast cancer, we found that the endometrial tumors oftamoxifen users had less favorable clinicopathologicalcharacteristics, and were more often p53-positive andestrogen-receptor negative.Psychosocial ResearchAssessing health-related quality of life(QL) in clinical research and clinicalpracticeNK Aaronson PhDJH Schornagel MD PhD 1M Hagedoorn PhD 2M Klein PhD 3SB Detmar MSc 4R Hoopman MSc 5KCA Sneeuw MSc 6MJ Muller MScWHJJ Cleyne 3J Grit 3WJM Oomen 3LDV Wever 4Group leaderAcademic staffPost-docPost-docGraduate studentGraduate studentGraduate studentStatistical analystResearch assistantResearch assistantResearch assistantResearch assistantThe use of QL assessments in daily clinical oncologypractice: an intervention study to facilitate doctor-patientcommunication in outpatient palliative care settings 4This prospective, randomized (cross-over) study isevaluating the efficacy of incorporating standardized QLassessments as a routine part of the outpatient palliativetreatment of cancer patients in terms of two primaryoutcomes: 1) facilitating doctor-patient communication;and 2) increasing physicians’ awareness of patients’physical and psychosocial health problems. The studysample includes 10 medical oncologists and 214 of theirpatients treated with palliative chemotherapy. In the interventiongroup, graphic summaries of the patients’ QL (asassessed by the EORTC QLQ-C30) were generated andshared with both the patients and their physiciansimmediately prior to outpatient clinic visits. To evaluatedoctor-patient communication, four consecutive medicalconsultations were audiotaped and content-analyzedusing standardized computer software (the RIAS system).To evaluate physicians’ awareness, comparisons weremade between physicians’ and patients’ ratings on theCOOP/WONCA charts. Preliminary results indicate thatpatients’ level of physical and psychosocial functioning,and their symptom experience, was discussed significantlymore frequently in the intervention than in thecontrol group (on average, a 20% increase in QL topicsdiscussed). Physicians in the intervention condition weremore successful at identifying patients with moderate tosevere problems in several QL domains (e.g. socialfunctioning, pain, fatigue). All of the physicians and 75%of the patients in the intervention condition believed thatthe intervention facilitated communication and expressedinterest in continued use of the procedure.The role of proxies in evaluating the QL of cancer patients 6In this study, carried out in collaboration with theUniversity of Connecticut Health Center (P Albertsen),patients with metastatic prostate cancer and theirspouses independently completed the EORTC QLQ-C30and a prostate cancer-specific questionnaire moduleassessing, in total, 21 QL outcomes. Systematic, butrelatively minor differences in mean scale scores werenoted for 5 of the 21 patient-proxy comparisons, withspouses rating the patients as having more QL impairmentsthan the patients themselves. Moderate to goodpatient-proxy agreement was observed at the individuallevel (ICC’s ranging from 0.40 to 0.75). The reliability andvalidity of spouses’ ratings were similar to that of thepatients. These results support our earlier findings thatproxies are able to evaluate, with a relatively high degreeof accuracy, patients’ physical and psychosocialfunctioning, symptom burden, and overall quality of life.The QL and neuropsychological status of patients withhigh-grade and low-grade glioma 3, 7In collaboration with the Departments of Neurology(JJ Heimans) and Medical Psychology (HM Van derPloeg) of the Vrije Universiteit, Amsterdam, twocompanion studies are being conducted to assess: 1) theimpact of low-grade and high-grade glioma and itstreatment on the QL (as measured by the SF-36) ofpatients and their partners; and 2) the relationshipbetween the patients’ neuropsychological status and theirperceived QL. Newly diagnosed patients with high-grade137PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGY
138PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGYglioma are assessed prospectively at 4-monthly intervals,along with a comparison group of patients with non-smallcell lung cancer (NSCLC). Mid-term to long-termsurvivors of low-grade glioma are assessed at a singlepoint in time, together with a comparison group ofpatients with low-grade hematologic malignancies. Todate, 68 patients and 50 controls have been entered intothe high-grade glioma study, and 185 patients and 23controls in the low-grade glioma study. Normative datafrom the general population are also available for boththe SF-36 and the neuropsychological test battery.Preliminary analyses of the baseline data from thehigh-grade glioma study indicate that the QL of gliomaand NSCLC patients is similar, with both groups deviatingsignificantly from normative data from the generalpopulation. Cognitive impairment, based on objectiveperformance tests, was found in 49% of the gliomapatients and in 26% of the NSCLC controls.Preliminary analyses comparing 145 low-grade gliomasurvivors with 145 age- and gender-matched generalpopulation controls revealed significant impairment in QLin the survivor group (on 7 of the 8 SF-36 scales).Additionally, significant neuropsychological deficitssuggestive of a reduced information processing capacitywere found in this survivor group. These findings indicatethat survivors of low-grade glioma continue to experiencesignificant QL and cognitive deficits for many years aftertheir primary diagnosis and treatment.QL assessment among ethnic minority cancer patients inthe Netherlands 5In 1999, preparatory work was carried out for a largescale study whose primary aims are to translate, adaptand validate two widely used generic QL questionnaires(the SF-36 and the COOP/WONCA charts) and twocancer-specific questionnaires (the EORTC QLQ-C30 andthe Rotterdam Symptom Checklist) for use amongTurkish and Moroccan cancer patients. The study instrumentshave been translated into the requisite languages,and procedures have been developed for recruitingpatients from regional hospitals. This project will facilitateinclusion of ethnic minorities in QL investigations, and willprovide a wealth of descriptive information on the impactof cancer and its treatment on the functional health andwell-being of these populations.Notes1 Division X.2 Fellow of the Dutch Cancer Society.3 Funding: Dutch Cancer Society, Project VU/<strong>NKI</strong> 96-1155.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-1134.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1724.6 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-2110.7 External collaborators: JJ Heimans MD PhD,Academic Hospital Vrije Universiteit, Amsterdam;HM Van der Ploeg PhD, Department of MedicalPsychology, Vrije Universiteit, Amsterdam.Publications: Quality of lifeAaronson NK, Fayers P. Quality of life. In: Souhami RL, Tannock I,Hohenberger P, Horiot JC, editors. Oxford Textbook of Oncology,2nd ed. Oxford: Oxford University Press (in press).Fosså SD, Curran D, Aaronson NK, Keuppens F, Kliment J,Robinson MRG, De Rijke TM, Hetherington J, Kil PJM, Rea LA.Quality of life of patients with newly diagnosed poor prognosis M1prostate cancer undergoing orchiectomy without or withMitomycin C. Eur J Urol (in press).Groenvold M, Fayers PM, Sprangers MAG, Bjorner JB, Klee MC,Aaronson NK, Bech P, Mouridsen HT. Anxiety and depression inbreast cancer patients at low risk of recurrence compared withthe general population - a valid comparison? J Clin Epidemiol1999; 52 : 523-30.Langendijk JA, Ten Velde GPM, Aaronson NK, De Jong JMA,Muller MJ, Wouters EFM. Quality of life after palliative radiotherapyin non-small cell lung cancer: a prospective study. Int J RadiatOncol Biol Phys (in press).Middleton MR, Grob JJ, Aaronson NK, Fierlbeck G, Tilgen W,Seiter S, Goreo M, Amadal S, Cebon J, Coates A, Dreno B, HenzM, Schadendorf D, Kapp A, Weiss J, Fraass U, Statkevich P,Muller M, Thatcher N. Randomized phase III study of temozolomideversus dacarbazine in the treatment of patients with advanced,metastatic malignant melanoma. J Clin Oncol (in press).Sneeuw KCA, Aaronson NK, Sprangers MAG, Detmar SB, WeverLDV, Schornagel JH. Evaluating the quality of life of cancerpatients: assessments by patients, significant others and nurses.Br J Cancer 1999; 81: 87-94.Sprangers MAG, Aaronson NK, De Haes JCJM. Onderzoek naarde kwaliteit van leven van kankerpatiënten. In: Van de Velde CJH,Bosman FT, Wagener DJ, redactie. Oncologie, 6e dr. Houten:Bohn Stafleu Van Loghum (in press).Sprangers MAG, Te Velde A, Aaronson NK. The construction andtesting of the EORTC colorectal cancer-specific quality of lifequestionnaire module (the QLQ-CR38). Eur J Cancer 1999; 35:238-47.Van der Zouwe N, Van Dam FSAM, Aaronson NK. Het gebruik vanalternatieve kankertherapieën naast de reguliere behandeling. In:Van de Velde CJH, Bosman FT, Wagener DJ, redactie. Oncologie,6e dr. Houten: Bohn Stafleu Van Loghum (in press).
Psychosocial issues in genetic counselingand testing for hereditary cancerNK Aaronson PhDI Kluijt MD 1FH Menko MD PhD 1BG Taal MD PhD 2M Van Beurden MD PhD 3S Verhoef MD 1EMA Bleiker PhD 4RM Rosenbrand MScMA Gerritsma 5LDV Wever 4ALE Van Rens 1G Wigbout 1J HollensteinGroup leaderAcademic staffAcademic staffAcademic staffAcademic staffAcademic staffPost-docGraduate studentResearch assistantResearch assistantGenetic nurseGenetic nurseUndergraduate studentScreening adherence among individuals at high risk ofdeveloping colorectal cancerThis retrospective, multicenter study is investigatingadherence to screening advice among individuals at anincreased risk of developing colorectal cancer who werecounseled at one of three familial cancer clinics inAmsterdam (<strong>AvL</strong>, AZVU, or AMC) in the period 1986-1996. Questionnaires were completed by 178 individuals(83% response rate). Preliminary results based on selfreportdata indicate that approximately 16% of thesample underwent screening (colonoscopy or sigmoidoscopy)less frequently than had been advised. The mostimportant reasons for non-adherence were the painful,unpleasant, and embarrassing nature of the screening,and the belief that screening was not necessary due tothe absence of symptoms. No statistically significantdifferences between ‘compliers’ and ‘non-compliers’ werefound as a function of sociodemographics, riskperception, or worries about cancer. Self-reportedadherence behavior will be confirmed, where possible, byobjective data obtained from medical chart audits.The psychosocial and behavioral impact of geneticcounseling for colorectal cancer (CRC): a prospective,multicenter study 4, 6The primary objectives of this prospective, multicenter(<strong>AvL</strong>, AZVU, AMC, RUG, and LUMC) study are to: 1)assess the effect of genetic counseling and testing onrisk perception, levels of distress, family relationships,work, and family and financial planning; 2) identify riskfactors for poor psychological adjustment to thecounseling and testing outcome and for early withdrawalfrom the genetic counseling process; and 3) establishrates of short-term compliance with recommendedscreening practices. The study will include approximately375 individuals. To date, 45 individuals have beenentered into the study.The physical and psychosocial impact of gynecologicalscreening or prophylactic oophorectomy among womenfrom hereditary breast/ovarian (HBOC) cancer families 7This cross-sectional, retrospective, multicenter (<strong>AvL</strong>,AZVU, AMC) study is investigating: 1) the decisionmakingprocess surrounding the choice of preventivehealth actions among women at increased risk ofdeveloping ovarian cancer; 2) the impact of screeningversus prophylactic surgery on psychosocial well-being;3) compliance with screening advice for those who optfor this form of prevention; and 4) the prevalence andseverity of menopausal symptoms among women whoopt for surgery, as well as the use and perceived benefitof hormone-replacement therapy. In 1999, preparatoryactivities were carried out, including identification of thestudy population, and selection and pilot-testing of thequestionnaires and interview schedules. In total, approximately375 women will be invited to participate in thestudy.Client satisfaction with family cancer clinics 5This study is evaluating client satisfaction with thequality of care provided at three family cancer clinics inAmsterdam (<strong>AvL</strong>, AZVU, and AMC). All individuals whocomplete the genetic counseling process are asked tocomplete a questionnaire assessing experiences with andthe perceived quality of the services provided, the role ofthe general practitioner in the genetic counselingprocess, and the impact of genetic testing on psychosocialwell-being, family interactions, work, familyplanning, and insurance eligibility. In total, 300 individualswill be included in the study. To date, 118 individualshave been surveyed.Notes1 Family Cancer Clinic, <strong>NKI</strong>/<strong>AvL</strong>.2 Division X.3 Division XI.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1858.5 Funding: Clinical Genetics Foundation, Amsterdam(SKGA).6 External collaborators: A Bröcker-Vriends MD PhD,Leiden University Medical Center; RH Sijmons MD,Academic Hospital Groningen; H Valdimarsdottir PhD,Mount Sinai School of Medicine, New York, USA.7 External collaborators: J Van der Velden MD PhD,Academic Medical Center, University of Amsterdam;RHM Verheijen MD PhD, Academic Hospital VrijeUniversiteit, Amsterdam; H Valdimarsdottir PhD, MountSinai School of Medicine, New York, USA.139PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGY
140PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGYPublications: Genetic counselingBleiker EMA, Aaronson NK. Genetic counseling for cancer: a familyissue. In: Cooper CL, Baider l, editors. Cancer and the Family,2nd ed. New York: John Wiley & Sons (in press).Bleiker EMA, Pouwer, F, Van der Ploeg HM, Leer JWH, Adèr HJ.Psychological distress two years after diagnosis of breast cancer:frequency and prediction. Patient Educ Couns (in press).Bleiker, EMA, Van der Linden MHM. Erfelijkheidsonderzoek bijkanker (2). MGV Maandbl Geest Volksgez 1999; 3: 290-1.Bleiker, EMA, Van der Ploeg HM. Psychosocial factors in the etiologyof breast cancer: a review of a popular link. Patient EducCouns 1999; 37: 201-14.Valdimarsdottir HB, Bovbjerg D, Brown K, Jacobsen P, SchwartzM, Bleiker EMA, Offit K, Borgen P, Heerdt A, Van Zee K. Cancerspecificdistress is related to women’s decisions to undergoBRCA1 testing. Cancer Res Ther Control 1999; 8: 61-8.FSAM Van Dam PhDW Boogerd MD PhD 1FJM Hilgers MD PhD 2JF Jongkind MSc 3S Rodenhuis MD PhD 1CJ Van As MSc 2SB Schagen MSc 4MJ Muller MScMEJ De Rond MScAS Biervliet 4BPC Kreukels 4RM Rosenbrand 4MCH Weevers 4W De Ruyter 3H AnderssonHA JansenART KalksmaTA OverbeekDCM Van RhijnA VlietstraSymptom perceptionand management incancer patientsGroup leaderAcademic staffAcademic staffAcademic staffAcademic staffAcademic staffGraduate studentStatistical analystNursing scientistResearch assistantResearch assistantResearch assistantResearch assistantResearch nurseUndergraduate studentUndergraduate studentUndergraduate studentUndergraduate studentUndergraduate studentUndergraduate studentCognitive deficits as a consequence of high-dose chemotherapyamong patients with high-risk breast cancer andhigh-grade lymphoma 4, 5The primary objective of this study is to investigate cognitivefunction prior to and following (adjuvant) high-dosechemotherapy in patients with high-risk breast cancer andhigh-grade lymphoma. The neuropsychological status ofthe patients is being assessed at three points in time with astandard battery of tests. Patient accrual started in April1998. To date, 428 test assessments have been carriedout.In collaboration with the Department of ClinicalNeurophysiology of the Slotervaart Hospital, neurophysiologicaltests were performed on a subgroup of 33 highriskbreast cancer patients who had participated in arandomized study comparing adjuvant high-dose (HD)chemotherapy with standard-dose (SD) chemotherapy.An additional control group included 13 high-risk breastcancer patients who had not received chemotherapy. Theneurophysiological examination consisted of P300 andquantitative EEG including analysis of asymmetry andblocking of alpha-rhythm. Patients were tested two yearsafter completion of treatment. Asymmetry of the alpharhythm of 0.5 Hz was found in 7 patients of the HDgroup, in 2 patients of the SD group and in none of thecontrol patients (p=0.02). An asymmetry of the alpharhythm of >0.2 Hz is considered as pathological. Theneurophysiological results did not correlate with theneuropsychological test results, nor with patients’subjective complaints about their cognitive functioning.In collaboration with the Department of ClinicalChemistry and the Laboratory for Animal Physiology ofthe University of Groningen, the effects of CTC chemotherapyin FVB mice were studied. A significant differencewas found between the treatment group and controlgroup with regard to long-term learning strategies. In thetreatment group, a diminished consolidation of informationwas observed, which could be indicative of longtermmemory deficits.Empowering the cancer patient with chronic pain 6Chronic pain is a major problem in cancer patients.Based on previous research in the <strong>AvL</strong>, an instructionmanual for nurses is being developed and problem areasfor pain management in the inpatient setting are beingidentified. Central to the program is instructing nurses inhow they can train patients to monitor their pain complaintsand to use pharmacological and non-pharmacological paininterventions effectively. This project is being carried out atthe University Hospital Rotterdam and at the Antoni vanLeeuwenhoek Hospital. Following initial evaluation, theprogram will be offered to other regional hospitals.Olfactory rehabilitation after total laryngectomyIn cooperation with Division XI, a method to rehabilitateolfaction in laryngectomized patients has been developed.This ‘Nasal Airflow Inducing Maneuver (NAIM)’, can belearned with 30 minutes of training. This technique could
e successfully learned by 57% of patients who could notsmell due to a total laryngectomy. Further work is beingcarried out to investigate the impact of NAIM on olfactionin daily life, and to better understand why some patientsare unable to learn and apply the technique.Notes1 Division X.2 Division XI.3 Nursing department, <strong>NKI</strong>/<strong>AvL</strong>.4 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1729.5 External collaborators: J Snel PhD, KR RidderinkhofPhD, Department of Psychology, University ofAmsterdam.6 External collaborators: R De Wit PhD, Department ofMedical Psychology and Psychiatry, ErasmusUniversity Rotterdam; FE Witkamp, University HospitalRotterdam.Publications: Symptom perceptionDe Rond MEJ, De Wit R, Van Dam FSAM, Van Campen BTM, DenHartog YM, Klievink RMA. A Pain Monitoring Program for nurses:effects on nurses’ pain knowledge and attitude. J Pain SymptomManage (in press).Van Dam FSAM. Alternatieve behandelingen bestrijden de angst,niet de kanker, Oncologica 1999; 14: 24-5.Van Dam FSAM. Meer gebruik van alternatieve diëten en vanandere alternatieve behandelingen door kankerpatiënten:Houtsmuller is in, Moerman is uit. Ned Tijdschr Geneeskd 1999;143: 1421-4.Van Dam FSAM. Psychosociale aspecten van kankerbehandeling:over kwaliteit van leven. In: CHN Veenhof, PA Voute, redactie.Behandeling van Kanker. Houten: Bohn Stafleu Van Loghum (inpress).Van Dam FSAM. Psychosociale zorg van de kankerpatiënt. In: Vande Velde CJH, Bosman FT, Wagener DJTh, redactie. Oncologie,6e ed. Houten: Bohn Stafleu Van Loghum (in press).Van Dam FSAM, Hilgers FJM, Emsbroek G, Touw FI, Van As CJ,De Jong N. Deterioration of olfaction and gustation as a consequenceof total laryngectomy. Laryngoscope 1999; 109: 1150-5.Van Dam FSAM, Roodbergen R, Jongkind H, Loonstra S.Evaluatie van de kwaliteit van de verpleegkundige zorgverlening àla carte: het Amsterdams Modulair Kwaliteitsbewaking Systeemvoor de Verpleegkundige Zorgverlening (AMKS-VZ). In: HandboekVerpleegkundig Konsult. Houten: Bohn Stafleu Van Loghum,1999.141PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGYDe Rond M, De Wit R, Van Dam F, Van Campen B, Den Hartog Y,Klievink R, Nieweg R, Noort J, Wagenaar M, Van Campen B. Dailypain assessment: value for nurses and patients. J Adv Nurs 1999;29: 436-44.Van der Zouwe N, Van Dam FSAM, Aaronson NK. Het gebruik vanalternatieve kankertherapieNn naast de reguliere behandeling. In:Van de Velde CJH, Bosman FT, Wagener DJTh, redactie.Oncologie, 6e ed. Houten: Bohn Stafleu Van Loghum (in press).De Rond MEJ, Van Dam FSAM, De Wit R. De kennis en attitudevan verpleegkundigen en artsen ten aanzien van pijn en pijnbestrijding.Tijdschr Gezondheidswetenschappen 1999; 77: 10-8.De Wit R, Van Dam F, Hanneman M, Zandbelt L, Van Buuren A,Van der Heijden K, Leenhouts G, Loonstra S, Huijer Abu-Saad H.Evaluation of the use of a pain diary in chronic cancer patients athome. Pain 1999; 79: 89-99.De Wit R, Van Dam F, Huijer Abu-Saad H, Loonstra S, Zandbelt L,Van Buuren A, Van der Heijden K, Leenhouts G. Empirical comparisonof commonly used measures to evaluate pain treatment incancer patients with chronic pain. J Clin Oncol 1999; 17: 1280-7.De Wit R, Van Dam F, Vielvoye-Kerkmeer A, Mattern C, HuijerAbu-Saad H. The treatment of chronic cancer pain in a cancerhospital in the Netherlands. J Pain Symptom Manage 1999; 17:333-50.Renckens CNM, Van Dam FSAM. Het Koningin Wilhelmina Fondsen de Houtsmuller-therapie bij kanker. Ned Tijdschr Geneeskd1999; 143: 1431-3.Schagen SB, Van Dam FSAM, Muller MJ, Boogerd W, LindeboomJ, Bruning PF. Cognitive deficits after postoperative adjuvant chemotherapyfor breast cancer. Cancer 1999; 85: 640-50.
142PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGYEpidemiologyRisk factors forhormone-related cancerFE Van Leeuwen PhD Group leaderAAM Hart MSc 1Academic staffI Kluyt MD 2Academic staffFH Menko MD PhD 2Academic staffJL Peterse MD 3Academic staffMA Rookus PhDAcademic staffEJT Rutgers MD PhD 4 Academic staffL Van ’t Veer PhD 3Academic staffS Verhoef MD 2Academic staffK Van der Kooy PhD 5 Post-docRM Brohet MSc 6Graduate studentEJ De Boer MSc 7Graduate studentH Klip MPH 8, 9Graduate studentJ Verloop MSc 10Graduate studentS Braak 9Research assistantPAM Braas 6Research assistantAC Buitelaar 6Research assistantBPG Maertzdorf 11Research assistantMCJ Schippers 9Research assistantAW Van den Belt-Dusebout 6, 9 Research assistantCM Versteegden 9Research assistantMMPGM Woordes-van Baalen 6 Research assistantC Spronk 5TechnicianALE Van Rens 2Genetic nurseG Wigbout 2Genetic nurseM HollmannUndergraduate studentJ TomasUndergraduate studentM Van VlietUndergraduate studentRisk factors for breast cancer5, 6, 10, 11, 12In 1999, we stopped the accrual of patients for ourpopulation-based case-control studies of risk factors forductal carcinoma in situ of the breast (n=546), andinvasive unilateral (n=1233) and contralateral breastcancer (n=348). An important aim of the study is tocompare risk factor profiles for different forms of breastcancer, as defined by histopathologic characteristics andgenetic alterations. For this purpose, we collected 1558(85%) of the 1832 tumor blocks from 43 pathologylabatories.Immunohistochemical staining and scoring forC-ErbB2, p53, estrogen and progestagen receptor,Cyclin D1 and bcl2 is in progress.In 1999 we conducted further analyses with data froma large, population-based case-control study of oralcontraceptive use and breast cancer. Breast cancercases, aged 20-54 at diagnosis (n=918), werepair-matched on age and region with controls randomlyselected from municipal registries. We investigated theassociation between lifetime physical activity and risk ofbreast cancer. Women who were more active than theirpeers at ages 10-12 had a 32% decreased risk of breastcancer. Women who had ever been engaged in recreationalphysical activity had a reduced risk of breastcancer compared to inactive women (relative risk(RR)=0.70, 95% CI=0.56-0.88). Neither very early recreationalactivity (before age 20) nor recent activity (last fiveyears) was associated with a greater risk reduction thanrecreational activity in the intermediate period. Leanwomen appeared to benefit more from the protectiveeffect of recreational physical activity than women with ahigher body mass index.We continued the accrual of participants for ournational genetic epidemiologic cohort study in breastand/or ovarian cancer families with the following aims: 1)to examine whether hormonal/life-style factors modifycancer risks in BRCA1/2 and non-BRCA1/2 families; 2)to assess in non-BRCA1/2 families the age-specificcumulative risks of breast, ovarian and other cancersbased on full pedigree information. So far, data collectionstarted in five out of the ten genetic centers in theNetherlands. Pedigree information of 348 families hasbeen collected from clinical genetic records and 563women out of 31 families have been approached tocomplete a mailed questionnaire on hormonal/life-stylefactors. So far, 445 questionnaires have been received. Intotal, the study will include 10,000 family members.Preliminary analyses were conducted to examine whichpedigree characteristics were most predictive for finding aBRCA1/2 mutation. In families with both breast andovarian cancer cases (n=67), BRCA1/2 mutations werefound in 64.2% of the families, whereas this proportionwas 17.4% in breast cancer-only families (n=167). Inthese families selected for breast and/or ovarian cancer,brain tumors were diagnosed more often than expectedfrom age-, calendar period-specific incidence data of thegeneral population.We examined cancer prevalence in women exposed todiethylstilbestrol (DES) in utero and registered at theNetherlands DES Information Center (NDESIC). Selfreportedcancers were checked in the medical records.Compared to the general population, a more than fourfoldincreased prevalence rate of invasive cervical cancerwas found among DES-daughters.Hyperstimulation of the ovary in relation to the risk ofhormone-related cancers7, 8, 9, 13We are conducting a large-scale cohort study toexamine whether women who have undergone hyperstimulationfor in vitro fertilization (IVF) are at increased riskof ovarian cancer and other hormone-related cancers. AllIVF centers in the Netherlands are collaborating in thisnationwide effort. A historical cohort of 20,000 subfertilewomen who received hyperstimulation for IVF between1983 and 1995 was identified. As a control group 7,500women were recruited whose subfertility was diagnosed
in the same hospitals, but who did not receive IVFtreatment. In 1999, address information was updated forall cohort members and 25,000 of those received a riskfactor questionnaire. The response rate is approximately70%. For 15,000 participating women, medical data(cause of infertility, details of fertility treatment) have beencollected from the medical records, including informationon 45,000 IVF cycles. Every five years, the incidence ofhormone-related cancers in the IVF group and the controlgroup will be compared by linkage with the NetherlandsCancer Registry.Within this large cohort of subfertile women, weinitiated a study examining determinants of age atmenopause. Factors of interest are cause of subfertility,number of retrieved oocytes at IVF and IVF treatment.Notes1 Division IX.2 Family Cancer Clinic, <strong>NKI</strong>/<strong>AvL</strong>.3 Division VIII.4 Division XI.5 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 95-1144.6 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1854.7 Funding: International Health Foundation, Utrecht.8 Funding: Prevention Fund, Project 28-2540.9 Funding: Ministry of Health.10 Funding: Prevention Fund, Project 28-28460.11 Funding: International Agency for Research on Cancer.12 External collaborator: DE Goldgar PhD, InternationalAgency for Research on Cancer, Lyon, France.13 External collaborators: CW Burger MD PhD, UniversityHospital Rotterdam; I Den Tonkelaar PhD, InternationalHealth Foundation Utrecht; ER Te Velde MD PhD,Academic Hospital Utrecht.Publications: Hormone related cancerLigtenberg MJL, Hogervorst FBL, Willems HW, Arts PJW, Brink G,Hageman S, Bosgoed EAJ, Van der Looij E, Rookus MA, DevileeP, Vos EMAW, Wigbout G, Struycken PM, Menko FH, Rutgers EJ,Hoefsloot EH, Mariman ECM, Brunner HG, Van ‘t Veer LJ.Characteristics of small breast and/or ovarian cancer families withgermline mutations in BRCA1 and BRCA2. Br J Cancer 1999; 79:1475-8.Rookus MA. De epidemiologie van mammacarcinoom, in het bijzonderin de menopauze. Bijblijven 1999; 15: 42-51.Rookus MA. Is screening op borstkanker nodig bij oestrogeensuppletie?Huisartsen Vademecum (in press).Rookus MA. Invited commentary: reporting bias in case-controlstudies on induced abortion and breast cancer. Am J Epidemiol(in press).Verloop J, Rookus MA, Van der Kooy K, Van Leeuwen FE.Physical activity and breast cancer risk in women aged 20-54years. J Natl Cancer Inst (in press).Cancer risk following medical treatmentFE van Leeuwen PhDBMP Aleman MD 1MPW Gallee MD PhD 2JL Peterse MD 2NS Russell MD 1L Van ‘t Veer PhD 2EAE Welp MPH 3WJ Klokman MD MScEK Adriaans 3MLR Beelen 3VB Hartog 3AW Van den Belt-DuseboutGroup leaderAcademic staffAcademic staffAcademic staffAcademic staffAcademic staffGraduate studentStatistical analystResearch assistantResearch assistantResearch assistantResearch assistantLong-term risk of second cancers following treatment forHodgkin’s disease, testicular cancer and breast cancer 3, 4The specific aims of this research project are: 1) toevaluate the risk of second cancers (SC) followingHodgkin’s disease (HD), breast cancer and testicularcancer over a period of up to 30 years, and to determinefor which SC types risk is increased compared with theincidence in the general population; 2) to similarly evaluatethe risk of cardiac death and acute myocardial infarction;3) to quantify the separate and combined effects ofdifferent treatments on SC risk. We are conducting threecohort studies which include 2,650 5-year survivors of HDtreated between 1966-1990, 2,200 5-year survivors oftesticular cancer treated between 1966 and 1990, and6,050 5-year survivors of breast cancer treated between1970 and 1987. Patients included in these cohorts weretreated in the Netherlands Cancer Institute, the Dr Danielden Hoed Cancer Center/EUR, the University hospitals ofLeiden and Groningen and hospitals participating in theEindhoven Cancer Registry.In 1999 we collected treatment data on 1,600 breastcancer patients treated between 1970 and 1976. Further,we conducted a more extensive analysis as to the effectof treatment on the risk of second malignancies in 1,253survivors of HD who were less than 40 years old atdiagnosis of HD. In all, 137 patients developed a SC,compared with 19.4 cases expected on the basis ofincidence rates in the general population (RR=7.0).Significantly increased RRs were observed for leukemia(RR=37.5), NHL (RR=21.5) and solid tumor overall(RR=6.1). The 25-year actuarial risk of SC overall was27.7% and of breast cancer (in females) 16.3%. The RRof solid malignancies rose with longer follow-up duration.Among patients with ≥20 years of follow-up, the RR was7.6-fold increased, slightly less than the RR of 9.1observed in the 15-19 year follow up period. The RR ofsolid tumors increased strongly with younger age at firsttreatment of HD. This was not only observed for breastcancer but also for all other solid tumors, with RRs of4.9, 6.9 and 12.7 for women first treated at ages 31-39,21-30, and ≤20, respectively. Reassuringly, the stronglyincreased solid tumor risks in patients who were veryyoung (20) at first treatment appear to decrease as these143PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGY
144PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGYpatients grow older. Among patients treated at age 20 orbefore, the RR of developing a solid tumor before age 40was significantly greater than the RR of solid tumordevelopment at ages 40-49 (RR=27.9 versus RR=4.2).In a related project we are examining to what extentATM heterozygosity increases the risk of radiationassociatedbreast cancer. Two case control studies havebeen conducted on patients who developed breast cancerfollowing radiotherapy. Patients and matched controlsdonated blood for analysis of germline mutations in theATM gene using the PTT test and subsequent sequencingwhen there were abnormal results. We found that classicalmutations in the ATM gene do not contribute to thestrongly increased risk of breast cancer following HD.Detailed results are discussed in the report of Division XIII.Tamoxifen and second cancer risk 5In the 1998 Scientific Report we described the firstresults of our nationwide case-control study (n=309)investigating the effects of tamoxifen on the risk andprognosis of endometrial cancer following breast cancer.We reported that the three-year endometrial cancerspecificsurvival was significantly worse for long-termtamoxifen users than for non-users. In 1999 we foundthat long-term tamoxifen users more often developedendometrial tumors with unfavorable clinicopathologicalcharacteristics (malignant mixed mesodermal tumors andsarcomas of the endometrium). Furthermore, theendometrial tumors of long-term tamoxifen users weremore often estrogen-receptor negative than those ofnon-users (61% versus 26%), and were more oftenp53-positive than those of non-users (31% versus 18%).Late health effects of nasopharyngeal radium irradiation inchildhood 6In close collaboration with the Reinaert Clinic inMaastricht and the US National Cancer Institute we areconducting a nationwide cohort study among childrenwho have undergone nasopharyngeal radium irradiation.The aim of the study is to examine the very long-termrisks of head and neck cancer and disorders related toradiation-exposure of the thyroid and pituitary glands.From nine Dutch hospitals a historic cohort wasconstructed of 5,392 children who were treated withradium at an ear-nose-throat (ENT) ward between 1945and 1980. The control group consists of 5,291 childrenwho were treated in the same hospital for ENT-relateddisorders, but without radium. After completion ofextensive follow-up procedures, a total of 624 (8.5%)deaths were observed. Cause of death information couldbe obtained for all but 2 deceased at StatisticsNetherlands. Due to incomplete treatment data the finalnumber of deceased persons eligible for analysis was616, 302 among the irradiated group and 314 amongcontrols. Among the irradiated group we observed 97deaths due to malignant disease whereas 84 wereexpected based on gender-, age- and calendar periodspecificreference data, rendering an observed/expected(O/E) ratio of 1.15 (95% CI, 0.93-1.40). Among controls,the O/E ratio was 1.01 (87/86.3). Analyses of tumorspecificmortality as well as direct comparisons of theexposed and non-exposed groups by survival analysisare underway. Furthermore, cancer incidence data werecollected and will be analyzed similarly. Dosimetric datawill soon be available for incorporation in further analyses.Notes1 Division IX.2 Division XIII.3 Funding: Dutch Cancer Society, Project <strong>NKI</strong> 98-1833.4 External collaborators: MA Crommelin MD, CatharinaHospital, Eindhoven; JGM Klijn MD PhD, ADG KrolMD, MB Van ‘t Veer MD PhD, Daniel den HoedCancer Center/Erasmus University Rotterdam; EMNoordijk MD PhD, Leiden University Medical Center;CL Land PhD, LB Travis MD PhD, RadiationEpidemiology Branch, National Cancer Institute, USA:M Stovall PhD, The University of Texas MD AndersonCancer Center, USA.5 External collaborator: J Benraadt MD, ComprehensiveCancer Center Amsterdam.6 External collaborators: PG Verduijn MD PhD, CMRonckers MSc, Reinaert Clinic, Maastricht.Publications: Cancer riskBroeks A, Russell NS, Floore AN, Urbanus JHM, Dahler EC, Van’t Veer MB, Hagenbeek A, Noordijk EM, Crommelin MA, VanLeeuwen FE, Van ‘t Veer LJ. Increased risk of breast cancerfollowing irradiation for Hodgkin’s disease is not a result of ATMgermline mutations. Int J Radiat Biol (in press).Broeks A, Urbanus JHM, Floore AN, Dahler EC, Klijn JGM,Rutgers EJT, Devilee P, Russell NS, Van Leeuwen FE, Van ’t VeerLJ. Classical ATM germline mutations contribute to breast cancersusceptibility. Am J Hum Genet (in press).Metayer C, Clarke EA, Glimelius B, Storm H, Pukkala E, VanLeeuwen FE, Lynch CF, Curtis RE, Holowaty EJ, Wikstrand G,Andersson M, Wiklund T, Gospodarowicz M, Travis LB. Secondcancer in long-term survivors of Hodgkin’s disease diagnosed inchildhood and adolescence. J Natl Cancer Inst (in press).Van Leeuwen FE. Does risk of endometrial cancer increase withlonger duration of tamoxifen use? Eur J Cancer 1998; 34: S44-5.Van Leeuwen FE, Klokman WJ, Van ’t Veer MB, Hagenbeek A,Krol ADG, Vetter UAO, Schaapveld M, Van Heerde P, BurgersJMV, Somers R, Aleman BMP. Long-term risk of second malignancyin survivors of Hodgkin’s disease treated during adolescenceor young adulthood. J Clin Oncol (in press).Van Leeuwen FE, Swerdlow AJ, Valagussa P, Tucker MA. Secondcancers. In: Mauch PM, Armitage JO, Diehl V, Hoppe RT, WeissLM, editors. Hodgkin’s disease. Philadelphia: Lippincott Williams& Wilkins, 1999: 607-32.
145Secretary Psychosocial Research and EpidemiologyM Van den HoornResearch staff positions (full time equivalents)Scientific permanent: 3.6Scientific project: 9.9Technical permanent: 6.0Technical project: 9.4PSYCHOSOCIAL RESEARCH AND EPIDEMIOLOGY
146XIII Division of DiagnosticOncologyDivision head M Van de VijverHeadMJ Van de Vijver MD PhDPermanent academic staffAPE Besnard MD, JMG Bonfrer PhD,D De Jong MD PhD, MPW Gallee MD PhD,CA Hoefnagel MD PhD, FBL Hogervorst PhD,W Koops MD, R Kröger MD, SH Muller PhD,PM Nederlof PhD, WJ Nooijen PhD,FA Pameijer MD PhD, JL Peterse MD,L Schultze Kool MD PhD,MJA Smid-Geirnaerdt MD PhD,RA Valdés Olmos MD PhD, LJ Van ‘t Veer PhD,MLF Van Velthuysen MD PhD, S Verhoef MDOther academic staffN Bijker, E Deurloo, IF Faneyte, KGH Gilhuys, H Klaren,W Klein Zeggelink, I Kluijt MD PhD, FH Menko MD PhD,LMTh Sterk MD, N Verra, M Van VlietPermanent technical staffD Atsma, LH Boerrigter-Barendsen,MS Boutmy-De Lange, G Brink, CPE Ottenheim,J Poodt, R Pruntel, R Regnerus, C Schippers-Gillissen,O Van Tellingen PhD, P WismanOther technical staffT Van WelsemGuestC Hari Aparici MDSecretarySG MassinkResearch funded positions (full time equivalent)Clinical permanent: 16.6Scientific Permanent: 3.1Clinical projects: 5.6Scientific projects: 0.8IntroductionThe Division of Diagnostic Oncology comprises theDepartments of Clinical Chemistry, Nuclear Medicine,Pathology and Radiology.The Department of Radiology is involved in an increasingnumber of collaborative research projects. There is collaborativework with the universities of Malmo and Leiden todevelop a new percutaneous method of isolated liverperfusion as a treatment for liver metastases for colorectalcancer. National collaboration projects include: evaluationof the value of MRI (and dynamic MRI) in the diagnosis andfollow-up of soft tissue tumors; dynamic MRI screening inwomen with an increased risk to develop breast cancer;assessment of the diagnostic value of stereotactic biopsyof occult breast lesions. In-house collaborative projectsinclude the treatment of head and neck malignancies withintra-arterial chemotherapy and radiotherapy (RADPLAT);quantitative assessment of treatment margins and implementationof multimodality imaging in breast-conservingtherapy. All these projects were started over the past twoyears, and the first results can be expected next year.Within the department of Pathology, much effort isbeing put into building a strong translational researchprogram. As part of the ‘Markerstudy project’, thecollection of DNA and mRNA from well characterizedtumours has continued. N Bijker, working on the analysisof a large clinical trial together with the EORTC BreastCancer Cooperative Group, has found that radiotherapyimproves local recurrence free survival in breast conservingtreatment of ductal carcinoma in situ (DCIS) of the breast.There have been site visits to the centers participating inthis clinical trial and the histology of the DCIS cases hasbeen reviewed. This has resulted in very high quality of theclinical and pathological data for this trial.Ongoing research on 131 I-MIBG in the diagnosis andtreatment of various tumor types continues to result inrefinements to diagnostic and therapeutic regimensinvolving this compound. The sentinel node procedure,an important clinical research area at our institute, is veryrapidly turning into a standard clinical procedure. This willresult in great benefit for patients with breast, vulva andpenis cancer and malignant melanoma; standard lymphnode dissection can now be reserved for only thosepatients with metastatic disease.
Department of Clinical ChemistryP Baas 1 , H Bardelmeijer, CGJ Cleypool,HM De Feij -de Graaf, BM Jansen, L Jansen 2 ,CM Korse, TC Linders, OE Nieweg 3 , M Ouwehand,M Rozenhart, JH Schouwink 1 , Y Souwer,HR Van der Woude, O Van Tellingen, E Van Zandbergen,JH Beijnen 1 , JMG Bonfrer, WJ NooijenPharmacological studies in miceWe have shown that the nonlinear pharmacokineticbehavior of paclitaxel in mice and patients is a pseudononlinearitycaused by Cremophor EL. This probablyoccurs through the formation of micelles which entrappaclitaxel in the plasma compartment. The linear pharmacokineticbehavior of docetaxel can be explained by thefact that the excipient polysorbate 80 is unable to formmicelles because of rapid degradation in plasma.In line with studies in mice, the use of the P-glycoproteinblocker cyclosporin A results in an enhanced oralbioavailability of paclitaxel in patients. Cyclosporin A isalso able to enhance the oral bioavailability of docetaxel inmice and clinical studies have been initiated. In spite of itsapparent activity in other studies the compound R101933was unable to increase the oral bioavailability of paclitaxelin mice and consequently further clinical testing was notattempted. In contrast, GF120918 was able to enhancethe oral bioavailability of paclitaxel to the level observed inP-glycoprotein deficient mice. Moreover, this compoundappears to be a very selective blocker of P-glycoprotein,since its co-administration to P-glycoprotein deficient micedid not change the pharmacokinetic handling of paclitaxel.Clinical studies with GF120918 have been initiated.The clinical studies with oral paclitaxel and cyclosporinA indicate a reduced oral bioavailability of paclitaxel athigher dose levels. Studies in mice suggest that this maydepend on the amount of Cremophor EL in the oralformulation. In P-glycoprotein deficient mice, only about5% of an oral dose of 10 mg/kg of paclitaxel wasrecovered in the feces indicating almost complete gastrointestinaluptake. However, the fecal recovery of paclitaxelincreased substantially when the amount of CremophorEL increased by 6-fold. Similar to the findings in plasma,Cremophor EL is thought to form micelles, which entrappaclitaxel, thus reducing the fraction of paclitaxelavailable for absorption.P-glycoprotein in the blood barrier barrier protects thebrain against the penetration of many toxic substances.The usefulness of various (presumed) P-glycoproteinblockers for increasing the brain penetration of paclitaxelhas been tested. Blocking of P-glycoprotein in the BBBhas proven to be very difficult. Only very effectiveblockers, such as GF120918, were able to partially blockP-glycoprotein in the BBB.Tumor markersUsing immunohistochemistry, S-100 protein can bedemonstrated in malignant melanoma cells. It was laterdemonstrated that the S-100 protein was also present inserum and a S-100B specific commercial test has beendeveloped. Previous studies have shown that the serumlevel of S-100B is an independent prognostic factor forsurvival in patients with malignant melanoma. Increasingmarker levels can predict recurrence of disease beforeclinical symptoms have developed.The evaluation of response to therapy in lungcarcinoma may sometimes be difficult. Cyfra 21.1 andTissue Polypeptide Antigen (TPA) were previouslyevaluated. A newly developed assay, using mAbs todetect specific epitopes of cytokeratin 19 fragments, wastested for its sensitivity and specificity in non small celllung cancer. It was demonstrated that the effectivenessof this marker, in terms of sensitivity/specificity, was nogreater than TPA and Cyfra 21.1.Notes1 Division X.2 Division IX.3 Division XI.Department of Nuclear MedicineE Bais 2 , H Boot 2 , JH Borger 1 , O Dalesio 4 ,J De Kraker 5 , L Jansen 3 , M Kooi 4 , BBR Kroon 3 ,C Mari Aparici, OE Nieweg 3 , BR Pieters 1 ,EJTh Rutgers 3 , BG Taal 2 , P Tanis 3 ,WW Ten Bokkel Huinink 2 , PA Voûte 5 , CA Hoefnagel,SH Muller, RA Valdés Olmos131I-MIBG therapy of neural crest and other tumorsFor the purpose of pooling European results of131I-MIBG (meta-iodobenzylguanidine) therapy in neuralcrest tumors, the data of 208 patients treated with131I-MIBG at the Netherlands Cancer Institute since 1984were reviewed. Objective response rates in malignantpheochromocytoma and paraganglioma were 43% and57%, respectively.140 children with neuroblastoma were treated with131I-MIBG and 3 clinical situations can be distinguished.1) In 59 patients receiving 131I-MIBG therapy afterconventional treatment had failed, the objective responserate was 52.7% and palliation was provided to mostpatients; 5 of these patients survived >5 years; hematologicaltoxicity occurred in 82.5%. 2) 27 patients withresidual tumor or first recurrence after chemotherapyreceived 131 I-MIBG in combination with oxygen underhyperbaric conditions. Partial remission was attained in41.7% and hematological toxicity occurred in 90%. 3) Incontrast, 54 patients with inoperable stage III or IV neuroblastomatreated with 131 I-MIBG at first diagnosis insteadof combination chemotherapy, had an objective responserate of 81.5% with considerably less hematologicaltoxicity (37.3%); 11 of 30 patients with >5 years followup are alive (longest survival >9 years).In 48 patients with symptomatic, metastatic carcinoid147DIAGNOSTIC ONCOLOGY
148DIAGNOSTIC ONCOLOGYtumors, no objective responses and minimal toxicity wasrecorded; however palliation with a mean duration of 8months was attained in 60% of the patients. In addition,2 of 5 patients with medullary thyroid carcinoma had apartial remission, while 4 had a palliative response to131I-MIBG therapy.In patients with non-neuroendocrine tumors whoreceived escalating doses of unlabeled MIBG in thecontext of a phase I study, scintigraphy using 131 I-MIBGdid not reveal tumor uptake in any of these tumours,confirming the specificity of this agent for neural cresttumours. The influence of unlabeled MIBG on the biodistributionof 131 I-MIBG was studied.Radioimmunoscintigraphy of radioimmunotherapyIn a pilot study of radioimmunoscintigraphy of neuroblastomausing 131 I-labeled chimeric chCE7 antibodies,encouraging results were obtained in 7 patients, demonstratingthe complementarity of this targeting modality to131I-MIBG imaging. In collaboration with the Paul ScherrerInstitute (PA Schubiger and I Novak-Hofer) a protocolwas submitted for a comparative study of combineddiagnostic scintigraphy using 131 I-chCE7 and 131 I-MIBG inselected cases of neuroblastoma.The multicenter phase I clinical study on radioimmunotherapyof medullary thyroid cancer using the two-steptargeting technique with bispecific immunoconjugate and131 I- labelled bivalent hapten (M96MTC) was concludedand the promising results in 24 patients were published.A phase II study is in preparation. A working party wascreated to explore the possibilities of starting up radioimmunotherapyof recurrent non-Hodgkin lymphoma usingradiolabeled anti-CD20 antibodies.Dosimetry of 131 I-therapy in differentiated thyroid carcinomaThe EU-project (F14CCT960009) on improvement ofdosimetry for 131 I-therapy of intrathoracic tumors wasconcluded in June 1999. In patients with differentiatedthyroid carcinoma and neural crest tumors, treated with131I-iodide or 131 I-MIBG respectively, absorbed radiationin pulmonary metastases was calculated, at theUniversity of Wuerzburg, after calibration of the gammacameras of participating centers. A follow up study is inpreparation.Sentinel Node LymphoscintigraphyThe findings of mammary lymphoscintigraphy wereevaluated in 150 consecutive patients with breastcarcinoma: 100 patients (group A) investigated in thevalidation phase of the study, and 50 (group B) after thedose of 99m Tc nanocolloid was optimized. In group A(mean dose 61.6 MBq, range 42-88 MBq) scintigraphyvisualized lymph nodes in 83 patients (83%) with anincrease in the visualization rate from 72% for the first 40patients to 90% for the last 60. Only patient age (p=0.01)and administered tracer dose (p=0.04) were found to besignificant factors for visualization in a multifactorialanalysis. In group B (mean dose 90.8 MBq, range 68-124 MBq) the visualization rate was 94%. In combinationwith intraoperative blue dye mapping and gammaprobe the overall identification rate was 90% for group Aand 98% in group B.A phantom study, performed to evaluate scattersuppression in sentinel node detection, showed that forsuperficial nodes the gamma probe should be fitted witha shield and for deep nodes with a collimator.111In antimyosin in anthracycline related cardiotoxicityA prospective longitudinal study was started in cooperationwith the University Hospital Sant Pau ofBarcelona (N16 AMBAR), to determine the value of 111 Inantimyosin in the detection of early subclinical anthracyclinecardiotoxicity and the prediction of late cardiac events. In24 patients who completed treatment, 111 In antimyosincardiac uptake, as measured by heart-to-lung ratios, wassignificantly increased (p=0.0001) at low cumulative dose(120-150 mg/m 2 ) and subsequent dose levels, whereas leftventricle ejection fraction and peak filling rate were bothonly significantly changed at high cummulative dose levels(360-450 mg/m 2 ). These results suggest that anthracyclinerelated myocyte damage precedes systolic and diastoliccardiac function alterations even at low cumulative doses.Internal mammary chainA computer assisted method to measure the lateralizationof internal mammary lymph nodes was developed.In 100 consecutive patients both analog and digitalmeasurements of two 57 cobalt point sources positionedon the jugular notch and xiphoid process correlated well(r=0.9). In approximately 70% of the patients the mostlateral lymph node was located less than 4 cm from thesternal midline. In cooperation with Division IX, thiscomputer assisted method will be used routinely inpatients to adjust the irradiation field.Diagnosis of pulmonary embolismIn cooperation with the Slotervaart Hospital, theDepartment of Nuclear Medicine has participated in amulticentre study on optimizing diagnostic strategies forpulmonary embolism (COG nr. D94-90). A total of 627consecutive patients clinically suspected for pulmonaryembolism were included and in 517 of them a diagnosticconclusion was reached. With respect to patients withsegmental or larger embolism and a high probabilityperfusion/ventilation scan, the sensitivity of spiral CT wasalmost 90%, whereas in subsegmental embolism thisdecreased to 21%. For lung ventilation, 99m Tc-technegaswas compared with Krypton-81, showing a relative lowconcordance (kappa 0.69) and limited clinical value.Notes1 Division IX.2 Division X.3 Division XI.4 Biometrics Department.5 Emma Kinderziekenhuis/AMC.
Department of PathologyGenetic alterations in tumorsD Atsma, N Bijker, O Dalesio 2 , L Duchateau 8 ,IS Fentiman 6 , M Gallee, FBL Hogervorst, J-P Julien 7 ,J Poodt, EJTh Ruthers 5 , C Schippers-Gillissen, B Taal 3 ,N Ter Haar 1 , M Van Beurden 4 , JA Van Dongen 5 ,ACM Van Lindert 4 , L Van Velthuysen, T Van Welsem,CJ Vos 1 , D De Jong, PM Nederlof JL Peterse,MJ Van de Vijver, LJ Van ’t Veer149DIAGNOSTIC ONCOLOGYMarker studyThe purpose of this project is to establish well-characterizedseries of various tumor types, for which DNA,mRNA and extensive clinicopathological information isavailable. These series are available for testing ofexpression pattern or mutational status of novel genes inassociation with pathological and clinical parameters.Seven series have been prepared: breast carcinomastage I and II; breast carcinoma stage III and IV;malignant melanoma (mainly lymph node metastases);renal cell carcinoma; malignant mesothelioma; gastriccarcinoma; malignant lymphoma. Future series willinclude squamous cell carcinoma of the head and neck;colon carcinoma; lung carcinoma; and gynecologicalmalignancies.Genetic alterations specific for breast and ovariancarcinomasThe purpose of this project is to characterize the(somatic) genetic alterations in breast and ovarian carcinomasof patients with BRCA1 germline mutations andcompare these with genetic alterations in sporadic breastcarcinomas. We have used comparative genomic hybridization(CGH) for the detection of genetic alterations in thefollowing set of tumors: 20 breast carcinomas fromBRCA1 germline mutation carriers; 29 breast carcinomasfrom patients with bilateral breast cancer (for 12 patientsFigure XIII.1Deletion of several regions on chromosome 4 in breast cancer.49 Breast carcinomas were analyzed by CGH; the frequency ofloss of various regions on chromosome 4 is depicted. It appearsthat there are four distinct regions that are likely to harbor atumor suppressor gene.Figure XIII. 2Model for the role of genetic alterations in the development ofinvasive breast cancer. There are at least four distinct pathwaysleading to different histologic types of breast cancer. Each ofthese pathways is characterized by specific genetic alterations.ILC = invasive lobular carcinoma; IDC = invasive ductalcarcinoma; LCIS = lobular carcinoma in situ; DCIS = ductalcarcinoma in situ.the tumors from both breasts were analyzed); 10 breastcarcinomas from patients that also developed ovariancarcinoma. Our first analysis indicates that the profile ofgenetic alterations in breast carcinomas from patientswith BRCA1 germline mutations differ, with respect to thefrequency with which gains and losses are observed,from patients with sporadic breast carcinoma.It has been reported that losses on chromosome 4 aremore frequent in carcinomas from patients with BRCA1germline mutations. We have focused on losses onchromosome 4 and identified four regions with frequentloss (Figure XIII.1). We do not find differences betweensporadic and BRCA1 associated carcinomas with respectto losses on chromosome 4.In collaboration with Leiden University Medical Centerwe have analyzed genetic alterations in a large series ofductal carcinomas in situ (DCIS) of the breast without aninvasive component. By comparing these with thegenetic alterations known to be present in invasive breastcancer, we have designed the model for breast cancerdevelopment (Figure XIII.2). In brief: inactivation of E-cadherin is involved in the development of all cases oflobular carcinoma in situ and is never found in thedevelopment of cancers of ductal type. Inactivation of a,not yet identified, tumor suppressor gene onchromosome 16q is involved in the development of welldifferentiated DCIS; amplification of the HER2/neu geneand mutational inactivation of the p53 gene are involvedin the development of poorly differentiated DCIS. It is notknown which genetic alterations play a role in theprogression of carcinoma in situ to invasive breastcancer. The identification of these genetic alterations issubject of ongoing studies presented elsewhere (DivisionVIII).
150DIAGNOSTIC ONCOLOGYDuctal carcinoma in situ of the breast: conservingtreatment: first results of EORTC trial 10853A randomized phase III clinical trial has beenconducted by the EORTC Breast Cancer CooperativeGroup, to investigate the role of radiotherapy in breastconserving treatment of DCIS. Women (n=1,010) withductal carcinoma in situ (DCIS) of the breast were treatedby complete local excision of the lesion and thenrandomly assigned to either no further treatment or toradiotherapy. At a median follow-up of 51 months, the 4-year local relapse-free interval was 84% in the grouptreated with local excision alone, compared with 91% inthe women treated by local excision plus radiotherapy(p=0.005, HR 0.62). Long-term follow-up will be neededto determine whether improved local control leads to areduction in distant metastases and deaths from breastcancer.Of the cases randomized, histologic sections from 845(84%) patients have been reviewed; in 694 cases thediagnosis DCIS was confirmed. In 44 cases a benignlesion was found; in 62 patients the lesion was consideredatypical ductal hyperplasia rather than DCIS, in 26cases a (micro)invasive lesion was found, and in another12 cases there was suspicion of invasion. At a medianfollow-up of 51 months only one event was seen in thegroup of ADH. The DCIS subtype was not significantlyrelated to the risk of local recurrence. However, poorlydifferentiated DCIS had a significantly higher rate ofdistant metastases than did the other subtypes (p=0.01).In a separate study, the diagnostic and therapeuticprocedures which were followed in the trial wereevaluated. It emerged that large variations occurred,particularly with respect to the surgical procedures andhistopathological work-up. Important risk factors liketumor size and margin status were poorly quantified inthe medical files. These findings emphasize the need forestablishing uniform guidelines for diagnostic and therapeuticprocedures for DCIS, and for clearly defined riskfactors for recurrence after BCT for DCIS.Notes1 Leiden University Medical Center, Funding: DutchCancer Society, Project RUL94-757.2 Biometrics Department.3 Division X.4 Division XI (Gynecology).5 Division XI (Surgery).6 Guy’s Hospital, London.7 Centre Henri Becquerel, Rouen.8 EORTC Data Center, Brussels.LymphomaLH Boerrigter-Barendsen, MS Boutmy-de Lange,T Dellemijn, FA Vyth-Dreese, H Boot, D De JongH.pylori eradication is generally accepted as the firstchoice of treatment for stage I low-grade gastric MALTlymphoma. Treatment failure may be attributed to theextent of the disease and to progression into an antigenindependentphase. Morphological and functionalimmunohistochemical markers were investigated toidentify this transition in 23 consecutive low-grade MALTlymphoma patients treated with H.pylori eradication in the<strong>NKI</strong>/<strong>AvL</strong>. Complete regression after H.pylori eradicationwas achieved in 13/23 patients (56%), partial regressionin 2 patients (9%) and no response in 8 patients (35%).Histological grading was highly predictive of clinicalresponse, especially in stage I patients, with completeremissions in 10/12 tumors with purely low-grade (typeA) morphology and 1/8 tumors with increased numbersof blasts (type B) (p=0.0046). Histological grading wasalso related to the expression of co-stimulatory markers(p=0.0061). CD86 as a single marker proved to be ofpredictive value for treatment outcome (p=0.0086). Thesetumor-related factors should be taken into account in thedecision to treat gastric MALT-NHL patients with H.pylorieradication alone or to add ‘classical’ anti-cancermodalities early in the course of follow-up.Since variations in diagnostic criteria and stagingprocedures in gastric MALT have important consequencesfor patient selection and strongly bias theoutcome of clinical trials, we performed a survey on themanagement of this disease among 19 leading instituteswith a special interest in this field in Europe, the UnitedStates and Japan. Minimum histological criteria variedamong pathologists with a notable influence of the classificationsystem used in the different countries. Detailedevaluation of the lymphoma distribution in the gastric walland routine staging of the GI-tract differed betweengroups lead by medical oncologists and gastro-enterologists.Similar effects were recorded for the role of gastricresection and radiotherapy.The Netherlands Cancer Institute FamilyCancer ClinicLH Boerrigter-Barendsen, G Brink, D Hahn,FBL Hogervorst, E Kaats, H Klaren, I Kluijt 2 , FH Menko 3 ,CPE Ottenheim, R Pruntel, R Regnerus, EJTh Rutgers4,M Van Beurden 1 , A Van Rens, S Verhoef, G Wigbout,LJ Van ’t VeerSince the start of the Family Cancer Clinic in 1995,over 500 families (approximately 1,400 individuals) havesought genetic advice in our hospital. DNA testing wasperformed in 310 breast cancer families (BRCA1/BRCA2)and in 130 colon cancer families (microsattellite instability,
mismatch repair genes: hMLH1/hMSH2/hMSH6).Moreover, DNA testing is carried out for approximately200 families counseled at the Academic MedicalHospital, Amsterdam. Germline mutations in one of thecancer susceptibility genes were found in 82 breastcancer families and in 8 colon cancer families. Inaddition, for 40 colon cancer families genomic instabilityin the tumor tissue (indicating the presence of mismatchrepair deficiency) was determined and used as a markerfor further genetic investigation and counseling. Ourevaluation of probabilities of finding a DNA mutationrevealed that positive test results can be found in 25% ofthe families tested. Specific ‘family characteristics’ raisethis chance.In 1999 special attention was given to the psychosocialneed of families in counseling. As part of a pilotstudy, all families counseled were offered standardpsychosocial care and over 80% of the participants werein favor of this support in addition to the geneticcounseling itself.It is well known that cancer susceptibility variesbetween and within families with a hereditary predisposition.In a nationwide cohort study (study-coordinatorsfrom the Department of Epidemiology and the FamilyCancer Clinic, see Division XII), gene-environment interactions,including hormonal and life-style factors, will beexamined in 1,400 high-risk breast and/or ovarian cancerfamilies. More specific risk estimates will also beassessed for families stratified according to their extent ofgenetic predisposition.Clinical outcome of treatment of BRCA1/BRCA2 breastcancer patients will be evaluated in a case-control studyfor breast conserving therapy and in a case-control studyfor contralateral breast cancer development after radiotherapy.Results will be essential for designing optimaltherapeutic strategies for BRCA1/BRCA2 carriers. Forpre-symptomatic BRCA1 and BRCA2 carriers, importantinformation might be generated that can be used indecision making between surveillance by mammographyor bilateral prophylactic mastectomy.carcinoma [n = 30] and T1 - T4 supraglottic carcinoma[n = 29]) treated with definitive RT. On the pretreatmentCT study, each tumor was assigned a high- or low-riskprofile for local failure after RT. The post-RT CT examinationswere evaluated for post-treatment changes using athree-point post-RT CT-score: 1 = expected post-RTchanges (Figure XIII.3); 2 = focal mass with a maximaldiameter of < 1cm and/or asymmetric obliteration oflaryngeal tissue planes; 3 = focal mass with a maximaldiameter of > 1cm, or < 50% estimated tumor volumereduction (Figure XIII.4). The local control rates at 2 yearspost-RT based on pre-treatment CT evaluation were 88%for low pre-treatment risk profile patients and 34% forhigh pretreatment risk profile patients (p = 0.0001).151DIAGNOSTIC ONCOLOGYNotes1 Division XI.2 Department of Clinical Genetics, Academic MedicalCenter, UvA-Amsterdam.3 Department of Clinical Genetics, Free UniversityHospital, AZVU-Amsterdam.4 Division XI.Department of RadiologyR Hermans, PS Kubilis, AA Mancuso, WM Mendenhall,JT Parsons, SP Stringer, H Van Tinteren, FA Pameijer 1Pre- and post-radiotherapy (RT) computedtomographic (CT) studies were used to predict localcontrol in 59 patients with laryngeal carcinoma (T3 glotticFigure XIII. 3CT images of a patient with a T3 carcinoma of the right truevocal cord and a low pretreatment risk profile. A. PretreatmentCT image at the true cord level shows involvement of the entireright cord, which is a paramedian position. The ipsilateral paraglotticspace is obliterated (large arrow), when compared to thecontralateral side (small arrow). B. CT image obtained 4 monthspost-RT at the same level. There is complete resolution of thetumor. The laryngeal tissues appear symmetric, and the paraglotticspace on the right side has reappeared (arrow); post-RTCT-score 1. The patient is without evidence of disease 31months after completion of radiotherapy.
152DIAGNOSTIC ONCOLOGYBased on post-treatment CT, the local control rates at 2years post-RT were 94% for score 1, 67% for score 2and 10% for score 3 (p= 0.0001). Post-RT CT-scoresadded significant information to the pre-treatment riskprofiles on prognosis. We conclude that pre-treatment CTrisk profiles, as well as post-RT CT evaluation, canidentify patients irradiated for laryngeal carcinomas athigh risk for developing local failure. When the post-RTCT-score is available, it proves to be an even betterprognosticator than pretreatment CT risk profile.Note1 Funding: Dutch Cancer Society Fellowship.Publications: Division XIIIFull papersAwada A, Punt CJA, Piccart MJ, Van Tellingen O, Van Manen L,Kerger J, Groot Y, Wanders J, Verweij J, Wagener DJT. Phase Istudy of Carzelesin (U-80,244) given (4-weekly) by intravenousbolus schedule. Br J Cancer 1999; 79: 1454-61.Bonfrer JMG, Korse CM. TPA and CA 15.3 measurements forbreast cancer monitoring in a routine setting. Int J Biol Markers1999; 14: 40-4.Boven E, Jansen WJM, Hulscher TM, Beijnen JH, Van Tellingen O.The influence of P170-glycoprotein modulators on the efficacyand the distribution of vincristine as well as on MDR1 expressionin BRO/mdr1.1 human melanoma xenografts. Eur J Cancer 1999;35: 840-9.Bijker N, Rutgers EJT, Peterse JL, Van Dongen JA, Hart AAM,Borger JH, Kroon BBR Low risk of locoregional recurrence of primarybreast carcinoma after treatment with a modification of theHalsted radical mastectomy and selective use of radiotherapy.Cancer 1999; 85: 1773-81.Chatal JF, Hoefnagel CA. Radionuclide therapy. Lancet 1999;354: 931-5.Clahsen PC, Van de Velde CJ, Duval C, Pallud C, Mandard AM,Delobelle-Deroide A, Van den Broek L, Van de Vijver MJ. The utilityof mitotic index, oestrogen receptor and Ki-67 measurementsin the creation of novel prognostic indices for node-negativebreast cancer. Eur J Surg Oncol 1999; 25: 356-63 .De Jong D, Aleman BMP, Taal BG, Boot H. Controversies andconsensus in the diagnosis, work-up and treatment of gastriclymphoma: an international survey. Ann Oncol 1999; 10: 275-80Baars JW, De Jong D, Willemse EM, Gras L, Dalesio O, VanHeerde P, Huygens PC, Van der Lelie H, Von dem Borne AEGK.Diffuse large B-cell non-Hodgkin lymphomas: the clinical relevanceof histological subclassification. Br J Cancer 1999; 79: 1770-6.Figure XIII. 4CT images of a patient with a T3 carcinoma of the left true vocalcord and a high pretreatment risk profile. C. Pretreatment CTimage just above the false cord level demonstrates involvementof the left aryepiglottic fold and obliteration of the paraglotticspace (arrow). D. CT image at the same level, obtained at 3months post-RT. A focal mass, in the left aryepiglottic fold, witha maximal diameter slightly over 1 cm (arrowheads) hasdeveloped; post-RT CT-score 3. Salvage laryngectomyconfirmed the presence of local recurrence. The patient is alivewithout evidence of disease 2 years, 3 months after theoperation.Elkhuizen PH, Voogd AC, Van den Broek LC, Tan IT, VanHouwelingen HC, Leer JW, Van de Vijver MJ. Risk factors for localrecurrence after breast-conserving therapy for invasive carcinomas:a case-control study of histological factors and alterations inoncogene expression. Int J Radiat Oncol Biol Phys 1999; 45:73-83.Hoefnagel CA, Clarke SEM, Fischer M, Chatal JF, Lewington VJ,Nilsson S, Troncone L, Vieira MR. Radionuclide therapy practiceand facilities in Europe. Eur J Nucl Med 1999; 26: 277-82.Hoefnagel CA, Moonen LMF, Haustermans KMG, Balm AJM.Imaging of tumour hypoxia in nuclear medicine. In: Van der KleijAJ, Voûte PA, Sminia P, editors. Oxygen and onco therapy 98; Vol
1533. Archimedes Hyperbarmedizin und Verlags-GmbH, 1998, 79-87.Hoefnagel CA. Therapy of neuroblastoma. The Update 1999; 6:53-9.Kraeber-Bodéré F, Bardet S, Hoefnagel CA, Vieira MR, Vuillez JP,Murat A, Ferreira TC, Bardiés M, Ferrer L, Resche I, Gautherot E,Rouvier E, Barbet J, Chatal JF. Radioimmunotherapy in medullarythyroid cancer using bispecific antibody and iodine-131-labeledbivalent hapten: papreliminary results of a phase I/II clinical trial.Clin Cancer Res 1999; 5: 3190s-8s.Kremer LCM, Tiel-van Buul MMC, Offringa M, Ottenkamp J,Valdés Olmos RA, Voûte PA. Indium-111-antimyosin scintigraphyin the early detection of heart damage after anthracycline therapyin children. J Clin Oncol 1999; 17: 1208-11.Ligtenberg MJL, Hogervorst FBL, Willems HW, Arts PJW, Brink G,Hageman S, Bosgoed EAJ, Van der Looij E, Rookus MA, DevileeP, Vos EMAW, Wigbout G, Struijcken PM, Menko FH, RutgersEJT, Hoefsloot EH, Mariman ECM, Brunner HG, Van ‘t Veer LJ.Characteristics of small breast and/or ovarian cancer families withgermline mutations in BRCA1 and BRCA2. Br J Cancer 1999; 79:1475-8.Mancuso AA, Mukherji SK, Schmalfuss I, Mendenhall W, ParsonsJ, Pameijer F, Hermans R, Kubilis P. Preradiotherapy computedtomography as a predictor of local control in supraglottic carcinoma.J Clin Oncol 1999 17: 631-7.Nieweg OE, Jansen L, Valdés Olmos RA, Rutgers EJT, PeterseJL, Hoefnagel CA, Kroon BBR. Lymphatic mapping and sentinellymph node biopsy in breast cancer. Eur J Nucl Med 1999; 26:S11-6.Pameijer FA, Hermans R, Mancuso AA, Mendenhall WM, ParsonsJT, Stringer SP, Kubilis PS, Van Tinteren H. Pre- and post-radiotherapycomputed tomography in laryngeal cancer: imagingbasedprediction of local failure. Int J Radiat Oncol Biol Phys1999; 45: 359-66.Taal BG, Hoefnagel CA, Rutgers M. Carcinoid tumors [letter to theeditor]. N Engl J Med 1999; 341:54.Ten Berge RL, Dukers DF, Oudejans JJ, Pulford K, OssenkoppeleGJ, De Jong D, Misere JF, Meijer CJ. Adverse effects of activatedcytotoxic T lymphocytes on the clinical outcome of nodal anaplasticlarge cell lymphoma. Blood 1999; 93: 2688-96.Valdés Olmos RA, Koops W, Loftus BM, Liem IH, Gregor RT,Hoefnagel CA, Hilgers FJM, Balm AJM. Correlative Tl-201 SPECT,MRI and ex-vivo Tl-201 uptake for detecting and characterizingcervical lymphadenopathy in head and neck squamous cell carcinoma.J Nucl Med 1999; 40: 1414-9.Valdés Olmos RA, Hoefnagel CA, Nieweg OE, Jansen L, RutgersEJTh, Borger J, Horenblas S, Kroon BBR. Lymphoscintigraphy inoncology: a rediscovered challenge. Eur J Nucl Med 1999; 26:S2-S10.Valdés Olmos RA, Jansen L, Muller SH, Hoefnagel CA, NiewegOE. Aportacion de la medicina nuclear al estudio del drenaje linfáticoy la identificacion de ganglio linfático centinela en oncologia.Rev Esp Med Nucl 1999; 18: 111-21.Van Asperen J, Van Tellingen O, Schinkel AH, Beijnen JH.Comparative pharmacokinetics of vinblastine after a 96-hour continuousinfusion in wild-type mice and mice lacking mdr1a P-glycoprotein.J Pharmacol Exp Ther 1999; 289: 329-33.Van Asperen J, Van Tellingen O, Tijssen F, Schinkel AH, BeijnenJH. Increased accumulation of doxorubicin and doxorubicinol incardiac tissue of mice lacking mdr1a P-glycoprotein. Br J Cancer1999; 79: 108-13.Van de Vijver MJ. The pathology of familial breast cancer: the pre-BRCA1/BRCA2 era: historical perspectives. Breast Cancer Res1999; 1: 27-30.Van der Sande JJ, Boogerd W, Kröger R, Kapelle AC. Recurrentspinal epidural metastases: a prospective study with a completefollow up. J Neurol Neurosurg Psychiatry 1999; 66: 623-27.DIAGNOSTIC ONCOLOGYSloane JP, Amendoeira I, Apostolikas N, Bellocq JP, Bianchi S,Boecker W, Bussolati G, Coleman D, Connolly CE, Eusebi V, DeMiguel C, Dervan P, Drijkoningen R, Elston CW, Faverly D, Gad A,Jacquemier J, Lacerda M, Martinez-Penuela J, Munt C, PeterseJL, Rank F, Sylvan M, Tsakraklides V, Zafrani B. Consistencyachieved by 23 European pathologists from 12 countries in diagnosingbreast disease and reporting prognostic features of carcinomas.European Commission Working Group on BreastScreening Pathology. Virchows Arch 1999; 434: 3-10.Szymanska H, Sitarz M, Krysiak E, Piskorowska J, CzarnomskaA, Skurzak H, Hart AA, De Jong D, Demant P. Genetics ofsusceptibility to radiation-induced lymphomas, leukemias andlung tumors studied in recombinant congenic strains. Int J Cancer1999 83 674-8.Van Tellingen O, Huizing MT, Nannan Panday VR, Schellens JHM,Nooijen WJ and Beijnen JH. Cremophor EL causes (pseudo) nonlinearpharmacokinetics of paclitaxel in patients. Br J Cancer1999; 81: 330-35.Van Tienhoven G, Voogd AC, Peterse JL, Nielsen M, AndersenKW, Mignolet F, Sylvester R, Fentiman IS, Van der Schueren E,Van Zijl K, Blichert-Toft M, Bartelink H, Van Dongen JA Prognosisafter treatment for loco-regional recurrence after mastectomy orbreast conserving therapy in two randomised trials (EORTC10801 and DBCG-82TM): EORTC Breast Cancer CooperativeGroup and the Danish Breast Cancer Cooperative Group. Eur JCancer 1999; 35: 32-8.
154DIAGNOSTIC ONCOLOGYVan Zandwijk N, Van ‘t Veer LJ, Antioxidants and the chemopreventionof lung cancer. In: Brambilla C, Brambilla E, editors. Lungtumors, fundamental biology and clinical management. New York:Marcel Dekker, 1999: 321-34.Vos CB, Ter Haar NT, Peterse JL, Cornelisse CJ, Van de Vijver MJ.Cyclin D1 gene amplification and overexpression are present inductal carcinoma in situ of the breast. J Pathol 1999; 187: 279-84.Voogd AC, Van der Horst F, Crommelin MA, Peterse JL, Van BeekMW, Repelaer Van Driel OJ, Van der Heijden LH, Coebergh JW.The relationship between findings on pre-treatment mammogramsand local recurrence after breast-conserving therapy forinvasive breast cancer. Eur J Surg Oncol 1999; 25: 273-9.Zuetenhorst H, Taal BG, Boot H, Valdés Olmos RA, HoefnagelCA. Longterm palliation in metastatic carcinoid tumours withvarious applications of meta-idobenzylguanidine: pharmacologicalMIBG, 131I-labeled MIBG and the combination. Eur JGastroenterol Hepatol 1999; 11: 1157-64.Full papers in pressBardelmeijer HA, Van Tellingen O, Schellens JHM, Beijnen JH. Theoral route for administering cytotoxic drugs: strategies to increasethe efficiency and consistency of drug delivery. Invest New Drugs1999 (in press).De Jong D, Boot H, Taal B. Histological grading with clinical relevancein gastric mucosa-associated lymphoid tissue (MALT) lymphoma.Recent Results Cancer Res 1999 (in press).Elkhuizen PHM, Van Slooten HJ, Clahsen PC, Hermans J, Van deVelde CJH, Van den Broek LCJM, Van de Vijver MJ and cooperatinginvestigators. The high local recurrence risk after breast conservingtherapy in node negative premenopausal patients isgreatly reduced by one cycle of perioperative chemotherapy, anEORTC Breast Cancer Cooperative Group study. J Clin Oncol1999 (in press).Hermans R, Pameijer FA, MancusoAA, ParsonsJT, et al.. Can follow-upcomputed tomography after definitive radiotherapy forlaryngeal or hypopharyngeal carcinoma detect failure earlier thanclinical examination alone? Radiology 1999 (in press)Hoefnagel CA. Therapy of neuroblastoma. J Nucl Med 1999 (inpress).Hoefnagel CA. Targeted radiotherapy of neuroblastoma. In:Abrams PG, Fritzberg AR, editors. Radioimmunotherapy of cancer.New York: Marcel Dekker, 1999 (in press).Hoefnagel CA, Taal BG, Sivro F, Boot H, Valdés Olmos RA.Enhancement of I-131 MIBG uptake in carcinoid tumours byadministration of unlabelled meta-iodobenzylguanidine. Nucl MedCommun (in press).Horenblas S, Jansen L, Meinhardt W, Hoefnagel CA, De Jong D,Nieweg OE. Detection of occult metastasis in squamous cell carcinomaof the penis using a dynamic sentinel node procedure. JUrol 1999 (in press).Julien JP, Bijker N, Fentiman IS, Peterse JL, Delledonne V,Rouanet P, Avril A, Sylvester R, Mignolet F, Bartelink H, VanDongen JA on behalf of the EORTC Breast Cancer CooperativeGroup and EORTC Radiotherapy group. The role of radiotherapyin breast conserving treatment for ductal carcinoma in situ (DCIS):first results of EORTC randomized phase III trial 10853. Lancet1999 (in press).Staalman CR and Hoefnagel CA. Imaging of neuroblastoma andmetastasis. In: Brodeur GM, Sawada T, Tsuchida Y, Voûte PA, editors.Neuroblastoma. Amsterdam: Elsevier, 1999 (in press).Theuws JCM, Muller SH, Seppenwoolde Y, Kwa SLA, BoersmaLJ, Hart GAM, Baas P, Lebesque JV. The effect of radiotherapyand chemotherapy on pulmonary function following treatment forbreast cancer and lymphoma. J Clin Oncol 1999 (in press)Van Asperen J, Van Tellingen O, Beijnen JH. The role of mdr1aP-glycoprotein in the biliary and intestinal secretion of doxorubicinand vinblastine in mice. Drug Metab Dispos 1999 (in press).Van de Vaart PJM, Belderbos J, De Jong D, Sneeuw KCA, MajoorD, Bartelink H, Begg AC. DNA-adduct levels as a predictor of outcomefor NSCLC patients receiving daily cisplatin and radiotherpay.Int. J Cancer 1999 (in press).Van Tellingen O, Beijnen JH, Verweij J, Scherrenburg EJ, NooijenWJ, Sparreboom A. Rapid esterase sensitive breakdown of polysorbate80 and its impact on the plasma pharmacokinetics ofdocetaxel and metabolites in mice. Clin Cancer Res 1999 (inpress).Theuws JCM, Muller SH, Seppenwoolde Y, Kwa SLA, BoersmaLJ, Hart GAM, Baas P, Lebesque JV. The effect of radiotherapyand chemotherapy on pulmonary function following treatment forbreast cancer and lymphoma. J Clin Oncol 1999 (in press).Valdés Olmos RA, Jansen L, Hoefnagel CA, Nieweg OE, MullerSH, Rutgers EJTh, Kroon BBR. Evaluation of mammary lymphoscintigraphyby single intratumoral injection for sentinel node identification.J Nucl Med 1999 (in press).Hoefnagel CA. Therapy of Neuroendocrine Tumors with MIBG. In:Salvajoli JV, editor: Radiotherapy. Rio de Janeiro: Editora MEDSI,1999 (in press).Vos CBJ, Ter Haar NT, Rosenberg C, Peterse JL, Cleton-JansenA-M, Cornelisse CJ, Van de Vijver MJ. Genetic alterations onchromosome 16 and 17 are important features of ductal carcinomain situ of the breast and are associated with histologic type. BrJ Cancer 1999 (in press).
155Local papersDe Klerk JMH, Goslings BM, Koppeschaar HPF, HuysmansDAKCJM, Hoekstra OS, Oyen WJG, Van Eck-Smit BLF,Hoefnagel CA, Jager PL, Lips P, Arndt JW, Krenning EP.Behandeling van het gedifferentieerde schildkliercarcinoom metjodium-131: op weg naar een landelijke consensus. Tijdschr NuclGeneeskd 1999; 21: 139-47.DIAGNOSTIC ONCOLOGYHoefnagel CA. MIBG therapie. In: Nascholingscursus medischnucleair werkers therapie, SOANG. Rotterdam, 1999: 8-14.Hoefnagel CA. Radionuclide therapy. In: Wiarda KS, redactie.Leerboek nucleaire geneeskunde SOANG. Maarssen: Elsevier/DeTijdstroom, 1999; pp 297-12.Jansen EPM, Valdés Olmos RA, Dewit LGH, Muller SH,Hamburger HL, Hoefnagel CA, Bartelink H. Residual pituitary adenomavisualized by functional 99mTc-HMPAO SPECT. TijdschrNucl Geneeskd 1999; 21: 76-9.Kroon BBR, Jansen L, Valdés Olmos RA, Peterse JL, HoefnagelCA, Nieweg OE. Sentinel node biopsie bij het melanoom: pro? In:Syllabus thema-avond de ‘Sentinel node biopsy’ bij hetmelanoom. Leiden: Werkgroep Huidtumoren IKW: 1999.Taal BG, Hoefnagel CA, De Jong D, Rutgers M, Boot H.Carcinoïde tumoren: recente ontwikkelingen binnen Nederland indiagnostiek en palliatieve behandeling. Ned Tijdschr Geneeskd1999; 143: 445-51.Taal BG, Van Loon H, Kahn N, De Jong D, Vasen HFA, Van ’t VeerLJ. De rol van genetische factoren bij het ontstaan van maagcarcinoom.Ned Tijdschr Geneeskd 1999; 143: 342-6.Valdés Olmos RA, Van Dongen A, Hoefnagel CA. Oncologie. In:Wiarda KS, redactie. Leerboek nucleaire geneeskunde SOANG.Maarssen: Elsevier/De Tijdstroom: 1999; pp 265-96.
156Biometrics DepartmentDivision head Otilia DalesioHeadOB Dalesio MScAcademic staffM Kooi MSc, H Van Tinteren MScPermanent technical staffA Hiemstra, K Hogema, I Jansen, J Lieverst,I Mandjes BSc, C Modder, M Mahn-Schaefers,A Reinders-Som, L Valkenet MD, T Van der Velde,W Van Waardenberg, A Wals, E WillemseOther technical staffD Baars, R Bakx, A Boucher, F De Lange, W Deurloo,F De Vries, L Frenken, R Hakvoort, J Maaskant, A Mathy,A Ndoye, D Roberts, R Tougha, E Van der Donk,E Van Soest, E Weeda, L ZiblatGuestJ Oosting PhDSecretaryL Rentenaar (until September)Research funded positions (full time equivalents)Scientific permanent: 1.5Scientific project: 1.0Technical permanent: 8.9Technical project: 8.8IntroductionThe Biometrics Department provides statisticalservices, data management and central information onclinical trials to the institute through different functionalunits: the statistical and data handling group, the tumorregister, the trial bureau and the trial secretariat. Thesupportive tasks include different degrees of collaborationin projects and clinical trials initiated within the clinic andthe research sections. In addition, the department hasdeveloped collaborations with external groups andfunctions as the data center for several studies ofdifferent national and international groups.There are two areas of special interest in which thedepartment has initiated research and has developedprojects during recent years: 1) the use of telematics inproviding information services; 2) meta-analyses oftreatment in cancer.At the end of 1999, the HORIZON project (EC DG XIII)was successfully completed, EC support for the activitiesin the area of telematics was increased and thedepartment was involved in several existing projects. Thedevelopment of the Extranet of Centres of Excellence inOncology (Onconnet) continued. New services wereadded to the TRION Intranet server offering informationon clinical trials. The different networks in the hospitalwere linked and protected by a router and a series ofProxy servers to allow access to a unique TRION serverfrom the different places in the hospital.A new system (year 2000 compatible) for online patientrandomization and registration in clinical trials (ALEA) wasdeveloped to replace PARADIGM, and will be in use inthe year 2000, not only at the Biometrics Department butalso at the Medical Research Council in UK and InstituteGustave Roussy in France.The 2nd cycle of meta-analysis in prostate cancer ofrandomized trials comparing standard hormonaltreatment with and without the addition of an antiandrogenwas finalized.
Study of chemotherapy with vitamin Aand/or N-acetylcysteine (EUROSCAN)H Van Tinteren, OB Dalesio, N Van Zandwijk 1The EUROSCAN study is a chemoprevention study,set up in 1987 as a joint venture of the EORTC Headand Neck Group and the EORTC Lung Group. The mainobjective is to investigate the effectiveness of vitamin A,N-acetylcysteine or the combination of both in preventingor delaying recurrences and second primary cancers inpatients treated curatively for oral, laryngeal or lungcancer. Almost 2600 patients have been included in the4 arms of the study and more than 1500 events wererecorded (recurrences, second tumors and deaths). TheDepartment was responsible for the statistical analysis.No benefit was observed either by the use of NAC orvitamin A in the incidence of 2nd tumors, recurrence rateor duration of survival. During 1999 a report of the resultswas submitted for publication.Notes1 Division X.Funding: DGV-EC Europe against Cancer program.Collaboration with NDDOStudy of adjuvant 5FU plus Levamisole incolorectal cancer (NACCP)B Taal, F Zoetmulder, OB Dalesio, H van TinterenAlthough the American Consensus meeting adopted5FU plus Levamisole as standard therapy in stage IIIcolon cancer shortly after the publication of Moertel et al.(N Engl J Med 1990; 322:352-8), many clinicians in theNetherlands remained unconvinced about the value ofadjuvant therapy in colorectal cancer. A cooperativegroup (the Netherlands Adjuvant Colorectal CancerProject) was therefore created to investigate this. Thegroup includes 52 hospitals in the Netherlands that treatapproximately 60% of colorectal cancer cases in thecountry. The Biometrics department provided statisticalsupport, central randomization and data handling andcoordinated data management. From 1990 to 1996,1,029 patients were randomized. Patients are followedfor recurrence and survival. The overall survival showed asignificant difference in favor of the adjuvant treatmentwith 68% 5-year survival compared to 58% in the controlarm. This benefit can also be described as a 25% (SD9%) reduction in the odds of dying (logrank p=0.007)(Figure 1).157BIOMETRICSD Baars, F De Vries, M Kooi, A Ndoye, H Van Tinteren,L Ziblat, OB DalesioFor the last 11 years the department has collaboratedwith the New Drug Development Office (NDDO) in thephase II studies of the Early Clinical Studies Group(ECSG) and the Biological Therapeutics DevelopmentStudy Group (BTDSG) of the EORTC. Patients are registeredcentrally, through on-line randomization by modemconnection or through telephone calls. Case record formsfrom more than 50 participating centers worldwide aresent to the department to be processed. Data entry,checking and querying takes place according to theEuropean Good Clinical Practice guidelines. Reports ofongoing studies are produced for the ECSG investigatorsand the sponsoring companies, together with statisticalanalysis for presentations and publications.In 1999 four phase II studies were finalized: 1)GI147211; 2) Carzelesin a DNA-sequence-specificalkynating agent; 3) UFT+Leucovorin in patients withgastric cancer; 4) TA-HPV in patients with cervicalcancer. Seven other studies continued with patient registrationand data collection. These include studies withDocetaxel, Paclitaxel, LU103793, Mage-3, UFT/5-FU+Leucovorin, ISIS 3521 and ISIS 5132. The totalnumber of patients in all studies is 724. From January1999 until November 1999, 69 new patients wereentered in the open studies.Figure 1Mortality results of FU and levamisol as adjuvant treatment vs noadjuvant treatment in colo-rectal cancer.Telematics projectsA Boucher, A Mathy, E Van der Donk, OB DalesioThe Biometrics Department has been involved intelematics projects for the last 11 years and has obtainedsupport of the EC to develop them. In 1999, thedepartment continued to play a key role in the AC:TION
158BIOMETRICScluster of oncology related EC funded projects in the 4thframework program of DGXIII – Telematics for Healthcare.The common denominator of this cluster of projectsemerged as what is referred to as Onconnect.net, anExtranet of European reference centers for cancer. Thecluster develops telematics services in the areas ofcancer treatment, research and education.The Global Horizon project, in which the BiometricsDepartment is a major partner, supports a G7 initiative todevelop global healthcare networks. Key persons inhealthcare policy in G7 countries and observer countriesare involved in the development of a political, organizationaland technical strategy for the implementation ofglobal healthcare networks for oncology, cardiology andother medical disciplines. The Netherlands has beenidentified as an observer country in these developments.As such, the institute is represented at the meetings ofthis group.In 1999, the Biometrics Department received additionalfunding to develop the Onconnect.net concept. Thisresulted in a concerted implementation plan addressingdifferent aspects of the implementation of a healthcareExtranet, such as legal issues (with Coopers andLybrand), ISO 9000 certification (with IKO) and thetechnological options (with Origin). In addition, replicationtools were developed in Java, a common helpdesk toolwas developed and taken into use for both theonconnect and Intranet services provided by Biometricsin the institute.Extranets are a fast evolving area in the Informationand Communication Technology (ICT) sector. In anextranet, a private network of collaborating partners iscreated based on the same technology as the Internet(TCP/IP). The only difference is the infrastructure: theExtranet uses direct links between participating institutesrather than through Internet Service Providers. Theadvantage of such a private infrastructure is that theperformance is deterministic: the bandwidth is allocatedon demand, which enables the use of services such asvideo, audio and conferencing tools. In addition, being aprivate infrastructure makes an Extranet less vulnerableto security breaches.A spin-off of these activities was the initiation of thedevelopment of a national component of theOnconnect.net. This national network (nl.onconnect.net)currently provides access to TRION (Trial InformationOnline), ALEA (Online patient randomization and registrationin clinical trials) and some international contentpackages (EuroTransMed realvideo and realaudio), as wellas generic IP communication tools such as Netmeeting.NoteFunding: DGXIII-EC telematics program.TRION (Trials On line)J Lieverts, L Rentenaar, D Roberts, R Tougha,E Van der Donk, OB DalesioTRION is a computer system developed by theBiometrics Department to support clinical research in theinstitute. In 1999 TRION was linked with the livedatabase as it is being used in the Trial Bureau. In effect,any data entered modified or deleted by BiometricsDepartment staff is immediately effective on TRION.Further, it was extended with a number of extra facilitiesand web sites. One of the new services on TRION is aweb based helpdesk. This site allows any TRION user todrop a support question or report an incident. Theincidents or questions are automatically forwarded to theappropriate support staff.The previous situation of TRION being offered throughfour different servers for WA, RT, DZA and the researchnet was changed into a single TRION server serving allnetworks. In addition, TRION is made available toexternal users through a login mechanism and anencryption of data transmitted from TRION over theInternet. This service will be offered to a restrictednumber of users in selected hospitals.Maximum androgen blockade inadvanced prostate cancer: an overview ofthe randomized trialsW Deurloo, H Van Tinteren, OB DalesioSince 1989 the Biometrics Department coordinates, incollaboration with the CTSU of the University of Oxford,an overview of all randomized trials of the treatment ofprostate cancer. The Prostate Cancer Trialists’Collaborative Group was created to make data availablefor this overview.In advanced prostate cancer androgen suppression(AS) by surgery or drugs controls testicular hormonesecretion, and the further addition of an anti-androgensuch as nilutamide, flutamide or cyproterone acetate(CPA) produces maximal androgen blockade (MAB).Several randomized trials have been carried out bydifferent groups world-wide to compare AS alone versusMAB and a collaborative meta-analysis of these trials,involving central re-analysis of the data on each of 8,275men (98% of those ever randomized) was organized.Follow-up was typically for about 5 years, and 71%had died. Five-year survival was 25.4% with MAB versus23.6% with AS alone, a non-significant gain of 1.8% SD1.3 (logrank 2p=0.11). There was no significant heterogeneityof benefit with respect to age or stage. The resultsfor CPA, which accounted for only one fifth of theevidence, appeared slightly unfavorable (five-year survival15.4% MAB versus 18.1% AS alone, difference –2.8%SD 2.4, logrank 2p=0.04 adverse), while those for
159BIOMETRICSFigure 2Mortality results of MAB vs standard hormonal treatment, bytype of anti-androgen in prostate cancernilutamide and flutamide appeared slightly favourable(five-year survival 27.6% MAB versus 24.7% AS alone,difference 2.9% SD 1.3, logrank 2p=0.005). Nonprostate-cancerdeaths (although not significantly affectedby treatment) accounted for some of the apparentlyadverse effects of CPA. Figure 2 presents overall survivalcurves of MAB compared to standard androgensuppression.NoteFunding: DG XII-EC BIOMED II program.
160Research FacilitiesThe research divisions within the <strong>NKI</strong>/<strong>AvL</strong> aresupported by a number of indispensable research servicefacilities, each comprising a group of experts whoprovide information, instruction and service assistance.Besides the facilities described below, the institute has acentral cryogenic storage facility, a glassware kitchen, a(electro-)technical workshop and an audiovisualdepartment.BiometricsOB Dalesio MSc, D Baars, R Bakx, A Boucher,F De Lange, W Deurloo, F De Vries, L Frenken,A Hiemstra, K Hogema, I Jansen, M Kooi MSc,J Lieverst, J Maaskant, I Mandjes BSc, A Mathy,C Modder, M Mahn-Schaefers, A Ndoye,A Reinders-Som, L Rentenaar (until September),D Roberts, R Tougha, L Valkenet MD, T Van der Velde,E Van der Donk, H Van Tinteren MSc,W Van Waardenberg, A Wals, E Willemse, E Weeda,L ZiblatIn addition to its own research activities (describedseparately), the Biometrics Department provides theinfrastructure for clinical and fundamental researchconcerning biostatistical support, centralized patient datacollection and documentation, data processing andcoordinated administration and monitoring of clinicaltrials. The statisticians collaborate in several research andclinical projects both within the institute and for nationaland international multicenter studies.The department maintains a Tumor Register database,with information on patients with benign tumors, premalignantand malignant tumors seen in the institutesince 1977. The database contains almost 97,000 registrations,including second tumors. In excess of 30,000patients are currently being followed up in the register.This database is a valuable resource for research.Support of the medical divisions for central administration,patient registration and data collection of clinicaltrials is provided through the Trial Office. Between July1998 and June 1999, 689 patients were entered in oneof the 92 trials open to accrual. One third of them wereincluded in studies supported by the Dutch CancerSociety or by the Health Insurance, a quarter in studiessponsored by industry and the rest in studies sponsoredby the institute. Registration and randomization servicesfor 9 national and 9 international studies were provided.In 1999 a quality assurance officer was appointed toreview, develop and standardize medical and administrativeprocedures related to clinical trials. During this yearthe department reviewed and documented all standardoperating procedures (SOPs) according to ISO guidelinesand a computer system was developed to maintain theSOPs updated and accessible.A course on Medical Statistics for researchers andphysicians that was piloted the previous year wasorganized twice in 1999 due to the great interestgenerated.BiophysicsGJF Blommestijn PhD, HHJ Brocks PhD,LCJM Oomen PhD, HJ Stoffers MSc, SA Turpijn-la Pas,IV Van de Pavert, GJ Van der Stroom,RO Van DrimmelenFigure 1Biophysics department; computers and network.
161Computers and NetworkThe <strong>NKI</strong>/<strong>AvL</strong> research network facility provides generalcomputer and network support for all research divisionsas well as specific ‘site wide’ services (such as e-mailfacilities) for hospital personnel. Tasks include: themanagement of routers, ethernet switches, file servers,job-and-database servers, the configuration of networksoftware on PCs and Apple Macintosh computers of endusers and, if necessary, the development and maintenanceof custom server and/or client side software.Special care is given to the integration of central dataacquisition systems, e.g. cell sorters, phosphor imagers,and confocal laser scanning microscopes, into thenetwork infrastructure. By this service heterogeneouslocal data and services, internet services and applicationprograms are integrated into a unified ‘scientific office’environment and put on the researcher’s desktop.RESEARCH FACILITIESDigital MicroscopyThe biophysics department also provides a digitalimage acquisition and analysis facility. There are twoconfocal laser scanning microscopes (one with continuouslyadjustable wavelength selection bands in all fouremission channels) and a microscope setup with acooled CCD-camera. A second microscope setup with acooled CCD-camera has been bought to meet the increasingneed for these systems.Electron MicroscopyJ Calafat PhD, JWRM JanssenThe facility consists of a Philips CM10 transmissionelectron microscope and Leica (cryo)-ultramicrotomes.Next year a second electron microscope will beFigure 2Biophysics department; digital microscopy.purchased. In addition to its own research activities(described in Division I), the facility assists researchers intheir ultrastructural morphological analysis of macromolecules,viruses, cells and tissues. Immunoelectron microscopyof ultrathin cryosections reveals a great wealth ofstructural details in the 2 to 100 nm range providinginformation that can not be obtained in another way. Thistechnique is used for the following studies: the exactlocalization of antigens/molecules in the cell organelles,co-localization of two different antigens using colloidalgold of different sizes, trafficking of molecules in the cell,and cell-cell and cell-matrix interactions.Flow cytometryE Noteboom, AS PfauthFigure 3Electron Microscopy.The FACS-facility harbors two sorters (one has beenupgraded with a HeNe laser), three analyzers and threecomputers systems for data analysis. The two operatorsmaintain the equipment, instruct users and assist withexperiments. Every user is trained so that he or she canoperate the analyzers independently.A wide variety of experiments are being performed,because every research group in the institute makes useof this facility. Examples include measurements ofapoptosis, cell cycle progression and cell surfacemarkers. Cell sorting experiments include those for transfectedcells (co-transfection with surface marker gene),progenitor cells, green fluorescent protein (GFP) andLacZ positive cells, and for subcloning cells. Sorting oflive as well as fixed cells is routinely carried out, includingfour way sorts, double laser experiments and sorting into96-well plates.
162RESEARCH FACILITIESLaboratory Animal DepartmentRGM Ten Berg DVM PhD, K Ankema, NH Bosnie,NJ Bovenkerk, MT Bulale, C Friederich, HMG Grimminck,D Grund, PJ Handgraaf, TL Hetem-Maidment,M Hoffmann, JJ Janssen, WST Kenbeek, J Kleinsma,FC Krekko, M Lageweg-Beumkes, AJL Lagro, AJ Linden,FT Nicolaas, AJ Schrauwers, C Spaans, HP Starrevelt,EH Tanger, MAM Timpico, AJM Tolkamp,R Van den Berg, FH Van der Ahe, D Van der Pijl,HCA Van Hattum, N Van Roosmaelen, WK Van ’t Wout,W Wolff, A ZwerverA large part of the oncology research in the institute iscarried out using rodent models (mice and rats). Thelaboratory animal facility is located in a separate wing inorder to maintain a good microbiological barrier. Thedepartment provides the infrastructure for animal experiments:production and maintenance of mice and rats,renders biotechnical assistance, sanitation of strains, andproduction of gnotobiotic animals. The facility possessesa large isolator unit for gnotobiology, sanitation andquarantine, plus a separate laboratory for microbiology.Cryopreservation of murine embryos are routinely carriedout using a vitrification method.Laboratory Animal Pathology andHistologyMA Van der Valk MSc, JC Bulthuis, CCJ De Goeij,DA Hoogervorst, EW Van MuylwijkAs cancer and tumorgenesis can be defined asprogressive changes in the relational and biologicalnature of tissues, both clinical and animal (histo-)pathology are indispensable in cancer research. With theincreasing production of transgenic and ‘knock-out’ mice,animal pathology is an important supportive disciplinewithin the institute.The animal pathology and histology department has awell-trained staff (including an animal pathologist) andmodern equipment. The department provides researcherswith basic histological techniques as well as full histopathologycarried out by the pathologist. Advice andinstruction are also given to researchers on histotechnicaland pathological aspects of their work.In the scope of animal health control, the pathologist isinvolved in the Sick Animal Program. Apart from serologyand bacteriology, routine screening on gastrointestinalendoparasites is performed histologically; this adds significantlyto the reliability of conventional techniques.LibraryS Bakker MSc, IS Benne, L Broertjes, IN Goede,GJ KroeskampThe library serves the research, clinical, nursing andparamedical departments of the institute and alsofunctions as the Central Cancer Library in theNetherlands. Occasionally patients are referred to thelibrary by the staff of the patient information center. Theaim of the library is to maintain an up-to-date collectionof both printed and electronic publications covering allaspects of clinical and experimental oncology and relatedresearch areas, and to play an active role as an intermediaryin the process of information provision anddocument delivery. The library provides access to themajor electronic literature databases and, increasingly, tothe full-text electronic version of scientific journals. Therole of the library as an information intermediary isextended with the responsibility to maintain the <strong>NKI</strong>/<strong>AvL</strong>Internet service consisting of a web-site with informationabout and from the institute and of an Intranet servicewith links to bibliographic and literature related databasesof the library and access to in-house and externallyavailable electronic resources and services. The libraryoffers current awareness services both in electronic andprinted format. On request literature searches, bibliographicinstruction, help and advise about literaturedatabase management (systems) are offered. The libraryis responsible for the scientometric analyses (based onimpact factors and citations) and the list of publicationspublished in the annual scientific report.DNA MicroarraysR Bernards PhD, RM Kerkhoven PhDIn January of 1999 a DNA microarray facility wasstarted at the Institute. This facility was made possible bya grant from the ‘Center for Biomedical Genetics’. Thefacility collaborates closely with a similar facility at LeidenUniversity to implement the use of DNA microarraytechnology in basic and translational research programs.In its first year of operation, a set of 40,000 sequenceverifiedhuman cDNAs was obtained and methods havebeen optimized to PCR amplify cDNA inserts from libraryplasmids on a large scale. Equipment to produce microarrays(spotter) and to read arrays (scanner) have beeninstalled and the first microarrays of some 2,000 geneshave been produced. At present, technology to generateprobes from small amounts of clinical material and tohybridize arrays with fluorescent probes are beingoptimized. Arrays with larger numbers of genes willbecome available in the next year.
Peptide synthesisLN Vernie MSc (until May), HAM HilkmannThis year 142 peptides were synthesized, mainly formembers of our institute but also for other research institutionsand universities collaborating within the frameworkof the Oncology Graduate School Amsterdam. As part ofroutine quality control each peptide is checked by HPLC.For elucidating the cause of a less successful synthesisand for a further control of the peptides, mass spectrometryis performed, in collaboration with the FreeUniversity of Amsterdam and the department ofPharmacy and Pharmacology of the Slotervaartziekenhuisof Amsterdam. A meeting for peptide chemists in theNetherlands has been organized at the institute to discusrecent developments in peptide synthesis.Most of the peptides synthesized are used for raisingantisera or for biological studies in tissue culture.However, a shift is noted towards the use of peptides inin vitro binding experiments. Peptides used for theproduction of antibodies are now routinely synthesizedonto a branching lysine core. The results of the multipleantigenic peptides are satisfactory.There is always a need for peptides with specialfeatures. Examples include the synthesis of peptideswhich were biotinylated, acetylated or contained aminoacids with defined side chains.Peptides are also being synthesized for clinical use; forthis purpose the synthesizer has been adapted toincrease the yield. In addition to normal routine controls,these peptides are extensively tested in the Departmentof Pharmacy and Pharmacology of the Slotervaartziekenhuisof Amsterdam.Small amounts of different peptides are synthesized onthe recently installed Syro multi peptide synthesizer (incollaboration with Division IV).the staff of the department takes an active part in variousresearch activities, including synthesis of [ 125 I]MIBG withlow specific activity (Division VIII) and synthesis of radiolabeledpeptides and proteins.Sequence FacilityLJ Van ’t Veer PhD, FBL Hogervorst PhD, R PruntelThe rapid increase in the number of DNA sequenceand fragment length analyses and the complexequipment required led to the establishment of asequence facility in March of this year. The facility isequipped with a ABI 377XL slab-gel automatedsequencer which can handle 64 samples simultaneously.The communication between the users, already morethan 85, and the facility is through the computer network.In the start-up phase of the facility, users perform thesequence reactions themselves. The chemicals can bepurchased from the facility. In addition, specific runs areperformed on request. On average, 1,500 samples areanalyzed by the sequence facility each month. Another1,500 samples concern fragment length analysis.In the near future an automated 96-capillary sequencerwill be purchased. This machine will enable us to carryout large sequence projects without delay. Furthermore,the facility will be moved to a dedicated laboratory andthe service will be extended (including sequence reactionand sample preparation).Transgenic Mouse ServicePJA Krimpenfort PhD, R Bobeldijk (until February),CJH Van Veen-Buurman, WK Van ‘t Wout (until April)163RESEARCH FACILITIESRadionuclide LaboratoryPAJ Jonkergouw MSc, TE Lamers, ALM LutsIn addition to departmental laboratories licensed forradioactive work, which are present on each floor of theresearch building, there is a central radiochemistry facility(class B) available for specific and general experimentaluse. The staff of the Radionuclide Laboratory offer helpand advice on all aspects of radioactive work. Thedepartment is equipped with up to date gamma andscintillation counters, gamma analyzers and HPLCapparatus for on line radiodetection. There are alsoseparate facilities for animal experiments with radioactivity.The department provides regular courses onRadiation Protection, level 5B, for all new personnel(including students and guests) whose work entails theuse of radioactive material.In addition to general aspects of education and safety,Figure 4Transgenic mouse service.
164RESEARCH FACILITIESIn collaboration with the breeding unit of the laboratoryanimal department, the transgenic mouse serviceroutinely provides researchers with genetically modifiedmouse strains. Two distinct techniques are being used:DNA injection into the pronuclei of zygotes and (modified)ES cell transfer into the blastocyst cavity. The unit alsoassists researchers who want to generate modified micethemselves or who want to perform specific embryologicalexperiments.Pronuclear injections were performed using over 25transgenic constructs, generated by investigators fromalmost all research divisions, resulting in a total of 120independent transgenic mouse strains. The standardrecipient zygotes are from the inbred FVB/N backgroundbut, upon request, zygotes from a different geneticbackground can be used (B10, B6, SJL) for specific (e.g.immunological) experiments.Genetically modified ES cell clones were generated byresearchers and injected into blastocysts giving rise tochimeras which have been used either in experimentsdirectly or for the establishment of mutant mouse strains.For chimeric studies a total of 12 clones were injectedand for the generation of mutant mouse strains 25clones. Currently, procedures are being developed to useES cells from genetic backgrounds other than thestandard 129/Ola (e.g. B6, Balb/C).Staff of other general research facilities:Cryogenic storage: MM Dijkstra, REJ KambeyGlassware kitchen: TAM Holman-van Doorn,M Aboutalib, EV Holman, REJ Kambey, HL KempffTechnical workshop: JA Marijnissen, WJ Kraan, CWJ SierAudiovisual department: JM Lomecky, SL Bakker,SM Grentje, ARM Jagt, C Koedijk, ER Tragter, CM WalleFigure 5Cryogenic storage.
Cancer Hospital165In 1999, the hospital of the Netherlands Cancer Institutecontinued to grow, both in terms of patient-care andclinical research output. The number of new patients seenat the hospital rose by 7% to well over 5,100. A total of41 clinical research protocols were reviewed by the institutionalreview committees, and 22 were activated.In order to deal with the ever increasing demand forpatient care, every attempt was made to preserve theaccessibility of the outpatient clinic. While it provedpossible to avoid delays before new patients could beseen and examined, the required number of surgicalprocedures exceeded the capacity of the hospital. Despite16% more surgical procedures than in 1998, the waitinglists for operations grew to sometimes unacceptablelevels. This led to increased referral of patients tocommunity hospitals for operations that can be doneeffectively outside a cancer center and it occasionallyforced surgeons of our institute to perform cancer surgeryin general hospitals. Other measures to accommodate theincreased patient flow included a further reduction of thein-hospital time for surgery, transfer of medical treatmentsto the day care facility and back-referral of medicalpatients to their previous hospitals. In spite of theseefforts, however, there are clearly limits to the capacity ofthe hospital and hard choices to regulate patient flow inthe next millennium may become unavoidable.On a more cheerful note, the high quality of the clinicalresearch of the institute is increasingly recognized bothnationally and internationally. In 1999, two very favorablesite visits of clinical research divisions were conducted byinternational site visit committees. The first was that of theDivision of Psychosocial Oncology and Epidemiology (sitevisitors: L Bernstein, P Ganz and D Patrick) and thesecond was that of the Department of Pathology (sitevisitors: D Sidransky, P Selby and M Stratton). Periodicsite visits to assess the quality and quantity of theresearch in the institute have been standard policy formany years. BBR Kroon, who chairs the SurgicalOncology Cluster of the institute was appointed Professorof Surgical Oncology at the University of Amsterdam. JHMSchellens, the medical oncologist in charge of the ClinicalPharmacology program, was appointed part-timeProfessor of Pharmacy at the University of Utrecht. Bothappointments strengthen the ties that the institute has withstrong university-based research programs.Many research themes were continued in 1999 anda range of novel topics, or variations of existing ones,were added. A very important recent development is therecognition that concurrent chemotherapy and radiationtherapy (‘chemo-radiotherapy’) leads to improved localcontrol in an astonishingly large variety of epithelial tumors,where sequential application of the two modalities offersno advantage at all. Investigators of the NetherlandsCancer Institute have pioneered this approach in the lastdecades, but the proof that chemo-radiotherapy alsoleads to improved overall survival is more recent andcomes from many large randomized studies on both sidesof the Atlantic. Clearly, a multidisciplinary institute such asthe Netherlands Cancer Institute is ideally suited to bringthis combination to new heights. A special clinical unit hasbeen established for this purpose as part of one of thetwo Medical Oncology wards.Another theme that fits exceptionally well in the specificinfrastructure of the institute is that of ‘translational’research. The combination of a fundamental researchlaboratory and a cancer hospital with a strongcommitment to clinical research is precisely what isneeded to let cancer patients benefit from the recentadvances in biology. To further increase the interactionsbetween these complementary halves, a fellowship foryoung specialists in internal medicine has beenestablished that consists of a 2-year fundamental researchperiod under the supervision of a fundamental scientist inthe institute, followed by 2 years of formal training inMedical Oncology. These ‘hybrid fellows’ are than able tocontinue some of their presence in the laboratory duringtheir clinical program and are in an ideal position todetermine possible areas of collaboration and cross-fertilization.The first of this new breed is JBAG Haanen, whoentered his clinical period in 1999 after working for twoyears in fundamental immunology. Similar fellowships inwhich fundamental training is offered outside the instituteare being offered by the Dutch Cancer Society and theseare also highly useful. M Verheij is an example of suchfellows. He interrupted his training in radiation oncology forfundamental research in signal transduction and apoptosisin the Memorial Sloan Kettering Cancer Center, New York.Verheij was appointed staff radiation oncologist aftercompleting his training in 1999.The clinical research infrastructure of the Hospital
166CANCER HOSPITALrequires continuous work and development. Not only isthere a yearly increase in the number of patients includedin early clinical studies, but the formal quality requirementsfor clinical studies are expanding rapidly, due to bothnational legislation and European directives. To accommodatethe need of the Clinical Pharmacology program toperform its work under Good Clinical Practice (GCP)conditions, the first Quality Assurance (QA) Officer wasappointed in 1999. Meanwhile, the Pharmacy completedits efforts to establish Good Manufacturing Practice (GMP)and Good Laboratory Practice (GLP) conditions and itreceived the official certification for both from the Ministryof Health, Welfare and Sports in 1999. These accomplishmentsmay be seen as appropriate recognition for manyyears of hard work.As in previous years, breast cancer was the tumor thatmost multi-disciplinary work focused on in the hospital. InSurgical Oncology, the application of the sentinel nodeconcept was carried further in 1999 and this techniquehas now become the standard of care for a subgroup ofbreast cancer patients. Critical contributions to the optimizationof the technique and to the education of surgeonsfrom other hospitals were made by surgeons, nuclearmedicine specialists and other specialists from theinstitute. The Dutch national study of high-dose chemotherapyin the adjuvant treatment of breast cancer, whichis led by the <strong>NKI</strong>/<strong>AvL</strong> in collaboration with workers fromGroningen University Hospital, was closed in the summerof 1999 after having randomized 885 patients. This is thelargest study of this kind in the world. It is likely tobecome the pivotal study answering the question whetheror not high-dose therapy is beneficial in this setting.Although a first meaningful analysis of the results will haveto wait until 2002, it is already clear that the transplantrelatedmortality in this study is below 1%, which is quiteacceptable when compared with the American study(7.4%). In the pathology laboratory, important progress hasbeen made with the establishment of a ‘golden series’ ofbreast cancer specimens. This series consists of snapfrozentumor tissue that is completely characterized pathologicallyand clinically and of which RNA is available foranalysis. The use of this golden series for a comprehensiveanalysis employing DNA micro-array technology isunder consideration. Current techniques allow the estimateof expression levels of tens of thousands of genes simultaneously,and an almost bewildering amount of informationcould be obtained by a systematic evaluation ofthe samples in this series, which would allow immediatecorrelation with clinical and pathological details. These andmany other studies focusing on breast cancer aredescribed in more detail in the sections of the divisions VIIIthrough XIII.Other tumors traditionally at the center of activities in acancer institute are melanoma, soft tissue sarcoma andhead- and neck tumors. Continuing research includedisolated limb perfusions, immunotherapy and, for headand neck tumors, intraarterial infusions with high-dosecisplatin and concurrent radiation therapy. These topicshave been described in previous annual reports but theirsuccesses continue. The same is true for the hyperthermicintraperitoneal chemotherapy (HIPEC), which is an experimentaltreatment for colorectal malignancies with intraperitonealdissemination. HIPEC has recently been recognizedin the Netherlands as the standard of care for patientswith peritoneal pseudomyxoma.The cancer hospital of the Netherlands Cancer Instituteis in an excellent position to further expand its integratedclinical research program to the benefit of cancer patients.Recent years have brought an impressive increase inactivity which has transformed the program to an internationallyleading one in many areas. It is remarkable that allthis could be achieved despite the fact that the fundingsystem for the Cancer Hospital is similar to that for ageneral hospital, rather than that for a university hospital.Unlike university hospitals, the Netherlands CancerInstitute does not receive any support for treatmentdevelopment or for its top-reference function. In collaborationwith the regional health care insurance authorities,the Ministry of Health, Welfare and Sports has beenapproached to reverse this undesirable situation and tooffer equal treatment to the Netherlands Cancer Institute’shospital. It is hoped that the proposed, more appropriate,funding structure will be established in the year 2000.There is no doubt that if this is done, clinical cancerresearch will continue to gain momentum and that morepatients will benefit more from the unique opportunitiesthat a specialized cancer institute may offer.Tumor DocumentationThe Biometrics Department of the Netherlands CancerInstitute has a computerized tumor registration system. Atotal of 5,168 new tumors were seen in the hospitalbetween 1 July 1998 and 30 June 1999, including 4,260malignancies, 35 pre-malignancies and 873 non-malignancies.Of the malignancies, 1,000 were seen only for asecond opinion, while 3,260 malignancies were actuallytreated.Table 1Tumor groupTreatment 2 nd opinion onlyHead and neck tumors 223 33Digestive system tumors 419 211Lung and pleural tumors 472 157Tumors of bone and soft tissues 81 30Malignant melanoma of skin 191 46Carcinoma of skin 118 6Breast tumors 944 232Gynecological tumors 147 62Urological tumors 363 108Brain and nervous system tumors 22 13Endocrine tumors 23 4Unknown primary tumors 91 52Lymphatic and hematopoieticsystem diseases 166 46
Clinical Trialsin the Netherlands Cancer Institute167
168CLINICAL TRAILSTYPE OF TITLE STUDY COORDINATOR PHASE ACTIVATED NO PTS.CANCER IN <strong>AvL</strong> (in italics: (CLOSED) IN <strong>AvL</strong>STUDY international coordinator) per 1.9.1999ALL SITESEORTC 13962 Phase I study of anti-epidermal growth factor receptor/CD64 bispecific antibody GC de Gast I 03/1998 0(MDX447) with recombinant human granulocyte macrophage-colony stimulating factorin patients with advanced adult solid tumors overexpressing the epidermal growthfactor receptor.EORTC 16973 Phase I study to determine the safety of E7070 in patients with a solid tumor on a JHM Schellens I 03/1998 12simple 1-hour i.v. infusion repeated every 3 weeks.EORTC 16980 Pharmacokinetic study into the effect of food on the oral bioavailability of S1 in JHM Schellens I 06/1998 10patients with solid tumors.(12/1998)M96BEPT A dose finding study of escalating doses of paclitaxel (taxol) with fixed doses of JH Schornagel I 12/1996 14bleomycin, etoposide, cisplatin (BEP) in patients with advanced solid tumors.(12/1998)M96MTC Phase I clinical study of radio-immunotherapy of medullary thyroid cancer using the CA Hoefnagel I 04/1996 1two-step-targeting technique with bispecific immuno-conjugate and iodine-131-labelled bivalent hapten.M96WIS Determination of the analgesic efficacy of three buprenorphine dosages versus APE Vielvoye-Kerkmeer II 07/1997 0placebo in a transdermal therapeutic system (TTS) in patients with tumor pain.M97D21 (suspended) Phase I study with D21266.WW ten Bokkel Huinink I 01/1998 22M97TIF A prospective, open-label, non-comparative, two center phase I trial to evaluate the JHM Schellens I 04/1998 6dosage and safety of topotecan administered as daily x5, 30 minutes intravenousinfusions every 3 weeks in combination with Ifosfamide in patients with advancedmalignancies.M98PLY A phase I dose ranging study of LY335979 administered in combination with paclitaxelJHM Schellens I 11/1998 6in patients with metastatic or locally advancedcancer.M98VIA Open non-comparative multicenter study to evaluate the impact of viagra on W Meinhardt II 11/1998 0treatment satisfaction SND-NL-98-002.<strong>AvL</strong> N94IAS A phase I study of intraperitoneally administered suramin in patients with cancer WW ten Bokkel Huinink I 10/1994 11localized in the abdominal cavity.<strong>AvL</strong> N94TPC mTHPC-PDT and basal cell carcinoma: phase I/II study to determine optimal P Baas I/II 02/1995 5treatment parameters.<strong>AvL</strong> N95MIB A phase I study of meta-iodobenzylguanidine. BG Taal I 10/1995 27<strong>AvL</strong> N96IRO A phase I dose finding study of irinotecan continuous i.v. infusion over fourteen days WW ten Bokkel Huinink I 02/1996 37in adult patients with malignant solid tumors.(09/1998)<strong>AvL</strong> N97FIR (suspended) Phase I trial with R115777 JHM Schellens I 12/1998 26
169<strong>AvL</strong> N97OTAX Oral bioavailability of paclitaxel in combination with cyclosporin A. JHM Schellens I 04/1997 90(suspended)<strong>AvL</strong> N97PCI Peri-operative combined immunotherapy. GC de Gast/AJM Balm I/IIb 02/1998 9<strong>AvL</strong> N97PIF Inter- and intrapatient variation in disposition of ifosfamide and its metabolites in JHM Schellens I 12/1998 13various treatment schedules.<strong>AvL</strong> N97PPA Pharmacokinetic study of a comparison of blood sampling of paclitaxel in different JHM Schellens I 12/1998 4sampling sites.<strong>AvL</strong> N97SPI A phase I study to evaluate the safety and pharmacokinetics of SPI-77. JHM Schellens I 06/1997 15(07/1999)<strong>AvL</strong> N98CTO Carboplatin + topotecan. WW Ten Bokkel Huinink I 04/1999 4<strong>AvL</strong> N98OCP Dose finding phase I study of orally administered irinotecan. JHM Schellens I 11/1998 14<strong>AvL</strong> N98PGF Oral bioavailability of paclitaxel in combination with GF120918. JHM Schellens I 02/1999 6(09/1999)<strong>AvL</strong> N98PNU A phase I study to evaluate MAG-CPT (PNU 166148) given as a daily intravenous WW Ten Bokkel Huinink I 03/1999 3administration for three consecutive days every 4 weeks in patients with advancedsolid tumorsBRAIN / CNSEORTC 26952 Treatment of primary CNS lymphoma in immunocompetent patients aged over 60 yrs JW Baars/W Boogerd II 06/1998 1with chemotherapy alone.(04/1999)EORTC 26972 Second line chemotherapy with temozolomide in recurrent oligodendroglial tumors W Boogerd II 10/1998 2after PCV-chemotherapy.M96CAUDA Surgery versus Radiotherapy for the treatment of metastatic epidural spinal cord & W Boogerd III 05/1997 0cauda equina compression.M98TCU Compassionate treatment guidelines of Temozolomide (Temodal) in the treatment of W Boogerd II 10/1998 3patients with recurrent glioblastoma, gliosarcoma, ana- plastic astrocytoma, mixedoligoastrocytroma or previously treated metastatic melanomaBREAST CANCEREORTC 10873 Breast conserving therapy for Paget’s disease of the nipple. EJTh Rutgers II 07/1988 20(03/1999)EORTC 10901 Postoperative adjuvant chemotherapy followed by adjuvant tamoxifen versus nil for PF Bruning III 04/1991 123patients with operable breast cancer.(03/1999)EORTC 10951 Randomized phase II study in first line hormonal treatment for metastatic breast PF Bruning II 11/1996 0cancer with exemestane or tamoxifen in postmenopausal patients.EORTC 10961 Doxorubicin/taxol combination versus doxorubicin/ cyclosphamide as first line chemotherapyPF Bruning III 02/1997 24in metastatic breast cancer. A randomized study.(02/1999)CLINICAL TRAILS
170CLINICAL TRAILSTYPE OF TITLE STUDY COORDINATOR PHASE ACTIVATED NO PTS.CANCER IN <strong>AvL</strong> (in italics: (CLOSED) IN <strong>AvL</strong>STUDY international coordinator) per 1.9.1999EORTC 10967 Randomized double-blind trial in postmenopausal women with primary breast cancer EJT Rutgers III 10/1998 3who have received adjuvant tamoxifen for 2-3 years, comparing subsequent adjuvantexemestane treatment with further tamoxifen.EORTC 16962B Phase II trial with LU10393 in patients with breast cancer and melanoma. JHM Schellens II 07/1997 1(09/1998)EORTC 16982A Phase II and pharmacologic trial with doxorubicin plus cyclophosphamide (AC) in JHM Schellens II 03/1998 18patients with advanced breast cancer.EORTC 22922 Phase III trial randomized trial investigating the role of internal mammary and medial GMM Bartelink III 11/1997 32supraclavicular lymph node chain irradiation in stage I-II breast cancer.M90MCB Treatment of meningeal carcinomatosis in breast cancer: the relevance of intraventricularW Boogerd III 04/1991 10chemotherapy.(03/1999)M93SCB Adjuvant chemotherapy followed by intensification with hematopoietic stem cell S Rodenhuis III 03/1993 154support treatment for patients with stage II or III breast cancer involving ∆4 axillary(07/1999)lymph nodes.M94WBR a Cranial irradiation with CMF versus CMF alone for breast carcinoma patients with W Boogerd III 04/1995 3brain metastases and systematic metastases.M94WBR b Chemotherapy versus cranial irradiation for breast carcinoma patients with brain W Boogerd III 04/1995 0metastases as only site of active metastatic disease.M96ATLAS Reliable assessment of the efficacy and safety of prolonging the use of adjuvant EJTh Rutgers III 01/1997 14tamoxifen. A large simple randomized study.M96BREAS Multicenter study of early diagnoses of lymph node metastasis of breast cancer OE Nieweg II 07/1999 83based on lymphatic mapping and sentinel node biopsy.(01/1999)M96SnET A phase II multinational open label study of single dose tin ethyl etiopurpurin (SnET2) WW ten Bokkel Huinink II 12/1996 0photodynamic therapy (PDT) in patients with advanced breast cancer for themanagement of cutaneous metastatic breast carcinoma.<strong>AvL</strong> N96DOP Phase I/II dose-finding study of weekly combination of doxorubicin and paclitaxel in WW ten Bokkel Huinink IV 05/1996 9patients with advanced breast cancer.(09/1999)<strong>AvL</strong> N97ERF Intervention study on the clinical value of measuring the functional activity of the H Bartelink III 09/1997 19estrogen receptor with the hER-FASAY yeast assay in the treatment of breast cancerwith tamoxifen.<strong>AvL</strong> N97TCI Multiple courses of very high dose chemotherapy ‘tiny ctc’ and immunotherapy with GC de Gast/S Rodenhuis II 02/1998 14peripheral blood progenitor cell and activated T-cell support in patients with advanced(09/1999)breast cancer.
171<strong>AvL</strong> N98LPK Phase II trial investigating the accuracy of localization of the parasternal lymph nodes BR Pieters II 12/1998 11by lymphoscintigraphy and echography.<strong>AvL</strong> N98ODO Oral bioavailability of docetaxel in combination with cyclosporin A and activity of the JHM Schellens I/II 10/1998 14combination in advanced breast cancer.MELANOMAEORTC 16962M Phase II trial with LU10393 in patients with breast cancer and melanoma. JHM Schellens II 07/1997 11(03/1999)EORTC 18952 OE Nieweg III 08/1996 21Randomized phase III trial of adjuvant Interferon-alfa treatment after resection of thickprimary melanoma and/or regional lymph node metastases.EORTC 18972 Phase I/II study of immunication with a MAGE-3 protein based vaccine plus immunologicalGC de Gast I/II 02/1998 1adjuvant SB AS-2 in HLA Class I selected patients with MAGE-3 positivetumors.M94MSL A multicenter clinical study of wide excision plus intra operative lymphatic mapping OE Nieweg III 07/1995 145with selective lymphadenectomy versus wide excision of the primary melanoma in thetreatment of patients with melanoma.M94TNF Isolated perfusion with TNFa and melphalan for irresectable metastatic melanoma of BBR Kroon II 05/1994 29the limb.M96PER An open randomized, prospective trial to compare the efficacy and safety of TNFa BBR Kroon III 01/1997 17and melphalan with melphalan alone via isolated limb perfusion for metastatic(01/1999)melanoma of the limb (stage IIa, IIb, IIIa, and IIIab).M97CIM Dose escalation study of sequential chemo-immunotherapy in patients with metastatic GC de Gast II 03/1998 13melanoma.(11/1998)M98TCU Compassionate treatment guidelines of Temozolomide (Temodal) in the treatment of W Boogerd II 10/1998 3patients with recurrent glioblastoma, gliosarcoma, ana- plastic astrocytoma, mixedoligoastrocytroma or previously treated metastatic melanoma<strong>AvL</strong> N98IRM Combined immunotherapy in metastatic renal cell carcinoma and malignant melanoma. GC de Gast I/II 03/1998 33(02/1999)<strong>AvL</strong> N98TIM Temozolomide followed by combined immunotherapy in metastatic malignant melanoma. GC de Gast II 10/1998 33<strong>AvL</strong> N99HTC High dose temozolomide and cisplatin, followed by combined immunotherapy with GC de Gast I 07/1999 3GM-CSF, low dose IL-2 and IFNa in patients with metastatic melanoma unresponsiveto immunotherapy.LEUKAEMIA / MDSMHOVON18 Autologus bone marrow transplantation with a radiation-free preparatory regimen JW Baars II 09/1996 3(BU/CY) in adult patients with first remission after conventional induction and intensification(04/1999)chemotherapy.MHOVON20 A randomized phase III study comparing low dose versus high dose interferon alpha- JW Baars III 09/1996 22B both combined with adapted doses of hydroxy-urea in chronic myeloid leukemia.CLINICAL TRAILS
172CLINICAL TRAILSTYPE OF TITLE STUDY COORDINATOR PHASE ACTIVATED NO PTS.CANCER IN <strong>AvL</strong> (in italics: (CLOSED) IN <strong>AvL</strong>STUDY international coordinator) per 1.9.1999M99TPO Multicenter, randomized, controlled open label study of recombinant thrombopoietin JW Baars III 03/1999 0(rhTPO) given as primary prophylaxis of intermediate dose melphalan (IDM)-inducedthrombocytopenia in patients with multiple myeloma included in the HOVON MM24phase III trial.MHOVON29 Risk adapted treatment of acute myelocytic leukemia (AML). JW Baars III 09/1996 10M96MYE Myelo-ablative chemo-/radiotherapy and autologous stem cell transplantation JW Baars III 08/1996 9compared with chemotherapy only in patients with multiple myeloma.LYMPHOMAS - HODGKIN’S DISEASEEORTC 20884 Stage III-IV Hodgkin’s disease: role of iceberg RT in CR. BMP Aleman/JW Baars III 09/1989 23EORTC 20931 Protocol H8 for a prospective controlled trial in clinical stage I-II supradiaphragmatic JW Baars III 10/1993 22Hodgkin’s disease; evaluation of treatment efficacy and (long term) toxicity in 3(12/1998)different prognostic subgroups.EORTC 20982 Prospective controlled trial in clinical stages I-II supradiaphragma- tic Hodgkin’s JW Baars III 12/1998 2Disease. Evaluation of treatment efficacy, (long term) toxicity and quality of life in twodifferent prognostic groups. (Trial H9).LYMPHOMAS - NON-HODGKIN’SEORTC 20981 Chimeric anti-CD20 monoclonal antibody (Mabthera) in remission induction and H Pruijt III 01/1999 0maintenance treatment of relapsed follicular non-Hodgkin’s lymphoma: a phase IIIrandomized clinical trial.EORTC 20901 Intensive consolidation therapy with autologous bone marrow rescue after standard JW Baars III 04/1991 17chemotherapy for intermediate grade and high grade non-Hodgkin’s lymphoma.(11/1998)EORTC 26952 Treatment of primary CNS lymphoma in immunocompetent patients aged over 60 yrs JW Baars/W Boogerd II 07/1998 1with chemotherapy alone.(04/1999)M94NHL Effect of recombinant G-CSF on the results of chemotherapy (CHOP) in elderly JW Baars III 11/1994 4patients with intermediate-high grade non-Hodgkin’s lymphoma, a prospective phaseIII study.JW Baars/LGH Dewit I/II 08/1996 4M96FNLTreatment with BEAM and total nodal irradiation, both followed by PSCT support asconsolidation after remission induction for patients with high risk relapsed orrefractory low grade non-Hodgkin’s lymphoma.WR Gerritsen/JW Baars I/II 06/1997 15M97010Phase I/II clinical trial to evaluate the safety and efficacy of a combination ofrituximab (anti-CD20) and G-CSF (filgrastim) given weekly to patients with B-celllymphoma.JW Baars III 12/1997 0M97H35Marrow-ablative chemo-radiotherapy and autologous stem cell transplantationfollowed by IFN-alpha maintenance versus IFN-alpha maintenance alone after a
173chemo-induced remission in patients with stages III or IV follicular NHL. Aprospective, randomized, phase III clinical trial.H Pruijt III 04/1999 2M99H26 Intensified CHOP of 12-weeks duration plus G-CSF compared with standard CHOP JW Baars II 03/1999 2of 24-weeks duration for patients with intermediate prognosis nonhodgkin’slymphoma (HOVON26).M99H40Intensified CHOP followed by triple high-dose chemotherapy with autologous stemcell support as first line treatment for high-risk non-Hodgkin’s lymphoma.<strong>AvL</strong> N97HOR Low dose radiotherapy (2x2Gy) for low-grade non-Hodgkin lymphoma. RLM Haas II 11/1997 25<strong>AvL</strong> N97ILA Phase I/II study of combined subcutaneous low-dose IL-2 and intravenous bispecific GC de Gast I/II 09/1998 3antibodies directed against T cells and (malignant) B cells (aCD3xaCD19 BsAb, SHR-(07/1999)1) in patients with B cell non-Hodgkin lymphoma.GYNECOLOGICAL TUMORSEORTC 16982T Phase II trial with paclitaxel plus carboplatin (TC) in patients with advanced ovarian JHM Schellens II 04/1998 12cancer. Early clinical studies group.EORTC 55874 Adjuvant RT for uterine sarcomas BNFM van Bunningen III 02/1989 4M98BAY A phase III comparison of BAY 12-9566 versus placebo as consolidation after WW Ten Bokkel Huinink III 01/1999 0standard chemotherapy in patients with epithelial ovarian cancer(09/1999)<strong>AvL</strong> N97TRI Feasibility study of a three-step (I-III) intensified treatment strategy for patients with N van der Vange/ Pilot 03/1998 5(suspended) late recurrence of ovarian cancer.WW ten Bokkel Huinink<strong>AvL</strong> N99FMO Phase Ib protocol for the study of fluorescein for the detection of metastases of N van der Vange Pilot 06/1999 0ovarian tumor in the abdominal cavity.URO-GENITAL TUMORSEORTC 16967 Phase II trial of 96-hours continuous infusion of paclitaxel as a single agent in JHM Schellens II 02/1997 3patients with bladder cancer resistant/ refractory to MVAC/ MVEC/ CMV.(01/1999)EORTC 30924 Randomized phase II trial in advanced urothelial tract tumors of high dose intensity JH Schornagel II 11/1993 28M-VAC chemotherapy + GCSF versus classic M-VAC.(11/1998)M94SAL Phase II study of a salvage regimen incorporating repeated ablative chemotherapy S Rodenhuis II 09/1994 15with autologous peripheral stem cell reinfusion in relapsing germ cell cancer.M97RAD Phase III study for prostate cancer, randomizing between two radiation dose levels JV Lebesque III 04/1997 74(68 Gy versus 78 Gy) and utilizing three dimensional conformal radiotherapy.M99IRM Combined immunotherapy in metastatic renal cell carcinoma. A phase II study of the GC de Gast II 02/1999 9Working Group Immunotherpy of the Netherlands<strong>AvL</strong> N98IRM Combined Immunotherapy in metastatic renal cell carcinoma and malignant melanoma. GC de Gast I/II 03/1998 33(02/1999)CLINICAL TRAILS
174CLINICAL TRAILSTYPE OF TITLE STUDY COORDINATOR PHASE ACTIVATED NO PTS.CANCER IN <strong>AvL</strong> (in italics: (CLOSED) IN <strong>AvL</strong>STUDY international coordinator) per 1.9.1999LUNG TUMORSEORTC 08941 Randomized trial of surgery versus radiotherapy in patients with stage IIIa NSCLC N van Zandwijk II 03/1996 18after a response to induction chemotherapy.EORTC 08972 A randomized phase III study comparing induction chemotherapy to daily low dose JSA Belderbos III 01/1999 6cisplatin both combined with high dose radiotherapy using concomitant boosttechnique in patients with inoperable NSCLC stage I, II and low volume stage IIIEORTC 08976 Phase II study of temozolomide in malignant mesothelioma. P Baas II 04/1998 9(11/1998)M93MAS Minimal access surgery in oncology. EJTh Rutgers 05/1993 0M96JMN Phase I/II study with BMS 182751 (JM216) and simultaneous radiation in locally N van Zandwijk I/II 07/1997 7advanced unresectable non small cell lung cancer.(03/1999)M96EBB The value of endobronchial branchytherapy in NSCLC. BMP Aleman III 10/1996 3(05/1999)M98CCR Combined chemotherapy (carboplatin, paclitaxel, etoposide) and concurrent radiotherapyP Baas II 09/1998 5as first line treatment in small cell lung cancer limiteddisease.M98TDR A phase I/II dose escalation study using three dimensional conformal radiation J Belderbos/J Lebesque I/II 06/1998 17therapy in patients with inoperable non-small cell lung cancer.M99GEM Phase II study of gemcitabine and cisplatin in malignant pleural mesothelioma. P Baas II 04/1999 4<strong>AvL</strong> N94ILC Immunoscintigraphy with monoclonal antibodies in patients with small cell lung cancer. N van Zandwijk 05/1994 0(11/1998)<strong>AvL</strong> N97FOS Combined modality treatment of malignant mesothelioma. P Baas I/II 01/1998 10(01/1999)<strong>AvL</strong> N98CIG Phase I study of dose-intensive Cisplatin + Gemcitabine in NSCLC JHM Schellens I 09/1998 29<strong>AvL</strong> N98MDM Phase II study of high dose methotrexate and doxorubicine in malignant mesothelioma. P Baas II 05/1998 10SOFT TISSUE/ OSTEOSARCOMAEORTC 62931 Randomized trial of adjuvant chemotherapy with high-dose doxorubicin, ifosfamide F van Coevorden III 04/1994 12and GM-CSF in high grade soft tissue sarcoma.EORTC 62933 Metastasectomy and chemotherapy for lung metastases from soft tissue sarcoma. A F van Coevorden III 08/1996 3randomized phase III study.EORTC 62971 Randomized phase III trial of two investigational schedules of Ifosfamide versus S Rodenhuis III 02/1998 12standard dose Doxorubicin in patients with advanced or metastatic soft tissuesarcoma.
175EORTC 62982 Phase II study on ET-743 in advanced soft tissue sarcomas of the adult. S Rodenhuis II 06/1999 0M93ESB A randomized study for the treatment of Ewings Sarcoma of Bone. S Rodenhuis III 10/1993 2M94ILP Isolated perfusion of the limb for limb salvage with TNFa and melpalan for irresectableBBR Kroon II 05/1994 35soft tissuesarcoma.GASTRO INTESTINAL CANCEREORTC 16972C Phase II trial with S-1 in patients with colorectal cancer. JHM Schellens II 02/1998 11(suspended)EORTC 16972G Phase II trial with S-1 in patients with gastric cancer. JHM Schellens II 02/1998 6(suspended)EORTC 22921 Four arm phase III clinical trial for T3-T4 resectable rectal cancer comparing preoperativeBMP Aleman III 10/1995 0irradiation combined with fluorouracil and leucovorin with or without post-operative adjuvant chemotherapy.M96CIS Evaluation of the effect of combined treatment of radiotherapy and Cisplatin in B Aleman/B Taal I 05/1996 5patients with inoperable esophagus carcinoma.M96PAN Randomized phase III trial comparing the effects of panorex injection + 5-fluorouracil/ FAN Zoetmulder III 08/1996 10leucovorin versus panorex injection alone in patients with surgically resected stage III(03/1999)carcinoma of the colon.M96TME Total Mesorectal Excision (TME) with or without pre-operative radiotherapy in FAN Zoetmulder III 08/1996 12treatment of primary rectal cancer.M97CPT A randomized phase II multi centre trial of irinotecan hydrochloride trihydrate (CPT11) WW ten Bokkel Huinink II 03/1998 25using different schedules in patients with metastatic colorectal cancer.(04/1999)<strong>AvL</strong> N94DGT Dynamic graciloplasty technique functional reconstruction to achieve anal continence FAN Zoetmulder I 05/1994 0after abdominoperineal resection (APRE) for rectal cancer.<strong>AvL</strong> N96INF A dose finding study of combined treatment with a fixed dose of Interferon-alpha and BG Taal I 08/1996 27escalating doses of meta-iodobenzyl-guanidin (MIBG) inmetastatic carcinoid tumors.<strong>AvL</strong> N97HIPEC Randomized study comparing hyperthermic intra-peritoneal chemotherapy (HIPEC) FAN Zoetmulder III 01/1998 48with mitomycin C in addition to i.v. 5FU/Leucovorin alone in patients with peritonealcarcinomatosis of colorectal origin.<strong>AvL</strong> N98ECF A phase II feasibility study of ECF in locally advanced or metastatic gastric cancer B Taal II 08/1998 13and adenocarcinoma at the esophagogastric junction.<strong>AvL</strong> N98PDO PDT in esophagus carcinoma. H Boot I/II 06/1998 3(suspended)<strong>AvL</strong> N99SAN Conversion of short-acting octretide to the long-acting compound octreotide B Taal II 03/1999 15(SandostatinLAR): a phase II dose finding study in metastatic carcinoid tumors.CLINICAL TRAILS
176CLINICAL TRAILSTYPE OF TITLE STUDY COORDINATOR PHASE ACTIVATED NO PTS.CANCER IN <strong>AvL</strong> (in italics: (CLOSED) IN <strong>AvL</strong>STUDY international coordinator) per 1.9.1999HEAD AND NECK TUMORSEORTC 22954 Phase II study on larynx preservation comparing radiotherapy versus concomitant RB Keus II 12/1996 7chemotherapy in resectable hypo-pharynx and larynx cancers.(04/1999)EORTC 24922 Randomized phase II trial of methotrexate versus two schedules of taxol in patients JH Schornagel II 08/1996 4with advanced squamous carcinoma of the head and neck.(12/1998)M95THP A phase II-B multicentre study on the effect of mTHPC-mediated PDT on primary AJM Balm II 10/1995 23squamous cell carcinomas of the head and neck.M97RTO Phase II multi-institutional trial of targeted supradose cisplatin chemoradiation for IB Tan II 09/1997 74stage IV squamous cell carcinoma of the head and neck.M98THP A multi-center, multi-national, open-label, single group and multiple dose study of IB Tan II 06/1999 0Foscan-mediated photodynamic therapy (PDT) for the palliative treatment of recurrent,refractory or second primary SCC of the H&N in patients considered incurable withsurgery or radiotherapy.M99PDT A multi-center retrospective study to examine the efficacy, tolerability and safety of IB Tan III 06/1999 17conventional radiotherapy and/or surgery on primary squamous cell carcinoma’s of(09/1999)the head and neck in patients who have a similar entry criteria as for the Foscanmediated PD 009003.<strong>AvL</strong> N96-1265 NKB 96-1265; Prediction of radiotherapy response using FISH to assessAJM Balm Pilot 06/1996 31chromosome damage in tumors and normal tissue.<strong>AvL</strong> N98RTB Carotid arterial acclusive disease following radiation therpay; A prospective study in W Boogerd Pilot 10/1998 0patients with a parotid tumor.ECSG TRIALS16962 B Phase II trial with LU10393 in patients with breast cancer and melanoma. JHM Schellens II 07/1997 1(09/1998)16962 M Phase II trial with LU10393 in patients with breast cancer and melanoma. JHM Schellens II 07/1997 11(03/1999)16967 Phase II trial of 96-hours continuous infusion of paclitaxel as a single agent in JHM Schellens II 02/1997 3patients with bladder cancer resistant/ refractory to MVAC/ MVEC/ CMV.(02/1999)
Invited Speakers177INVITED SPEAKERSAhmed S (UK)Germline immortality in C. elegans.Amaya E (UK)Insertional mutagenesis through gene trap approaches inXenopus.Berzins S (Australia)Peripheral T-cell homeostasis and the paradox of thymicemigration.Blom B (USA)The novel cytokine IL-30 induces Th1 differentiation.Burgering B (the Netherlands)Cell cycle control by the PI 3-kinase/PKB/Forkhead pathway.Brenner M (USA)Antigen presentation by CD1: a distinct arm of the immunesystem.Brindley DN (Canada)Role of lipid phosphate phosphatases in regulating cellsignalling and division by exogenous lysophosphatidate.Burridge K (USA)Cell-matrix adhesions: assembly and signaling.Cabot M (USA)Ceramide glycosylation and resistance to chemotherapy: a cellsurvival pathway.Castle JD (USA)Regulation of compound exocytosis in mast cells.Cerundolo V (UK)MHC class I deficiency syndrome.Clevers H (the Netherlands)The APC of TCF.Cole M (USA)Essential cofactors for c-Myc and E2F1 oncogenesis.Daaka Y (USA)Regulation of Erk activation by G protein-coupled receptors.Dogterom M (the Netherlands)Force generation by microtubule polymerization.Dowdy SF (USA)Protein transduction into the mouse and diametrically opposedregulation of pRB in G1.D’Souza-Schorey C ( USA)Actin remodeling and membrane traffic: coordinated regulationby ARF6, Rac1 and RhoA.Fehling J (Switzerland)Deciphering the function of the pre-T cell receptor α gene:studies with TCR-transgenic and gene-targeted mice.Foulkes W (Canada)Clinicopatholagical features and survival in hereditary breastcancer.Gamel C (the Netherlands)Ontwikkeling van een verpleegkundige interventie: Voorlichtingondersteunend gesprek over de seksuele gevolgen vangynaecologische kanker.Goodman SL (Germany)Alpha-V integrins as targets for tumour therapy.Hayday AC (United Kingdom)The pre-T cell receptor as a transient inhibitor of apoptosis.Heeren RMA (the Netherlands)Chemical imaging of macromolecules in biological tissue withmass spectrometry.Hogg N (UK)How leukocytes use adhesion in an immune response.Hol W (USA)Protein crystallography, combinatorial chemistry and drugdesign for cholera and trypanosomiasis.Holstege F (USA)Genome-wide analysis of transcriptional circuitry.James DE (Australia)Regulation of GLUT4 traffic in adipocyes.Jones G (UK)Role of Rho proteins in regulation of macrophage migration.Kanaar R (the Netherlands)Roles of recombination in DNA damage repair.Kenyon C (USA)Genes and cells that regulate the aging process in C. Elegans.Kopf M (Switzerland)The cytokines responsible for asthma.Land C (USA)Radiation-related breast cancer risk: implications of the A-bombsurvivor studies.Lechleitner S (Austria)The role of the transcription factor IRF-1 in endothelial VCAM-1expression.Marks L USA)Exploiting technology to develop predictors of radiation-inducedlung injury: limits and lessons.Matsuda M (Japan)A link between tyrosine kinases and low-molecular-weight Geproteins, Rap1 and Rac.
178McKerracher L (Canada)Neurolan interactions with growth inhibitory substrates: role ofRho GTPase.Noelle RJ (USA)Role of CD40 and its ligand in the regulation of cellular andhumoral immunity.Peifer M (USA)Cell adhesion, signal transduction and cancer: the Armadilloconnection.Petit V (France)The role of paxillin in the epithelial-mesenchymal transitions inan in vitro system.Rangnekar VM (USA)Role of the leucine-zipper protein Par-4 in the regulation ofapoptosis.Schimpl A (Germany)Control of terminal B cell differentiation by Blimp-1.Schömig E (Germany)No escape for catecholamines: non-neuronal uptake ofbiogenic amines.Scott S (UK)Strategies for radiation-mediated gene therapy of cancer.Shortman K (Australia)A lymphoid-related dendritic cell lineage: developmental controland function.Sternberg PW (USA)Signal transduction during C. elegans development.Terhorst C (USA)Characterization of the product of the X-linkedlymphoproliferative disease gene, SAP.The H-S (Canada)Role of anergic T cells in autoimmune reactions.Tschopp J (Switzerland)Fas-induced apoptosis.Van de Rijn M (USA)Gene microarray analysis of human breast carcinoma.Van den Berg T (the Netherlands)Suppression of macrophage function by SIRPα ligation.Van Leeuwen J (USA)The oncogenic 70Z mutant blocks the PTB domain dependentnegative regulation of ZAP-70 by Cbl.Van Meer G (the Netherlands)Glycolipid topology and fuction; role of MDR and lateraldomains.Venkitaraman A (UK)DNA repair and tumorigenesis in cells that lack the breastcancer susceptibility gene, BRCA2.Wang X-F (USA)TGF-β signaling mechanisms.Wiley DC (USA)Structural studies of viral entry in influenza, HIV-1, and Ebolaviruses.
Projects supported by the Dutch Cancer society179Number of Title Div. Principal Starting Endedproject Investigator Date<strong>NKI</strong> 94-777 Development and clinical application of three-dimensional IX M Van Herk July ’94 May ’99image correlation algorithms with emphasis on applicationsin radiotherapy.<strong>NKI</strong> 95-954 Opening of ion channels by the mitogenic serum III W Moolenaar Dec ’95 Dec ’99phospholipid LPA: role of p60 src.<strong>NKI</strong> 95-956 The role of the retinoblastoma gene Rb-1 in murine II H Te Riele July ’95development and tumorigenesis.<strong>NKI</strong> 95-958 Susceptibility to tumorigenesis by loss of mismatch-repair II H Te Riele Oct ’95controlled genetic stability.<strong>NKI</strong> 95-960 T-cell development from CD34+ cell populations used for IV H Spits May ’95stem cell transplantations in cancer patients and from inW Gerritsenvitro expanded CD34+ cells.<strong>NKI</strong> 95-962 Cell cycle regulation by novel members of the E2F II R Bernards Sept ’95transcription factor family.<strong>NKI</strong> 95-963 Analysis of the function of MRP, the multidrug resistance V P Borst July ’95associated protein, by disruption of the Mrp gene in mice.<strong>NKI</strong> 95-969 Role of G-protein in metastasis. I E Roos Jan ’95 Dec ’99<strong>NKI</strong> 95-970 Biochemical characterization of Bmi-1 target genes. II M Van Lohuizen Dec ’95 Dec ’99<strong>NKI</strong> 95-978 Control of cell growth and differentiation by LPA. III W Moolenaar Febr ’95 Oct ’99<strong>NKI</strong> 95-979 The role of the alternative domains of the integrin α6 I A Sonnenberg Sept ’95 Oct ’99subunit in signal transduction and ligand binding.<strong>NKI</strong> 95-982 The influence of cytosolic degradation in normal and VI J Neefjes Dec ’95transformed cells on the generation of MHC class Ipresentable peptides.<strong>NKI</strong> 95-987 T-cell activation by CD3xCD19 bispecific antibody and IL- X/IV G De Gast May ’95 May ’992 in B-lineage leukemia/lymphoma.E BastXIII D De Jong<strong>NKI</strong> 95-1059 Individualization of cisplatin chemotherapy in patients with X/VIII J Schellens May ’95 May ’99solid tumors using a predetermined pharmacokineticJ Verweijdynamic response relationship.G Stoter<strong>NKI</strong> 95-1134 The use of quality of life assessments in daily oncology XII N Aaronson Sept ’95practice: an intervention study to facilitate doctor-patient X J Schornagelcommunication in outpatient palliative care settings.<strong>NKI</strong> 95-1144 Comparison of risk factors for ductal carcinoma in situ of XII F Van Leeuwen May ’95the breast, with differentation according to histology and XIII J Petersegenetic alterations.<strong>NKI</strong> 96-1155 The quality of life and neuropsychological status of patients XII N Aaronson Aug ’96with high-grade and low-grade glioma, and the quality ofJ Heimanslife of their partners.H Van der Ploeg<strong>NKI</strong> 96-1172 Immunotherapy of Hodgkin’s disease with B7-immunotoxin. X/IV G De Gast Nov ’96XIII D De Jong
180PROJECTSNumber of Title Div. Principal Starting Endedproject Investigator DateVU 96-1260 Regulatory aspects of carrier-mediated transport of X J Peters Jan ’96 Dec ’99methotrexate and novel antifolates: molecular mechanismsJ Schornageland impact for folate-based chemotherapy.<strong>NKI</strong> 96-1265 Prediction of radiotherapy response using FISH to assess VIII A Begg April ’96chromosome damage in tumors and normal tissues. IX H Bartelink<strong>NKI</strong> 96-1266 The role of ceramide-induced signal transduction events in III W Van Blitterswijk June ’96apoptosis induction.J Borst<strong>NKI</strong> 96-1267 The role of Tiam1 in Rac-mediated signaling. I J Collard May ’96<strong>NKI</strong> 96-1268 Functional activity of the estrogen receptor in human VIII/XIII L Van ’t Veer Jan ’96breast cancer.IX H Bartelink<strong>NKI</strong> 96-1269 Heat shock proteins as a tool in tumor antigen IV A Kruisbeek April ’96presentation.<strong>NKI</strong> 96-1275 Melanoma-specific CTL, generated in vitro using dendritic IV H Spits June ’96cells expressing melanoma antigens, as therapeutic for anK Weijeradoptive cellular immunotherapy.<strong>NKI</strong> 96-1276 Principles for generation of a T-cell mediated anti-tumor IV A Kruisbeek March ’96response.<strong>NKI</strong> 96-1279 Three-dimensional structure determination of MutS and II T Sixma Jan ’97Msh2, proteins involved in DNA mismatch repair andimplicated in human cancer.<strong>NKI</strong> 96-1284 Invasive genes in development and cancer: positional VII D Barlow Febr ’96cloning of a gene regulating invasive properties ofembryonic trophoblasts.<strong>NKI</strong> 96-1302 Dose verification during conformal radiotherapy. IX B Mijnheer July ’96J Lebesque<strong>NKI</strong> 96-1305 Analysis of the relationship between the level of α6β4 and I A Sonnenberg Oct ’96the agressiveness of squamous cell carcinomas usingtransgenic and knock-out mouse strains.<strong>NKI</strong> 96-1308 Improvement of geometrical accuracy to allow reduction of IX J Lebesque Aug ’96treatment margins in conformal radiotherapy.M Van Herk<strong>NKI</strong> 96-1376 Identification of cell-cycle regulatory proteins as targets for II R Bernards Nov ’96the Ras signal cascade.<strong>NKI</strong> 97-1430 The contribution of ATM heterozygosity to the risk of VIII/XIII L Van ’t Veer Febr ’97radiation-induced breast cancer.IX N RussellXII F Van Leeuwen<strong>NKI</strong> 97-1431 Cyclin D1 as a regulator of estradiol-mediated proliferation, II R Bernards Sept ’97mechanism and clinical implications.VI R Michalides<strong>NKI</strong> 97-1433 Identification of new genes contributing to anticancer drug VIII A Schinkel March ’97resistance using retroviral activation or differential cDNAscreening in cell lines deficient for drug-transporting P-glycoprotein.<strong>NKI</strong> 97-1434 Mdr knockout mice as a model system for the in vivo VIII A Schinkel Oct ’97modulation of P-glycoprotein-mediated drug transport.<strong>NKI</strong> 97-1435 The role of the sphingomyelin signal transduction pathway IX M Verheij June ’97in radiation-induced apoptosis.H BartelinkIII W Van Blitterswijk<strong>NKI</strong> 97-1436 Gene interactions and functions in multigenic susceptibility VII P Demant Febr ’97to colon cancer.<strong>NKI</strong> 97-1439 Pharmacokinetics and pharmacodynamics of X J Beijnen Febr ’97cyclophosphamide, thiotepa and carboplatin (‘CTC’) inS Rodenhuishigh-dose chemotherapy regimens.<strong>NKI</strong> 97-1440 Mechanisms of synergy between platinum compounds and X/VIII J Schellens Sept ’97topoisomerase I inhibitors in vitro and in vivo in patientsJ Brouwerwith solid tumors.J Verweij
181Number of Title Div. Principal Starting Endedproject Investigator Date<strong>NKI</strong> 97-1441 Role of the Cbl-proto-oncogene product in the regulation III J Borst Aug ’97of lymphocyte antigen receptor signaling andlymphomagenesis.PROJECTS<strong>NKI</strong> 97-1442 Manipulation of protein-protein interactions that mediate IV T Schumacher April ’97Ras- dependent cellular transformation.<strong>NKI</strong> 97-1443 Identification of novel invasion- and metastasis-inducing I J Collard Jan ’97genes by retroviral expression cloning and proviral tagging.<strong>NKI</strong> 97-1444 The role of endothelial cell damage in the development of VIII F Stewart Jan ’97renal radiation injury and possible mechanisms for IX L Dewitintervention.<strong>NKI</strong> 97-1446 Photodynamic therapy for malignant mesothelioma: X P Baas Jan ’97preclinical optimization and clinical application.VIII F StewartW Star<strong>NKI</strong> 97-1447 A new generation of conditional mouse mutants to study VII A Berns Jan ’97onset, progression, and therapy of a wide range of definedtumors.<strong>NKI</strong> 97-1467 The integrin alfa-V/beta-6 and the hyaluronic acid receptor I E Roos Jan ’97RHAMM: roles in carcinoma invasion and metastasis.<strong>NKI</strong> 97-1468 Detection of minimal tumor cell admixture in bone marrow X S Rodenhuis March ’97and peripheral progenitor cell preparations of patients with VIII/XIII L Van ‘t Veerbreast cancer.<strong>NKI</strong> 97-1561 The molecular mechanism(s) regulating imprinted gene VII D Barlow Jan ’97expression at the IGF2R locus.<strong>NKI</strong> 97-1589 Implementation of a Pain Education Program (PEP) for XII F Van Dam Dec ’98`cancer patients with chronic pain by nurses.J PasschierA Vielvoye-Kerkmeer<strong>NKI</strong> 98-1679 Chemokine receptor homologs: role in dissemination of I E Roos Jan ’98hematopoietic malignancies.XIII D De Jong<strong>NKI</strong> 98-1680 Role of Tumor Necrosis Factor receptor family members III J Borst Nov ’98and the FLICE protease in apoptosis-induction by DNAdamaginganti-cancer regimens.<strong>NKI</strong> 98-1682 Patient setup and treatment verification for conformal IX M Van Herk Jan ’98therapy using dynamic beam intensity modulation.K Gilhuijs<strong>NKI</strong> 98-1724 Quality of life assessment in ethnic minorities cancer XII N Aaronson Nov ’98patients in the Netherlands: A study of the SF-36, theCOOP/WONCA charts, the EORTC QLQ-C30 and theRotterdam Symptom Checklist.<strong>NKI</strong> 98-1729 Long-term cognitive deficits as a consequence of highdoseXII F Van Dam Febr ’98chemotherapy: a role in high-risk breast cancer X W Boogerdpatients and high-grade lymphoma patients.<strong>NKI</strong> 98-1794 The contribution of the MRP (multidrug resistance V P Borst Jan ’98associated protein) family to drug resistance.<strong>NKI</strong> 98-1795 Rho signaling: role in differentiation and transformation. III W Moolenaar Oct ’98<strong>NKI</strong> 98-1796 Regulation of primary and memory tumor-specific T-cell IV A Kruisbeek Jan ’98responses by signaling through the family of CD28/CTLA4-receptors.<strong>NKI</strong> 98-1798 Genetic alterations involved in local recurrence and XIII M Van de Vijver Oct ’98progression of invasive and non-invasive breast cancerJ Peterseafter breast conserving therapy.IX H Bartelink<strong>NKI</strong> 98-1799 Pharmacology of orally administered taxanes: a preclinical X J Schellens Sept ’98mechanism study and clinical evaluation.J Beijnen<strong>NKI</strong> 98-1830 Dose-volume-effect relationships for local control and IX J Lebesque July ’98normal tissue complications for prostate patients treatedL Boersmawith three-dimensional conformal radiotherapy.P Koper
182PROJECTSNumber of Title Div. Principal Starting Endedproject Investigator Date<strong>NKI</strong> 98-1831 Clinical implementation of conformal radiotherapy of lung IX B Mijnheer Nov ’98cancer using dynamic beam intensity modulation.E DamenH Bartelink<strong>NKI</strong> 98-1832 The SCC-1 (Susceptibility to colon cancer - 1) gene: VII P Demant May ’98isolation and functional analysis.<strong>NKI</strong> 98-1833 Long-term risk of second cancer following treatment of XII F Van Leeuwen June ’98Hodgkin’s disease, testicular cancer and breast cancer. IX B Aleman<strong>NKI</strong> 98-1837 Identification and cloning of a lung tumor susceptibility VII M Snoek June ’98gene located in the Hsp70-G7 interval of the MHC class IIIregion of the mouse.<strong>NKI</strong> 98-1838 Different response of RER + and RER - tumors to II H Te Riele Jan ’98chemotherapy.X S RodenhuisXIII D De Jong<strong>NKI</strong> 98-1839 The role of Tiam1 in E-cadherin-mediated homophilic I J Collard May ’98adhesion.<strong>NKI</strong> 98-1854 Risk assessment and gene-environmental interactions in XII F Van Leeuwen Jan ’98breast and/or ovarian cancer families.XIII L Van ’t Veer<strong>NKI</strong> 98-1858 The psychological and behavioral impact of genetic XII N Aaronson May ’98counseling for colorectal cancer: a prospective multicenterF Menkostudy.X B Taal<strong>NKI</strong> 98-2110 Quality of life assessment in clinical oncology research. XII N Aaronson July ’98F Van Dam<strong>NKI</strong> 99-2036 Molecular analysis of the cytotoxic T cell response. IV T Schumacher Nov ’99A Kruisbeek<strong>NKI</strong> 99-2042 G protein control of cell proliferation and transformation. III W Moolenaar Oct ’99<strong>NKI</strong> 99-2043 Dose escalation study for non-small cell lung cancer IX J Lebesque April ’99(NSCLC) using three-dimensional conformal radiotherapywith tight treatment margins and functionally optimizedJ BelderbosL Boersmaradiation treatment plans.<strong>NKI</strong> 99-2048 Characterization of antigen specific and biological IV H Spits Jan ’99responses of CD4 + melanoma specific T cells.X G De Gast<strong>NKI</strong> 99-2051 Modulation of normal human T cell development by IV H Spits April ’99ectopic expression of TAL-1, -2 and LYL in T cellprogenitor cells.<strong>NKI</strong> 99-2052 Structure-function studies of cyclin D1 in complex with II T Sixma Jan ’99nuclear hormone receptors and/or coactivators.R Bernards<strong>NKI</strong> 99-2053 Dephosphorylation of retinoblastoma family proteins by II R Bernards Sept ’99protein phosphatase 2A.<strong>NKI</strong> 99-2054 The role of interleukin-10 in immunosuppression of tumor VI J Neefjes Febr ’99responses.IV H Spits<strong>NKI</strong> 99-2055 The role of the nuclear inositide pathway in cell cycle III N Divecha Dec ’99progression.<strong>NKI</strong> 99-2056 Mechanism of cell cycle regulation and control of cellular II M Van Lohuizen May ’99lifespan by the Polycomb-group and oncogene Bmi1.<strong>NKI</strong> 99-2058 Development of a mouse model to study the genetic basis VII A Berns Aug ’99of mesothelioma.<strong>NKI</strong> 99-2060 Mechanisms of reduced cellular accumulation of X J Schellens June ’99topoisomerase I inhibitors.VIII A Schinkel<strong>NKI</strong> 99-2117 Control of cell cycle progression by integrin mediated I A Sonnenberg April ’99adhesion.
Major projects supported by other organizations183PROJECTSGranting agency Title Div. Principalproject numberinvestigatorNWO 901-01-165 Characterization of Tiam-1 interacting proteins. I J CollardNWO 902-11-060 Role of BP180 in keratinocyte adhesion. I A SonnenbergM JonkmanNetherlands Heart Foundation Functional analysis of the integrin variants, α6A and β1D, I A Sonnenberg96-006in cardiogenesis.Dutch Kidney Foundation The role of the integrin α3β1 in the development and I A SonnenbergC96.1581 pathophysiology of the glomerus.J WeeningEEC Functional analysis of the ?1D integrin in myogenesis. I A SonnenbergERBFMBICT961823EEC The role of the tumor metastasis gene TIAM1 in cell I J CollardERBFMBICT971964signaling and development.EEC Identification and functional analysis of the genes involved I A SonnenbergERBCHRXCT972062in junctional epidermolysis bullosa, disorders affectingadhesion of epithelial cells.Dystrophic Epidermolysis The role of BP180 and α6β4 in human diseases. I A SonnenbergBullosa Res. Assoc.Deutsche Forschungs Identification and characterization of proteins that regulate I J CollardGemeinschaftTiam1/Rac1 depended signal transduction pathways.SA 763/1-1Dr Mildred Scheel Foundation Signaling pathway by p120GAP. I J Collardfor Cancer Research683 400001EEC-Bio-CT98-5060 Tiam1/Rac signalling in neuronal differentiation. I J CollardDystrophic Epidermolysis Assembly of hemidesmosomes and identification of novel I A SonnenbergBullosa Researchhemidesmosomal components.Association (UK)Netherlands Heart Functional analysis of plakoglobin in the formation of the I A SonnenbergFoundation 98.044intercalated discs.EEC CT97-2062 \Identification and functional analysis of the genes involved I A Sonnenbergin junctional epidermolysis bullosa, disorders affectingadhesion of epithelial cells.NWO-SLW 805.17.541 In vivo and in vitro analysis of effects on IL-7 response, II M Van Lohuizensurvival and differentiation of pro-T cells by the oncogeneand Polycomb-group gene Bmi1.STW VBI.4568 Program for discovery of novel drugs, based on the II T Sixmautilization of a naturally occurring soluble protein analog ofthe nicotinic acetylcholine receptors.Biomed II Role of genomic instability in environmental carcinogenesis. II H YamasakiENV4-CT97-0469H Te RieleBiomed II MYC network proteins in tumorigenesis. II M EilersBMH4-CT98-3532R Bernards
184PROJECTSGranting agency Title Div. Principalproject numberinvestigatorNWO MW 901-02-223 Crystal structure determination of the components of an II T SixmaE2/E3 ligase ubiquitination system involved in cell-cyclecontrol.NWO Pionier 906-99-001 Mechanism of gene repression by mammalian PolycombgroupII M Van Lohuizenproteins: connections to cell cycle regulation andother silencing processes.NWO CW 98016 The Process of transposition: three-dimensional structure II T Sixmaanalysis of Tc1 and Tc3 transposase from Caenorhabditiselegans.NWO CW JC 99548 Structural studies of DNA mismatch repair. II T SixmaHFSP RG0249/1999-M 103 Upstream and downstream regulatory controls in the Rb pathway. II K HelinR BernardsSON 330-210 The role of diacylglycerol kinase in cell signal transduction. III W Van BlitterswijkEEC ERBFMBICT 972142 Nuclear inositide cycle. III N DivechaNWO/SLW 805-05-103 Rho signaling by G-protein coupled receptors. III W MoolenaarNWO 901-07-095 Role of the CD27/CD70 receptor-ligand pair in control of III J Borstthe immune response.R Van LierNWO-MW 901-08-317 The role of the IL-7 receptor in development of human T cells. IV H SpitsNWO-MW 901-02-215 Identification of small molecule ligands for cellular proteins. IV T SchumacherNWO-ALW 805-17-531 Identification and characterization of genes involved in T- IV H Spitscell commitment.National Multiple Sclerosis How antigen processing pathways affect negative selection IV A KruisbeekSociety (USA) RG 2940-A-1 of MBP reactive T cells.Human Frontier Science Pre-TCR expression and function in developping T cells. IV A KruisbeekProgram Organization (HFSPO)RG 0335/1998-MNWO-MW (Programma) Cytoplasmic and nuclear signaling pathways involved in IV A Kruisbeek901-07-096negative selection of MBP rective T cells.Son 331-26 Antigenic variation in trypanosomes; mechnisms of gene V P Borsttransposition and alterations in gene expression.NWO 902-23-097 Mechanisms and pathophysiological significance of V P BorstR Oude Elferinkhepatobiliary lipid transport.SON 335-210 DNA-transposition in animal cells. V R PlasterkNWO-SLW G protein in C. elegans. V R PlasterkNWO-GMW 90104094 Genetic analysis of memory defects. V R PlasterkHFSP RG 0099 Perception of odors, tastes and temperature: attraction V R Plasterkand aversion of C. elegans.NWO 901-04-209 Genetic analysis of wiring defects of neurons involved in V R Plasterktaste perception in C. elegans.NWO 048-011-021 Investigation of membrane transport proteins involved in V P Borstmultidrug resistance of cancer.SON 97045 Tc1-type transposons: mechanism and regulation of V R Plasterkjumping, and application as vectors for transgenesis.SON 97046 Function and biosynthesis of a new modified base V P Borstdiscovered in trypanosome DNA, B-D-glucosylhydroxymethyluracilor J.NWO 940-70-008 Genetic identification of new drug targets in serpentine V R Plasterkreceptor signaling in the central nervous system.
185Granting agency Title Div. Principalproject numberinvestigatorEEG 980217 TMR research networks C. elegans. V R PlasterkNWO ALW 805-48-009 The molecular mechanism of smell and taste: perception V R Plasterkvia G-protein coupled receptors in the nematode C.elegans.PROJECTSSB 204269 Identification of the Molecular target of SB-204269 in C. elegans. V R PlasterkNato lst. Clg. 97 4931 Regulations of Retrotransposition in C. elegans. V R PlasterkNWO (Medische Substrate specificity of the MHC-coded peptide pump and VI J NeefjesWetenschappen) 901-09-027 generation of MHC class I presentable peptides.NWO 901-09-28 The influence of cytosolic degradation in normal and VI J Neefjestransformed cells on the generation of MHC class Ipresentable peptides.NWO/PGS 030-90-57 Processes involved in antigen presentation by MHC VI J Neefjesmolecules and the release of cytosolic granules.EEC ERB Intracellular mechanisms of antigen processing and VI J NeefjesFMRX-CT96-0069presentation by the MHC class I and class II molecules.EEC PL 960505 Biochemical basis of rational vaccine design for induction VI J Neefjesof protective immunity.Biotag Cloning of epiglycanin cDNA. VI J HilkensCentocor Regulation of episialin expression in cancer and normal tissue. VI J HilkensNIH R01-CA79580-01 Molecular studies on MUC 1/Episialin Promoter. VI J HIlkensEEC BMH4-CT96-1518 Development of murine transgenic systems for the VII A Bernsexperimental study of tumor initiation, progression andtreatment.NWO 925-01-001 Genes and mechanisms in the multigenic control of cancer VII P Demantsusceptibility: the mouse model and application to humancancer.EC ERB IC-CT98-0317 Genetic dissection of multigenic predisposition to disease VII P Demantin the mouse model.EC BIO4 CT97 4850 Recombinant Congenic Strain Mouse Facility. VII P DemantEC BIO4 CY98 0445 RCS system for identification of genes responsible for VII P Demantmultigenic control of disease susceptibility.AIDS Fonds project 4011 The role of P-glycoprotein in the oral bioavailability and VIII A Schinkelpenetration of HIV protease inhibitors into HIV sanctuarysites.EEC (DGXII) A code of practice for dosimetry of boron neutron capture IX B MijnheerSMT4-CT98-2145therapy (BNCT) in Europe.STW Application of an electronic portal imaging device for IX B MijnheerBGN 33-3240dosimetry in radiotherapy.M Van HerkSTW (BGN 33-3240) Portal image analysis. IX M Van HerkHealth Insurance Council Prospective study on the influence of high dose X S RodenhuisFund for Investigative Medicine chemotherapy with peripheral stem cell support on09-94-51disease-free survival of patients with breast cancer and 4or more lymphnode metastases.Schumacher-Kramer Stichting Autologous bone marrow transplantation in breast cancer. X S RodenhuisRaad voor Gezondheids- Bioanalysis and clinical pharmacology of anti-retroviral drugs. X J BeijnenonderzoekRaad voor Gezondheids- Bioanalysis and clinical pharmacology of HIV protease inhibitors. X J BeijnenonderzoekEC Biomed-2 PL 96-2333 Population analysis of anticancer drug treatment. X J Schellens
186PROJECTSGranting agency Title Div. Principalproject numberinvestigatorEC Biomed-2 Fluorescence imaging for detection, localization and XI H SterenborgPL 96-2260staging for superficial cancer and pre-cancer in the femaleN Van der Vangegenital tract.VIII F StewartHealth Insurance Council HIPEC in peritonitis carcinomatosa of colorectal origin. XI F ZoetmulderFund for Investigative Medicine98-41Health Insurance Council Breast cancer screening in cases of familial pre-disposition. XI E RutgersFund for Investigative MedicineJ Klijn98-3Scotia Pharmaceuticals mTHPC photodynamic therapy in early staged primary XI B Tanhead and neck cancers.Atos Medical Development and evaluation of a second generation XI F HilgersProvox voice prosthesis.A AckerstaffXII N AaronsonStichting Mundo Crastini Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in XI F ZoetmulderMelioriperitonitis carcinomatosa of colorectal origin.Prevention Fund/Organon Hyperstimulation of the ovary and risk of ovarian cancer. XII F Van Leeuwen28-2540 C BurgerLandelijk Centrum Evaluation of the quality of nursing care: the development XII F Van DamVerpleging & Verzorging of a modular system.950815Prevention Fund Physical activity and risk of breast cancer. XII F Van Leeuwen28-28460 M RookusStichting Klinische Genetica Satisfaction and knowledge about heriditary testing and XII N AaronsonAmsterdamcounseling.F MenkoXI E RutgersRoss Products Health-related quality of life of cachexic patients with XII N Aaronsonadvanced pancreatic cancer treated with an n-3 fatty acidenriched oral supplement versus an isonitrogeneousisocaloric oral supplement: a double blind, randomizedphase III study.International Health IVF treatment, unexplained subfertility and number of XII F Van LeeuwenFoundationretrieved oocytes in relation to age at menopause.C BurgerHealth Insurance Council Surgical biopsy vs needle biopsy for breast cancer. XIII P BesnardFund for Investigative Medicine XI E Rutgers97-032 XIII J PeterseW MaliEC Biomed-2 Systematic overview (meta-analysis) of all randomized trials Biom O DalesioBMH4-CT96-0113of treatment of prostate cancer.H Van TinterenEC Telematica HORIZON and Global HORIZON.Biom O DalesioHC 1106E Van der Donk
Personnel-Project index187Aalders MCG 132Aaronson NK 137, 139Ackerstaff AH 128Adriaans EK 143Agami R 32Ahmadian MR 24Aleman BMP 117, 143Allen JD 91Andersson H 140Ankema K 162Atsma D 149Baars D 157, 160Baars JW 115Baas F 64Baas P 89, 104, 112, 117, 147Bais EM 112, 147Bakker AQ 53Bakker S 162Bakx R 160Balkenende A 73Balm AJM 117, 127, 128Bapat S 89Bardelmeijer H 114, 147Barlow D 81Bartelink H 87, 94, 96, 99, 105, 107, 130Batchelor D 115, 127Bathoorn A 24Bedeker I 114Beelen MLR 143Begg AC 87, 107, 128Beijersbergen R 82Beijnen JH 93, 112, 114, 115, 130, 147Belderbos JSA 103, 104, 107, 117Benne IS 162Berezikov E 62Bernards R 32, 162Berns A 76Berns K 32Besnard APE 130Biervliet AS 140Bijker N 130, 149Bins A 51Bischof F 51Bleeker F 76Bleiker EMA 139Blommestijn GJF 160Blyweert W 87Bobeldijk R 163Boer M 74Boerrigter-Barendsen LH 150Boersma LJ 104Boersma M 106Bohlander M 93Bonfrer JMG 127, 147Bontjer I 44Boogerd W 140Boot H 117, 130, 147, 150Borger JH 103, 105, 106, 130, 147Borst J 44Borst P 64, 66Bos E 71Bos KE 128Bos L 101Bosch C 96Bosma AJ 94Bosnie NH 162Boter M 22Boucher A 157, 160Bouma M 114Boutmy-de Lange MS 150Bovenkerk NJ 162Braak S 142Braas PAM 142Brejc K 39Brink G 150Brinkhuis RF 91Brocks HHJ 160Broeks A 94Broertjes L 162Brohet RM 142Bronk M 32Brouwer C 34Bruinvis IAD 103, 104Brummelkamp T 32Buitelaar AC 142Bulale MT 162Bulthuis JC 162Calafat J 30, 161Carlee L 82Chaves I 66Cillessen S 82Claij N 34Clark D 53Clarke J 47, 127Cleyne WHJJ 137Cleypool CGJ 114, 147Coccoris M 55Coco Martin JM 87, 128Collard JG 24Copper MP 128Cordaro T 51Couwenberg F 53Cross M 66Csikos T 83Cuadrado Lopez M 81Cuppen E 62Custers F 117D’Santos C 47Dahler E 94Dahmen E 87Dalesio OB 112, 115, 117, 147, 149, 157, 158, 160Damen EMF 103, 105Danen E 27Dannenberg J-H 34De Boer EJ 142De Boer JB 130De Boer R 99De Bree E 130De Feij –de Graaf HM 147De Gast GC 57, 115, 127De Goede JJP 104
188PERSONNEL-PROJECT INDEXDe Goeij CCJ 162De Groot K 83De Haas M 64De Jaeger K 103, 104De Jong D 57, 117, 131, 149, 150De Jong LA 93De Jong Y 71De Jonge H 27De Klerk G 112De Kraker J 147De Lange F 160De Melker A 44De Moes J 83De Rond MEJ 140De Ruyter W 140De Visser K 51De Vries E 44De Vries F 157, 160De Vries JDH 127De Vries SS 34De Widt JJM 45Dekker HMJ 34Dekker N 99Dellemijn TAM 57, 150Delzenne-Goette E 83Demant P 83Detmar SB 137Deurloo W 158, 160Dewit LGH 89Dijsselbloem E 83Diks S 45Dirks A 66Divecha N 47Dooijes D 66Dorresteijn LDA 128Douma S 32Dubbelman AC 112Duchateau L 149Dusseljee S 69Eggermont AMM 127Elias S 57Engelsman M 101Engering A 71Enzlin J 39Evers R 64Faneyte IF 96, 130Fentiman IS 149Fernandez-Borja M 69Filius P 99Fischer SEJ 62Floore AN 94Floot BGJ 89Fluitsma D 71Fontao L 27Fontijn D 55Fraas BA 103Frenken L 1 60Friederich C 162Gaemers I 74Gajewska M 83Gallee MPW 143, 147Garcia-Saez I 62Geerts HAM 27Gerrits H 66Gerritsma MA 139Giepmans BNG 42Gilhuijs KGA 99Gimond C 27Goedbloed C 104Goede IN 162Gonggrijp S 1 28Goumans M-J 49Grimminck HMG 1 62Grit J 137Grummels A 87Grund D 162Grunstra ME 130Guo J 64Gustafson 127Haanen JBAG 55, 115Habets R 29Hagedoorn M 137Hahn D 150Haks M 51Halstead J 47Handgraaf PJ 162Hart AAM 105, 128, 142Hartog VB 143Haustermans KMG 87, 128Havelkova H 83Haverkamp T 62Hazendonk E 62Heemsbergen WD 104Hendriks J 44Hendriksen J 74Hengeveld GM 42Hermans R 151Hetem-Maidment TL 162Hiemstra A 160Hijmans EM 32Hilgers FJM 128, 140Hilkens J 74Hilkmann HAM 163Hillebrand MJX 114Hilliard M 62Hoebers FJP 105Hoefnagel CA 117, 127, 130, 131, 147Hoetelmans RMW 114Hoffmann M 162Hofland I 87Hogema K 160Hogervorst FBL 149, 150, 163Hollenstein J 139Hollmann M 142Hollo Z 64Holtkamp M 115Hoogeman M 104Hoogervorst DA 76, 162Hooijberg E 53Hoopman R 137Horenblas S 131Houssa B 45Huisman MT 91Huitema ADR 112, 114,Hurkmans CW 103, 105Israëls SP 115, 127Iszvak Z 62Itoh F 49Itoh S 49Ivics Z 62Jacobs JJL 37Jalink K 29Jansen BM 147Jansen G 62Jansen HA 140Jansen I 160Jansen L 34, 127, 130, 131, 147Jansen SE 114Janssen JJ 162Janssen JWRM 30, 161Janssen L 24Jongkind JF 140Jonker JW 91Jonkergouw PAJ 163Jonkers J 76Jordens I 69Jovine L 39Julien J-P 149Kaag MM 130Kaas R 130
Kaats E 150Kalkman E 104Kalksma ART 140Kamp MK 22Kamphorst J 22Keblusek P 37Keijzers S 128Kenbeek WST 162Kerbusch Th 112, 114Kerkhoven RM 32, 162Kersten MJ 59, 115, 127Kessels HH 55Ketting R 62Keuning KDHM 128Keus RB 107, 128Kieboom K 37Kieft R 66Kikkert R 44Klaren H 130, 150Klausner JM 127Klein MG 132, 137Kleinsma J 162Klip H 142Klitsie I 51Klokman WJ 143Klop WMC 128Klous A 83Kluijt FHKluijt I 150Kluyt I 139, 142Knipscheer P 39, 76Koch R 62Kooi M 147, 157, 160Kool M 64Koopman-Kroon FJ 114Koper P 104Korse CM 147Koster J 27Kramer D 27Kranenburg O 42Kreft M 27Krekko FC 162Kreukels BPC 140Krimpenfort PJA 76, 163Kristel P 96Kroeskamp GJ 162Kroon BBR 127, 128, 130, 147Kroon FHM 128Kruijtzer CMF 112Kruisbeek AM 51Kubilis PS 151Kueter E 53Kuikman I 27Kuin A 89Kwaks T 32Lacerda H 42Lageweg-Beumkes M 162Lagro AJL 162Lambrechts AC 94Lamers EA 104Lamers M 39Lamers TE 163Lanson JH 101Laureijs G 101Lebesque JV 99, 103, 104, 105Lejeune FJ 127Liénard D 127Lieverts J 112, 158, 160Ligthart S 22Linden AJ 162Linders TC 147Linthorst G 115Loomans CJM 32Loonstra A 76Los A 45Louwe R 101Lund A 37Luts ALM 163Lyle R 81Lyons S 76Maaskant JM 112, 160Maertzdorf BPG 142Mahn-Schaefers M 112, 160Maliepaard M 93, 112Malingré MM 112, 114Malliri A 24Mallo H 112, 115Mancuso AA 151Mandjes I 112, 160Mari Aparici C 147Marino S 76Marissen W 51Marsman M 69Martins C 76Masselink H 32Mathôt RAA 112, 114Mathy A 157, 160Matthesius F 76McShan DL 103Meijer GJ 104Meinhardt W 131Mendenhall WM 151Menko FH 139, 142, 150Merel P 76Meuwissen R 76Micelli F 76Michalides RJAM 73, 128Mijnheer BJ 99, 101, 103, 104, 105Mikkers H 76Minderhoud TJ 103MLF Veldhuysen 117Modder C 160Mol C 64Moolenaar WH 42Moonen L 107Moorman C 62Motta MC 37Mulder J 42Muller MJ 137, 140Muller P 104Muller SH 99, 104, 105, 127, 130, 147Mussmann R 66Nan-Offeringa L 114Naspetti M 53Ndoye A 157, 160Nederlof PM 149Neefjes J 69Neisig A 69Nicolaas FT 162Nievers M 27Nieweg OE 127, 130, 131, 147Nijkamp W 82Nooijen WJ 115, 147Noordanus RP 128Noteboom E 161Nuyen B 114Olivio C 24Oomen LCJM 24, 160Oomen WJM 137Oosterhoff Y 117Oosterkamp R 32Op de Coul BMR 128Oppelaar H 89Ottenheim CPE 150Ouwehand M 114, 147Overbeek TA 140Overdijk D 53Pameijer FA 128, 151Parsons JT 151Peeper DS 32Pépin E 51189PERSONNEL-PROJECT INDEX
190PERSONNEL-PROJECT INDEXPeters AR 99Peters PJ 71Peterse JL, 96, 105, 130, 142, 143, 149Pfauth AS 161Pieters BR 94, 103, 105, 106, 130, 147Plasterk RHA 62Ploeger LS 99Pluim D 93, 112Poodt J 149Postma FR 42Pothof J 62Pouwels J 32Price L 24Profijt M 114Pruijt JFM 115Pruntel R 150, 163Qaedvlieg P 117Quon K 76Raaijmakers N 101Ran L 42Rasch CRN 99, 104, 107Regnerus R 150Reid T 24Reinders-Som A 160Reits EAJ 69Remeijer P 99Rentenaar L 158, 160Ridderbos JN 94Robanus Maandag E 96Roberts D 158, 160Rodenhuis S 94, 112, 115, 140Roefs M 47Rookus MA 142Roos E 22Roozendaal GK 127Rosenbrand RM 139, 140Rosing H 114Rozenhart M 147Ruevekamp MC 89Ruiter GA 45, 107Ruivenkamp C 83Ruizendaal J 53Russell NS 87, 94, 143Rutgers EJTh 130, 142, 147, 149, 150Ruuls-Van Stalle EMF 22Ruurs P 45Saarnak AE 103, 105, 106Sabatini B 66Saeki T 64Sander EE 24Saridjan N 34Schagen SB 140Scheijen BGPH 32Schellens JHM 93, 112, 114, 117Schepers K 55Schinkel AH 91, 93Schippers MCJ 142Schippers-Gillissen C 149Schlag PM 127Schneider P 74Schoemaker NE 112, 114Schornagel JH 112, 115, 128, 137Schot M 112Schouwink JH 89, 147Schraffordt Koops H 127Schrama J 115Schrauwers AJ 162Schreurs M 59Schrijvers A 112Schuijff L 34Schultz I 83Schultze Kool L 107, 128Schumacher TNM 55Sein J 57, 115Seppenwoolde Y 104Shvarts A 32Silvis W 73Simmer F 62Sixma TK 39Slaper-Cortenbach ICM 115Sleutels F 81Smeele S 51Smit JW 91Smit L 44Smitsmans MHP 99Smulders BS 103, 104Sneeuw KCA p137Snoek M 83Soede RDM 22Sonnenberg A 27Sonneveld P 27Souwer Y 147Spaans C 162Sparidans RW 114Spee PJL 69Spits H 53Sprong D 87Spronk C 142Starrevelt HP 162Steggerda MJ 103, 106Steinmann G 127Sterenborg HJCM 132Sterk LMTh 27Stewart FA 89, 117, 132Stoffers HJ 160Stötter G 55Stringer SP 151Strobbe LJA 127Stroeken PJM 22Swart M 112Taal BG 117, 139, 147, 149, 157Tan IB 107, 128Tanger EH 162Tanis PJ 127Te Poele JAM 89Te Riele H 34Ten Berg RGM 162Ten Bokkel Huinink WW 112, 114, 131, 132, 147Ten Dijke P 49Ten Klooster JP 24Tepper AD 44, 45Ter Haar N 149Theuws JCM 104Thijssen K 62Thingstad T 74Thorikay M 49Tibben MM 114Tijsterman M 62Timmers AP 128Timpico MAM 162Tirion F 51Tjin E 71Toebes M 55Tolkamp AJM 162Tomas J 142Tougha R 158, 160TreurMulder M 83Tripodis N 83Turpijn-la Pas SA 160Uiterwaal H 101Ulbert S 66Urbanus JHM 94Valdés Olmos RA 117, 127, 128, 130, 147Valdimarsdottir G 49Valent Q 51Valkenet L 160Van ‘t Veer LJ 94, 105, 117, 142, 143, 149, 150, 163Van ‘t Wout WK 34, 162, 163Van Amerongen R 76Van As CJ 128, 140
Van Beurden M 132, 139, 149, 150Van Blitterswijk WJ 45, 107Van Bunningen BNFM 106Van Coevorden F 117, 130Van Dalen AJ 99Van Dam FSAM 128, 140Van de Kasteele WF 57, 115Van de Pavert IV 87, 160Van de Vaart PJM 107Van de Ven PJH 99Van de Vijver MJ 96, 130, 132, 149Van Deemter L 64Van Delft S 24Van den Belt-Dusebout AW 142, 143Van den Berg C 62Van den Berg R 162Van den Berk P 59Van den Bogaard CJC 57Van den Bongard DHJG 114Van Den Boom M 55Van Den Brakel J 51Van der Ahe FH 162Van der Borch I 81Van der Donk E 157, 158, 160Van der Flier A 27Van der Gulden H 76Van der Hoeven PCJ 45Van der Horst G 44Van der Horst M 62Van der Kammen RA 24Van der Kooy K 83, 142Van der Linden S 62Van der Pijl D 162Van der Put R 114Van der Riet D 39Van der Schueren B 87Van Der Sman J 32Van der Stroom GJ 160Van der Valk MA 76, 162Van der Vange N 89, 130, 132Van der Veen SAJM 128Van der Velde T 160Van der Velden M 74Van der Wal A 89Van der Wal J 29Van der Wel N 71Van der Woude HR 147Van Dijk MAJ 94Van Dijk WJ 39Van Dongen JA 147Van Donselaar E 71Van Drimmelen RO 160Van Etten I 42Van Gastelen MA 93Van Gijn R 114Van Ham SM 69Van Hattum HCA 162Van Heeswijk RPG 114Van Helvoort A 64Van Herk M 99, 101,104Van Horck FPG 42Van Ingen K 101Van Kesteren Ch 112, 114Van Kleef EM 89Van Klink Y 34Van Kooy M 83Van Leeuwen F 42Van Leeuwen FE, 94, 130, 142, 143Van Leeuwen S 27Van Leusden MR 27Van Lindert ACM 132, 149Van Lith MJTM 69Van Lohuizen M 37Van Luenen HGAM 62Van Muylwijk EW 162Van Oijen M 57Van Poll D 127Van Poppel N 22Van Puijenbroek A 57Van Rens ALE 139, 142, 150Van Rhijn DCM 140Van Rijthoven EAM 22Van Roosmaelen N 162Van Schooten FJ 117Van Slooten GW 127, 130Van Tellingen O 114, 147Van Tinteren H 117, 151, 157, 158, 160Van Veen RLP 89Van Veen-Buurman CJH 163Van Velthuysen L 149Van Velthuysen MLF 128Van Vliet M 142Van Vugt H 83Van Waardenberg W 160Van Waardenburg RCAM 93, 112Van Welsem T 149Van Wezel T 83Van Zandbergen E 147Van Zandwijk N 112, 117, 157Vander Poorten VLM 128Vastenhouw N 32Veldkamp AI 114Vens C 87Venselaar J 101Verhaagh S 81Verheij M 107Verheijen M 62Verhoef S 139, 142, 150Verhoeven E 37Verlaan I 42Verlaan M 37Verloop J 142Vernie LN 163Verra N 57, 115Verschoor T 73Versteegden CM 142Verwijs M 87Verwoerd D 69Vijlbrief HP 104Vijlbrief RE 99Vink J 76Visser B 53Vlietstra A 140Volders H 74Voncken JW 37Vooijs M 76Voordouw A 53Voorhoeve PM 32Vooys W 57Vos CJ 149Vos JC 69Voûte PA 147Vrieling C 105Vyth-Dreese FA 57, 115, 150Wagenaar E 91Wals A 160Weder P 51Weeda E 160Weenink C 117Weevers MCH 140Weijer K 53Welp EAE 143Werner A 44Westermann AM 115Wever LDV 137, 139Whyatt D 32Wicks S 62Wiegant W 53Wielinga P 64Wienholds E 62Wientjens E 37Wigbout G 139, 142, 150Wijnands E 51Wijnands YM 22Wijnholds J 64191PERSONNEL-PROJECT INDEX
192PERSONNEL-PROJECT INDEXWillemse E 160Winterwerp H 39Witkamp AJ 130Witte AMC 117Wittkämper FW 101Woerdeman LAE 128Wolff W 162Wolkers M 55Wolterink R 106Woordesvan Baalen MMPGM 142Wubbolts RW 69Yan D 104Yasuda Y 53Zeelenberg IS 22Zelcer N 64Zerp SF 45, 107Zevering Y 51Ziblat L 157, 160Zijp L 99Zoetmulder FAN 117, 130, 132, 157Zondag G 24Zuur CL 128Zwart R 81Zwerver A 162Zwijsen RML 32
Colofon193Chief editorFA StewartEditorsAJM BalmIS BenneF GodsonWJ Van BlitterswijkH Van LuenenEJ VosFA Vyth-DreesePhotograph HM The Queen BeatrixVoor inlichtingen/toestemming:Rijksvoorlichtingsdienst,afd. Pers en Publiciteit/FOTOPostbus 200092500 EA ’s-GravenhageFoto: Ruud Taal/Capital PhotosCopyright RVDCover Photograph P BorstPaul HuffCover Photograph AJM BernsLoek ZuijderduinOther Photographs and IllustrationsAudiovisual ServicesThe Netherlands Cancer InstituteAntoni van Leeuwenhoek HuisPlesmanlaan 1211066 CX AmsterdamThe NetherlandsSL BakkerSM DrentjeARM JagtAF JansC KoedijkJM LomeckySH OngER TragterCM WallePrinted by De Bussy Ellerman Harms