


Passive Articulated and Non-Articulated Ankle–Foot Orthoses for Gait Rehabilitation: A Narrative Review

1
Faculty of Mechanical Engineering, Institute of Mechanics, Otto Von Guericke University Magdeburg, Universitätsplatz 2, 39106 Magdeburg, Germany
2
Faculty of Mechanical Engineering and Informatics, University of Miskolc, 3515 Miskolc, Hungary
3
Faculty of Biomedical Engineering, Al-Andalus University for Medical Sciences, Tartous, Syria
*
Author to whom correspondence should be addressed.
Healthcare 2023, 11(7), 947; https://doi.org/10.3390/healthcare11070947
Submission received: 29 January 2023
/
Revised: 28 February 2023
/
Accepted: 10 March 2023
/
Published: 24 March 2023
(This article belongs to the Special Issue Advances in Musculoskeletal Rehabilitation and Therapy)
Abstract
:The aim of this work was to study the different types of passive articulated and non-articulated ankle–foot orthoses for gait rehabilitation in terms of working principles, control mechanisms, features, and limitations, along with the recent clinical trials on AFOs. An additional aim was to categorize them to help engineers and orthotists to develop novel designs based on this research. Based on selected keywords and their composition, a search was performed on the ISI Web of Knowledge, Google Scholar, Scopus, and PubMed databases from 1990 to 2022. Forty-two studies met the eligibility criteria, which highlighted the commonly used types and recent development of passive articulated and non-articulated ankle–foot orthoses for foot drop. Orthotists and engineers may benefit from the information obtained from this review article by enhancing their understanding of the challenges in developing an AFO that meets all the requirements in terms of ease of use, freedom of movement, and high performance at a relatively low cost.
1. Introduction
Human walking is typically conceptualized as the repetitive movement of the limbs and is a distinctive feature of human locomotion, with each individual possessing a distinct style of walking [1]. Humans with conditions that affect the hip, knee, or ankle bones, nerves, muscles, or joints may have difficulties in walking. This can lead to falls and injuries if the problems are not addressed [2]. Deficiencies in the nerves, muscles, bones, or spinal cord can also cause people to have trouble walking; these deficiencies are typically hereditary. People with gait disabilities can be aided by devices such as assistive footwear or rehabilitation. This process is referred to as gait rehabilitation and typically involves several stages [3,4]. Ankle-foot orthoses are used to support patients with abnormal gait; they are also used for rehabilitation [5]. These orthotics devices are typically referred to as ankle–foot orthoses or AFOs. Passive AFOs do not contain electrical boards, but they incorporate springs, dampers, or mechanisms that control the motion between the bone stubs in the foot [6]. Passive AFOs can be used in daily life, as they are compact in size [5].
There are different classifications for passive AFOs. For example, based on the relative motion between the shank parts of AFOs and the foot [7], they are also classified into two types: articulated and non-articulated (fixed) AFOs. While articulated AFOs are two-piece devices made of lightweight thermoplastics or carbon composites connected by joints, non-articulated AFOs are single pieces made of lightweight thermoformable materials, such as polyethylene or polypropylene. The shank parts of the AFO and the foot are connected by using springs, dampers, hinges, or flexion stops [8]. According to Alexander and Xing [9] other classifications are used to define AFO types. Solid AFO (SAFO) refers to solid plastic AFOs (PAFOs) or metallic AFOs [10], rigid AFOs [11,12], fixed AFOs [13], or solid AFOs [14,15,16,17,18]. Hinged AFO (HAFO) refers to hinged AFOs [15,16,17,19,20,21] or articulated AFOs [10,12]. Posterior -leaf-spring AFO (PLS) refers to posterior-leaf-spring and spring-type AFOs [17,22,23]. Floor-reaction AFO (FRO) refers to FROs [24,25] or ground-reaction AFOs [10,26]. Finally, carbon-fiber-spring AFOs (CFOs) have been described [13]. According to [27], the term passive AFO comprises only six categories: posterior-leaf-spring AFO, solid AFO, short-Leg AFO, dorsiflexion-assist AFO, plantar-flexion-stop AFO, and energy-return AFO. However, this paper studies the different types of passive articulated and non-articulated ankle–foot orthoses for gait rehabilitation in terms of working principles, control mechanisms, features, and limitations, along with the recent clinical trials on AFOs. In addition, this study categorizes AFOs to help engineers and orthotists to develop novel designs based on the literature.
2. Methods
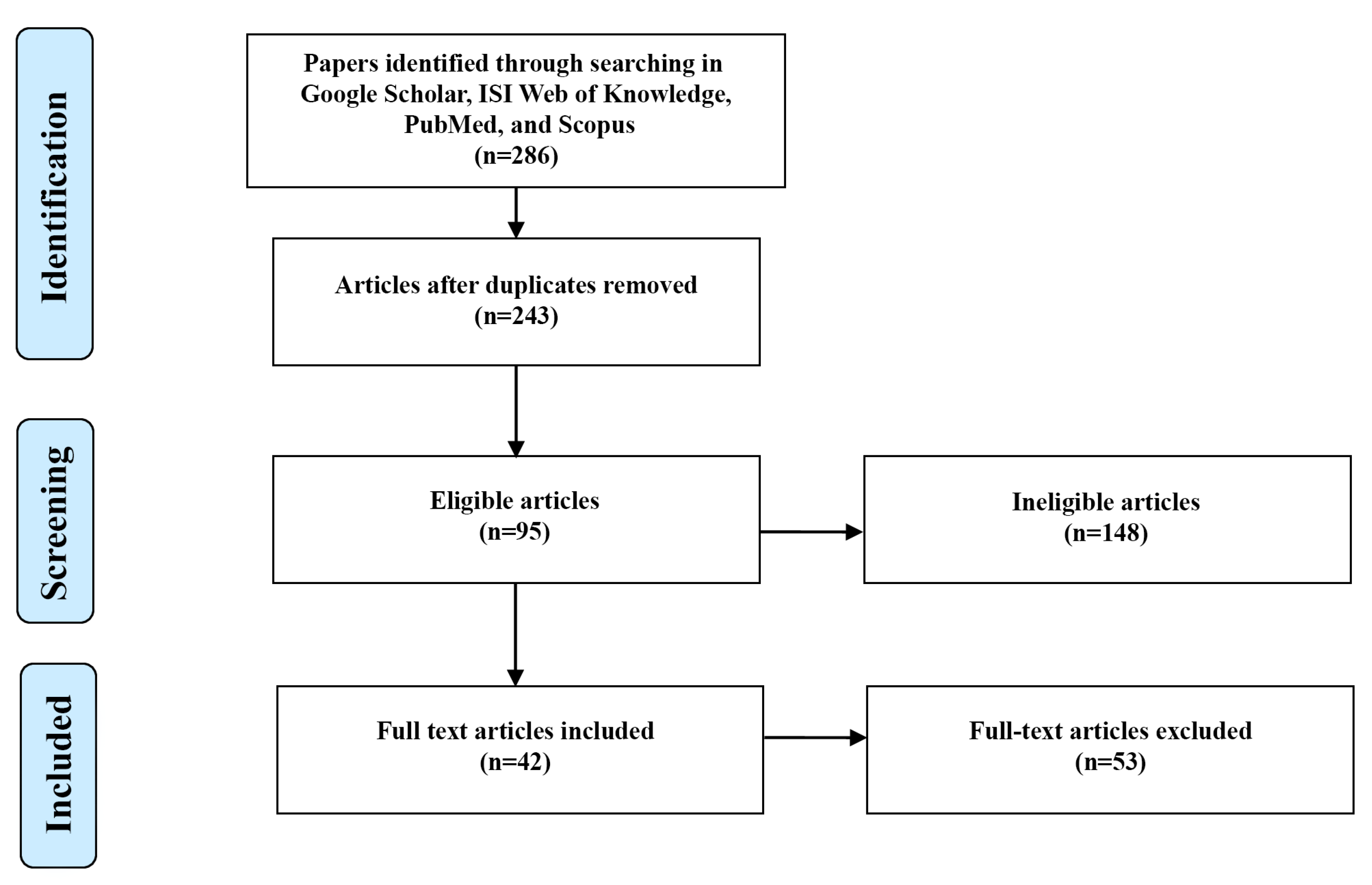
A literature search was conducted on Scopus, Google Scholar, ISI Web of Knowledge, and PubMed (from 1990 to 2022), as shown in Figure 1, and cited references from proper articles were thoroughly reviewed. The selected keywords in the search process were: “ankle-foot orthosis (AFO)”, “passive”, “articulated”, “non-articulated”, “solid AFO (SAFO)”, “posterior leaf spring AFO (PLS)”, “floor reaction AFO (FRO)”, “carbon fiber AFO (CFO)”, “short leg AFO”, “dorsiflexion assist AFO”, “plantarflexion stop AFO”, “energy return AFO”, “3D printed AFO”, and “SMA AFO”.
By adopting the comparative research equation, the main research question devised was: What are the comparative features and limitations of different types of passive articulated ankle–foot orthoses for gait rehabilitation? Inclusion criteria: Studies that investigated the use of passive articulated and non-articulated ankle–foot orthoses for gait rehabilitation, studies that compared different types of passive articulated and non-articulated ankle–foot orthoses, studies published in peer-reviewed journals between 1990 and 2022, and studies that were written in English or for which English translations were available. Exclusion criteria: Studies that investigated the effects of ankle–foot orthoses on athletic performance, rather than gait rehabilitation; studies that were based on animal models or in vitro testing, rather than human subjects; studies published before the year 1990, or not published in peer-reviewed journals; and studies that were not written in English or did not have English translations available.
3. Results and Discussion
3.1. Metal AFOs
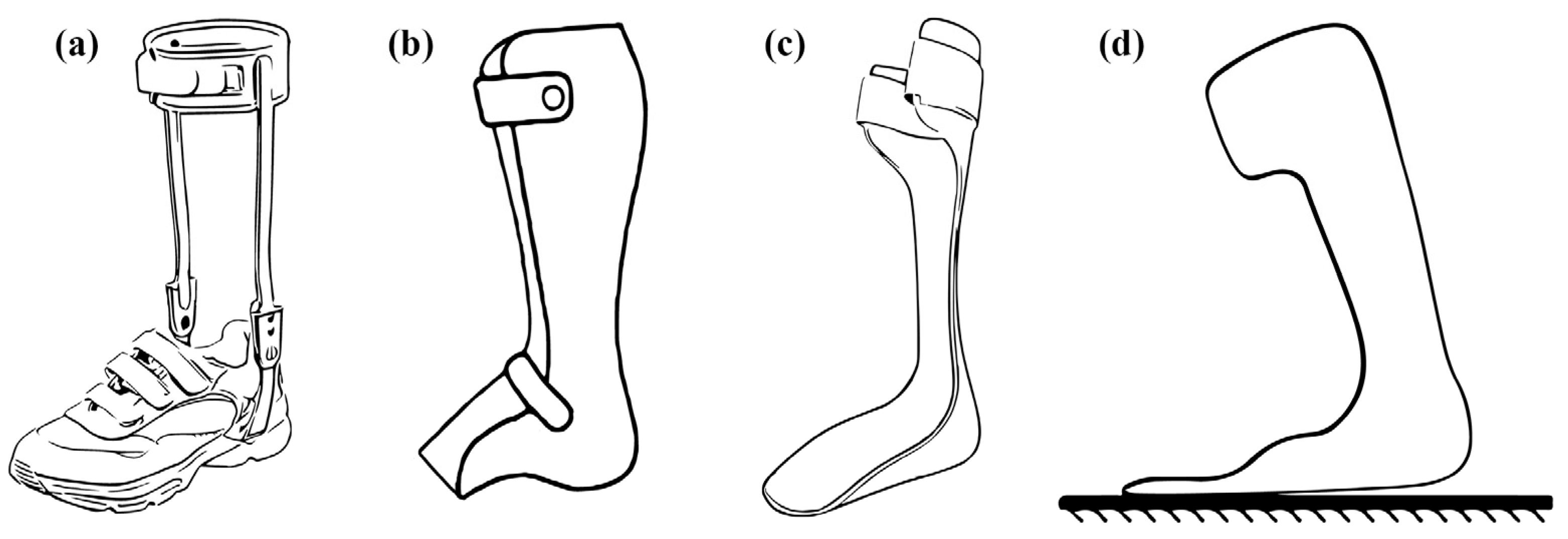
Metal AFOs (conventional AFOs) provide support for the foot, ankle, and lower leg [28]. They are used by patients with damaged nerves and muscles in their lower extremities [29]. These prostheses provide support through a calf strap, which creates direct skin-to-skin contact (Figure 2). Metal ankle supports connect to the shoes via bars that do not touch the wearer’s skin; they reduce pressure on the soft tissue in the ankle by distributing weight across several ankle fins. However, their heavy weight and cumbersome nature are among their major drawbacks. Therefore, users currently find it practical to replace these metal supports with a more energy-efficient alternative: plastic AFOs [30]. Berkelman et al. [31] presented a four-bar mechanism used in an ankle–foot-orthosis design. This design had link joints that were pivoted with aluminum bars.
A portion of this design involves providing an additional force to aid in lifting the foot during the swing phase. The concept behind this device is that the knee and ankle move together to connect and generate this assistive force. A curved bar attaches at the calf and foot, along with a link attachment that connects it to the back of the thigh. When the knee is flexed at 5 to 20 degrees, the thigh makes contact with the bar to generate a lifting action through the four-bar linkage motion at the ankle. A knee that is not bent provides additional torque to the ankle when it is pushed into a flexed position. However, keeping the knee straight prevents this force from being generated. Instead, increased torque at the ankle occurs through knee flexion. The main drawbacks of this prototype include its bulky appearance, lack of toe-drag assistance, uncomfortable weight distribution, and lack of foot-slap prevention. Additional adjustments can be made to the timing and amount of assistance by changing the spring stiffness, the lengths of the links, and the point of attachment. In some cases, individual users can adjust these factors. Ghosh et al. [32,33] introduced an AFO containing a six-bar mechanical linkage. The study also established 11 task points (standard data) for the synthesis of toe movement during normal walking. Upon evaluation, it was found that there was a ±10 degree of discrepancy between the simulation data of the device and the standard data of a healthy individual. A gait analysis revealed certain limitations in this AFO, including a ±12 percent error in the knee and ankle angles and one missing task point for the toe movement out of the eleven task points defined for normal walking.
3.2. Plastic AFOs (PAFOs)
Plastic AFOs (PAFOs) are mainly made of thermoplastics, such as polyethylene or polypropylene, and are among the most widely used solid orthoses in clinical practice due to their numerous advantages, such as their relatively low cost, the ease with which they can be cleaned, good aesthetics, and easy desorption [34,35]. Plastic AFOs (Figure 2b) can be utilized to limit motion in the sagittal plane of the ankle during stance and swing phases, as well as to provide medial and lateral stability during different stances and anterior entry, with the use of support strapping at the proximal end and, potentially, at the ankle and forefoot. The underlying mechanism of these devices is the provision of the force necessary to generate an ankle plantar-flexor moment, thus enabling weight bearing on the distal aspect of the foot.
The stiffness of PAFOs depends on the shape of the flexible region, material properties, and thickness. However, their fabrication is carried out by the trial-and-error method, resulting in a negative effect on the knee during walking. If these PAFOs are overly stiff, they may delay the loading response, and the knee can become more flexed. If the PAFOs are less stiff, they affect the patient through the excessive extension of their knee. Therefore, PAFOs should be designed to provide minimum ankle stiffness [36].
3.3. Posterior-Leaf-Spring AFOs (PLS AFOs)
Posterior-leaf-spring AFOs (PLS AFOs) are solid AFOs (SAFOs), but, unlike conventional AFOS [37], they have a characteristic trim line located behind the ankle and leaf-shaped corrugation near the ankle (Figure 2c). The leaf-like creases are intended to strengthen the part of the ankle with the greatest amount of movement and repeated loadings. In addition, they act as a spring in the ankle, which allows slight dorsiflexion in the mid and terminal stances, and this elasticity can also marginally assist the push-off function in the terminal stance [38].
Furthermore, PLS AFOs can be applied to limit excessive equinus during swinging, thinner ankle coverage, which allows sagittal-plane motion in dorsiflexion during weight-bearing, a trim line posterior to the medial and lateral malleolus, and support strapping at the proximal tibia. In addition, they increase control over the instability of the ankle, as the ankle trim line extends further to the front of the ankle joint. However, PLS AFOs do not contribute significantly to ankle stability, as the trim line is behind the ankle. Thus, PLS AFOs are limited in their control of the varus/valgus [38,39].
3.4. Ground (Floor)-Reaction AFOs (GRAFOs or FRAFOs)
Ground- or floor-reaction ankle–foot orthoses (GRAFOs or FRAFOs) are types of custom-fabricated, molded plastic, AFO capable of tri-planar control of the foot/ankle complex [26]. Ground-reaction ankle–foot orthoses (Figure 2d) can be applied to provide ankle support to reduce ankle dorsiflexion and excessive knee flexion in stance via plantar-flexion knee-extension couple, rear or anterior entry, and large proximal tibial strapping, to support greater forces on the anterior tibia. Furthermore, they can be used in cases of adult-acquired flatfoot, posterior tibial tendon dysfunction (PTTD), cerebral palsy, brain injuries, Achilles tendonitis, osteoarthritis, spina bifida, spinal cord injuries, and post-polio paralysis.
Furthermore, SAFOs and GRAFOs are types of AFO that both apply a corrective internal plantar-flexion momentum to the ankle. Both apply this correction by producing an ankle-dorsiflexion moment through similar mechanical means [40]. In functional terms, they are similar. The GRAFOs use an anterior tibial shell to connect to the tibia in order to prevent the dorsiflexion of the ankle. Other GRAFO factors include using particular values, such as resistance to ankle flexion. The design of AFOs, despite significant variation, has only two basic types. One is the tibial shell design, and the other involves the use of a neutral angle, which alleviates the effects of knee flexion. It has been shown that GRAFO designs do not outperform SAFO designs in terms of reducing excessive knee flexion for individuals with certain disorders, such as CP. Instead, it has been shown that SAFOs are more effective at reducing knee flexion for individuals with CP, and that they have a significant effect on improving crouch gait for people with disabilities.
3.5. Type I, Type II, and DACS AFOs
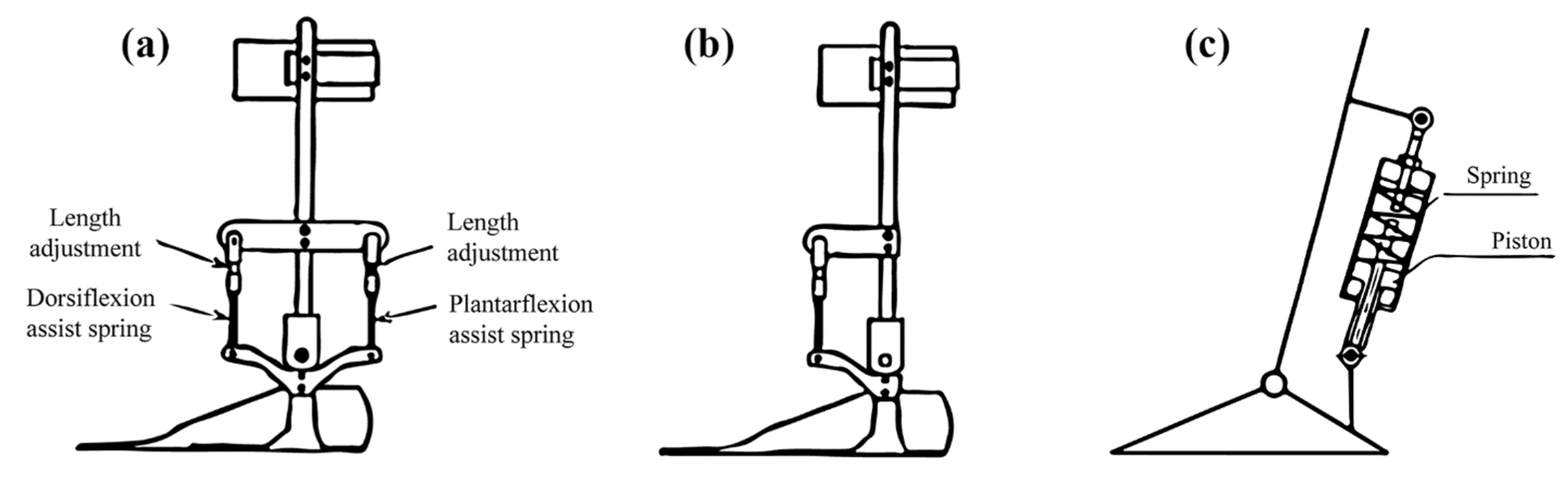
Yamamoto et al. [41] introduced AFOs for individuals with hemiplegia, in which the level of assistive moments and the initial angle of the ankle can be adjusted easily. The design of these AFOs, referred to as Type 1 AFOs, included both dorsiflexion- and plantar-flexion-assistance moments. The foot component of the AFO was constructed by plastic material connected by two aluminum uprights with Klenzak joints and featured two springs, one of which was located on the anterior and another on the posterior side of the ankle joint (Figure 3a). In contrast, the anterior spring generates the dorsiflexion-assistance moment, while the posterior spring generates the plantar-flexion-assistance moment [42]. These assistance moments and the initial angle of the ankle can be separately adjusted by altering the lengths of the springs. As a result of their gait analysis, the authors determined that the presence of the posterior spring caused discomfort for hemiplegic patients and, therefore, a plantar-flexion assistance moment was deemed unnecessary for this patient population. Consequently, Type 2 AFOs (Figure 3b) were developed, which do not incorporate a posterior spring. This design allows greater freedom of movement in the ankle during dorsiflexion. A gait analysis revealed that this design leads to a reduction in the knee-flexion moment and the absence of quick plantar flexion in the ankle [41,42,43].
To provide assistance to people with DACS AFOs, a spring-loaded mechanism was added to the device’s shank. Due to these innovations, DACS AFOs were able to help people with restricted mobility. These AFOs contained two pieces: a plastic foot and an aluminum shank connected by an ankle (Figure 3c). By lengthening the assistance device, the DACS AFO’s ankle angle could be altered [6]. The application of a piston to compress the spring in the AFO design resulted in the generation of an assistance moment that was proportional to the plantar-flexion angle when the ankle rotated towards plantar flexion. However, when the ankle rotated in the opposite direction, towards dorsiflexion, the foot component of the AFO was able to rotate freely due to the minimal friction in the slider component and, thus, did not generate a plantar-flexion-assistance moment. The implementation of this DACS AFO design was found to enhance walking speed through the reduction in knee hypertension and the improvement in delayed progression in the hip joint. However, a drawback of this design was the utilization of large spring units, which contributed to its bulky size [6].
3.6. Plantar-Flexion-Stop AFOs (AFO-PSs)
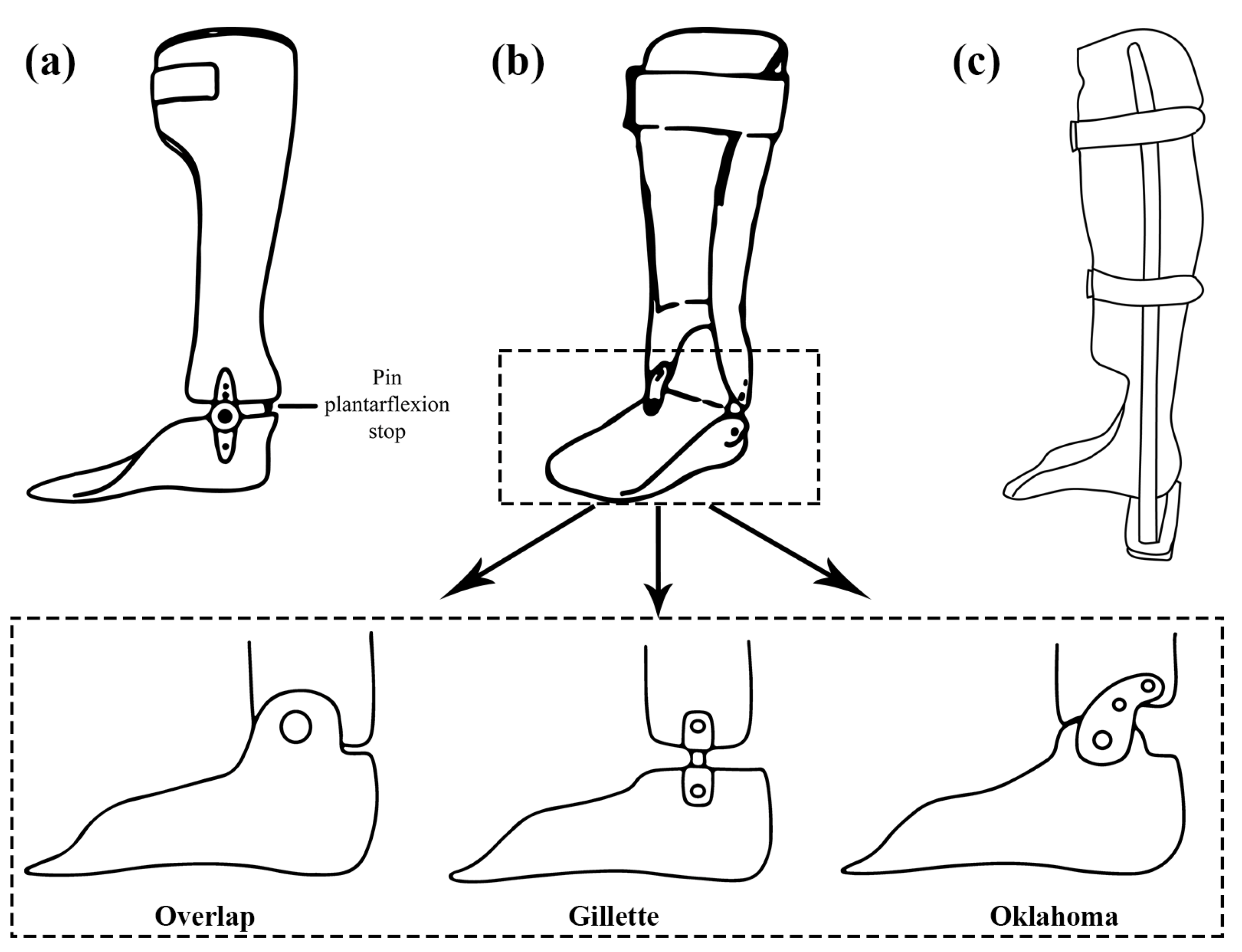
An investigation was conducted to determine the impact of the plantar-flexion resistance of ankle–foot orthoses (AFO-PS) on the gait of stroke patients in the subacute phase, utilizing an AFO with a plantar-flexion stop [44]. The use of a plantar-flexion stop in the design of an ankle–foot orthosis results in increased dorsiflexion and knee flexion during the early stance phase of gait, which may lead to an increase in hip flexion. The ankle of the AFO-PS does not move into plantar flexion (Figure 4a). During gait with the AFO-PS, patients demonstrated a greater forward inclination of the pelvis upon initial contact compared to walking with shoes without an AFO. The use of an AFO-PS leads to a flexed alignment of the lower limb and a forward tilt of the pelvis [45]. The AFO-PS has been shown to improve dorsiflexion during the swing and early stance phases; however, it also results in a greater external knee-flexion moment during the loading phase compared to walking with shoes only and able-bodied control participants [46]. This increased acceleration into knee flexion may reduce knee hyperextension, but it can also cause instability in individuals with quadriceps weakness [45].
3.7. Hinged AFOs (HAFOs)
Ankle–foot orthoses (AFOs) with hinges, commonly referred to as hinged AFOs (HAFOs), are utilized when some level of ankle mobility is desired while certain limitations are still necessary [38]. The most prevalent HAFO designs include the overlap, Gillette, and Oklahoma joints (Figure 4b). The overlap joint restricts plantar flexion by interlocking the foot and shank shells, and it is secured by means of a rivet. The Gillette joint, on the other hand, links the shank shell to the foot shell as a separate entity, enabling movement in both the plantar-flexion and dorsiflexion directions. The Oklahoma joint, similar to the Gillette joint, establishes a connection between the shank shell and the foot shell as separate components, thus creating a gap between the shank shell and the posterior aspect of the foot shell, thereby allowing plantar flexion until the two parts make contact [38]. However, plantar flexion can also be fully restricted by positioning the shells at a 90-degree angle without any intervening space [38].
Hinged ankle–foot orthoses can be utilized to incorporate an articulating ankle joint, enabling dorsiflexion in the sagittal plane during stance while prohibiting plantar flexion during swing, as well as featuring support straps at the proximal tibia and, occasionally, at the ankle and forefoot [47]. These HAFOs may be equipped with a posterior strap to restrict the range of dorsiflexion [48]. It is important to note that they should not be employed by individuals with significant mediolateral instability of the ankle and are more appropriate for patients with adequate control over their knee joints [16,49,50].
3.8. Patellar-Tendon-Bearing AFO (PTB-AFO)
Patellar-tendon-bearing ankle–foot orthoses (PTB AFOs) differ from other types of plantar-ankle orthosis in that they include an additional anterior shell to assist in weight bearing via the patellar tendon [51]. This results in a reduction in the weight on the ankle, heel, and sole, potentially leading to a decrease in pain in these regions (Figure 4c) [51,52]. These orthoses are employed in situations that necessitate a reduction in pressure on the foot, such ulcers, calcanectomy, plantar skin grafts, severe ankle trauma/foot injuries, and fractures [38]. In essence, the brace was designed to shift the weight-bearing loads from the tibia, fibula, and foot bones to the lateral uprights [51]. The application of PTB AFOs can decrease the overall maximum plantar pressure on the foot; however, it may result in an increase in localized plantar pressure in the forefoot [53]. An excessive elevation of the heel reduces the contact area, thereby exacerbating the focal pressure on the forefoot. In general, a combination of the maximization of heel clearance and the restriction of ankle-joint movement appears to be the most effective means of reducing plantar pressure [51].
3.9. AFOs with Oil Dampers (AFO-ODs)
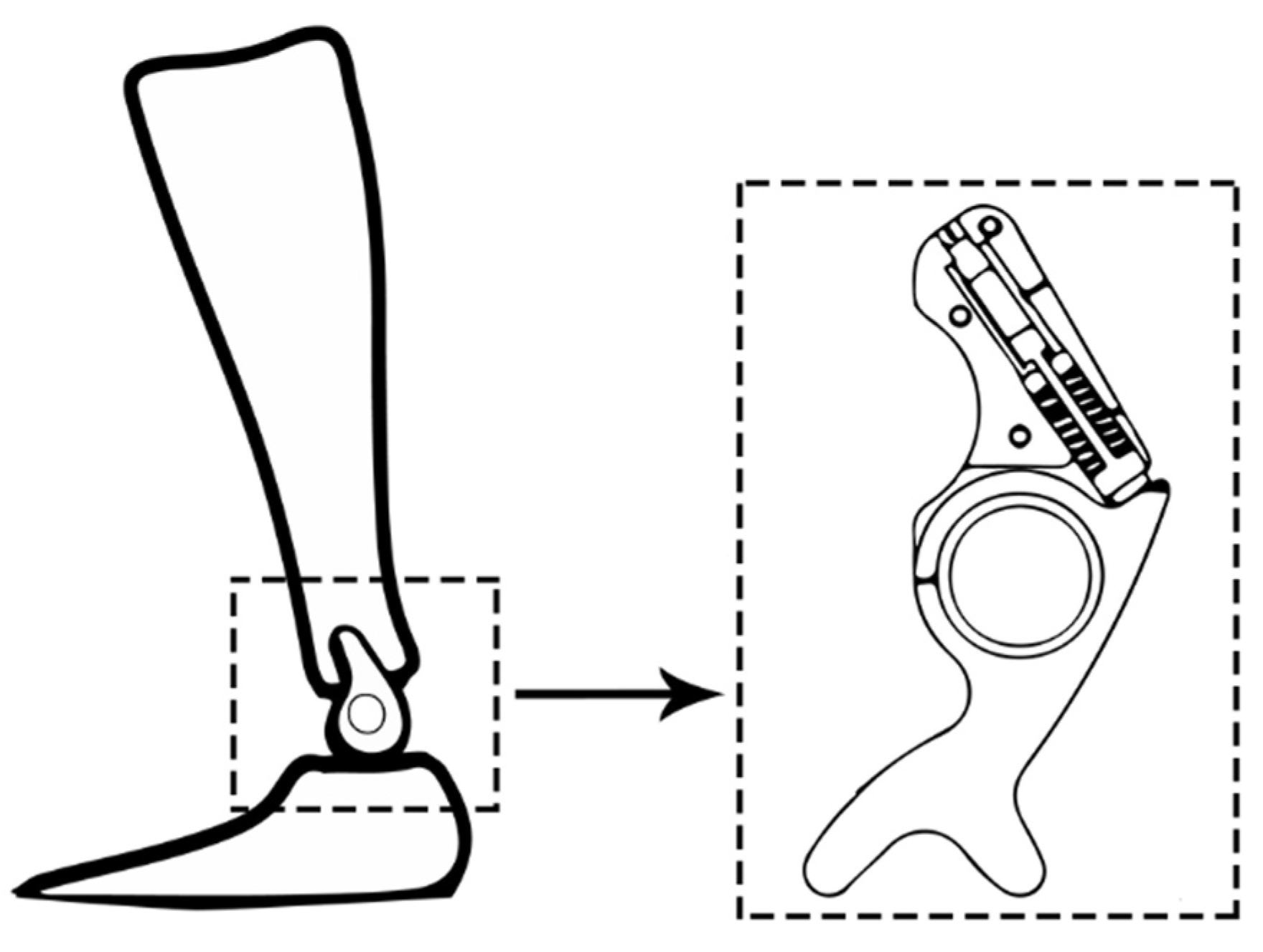
The ankle–foot orthosis with oil damper (AFO-OD) was developed to aid heel-rocker function [54,55]. It features a functional unit (the oil damper) positioned on the lateral side of the ankle joint [56]. This unit contains a compact hydraulic cylinder, which can offer resistance against plantar flexion as required (Figure 5). During initial contact, when the ankle joint undergoes plantar flexion, the piston rod is pushed upward into the cylinder, which is filled with oil, resulting in resistance. Subsequently, upon the completion of plantar-flexion motion, a spring returns the piston to its initial position. The resistance of the oil damper can be easily modified by adjusting a screw [57].
3.10. Pneumatic Harvested AFOs (PhAFOs)
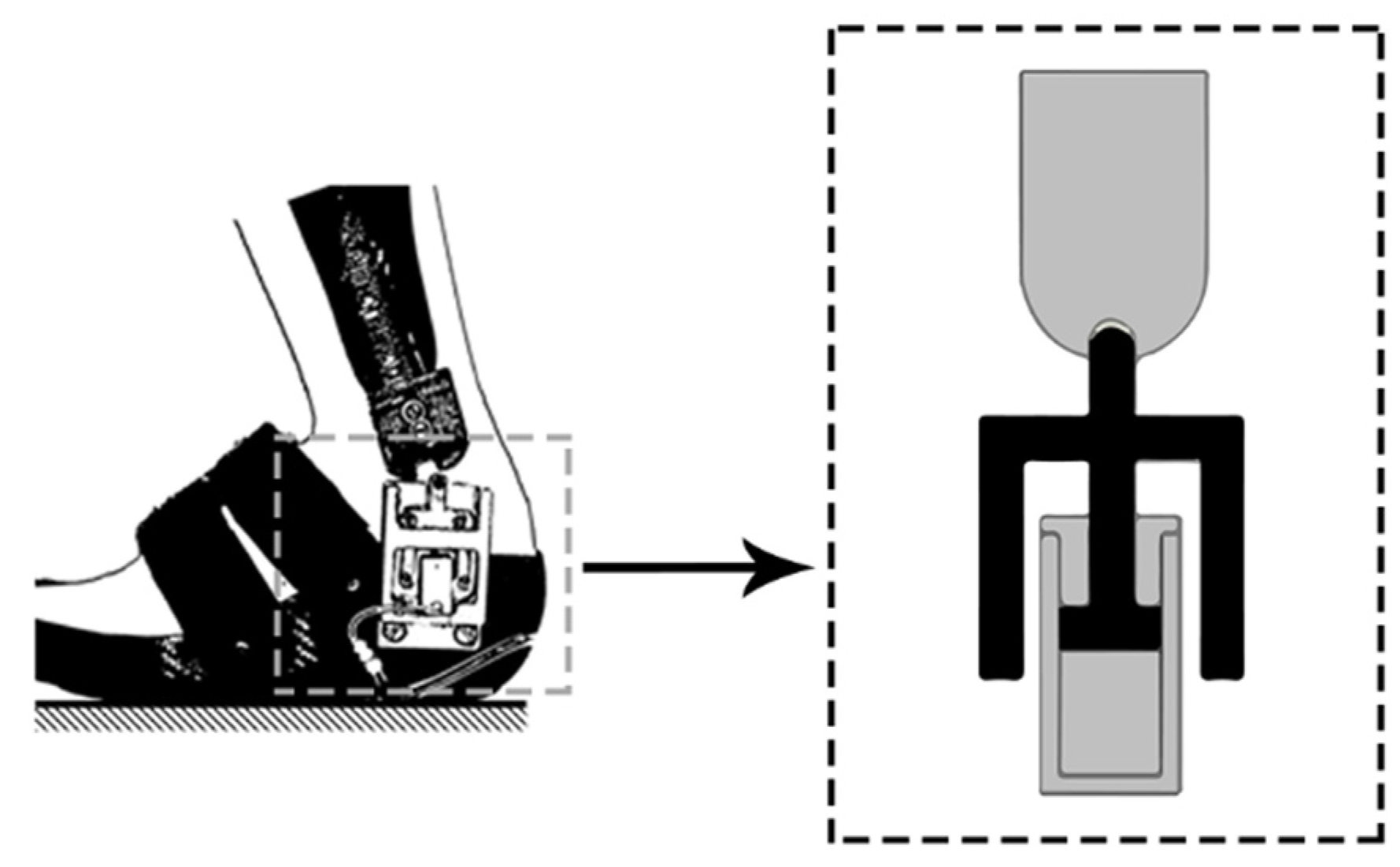
Chin et al. [58,59] presented the concept of pneumatic harvested ankle–foot orthoses (PhAFOs), which are composed of two components fabricated from carbon-composite laminate: the tibial upright and the footplate. The sole of the device includes a bellow pump, an actuator, two check valves, a pressure-release valve, and a cam-lock mechanism attached on the lateral side of the PhAFO (Figure 6). The actuator in the PhAFO is composed of a roller follower, a linear cylinder, and a guide rail. During heel contact, compressed air is expelled from the cylinder into the atmosphere via the release valve.
The operation of the PhAFO involved a spring in the cylinder returning to its initial position, which then unlocked the cam and facilitated plantar flexion of the foot. During the stance phase, the bellow pump compressed and the release valve closed, leading to the extension of the roller follower, allowing free dorsiflexion due to the cam’s design. The cam mechanism, activated by the roller follower, ensured the absence of toe drag during the swing phase, as demonstrated in a gait-analysis study performed on a healthy individual wearing a shoe on one foot and a PhAFO on the other. The results of the kinetic and kinematic data analysis indicated that the toe had adequate clearance during the swing phase, although excessive dorsiflexion was observed during the mid-swing [42].
3.11. Short-Leg AFOs
The utilization of this particular type of ankle–foot orthosis is simple and convenient in terms of fitting it into footwear, and it is comparatively lightweight. Short-leg AFOs provide remarkable control over the foot and are considered to be an appropriate option for individuals suffering from flat feet. These devices maintain the foot in a perpendicular orientation with respect to the leg and, additionally, they can effectively counter the inward rotation of the foot, which is frequently observed in stroke patients with drop-foot [27]. One drawback of the fixed-hinge AFO prescribed for drop-foot is that it restricts plantar flexion and dorsiflexion, leading to an unnatural gait compared to other AFOs. Additionally, its shorter length makes it less suitable for taller individuals [27].
3.12. Energy-Return AFOs
The implementation of this type of ankle–foot orthosis, characterized by the incorporation of natural flexibility for enhancing dorsiflexion, has proven to be an effective solution. This AFO, often made from lightweight carbon-graphite materials, offers exceptional control without adding substantial weight. Clinical studies have demonstrated that the utilization of this AFO in individuals with hemiparetic stroke resulted in a 20% increase in walking speed and a 12% reduction in the energy cost per meter, as measured by oxygen consumption, when compared to unassisted walking [60]. In a separate study [61], the utilization of this type of AFO was shown to furnish support throughout the entire stance phase and enhance energy return during the third rocker phase of gait in a population consisting mainly of individuals with spina bifida. Furthermore, the spring element in the AFO contributed to a gait that was more in line with physiological principles.
A study published in 2008 [62] found that for individuals with spina bifida, the utilization of an energy-return ankle–foot orthosis resulted in more physiological ankle and knee kinematics and subsequently demonstrated a functional improvement in comparison to a more conventional orthotic device. However, the study also found that the kinetics and kinematics during the stance phase were significantly influenced by the alignment of the orthosis with the patients’ footwear. While these types of AFO possess numerous benefits, they may not be suitable for all individuals. Individuals with very large calf muscles or those who possess a naturally long stride, such as tall individuals, may encounter difficulties while utilizing these devices. Additionally, patients with spasticity or tight Achilles tendons may not find these AFOs to be optimal for their condition [63].
3.13. Three-Dimensionally Printed AFOs
Recently, there have been several attempts to produce an ankle–foot orthosis through the use of three-dimensional (3D) printing technology. These 3D-printed AFOs have the advantage of being easier to manufacture, with less skill and effort required, as well as being more easily replicable, compared to traditionally manufactured orthoses made through the molding of thermoplastic materials [64]. The repetition of AFO production is facilitated as the 3D-modeling file of the design is retained once. Furthermore, if an automated software program for orthotic design is established utilizing the pre-programmed orthotic-template design, the production of the AFO is simplified and can be personalized by patients themselves [64].
In recent years, several studies have been conducted to assess the viability of using 3D-printing technology to produce AFOs. These studies have focused on determining the functional properties of AFOs based on physical features, such as bending or rotational stiffness, and other material characteristics. Out of these studies, two replicated the design of a posterior-leaf-spring AFO [65,66], one replicated the design characteristics of a prefabricated carbon-fiber AFO [67], and six developed novel AFO designs [64,68,69,70,71,72]. The innovative concepts comprised the elaboration of a computer-aided, modeled, parameterized ankle–foot orthosis [68,69].
One investigation resulted in the production of a segmented ankle–foot orthosis, composed of 3D-printed foot and calf components, as well as a central, interchangeable carbon-fiber spring [71]. Another study incorporated a 3D-printed component with gas springs and commercially available bearings to yield an AFO with adjustable stiffness [70]. Other design configurations comprised ankle–foot orthoses that incorporated 3D-printing technology in the creation of 3-mm calf and foot sections connected by two carbon-fiber rods [72]. Additionally, other 3D-printed devices were developed for the support of the ankle and foot and were secured using laces [73].
The only investigation that did not result in the creation of a dynamic passive ankle–foot orthosis utilized 3D printing to fabricate a solid AFO, although no evaluation tests were conducted on this device [74]. A patient-satisfaction survey was conducted in another study [64] to compare the usage of a traditional AFO with that of a 3D-printed AFO. In regards to weight and usability, findings indicate that participants express a higher degree of satisfaction with 3D-printed AFOs. The conventional AFO was deemed challenging to wear due to its thickness [75]. Furthermore, studies have demonstrated that 3D-printed ankle–foot orthoses provide greater comfort during use [66] and elicit positive feedback regarding gait patterns following one hour of walking [68].
3.14. SMA-Based AFOs
Shape-memory alloys (SMAs) have been suggested as a potential solution to the issues associated with conventional ankle–foot orthoses, which are typically characterized by their weight, bulkiness, and limited functionality. The superiority of SMA-based AFOs is demonstrated by their lighter weight and more streamlined design, due to their higher power-to-weight ratio [76]. A study conducted by a researcher incorporated the use of superelastic wires and the installation of 14 plastic pulleys using screws and spacers [77].
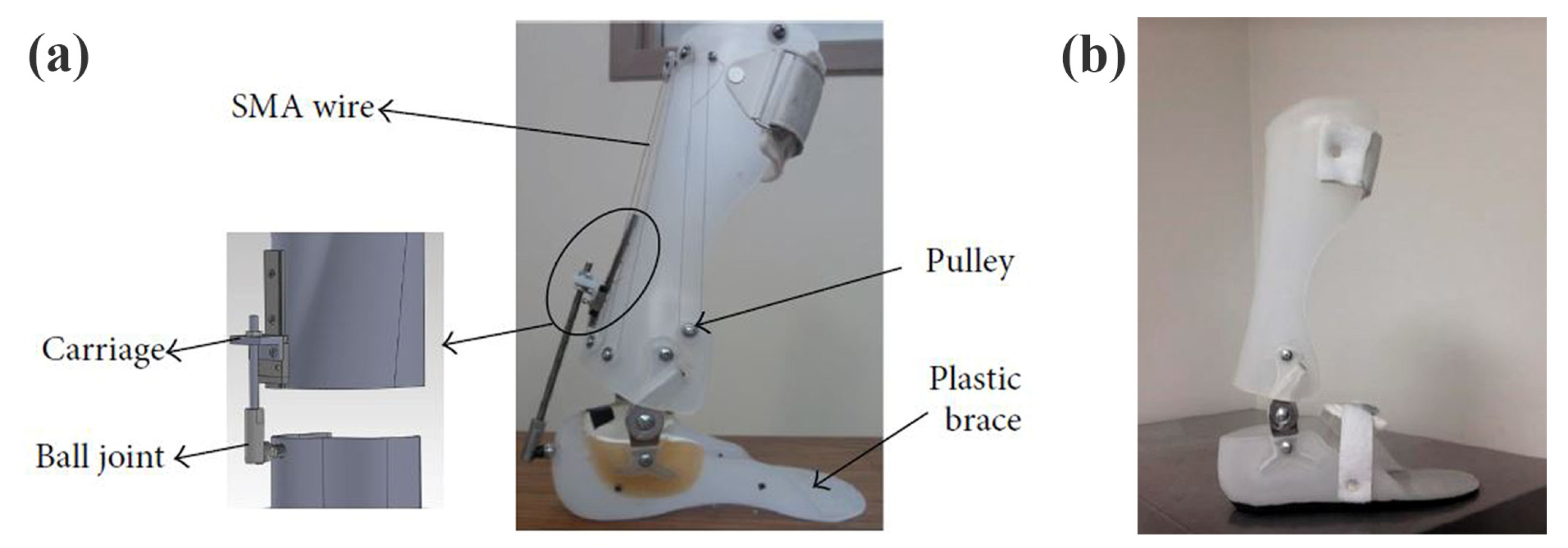
Another study employed a different approach, wherein the superelastic wires were affixed to the brace at one end and connected to a carriage at the other, as illustrated in Figure 7 [78]. Additionally, two novel adaptive solutions for the AFO mechanism based on SMA technology were proposed by other researchers, with the aim of modifying the stiffness in bending and torsion [79]. The first design concept involves altering the inner diameter and length of a superelastic rod in response to different controlled axial loads, thereby enabling the provision of variable torsional stiffness. The second design concept for SMA-based adaptive solutions for the AFO mechanism involved controlling the bending stiffness by adjusting the position of a slider in relation to the active length of a superelastic hinge. Furthermore, another study produced an AFO device that encompasses two superelastic SMA springs, a two-part brace, and two hinges, with an internal hole for mounting the springs, as illustrated in Figure 7 [80].
The stiffness profile of the ankle was found to resemble that of natural walking when NiTi springs were employed, and the shape-memory alloy (SMA) AFOs were capable of fulfilling the torque-angle specifications of the ankle-support device. Nonetheless, SMA-based AFOs present several limitations, including a low efficiency, of approximately 10%, and a limited bandwidth. Furthermore, the deflection of the SMA element occurs within a narrow temperature range, resulting in challenges in regulating partial contractions [81]. Table 1 presents a detailed summary of the passive articulated and non-articulated ankle–foot-orthosis types in terms of the control element, moment mechanism, features, and limitations.
3.15. Clinical Trials on AFOs
Kluding et al. [82] conducted a study examining the utility of ankle–foot orthoses (AFOs), using 197 stroke patients walking at normal and fast speeds. The study revealed that significant improvements in comfortable and fast walking speeds (0.18 m/s) were observed [82]. In a separate investigation, De Paula et al. [83] explored the impact of various types of AFO on the mobility and dynamic balance of 50 stroke patients. The study demonstrated that the use of AFOs led to better mobility and improved balance, as evaluated through the Timed Up and Go (TUG) test and Tinetti’s mobility scale.
Schwarze et al. [84] conducted a comparative study to evaluate the efficacy of laterally wedged insoles (LWI) and ankle–foot orthoses (AFOs) in 39 patients with medial-knee osteoarthritis. The maximum values of the knee-adduction moment (eKAM) and the Oxford Knee Score (OKS) were used as indices to assess the outcomes. The results demonstrated that both interventions led to significant improvements in the analyzed indices. Additionally, the use of AFO led to a substantial reduction in the maximum eKAM value, of 18%.
Bashir et al. [85] conducted a qualitative study aimed at exploring the perceptions of 15 male patients with peripheral artery disease regarding the use of ankle–foot orthoses (AFOs). The participants were divided into two groups: those who completed the AFO intervention and those who withdrew from it. The analysis of the semi-structured interviews revealed that the group that withdrew from the AFO intervention reported higher levels of physical discomfort. Conversely, the group that completed the intervention reported positive aspects, such as ease of standing and walking, as well as a reduction in pain.
In a study conducted by Miller et al. [86], the clinical and cost effectiveness of ankle–foot orthoses (AFOs) and functional electrical stimulation (FES) were compared over a period of 12 months in 85 individuals with multiple sclerosis and foot drop. The assessment of gait included various indices, such as the oxygen cost of walking, the Multiple Sclerosis Impact Scale-29, and the Modified Fatigue Impact Scale. The study findings revealed that the use of AFOs led to faster walking speeds in patients after 12 months, with significant improvements in various gait-assessment indices.
Raposo et al. [87] conducted a systematic review to assess the impact of ankle–foot orthoses (AFOs) on the gait of children diagnosed with spastic bilateral cerebral palsy (CP), using kinetic, kinematic, and functional outcomes. The study population consisted of 285 children with spastic bilateral CP, and the effects of five different types of AFO (solid, dynamic, hinged, ground-reaction, and posterior-leaf-spring) were analyzed. The analysis of the data showed significant differences in various gait parameters, such as walking speed, stride length, cadence, range of motion, ground-force reaction, joint moment, and functional score, when ankle–foot orthoses (AFOs) were used. This suggests that the utilization of AFOs by children diagnosed with spastic bilateral cerebral palsy (CP) may mitigate the effects of pathological gait, leading to consistent improvements in certain kinematic, kinetic, and spatial–temporal parameters.
Yeh et al. [88] developed an innovative energy-storage 3D-printed ankle–foot orthosis (ESP-AFO) and examined its impact on gait improvement in 12 stroke patients. The gait analysis was conducted using a motion-capture system, and the participants’ satisfaction and fatigue were also evaluated. The study findings revealed that the use of the ESP-AFOs led to a significant increase in bilateral gait velocity and stride length. Additionally, the ESP-AFO was shown to reverse drop-foot during the swing phase and to generate a greater ankle moment in the terminal stance, indicating that the newly developed custom-made ESP-AFO resulted in enhanced gait performance and higher satisfaction levels.
Fatone et al. [89] conducted a literature review to identify instruments utilized for evaluating the experience and outcomes of custom ankle–foot orthosis (AFO) care in individuals diagnosed with neurologic and traumatic conditions. The majority of the instruments utilized in the assessment of mobility included the 10-m-walk test, 6-min-walk test, Berg Balance Scale, Timed Up and Go, and Rivermead Mobility Index. These instruments demonstrated satisfactory reliability and validity and were regarded as viable options for developing quality measures pertaining to custom ankle–foot orthosis (AFO) care.
Moll et al. [90] conducted a study to evaluate the levels of activity and participation in daily life of 25 children diagnosed with cerebral palsy (CP), after the utilization of functional electrical stimulation (FES) and an ankle–foot orthosis (AFO). Each participant underwent twelve weeks of conventional treatment (AFO/adapted shoes), followed by 12 weeks of FES treatment, separated by a six-week washout phase. The researchers anticipated improvements in the level of bodily functions and structures, as well as activities, such as ankle kinematics and kinetics, which were measured using 3D gait analysis.
4. Conclusions
This literature review examined various currently available designs and types of passive ankle–foot orthosis (AFO). However, it was found that designing an AFO that is suitable for every patient remains a challenge, as the nature of disability varies among patients. Additionally, there is an ongoing challenge to develop an AFO that strikes a balance between ease of use, freedom of movement, high performance, and relatively low cost. Future studies should focus on identifying gaps in current knowledge and exploring emerging technologies to improve the efficacy, comfort, and cost-effectiveness of AFOs for individuals with gait disorders.
Author Contributions
Conceptualization, investigation, and writing—original draft: H.M.N. and M.A.D.; conceptualization, supervision, and writing—review and editing: S.S. and D.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Silva, R.; Veloso, A.; Alves, N.; Fernandes, C.; Morouço, P. A Review of Additive Manufacturing Studies for Producing Customized Ankle-Foot Orthoses. Bioengineering 2022, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.J.; Ryu, J.H. Neuromuscular Problems in Foot and Ankle: Evaluation and Workup. Foot Ankle Clin. 2014, 19, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Carrera, I.; Moreno, H.A.; Sierra, S.; Campos, A.; Munera, M.; Cifuentes, C.A. Technologies for Therapy and Assistance of Lower Limb Disabilities: Sit to Stand and Walking. In Exoskeleton Robots for Rehabilitation and Healthcare Devices; Springer: Singapore, 2020. [Google Scholar]
- Zhou, C.; Yang, Z.; Li, K.; Ye, X. Research and Development of Ankle-Foot Orthoses: A Review. Sensors 2022, 22, 6596. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Zi, B.; Zeng, Y.; Qin, L.; Liao, W.-H. Ankle-Foot Orthoses for Rehabilitation and Reducing Metabolic Cost of Walking: Possibilities and Challenges. Mechatronics 2018, 53, 241–250. [Google Scholar] [CrossRef]
- Kubasad, P.R.; Todeti, S.R.; Kamat, Y.D. A Review on Designs of Various Ankle Foot Orthosis (AFO) Used to Treat Drop Foot Disease. In Mechanism and Machine Science; Springer: Singapore, 2021. [Google Scholar]
- Kobayashi, T.; Leung, A.K.; Akazawa, Y.; Hutchins, S.W. Correlations between Berg Balance Scale and Gait Speed in Individuals with Stroke Wearing Ankle-Foot Orthoses-a Pilot Study. Disabil. Rehabil. Assist. Technol. 2016, 11, 219–222. [Google Scholar] [CrossRef]
- Saeedi, H.; Pourhoseingholi, E. Comparison the Effect of Kinetic Parameters of Innovative Storing-Restoring Hybrid Passive (Comfort Gait) Ankle-Foot Orthosis (AFO) with Posterior Leaf Spring AFO in Drop-Foot Patients: A Prospective Cohort Study: A Prospective Cohort Study. Curr. Orthop. Pract. 2020, 31, 437–441. [Google Scholar] [CrossRef]
- Alexander, M.A.; Xing, Y.; Bhagia, S. Lower Limb Orthotics; Webmd LLC.: New York, NY, USA, 2007. [Google Scholar]
- Caliskan Uckun, A.; Celik, C.; Ucan, H.; Ordu Gokkaya, N.K. Comparison of Effects of Lower Extremity Orthoses on Energy Expenditure in Patients with Cerebral Palsy. Dev. Neurorehabil. 2014, 17, 388–392. [Google Scholar] [CrossRef]
- Jagadamma, K.C.; Coutts, F.J.; Mercer, T.H.; Herman, J.; Yirrell, J.; Forbes, L.; Van Der Linden, M.L. Optimising the Effects of Rigid Ankle Foot Orthoses on the Gait of Children with Cerebral Palsy (CP)-an Exploratory Trial. Disabil. Rehabil. Assist. Technol. 2015, 10, 445–451. [Google Scholar] [CrossRef]
- Hayek, S.; Hemo, Y.; Chamis, S.; Bat, R.; Segev, E.; Wientroub, S.; Yzhar, Z. The Effect of Community-Prescribed Ankle-Foot Orthoses on Gait Parameters in Children with Spastic Cerebral Palsy. J. Child. Orthop. 2007, 1, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Butler, P.B.; Farmer, S.E.; Stewart, C.; Jones, P.W.; Forward, M. The Effect of Fixed Ankle Foot Orthoses in Children with Cerebral Palsy. Disabil. Rehabil. Assist. Technol. 2007, 2, 51–58. [Google Scholar] [CrossRef]
- Brehm, M.-A.; Harlaar, J.; Schwartz, M. Effect of Ankle-Foot Orthoses on Walking Efficiency and Gait in Children with Cerebral Palsy. J. Rehabil. Med. 2008, 40, 529–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, B.C.; Russell, S.D.; Abel, M.F. The Effects of Ankle Foot Orthoses on Energy Recovery and Work during Gait in Children with Cerebral Palsy. Clin. Biomech. 2012, 27, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalvand, H.; Dehghan, L.; Feizi, A.; Hosseini, S.A.; Amirsalari, S. The Impacts of Hinged and Solid Ankle-Foot Orthoses on Standing and Walking in Children with Spastic Diplegia. Iran. J. Child Neurol. 2013, 7, 12–19. [Google Scholar] [PubMed]
- Reeves, B.C.; Deeks, J.J.; Higgins, J.P. 13 Including Non-Randomized Studies. Cochrane Handb. Syst. Rev. Interv. 2008, 1, 389–432. [Google Scholar]
- Vanwala, J.; Diwan, S.; Shah, S.; Vyas, N. Effect of Ankle Foot Orthosis on Energy Expenditure Index and Gait Speed in Spastic Cerebral Palsy Children: An Observational Study. Int. J. Contemp. Pediatr. 2014, 1, 17. [Google Scholar] [CrossRef]
- Balaban, B.; Yasar, E.; Dal, U.; Yazicioglu, K.; Mohur, H.; Kalyon, T.A. The Effect of Hinged Ankle-Foot Orthosis on Gait and Energy Expenditure in Spastic Hemiplegic Cerebral Palsy. Disabil. Rehabil. 2007, 29, 139–144. [Google Scholar] [CrossRef]
- Zhao, X.; Xiao, N.; Li, H.; Du, S. Day vs. Day-Night Use of Ankle-Foot Orthoses in Young Children with Spastic Diplegia: A Randomized Controlled Study: A Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2013, 92, 905–911. [Google Scholar] [CrossRef]
- Schweizer, K.; Brunner, R.; Romkes, J. Upper Body Movements in Children with Hemiplegic Cerebral Palsy Walking with and without an Ankle-Foot Orthosis. Clin. Biomech. 2014, 29, 387–394. [Google Scholar] [CrossRef]
- Moher, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Chinese Edition). Zhong Xi Yi Jie He Xue Bao 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Van Gestel, L.; Molenaers, G.; Huenaerts, C.; Seyler, J.; Desloovere, K. Effect of Dynamic Orthoses on Gait: A Retrospective Control Study in Children with Hemiplegia. Dev. Med. Child Neurol. 2008, 50, 63–67. [Google Scholar] [CrossRef]
- Lucareli, P.R.G.; Lima, M.d.O.; Lucarelli, J.G.d.A.; Lima, F.P.S. Changes in Joint Kinematics in Children with Cerebral Palsy While Walking with and without a Floor Reaction Ankle-Foot Orthosis. Clinics 2007, 62, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogozinski, B.M.; Davids, J.R.; Davis, R.B., III; Jameson, G.G.; Blackhurst, D.W. The Efficacy of the Floor-Reaction Ankle-Foot Orthosis in Children with Cerebral Palsy. J. Bone Joint Surg. Am. 2009, 91, 2440–2447. [Google Scholar] [CrossRef]
- El-Kafy, A. The Clinical Impact of Orthotic Correction of Lower Limb Rotational Deformities in Children with Cerebral Palsy: A Randomized Controlled Trial. Clin. Rehabil. 2014, 28, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Khadem, A. An Ankle-Foot Orthosis Powered by Artificial Pneumatic Muscles; Khajeh Nasir Toosi University of Technology (KNTU): Tehran, Iran, 2019. [Google Scholar]
- Pomeranz, B.; Adler, U.; Shenoy, N.; Macaluso, C.; Parikh, S. Prosthetics and Orthotics for the Older Adult with a Physical Disability. Clin. Geriatr. Med. 2006, 22, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Lewallen, J.; Miedaner, J.; Amyx, S.; Sherman, J. Effect of Three Styles of Custom Ankle Foot Orthoses on the Gait of Stroke Patients While Walking on Level and Inclined Surfaces. J. Prosthet. Orthot. 2010, 22, 78–83. [Google Scholar] [CrossRef]
- Murphy, D.P.; Webster, J.B.; Lovegreen, W.; Simoncini, A. Lower Limb Orthoses. In Braddom’s Physical Medicine and Rehabilitation; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Berkelman, P.; Rossi, P.; Lu, T.; Ma, J. Passive Orthosis Linkage for Locomotor Rehabilitation. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar]
- Ghosh, S.; Robson, N.; McCarthy, J.M. Design of Wearable Lower Leg Orthotic Based on Six-Bar Linkage. In Proceedings of the Volume 5A: 41st Mechanisms and Robotics Conference, Cleveland, OH, USA, 6–9 August 2017; American Society of Mechanical Engineers: New York, NY, USA, 2017. [Google Scholar]
- Ghosh, S.; Robson, N.; McCarthy, J.M. Development of Customized Orthotics Based on Lower-Leg Anthropometric Data and Task. In Advances in Human Factors in Wearable Technologies and Game Design; Springer International Publishing: Cham, Switzerland, 2018; pp. 54–63. ISBN 9783319606385. [Google Scholar]
- Chang, M.C.; Chun, M.H. The Effects of a Short Ankle-Foot Orthosis on Gait in Patients with Post-Stroke Hemiplegia. Neurol. Asia 2019, 24, 103–107. [Google Scholar]
- Darwich, A.; Nazha, H.; Sliman, A.; Abbas, W. Ankle-Foot Orthosis Design between the Tradition and the Computerized Perspectives. Int. J. Artif. Organs 2020, 43, 354–361. [Google Scholar] [CrossRef]
- Ramsey, J.A. Development of a Method for Fabricating Polypropylene Non-Articulated Dorsiflexion Assist Ankle Foot Orthoses with Predetermined Stiffness. Prosthet. Orthot. Int. 2011, 35, 54–69. [Google Scholar] [CrossRef]
- Surmen, H.K.; Akalan, N.E.; Arslan, Y.Z. Design, Manufacture, and Selection of Ankle-Foot-Orthoses. In Advanced Methodologies and Technologies in Artificial Intelligence, Computer Simulation, and Human-Computer Interaction; IGI Global: Hershey, PA, USA, 2019. [Google Scholar]
- Choo, Y.J.; Chang, M.C. Commonly Used Types and Recent Development of Ankle-Foot Orthosis: A Narrative Review. Healthcare 2021, 9, 1046. [Google Scholar] [CrossRef]
- Delarque, A. Management of Chronic Conditions in the Foot and Lower Leg. J. Rehabil. Med. 2016, 48, 322. [Google Scholar]
- Ries, A.J.; Schwartz, M.H. Ground Reaction and Solid Ankle-Foot Orthoses Are Equivalent for the Correction of Crouch Gait in Children with Cerebral Palsy. Dev. Med. Child Neurol. 2019, 61, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, S.; Ebina, M.; Miyazaki, S.; Kawai, H.; Kubota, T. Development of a New Ankle-Foot Orthosis with Dorsiflexion Assist, Part 1: Desirable Characteristics of Ankle-Foot Orthoses for Hemiplegic Patients. J. Prosthet. Orthot. 1997, 9, 174–179. [Google Scholar] [CrossRef]
- Sen, D.; Mohan, S.; Ananthasuresh, G.K. Mechanism and Machine Science: Select Proceedings of Asian MMS 2018; Springer Nature: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Yamamoto, S.; Ebina, M.; Kubo, S.; Hayashi, T.; Akita, Y.; Hayakawa, Y. Development of an Ankle-Foot Orthosis with Dorsiflexion Assist, Part 2: Structure and Evaluation. JPO J. Prosthet. Orthot. 1999, 11, 24–28. [Google Scholar] [CrossRef]
- Yamamoto, S.; Tanaka, S.; Motojima, N. Comparison of Ankle-Foot Orthoses with Plantar Flexion Stop and Plantar Flexion Resistance in the Gait of Stroke Patients: A Randomized Controlled Trial. Prosthet. Orthot. Int. 2018, 42, 544–553. [Google Scholar] [CrossRef]
- Mulroy, S.J.; Eberly, V.J.; Gronely, J.K.; Weiss, W.; Newsam, C.J. Effect of AFO Design on Walking after Stroke: Impact of Ankle Plantar Flexion Contracture. Prosthet. Orthot. Int. 2010, 34, 277–292. [Google Scholar] [CrossRef] [Green Version]
- Fatone, S.; Gard, S.A.; Malas, B.S. Effect of Ankle-Foot Orthosis Alignment and Foot-Plate Length on the Gait of Adults with Poststroke Hemiplegia. Arch. Phys. Med. Rehabil. 2009, 90, 810–818. [Google Scholar] [CrossRef]
- Scotland, N.Q. Use of Ankle Foot Orthoses Following Stroke; NHS Quality Improvement Scotland: Edinburgh, Scotland, 2009. [Google Scholar]
- Buckon, C.E.; Thomas, S.S.; Jakobson-Huston, S.; Moor, M.; Sussman, M.; Aiona, M. Comparison of Three Ankle-Foot Orthosis Configurations for Children with Spastic Hemiplegia. Dev. Med. Child Neurol. 2001, 43, 371–378. [Google Scholar] [CrossRef]
- Rha, D.-W.; Kim, D.J.; Park, E.S. Effect of Hinged Ankle-Foot Orthoses on Standing Balance Control in Children with Bilateral Spastic Cerebral Palsy. Yonsei Med. J. 2010, 51, 746–752. [Google Scholar] [CrossRef] [Green Version]
- Son, I.; Lee, D.; Hong, S.; Lee, K.; Lee, G. Comparison of Gait Ability of a Child with Cerebral Palsy According to the Difference of Dorsiflexion Angle of Hinged Ankle-Foot Orthosis: A Case Report. Am. J. Case Rep. 2019, 20, 1454–1459. [Google Scholar] [CrossRef]
- Alimerzaloo, F.; Kashani, R.V.; Saeedi, H.; Farzi, M.; Fallahian, N. Patellar Tendon Bearing Brace: Combined Effect of Heel Clearance and Ankle Status on Foot Plantar Pressure. Prosthet. Orthot. Int. 2014, 38, 34–38. [Google Scholar] [CrossRef]
- Choo, Y.J.; Park, C.H.; Chang, M.C. Rearfoot Disorders and Conservative Treatment: A Narrative Review. Ann. Palliat. Med. 2020, 9, 3546–3552. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Nagata, K.; Goto, T.; Hoshiko, H.; Inoue, A. The Effect of the Patellar Tendon-Bearing Cast on Loading. J. Bone Joint Surg. Br. 2000, 82, 228–232. [Google Scholar] [CrossRef]
- Yamamoto, S.; Hagiwara, A.; Mizobe, T.; Yokoyama, O.; Yasui, T. Development of an Ankle-Foot Orthosis with an Oil Damper. Prosthet. Orthot. Int. 2005, 29, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, O.; Sashika, H.; Hagiwara, A.; Yamamoto, S.; Yasui, T. Kinematic Effects on Gait of a Newly Designed Ankle-Foot Orthosis with Oil Damper Resistance: A Case Series of 2 Patients with Hemiplegia. Arch. Phys. Med. Rehabil. 2005, 86, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Fuchi, M.; Yasui, T. Change of Rocker Function in the Gait of Stroke Patients Using an Ankle Foot Orthosis with an Oil Damper: Immediate Changes and the Short-Term Effects. Prosthet. Orthot. Int. 2011, 35, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Ohata, K.; Yasui, T.; Tsuboyama, T.; Ichihashi, N. Effects of an Ankle-Foot Orthosis with Oil Damper on Muscle Activity in Adults after Stroke. Gait Posture 2011, 33, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Chin, R.; Hsiao-Wecksler, E.T.; Loth, E.; Kogler, G.; Manwaring, S.D.; Tyson, S.N.; Shorter, K.A.; Gilmer, J.N. A Pneumatic Power Harvesting Ankle-Foot Orthosis to Prevent Foot-Drop. J. Neuroeng. Rehabil. 2009, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Chin, R.; Hsiao-Wecksler, E.T.; Loth, E.; Alleyne, A.; Manwaring, S.; Shorter, K.A.; Tyson, S.N.; Kogler, G. Portable Pneumatic Power-Harvesting Ankle-Foot-Orthosis. In Proceedings of the ASME 2008 Summer Bioengineering Conference, Parts A and B, Marco Island, FL, USA, 25–29 June 2008; American Society of Mechanical Engineers: New York, NY, USA, 2008. [Google Scholar]
- Danielsson, A.; Sunnerhagen, K.S. Energy Expenditure in Stroke Subjects Walking with a Carbon Composite Ankle Foot Orthosis. J. Rehabil. Med. 2004, 36, 165–168. [Google Scholar] [CrossRef] [Green Version]
- Alimusaj, M.; Knie, I.; Wolf, S.; Fuchs, A.; Braatz, F.; Döderlein, L. Functional impact of carbon fiber springs in ankle-foot orthoses. Orthopade 2007, 36, 752–756. [Google Scholar] [CrossRef]
- Wolf, S.I.; Alimusaj, M.; Rettig, O.; Döderlein, L. Dynamic Assist by Carbon Fiber Spring AFOs for Patients with Myelomeningocele. Gait Posture 2008, 28, 175–177. [Google Scholar] [CrossRef]
- Groner, C. Strengthening the Case for Carbon Fiber AFOs. LER 2010, 2, 23–30. [Google Scholar]
- Cha, Y.H.; Lee, K.H.; Ryu, H.J.; Joo, I.W.; Seo, A.; Kim, D.H.; Kim, S.J. Ankle-Foot Orthosis Made by 3D Printing Technique and Automated Design Software. Appl. Bionics Biomech. 2017, 2017, 9610468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creylman, V.; Muraru, L.; Pallari, J.; Vertommen, H.; Peeraer, L. Gait Assessment during the Initial Fitting of Customized Selective Laser Sintering Ankle Foot Orthoses in Subjects with Drop Foot. Prosthet. Orthot. Int. 2013, 37, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavroidis, C.; Ranky, R.G.; Sivak, M.L.; Patritti, B.L.; DiPisa, J.; Caddle, A.; Gilhooly, K.; Govoni, L.; Sivak, S.; Lancia, M.; et al. Patient Specific Ankle-Foot Orthoses Using Rapid Prototyping. J. Neuroeng. Rehabil. 2011, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Faustini, M.C.; Neptune, R.R.; Crawford, R.H.; Stanhope, S.J. Manufacture of Passive Dynamic Ankle-Foot Orthoses Using Selective Laser Sintering. IEEE Trans. Biomed. Eng. 2008, 55, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Schrank, E.S.; Stanhope, S.J. Dimensional Accuracy of Ankle-Foot Orthoses Constructed by Rapid Customization and Manufacturing Framework. J. Rehabil. Res. Dev. 2011, 48, 31–42. [Google Scholar] [CrossRef]
- Schrank, E.S.; Hitch, L.; Wallace, K.; Moore, R.; Stanhope, S.J. Assessment of a Virtual Functional Prototyping Process for the Rapid Manufacture of Passive-Dynamic Ankle-Foot Orthoses. J. Biomech. Eng. 2013, 135, 101011–101017. [Google Scholar] [CrossRef]
- Telfer, S.; Pallari, J.; Munguia, J.; Dalgarno, K.; McGeough, M.; Woodburn, J. Embracing Additive Manufacture: Implications for Foot and Ankle Orthosis Design. BMC Musculoskelet. Disord. 2012, 13, 84. [Google Scholar] [CrossRef] [Green Version]
- Walbran, M.; Turner, K.; McDaid, A.J. Customized 3D Printed Ankle-Foot Orthosis with Adaptable Carbon Fibre Composite Spring Joint. Cogent Eng. 2016, 3, 1227022. [Google Scholar] [CrossRef]
- Deckers, J.P.; Vermandel, M.; Geldhof, J.; Vasiliauskaite, E.; Forward, M.; Plasschaert, F. Development and Clinical Evaluation of Laser-Sintered Ankle Foot Orthoses. Plast. Rubber Compos. 2018, 47, 42–46. [Google Scholar] [CrossRef]
- Scheffers, G.; Hiller, C.; Refshauge, K.; Burns, J. Prescription of Foot and Ankle Orthoses for Children with Charcot–Marie–Tooth Disease: A Review of the Evidence. Phys. Ther. Rev. 2012, 17, 79–90. [Google Scholar] [CrossRef]
- Aydin, L.; Kucuk, S. A Method for More Accurate FEA Results on a Medical Device Developed by 3D Technologies. Polym. Adv. Technol. 2018, 29, 2281–2286. [Google Scholar] [CrossRef]
- Wojciechowski, E.; Chang, A.Y.; Balassone, D.; Ford, J.; Cheng, T.L.; Little, D.; Menezes, M.P.; Hogan, S.; Burns, J. Feasibility of Designing, Manufacturing and Delivering 3D Printed Ankle-Foot Orthoses: A Systematic Review. J. Foot Ankle Res. 2019, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Behera, A. Smart Applications of NiTi Shape Memory Alloy in Biomedical Industries. In Nickel-Titanium Smart Hybrid Materials; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Bhadane-Deshpande, M. Towards a Shape Memory Alloy Based Variable Stiffness Ankle Foot Orthosis; University of Toledo: Toledo, ON, Canada, 2012. [Google Scholar]
- Deberg, L.; Taheri Andani, M.; Hosseinipour, M.; Elahinia, M. An SMA Passive Ankle Foot Orthosis: Design, Modeling, and Experimental Evaluation. Smart Mater. Res. 2014, 2014, 72094. [Google Scholar] [CrossRef] [Green Version]
- Mataee, M.G.; Andani, M.T.; Elahinia, M. Adaptive Ankle–Foot Orthoses Based on Superelasticity of Shape Memory Alloys. J. Intell. Mater. Syst. Struct. 2015, 26, 639–651. [Google Scholar] [CrossRef]
- Amerinatanzi, A.; Zamanian, H.; Shayesteh Moghaddam, N.; Jahadakbar, A.; Elahinia, M. Application of the Superelastic NiTi Spring in Ankle Foot Orthosis (AFO) to Create Normal Ankle Joint Behavior. Bioengineering 2017, 4, 95. [Google Scholar] [CrossRef] [Green Version]
- Nematollahi, M.; Baghbaderani, K.S.; Amerinatanzi, A.; Zamanian, H.; Elahinia, M. Application of NiTi in Assistive and Rehabilitation Devices: A Review. Bioengineering 2019, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Kluding, P.M.; Dunning, K.; O’Dell, M.W.; Wu, S.S.; Ginosian, J.; Feld, J.; McBride, K. Foot Drop Stimulation versus Ankle Foot Orthosis after Stroke: 30-Week Outcomes. Stroke 2013, 44, 1660–1669. [Google Scholar] [CrossRef] [Green Version]
- de Paula, G.V.; da Silva, T.R.; de Souza, J.T.; Luvizutto, G.J.; Bazan, S.G.Z.; Modolo, G.P.; Winckler, F.C.; de Oliveira Antunes, L.C.; Martin, L.C.; da Costa, R.D.M.; et al. Effect of Ankle-Foot Orthosis on Functional Mobility and Dynamic Balance of Patients after Stroke: Study Protocol for a Randomized Controlled Clinical Trial. Medicine 2019, 98, e17317. [Google Scholar] [CrossRef]
- Schwarze, M.; Bartsch, L.P.; Block, J.; Alimusaj, M.; Jaber, A.; Schiltenwolf, M.; Wolf, S.I. A Comparison between Laterally Wedged Insoles and Ankle-Foot Orthoses for the Treatment of Medial Osteoarthritis of the Knee: A Randomized Cross-over Trial. Clin. Rehabil. 2021, 35, 1032–1043. [Google Scholar] [CrossRef]
- Bashir, A.Z.; Dinkel, D.M.; Bapat, G.M.; Despiegelaere, H.; Hassan, M.; Johanning, J.M.; Pipinos, I.I.; Myers, S.A. Considerations for Implementation of an Ankle-Foot Orthosis to Improve Mobility in Peripheral Artery Disease. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100092. [Google Scholar] [CrossRef] [PubMed]
- Renfrew, L.; Paul, L.; McFadyen, A.; Rafferty, D.; Moseley, O.; Lord, A.C.; Bowers, R.; Mattison, P. The Clinical- and Cost-Effectiveness of Functional Electrical Stimulation and Ankle-Foot Orthoses for Foot Drop in Multiple Sclerosis: A Multicentre Randomized Trial. Clin. Rehabil. 2019, 33, 1150–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricardo, D.; Raposo, M.R.; Cruz, E.B.; Oliveira, R.; Carnide, F.; Veloso, A.P.; João, F. Effects of Ankle Foot Orthoses on the Gait Patterns in Children with Spastic Bilateral Cerebral Palsy: A Scoping Review. Children 2021, 8, 903. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Yeh, C.-H.; Tsai, Y.-C.; Kuo, L.-C.; Hsu, H.-Y.; Chuang, P.-H.; Chang, K.; Su, F.-C. Evidence-Based Customized Ankle-Foot Orthosis with Energy Storage. J. Med. Biol. Eng. 2021, 41, 126–136. [Google Scholar] [CrossRef]
- Fatone, S.; Jerousek, S.; Slater, B.C.S.; Deutsch, A.; LaVela, S.L.; Peterson, M.; Soltys, N.T.; McPherson, V.; Heinemann, A.W. Identifying Instruments to Assess Care Quality for Individuals with Custom Ankle Foot Orthoses: A Scoping Review. Arch. Phys. Med. Rehabil. 2021, 102, 709–734. [Google Scholar] [CrossRef]
- Moll, I.; Marcellis, R.G.J.; Coenen, M.L.P.; Fleuren, S.M.; Willems, P.J.B.; Speth, L.A.W.M.; Witlox, M.A.; Meijer, K.; Vermeulen, R.J. A Randomized Crossover Study of Functional Electrical Stimulation during Walking in Spastic Cerebral Palsy: The FES on Participation (FESPa) Trial. BMC Pediatr. 2022, 22, 37. [Google Scholar] [CrossRef]
Figure 1.
Selection procedure utilized in this study.

Figure 2.
Solid AFOs: (a) metal AFO, (b) plastic AFO, (c) posterior-leaf-spring AFO, (d) Ground-reaction AFOs.
Figure 2.
Solid AFOs: (a) metal AFO, (b) plastic AFO, (c) posterior-leaf-spring AFO, (d) Ground-reaction AFOs.

Figure 3.
(a) Type I AFO, (b) Type II AFO, (c) DACS AFO.

Figure 4.
(a) Plantar-flexion stop AFO, (b) hinged AFO, (c) patellar-tendon-bearing AFO.

Figure 5.
AFO with an oil damper [55]; with permission from Elsevier (License Number: 5513260140134).
Figure 5.
AFO with an oil damper [55]; with permission from Elsevier (License Number: 5513260140134).

Figure 6.
Pneumatic harvested AFO [59]; with permission from Springer Nature (Creative Commons license, http://creativecommons.org/licenses/by/4.0/).
Figure 6.
Pneumatic harvested AFO [59]; with permission from Springer Nature (Creative Commons license, http://creativecommons.org/licenses/by/4.0/).

Figure 7.
Images of SMA-based AFOs. (a) Superelastic-wire-based AFO [78]; with permission from Hindawi (Creative Commons license, http://creativecommons.org/licenses/by/4.0/). (b) Spring-based AFO [80]; with permission from MDPI (Creative Commons license, http://creativecommons.org/licenses/by/4.0/).
Figure 7.
Images of SMA-based AFOs. (a) Superelastic-wire-based AFO [78]; with permission from Hindawi (Creative Commons license, http://creativecommons.org/licenses/by/4.0/). (b) Spring-based AFO [80]; with permission from MDPI (Creative Commons license, http://creativecommons.org/licenses/by/4.0/).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Detailed summary of the passive articulated and non-articulated ankle–foot-orthosis types.
| Type | Control Element | Moment Mechanism | Features | Limitations |
|---|---|---|---|---|
| Metal AFO [28,29,30,31,32,33] | Springs/or hinges/or stops | Assistance/resistance or assistance/or locking |
|
|
| Plastic AFO [34,35,36] | One-way frictional clutch | Resistance |
|
|
| Posterior-leaf-spring AFO [37,38,39] | Plastic shell | Resistance |
|
|
| Ground-Reaction AFO [26,40] | Posterior leaf spring and a rigid footplate | Assistance |
|
|
| Yamamoto Type I [41,42,43] | Two springs | Assistance |
|
|
| Yamamoto Type II [41,42,43] | One spring | Assistance |
|
|
| Dorsiflexion-assistance-controlled spring AFO [42] | Dorsiflexion-assistance spring | Assistance |
|
|
| Plantar-flexion-stop AFO [44,45,46] | Stops | Resistance |
|
|
| Hinged AFO [16,38,47,48,49,50] | Hinges | Resistance or assistance |
|
|
| Patellar-tendon-bearing AFO [38,51,52,53] | Rigid frame | Resistance |
|
|
| AFO with an oil damper [54,55,56,57] | Hydraulic damper | Resistance/assistance |
|
|
| Pneumatic harvested AFO [48,58,59] | Pneumatic cylinder | Resistance/assistance |
|
|
| Short-leg AFO [27] | Hinges or rigid shell | Assistance |
|
|
| Energy-return AFO [60,61,62,63] | Spring-like mechanism | Resistance/assistance |
|
|
| Three-dimensionally printed AFO [64,65,66,67,68,69,70,71,72,73,74] | Design-based element | Resistance/or assistance/or locking |
|
|
| SMA-based AFO [76,77,78,79,80,81] | SMA element | Resistance/assistance |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nazha, H.M.; Szávai, S.; Darwich, M.A.; Juhre, D. Passive Articulated and Non-Articulated Ankle–Foot Orthoses for Gait Rehabilitation: A Narrative Review. Healthcare 2023, 11, 947. https://doi.org/10.3390/healthcare11070947
AMA Style
Nazha HM, Szávai S, Darwich MA, Juhre D. Passive Articulated and Non-Articulated Ankle–Foot Orthoses for Gait Rehabilitation: A Narrative Review. Healthcare. 2023; 11(7):947. https://doi.org/10.3390/healthcare11070947
Chicago/Turabian StyleNazha, Hasan Mhd, Szabolcs Szávai, Mhd Ayham Darwich, and Daniel Juhre. 2023. "Passive Articulated and Non-Articulated Ankle–Foot Orthoses for Gait Rehabilitation: A Narrative Review" Healthcare 11, no. 7: 947. https://doi.org/10.3390/healthcare11070947
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.