
Effect of the Adhesive Strategy on Clinical Performance and Marginal Integrity of a Universal Adhesive in Non-Carious Cervical Lesions in a Randomized 36-Month Study

 , , and
, , and 
Abstract
:
1. Introduction
- (1)
- The universal adhesive would result in lower cumulative failure rates than the reference system in all application modes (clinical performance of adhesives/application mode, primary outcome).
- (2)
- In QMA, the universal adhesive would show fewer marginal gaps and more perfect restoration margins than the reference system in all conditioning modes (marginal quality, secondary outcome).
- (3)
- With time, marginal gap progression and a decrease in perfect margin can be detected (gap progression).
- (4)
- Clinical restoration assessment and QMA are consistent in their statements. Group differences can be identified earlier by QMA (method performance/power, tertiary outcome).
2. Materials and Methods
2.1. Study Design (According to CONSORT)
2.2. Study Population
2.3. Restorative Procedure
2.4. Impression and Replica Production
2.5. Study Outcomes
2.5.1. Clinical Evaluation
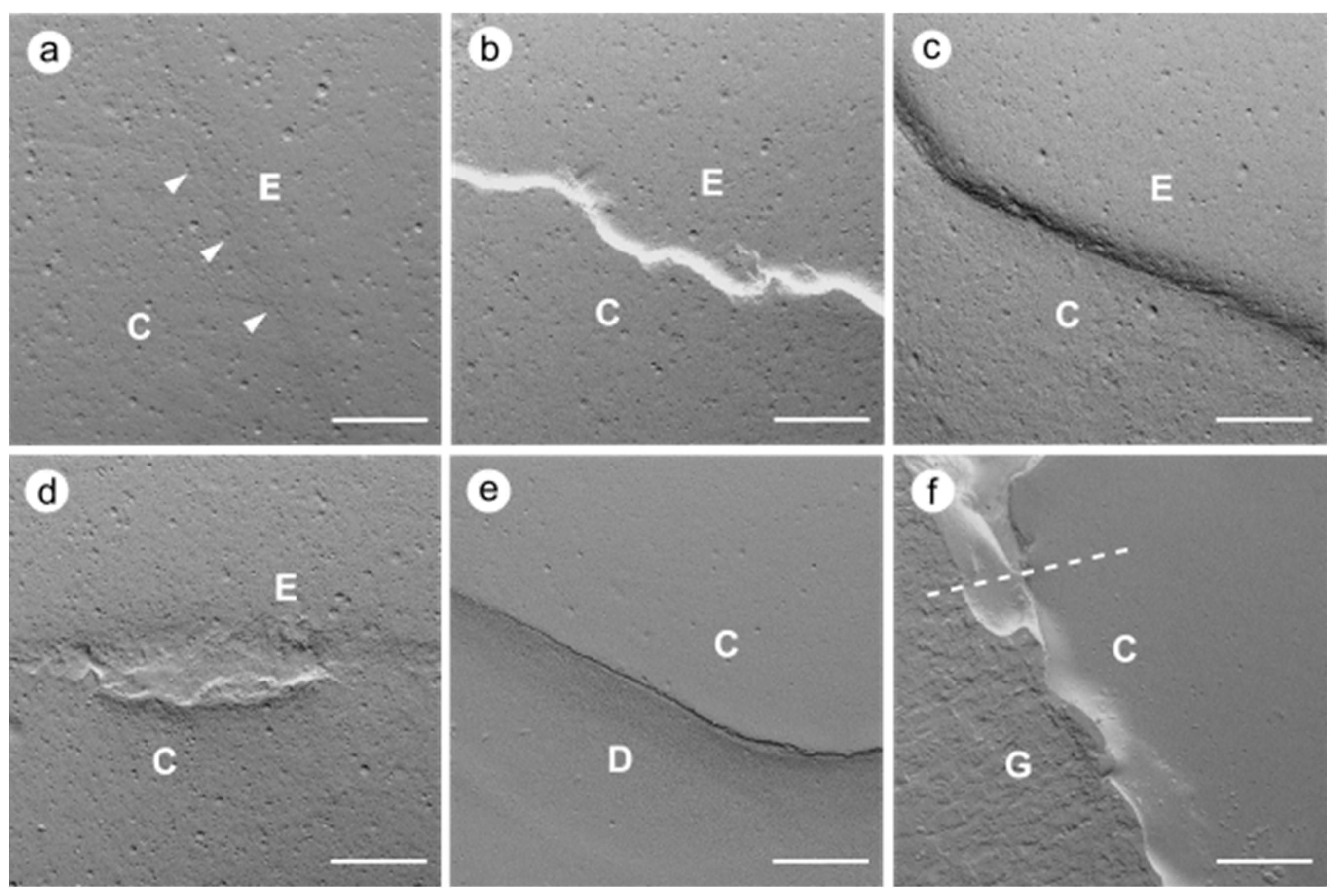
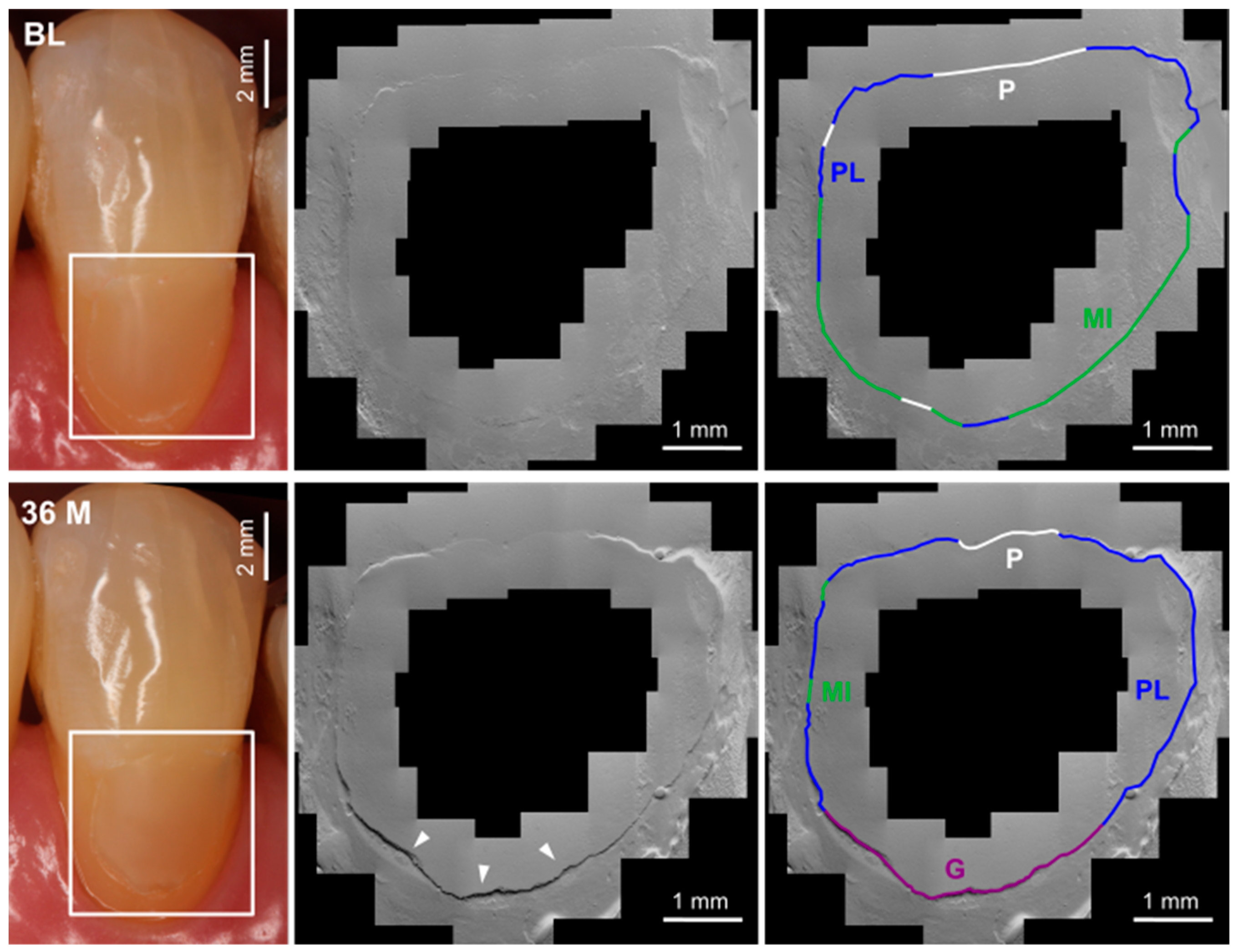
2.5.2. Quantitative Margin Analysis
2.6. Statistical Analysis
3. Results
3.1. Clinical Evaluation
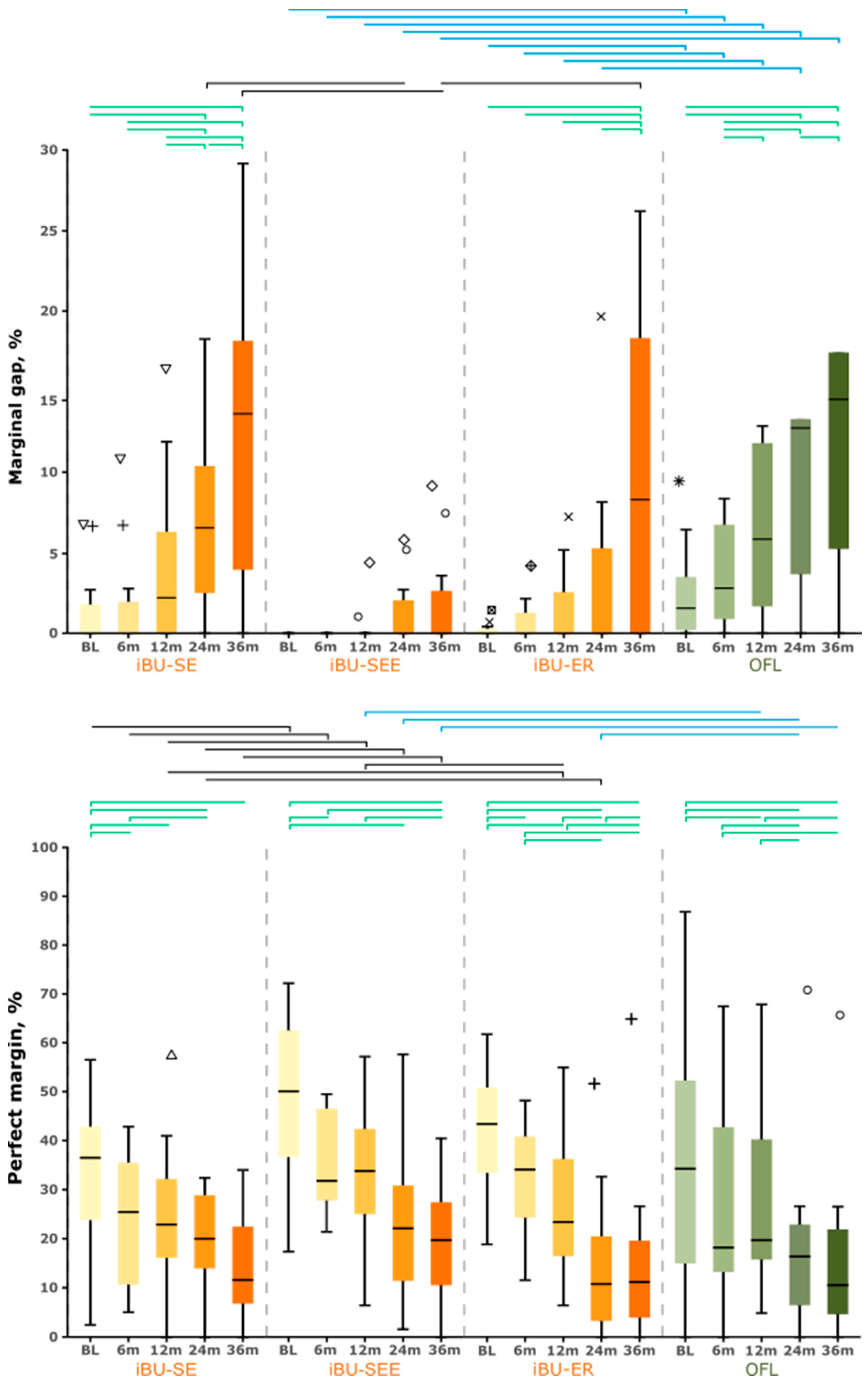
3.2. Quantitative Margin Analysis
3.3. Clinic and Quantitative Margin Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Almeida, R.A.M.; Lima, S.N.L.; Nassif, M.V.; Mattos, N.H.R.; de Matos, T.P.; de Jesus Tavarez, R.R.; Cardenas, A.F.M.; Bandeca, M.C.; Loguercio, A.D. Eighteen-month clinical evaluation of a new universal adhesive applied in the “no-waiting” technique: A randomized clinical trial. Clin. Oral Investig. 2022, 27, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Sofan, E.; Sofan, A.; Palaia, G.; Tenore, G.; Romeo, U.; Migliau, G. Classification review of dental adhesive systems: From the IV generation to the universal type. Ann. Stomatol. 2017, 8, 1–17. [Google Scholar] [CrossRef]
- Elkaffas, A.A.; Hamama, H.H.H.; Mahmoud, S.H. Do universal adhesives promote bonding to dentin? A systematic review and meta-analysis. Restor. Dent. Endod. 2018, 43, e29. [Google Scholar] [CrossRef] [PubMed]
- Oz, F.D.; Kutuk, Z.B.; Ozturk, C.; Soleimani, R.; Gurgan, S. An 18-month clinical evaluation of three different universal adhesives used with a universal flowable composite resin in the restoration of non-carious cervical lesions. Clin. Oral Investig. 2019, 23, 1443–1452. [Google Scholar] [CrossRef]
- Cuevas-Suárez, C.E.; da Rosa, W.L.d.O.; Lund, R.G.; da Silva, A.F.; Piva, E. Bonding performance of universal adhesives: An updated systematic review and meta-analysis. J. Adhes. Dent. 2019, 21, 7–26. [Google Scholar] [CrossRef]
- Oz, F.D.; Ergin, E.; Canatan, S. Twenty-four-month clinical performance of different universal adhesives in etch-and-rinse, selective etching and self-etch application modes in NCCL—A randomized controlled clinical trial. J. Appl. Oral Sci. 2019, 27, e20180358. [Google Scholar] [CrossRef]
- Perdigão, J.; Ceballos, L.; Giráldez, I.; Baracco, B.; Fuentes, M.V. Effect of a hydrophobic bonding resin on the 36-month performance of a universal adhesive-a randomized clinical trial. Clin. Oral Investig. 2019, 24, 765–776. [Google Scholar] [CrossRef]
- van Meerbeek, B.; Yoshihara, K.; van Landuyt, K.; Yoshida, Y.; Peumans, M. From Buonocore’s Pioneering Acid-Etch Technique to Self-Adhering Restoratives. A Status Perspective of Rapidly Advancing Dental Adhesive Technology. J. Adhes. Dent. 2020, 22, 7–34. [Google Scholar] [CrossRef]
- Wagner, A.; Wendler, M.; Petschelt, A.; Belli, R.; Lohbauer, U. Bonding performance of universal adhesives in different etching modes. J. Dent. 2014, 42, 800–807. [Google Scholar] [CrossRef]
- de Oliveira da Rosa, W.L.; Piva, E.; da Silva, A.F. Bond strength of universal adhesives: A systematic review and meta-analysis. J. Dent. 2015, 43, 765–776. [Google Scholar] [CrossRef]
- Chen, H.; Feng, S.; Jin, Y.; Hou, Y.; Zhu, S. Comparison of bond strength of universal adhesives using different etching modes: A systematic review and meta-analysis. Dent. Mater. J. 2022, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hardan, L.; Bourgi, R.; Kharouf, N.; Mancino, D.; Zarow, M.; Jakubowicz, N.; Haikel, Y.; Cuevas-Suárez, C.E. Bond strength of universal adhesives to dentin: A systematic review and meta-analysis. Polymers 2021, 13, 814. [Google Scholar] [CrossRef] [PubMed]
- Perdigao, J. Current perspectives on dental adhesion: (1) Dentin adhesion—Not there yet. Jpn. Dent. Sci. Rev. 2020, 56, 190–207. [Google Scholar] [CrossRef] [PubMed]
- Perdigão, J.; Araujo, E.; Ramos, R.Q.; Gomes, G.; Pizzolotto, L. Adhesive dentistry: Current concepts and clinical considerations. J. Esthet. Restor. Dent. 2021, 33, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Haak, R.; Hähnel, M.; Schneider, H.; Rosolowski, M.; Park, K.-J.; Ziebolz, D.; Häfer, M. Clinical and OCT outcomes of a universal adhesive in a randomized clinical trial after 12 months. J. Dent. 2019, 90, 103200. [Google Scholar] [CrossRef] [PubMed]
- Atalay, C.; Ozgunaltay, G.; Yazici, A.R. Thirty-six-month clinical evaluation of different adhesive strategies of a universal adhesive. Clin. Oral Investig. 2020, 24, 1569–1578. [Google Scholar] [CrossRef]
- Gonçalves, D.F.M.; Shinohara, M.S.; Marão de Andrade Carvalho, P.R.; de Souza e Silva Ramos, F.; de Castro Oliveira, L.; Omoto, É.M.; Fagundes, T.C. Three-year evaluation of different adhesion strategies in non-carious cervical lesion restorations: A randomized clinical trial. J. Appl. Oral Sci. 2021, 29, e20210192. [Google Scholar] [CrossRef]
- Manarte-Monteiro, P.; Domingues, J.; Teixeira, L.; Gavinha, S.; Manso, M.C. Universal adhesives and adhesion modes in non-carious cervical restorations: 2-year randomised clinical trial. Polymers 2021, 14, 33. [Google Scholar] [CrossRef]
- de Paris Matos, T.; Perdigão, J.; de Paula, E.; Coppla, F.; Hass, V.; Scheffer, R.F.; Reis, A.; Loguercio, A.D. Five-year clinical evaluation of a universal adhesive: A randomized double-blind trial. Dent. Mater. 2020, 36, 1474–1485. [Google Scholar] [CrossRef]
- Oz, F.D.; Ozturk, C.; Soleimani, R.; Gurgan, S. Sixty-month follow up of three different universal adhesives used with a highly-filled flowable resin composite in the restoration of non-carious cervical lesion. Clin. Oral Investig. 2022, 26, 5377–5387. [Google Scholar] [CrossRef]
- Ruschel, V.C.; Shibata, S.; Stolf, S.C.; Chung, Y.; Baratieri, L.N.; Heymann, H.O.; Walter, R. Eighteen-month clinical study of universal adhesives in noncarious cervical lesions. Oper. Dent. 2018, 43, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Perdigão, J.; Kose, C.; Mena-Serrano, A.P.; de Paula, E.A.; Tay, L.Y.; Reis, A.; Loguercio, A.D. A new universal simplified adhesive: 18-month clinical evaluation. Oper. Dent. 2014, 39, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, M.V.; Perdigão, J.; Baracco, B.; Giráldez, I.; Ceballos, L. Effect of an additional bonding resin on the 5-year performance of a universal adhesive: A randomized clinical trial. Clin. Oral Investig. 2022, 27, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Lawson, N.C.; Robles, A.; Fu, C.-C.; Lin, C.P.; Sawlani, K.; Burgess, J.O. Two-year clinical trial of a universal adhesive in total-etch and self-etch mode in non-carious cervical lesions. J. Dent. 2015, 43, 1229–1234. [Google Scholar] [CrossRef]
- Ruschel, V.C.; Stolf, S.C.; Shibata, S.; Chung, Y.; Boushell, L.W.; Baratieri, L.N.; Walter, R. Three-year clinical evaluation of universal adhesives in non-carious cervical lesions. Am. J. Dent. 2019, 32, 223–228. [Google Scholar] [PubMed]
- Zanatta, R.F.; Silva, T.M.; Esper, M.; Bresciani, E.; Gonçalves, S.; Caneppele, T. Bonding performance of simplified adhesive systems in noncarious cervical lesions at 2-year follow-up: A double-blind randomized clinical trial. Oper. Dent. 2019, 44, 476–487. [Google Scholar] [CrossRef]
- Josic, U.; Mazzitelli, C.; Maravic, T.; Radovic, I.; Jacimovic, J.; Mancuso, E.; Florenzano, F.; Breschi, L.; Mazzoni, A. The influence of selective enamel etch and self-etch mode of universal adhesives’ application on clinical behavior of composite restorations placed on non-carious cervical lesions: A systematic review and meta-analysis. Dent. Mater. 2022, 38, 472–488. [Google Scholar] [CrossRef]
- Szesz, A.; Parreiras, S.; Reis, A.; Loguercio, A.D. Selective enamel etching in cervical lesions for self-etch adhesives: A systematic review and meta-analysis. J. Dent. 2016, 53, 1–11. [Google Scholar] [CrossRef]
- Merle, C.L.; Fortenbacher, M.; Schneider, H.; Schmalz, G.; Challakh, N.; Park, K.-J.; Häfer, M.; Ziebolz, D.; Haak, R. Clinical and OCT assessment of application modes of a universal adhesive in a 12-month RCT. J. Dent. 2022, 119, 104068. [Google Scholar] [CrossRef]
- Hickel, R.; Roulet, J.-F.; Bayne, S.C.; Heintze, S.D.; Mjör, I.A.; Peters, M.C.; Rousson, V.; Randall, R.; Schmalz, G.; Tyas, M.J.; et al. Recommendations for conducting controlled clinical studies of dental restorative materials. Clin. Oral Investig. 2007, 11, 5–33. [Google Scholar] [CrossRef]
- Hickel, R.; Peschke, A.; Tyas, M.J.; Mjör, I.A.; Bayne, S.C.; Peters, M.C.; Hiller, K.-A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation—Clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples. J. Adhes. Dent. 2010, 12, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Steigerwald-Otremba, A.S.; Häfer, M.; Krause, F.; Scholz, M.; Haak, R. Is optical coherence tomography a potential tool to evaluate marginal adaptation of class III/IV composite restorations in vivo? Oper. Dent. 2019, 44, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Roulet, J.-F.; Reich, T.; Blunck, U.; Noack, M.J. Quantitative margin analysis in the scanning electron microscope. Scanning Microsc. 1989, 3, 147–158. [Google Scholar] [PubMed]
- Ernst, C.-P.; Galler, P.; Willershausen, B.; Haller, B. Marginal integrity of class V restorations: SEM versus dye penetration. Dent. Mater. 2008, 24, 319–327. [Google Scholar] [CrossRef]
- Roulet, J.-F. Marginal integrity: Clinical significance. J. Dent. 1994, 22, S9–S12. [Google Scholar] [CrossRef] [PubMed]
- Roggendorf, M.J.; Krämer, N.; Appelt, A.; Naumann, M.; Frankenberger, R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J. Dent. 2011, 39, 643–647. [Google Scholar] [CrossRef]
- Bortolotto, T.; Bahillo, J.; Richoz, O.; Hafezi, F.; Krejci, I. Failure analysis of adhesive restorations with SEM and OCT: From marginal gaps to restoration loss. Clin. Oral Investig. 2015, 19, 1881–1890. [Google Scholar] [CrossRef]
- Frankenberger, R.; Krämer, N.; Lohbauer, U.; Nikolaenko, S.A.; Reich, S.M. Marginal integrity: Is the clinical performance of bonded restorations predictable in vitro? J. Adhes. Dent. 2007, 9 (Suppl. S1), 107–116. [Google Scholar]
- Frankenberger, R.; Krämer, N.; Petschelt, A. Technique sensitivity of dentin bonding: Effect of application mistakes on bond strength and marginal adaptation. Oper. Dent. 2000, 25, 324–330. [Google Scholar]
- Frankenberger, R.; Tay, F.R. Self-etch vs etch-and-rinse adhesives: Effect of thermo-mechanical fatigue loading on marginal quality of bonded resin composite restorations. Dent. Mater. 2005, 21, 397–412. [Google Scholar] [CrossRef]
- Haak, R.; Brückner, A.; Häfer, M.; Scholz, M.; Schneider, H. Is there an association between clinical and SEM quantitative marginal analysis in a 90-month trial? J. Adhes. Dent. 2021, 23, 37–46. [Google Scholar] [CrossRef]
- Haak, R.; Werner, M.S.; Schneider, H.; Häfer, M.; Schulz-Kornas, E. Clinical Outcomes and Quantitative Margin Analysis of a Universal Adhesive Using a Randomized Clinical Trial over Three Years. J. Clin. Med. 2022, 11, 6910. [Google Scholar] [CrossRef] [PubMed]
- Thévenaz, P. MosaicJ. Available online: http://bigwww.epfl.ch/thevenaz/mosaicj/ (accessed on 15 November 2022).
- Kunzelmann, K.-H. KHKs jQuantiGap. Available online: http://www.kunzelmann.de/4_software-imagej-quantitative_margin_analysis.html (accessed on 15 November 2022).
- Carrilho, E.; Cardoso, M.; Marques Ferreira, M.; Marto, C.M.; Paula, A.; Coelho, A.S. 10-MDP based dental adhesives: Adhesive interface characterization and adhesive stability—A systematic review. Materials 2019, 12, 790. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Dai, S.; Yang, J.; Shen, J.; Liao, M.; Xie, H.; Chen, C. Glycerol phosphate dimethacrylate: An alternative functional phosphate ester monomer to 10-methacryloyloxydecyl dihydrogen phosphate for enamel bonding. ACS Omega 2020, 5, 24826–24837. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, K.; Nagaoka, N.; Hayakawa, S.; Okihara, T.; Yoshida, Y.; van Meerbeek, B. Chemical interaction of glycero-phosphate dimethacrylate (GPDM) with hydroxyapatite and dentin. Dent. Mater. 2018, 34, 1072–1081. [Google Scholar] [CrossRef] [PubMed]
- Çelik, E.U.; Aka, B.; Yilmaz, F. Six-month clinical evaluation of a self-adhesive flowable composite in noncarious cervical lesions. J. Adhes. Dent. 2015, 17, 361–368. [Google Scholar] [CrossRef] [PubMed]
- de Paula, E.A.; Tay, L.Y.; Kose, C.; Mena-Serrano, A.P.; Reis, A.; Perdigão, J.; Loguercio, A.D. Randomized clinical trial of four adhesion strategies in cervical lesions: 12-month results. Int. J. Esthet. Dent. 2015, 10, 122–145. [Google Scholar]
- Peumans, M.; de Munck, J.; van Landuyt, K.L.; Poitevin, A.; Lambrechts, P.; van Meerbeek, B. A 13-year clinical evaluation of two three-step etch-and-rinse adhesives in non-carious class-V lesions. Clin. Oral Investig. 2012, 16, 129–137. [Google Scholar] [CrossRef]
- Dreweck, F.D.S.; Burey, A.; de Oliveira Dreweck, M.; Fernandez, E.; Loguercio, A.D.; Reis, A. Challenging the concept that OptiBond FL and Clearfil SE Bond in NCCLs are gold standard adhesives: A systematic review and meta-analysis. Oper. Dent. 2021, 46, E276–E295. [Google Scholar] [CrossRef]
- Peumans, M.; Wouters, L.; de Munck, J.; van Meerbeek, B.; van Landuyt, K. Nine-year clinical performance of a HEMA-free one-step self-etch adhesive in noncarious cervical lesions. J. Adhes. Dent. 2018, 20, 195–203. [Google Scholar] [CrossRef]
- van Landuyt, K.L.; de Munck, J.; Ermis, R.B.; Peumans, M.; van Meerbeek, B. Five-year clinical performance of a HEMA-free one-step self-etch adhesive in noncarious cervical lesions. Clin. Oral Investig. 2014, 18, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Karan, K.; Yao, X.; Xu, C.; Wang, Y. Chemical profile of the dentin substrate in non-carious cervical lesions. Dent. Mater. 2009, 25, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H. Resin bonding to cervical sclerotic dentin: A review. J. Dent. 2004, 32, 173–196. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Ruffieux, C.; Rousson, V. Clinical performance of cervical restorations-a meta-analysis. Dent. Mater. 2010, 26, 993–1000. [Google Scholar] [CrossRef]
- Mahn, E.; Rousson, V.; Heintze, S.D. Meta-analysis of the influence of bonding parameters on the clinical outcome of tooth-colored cervical restorations. J. Adhes. Dent. 2015, 17, 391–403. [Google Scholar] [CrossRef]
- Lührs, A.-K.; Jacker-Guhr, S.; Günay, H.; Herrmann, P. Composite restorations placed in non-carious cervical lesions-Which cavity preparation is clinically reliable? Clin. Exp. Dent. Res. 2020, 6, 558–567. [Google Scholar] [CrossRef]
- Loguercio, A.D.; Luque-Martinez, I.V.; Fuentes, S.; Reis, A.; Muñoz, M.A. Effect of dentin roughness on the adhesive performance in non-carious cervical lesions: A double-blind randomized clinical trial. J. Dent. 2018, 69, 60–69. [Google Scholar] [CrossRef]
- Heintze, S.D. Clinical relevance of tests on bond strength, microleakage and marginal adaptation. Dent. Mater. 2013, 29, 59–84. [Google Scholar] [CrossRef]
- Hosseini, M.; Raji, Z.; Kazemian, M. Microshear Bond Strength of Composite to Superficial Dentin by Use of Universal Adhesives with Different pH Values in Self-Etch and Etch & Rinse Modes. Dent. Res. J. 2023, 20, 5. [Google Scholar]
- van Meerbeek, B.; Yoshihara, K.; Yoshida, Y.; Mine, A.; de Munck, J.; van Landuyt, K.L. State of the art of self-etch adhesives. Dent. Mater. 2011, 27, 17–28. [Google Scholar] [CrossRef]
- Peumans, M.; de Munck, J.; Mine, A.; van Meerbeek, B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent. Mater. 2014, 30, 1089–1103. [Google Scholar] [CrossRef] [PubMed]
- Nagarkar, S.; Theis-Mahon, N.; Perdigão, J. Universal dental adhesives: Current status, laboratory testing, and clinical performance. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 2121–2131. [Google Scholar] [CrossRef] [PubMed]
- Arbildo, H.; Lamas-Lara, C.; Cruzado-Oliva, F.; Rosas-Prado, C.; Gómez-Fuerte, A.; Vásquez-Rodrigo, H. Comparison of the clinical effect of the adhesive strategies of universal adhesives in the treatment of non-carious cervical lesions. Systematic review and meta-analysis. J. Oral Res. 2018, 7, 210–222. [Google Scholar] [CrossRef]
- Haak, R.; Schäfer, P.; Hanßen, B.; Ziebolz, D.; Park, K.J.; Häfer, M.; Schmalz, G.; Schneider, H. OCT evaluation of marginal and internal interface integrity of class V composite restorations after 36 to 48 months. J. Adhes. Dent. 2022, 24, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Celik, C.; Cehreli, S.B.; Arhun, N. Resin composite repair: Quantitative microleakage evaluation of resin-resin and resin-tooth interfaces with different surface treatments. Eur. J. Dent. 2015, 9, 92–99. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | iBU-SE | iBU-SEE | iBU-ER | OFL | Lost iBU-SE | Lost iBU-SEE | Lost iBU-ER | Lost OFL |
|---|---|---|---|---|---|---|---|---|
| Nclinic/NQMA | 50/11 1 | 29/11 1 | 50/11 1 | 50/11 1 | 1/1 2 | 1/1 2 | 8/7 2 | 17/14 2 |
| Adhesive | iBond Universal | OptiBond FL | iBond Universal | OptiBond FL | ||||
| Application Mode | self-etch (SE) | selective-enamel- etch (SEE) | etch-and-rinse (ER) | etch-and-rinse (ER) | self-etch (SE) | selective-enamel- etch (SEE) | etch-and-rinse (ER) | etch-and-rinse (ER) |
| Composite | Venus Diamond Flow | |||||||
| Arc Distribution | ||||||||
| Maxillary | 27/8 | 19/8 | 31/9 | 31/6 | -/- | -/- | 5/4 | 9/7 |
| Mandibular | 23/3 | 10/3 | 19/2 | 19/5 | 1/1 | 1/1 | 3/3 | 8/7 |
| Tooth Distribution | ||||||||
| Incisor | 8/1 | 8/2 | 12/2 | 11/2 | -/- | -/- | 1/1 | 4/2 |
| Canine | 12/2 | 6/2 | 14/5 | 12/3 | 1/1 | -/- | 2/2 | 2/2 |
| Premolar | 30/8 | 15/7 | 24/4 | 27/6 | -/- | 1/1 | 5/4 | 11/10 |
| Lesion Borderline | ||||||||
| Enamel | -/- | -/- | -/- | -/- | -/- | -/- | -/- | -/- |
| Dentin | 1/- | -/- | -/- | -/- | -/- | -/- | -/- | -/- |
| Mixed (enamel/dentin) | 49/11 | 29/11 | 50/11 | 50/11 | 1//1 | 1/1 | 8/7 | 17/14 |
| Lesion Depth | ||||||||
| Shallow (<1 mm) | 6/- | 9/3 | 8/1 | 6/- | -/- | 1/1 | 1/1 | 2/2 |
| Medium (1–2 mm) | 42/11 | 19/8 | 41/10 | 42/11 | 1/1 | -/- | 7/6 | 13/12 |
| Deep (>2 mm) | 2/- | 1/- | 1/- | 2/- | -/- | -/- | -/- | 2/- |
| Material | Composition | Application | Manufacturer | |
|---|---|---|---|---|
| Etchant | Ultra-Etch® | 35% H3PO4 |
| Ultradent Products, Inc.; South Jordan, UT, USA |
| Adhesive | iBond® Universal | Methacrylate-monomer, 4-META, 10-MDP, acetone, water; pH 1.8 (LOT: 010021) |
| Kulzer GmbH; Hanau, Germany |
| OptiBondTM FL | Primer: HEMA, GPDM, MMEP, water, ethanol, photoinitiator (CQ), BHT (LOT: 5534310) Adhesive: Bis-GMA, HEMA, GPDM, GDMA, photoinitiator (CQ), ODMAB, fillers, barium aluminoborosilicate (LOT: 5592338) |
| Kerr GmbH; Herzogenrath, Germany | |
| Composite | Venus® Diamond Flow | UDMA, EBADMA, Ba-Al-F silicate glass, YbF3, SiO2, photoinitiators (LOT: 010113) |
| Kulzer GmbH; Hanau, Germany |
| iBU-SE | iBU-SEE | iBU-ER | OFL | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BL | 6 m | 12 m | 24 m | 36 m | BL | 6 m | 12 m | 24 m | 36 m | BL | 6 m | 12 m | 24 m | 36 m | BL | 6 m | 12 m | 24 m | 36 m | |
| Restored teeth, n 1 | 50 | 49 | 47 | 45 | 45 | 29 | 28 | 26 | 24 | 23 | 50 | 49 | 47 | 45 | 44 | 50 | 49 | 45 | 39 | 33 |
| Reassessment rate, % | 100 | 98 | 94 | 90 | 90 | 100 | 96.6 | 89.7 | 82.8 | 79.3 | 100 | 98 | 94 | 90 | 88 | 100 | 98 | 90 | 78 | 66 |
| Aesthetic criteria 2 | ||||||||||||||||||||
| Non-acceptable, % | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2.6 3 | 0 | 0 | 0 | 0 | 0 |
| Functional criteria 2 | ||||||||||||||||||||
| Non-acceptable, % | 0 | 0 | 0 | 0 | 2.2 4 | 0 | 0 | 0 | 0 | 4.3 4 | 0 | 0 | 2.1 4 | 4.3 4 | 17.4 4 | 0 | 6.1 4 | 16.7 4 | 29.8 4 | 36.2 4 |
| Biological criteria 2 | ||||||||||||||||||||
| Non-acceptable, % | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Cumulative failure rate (total score) 5 | ||||||||||||||||||||
| Non-acceptable, % | 0 | 0 | 0 | 0 | 2.2 4 | 0 | 0 | 0 | 0 | 4.3 4 | 0 | 0 | 2.1 4 | 4.3 4 | 19.6 6 | 0 | 6.1 4 | 16.7 4 | 29.8 4 | 36.2 4 |
| Time | %/pi | iBU-SE vs. iBU-SEE | iBU-SE vs. iBU-ER | iBU-SEE vs. iBU-ER | iBU-SE vs. OFL | iBU-SEE vs. OFL | iBU-ER vs. OFL | |
|---|---|---|---|---|---|---|---|---|
| Marginal staining score 2 or 3 | 6 m | % | 10.7/10.7 | 12.2/10.2 | 10.7/3.6 | 12.2/8.7 | 10.7/3.8 | 10.2/8.7 |
| pi | ≥0.625 | |||||||
| 12 m | % | 26.9/23.1 | 19.1/23.9 | 23.1/25.0 | 19.1/25.0 | 23.1/22.2 | 23.9/25.0 | |
| pi | ≥0.344 | |||||||
| 24 m | % | 41.7/33.3 | 40.0/34.1 | 33.3/33.3 | 40.0/21.2 | 33.3/23.5 | 34.1/21.2 | |
| pi | ≥0.146 | |||||||
| 36 m | % | 45.8/45.5 | 40.9/24.3 | 45.5/19.0 | 40.9/23.3 | 45.5/26.7 | 24.3/23.3 | |
| pi | ≥0.092 | |||||||
| Marginal adaptation score 2 or 3 | 6 m | % | 50.0/46.4 | 40.8/53.1 | 46.4/53.6 | 40.8/50.0 | 46.4/46.2 | 53.1/50.0 |
| pi | ≥0.286 | |||||||
| 12 m | % | 50.0/46.2 | 53.2/53.2 | 46.2/44.0 | 53.2/70.0 | 46.2/68.2 | 53.2/70.0 | |
| pi | 1.000 | 0.064 1 | ≥0.167 | |||||
| 24 m | % | 66.7/58.3 | 60.0/75.0 | 58.3/75.0 | 60.0/66.7 | 58.3/64.7 | 75.0/66.7 | |
| pi | ≥0.118 | |||||||
| 36 m | % | 79.2/72.7 | 70.5/75.7 | 72.7/76.2 | 70.5/73.3 | 72.7/60.0 | 75.7/73.3 | |
| pi | ≥0.727 | |||||||
| Fractures and retention score 5 2 | 6 m | % | 0.0/0.0 | 0.0/0.0 | 0.0/0.0 | 0.0/6.1 | 0.0/7.1 | 0.0/6.1 |
| pi | n. c. | 0.250 | 0.500 | 0.250 | ||||
| 12 m | % | 0.0/0.0 | 0.0/2.1 | 0.0/3.8 | 0.0/16.7 | 0.0/18.5 | 2.1/16.7 | |
| pi | n. c. | 1.000 | 1.000 | 0.016 | 0.125 | 0.070 1 | ||
| 24 m | % | 0.0/0.0 | 0.0/4.3 | 0.0/4.0 | 0.0/29.8 | 0.0/34.6 | 4.3/29.8 | |
| pi | n. c. | 1.000 | 1.000 | <0.001 | 0.016 | 0.003 | ||
| 36 m | % | 0.0/4.3 | 2.2/17.4 | 4.3/12.5 | 2.2/36.2 | 4.3/42.3 | 17.4/36.2 | |
| pi | 1.000 | 0.070 1 | 1.000 | <0.001 | 0.016 | 0.039 | ||
| Cumulative failure rate (total score) 3 | 6 m | % | 0.0/0.0 | 0.0/0.0 | 0.0/0.0 | 0.0/6.1 | 0.0/7.1 | 0.0/6.1 |
| pi | n. c. | n. c. | n. c. | 0.250 | 0.500 | 0.250 | ||
| 12 m | % | 0.0/0.0 | 0.0/2.1 | 0.0/3.8 | 0.0/16.7 | 0.0/18.5 | 2.1/16.7 | |
| pi | n. c. | 1.000 | 1.000 | 0.016 | 0.125 | 0.070 1 | ||
| 24 m | % | 0.0/0.0 | 0.0/4.3 | 0.0/4.0 | 0.0/29.8 | 0.0/34.6 | 4.3/29.8 | |
| pi | n. c. | 1.000 | 1.000 | <0.001 | 0.016 | 0.003 | ||
| 36 m | % | 0.0/4.3 | 2.2/19.6 | 4.3/16.0 | 2.2/36.2 | 4.3/42.3 | 19.6/36.2 | |
| pi | 1.000 | 0.039 | 0.625 | <0.001 | 0.016 | 0.146 | ||
| Parameter | Period | iBU-SE | iBU-SEE | iBU-ER | OFL |
|---|---|---|---|---|---|
| Marginal staining score 2 or 3 | BL to 6 m | 0.063 1 | 0.250 | 0.125 | 0.250 |
| BL to 12 m | 0.021 | 0.031 | 0.002 | 0.004 | |
| BL to 24 m | <0.001 | 0.008 | <0.001 | 0.016 | |
| BL to 36 m | <0.001 | 0.002 | 0.002 | 0.016 | |
| Marginal adaptation score 2 or 3 | BL to 6 m | 0.012 | 0.109 | <0.001 | 0.001 |
| BL to 12 m | <0.001 | 0.109 | <0.001 | <0.001 | |
| BL to 24 m | <0.001 | 0.039 | <0.001 | <0.001 | |
| BL to 36 m | <0.001 | 0.001 | <0.001 | <0.001 | |
| Fractures/retention score 5 2 Cumulative failure rate (all criteria) | BL to 6 m | n. c. | n. c. | n. c. | 0.250 |
| BL to 12 m | n. c. | n. c. | 1.000 | 0.016 | |
| BL to 24 m | n. c. | n. c. | 1.000 | <0.001 | |
| BL to 36 m | 1.000 | 1.000 | 0.016F/R 0.008CFR | <0.001 |
| Parameter | iBU SE vs. SEE | iBU-SE vs. ER | iBU-SEE vs. ER | iBU-SE vs. OFL | iiBU-SEE vs. OFL | iBU-ER vs. OFL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | pi | % | pi | % | pi | % | pi | % | pi | % | pi | ||
| Marginal gap | BL | 1.5/0.0 | 0.125 | 1.5/0.2 | 0.125 | 0.0/0.2 | 0.250 | 1.5/2.5 | 0.426 | 0.0/2.5 | 0.008 | 0.2/2.5 | 0.027 |
| 6 m | 2.0/0.0 | 0.063 1 | 2.0/0.9 | 0.438 | 0.0/0.9 | 0.063 1 | 2.0/3.7 | 0.322 | 0.0/3.7 | 0.004 | 0.9/3.7 | 0.012 | |
| 12 m | 4.3/0.5 | 0.078 | 4.3/1.8 | 0.313 | 0.5/1.8 | 0.063 1 | 4.3/9.9 | 0.160 | 0.5/9.9 | 0.004 | 1.8/9.9 | 0.020 | |
| 24 m | 6.8/1.4 | 0.027 | 6.8/3.7 | 0.164 | 1.4/3.7 | 0.219 | 6.8/8.7 | 0.232 | 1.4/8.7 | 0.002 | 3.7/8.7 | 0.027 | |
| 36 m | 12.4/2.1 | 0.014 | 12.4/11.6 | 0.910 | 2.1/11.6 | 0.016 | 12.4/11.4 | 0.846 | 2.1/11.4 | 0.002 | 11.6/11.4 | 0.824 | |
| Perfect margin | BL | 31.7/49.3 | 0.024 | 31.7/41.5 | 0.147 | 49.3/41.5 | 0.275 | 31.7/38.1 | 0.240 | 49.3/38.1 | 0.278 | 41.5/38.1 | 0.465 |
| 6 m | 20.3/39.7 | 0.005 | 20.3/32.9 | 0.067 1 | 39.7/32.9 | 0.320 | 20.3/27.2 | 0.175 | 39.7/27.2 | 0.054 1 | 32.9/27.2 | 0.278 | |
| 12 m | 16.9/43.2 | 0.001 | 16.9/30.4 | 0.042 | 43.2/30.4 | 0.027 | 16.9/22.5 | 0.320 | 43.2/22.5 | 0.003 | 30.4/22.5 | 0.278 | |
| 24 m | 11.8/30.7 | 0.010 | 11.8/22.6 | 0.014 | 30.7/22.6 | 0.275 | 11.8/11.3 | 0.695 | 30.7/11.3 | 0.014 | 22.6/11.3 | 0.024 | |
| 36 m | 13.3/27.3 | 0.032 | 13.3/15.2 | 0.520 | 27.3/15.2 | 0.193 | 13.3/10.9 | 0.831 | 27.3/10.9 | 0.014 | 15.2/10.9 | 0.365 | |
| Parameter | iBU-ER Remaining vs. Lost | OFL Remaining vs. Lost | |||
|---|---|---|---|---|---|
| % | pi | % | pi | ||
| Marginal gap, % | BL | 0.1/0.5 | 0.581 | 3.4/2.6 | 0.494 |
| 6 m | 0.8/2.0 | 0.379 | 3.0/6.3 | 0.141 | |
| 12 m | 1.7/2.8 | 0.612 | 5.2/9.8 | 0.394 | |
| 24 m | 3.7/3.8 | 0.953 | 6.2/8.2 | 1.000 | |
| Perfect margin, % | BL | 40.4/44.5 | 0.740 | 42.5/43.0 | 0.856 |
| 6 m | 30.6/31.4 | 1.000 | 25.3/32.7 | 0.056 1 | |
| 12 m | 29.2/23.3 | 0.536 | 27.8/25.0 | 0.694 | |
| 24 m | 22.2/20.1 | 0.713 | 17.4/23.4 | 0.517 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haak, R.; Stache, G.; Schneider, H.; Häfer, M.; Schmalz, G.; Schulz-Kornas, E. Effect of the Adhesive Strategy on Clinical Performance and Marginal Integrity of a Universal Adhesive in Non-Carious Cervical Lesions in a Randomized 36-Month Study. J. Clin. Med. 2023, 12, 5776. https://doi.org/10.3390/jcm12185776
Haak R, Stache G, Schneider H, Häfer M, Schmalz G, Schulz-Kornas E. Effect of the Adhesive Strategy on Clinical Performance and Marginal Integrity of a Universal Adhesive in Non-Carious Cervical Lesions in a Randomized 36-Month Study. Journal of Clinical Medicine. 2023; 12(18):5776. https://doi.org/10.3390/jcm12185776
Chicago/Turabian StyleHaak, Rainer, Gesa Stache, Hartmut Schneider, Matthias Häfer, Gerhard Schmalz, and Ellen Schulz-Kornas. 2023. "Effect of the Adhesive Strategy on Clinical Performance and Marginal Integrity of a Universal Adhesive in Non-Carious Cervical Lesions in a Randomized 36-Month Study" Journal of Clinical Medicine 12, no. 18: 5776. https://doi.org/10.3390/jcm12185776