
Knee Arthrodesis with a Modular Silver-Coated Endoprosthesis for Infected Total Knee Arthroplasty with Extensive Bone Loss: A Retrospective Case-Series Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
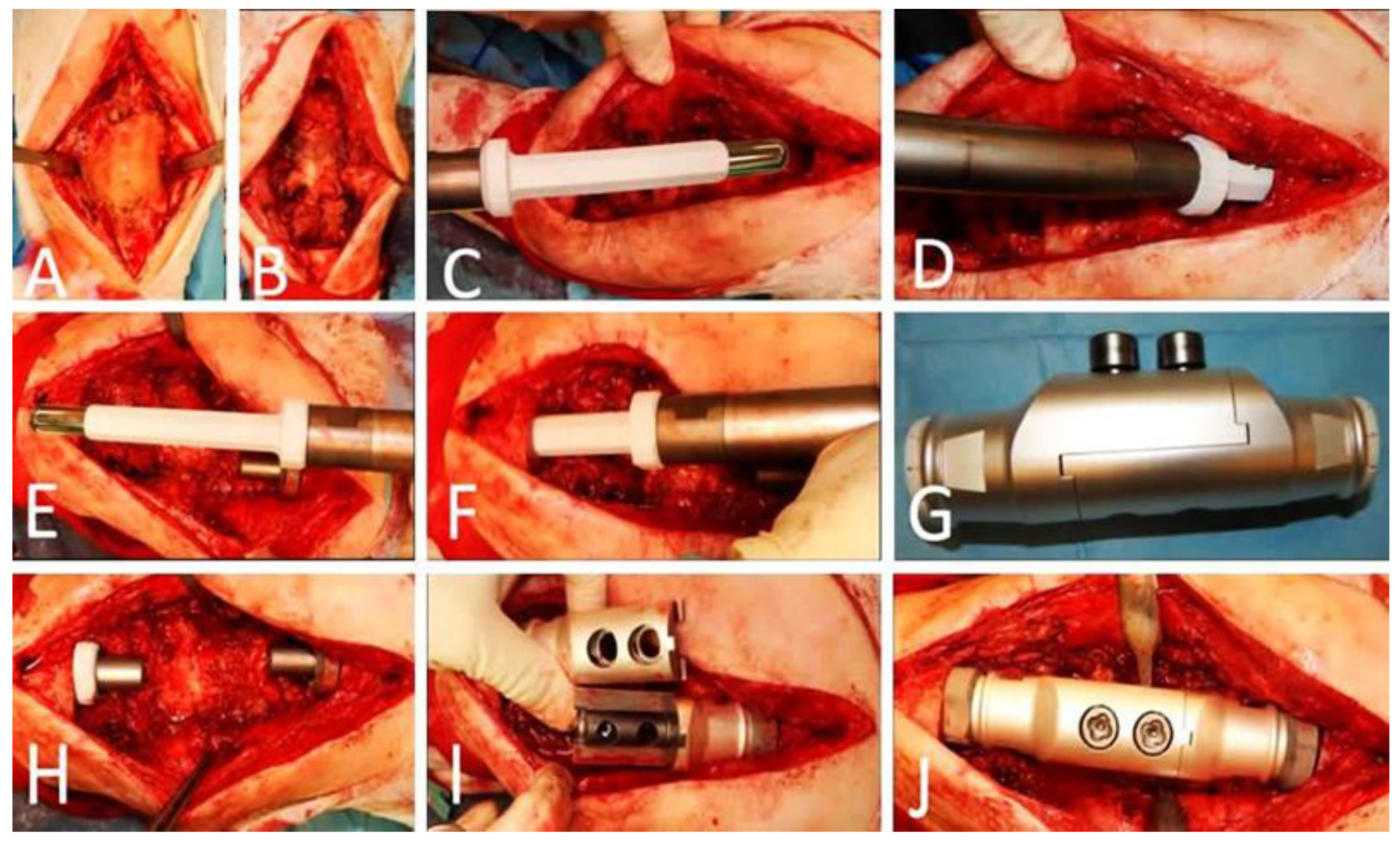
2.1. Technique
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical and Surgical Outcomes
4. Discussion
5. Conclusions
- Knee arthrodesis is an important alternative to amputation in infected and multiple revised TKA.
- It provides functional improvement and eradication of the infection.
- The application of silver-coated knee arthrodesis implants is associated with increased implant survivorship as well as with satisfactory mid-term clinical and patient-reported outcomes as the limb salvage procedure for failed infected TKA with significant bone loss and extensor tendon deficit.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watanabe, K.; Minowa, T.; Takeda, S.; Otsubo, H.; Kobayashi, T.; Kura, H.; Yamashita, T. Outcomes of knee arthrodesis following infected total knee arthroplasty: A retrospective analysis of 8 cases. Mod. Rheumatol. 2014, 24, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Emerson, R.H.; Muncie, M.; Tarbox, T.R.; Higgins, L.L. Comparison of a Static with a Mobile Spacer in Total Knee Infection. Clin. Orthop. Relat. Res. 2002, 404, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.S.; Masri, B.; Campbell, D.; McGraw, R.W.; Beauchamp, C.P.; Duncan, C.P. The PROSTALAC functional spacer in two-stage revision for infected knee replacements: Prosthesis of antibiotic loaded acrylic cement. J. Bone Jt. Surg. 2000, 82, 807–812. [Google Scholar] [CrossRef]
- Cochran, A.R.; Ong, K.L.; Lau, E.; Mont, M.A.; Malkani, A.L. Risk of Reinfection After Treatment of Infected Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 156–161. [Google Scholar] [CrossRef]
- Arroyo, J.S.; Garvin, K.L.; Neff, J.R. Arthrodesis of the Knee with a Modular Titanium Intramedullary Nail. J. Bone Jt. Surg. 1997, 79, 26–35. [Google Scholar] [CrossRef]
- Conway, J.D.; Mont, M.A.; Bezwada, H.P. Arthrodesis of the knee. J. Bone Jt. Surg. 2004, 86, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Capanna, R.; Biagini, R.; Ruggieri, P.; Bettelli, G.; Casadei, R.; Campanacci, M. Temporary resection-arthrodesis of the knee using an intramedullary rod and bone cement. Int. Orthop. 1989, 13, 253–258. [Google Scholar] [CrossRef]
- Robinson, M.; Piponov, H.I.; Ormseth, A.; Helder, C.W.; Schwartz, B.; Gonzalez, M.H. Knee Arthrodesis Outcomes After Infected Total Knee Arthroplasty and Failure of Two-stage Revision with an Antibiotic Cement Spacer. JAAOS Glob. Res. Rev. 2018, 2, e077. [Google Scholar] [CrossRef]
- Charnley, J.C. Positive pressure in arthrodesis of the knee joint. J. Bone Jt. Surg. Br. 1948, 30, 478–486. [Google Scholar] [CrossRef]
- Razii, N.; Abbas, A.M.I.; Kakar, R.; Agarwal, S.; Morgan-Jones, R. Knee arthrodesis with a long intramedullary nail as limb salvage for complex periprosthetic infections. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 907–914. [Google Scholar] [CrossRef]
- Lee, S.; Jang, J.; Seong, S.C.; Lee, M.C. Distraction arthrodesis with intramedullary nail and mixed bone grafting after failed infected total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Razii, N.; Kakar, R.; Morgan-Jones, R. Knee Arthrodesis in the Infected Total Knee Arthroplasty. In The Book the Infected Total Knee Arthroplasty; Springer: Berlin/Heidelberg, Germany, 2018; pp. 165–180. [Google Scholar]
- Gathen, M.; Schmolders, J.; Wimmer, M.D.; Gravius, N.; Randau, T.M.; Gravius, S.; Friedrich, M. Modular arthrodesis system TITAN (KAM-TITAN) after failed revision total knee arthroplasty: Operative technique and clinical experience. Oper. Orthop. Traumatol. 2020, 32, 58–72. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, D.E.; Rand, J. Intramedullary arthrodesis of the knee after failed total knee arthroplasty. J. Bone Jt. Surg. 1994, 76-A, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Corona, P.S.; Jurado, M.; Scott-Tennent, A.; Fraile, R.; Carrera, L.; Vicente, M. Uniplanar versus biplanar monolateral external fixator knee arthrodesis after end-stage failed infected total knee arthroplasty: A comparative study. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 815–825. [Google Scholar] [CrossRef]
- Charnley, J.; Lowe, H.G. A study of the end-results of compression arthrodesis of the knee. J. Bone Jt. Surg. 1958, 40-B, 633–635. [Google Scholar] [CrossRef]
- Oostenbroek, H.J.; Van Roermund, P.M. Arthrodesis of the knee after an infected arthroplasty using the Ilizarov method. J. Bone Jt. Surg. 2001, 83-B, 50–54. [Google Scholar] [CrossRef]
- Kuo, A.C.; Meehan, J.P.; Lee, M. Knee Fusion Using Dual Platings with the Locking Compression Plate. J. Arthroplast. 2005, 20, 772–776. [Google Scholar] [CrossRef]
- Balato, G.; Rizzo, M.; Ascione, T.; Smeraglia, F.; Mariconda, M. Re-infection rates and clinical outcomes following arthrodesis with intramedullary nail and external fixator for infected knee prosthesis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2018, 19, 361. [Google Scholar] [CrossRef]
- Klinger, H.-M.; Spahn, G.; Schultz, W.; Baums, M.H. Arthrodesis of the knee after failed infected total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 447–453. [Google Scholar] [CrossRef]
- Bartlett, W.; Vijayan, S.; Pollock, R.; Skinner, J.; Blunn, G.; Cannon, S.; Briggs, T. The Stanmore Knee Arthrodesis Prosthesis. J. Arthroplast. 2011, 26, 903–908. [Google Scholar] [CrossRef]
- White, S.P.; Porteous, A.J.; Newman, J.H.; Mintowt-Czyz, W.; Barr, V. Arthrodesis of the knee using a custom-made intramedullary coupled device. J. Bone Jt. Surg. 2003, 85, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Alt, V. Antimicrobial coated implants in trauma and orthopaedics—A clinical review and risk-benefit analysis. Injury 2017, 48, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Li, Y.; Huo, K.; Gao, B.; Xiong, W. Long-lasting in vivo and in vitro antibacterial ability of nanostructured titania coating incorporated with silver nanoparticles. J. Biomed. Mater. Res. Part A 2014, 102, 3488–3499. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Cao, H.; Zhao, Y.; Zhu, C.; Cheng, T.; Wang, Q.; Peng, X.; Cheng, M.; Wang, J.; Jin, G.; et al. In vitro and in vivo anti-biofilm effects of silver nanoparticles immobilized on titanium. Biomaterials 2014, 35, 9114–9125. [Google Scholar] [CrossRef] [PubMed]
- Schmolders, J.; Koob, S.; Schepers, P.; Pennekamp, P.H.; Gravius, S.; Wirtz, D.C.; Placzek, R.; Strauss, A.C. Lower limb reconstruction in tumor patients using modular silver-coated megaprostheses with regard to perimegaprosthetic joint infection: A case series, including 100 patients and review of the literature. Arch. Orthop. Trauma Surg. 2017, 137, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Wilding, C.P.; Cooper, G.A.; Freeman, A.K.; Parry, M.C.; Jeys, L. Can a Silver-Coated Arthrodesis Implant Provide a Viable Alternative to Above Knee Amputation in the Unsalvageable, Infected Total Knee Arthroplasty? J. Arthroplast. 2016, 31, 2542–2547. [Google Scholar] [CrossRef] [PubMed]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Infectious Diseases Society of America. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef]
- Papadopoulos, A.; Ribera, A.; Mavrogenis, A.F.; Rodriguez-Pardo, D.; Bonnet, E.; Salles, M.J.; del Toro, M.D.; Nguyen, S.; Blanco-García, A.; Skaliczki, G.; et al. Multidrug-resistant and extensively drug-resistant Gram-negative prosthetic joint infections: Role of surgery and impact of colistin administration. Int. J. Antimicrob. Agents 2019, 53, 294–301. [Google Scholar] [CrossRef]
- Johnson, E.W. Visual Analog Scale (VAS). Am. J. Phys. Med. Rehabilitation 2001, 80, 717. [Google Scholar] [CrossRef]
- Henderson, E.R.; Groundland, J.S.; Pala, E.; Dennis, J.A.; Wooten, R.; Cheong, D.; Windhager, R.; Kotz, R.I.; Mercuri, M.; Funovics, P.T.; et al. Failure Mode Classification for Tumor Endoprostheses: Retrospective Review of Five Institutions and a Literature Review. J. Bone Jt. Surg. 2011, 93, 418–429. [Google Scholar] [CrossRef]
- Zardi, E.M.; Franceschi, F. Prosthetic joint infection. A relevant public health issue. J. Infect. Public Health 2020, 13, 1888–1891. [Google Scholar] [CrossRef]
- Lichstein, P.; Su, S.; Hedlund, H.; Suh, G.; Maloney, W.J.; Goodman, S.B.; Huddleston, J.I. Treatment of Periprosthetic Knee Infection with a Two-stage Protocol Using Static Spacers. Clin. Orthop. Relat. Res. 2016, 474, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Somayaji, H.S.; Tsaggerides, P.; Ware, H.E.; Dawd, G.S.E. Knee arthrodesis—A review. Knee 2008, 15, 247–254. [Google Scholar] [CrossRef]
- Rand, J.A.; Bryan, R.S. The outcome of failed knee arthrodesis following total knee arthroplasty. Clin. Orthop. Relat. Res. 1986, 205, 86–92. [Google Scholar] [CrossRef]
- Rao, M.; Richards, O.; Meyer, C.; Jones, R.S. Knee stabilisation following infected knee arthroplasty with bone loss and extensor mechanism impairment using a modular cemented nail. Knee 2009, 16, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Iacono, F.; Bruni, D.; Presti, M.L.; Raspugli, G.; Bondi, A.; Sharma, B.; Marcacci, M. Knee arthrodesis with a press-fit modular intramedullary nail without bone-on-bone fusion after an infected revision TKA. Knee 2012, 19, 555–559. [Google Scholar] [CrossRef]
- Putman, S.; Kern, G.; Senneville, E.; Beltrand, E.; Migaud, H. Knee arthrodesis using a customised modular intramedullary nail in failed infected total knee arthroplasty. Orthop. Traumatol. Surg. Res. 2013, 99, 391–398. [Google Scholar] [CrossRef]
- Scarponi, S.; Drago, L.; Romanò, D.; Logoluso, N.; Peccati, A.; Meani, E.; Romanò, C.L. Cementless modular intramedullary nail without bone-on-bone fusion as a salvage procedure in chronically infected total knee prosthesis: Long-term results. Int. Orthop. 2014, 38, 413–418. [Google Scholar] [CrossRef]
- Gallusser, N.; Goetti, P.; Luyet, A.; Borens, O. Knee arthrodesis with modular nail after failed TKA due to infection. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 1307–1312. [Google Scholar] [CrossRef]
- Faure, P.-A.; Putman, S.; Senneville, E.; Beltrand, E.; Behal, H.; Migaud, H. Knee arthrodesis using a custom modular intramedullary nail in failed, infected knee arthroplasties: A concise follow-up note of 31 cases at a median of 13 years post-arthrodesis. Orthop. Traumatol. Surg. Res. 2021, 107, 102898. [Google Scholar] [CrossRef]
- Mayes, W.H.; Severin, A.C.; Mannen, E.M.; Edwards, P.K.; Barnes, C.L.; Stambough, J.B.; Mears, S.C. Management of Periprosthetic Joint Infection and Extensor Mechanism Disruption with Modular Knee Fusion: Clinical and Biomechanical Outcomes. Arthroplast. Today 2021, 8, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Stavrakis, A.I.; Mayer, E.N.; Devana, S.K.; Chowdhry, M.; Dipane, M.V.; McPherson, E.J. Outcomes of Modular Knee Arthrodesis for Challenging Periprosthetic Joint Infections. Arthroplast. Today 2022, 13, 199–204. [Google Scholar] [CrossRef]
- Angelini, A.; Henderson, E.; Trovarelli, G.; Ruggieri, P. Is There a Role for Knee Arthrodesis with Modular Endoprostheses for Tumor and Revision of Failed Endoprostheses? Clin. Orthop. Relat. Res. 2013, 471, 3326–3335. [Google Scholar] [CrossRef] [PubMed]
- Savvidou, O.D.; Kaspiris, A.; Trikoupis, I.; Kakouratos, G.; Goumenos, S.; Melissaridou, D.; Papagelopoulos, P.J. Efficacy of antimicrobial coated orthopaedic implants on the prevention of periprosthetic infections: A systematic review and meta-analysis. J. Bone Jt. Infect. 2020, 5, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Fabritius, M.; Al-Munajjed, A.A.; Freytag, C.; Jülke, H.; Zehe, M.; LeMarchand, T.; Arts, J.J.; Schumann, D.; Alt, V.; Sternberg, K. Antimicrobial Silver Multilayer Coating for Prevention of Bacterial Colonization of Orthopedic Implants. Materials 2020, 13, 1415. [Google Scholar] [CrossRef] [PubMed]
- Diez-Escudero, A.; Hailer, N.P. The role of silver coating for arthroplasty components. Bone Jt. J. 2021, 103-B, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Donati, F.; Di Giacomo, G.; D’adamio, S.; Ziranu, A.; Careri, S.; Rosa, M.; Maccauro, G. Silver-Coated Hip Megaprosthesis in Oncological Limb Savage Surgery. BioMed Res. Int. 2016, 2016, 9079041. [Google Scholar] [CrossRef]
- Hardes, J.; Ahrens, H.; Gebert, C.; Streitbuerger, A.; Buerger, H.; Erren, M.; Gunsel, A.; Wedemeyer, C.; Saxler, G.; Winkelmann, W. Lack of toxicological side-effects in silver-coated megaprostheses in humans. Biomaterials 2007, 28, 2869–2875. [Google Scholar] [CrossRef]
- Zajonz, D.; Birke, U.; Ghanem, M.; Prietzel, T.; Josten, C.; Roth, A.; Fakler, J.K. Silver-coated modular Megaendoprostheses in salvage revision arthroplasty after periimplant infection with extensive bone loss—A pilot study of 34 patients. BMC Musculoskelet. Disord. 2017, 18, 383. [Google Scholar] [CrossRef]
- Gosheger, G.; Hardes, J.; Ahrens, H.; Streitburger, A.; Buerger, H.; Erren, M.; Gunsel, A.; Kemper, F.H.; Winkelmann, W.; Von Eiff, C. Silver-coated megaendoprostheses in a rabbit model—An analysis of the infection rate and toxicological side effects. Biomaterials 2004, 25, 5547–5556. [Google Scholar] [CrossRef]
- Scoccianti, G.; Frenos, F.; Beltrami, G.; Campanacci, D.A.; Capanna, R. Levels of silver ions in body fluids and clinical results in silver-coated megaprostheses after tumour, trauma or failed arthroplasty. Injury 2016, 47 (Suppl. S4), S11–S16. [Google Scholar] [CrossRef]
- Ismat, A.; Alt, V.; Heiss, C.; Rupp, M. Limb-saving Knee Arthrodesis with a Silver-coated Arthrodesis Rod in a Patient with Aspergillus Osteomyelitis of the Knee. Strat. Trauma Limb Reconstr. 2020, 15, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Indrayan, A.; Mishra, A. The importance of small samples in medical research. J. Postgrad. Med. 2021, 67, 219–223. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Gender | Age (Years) | BMI (kg/m2) | Soft Tissue Coverage | Follow-Up (Months) | Clinical Outcome | Limb Length Discrepancy (cm) | VAS (0–5) | OKS |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 66 | 24 | Adequate | 59 | Success–Supression | 2 | 3 | 42 |
| 2 | M | 73 | 27 | Adequate | 24 | Success | 1.5 | 1 | 24 |
| 3 | F | 62 | 29 | Gastrocnemius flap | 36 | Failure | 3 | 3 | 47 |
| 4 | F | 70 | 27 | Adequate | 27 | Success–Supression | 3 | 3 | 44 |
| 5 | M | 57 | 31 | Gastrocnemius flap | 24 | Success | 2 | 2 | 31 |
| 6 | F | 72 | 30 | Adequate | 29 | Success | 1.5 | 2 | 28 |
| 7 | F | 75 | 22 | Adequate | 25 | Success | 1.5 | 1 | 27 |
| 8 | F | 61 | 27.5 | Adequate | 26 | Success | 1.5 | 2 | 27 |
| Study | Country | Number of pts * | Age (y.o) | Infecting Organism Isolated | Type of Modular Arthrodesis Prosthesis | Outcomes |
|---|---|---|---|---|---|---|
| Rao et al. 2009 [36] | United Kingdom | 7 | 72.3 (64–86) | 2 pts with S. aureus, Staphylococcus sciuri, Coag negative staph, 2 pts with more than one organisms | Endo-Model® Knee Fusion Nail (Newsplint, UK/Waldemar Link®, GmbH & Co. KG, Hamburg, Germany) | 4 pts with complete relief from their pain, VAS pain score improved from a mean of 7.9 (7.5–9.2) pre-operatively to 1.5 (0–6.4) postoperatively, 2 pts required revision (the first due to fracture in cement mantle of the femoral component, the second due to infection and insufficient fracture of the femoral shaft), infection recurrence 14.3% |
| Bartlett et al. 2011 [21] | United Kingdom | 10 *** | 51.5 (35–70) | Not Applicable | Stanmore knee arthrodesis (Stanmore Implants Worldwide, Middlesex, UK) | In total, 1 pt died 24 months post-op (not related to procedure), 1 pt above the knee amputation, 1 pt with fracture of the growing mechanism shaft. Among 9 pts with PJI, 1 pt with recurrent infection, 1 pt with wound dehiscence, independently immobilize, improvement of pain |
| Iacono, et al. 2012 [37] | Italy | 22 | 69.3 (53–85) | Not Applicable | Link nail (Link Laboratory, Hamburg, Germany | 3 pts with recurrent infection -(2 of whom underwent amputation), 8 of the rest 8 patients (38.09%) with no pain (VAS = 0), 5 pts (23.8%) with score of 1, 3 pts (14.28%) with score of 2, 1 (4.7%) scored 3, 1 pt with 8 score (mean VAS 1.2), 1 intraoperative shaft fracture, 90% of the pts satisfied with the result. Infection recurrence 14.3% |
| Putman, et al. 2013 [38] | France | 31 | 67 (48–80) | S. aureus in 10 cases (including 1 case with methicillin-resistant SA [MRSA]), coagulase-negative Staphylococcus (CNS) in six cases (including 1 with methicillin-resistant CNS [MRCNS]). In 7 (22.5%) pts several organisms | Customized dual-component arthrodesis nail (Link EndoModelTM, Boves, France) | In 3 pts sinus tracts with recurrent clinical infection, required revision surgery, residual pain without recurrent infection in 14 patients, dissatisfaction in 22 pts, 3 of them died more than 24 months after the knee arthrodesis. None of the pts required amputation for uncontrolled infection. 67% bone union achieved. 26 % recurrent infection(required revision) |
| Scarponi, et al. 2014 [39] | Italy | 38 | 65 (46–82) | S. aureus in 19 cases, 10 with MRSA), coagulase-negative Staphylococci in 12 patients (five methicillin resistant), Streptococcus spp. in 5 pts, P. aeruginosa in 3, Enterobacter spp. In 3, Escherichia coli in 3, Enterococcus faecalis in 3 | Endo-Model® Knee Fusion Nail SK Modular System®, Waldemar-Link, Hamburg, Germany | At a two-year follow-up, 4 pts with infection recurrence, 2 of whom underwent above-knee amputation. 2 of the rest with pain in the operated leg at rest, 20 pts without or very mild pain, 9 with moderate pain and 5 with more severe pain. |
| Galluser, et al. 2015 [40] | Switzerland | 15 | 67 (42–87) | Not Applicable | Wichita Fusion NailR | Mean follow up of 33 months. 9 with primary fusion (75%), 3 pts needed a surgical revision for non-union or wound dehiscence, 1 with peroneal nerve palsy. Infection rate 0% |
| Wilding, et al. 2016 [27] | United Kingdom | 8 | 64.9 (55–75) | 7/8 organism isolation prior arthrodesis, 3 with polymicrobial, 1 pt with rifampicin resistant strain of gram positive Staphylococcus | RS Arthrodesis 90 Implant, Implantcast, Buxtehude, Germany | 1 pt lost to follow up, 37.5% post-op complications, 2 pt with re-operation recurrent infection (1 with superficial collection, improvement in pain, mobilization from seated, no change in kneeling (inability pre-operatively) |
| Faure, et al. 2020 [41] ** | France | 31 | 67 (48–80) | 62% same bacteria during revisions (5 of 8 cases with revision) | Customized dual-component arthrodesis nail (Link EndoModelTM, Boves, France) | Median follow-up of 158 months (138–163), no mechanical failures (implant breakage or aseptic loosening). 8 pts (26%) undergo revision surgery (all had infections) (2 since 2012). In 5 pts (16%) implants change, 3 pts (10%) need debridement and lavage before suppressive antibiotics. 16 % incidence of implant change and surgical revision at 10 years. 16 pts died in total. |
| Mayes, et al. 2020 [42] | USA | 15 | 68.5 (45–85) | None in 4 cases, one pathogen in 8 cases (P.mirabilis, Oxacillin-resistant Staphylococcus aureus, Group B Streptococcus, P. aeruginosa, S. epidermidis, Enterobacter cloacae Enterobacter cloacae, Streptococcus), more than 1 in 2 cases | 14 pts * with Stryker (Kalamazoo, MI) GMRS system, 1 pt with a Biomet (Warsaw, IN) Orthopedic Salvage System modular KF | 2 of the pts died postoperatively (one immediately from pulmonary embolism, due to cement embolization, one opted for AKA (unhappy with the result), none of the pts * with clinical signs of persistent or recurrent infection, and no one on suppressive antibiotics. |
| Stavrakis, et al. 2022 [43] | USA | 81 | 67 (45–84) | S. epidermidis most common organism (22.2% of cases), 18.5% with S. aureus (60% methicillin-sensitive Staphylococcus aureus, 40% methicillin-resistant Staphylococcus aureus). 11% of patients with multiorganism infection, 11.1% culture-negative | OSS Modular Arthrodesis System, Zimmer Biomet, Warsaw, IN | 17% with persistent infection or reinfection, 7.4 % of them underwent above knee amputation, knee function unchanged based, did get worse clinically. Over 80% of pts underwent reimplantation and endoprosthetic reconstruction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savvidou, O.D.; Kaspiris, A.; Goumenos, S.; Trikoupis, I.; Melissaridou, D.; Kalogeropoulos, A.; Serenidis, D.; Georgoulis, J.-D.; Lianou, I.; Koulouvaris, P.; et al. Knee Arthrodesis with a Modular Silver-Coated Endoprosthesis for Infected Total Knee Arthroplasty with Extensive Bone Loss: A Retrospective Case-Series Study. J. Clin. Med. 2023, 12, 3600. https://doi.org/10.3390/jcm12103600
Savvidou OD, Kaspiris A, Goumenos S, Trikoupis I, Melissaridou D, Kalogeropoulos A, Serenidis D, Georgoulis J-D, Lianou I, Koulouvaris P, et al. Knee Arthrodesis with a Modular Silver-Coated Endoprosthesis for Infected Total Knee Arthroplasty with Extensive Bone Loss: A Retrospective Case-Series Study. Journal of Clinical Medicine. 2023; 12(10):3600. https://doi.org/10.3390/jcm12103600
Chicago/Turabian StyleSavvidou, Olga D., Angelos Kaspiris, Stavros Goumenos, Ioannis Trikoupis, Dimitra Melissaridou, Athanasios Kalogeropoulos, Dimitris Serenidis, Jim-Dimitris Georgoulis, Ioanna Lianou, Panagiotis Koulouvaris, and et al. 2023. "Knee Arthrodesis with a Modular Silver-Coated Endoprosthesis for Infected Total Knee Arthroplasty with Extensive Bone Loss: A Retrospective Case-Series Study" Journal of Clinical Medicine 12, no. 10: 3600. https://doi.org/10.3390/jcm12103600