
Chest Drainage Therapy: What Comes out of Pandora’s Box Can Affect Patient Outcomes
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. How Air Moves along the Entire UWSD System (Wet-Wet and Wet-Dry CDUs)
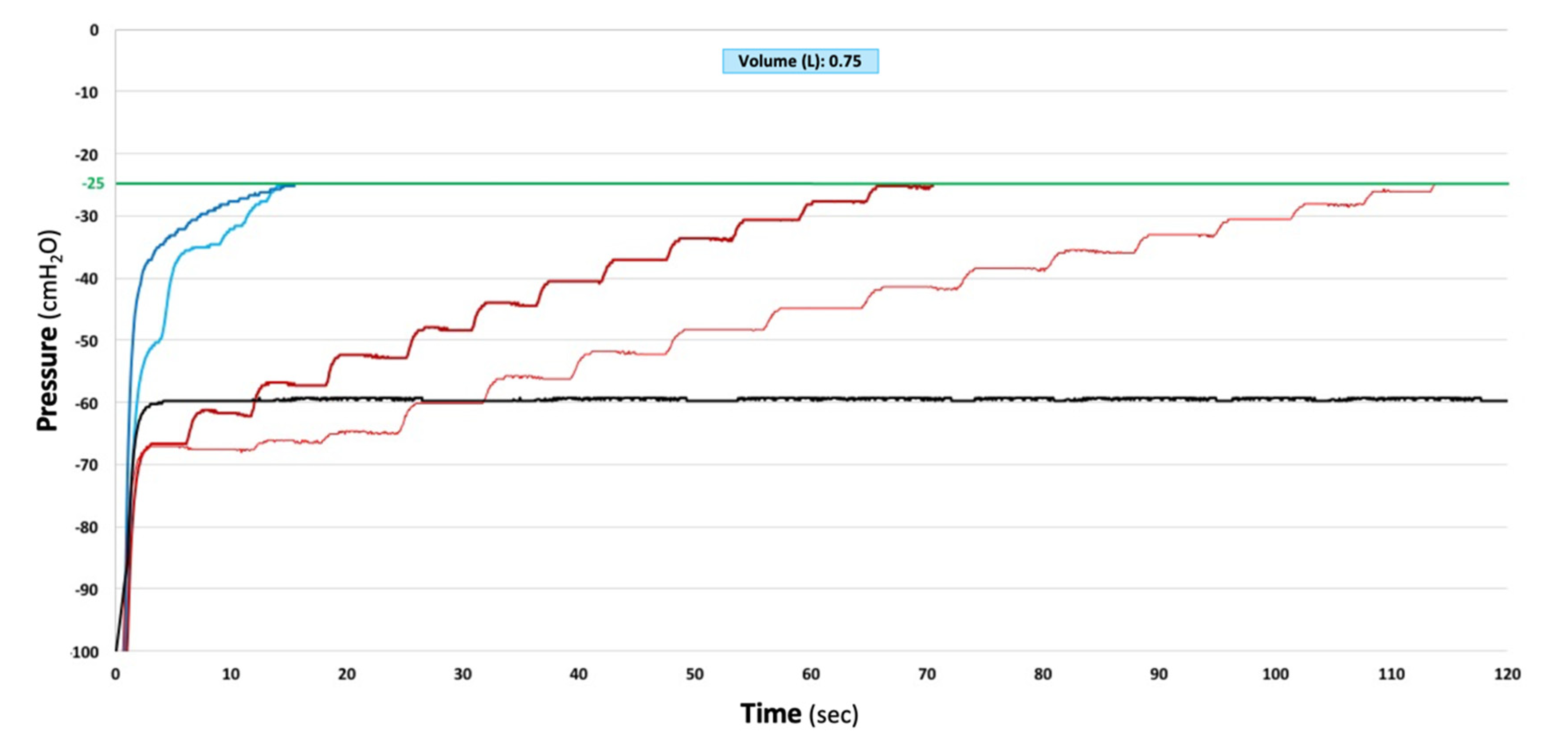
3.2. How CDUs Manage the Build-Up of Large Negative Intrapleural Pressure
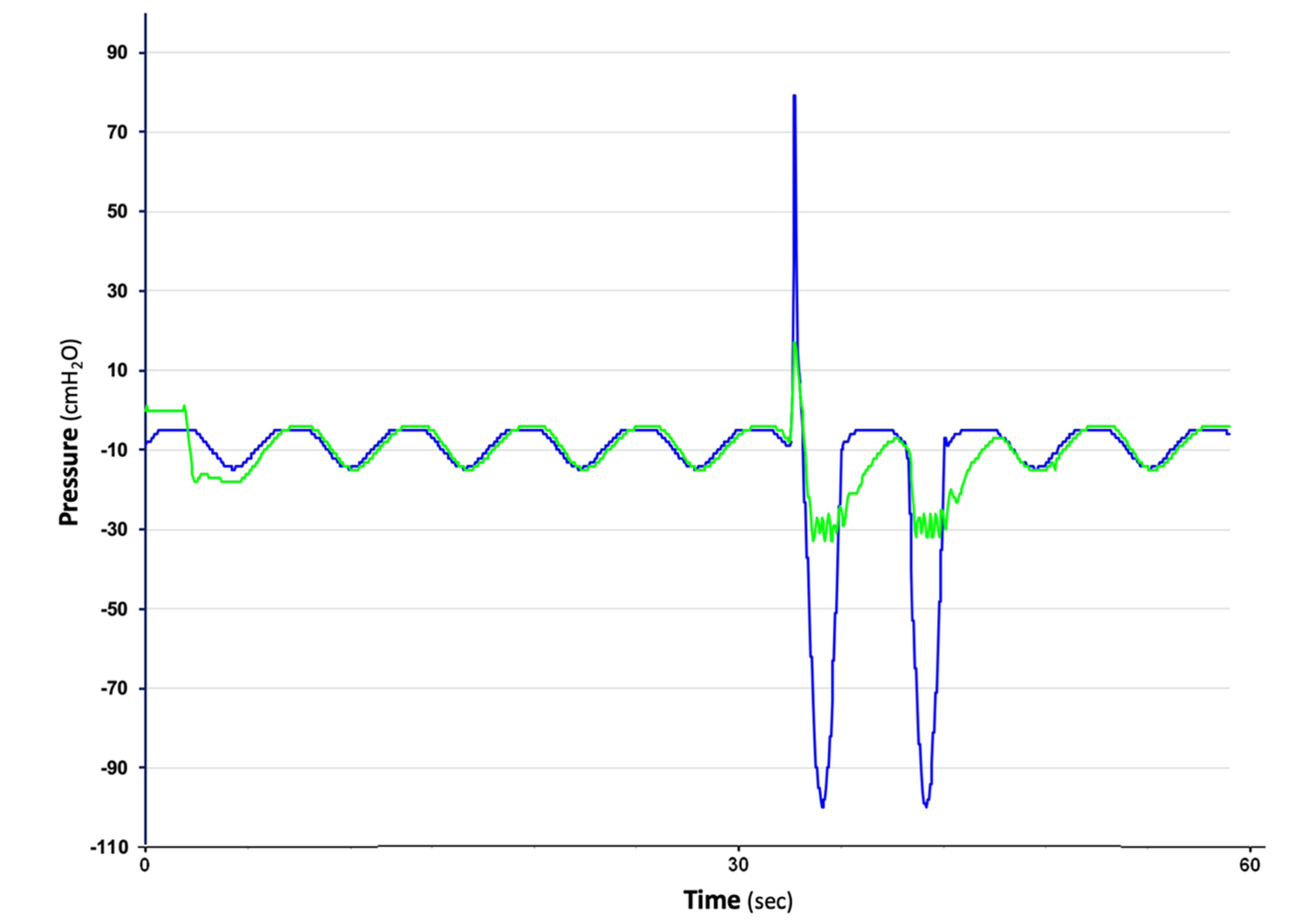
3.3. How CDUs Manage the Accumulation of Positive Intrapleural Pressure
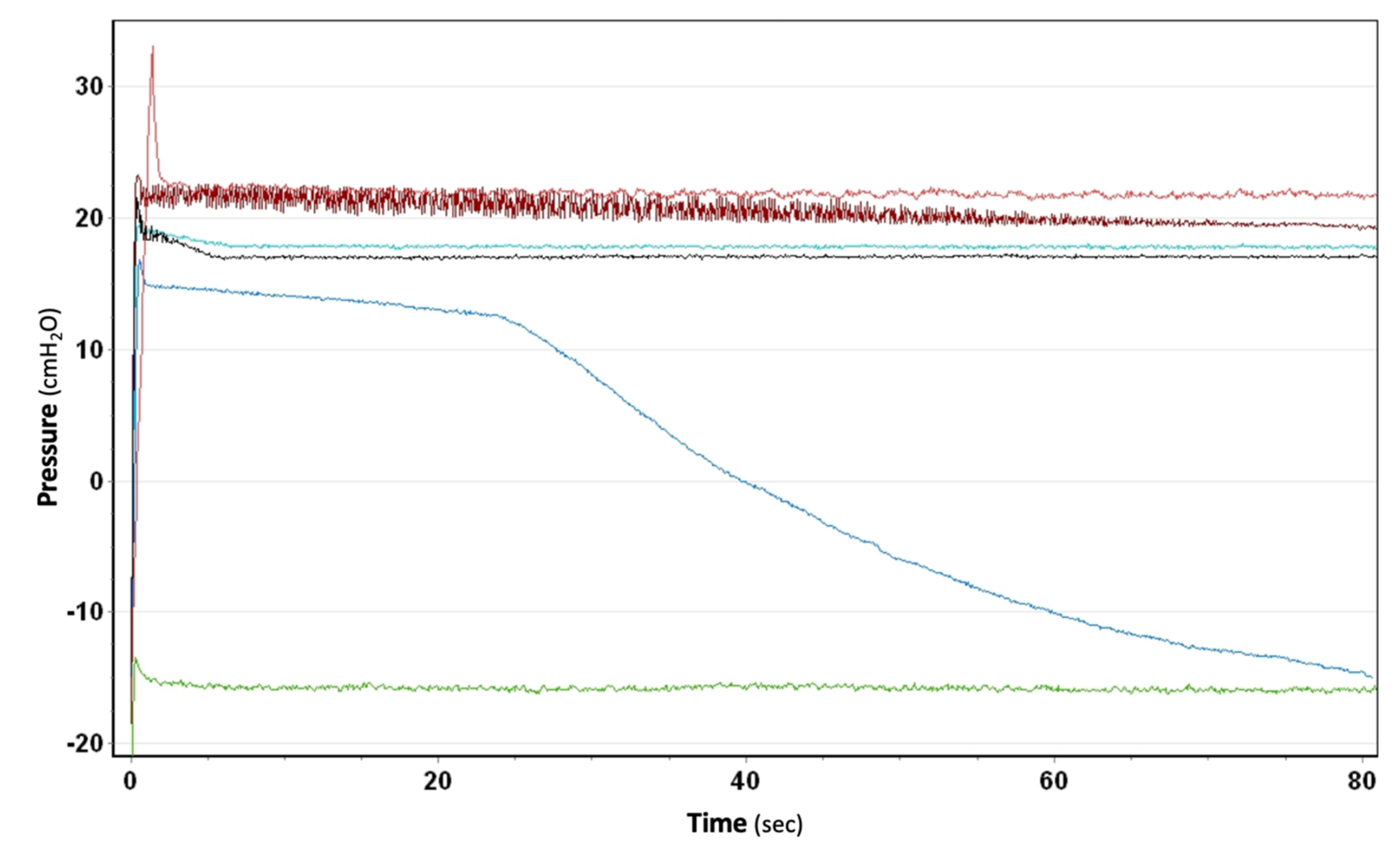
3.4. How Suction Is Generated and Whether the Set Amount Is Effectively Maintained through the Canister, Even in the Presence of Air Leaks
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Batchelder, T.L.; Morris, K.A. Critical factors in determining adequate pleural drainage in both the operated and non-operated chest. Am. Surg. 1962, 2, 296–302. [Google Scholar]
- Enerson, D.M.; McIntyre, R.N. A comparative study of the physiology and physics of pleural drainage systems. J. Thorac. Cardiovasc. Surg. 1966, 5, 40–46. [Google Scholar] [CrossRef]
- Rusch, V.W.; Capps, J.S.; Tyler, M.L.; Pierson, D.L. The Performance of Four Pleural Drainage Systems in an Animal Model of Bronchopleural Fistula. Chest 1988, 93, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Baumann, M.H.; Patel, P.B.; Roney, C.W.; Petrini, M.F. Comparison of Function of Commercially Available Pleural Drainage Units and Catheters. Chest 2003, 123, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Munnell, E.R. Thoracic Drainage. Ann. Thorac. Surg. 1997, 63, 1497–1502. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Medical Devices: Managing the Mismatch. An Outcome of the Priority Medical Devices Project; WHO (World Health Organization): Geneva, Switzerland, 2010.
- ISO 10079-1; Medical Suction Equipment—Part 1: Electrically Powered Suction Equipment. ISO: Geneva, Switzerland, 2022.
- Zisis, C.; Tsirgogianni, K.; Lazaridis, G.; Lampaki, S.; Baka, S.; Mpoukovinas, I.; Karavasilis, V.; Kioumis, I.; Pitsiou, G.; Katsikogiannis, N.; et al. Chest Drainage Systems in Use. Ann. Trasl Med. 2015, 3, 43. [Google Scholar]
- FDA. Make Sure the Medical Device You Choose Is Designed for You; FDA: Silver Spring, MD, USA, 2017.
- Dernevik, L. Extreme Negative Intrathoracis Pressure. Eur. J. Cardiothorac. Surg. 1999, 15, 225–226. [Google Scholar]
- Barnas, G.M.; Gilbert, T.B.; Krasna, M.J.; McGinley, M.J.; Fiocco, M.; Orens, J.B. Acute Effects of Bilateral Lung Volume Reduction Surgery on Lung and Chest Wall Mechanical Properties. Chest 1998, 114, 61–68. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J.; Collino, F.; Maiolo, G.; Rapetti, F.; Tonetti, T.; Vasques, F.; Quintel, M. The future of mechanical ventilation: Lessons from the present and the past. Critical. Care. 2017, 21, 183. [Google Scholar] [CrossRef]
- Bar-El, Y.; Ross, A.; Kablawi, A.; Egenburg, S. Potentially Dangerous Negative Intrapleural Pressures Generated by Ordinary Pleural Drainage Systems. Chest 2001, 119, 511–514. [Google Scholar] [CrossRef]
- Duncan, C.; Erickson, R. Pressures Associated with Chest Tube Stripping. Heart Lung 1982, 11, 166–171. [Google Scholar] [PubMed]
- Stouby, A.; Neckelmann, K.; Licht, P.B. Reverse airflow in certain chest drains may be misinterpreted as prolonged air leakage. World J. Surg. 2011, 35, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, J.; Lijkendijk, M.; Licht, P.B.; Stenger, M. New chest drainage unit with integrated CO2-detector demonstrates false air leak. Surg. Innov. 2021, 29, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Roe, B.B. Physiologic Principles of Drainage of the Pleural Space. With Special Reference to High Flow, High Vacuum Suction. Am. J. Surg. 1958, 96, 246–253. [Google Scholar] [CrossRef]
- Kam, A.C.; O’Brien, M.; Kam, P.C.A. Pleural Drainage Systems. Anaesthesia 1993, 48, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Dernevik, L.; Belboul, A.; Rådberg, G. Initial Experience with the World’s First Digital Drainage System. The Benefits of Recording Air Leaks with Graphic Representation. Eur. J. Cardiothorac. Surg. 2007, 31, 209–213. [Google Scholar] [CrossRef]
- Cerfolio, R. Clinical Use of a Digital Air Leak System. 2008. Available online: https://www.ctsnet.org/article/clinical-use-digital-air-leak-system (accessed on 4 July 2022).
- Marasco, R.D.; Giudice, G.; Lequaglie, C. How to distinguish an active air leak from a pleural space effect. Asian Cardiovasc Thorac Ann. 2012, 20, 682–688. [Google Scholar] [CrossRef]
- Miller, K.S.; Sahn, S.A. Chest Tubes. Indications, Technique, Management and Complications. Chest 1987, 91, 258–264. [Google Scholar] [CrossRef]
- Boggs, D.; Kinasewitz, G.T. Pathophysiology of the Pleural Space. Am. J. Med. Sci. 1995, 309, 53–59. [Google Scholar] [CrossRef]
- Poledna, M. A mercury manometer with a signal device for control of negative pressure in the pleural cavity after lung operations. Rozhl Chir. 1962, 41, 410–412. [Google Scholar]
- Capps, J.S.; Tyler, M.L.; Rusch, V.W.; Pierson, D.J. Potential of chest drainage units to evacuate bronchopleural air leaks. Chest 1985, 88, 57S. [Google Scholar]
- Powner, D.J.; Cline, C.D.; Rodman, G.H., Jr. Effect of chest-tube suction on gas flow through a bronchopleural fistula. Crit. Care Med. 1985, 13, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Manzanet, G.; Vela, A.; Corell, R.; Morón, R.; Calderón, R.; Suelves, C. A Hydrodynamic Study of Pleural Drainage Systems. Some Practical Consequences. Chest 2005, 127, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Dernevik, L. Kniven i Bröstet igen: Äventyr med Thoraxkirurgi; Books on Demand Gmbh: Norderstedt, Germany, 2021. [Google Scholar]
- Walcott-Sapp, S.; Sukumar, M.; A History of Thoracic Drainage: From Ancient Greeks to Wound Sucking Drummers to Digital Monitoring. CTSNet 2015. Available online: https://www.ctsnet.org/article/history-thoracic-drainage-ancient-greeks-wound-sucking-drummers-digital-monitoring (accessed on 4 July 2022).
- Grègoire, J.; Deslauriers, J. Surgical techniques in the pleura. Closed drainage and suction systems. In Thoracic Surgery, 2nd ed.; Griffith Pearson, F., Ed.; Churchill Livingstone: New York, NY, USA, 2002; pp. 1281–1300. [Google Scholar]
- Woolf, S.H.; Grol, R.; Hutchinson, A.; Eccles, M.; Grimshaw, J. Potential benefits, limitations, and harms of clinical guidelines. BMJ 1999, 318, 527–530. [Google Scholar] [CrossRef]
- Correa, V.C.; Lugo-Agudelo, L.H.; Aguirre-Acevedo, D.C.; Contreras, J.A.; Borrero, A.M.; Patiño-Lugo, D.F.; Valencia, D.A. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: A systematic metareview. Health Res. Policy Syst. 2020, 18, 74. [Google Scholar] [CrossRef]
- French, D.G.; Dilena, M.; LaPlante, S.; Shamji, F.; Sundaresan, S.; Villeneuve, J.; Seely, A.; Maziak, D.; Gilbert, S. Optimizing postoperative care protocols in thoracic surgery: Best evidence and new technology. J. Thorac. Dis. 2016, 8 (Suppl. 1), S3–S11. [Google Scholar]
- Hashmi, U.; Nadeem, M.; Aleem, A.; Khan, F.U.; Gull, R.; Ullah, K.; Khan, I.H. Dysfunctional Closed Chest Drainage—Common Causative Factors and Recommendations for Prevention. Cureus 2018, 10, e2295. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. MAUDE Adverse Event Report: Covidien Aqua-Seal CDU Chest Drainage Kit; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2018.
- Brunelli, A.; Beretta, E.; Cassivi, S.D.; Cerfolio, R.J.; Detterbeck, F.; Kiefer, T.; Miserocchi, G.; Shrager, J.; Singhal, S.; Van Raemdonck, D.; et al. Consensus definitions to promote an evidence-based approach to management of the pleural space. A collaborative proposal by ESTS, AATS, STS, and GTSC. Eur. J. Cardiothorac. Surg. 2011, 40, 291–297. [Google Scholar] [CrossRef]
- Detsky, A.S. Sources of bias for authors of clinical practice guidelines. CMAJ 2006, 175, 1033. [Google Scholar] [CrossRef]
- Jureidini, J.; McHenry, L.B. The illusion of evidence based medicine. BMJ 2022, 376, o702. [Google Scholar] [CrossRef]
- Novella, S. Announcing the Science-Based Medicine Blog. 2008. Available online: https://sciencebasedmedicine.org/hello-world/ (accessed on 4 July 2022).
- Gorski, S. “Hard science” and Medical School. 2010. Available online: https://sciencebasedmedicine.org/hard-science-and-medical-school/ (accessed on 4 July 2022).
- Ingraham, P. Why “Science”-Based Instead of “Evidence”-Based? 2014. Available online: https://www.painscience.com/articles/ebm-vs-sbm.php (accessed on 4 July 2022).
- Lijkendijk, M.; Licht, P.B.; Neckelmann, K. Electronic versus traditional chest tube drainage following lobectomy: A randomized trial. Eur. J. Cardiothorac. Surg. 2015, 48, 893–898. [Google Scholar] [CrossRef]
- Gao, S.; Zhang, Z.; Aragón, J.; Brunelli, A.; Cassivi, S.; Chai, Y.; Chen, C.; Chen, C.; Chen, G.; Chen, H.; et al. The Society for Translational Medicine: Clinical practice guidelines for the postoperative management of chest tube for patients undergoing lobectomy. J. Thorac. Dis. 2017, 9, 3255–3264. [Google Scholar] [CrossRef]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Hu, K.; Judson, M.A.; Fabian, T.; Nabagiez, J.P.; Feustel, P.J.; Fantauzzi, J.; Chieng, H.; Austin, A.; Vancavage, R.; et al. Association between Drainage—Dependent Prolonged Air Leak after Partial Lung Resection and Clinical Outcomes: A Prospective Cohort Study. Ann. Thorac. Surg. 2021, 19, 389–398. [Google Scholar] [CrossRef]
- Kaya, G.K. Rational Decision-Making in Purchasing Medical Devices. 2021. Available online: http://ieomsociety.org/proceedings/2021rome/384.pdf (accessed on 4 July 2022).
- Salmasi, S.; Ming, L.C.; Khan, T.M. Interaction and medical inducement between pharmaceutical representatives and physicians: A meta-synthesis. J. Pharm. Policy Pract. 2016, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Fickweiler, F.; Fickweiler, W.; Urbach, E. Interactions between physicians and the pharmaceutical industry generally and sales representatives specifically and their association with physicians’ attitudes and prescribing habits: A systematic review. BMJ 2017, 7, e016408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, Q.; Hutchison, K.; Johnson, J.; Blakely, B.; Clay-Wlliams, R.; Richards, B.; Rogers, W.A. Device representatives in hospitals: Are commercial imperatives driving clinical decision-making? J. Med. Ethics 2018, 44, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Aramal-Gracia, S. Medical Device Companies and Doctors: Do Their Interactions Affect Medical Treatments? ECARES Working Paper, European Center for Advanced Research in Economics and Statistics. 2020. Available online: https://ideas.repec.org/p/yor/hectdg/22-10.html (accessed on 4 July 2022).
- Pecchia, L.; Pallikarakis, N.; Magjarevic, R.; Iadanza, E. Health Technology Assessment and Biomedical Engineering: Global trends, gaps and opportunities. Med. Eng. Phys. 2019, 72, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Sanger, T. Health, Technology and Engineering. University of Southern California. Available online: https://catalogue.usc.edu/preview_program.php?catoid=11&poid=10864 (accessed on 4 July 2022).
- Beckmann, J.S.; Lew, D. Reconciling evidence-based medicine and precision medicine in the era of big data: Challenges and opportunities. Genome Med. 2016, 8, 134. [Google Scholar] [CrossRef]
- Elemento, O. The future of precision medicine: Towards a more predictive personalized medicine. Emerg Top. Life Sci. 2020, 4, 175–177. [Google Scholar]
- Kohler, S. Precision Medicine—Moving away from one-size-fits-all. In Quest: Science for South Africa; Academy of Science of South Africa: Pretoria, South Africa, 2018; Volume 14. [Google Scholar]
- CDC Features Precision Medicine: What Does it Mean for Your Health? 2018. Available online: https://www.cdc.gov/features/precision-medicine/index.html (accessed on 4 July 2022).
- Maier, M. Personalized medicine—A tradition in general practice! Eur J. Gen. Pract. 2019, 25, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Wolverton, M. One Size Does not Fit All. 2016. Available online: https://www.pennmedicine.org/news/publications-and-special-projects/penn-medicine-magazine/archived-issues/2016/summer-2016/size (accessed on 4 July 2022).
- Greenhalgh, P. Rethinking One-Size-Fits-All. 2013. Available online: https://www.team-consulting.com/insights/rethinking-one-size-fits-all/ (accessed on 4 July 2022).
- QMED Staff. Why Size Matters When It Comes Down to Medical Devices. 2015. Available online: https://www.mddionline.com/why-size-matters-when-it-comes-medical-devices (accessed on 4 July 2022).
- Sheridan, D. When It Comes to Medical Equipment, One Size Doesn’t Fit All. OHSU News. 2018. Available online: https://news.ohsu.edu/2018/12/18/releases-20181218 (accessed on 4 July 2022).
- Rodwin, M.A. Conflict of Interests and the Future of Medicine: The United States, France and Japan; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Medical devices must be carefully validated. Nat. Biomed. Eng. 2018, 2, 625–626. [CrossRef]
- Sezdi, M. Performance analysis for medical devices. Biomed. Eng. Res. 2013, 2, 139–146. [Google Scholar] [CrossRef]
- Smith, V.; Warty, R.; Nair, A.; Krishnan, S.; Sursas, J.A.; Costa, F.D.; Vollenhoven, B.; Wallace, E.M. Defining the clinician’s role in early health technology assessment during medical device innovation—A systematic review. BMC Health Serv Res. 2019, 19, 514. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.D.; Petersen, A.J.; Karliner, L.S.; Tice, J.A. Who is Responsible for Evaluating the Safety and Effectiveness of Medical Devices? The Role of Independent Technology Assessment. J. Gen. Intern. Med. 2008, 23 (Suppl. 1), 57–63. [Google Scholar] [CrossRef] [PubMed]
- Medical Device Coordination Group (MDCG). Guidance on Significant Changes Regarding the Transitional Provision under Article 120 of the MDR with Regard to Devices Covered by Certificates According to MDD or AIMDD. 2020. Available online: https://health.ec.europa.eu/system/files/2020-09/md_mdcg_guidance_significant_changes_annexes_en_0.pdf (accessed on 4 July 2022).
- IEC (International Electrotechnical Commission). Medical Electrical Equipment; 60601-1:2022 SER Series; IEC: Geneva, Switzerland, 2022; Available online: https://webstore.iec.ch/publication/2603 (accessed on 4 July 2022).
- Klessascheck, M. Essential Performance in Medical Devices; Johner Institute: Konstanz, Germany, 2021; Available online: https://www.johner-institute.com/articles/johner-institute/essential-performance-in-medical-devices/ (accessed on 4 July 2022).
- Longstaffe, C. Users of Poorly Designed Medical Devices May Work Inefficiently or Contribute to Unintended Harm. Nursing Times. 2021. Available online: https://www.nursingtimes.net/opinion/users-of-poorly-designed-medical-devices-may-work-inefficiently-or-contribute-to-unintended-harm-12-10-2021/ (accessed on 4 July 2022).
- Miclăuş, T.; Valla, V.; Koukoura, A.; Nielsen, A.A.; Dahlerup, B.; Tsianos, G.I.; Vassiliadis, E. Impact of Design on Medical Device Safety. Ther. Innov. Regul. Sci. 2020, 54, 839–849. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manufacturer | Unit Name | Canister Chambers (n) | Water-Seal Chamber Characteristics | Suction Control | CDU Type | |||
|---|---|---|---|---|---|---|---|---|
| Reservoir Size (mL) | Water Manometer ≥20 cmH2O | Delaying Mechanism | ||||||
| Float Valve | Notch | |||||||
| Atrium/Maquet (Getinge Group) (Gothenburg, Sweden) | Express | 3 | Optional | - | - | - | Dial | Dry-Dry |
| Oasis | 45 | Yes | Yes | Yes | Wet-Dry | |||
| Ocean | Water level | Wet-Wet | ||||||
| Bio-Thorametrix (Gronsveld, The Netherlands) | High capacity | 3 | 60 | Yes | No | No | Water level | Wet-Wet |
| Dial | Wet-Dry | |||||||
| Single | 1 | 100 | Yes | - | - | 3rd bottle | Wet-Wet | |
| Cardinal Health/Covidien (Argyle line) (Dublin, OH, USA) | Altitude | 3 | 80 | Yes | Yes | No | Dial | Wet-Dry |
| Sentinel Seal | 4 | 90 | ||||||
| Aqua-Seal | 3 | 45 | Water level | Wet-Wet | ||||
| One Bottle | 1 | 400 | - | - | 3rd bottle | Wet-Wet | ||
| Thora-Seal I | 1 | 370 | - | - | 2nd CDU | Wet-Wet | ||
| Thora-Seal II | 2 (in series) | 120 | - | - | Water level | Wet-Wet | ||
| Thora-Seal III | 3 | 110 | No | No | Water level | Wet-Wet | ||
| Eurosets (Medolla, Italy) | Rome | 3 | 45 | Yes | Yes | Yes | Dial | Wet-Dry |
| Venice | Water level | Wet-Wet | ||||||
| Meditea/HMC (Mirandola, Italy) | Thoraflow | 1 | 200 | Yes | - | - | 3rd bottle | Wet-Wet |
| Redax (Drentech line) (Poggio Rusco, Italy) | Chest | 1 | 500 | Yes | - | - | 2nd CDU | Wet-Wet |
| Compact | 3 | 45 | No | Yes | No | Water level | Wet-Wet | |
| Variant dry | Dial | Wet-Dry | ||||||
| Simple 3 Mobile | 2 | Add-on PSU | Wet-Dry | |||||
| Dune | 3 | Optional | - | - | - | Dial | Dry-Dry | |
| Simple Simple Plus | 2 | 70 | No | Yes | No | Add-on PSU | Wet-Dry | |
| Rocket medical (Washington, UK) | Rocket BLUE | 1 | 500 | Yes | - | - | Add-on PSU | Wet-Dry |
| Teleflex (Pleur-evac line) (Wayne, PA, USA) | A6000 Cactus | 3 | 70 | Yes | Yes | Yes | Dial | Wet-Dry |
| A7000 | Water level | Wet-Wet | ||||||
| Sahara 1100 | Optional | - | - | - | Dial | Dry-Dry | ||
| ATMOS (Lenzkirch, Germany) | S201 | 1 | Optional | - | - | - | Electronic pump | Dry-Dry |
| S201 re-style | ||||||||
| C051 | No | |||||||
| Medela (Baar, Switzerland) | Thopaz | 1 | No | - | - | - | Electronic pump | Dry-Dry |
| Thopaz+ | ||||||||
| Total | 32 | 3 | ||||||
| Seal | Suction | Classification |
|---|---|---|
| Wet | Wet | |
| Wet | Dry | Thoracic drainage |
| Dry | Dry | |
| Low-flow/low-vacuum pump |
| Manufacturer | Vacuum Conditions Permitting Reverse Air Flow | Mechanisms | Circumference Notched | |||
|---|---|---|---|---|---|---|
| Level (cmH2O) | Duration (Seconds) | Emptying Reservoir | Bending Surface | |||
| Atrium/Maquet | 25 | 64 | X | Yes | ||
| Bio-Thorametrix | 28 | 29 | X | Yes | ||
| 80 | 1 | X | ||||
|
Cardinal Health/
Covidien | Aquaseal | 30 | 20 | X | No | |
| 35 | 3 | X | ||||
| Thoraseal III | 24 | 18 | X | |||
| 40 | 7 | X | ||||
| Eurosets | 24 | 42 | X | Yes | ||
| 63 | 1 | X | ||||
| Redax | 131 | 244 | X | X | No | |
| 25 | 1 | X | ||||
| Teleflex | 29 | 119 | X | Yes | ||
| To include the functions of the three-bottle system |
| To integrate a dedicated patient assessment manometer (the “fourth bottle”) |
| To have automatic positive and negative pressure relief valves |
| To quickly compensate for pressure changes |
| To allow high-flow rates at low-pressures |
| To display real-time data on air leaks and intrapleural pressures for instant clinical use, and to store them for clinical multi-disciplinary discussion and future research purposes |
| To warn medical personnel of any sudden intrapleural change |
| To adjust therapy as patients recover |
| To work in synchrony with mechanical ventilators |
| To allow direct assessment of ‘true’ or ‘false’ air leakage |
| To include an automated line-clearing chest tube system |
| To include an independent source of vacuum |
| To be portable |
| To be a ‘home medical device’ with remote control |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonicelli, A.; Monaco, F.; Carretta, A.; Burt, B.M.; Sonett, J.R.; Veronesi, G. Chest Drainage Therapy: What Comes out of Pandora’s Box Can Affect Patient Outcomes. J. Clin. Med. 2022, 11, 5311. https://doi.org/10.3390/jcm11185311
Antonicelli A, Monaco F, Carretta A, Burt BM, Sonett JR, Veronesi G. Chest Drainage Therapy: What Comes out of Pandora’s Box Can Affect Patient Outcomes. Journal of Clinical Medicine. 2022; 11(18):5311. https://doi.org/10.3390/jcm11185311
Chicago/Turabian StyleAntonicelli, Alberto, Fabrizio Monaco, Angelo Carretta, Bryan M. Burt, Joshua R. Sonett, and Giulia Veronesi. 2022. "Chest Drainage Therapy: What Comes out of Pandora’s Box Can Affect Patient Outcomes" Journal of Clinical Medicine 11, no. 18: 5311. https://doi.org/10.3390/jcm11185311