
Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review

 , ,
, ,
Abstract
:1. Introduction
2. Sleep Disturbances in Immune Diseases

{kind=link}
| IBD | SLE | RA | Psoriasis | Fibromyalgia | MS | Healthy | |
|---|---|---|---|---|---|---|---|
| Insomnia | 22.3–49.6% [9,15] | 33.3–71.1% [16,17,18,19] | 25.6–70.87% [20,21,22] | 5.9–60% [23,24,25] | 30.5% [26] | 12.5–58% [27,28,29] | 10.5–22.6% [18,21,22,23,25] |
| RLS | 7.34–27.8% [30,31,32] | 20–40.47% [16,33,34,35] | 25–40.35% [36,37] | 15.1–40% [23,38,39,40] | 33–64% [41,42,43,44] | 12.1–57.5% [45] | 4.8–14.2% [23,30,31,33,34,35,39,40] |
| OSA | 13% [5] | 23–42% [34,46,47] | 26.3–80% [48,49] | 36–81.8% [23,50,51] | 24.4–52.6% [52] | 21–78% [53,54,55] | 1.5–38% [23,34,50,51,56] |
| High PSQI | 43.6–67.5% [9,30,57] | 55.4–76.7% [10,58,59,60,61,62,63] | 38.5–86.5% [64,65,66,67,68,69] | 78.3–90% [40,70] | 96% [71] | 44–65% [12,72,73] | 13.4–33.9% [9,30,40,66,70,74] |
2.1. Sleep Assessment Methods
2.2. Insomnia
2.3. Sleep-Disordered Breathing
2.4. Circadian Rhythm
2.5. Restless Leg Syndrome
2.6. Summary
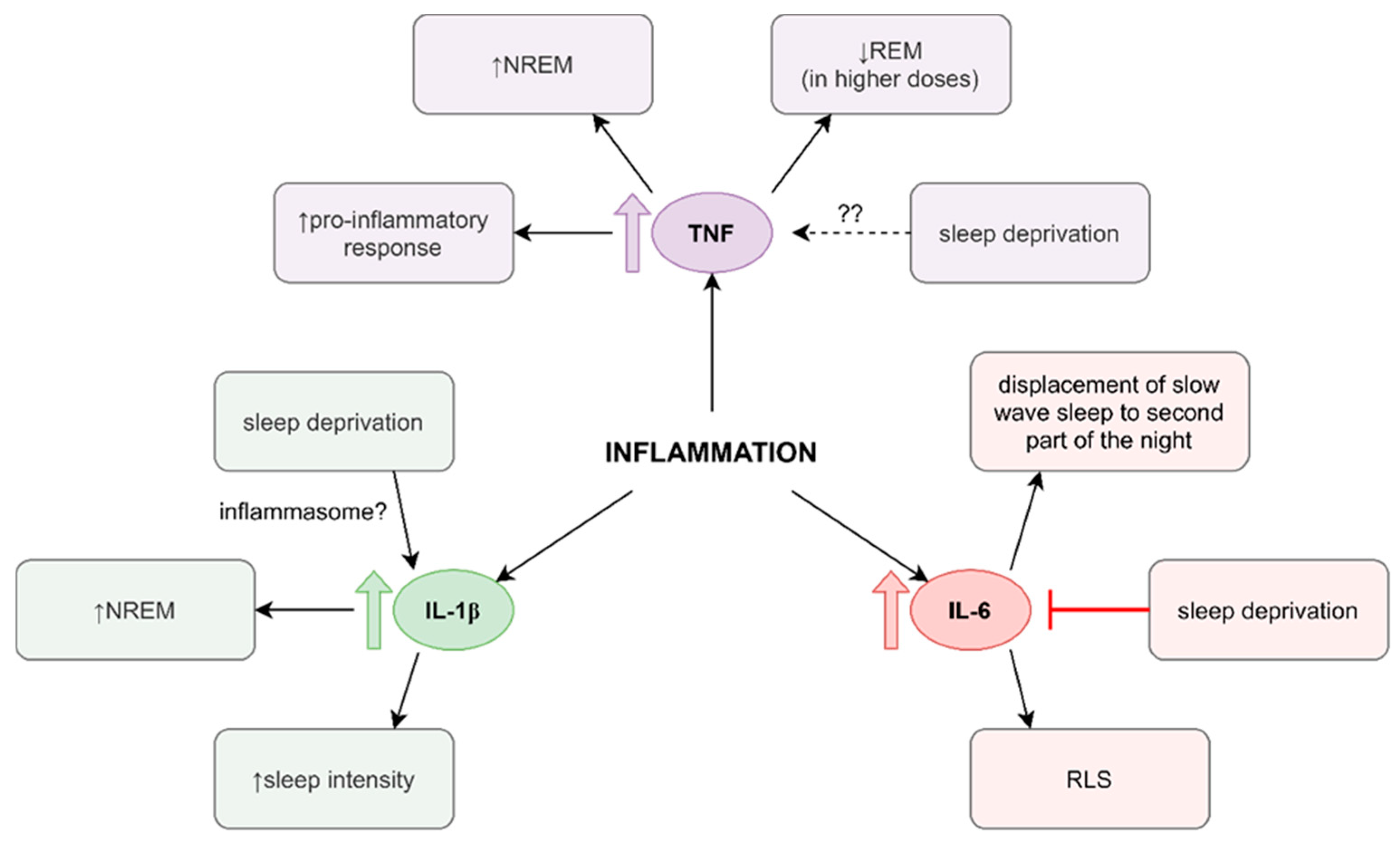
3. Sleep and Inflammation
4. Therapy with Monoclonal Antibodies
5. Treatment of Patients with Chronic Inflammatory Diseases and Comorbid Sleep Disorders
5.1. Cognitive–Behavioral Therapy for Insomnia
5.2. Hypnotic Drugs
5.3. Melatonin
5.4. Probiotics
5.5. Anti-Inflammatory Treatment
5.6. Continuous Positive Airway Pressure
5.7. Summary
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Health Organization: Genewa, Switzerland, 2019. [Google Scholar]
- Grandner, M.A.; Patel, N.P.; Gehrman, P.R.; Xie, D.; Sha, D.; Weaver, T.; Gooneratne, N. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Med. 2010, 11, 470–478. [Google Scholar] [CrossRef] [Green Version]
- Wickwire, E.M.; Geiger-Brown, J.; Scharf, S.M.; Drake, C.L. Shift Work and Shift Work Sleep Disorder: Clinical and Organizational Perspectives. Chest 2017, 151, 1156–1172. [Google Scholar] [CrossRef] [PubMed]
- Lashley, F.R. A Review of Sleep in Selected Immune and Autoimmune Disorders. Holist. Nurs. Pract. 2003, 17, 65–80. [Google Scholar] [CrossRef] [Green Version]
- Kinnucan, J.A.; Rubin, D.T.; Ali, T. Sleep and Inflammatory Bowel Disease: Exploring the Relationship between Sleep Disturbances and Inflammation. Gastroenterol. Hepatol. 2013, 9, 718–727. [Google Scholar]
- Reimer, M.A.; Flemons, W.W. Quality of life in sleep disorders. Sleep Med. Rev. 2003, 7, 335–349. [Google Scholar] [CrossRef]
- Lichstein, K.L.; Means, M.K.; Noe, S.L.; Aguillard, R.N. Fatigue and sleep disorders. Behav. Res. Ther. 1997, 35, 733–740. [Google Scholar] [CrossRef]
- Roizenblatt, M.; Neto, N.S.R.; Tufik, S.; Roizenblatt, S. Pain-related diseases and sleep disorders. Braz. J. Med. Biol. Res. 2012, 45, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Sochal, M.; Małecka-Panas, E.; Gabryelska, A.; Talar-Wojnarowska, R.; Szmyd, B.; Krzywdzińska, M.; Białasiewicz, P. Determinants of Sleep Quality in Inflammatory Bowel Diseases. J. Clin. Med. 2020, 9, 2921. [Google Scholar] [CrossRef]
- Da Costa, D.; Bernatsky, S.; Dritsa, M.; Clarke, A.E.; Dasgupta, K.; Keshani, A.; Pineau, C. Determinants of sleep quality in women with systemic lupus erythematosus. Arthritis Rheum. 2005, 53, 272–278. [Google Scholar] [CrossRef]
- Abbasi, M.; Yazdi, Z.; Rezaie, N. Sleep disturbances in patients with rheumatoid arthritis. Niger. J. Med. 2013, 22, 181–186. [Google Scholar] [PubMed]
- Vitkova, M.; Rosenberger, J.; Gdovinova, Z.; Szilasiova, J.; Mikula, P.; Groothoff, J.W.; Reijneveld, S.A.; Van Dijk, J.P. Poor sleep quality in patients with multiple sclerosis: Gender differences. Brain Behav. 2016, 6, e00553. [Google Scholar] [CrossRef]
- Marsella, J.L.; Sharkey, K.M. Sex Differences in Sleep Disorders. In Sleep Disorders in Women: A Guide to Practical Management; Attarian, H., Viola-Saltzman, M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 65–81. [Google Scholar]
- Benros, M.E. Autoimmune diseases can be associated with depression. Évid. Based Ment. Health 2016, 19, e27. [Google Scholar] [CrossRef]
- Araki, M.; Shinzaki, S.; Yamada, T.; Arimitsu, S.; Komori, M.; Shibukawa, N.; Mukai, A.; Nakajima, S.; Kinoshita, K.; Kitamura, S.; et al. Psychologic stress and disease activity in patients with inflammatory bowel disease: A multicenter cross-sectional study. PLoS ONE 2020, 15, e0233365. [Google Scholar] [CrossRef] [PubMed]
- Falup-Pecurariu, C.; Duca, L.; Moarcas, M. High prevalence of restless legs syndrome in systemic lupus erythematosus. Sleep Med. 2013, 14, e118. [Google Scholar] [CrossRef]
- Palagini, L.; Mauri, M.; Faraguna, U.; Carli, L.; Tani, C.; Dell’Osso, L.; Mosca, M.; Riemann, D. Insomnia symptoms, perceived stress and coping strategies in patients with systemic lupus erythematosus. Lupus 2016, 25, 988–996. [Google Scholar] [CrossRef]
- Palagini, L.; Tani, C.; Bruno, R.M.; Gemignani, A.; Mauri, M.; Bombardieri, S.; Riemann, D.; Mosca, M. Poor sleep quality in systemic lupus erythematosus: Does it depend on depressive symptoms? Lupus 2014, 23, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. Evaluation of Mental Health Factors among People with Systemic Lupus Erythematosus during the SARS-CoV-2 Pandemic. J. Clin. Med. 2020, 9, 2872. [Google Scholar] [CrossRef]
- Mustafa, M.; Bawazir, Y.; Merdad, L.; Wali, S.; Attar, S.; Fathaldin, O.; Bahlas, S.; Alhejaili, F.; Aljohaney, A.; Jan, A.; et al. Frequency of sleep disorders in patients with rheumatoid arthritis. Open Access Rheumatol. Res. Rev. 2019, 11, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Sivertsen, B.; Krokstad, S.; Øverland, S.; Mykletun, A. The epidemiology of insomnia: Associations with physical and mental health. J. Psychosom. Res. 2009, 67, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, B.; Kłak, A.; Raciborski, F.; Maślińska, M. The prevalence of depression and insomnia symptoms among patients with rheumatoid arthritis and osteoarthritis in Poland: A case control study. Psychol. Health Med. 2019, 24, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.A.; Simpson, F.C.; Gupta, A.K. Psoriasis and sleep disorders: A systematic review. Sleep Med. Rev. 2016, 29, 63–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, V.; Myers, B.; Brownstone, N.; Thibodeaux, Q.; Chan, S.; Liao, W.; Bhutani, T. Update on Sleep and Pulmonary Comorbidities in Psoriasis. Curr. Dermatol. Rep. 2020, 9, 30–35. [Google Scholar] [CrossRef]
- Jensen, P.; Zachariae, C.; Skov, L.; Zachariae, R. Sleep disturbance in psoriasis: A case-controlled study. Br. J. Dermatol. 2018, 179, 1376–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.-J.; Huang, C.-L.; Fan, Y.-C.; Chen, T.-Y.; Tsai, P.-S. Insomnia Increases Symptom Severity and Health Care Utilization in Patients with Fibromyalgia: A Population-based Study. Clin. J. Pain 2019, 35, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Viana, P.; Rodrigues, E.; Fernandes, C.; Matas, A.; Barreto, R.D.; Mendonça, M.; Peralta, R.; Geraldes, R. InMS: Chronic insomnia disorder in multiple sclerosis–a Portuguese multicentre study on prevalence, subtypes, associated factors and impact on quality of life. Mult. Scler. Relat. Disord. 2015, 4, 477–483. [Google Scholar] [CrossRef]
- Alhazzani, A.A.; Alshahrani, A.; Alqahtani, M.; Alamri, R.; Alqahtani, R.; Alqahtani, M.; Alahmarii, M. Insomnia among non-depressed multiple sclerosis patients: A cross-sectional study. Egypt. J. Neurol. Psychiatry Neurosurg. 2018, 54, 17. [Google Scholar] [CrossRef] [Green Version]
- Stanton, B.R.; Barnes, F.; Silber, E. Sleep and fatigue in multiple sclerosis. Mult. Scler. J. 2006, 12, 481–486. [Google Scholar] [CrossRef]
- Caloz, E.; Vullièmoz, M.; Rubio, J.H.; Pittet, V.; Barry, P.M.; Michetti, P.; Heinzer, R.; Maillard, M.H. P808 Prevalence and factors associated with sleep disturbances in inflammatory bowel disease patients compared with normal controls. J. Crohn’s Colitis 2020, 14, S631–S632. [Google Scholar] [CrossRef] [Green Version]
- Mosli, M.H.; Bukhari, L.M.; Khoja, A.A.; Ashour, N.A.; Aljahdali, H.R.; Khoja, O.A.; Alhejaili, F.F.; Saadah, O.I. Inflammatory bowel disease and restless leg syndrome. Neurosciences 2020, 25, 301–307. [Google Scholar] [CrossRef]
- Takahara, I.; Takeshima, F.; Ichikawa, T.; Matsuzaki, T.; Shibata, H.; Miuma, S.; Akazawa, Y.; Miyaaki, H.; Taura, N.; Nakao, K. Prevalence of Restless Legs Syndrome in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2017, 62, 761–767. [Google Scholar] [CrossRef]
- Hassan, N.; Pineau, C.A.; Clarke, A.E.; Vinet, E.; Ng, R.; Bernatsky, S. Systemic Lupus and Risk of Restless Legs Syndrome. J. Rheumatol. 2011, 38, 874–876. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.; Pedro, S.; Michaud, K. CS-30 Sleep Disturbances among Women with Systemic Lupus Erythematosus (SLE). Lupus Sci. Med. 2018, 5, A39.32–A40. [Google Scholar]
- Kucuk, A.; Uslu, A.U.; Yilmaz, R.; Salbaş, E.; Solak, Y.; Tunc, R. Relationship between prevalence and severity of restless legs syndrome and anemia in patients with systemic lupus erythematosus. Int. J. Rheum. Dis. 2017, 20, 469–473. [Google Scholar] [CrossRef]
- Gjevre, J.A.; Taylor-Gjevre, R.M. Restless Legs Syndrome as a Comorbidity in Rheumatoid Arthritis. Autoimmune Dis. 2013, 2013, 352782. [Google Scholar] [CrossRef]
- Taylor-Gjevre, R.M.; Gjevre, J.A.; Nair, B.V. Increased nocturnal periodic limb movements in rheumatoid arthritis patients meeting questionnaire diagnostic criteria for restless legs syndrome. BMC Musculoskelet. Disord. 2014, 15, 378. [Google Scholar] [CrossRef] [Green Version]
- Temel, A.B.; Karaman, N.S.; Bozkurt, S.; Karakaş, A.A.; Yılmaz, E.; Alpsoy, E. Prevalence of Restless Legs Syndrome among Psoriasis Patients and Association with Depression and Sleep Quality. Turk. J. Dermatol. 2016, 10, 110–115. [Google Scholar] [CrossRef]
- Güler, S.; Tekatas, A.; Arican, O.; Kaplan, O.S.; Dogru, Y. Restless legs syndrome and insomnia frequency in patients with psoriasis. Ideggyogy 2015, 68, 331–336. [Google Scholar] [CrossRef]
- Nowowiejska, J.; Baran, A.; Lewoc, M.; Grabowska, P.; Kaminski, T.W.; Flisiak, I. The Assessment of Risk and Predictors of Sleep Disorders in Patients with Psoriasis—A Questionnaire-Based Cross-Sectional Analysis. J. Clin. Med. 2021, 10, 664. [Google Scholar] [CrossRef]
- Civelek, G.M.; Ciftkaya, P.O.; Karatas, M. Evaluation of restless legs syndrome in fibromyalgia syndrome: An analysis of quality of sleep and life. J. Back Musculoskelet. Rehabil. 2014, 27, 537–544. [Google Scholar] [CrossRef]
- Viola-Saltzman, M.; Watson, N.F.; Bogart, A.; Goldberg, J.; Buchwald, D. High Prevalence of Restless Legs Syndrome among Patients with Fibromyalgia: A Controlled Cross-Sectional Study. J. Clin. Sleep Med. 2010, 6, 423–427. [Google Scholar] [CrossRef]
- Yunus, M.B.; Aldag, J.C. Restless legs syndrome and leg cramps in fibromyalgia syndrome: A controlled study. BMJ 1996, 312, 1339. [Google Scholar] [CrossRef] [Green Version]
- Stehlik, R.; Arvidsson, L.; Ulfberg, J. Restless Legs Syndrome Is Common among Female Patients with Fibromyalgia. Eur. Neurol. 2009, 61, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Hernández, L.L.; León, M.P.; Fuentes, N.A.C.; Sánchez, A.J.U.; Chocán, J.L.C.; Sánchez, M.D. Restless legs syndrome in patients with multiple sclerosis: Evaluation of risk factors and clinical impact. Neurología 2021, in press. [Google Scholar] [CrossRef]
- Efat, E. Sleep pattern changes in patients with connective tissue diseases. Egypt. J. Chest Dis. Tuberc. 2016, 65, 655–660. [Google Scholar] [CrossRef] [Green Version]
- Iaboni, A.; Ibanez, D.; Gladman, D.D.; Urowitz, M.B.; Moldofsky, H. Fatigue in systemic lupus erythematosus: Contributions of disordered sleep, sleepiness, and depression. J. Rheumatol. 2006, 33, 2453–2457. [Google Scholar]
- Silva, S.I.C.; Caldeira, V.; Sousa, C.; Pinheiro, S.; Murinello, N.; Cardoso, J. Risk of obstructive sleep apnea in patients with rheumatoid arthritis and its impact on quality of life. Eur. Respir. J. 2019, 54, PA864. [Google Scholar] [CrossRef]
- Shen, T.-C.; Hang, L.-W.; Liang, S.-J.; Huang, C.-C.; Lin, C.-L.; Tu, C.-Y.; Hsia, T.-C.; Shih, C.-M.; Hsu, W.-H.; Sung, F.-C. Risk of obstructive sleep apnoea in patients with rheumatoid arthritis: A nationwide population-based retrospective cohort study. BMJ Open 2016, 6, e013151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Psoriasis and Sleep Apnea: A Danish Nationwide Cohort Study. J. Clin. Sleep Med. 2016, 12, 663–671. [Google Scholar] [CrossRef]
- Shalom, G.; Dreiher, J.; Cohen, A. Psoriasis and obstructive sleep apnea. Int. J. Dermatol. 2016, 55, e579–e584. [Google Scholar] [CrossRef]
- Eshak, N.; Vutthikraivit, W.; Beltagy, A. Obstructive Sleep Apnea in Fibromyalgia Patients: A Meta-Analysis [Abstract]; Wiley: Atlanta, GA, USA, 2020. [Google Scholar]
- Kaminska, M.; Kimoff, R.J.; Benedetti, A.; Robinson, A.; Bar-Or, A.; Lapierre, Y.; Schwartzman, K.; Trojan, D.A. Obstructive sleep apnea is associated with fatigue in multiple sclerosis. Mult. Scler. J. 2012, 18, 1159–1169. [Google Scholar] [CrossRef]
- Diaz-Piedra, C.; Di Stasi, L.L.; Baldwin, C.M.; Buela-Casal, G.; Catena, A. Sleep disturbances of adult women suffering from fibromyalgia: A systematic review of observational studies. Sleep Med. Rev. 2015, 21, 86–99. [Google Scholar] [CrossRef]
- Singh, M.; Gavidia, R.; Dunietz, G.L.; Washnock-Schmid, E.; Romeo, A.R.; Hershner, S.; Chervin, R.D.; Braley, T.J. Validation of an obstructive sleep apnea symptom inventory in persons with multiple sclerosis. Mult. Scler. J. 2021, 13524585211013014. [Google Scholar] [CrossRef] [PubMed]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, C.; Savarino, E.V.; Marsilio, I.; Lorenzon, G.; Gavaruzzi, T.; D’Incà, R.; Zingone, F. Sleep disturbance in Inflammatory Bowel Disease: Prevalence and risk factors–A cross-sectional study. Sci. Rep. 2020, 10, 507. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekhara, P.K.S.; Jayachandran, N.V.; Rajasekhar, L.; Thomas, J.; Narsimulu, G. The prevalence and associations of sleep disturbances in patients with systemic lupus erythematosus. Mod. Rheumatol. 2009, 19, 407–415. [Google Scholar] [CrossRef]
- Gholamrezaei, A.; Hosseini, N.; Bonakdar, Z.S. Sleep quality in women with systemic lupus erythematosus. Sleep Med. 2013, 14, e136. [Google Scholar] [CrossRef]
- Margiotta, D.P.E.; Laudisio, A.; Navarini, L.; Basta, F.; Mazzuca, C.; Angeletti, S.; Ciccozzi, M.; Incalzi, R.A.; Afeltra, A. Pattern of sleep dysfunction in systemic lupus erythematosus: A cluster analysis. Clin. Rheumatol. 2019, 38, 1561–1570. [Google Scholar] [CrossRef]
- Kotb, H.; Rady, H.; Ghanim, D.H. Sleep disturbance in female patients with systemic lupus erythematosus and its relation to disease parameters. Egypt. Rheumatol. 2013, 35, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Inoue, M.; Shiozawa, K.; Yoshihara, R.; Yamane, T.; Shima, Y.; Hirano, T.; Makimoto, K. Predictors of poor sleep quality in patients with systemic lupus erythematosus. Clin. Rheumatol. 2017, 36, 1053–1062. [Google Scholar] [CrossRef]
- Magro, R.; Camilleri, L.; Borg, A. Fri0178 predictive factors for poor sleep quality in systemic lupus erythematosus. Ann. Rheum. Dis. 2020, 79, 673. [Google Scholar] [CrossRef]
- Kontodimopoulos, N.; Stamatopoulou, E.; Kletsas, G.; Kandili, A. Disease activity and sleep quality in rheumatoid arthritis: A deeper look into the relationship. Expert Rev. Pharm. Outcomes Res. 2020, 20, 595–602. [Google Scholar] [CrossRef]
- Son, C.-N.; Choi, G.; Lee, S.-Y.; Lee, J.-M.; Lee, T.-H.; Jeong, H.-J.; Jung, C.-G.; Kim, J.-M.; Cho, Y.-W.; Kim, S.-H. Sleep quality in rheumatoid arthritis, and its association with disease activity in a Korean population. Korean J. Intern. Med. 2015, 30, 384–390. [Google Scholar] [CrossRef]
- Guo, G.; Fu, T.; Yin, R.; Zhang, L.; Zhang, Q.; Xia, Y.; Li, L.; Gu, Z. Sleep quality in Chinese patients with rheumatoid arthritis: Contributing factors and effects on health-related quality of life. Health Qual. Life Outcomes 2016, 14, 151. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.; Chalk, A.; Sharma, P.; Dahiya, S.; Galloway, J. A cross-sectional study of sleep and depression in a rheumatoid arthritis population. Clin. Rheumatol. 2021, 40, 1299–1305. [Google Scholar] [CrossRef]
- Szady, P.; Bączyk, G.; Kozłowska, K. Fatigue and sleep quality in rheumatoid arthritis patients during hospital admission. Reumatologia 2017, 55, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Radwan, A.; Borai, A. Quality of sleep in rheumatoid arthritis patients: Relationship with disease activity, depression and functional status. Egypt. Rheumatol. 2021, 43, 183–187. [Google Scholar] [CrossRef]
- Saçmacı, H.; Gürel, G. Sleep disorders in patients with psoriasis: A cross-sectional study using non-polysomnographical methods. Sleep Breath. 2019, 23, 893–898. [Google Scholar] [CrossRef]
- Bigatti, S.M.; Hernandez, A.M.; Cronan, T.A.; Rand, K.L. Sleep disturbances in fibromyalgia syndrome: Relationship to pain and depression. Arthritis Rheum. 2008, 59, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merlino, G.; Fratticci, L.; Lenchig, C.; Valente, M.; Cargnelutti, D.; Picello, M.; Serafini, A.; Dolso, P.; Gigli, G.L. Prevalence of ‘poor sleep’ among patients with multiple sclerosis: An independent predictor of mental and physical status. Sleep Med. 2009, 10, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Parmenter, B.A.; Haselkorn, J.K.; Lovera, J.F.; Bourdette, D.; Boudreau, E.; Cameron, M.H.; Turner, A.P. Sleep and its associations with perceived and objective cognitive impairment in individuals with multiple sclerosis. J. Sleep Res. 2017, 26, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Carrillo, C.; Sadeghi, N.; FitzGerald, J.D.; Ranganath, V.K.; Nicassio, P.M. Sleep Loss Exacerbates Fatigue, Depression, and Pain in Rheumatoid Arthritis. Sleep 2012, 35, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Gjevre, R.M.; Nair, B.V.; Gjevre, J.A. Obstructive sleep apnoea in relation to rheumatic disease. Rheumatology 2013, 52, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Munger, K.L.; Batool-Anwar, S.; De Vito, K.; Ascherio, A.; Gao, X. Association of multiple sclerosis with restless legs syndrome and other sleep disorders in women. Neurology 2012, 78, 1500–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manconi, M.; Rocca, M.A.; Ferini-Strambi, L.; Tortorella, P.; Agosta, F.; Comi, G.; Filippi, M. Restless legs syndrome is a common finding in multiple sclerosis and correlates with cervical cord damage. Mult. Scler. J. 2008, 14, 86–93. [Google Scholar] [CrossRef]
- de Resende Guimarães, M.F.B.; Rodrigues, C.E.M.; Gomes, K.W.P.; Machado, C.J.; Brenol, C.V.; Krampe, S.F.; De Andrade, N.P.B.; Kakehasi, A.M. High prevalence of obesity in rheumatoid arthritis patients: Association with disease activity, hypertension, dyslipidemia and diabetes, a multi-center study. Adv. Rheumatol. 2019, 59, 44. [Google Scholar] [CrossRef] [PubMed]
- Tettey, P.; Balogun, S. Obesity and multiple sclerosis: Prevalence, susceptibility and progression in disability. Futur. Neurol. 2017, 12, 149–157. [Google Scholar] [CrossRef]
- Dias, D.N.G.; Marques, M.A.A.; Bettini, S.C.; Paiva, E.D.S. Prevalence of fibromyalgia in patients treated at the bariatric surgery outpatient clinic of Hospital de Clínicas do Paraná-Curitiba. Rev. Bras. Reum. 2017, 57, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.-C.; Chen, W.-S.; Chang, Y.-S.; Lin, Y.-C.; Huang, Y.-H.; Tsai, C.-Y.; Chen, J.-H.; Chang, C.-C. Risk of obstructive sleep apnea in patients with Sjögren syndrome and Behçet’s disease: A nationwide, population-based cohort study. Sleep Breath. 2020, 24, 1199–1205. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hublin, C.; Kaprio, J.; Partinen, M.; Koskenvuo, M.; Heikkilä, K. The Ullanlinna Narcolepsy Scale: Validation of a measure of symptoms in the narcoleptic syndrome. J. Sleep Res. 1994, 3, 52–59. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.J.; Song, M.L.; Cho, Y.W. Clinical Characteristics of Primary Insomniacs with Sleep-State Misperception. J. Clin. Neurol. 2015, 11, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Edinger, J.D.; Krystal, A.D. Subtyping primary insomnia: Is sleep state misperception a distinct clinical entity? Sleep Med. Rev. 2003, 7, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Wyatt, J.K.; Stepanski, E.J.; Olsen, M.K.; Stechuchak, K.M.; Carney, C.E.; Chiang, A.; Crisostomo, M.I.; Lineberger, M.D.; Means, M.K.; et al. Testing the Reliability and Validity of DSM-IV-TR and ICSD-2 Insomnia Diagnoses: Results of a multitrait-multimethod analysis. Arch. Gen. Psychiatry 2011, 68, 992–1002. [Google Scholar] [CrossRef] [Green Version]
- Jackowska, M.; Ronaldson, A.; Brown, J.; Steptoe, A. Biological and psychological correlates of self-reported and objective sleep measures. J. Psychosom. Res. 2016, 84, 52–55. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Camiletti-Moirón, D.; Munguía-Izquierdo, D.; Álvarez-Gallardo, I.C.; Ruiz, J.R.; Ortega, F.B.; Delgado-Fernández, M. Agreement between self-reported sleep patterns and actigraphy in fibromyalgia and healthy women. Clin. Exp. Rheumatol. 2015, 33, S58–S67. [Google Scholar]
- Lemola, S.; Ledermann, T.; Friedman, E.M. Variability of Sleep Duration Is Related to Subjective Sleep Quality and Subjective Well-Being: An Actigraphy Study. PLoS ONE 2013, 8, e71292. [Google Scholar] [CrossRef] [Green Version]
- Tomita, S.; Kitajima, T.; Mekata, T.; Tsuchiya, A.; Sano, W.; Esaki, Y.; Marina, H.; Fujita, S.; Iwata, N. Comparison of sleep diary and actigraphy to evaluate total sleep time in hypersomnia patients. Sleep Biol. Rhythm. 2013, 11, 65–73. [Google Scholar] [CrossRef]
- Kaplan, K.A.; Talbot, L.S.; Gruber, J.; Harvey, A.G. Evaluating sleep in bipolar disorder: Comparison between actigraphy, polysomnography, and sleep diary. Bipolar Disord. 2012, 14, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Franklin, K.A.; Lindberg, E. Obstructive sleep apnea is a common disorder in the population—a review on the epidemiology of sleep apnea. J. Thorac. Dis. 2015, 7, 1311–1322. [Google Scholar] [CrossRef]
- Spicuzza, L.; Caruso, D.; Di Maria, G. Obstructive sleep apnoea syndrome and its management. Ther. Adv. Chronic Dis. 2015, 6, 273–285. [Google Scholar] [CrossRef] [Green Version]
- Ananthakrishnan, A.N.; Long, M.D.; Martin, C.F.; Sandler, R.S.; Kappelman, M.D. Sleep Disturbance and Risk of Active Disease in Patients with Crohn’s Disease and Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2013, 11, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Foral, P.; Knezevich, J.; Dewan, N.; Malesker, M. Medication-Induced Sleep Disturbances. Consult. Pharm. 2011, 26, 414–425. [Google Scholar] [CrossRef]
- Sochal, M.; Małecka-Panas, E.; Gabryelska, A.; Fichna, J.; Talar-Wojnarowska, R.; Szmyd, B.; Białasiewicz, P. Brain-derived neurotrophic factor is elevated in the blood serum of Crohn’s disease patients, but is not influenced by anti-TNF-α treatment—A pilot study. Neurogastroenterol. Motil. 2021, 33, e13978. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; Jordan, A.S.; Merchia, P.; Malhotra, A. Central Sleep Apnea: Pathophysiology and Treatment. Chest 2007, 131, 595–607. [Google Scholar] [CrossRef]
- Yamauchi, M.; Fujita, Y.; Kumamoto, M.; Yoshikawa, M.; Ohnishi, Y.; Nakano, H.; Strohl, K.P.; Kimura, H. Nonrapid Eye Movement-Predominant Obstructive Sleep Apnea: Detection and Mechanism. J. Clin. Sleep Med. 2015, 11, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-W.; Taranto-Montemurro, L. When do gender differences begin in obstructive sleep apnea patients? J. Thorac. Dis. 2019, 11, S1147–S1149. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-S.; Chang, Y.-S.; Chang, C.-C.; Chang, D.-M.; Chen, Y.-H.; Tsai, C.-Y.; Chen, J.-H. Management and Risk Reduction of Rheumatoid Arthritis in Individuals with Obstructive Sleep Apnea: A Nationwide Population-Based Study in Taiwan. Sleep 2016, 39, 1883–1890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabryelska, A.; Sochal, M.; Wasik, B.; Bialasiewicz, P. Patients With Obstructive Sleep Apnea Are Over Four Times More Likely to Suffer From Psoriasis Than the General Population. J. Clin. Sleep Med. 2018, 14, 153. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.; Feng, X.; Li, X.; Wang, D.; Sun, L. Hypoxia-inducible factor 1 in autoimmune diseases. Cell. Immunol. 2016, 303, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Szmyd, B.; Szemraj, J.; Stawski, R.; Sochal, M.; Białasiewicz, P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1α protein. J. Clin. Sleep Med. 2020, 16, 1761–1768. [Google Scholar] [CrossRef]
- Kang, J.-H.; Lin, H.-C. Obstructive sleep apnea and the risk of autoimmune diseases: A longitudinal population-based study. Sleep Med. 2012, 13, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Rijo-Ferreira, F.; Takahashi, J.S. Genomics of circadian rhythms in health and disease. Genome Med. 2019, 11, 82. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.K.; Kim, D.; Kim, K.; Boo, K.; Yu, Y.S.; Kim, I.S.; Jeon, Y.; Im, S.-K.; Lee, S.-H.; Lee, J.M.; et al. RORα is crucial for attenuated inflammatory response to maintain intestinal homeostasis. Proc. Natl. Acad. Sci. USA 2019, 116, 21140–21149. [Google Scholar] [CrossRef] [Green Version]
- Stokes, K.; Cooke, A.; Chang, H.; Weaver, D.; Breault, D.T.; Karpowicz, P. The Circadian Clock Gene BMAL1 Coordinates Intestinal Regeneration. Cell. Mol. Gastroenterol. Hepatol. 2017, 4, 95–114. [Google Scholar] [CrossRef] [Green Version]
- Kaneshiro, K.; Yoshida, K.; Morii, K.; Oketani, Y.; Uchida, K.; Yaekura, A.; Okumura, I.; Hashimoto, T.; Kawasaki, Y.; Shibanuma, N.; et al. Expressions of circadian clock genes represent disease activities of RA patients treated with biological DMARDs. Mod. Rheumatol. 2020, 30, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Nakai, A.; Kaneshiro, K.; Hashimoto, N.; Suzuki, K.; Uchida, K.; Hashimoto, T.; Kawasaki, Y.; Tateishi, K.; Nakagawa, N.; et al. TNF-α induces expression of the circadian clock gene Bmal1 via dual calcium-dependent pathways in rheumatoid synovial cells. Biochem. Biophys. Res. Commun. 2018, 495, 1675–1680. [Google Scholar] [CrossRef]
- Liu, X.; Yu, R.; Zhu, L.; Hou, X.; Zou, K. Bidirectional Regulation of Circadian Disturbance and Inflammation in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 1741–1751. [Google Scholar] [CrossRef]
- Noguchi, T.; Wang, C.W.; Pan, H.; Welsh, D.K. Fibroblast Circadian Rhythms of PER2 Expression Depend on Membrane Potential and Intracellular Calcium. Chrono Int. 2012, 29, 653–664. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Hashiramoto, A.; Okano, T.; Yamane, T.; Shibanuma, N.; Shiozawa, S. TNF-α modulates expression of the circadian clock genePer2in rheumatoid synovial cells. Scand. J. Rheumatol. 2013, 42, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Sonnenberg, A. Occupational distribution of inflammatory bowel disease among German employees. Gut 1990, 31, 1037–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, Y.; Cohen, S.; Chapnik, N.; Ben-Tov, A.; Yerushalmy-Feler, A.; Dotan, I.; Tauman, R.; Froy, O. Clock Gene Disruption Is an Initial Manifestation of Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 115–122.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magrini, A.; Pietroiusti, A.; Coppeta, L.; Babbucci, A.; Barnaba, E.; Papadia, C.; Iannaccone, U.; Boscolo, P.; Bergamaschi, E.; Bergamaschi, A. Shift work and autoimmune thyroid disorders. Int. J. Immunopathol. Pharmacol. 2006, 19, 31–36. [Google Scholar]
- Najafi, M.R.; Toghianifar, N.; Etemadifar, M.; Haghighi, S.; Maghzi, A.H.; Akbari, M. Circadian rhythm sleep disorders in patients with multiple sclerosis and its association with fatigue: A case-control study. J. Res. Med. Sci. 2013, 18, S71–S73. [Google Scholar]
- To, H. Chronotherapy for rheumatoid arthritis: Current perspectives. ChronoPhysiology Ther. 2016, 6, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Szmyd, B.; Rogut, M.; Białasiewicz, P.; Gabryelska, A. The impact of glucocorticoids and statins on sleep quality. Sleep Med. Rev. 2021, 55, 101380. [Google Scholar] [CrossRef]
- Ando, H.; Fujimura, A. Drug chronotherapy: The coordination of biological rhythms with medical treatment. Jpn. J. Clin. Med. 2012, 70, 1222–1226. [Google Scholar]
- Martínez-García, E.A.; Zavala-Cerna, M.G.; Lujano-Benítez, A.V.; Sánchez-Hernández, P.E.; Martín-Márquez, B.T.; Sandoval-García, F.; Mercado, M.V.-D. Potential Chronotherapeutic Optimization of Antimalarials in Systemic Lupus Erythematosus: Is Toll-Like Receptor 9 Expression Dependent on the Circadian Cycle in Humans? Front. Immunol. 2018, 9, 1497. [Google Scholar] [CrossRef]
- Brass, S.D.; Duquette, P.; Proulx-Therrien, J.; Auerbach, S. Sleep disorders in patients with multiple sclerosis. Sleep Med. Rev. 2010, 14, 121–129. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Tsianos, V.E.; Katsanos, K.H.; Giannopoulos, S.; Tsianos, E.V. Restless legs syndrome in patients with Crohn’s disease. Ann. Gastroenterol. 2013, 26, 186. [Google Scholar]
- Pamuk, O.N.; Tekatas, A. FRI0123 The Relationship between Ankylosing Spondylitis and Restless Leg Syndrome. Ann. Rheum. Dis. 2014, 73, 426. [Google Scholar] [CrossRef]
- Connor, J.R.; Boyer, P.J.; Menzies, S.L.; Dellinger, B.; Allen, R.P.; Ondo, W.G.; Earley, C.J. Neuropathological examination suggests impaired brain iron acquisition in restless legs syndrome. Neurology 2003, 61, 304–309. [Google Scholar] [CrossRef]
- Kaitha, S.; Bashir, M.; Ali, T. Iron deficiency anemia in inflammatory bowel disease. World J. Gastrointest. Pathophysiol. 2015, 6, 62–72. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflügers Arch. Eur. J. Physiol. 2012, 463, 121–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, J.; Günter, M.; Schuhmacher, J.; Bieber, K.; Pöschel, S.; Schütz, M.; Engelhardt, B.; Oster, H.; Sina, C.; Lange, T.; et al. Sleep enhances numbers and function of monocytes and improves bacterial infection outcome in mice. Brain Behav. Immun. 2020, 87, 329–338. [Google Scholar] [CrossRef]
- Rohleder, N.; Aringer, M.; Boentert, M. Role of interleukin-6 in stress, sleep, and fatigue. Ann. N. Y. Acad. Sci. 2012, 1261, 88–96. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabay, C. Interleukin-6 and chronic inflammation. Arthritis Res. 2006, 8 (Suppl. S2), S3. [Google Scholar] [CrossRef] [Green Version]
- Thomas, K.S.; Motivala, S.; Olmstead, R.; Irwin, M.R. Sleep depth and fatigue: Role of cellular inflammatory activation. Brain Behav. Immun. 2011, 25, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R.; Opp, M.R. Sleep Health: Reciprocal Regulation of Sleep and Innate Immunity. Neuropsychopharmacology 2017, 42, 129–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dienz, O.; Rincon, M. The effects of IL-6 on CD4 T cell responses. Clin. Immunol. 2009, 130, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 mediates hypoferremia of in-flammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, R.; Zhou, H.; Su, S.B. A critical role for interleukin-1β in the progression of autoimmune diseases. Int. Immunopharmacol. 2013, 17, 658–669. [Google Scholar] [CrossRef] [PubMed]
- Clinton, J.M.; Davis, C.J.; Zielinski, M.R.; Jewett, K.A.; Krueger, J.M. Biochemical Regulation of Sleep and Sleep Biomarkers. J. Clin. Sleep Med. 2011, 7, S38–S42. [Google Scholar] [CrossRef]
- Hurtado-Alvarado, G.; Pavón, L.; Castillo-García, S.A.; Hernández, M.E.; Domínguez-Salazar, E.; Velázquez-Moctezuma, J.; Gómez-González, B. Sleep Loss as a Factor to Induce Cellular and Molecular Inflammatory Variations. Clin. Dev. Immunol. 2013, 2013, 801341. [Google Scholar] [CrossRef]
- Kaneko, N.; Kurata, M.; Yamamoto, T.; Morikawa, S.; Masumoto, J. The role of interleukin-1 in general pathology. Inflamm. Regen. 2019, 39, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zielinski, M.R.; Gerashchenko, D.; Karpova, S.A.; Konanki, V.; McCarley, R.W.; Sutterwala, F.S.; Strecker, R.E.; Basheer, R. The NLRP3 inflammasome modulates sleep and NREM sleep delta power induced by spontaneous wakefulness, sleep deprivation and lipopolysaccharide. Brain Behav. Immun. 2017, 62, 137–150. [Google Scholar] [CrossRef] [Green Version]
- Conrad, C.; Di Domizio, J.; Mylonas, A.; Belkhodja, C.; DeMaria, O.; Navarini, A.A.; Lapointe, A.-K.; French, L.E.; Vernez, M.; Gilliet, M. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat. Commun. 2018, 9, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, H.J.; Mills, P.J.; Ancoli-Israel, S.; Loredo, J.S.; Ziegler, M.G.; Dimsdale, J.E. The roles of TNF-α and the soluble TNF receptor I on sleep architecture in OSA. Sleep Breath. 2009, 13, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalliolias, G.D.; Ivashkiv, L.B. TNF biology, pathogenic mechanisms and emerging therapeutic strategies. Nat. Rev. Rheumatol. 2016, 12, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, N.; Ramesh, V.; Gozal, D. TNF-α and Temporal Changes in Sleep Architecture in Mice Exposed to Sleep Fragmentation. PLoS ONE 2012, 7, e45610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockstrom, M.D.; Chen, L.; Taishi, P.; Nguyen, J.T.; Gibbons, C.M.; Veasey, S.C.; Krueger, J.M. Tumor necrosis factor alpha in sleep regulation. Sleep Med. Rev. 2018, 40, 69–78. [Google Scholar] [CrossRef]
- Lattova, Z.; Keckeis, M.; Maurovich-Horvat, E.; Wetter, T.C.; Wilde-Frenz, J.; Schuld, A.; Pollmächer, T. The stress hormone system in various sleep disorders. J. Psychiatr. Res. 2011, 45, 1223–1228. [Google Scholar] [CrossRef]
- Li, J.; Bidlingmaier, M.; Petru, R.; Gil, F.P.; Loerbroks, A.; Angerer, P. Impact of shift work on the diurnal cortisol rhythm: A one-year longitudinal study in junior physicians. J. Occup. Med. Toxicol. 2018, 13, 23. [Google Scholar] [CrossRef]
- Fekedulegn, D.; Burchfiel, C.M.; Violanti, J.M.; Hartley, T.A.; Charles, L.E.; Andrew, M.E.; Miller, D.B. Associations of Long-term Shift Work with Waking Salivary Cortisol Concentration and Patterns among Police Officers. Ind. Health 2012, 50, 476–486. [Google Scholar] [CrossRef] [Green Version]
- Heaney, J.L.J.; Phillips, A.C.; Carroll, D. Aging, Health Behaviors, and the Diurnal Rhythm and Awakening Response of Salivary Cortisol. Exp. Aging Res. 2012, 38, 295–314. [Google Scholar] [CrossRef] [Green Version]
- Ken-Dror, G.; Fry, C.H.; Murray, P.; Fluck, D.; Han, T.S. Changes in cortisol levels by continuous positive airway pressure in patients with obstructive sleep apnoea: Meta-analysis of 637 individuals. Clin. Endocrinol. 2021, 95, 909–917. [Google Scholar] [CrossRef]
- Kritikou, I.; Basta, M.; Vgontzas, A.N.; Pejovic, S.; Fernandez-Mendoza, J.; Liao, D.; Bixler, E.O.; Gaines, J.; Chrousos, G.P. Sleep apnoea and the hypothalamic–pituitary–adrenal axis in men and women: Effects of continuous positive airway pressure. Eur. Respir. J. 2016, 47, 531–540. [Google Scholar] [CrossRef]
- Minami, T.; Tachikawa, R.; Matsumoto, T.; Murase, K.; Tanizawa, K.; Inouchi, M.; Handa, T.; Oga, T.; Hirai, T.; Chin, K. Adrenal gland size in obstructive sleep apnea: Morphological assessment of hypothalamic pituitary adrenal axis activity. PLoS ONE 2019, 14, e0222592. [Google Scholar] [CrossRef] [PubMed]
- Wittenberg, G.M.; Stylianou, A.; Zhang, Y.; Sun, Y.; Gupta, A.; Jagannatha, P.S.; Wang, D.; Hsu, B.; Curran, M.E.; Khan, S.; et al. Effects of immunomodulatory drugs on depressive symptoms: A mega-analysis of randomized, placebo-controlled clinical trials in inflammatory disorders. Mol. Psychiatry 2020, 25, 1275–1285. [Google Scholar] [CrossRef] [Green Version]
- Sochal, M.; Krzywdzińska, M.; Gabryelska, A.; Talar-Wojnarowska, R.; Małecka-Panas, E. Efficiency and safety of one-year anti-TNF-α treatment in Crohn’s disease: A Polish single-centre experience. Gastroenterol. Rev. 2020, 15, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Sochal, M.; Krzywdzińska, M.; Gabryelska, A.; Talar-Wojnarowska, R.; Białasiewicz, P.; Małecka-Panas, E. A simple index to predict the efficiency of adalimumab treatment in Crohn’s disease with a limited duration of therapy. Pol. Arch. Intern. Med. 2020, 130, 910–912. [Google Scholar] [CrossRef]
- Deodhar, A.; Braun, J.; Inman, R.D.; Mack, M.; Parasuraman, S.; Buchanan, J.; Hsu, B.; Gathany, T.; Van Der Heijde, D. Golimumab reduces sleep disturbance in patients with active ankylosing spondylitis: Results from a randomized, placebo-controlled trial. Arthritis Rheum. 2010, 62, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; Gooch, K.; Michel, B.; Herold, M.; Thorner, A.; Wong, R.; Kron, M.; Chen, N.; Kupper, H. Adalimumab Improves Sleep and Sleep Quality in Patients with Active Ankylosing Spondylitis. J. Rheumatol. 2011, 38, 79–86. [Google Scholar] [CrossRef]
- Zamarron, C.; Maceiras, F.; Mera, A.; Gómez-Reino, J.J. Effect of the first infliximab infusion on sleep and alertness in patients with active rheumatoid arthritis. Ann. Rheum. Dis. 2004, 63, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Fragiadaki, K.; Tektonidou, M.G.; Konsta, M.; Chrousos, G.P.; Sfikakis, P.P. Sleep Disturbances and Interleukin 6 Receptor Inhibition in Rheumatoid Arthritis. J. Rheumatol. 2012, 39, 60–62. [Google Scholar] [CrossRef]
- Gossec, L.; Steinberg, G.; Rouanet, S.; Combe, B. Fatigue in rheumatoid arthritis: Quantitative findings on the efficacy of tocilizumab and on factors associated with fatigue. The French multicentre prospective PEPS Study. Clin. Exp. Rheumatol. 2015, 33, 664–670. [Google Scholar] [PubMed]
- Mease, P.; Walsh, J.A.; Baraliakos, X.; Inman, R.; De Vlam, K.; Wei, J.C.-C.; Hunter, T.; Gallo, G.; Sandoval, D.; Zhao, F.; et al. Translating Improvements with Ixekizumab in Clinical Trial Outcomes into Clinical Practice: ASAS40, Pain, Fatigue, and Sleep in Ankylosing Spondylitis. Rheumatol. Ther. 2019, 6, 435–450. [Google Scholar] [CrossRef] [Green Version]
- van der Zweerde, T.; Bisdounis, L.; Kyle, S.D.; Lancee, J.; van Straten, A. Cognitive behavioral therapy for insomnia: A meta-analysis of long-term effects in controlled studies. Sleep Med. Rev. 2019, 48, 101208. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Breen, E.C.; Witarama, T.; Carrillo, C.; Sadeghi, N.; Arevalo, J.M.; Ma, J.; Nicassio, P.; Bootzin, R.; et al. Cognitive Behavioral Therapy and Tai Chi Reverse Cellular and Genomic Markers of Inflammation in Late-Life Insomnia: A Randomized Controlled Trial. Biol. Psychiatry 2015, 78, 721–729. [Google Scholar] [CrossRef] [Green Version]
- Vich Vila, A.; Collij, V.; Sanna, S.; Sinha, T.; Imhann, F.; Bourgonje, A.; Mujagic, Z.; Jonkers, D.M.A.E.; Masclee, A.A.M.; Fu, J.; et al. Impact of commonly used drugs on the composition and metabolic function of the gut microbiota. Nat. Commun. 2020, 11, 362. [Google Scholar] [CrossRef] [PubMed]
- Bultink, I.E.M.; de Vries, F.; van Vollenhoven, R.F.; Lalmohamed, A. Mortality, causes of death and influence of medication use in patients with systemic lupus erythematosus vs matched controls. Rheumatology 2021, 60, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Braley, T.J.; Segal, B.M.; Chervin, R.D. Hypnotic use and fatigue in multiple sclerosis. Sleep Med. 2015, 16, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Groselj, L.D.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Guina, J.; Merrill, B. Benzodiazepines I: Upping the Care on Downers: The Evidence of Risks, Benefits and Alternatives. J. Clin. Med. 2018, 7, 17. [Google Scholar] [CrossRef] [Green Version]
- Mehrez, S.I.; El-Kharashi, O.A. Diazepam dose-dependently Aggravates Mucosal Damage in a Rat Model of Ulcerative Colitis. Egypt. J. Basic Clin. Pharmacol. 2013, 3, 21–29. [Google Scholar] [CrossRef]
- Roth, T.; Price, J.M.; Amato, D.A.; Rubens, R.P.; Roach, J.M.; Schnitzer, T.J. The Effect of Eszopiclone in Patients with Insomnia and Coexisting Rheumatoid Arthritis. Prim. Care Companion J. Clin. Psychiatry 2009, 11, 292–301. [Google Scholar] [CrossRef]
- Yeung, W.-F.; Chung, K.-F.; Yung, K.-P.; Ng, T.H.-Y. Doxepin for insomnia: A systematic review of randomized placebo-controlled trials. Sleep Med. Rev. 2015, 19, 75–83. [Google Scholar] [CrossRef]
- Iskandar, H.N.; Cassell, B.; Kanuri, N.; Gyawali, C.P.; Gutierrez, A.; Dassopoulos, T.; Ciorba, M.A.; Sayuk, G.S. Tricyclic Antidepressants for Management of Residual Symptoms in Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2014, 48, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Mews, M.R.; Rombold, F.; Quante, A. Efficacy and Safety of Low-Dose Doxepin in Depressed Patients Suffering From Insomnia: A Retrospective, Naturalistic Case Series Analysis. Prim. Care Companion CNS Disord. 2014, 16, PCC.13m01567. [Google Scholar] [CrossRef] [Green Version]
- Sobańska, A.; Wichniak, A.; Wierbicka, A.; Szatkowska, E.; Czasak, K.; Musińska, I.; Jernajczyk, W. Mianserin for primary insomnia treatment. Sen 2006, 6, 58–63. [Google Scholar]
- Bennett, T.; Bray, D.; Neville, M.W. Suvorexant, a Dual Orexin Receptor Antagonist for the Management of Insomnia. Pharm. Ther. 2014, 39, 264–266. [Google Scholar]
- Auld, F.; Maschauer, E.L.; Morrison, I.; Skene, D.J.; Riha, R.L. Evidence for the efficacy of melatonin in the treatment of primary adult sleep disorders. Sleep Med. Rev. 2017, 34, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, A.; Honda, M.; Hayashino, Y. Ramelteon for the treatment of insomnia in adults: A systematic review and meta-analysis. Sleep Med. 2014, 15, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Mi, W.-F.; Tabarak, S.; Wang, L.; Zhang, S.-Z.; Lin, X.; Du, L.-T.; Liu, Z.; Bao, Y.-P.; Gao, X.-J.; Zhang, W.-H.; et al. Effects of agomelatine and mirtazapine on sleep disturbances in major depressive disorder: Evidence from polysomnographic and resting-state functional connectivity analyses. Sleep 2020, 43, zsaa092. [Google Scholar] [CrossRef]
- De Berardis, D.; Fornaro, M.; Serroni, N.; Campanella, D.; Rapini, G.; Olivieri, L.; Srinivasan, V.; Iasevoli, F.; Tomasetti, C.; De Bartolomeis, A.; et al. Agomelatine beyond Borders: Current Evidences of Its Efficacy in Disorders Other than Major Depression. Int. J. Mol. Sci. 2015, 16, 1111–1130. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.-S.; Chung, S.-H.; Lee, S.-K.; Kim, J.-H.; Kim, J.-B.; Kim, T.-K.; Kim, D.-S.; Baik, H.-W. Melatonin improves experimental colitis with sleep deprivation. Int. J. Mol. Med. 2015, 35, 979–986. [Google Scholar] [CrossRef]
- Kim, J.-Y.; Lee, Y.-D.; Kim, B.-J.; Kim, S.-P.; Kim, D.-H.; Jo, K.-J.; Lee, S.-K.; Lee, K.-H.; Baik, H.-W. Melatonin improves inflammatory cytokine profiles in lung inflammation associated with sleep deprivation. Mol. Med. Rep. 2012, 5, 1281–1284. [Google Scholar] [CrossRef]
- Zhou, L.-L.; Wei, W.; Si, J.-F.; Yuan, D.-P. Regulatory Effect of Melatonin on Cytokine Disturbances in the Pristane-Induced Lupus Mice. Mediat. Inflamm. 2010, 2010, 951210. [Google Scholar] [CrossRef]
- Macdonald, I.J.; Huang, C.-C.; Liu, S.-C.; Tang, C.-H. Reconsidering the Role of Melatonin in Rheumatoid Arthritis. Int. J. Mol. Sci. 2020, 21, 2877. [Google Scholar] [CrossRef]
- Chojnacki, C.; Wisniewska-Jarosinska, M.; Walecka-Kapica, E.; Klupinska, G.; Jaworek, J.; Chojnacki, J. Evaluation of melatonin effectiveness in the adjuvant treatment of ulcerative colitis. J. Physiol. Pharmacol. 2011, 62, 327–334. [Google Scholar]
- Mu, Q.; Zhang, H.; Liao, X.; Lin, K.; Liu, H.; Edwards, M.R.; Ahmed, S.A.; Yuan, R.; Li, L.; Cecere, T.E.; et al. Control of lupus nephritis by changes of gut microbiota. Microbiome 2017, 5, 73. [Google Scholar] [CrossRef]
- Wilkins, T.; Sequoia, J. Probiotics for Gastrointestinal Conditions: A Summary of the Evidence. Am. Fam. Physician 2017, 96, 170–178. [Google Scholar]
- Morshedi, M.; Hashemi, R.; Moazzen, S.; Sahebkar, A.; Hosseinifard, E.-S. Immunomodulatory and anti-inflammatory effects of probiotics in multiple sclerosis: A systematic review. J. Neuroinflammation 2019, 16, 231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhanoa, H. Probiotics for the Management of Rheumatoid Arthritis. In Bioactive Food as Dietary Interventions for Arthritis and Related Inflammatory Diseases, 2nd ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 23–35. [Google Scholar] [CrossRef] [Green Version]
- Szentirmai, É.; Millican, N.S.; Massie, A.R.; Kapas, L. Butyrate, a metabolite of intestinal bacteria, enhances sleep. Sci. Rep. 2019, 9, 7035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, H.; Lee, J.-H.; Lloyd, J.; Walter, P.; Rane, S.G. Beneficial Metabolic Effects of a Probiotic via Butyrate-induced GLP-1 Hormone Secretion. J. Biol. Chem. 2013, 288, 25088–25097. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.S.; Roller, R.; Mika, A.; Greenwood, B.N.; Knight, R.; Chichlowski, M.; Berg, B.M.; Fleshner, M. Dietary Prebiotics and Bioactive Milk Fractions Improve NREM Sleep, Enhance REM Sleep Rebound and Attenuate the Stress-Induced Decrease in Diurnal Temperature and Gut Microbial Alpha Diversity. Front. Behav. Neurosci. 2017, 10, 240. [Google Scholar] [CrossRef]
- Moser, N.J.; Phillips, B.A.; Guthrie, G.; Barnett, G. Effects of Dexamethasone on Sleep. Pharmacol. Toxicol. 1996, 79, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Kraemer, D.F.; Kanar, O.; Berry, A.C.; Smotherman, C.; Eid, E. Immunomodulator and Biologic Agent Effects on Sleep Quality in Patients with Inflammatory Bowel Disease. Ochsner J. 2018, 18, 76–80. [Google Scholar] [PubMed]
- Unnikrishnan, D.C.; Jun, J.; Polotsky, V. Inflammation in sleep apnea: An update. Rev. Endocr. Metab. Disord. 2015, 16, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ditmer, M.; Gabryelska, A.; Turkiewicz, S.; Białasiewicz, P.; Małecka-Wojciesko, E.; Sochal, M. Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. J. Clin. Med. 2022, 11, 67. https://doi.org/10.3390/jcm11010067
Ditmer M, Gabryelska A, Turkiewicz S, Białasiewicz P, Małecka-Wojciesko E, Sochal M. Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. Journal of Clinical Medicine. 2022; 11(1):67. https://doi.org/10.3390/jcm11010067
Chicago/Turabian StyleDitmer, Marta, Agata Gabryelska, Szymon Turkiewicz, Piotr Białasiewicz, Ewa Małecka-Wojciesko, and Marcin Sochal. 2022. "Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review" Journal of Clinical Medicine 11, no. 1: 67. https://doi.org/10.3390/jcm11010067