Biodegradable Metallic Wires in Dental and Orthopedic Applications: A Review
by

Mohammad Asgari
1,2, 
Ruiqiang Hang
1,3,
Chang Wang
4,5,
Zhentao Yu
4,5,
Zhiyong Li
1,2,* and
Yin Xiao
1,2,6,* 1
The Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, QLD 4059, Australia
2
School of Chemistry, Physics & Mechanical Engineering, Science & Engineering Faculty, Queensland University of Technology, Brisbane, QLD 4000, Australia
3
Research Institute of Surface Engineering, Taiyuan University of Technology, Taiyuan 030024, China
4
Northwest Institute for Nonferrous Metal Research, Shaanxi Key Laboratory of Biomedical Metal Materials, Xi’an 710016, China
5
China-Australia Joint Research Centre of Biomedical Metallic Materials, Shaanxi Key Laboratory of Biomedical Metal Materials, Xi’an 710016, China
6
The Australia-China Centre for Tissue Engineering and Regenerative Medicine (ACCTERM), Queensland University of Technology, Brisbane, QLD 4059, Australia
*
Authors to whom correspondence should be addressed.
Metals 2018, 8(4), 212; https://doi.org/10.3390/met8040212
Submission received: 30 January 2018
/
Revised: 22 March 2018
/
Accepted: 22 March 2018
/
Published: 26 March 2018
(This article belongs to the Special Issue Biodegradable Metals)
Abstract
:Owing to significant advantages of bioactivity and biodegradability, biodegradable metallic materials such as magnesium, iron, and zinc and their alloys have been widely studied over recent years. Metallic wires with superior tensile strength and proper ductility can be fabricated by a traditional metalworking process (drawing). Drawn biodegradable metallic wires are popular biodegradable materials, which are promising in different clinical applications such as orthopedic fixation, surgical staples, cardiovascular stents, and aneurysm occlusion. This paper presents recent advances associated with the application of biodegradable metallic wires used in dental and orthopedic fields. Furthermore, the effects of some parameters such as the surface modification, alloying elements, and fabrication process affecting the degradation rate as well as biocompatibility, bioactivity, and mechanical stability are reviewed in the most recent works pertaining to these materials. Finally, possible pathways for future studies regarding the production of more efficient biodegradable metallic wires in the regeneration of bone defects are also proposed.
1. Introduction
Metallic wires have been widely used in a wide range of industries in different applications. Drawing is a conventional metal forming process which has been applied to fabricate metallic wire. Briefly, this process continuously decreases the cross-sectional area of a specimen by pulling it through a single (in single-pass drawing) or series (in the multi-pass drawing) of the conical die(s) [1]. Figure 1 shows the schematic of die geometry in single-pass wire drawing process. di, do and α are the input diameter, the output diameter and die angle respectively. Due to imparting of a huge cold working happened during the drawing process, production of thin metallic wire with considerable strength is potentially achievable [2]. Equation (1) represents the percentage of cold work that could be achieved by single-pass wire drawing process [3]:
Moreover, different intermediate and/or post heat treatments coinciding with precise die(s) design and manufacturing could lead to the fabrication of the fine wire with acceptable ductility for different applications [3].
Over recent decades, the application of the wire drawing process in the production of biomedical metallic wires has been investigated. Drawn wires from titanium (Ti) and its alloys, stainless steels (SSs), and nitinol have been used in different medical devices such as cardiovascular stents [4], coronary guide catheter [5], coil occlusion of the aneurysm [6], Kirschner wires (K-wire) [7], orthodontic archwires [8], ligature wire [9], surgical sutures and versus staples [10]. Based on the application, such devices might be implanted either for a short or long time in the human body and regardless of the duration time, after finishing their mission, they should be removed from the body by a secondary operation. Because they cannot be degraded by human body fluids and, in some cases, if they are kept for more time, they will lead to complications such as harsh inflammations [11].
To decrease the clinical expenses and increase the quality of life of patients by reducing any secondary surgeries for removal of metal implants as well as minimizing any negative consequences, a new generation of metallic biomaterials has been introduced as a temporary support. These kinds of materials, called biodegradable metals (BMs), are strong enough during the target tissue healing process and can be gradually resorbed in the human body [12,13]. The degradation of BMs mainly ascribes to electrochemical corrosion, during which process the metal atoms lose their free electrons, become cations and enter body fluids. The content and the releasing allowance of those ions should not be toxic to the human body, especially for the surrounding host tissues [14]. To that aim, up to now different biodegradable alloys have been introduced. Among them, magnesium (Mg), iron (Fe), zinc (Zn), and their alloys as biodegradable implant metals are the three main categories that are considered more than other beneficial elements such as calcium (Ca) and strontium (Sr) [13].
In addition to the structural role of Mg, Fe, Zn, and their alloys as an implant device, they play important roles in many metabolic reactions and biological mechanisms of the body and consequently reduce the healing duration [15]. That is the reason they are named nutrient metals (NMs) [14,16]. Up to now, many studies have been conducted to increase the performance of these NMs by enhancing their initial mechanical properties and mitigating their potential drawbacks such as imperfect degradation rate to convert them from mechanical replacement devices to nutrient implants.
As an implant device, BMs in the shape of wire were firstly applied in 1878 by Edward C. Huse. He used pure Mg wire as a ligature to stop bleeding vessels. Although Huse reported the first clinical application of Mg wire, the Austrian surgeon Prof. Dr. Erwin Payr is known as the pioneer in the field of biodegradable Mg implants. His valuable results and consequently his inspiring articles published from 1892 to 1905 led to the utilization of biodegradable metallic wires in both human and animal models by other researchers [17]. Andrews in 1917 [18], and Seelig in 1924 [19] were early followers who investigated the animal in vivo experiments of pure Mg wire. From that time, a considerable number of feasibility studies have been done to propose Mg, Fe and more recently Zn and their alloys as ideal candidates in interventional clinical devices such as cardiovascular stents [20], and orthopedic implants [1,21]. However, there are still some challenges including improvement of both the surface and bulk properties such as corrosion resistance, bioactivity, strength, ductility, and toxicity. These properties need to be modified by more investigations to approve the application of BMs and their alloys in different medical operations without any negative consequences about the health of patients.
The present review mainly focuses on the recent progress related to the usage of biodegradable metallic wires in the orthopedic and dental studies. To that aim, the positive and any possible negative effects of Mg, Fe, and Zn on the bone biological mechanisms and bone healing process are generally presented first. Then, the history of clinical application development of each of these metals and their alloys in the shape of wires is reviewed. Furthermore, any other related scientific results to in vitro and in vivo studies of the biodegradable metallic wires are briefly summarized. Finally, the remaining problems in this research field that could be addressed in the future work are discussed and some possible options that are beneficial to the improvement of the clinical performance of these wires in the bone applications are also proposed.
2. Biological and Mechanical Aspects of Biodegradable Metallic Materials for Bone Regeneration Applications
2.1. Mg and Its Alloys
2.1.1. Advantages of Mg and Its Alloys
Mg as a mineral is the fourth most abundant cation element in the body [22]. It has a pivotal role in many body metabolisms including enzymatic reaction, the formation of apatite, and bone cells adsorption [23]. About half of the total amount of Mg in our body is stored in bone tissue [24]. Wu et al. reported that Mg ions (Mg2+) govern a stimulating effect on the new bone formation by increasing the proliferation and differentiation of osteogenic (stem) cells via osteogenesis-related signaling pathways in vitro [25]. The release of Mg2+ is related to the chemical reaction of Mg in the human body fluids based on the following reaction which produces Mg hydroxide (Mg(OH)2) and hydrogen gas (H2) evolution [26]:
Zheng et al. [27] presented a degradation mechanism for Mg in the physiological environment by the following anodic dissolution and cathodic reduction reactions:
Mg2+ (aq) + 2OH− → Mg(OH)2 (s) (cathodic reaction)
It is clear that Mg2+ originates from the anodic reaction. Then, some of them take part in a reaction with hydroxide ions (OH−) to produce Mg(OH)2, while others enter the solution.
Mg(OH)2, which is called milk of magnesia, includes both water and MgO solid particles. Hence, some part of it can convert to MgO and vice versa (see Equation (6)):
Both of Mg(OH)2 and MgO are beneficial inorganic materials to the body [28]. In addition to the conventional medical application of Mg(OH)2 which has been widely used as an antacid to neutralize stomach acid and a laxative, it also possesses numerous valuable properties including excellent biocompatibility, nontoxic antibacterial activity, and high drug loading ability [29]. In bone regeneration application, as a major degradation product from any magnesium alloys, Mg(OH)2 can enhance the bone formation and temporarily decrease the bone resorption resulting in a higher bone mass [30,31]. Therefore, it could be a potential protective coating material for Mg-based implants to reduce the corrosion rate and improve bone ingrowth simultaneously [31].
Regardless of the wide range of industrial applications, MgO similar to Mg(OH)2 is applied as both an antacid and a laxative. It is also used as a drying agent because it rapidly reacts with water and creates Mg(OH)2 [28]. MgO in shape of nanoparticles has been introduced as a novel antibacterial material to enhance tissue regeneration process and reduce bacterial infection during orthopedic implantations [32]. Huang et al. [33] claimed that the toxicity of MgO against bacteria increased by reducing its particle size. Hickey et al. [32] fabricated nanocomposites using MgO nanoparticles to mineralize poly(l-lactic acid) (PLLA) and applied in traumatic brain injury(TBI)-related orthopedic tissue regeneration. They reported that all the seeded bacteria were killed by PLLA/MgO nanocomposite. Therefore, MgO, as one of the corrosion products of Mg and its alloys play an antibacterial role for orthopedic tissue engineering applications.
In terms of mechanical aspects, Mg and its biocompatible alloys are more advantageous in bone applications in comparison with other metallic materials, ceramics, and biodegradable polymers (BPs). Because the mechanical properties of Mg are more similar to those of natural cortical bone compared to other materials which can decrease the stress shielding effect and prevent consequent bone resorption in the implanted sites [34,35], that makes Mg the most attractive biodegradable material in the orthopedic devices and implants as a suitable substitution for the non-bioresorbable one. Table 1 summarizes the information about the typical mechanical properties of cortical bone and commonly used metallic biomaterials.
2.1.2. Disadvantages of Mg and Its Alloys
The standard electrode potential for Mg(s) ↔ Mg2+(aq) + 2e− reaction is very low (−2.37 V) [38], making Mg very reactive in aqueous solutions such as body fluids. Although there is a gap between in vitro and in vivo results regarding the corrosion mechanism of Mg [39], commonly for both in vitro and in vivo the oxide film formed on the surface of Mg is porous rather than dense, thus cannot effectively prevent direct contact between metallic Mg and solution, leading to the rapid degradation of Mg and its alloys. The reduction in the mechanical stability due to the stress corrosion cracking is the first negative consequence related to such high corrosion rate of Mg and its alloys, risking the adequate load shielding over the tissue regeneration duration, especially in load-bearing applications [13,40]. Therefore, it is vitally important that there should be a balance between the degradation time and the healing period of damaged tissue to prevent implantation mechanical failure. It is the point that should be considered in the geometry design, material selection, and fabrication process of all BMs and their alloys generally, and more critical for Mg and its alloys.
Hydrogen gas (H2) evolution is another challenging issue in the application of Mg and its alloys in the body. Based on Equation (2), 1 g of pure Mg could produce 1 liter (L) of H2 gas [41]. Rely on previous in vivo experiments, some of this gas is soluble in the blood. The solubility of H2 depends on the amount of the blood flow in the implantation site. The remained H2 bubbles are accumulated in the local host tissue and create gas cavity endangering the cell adhesion to implants [42]. In some applications such as cardiovascular stents, due to the convective transport phenomena, the evolution of H2 is not as concerning as orthopedic applications; because bone inherently is a poorly vascularized tissue leading to the formation of H2 cavities potentially [26]. Some animal studies have shown that it might be dangerous [43]. In 2016, Noviana et al. [41] investigated the effect of H2 evolution from porous pure-magnesium implants on the mortality of adult rats. They reported that the cavity formation was not tolerable for all the rats and the survival rate at Day 18 post-implantation reached zero percent (see Figure 2). Hence, such amount of post-implantation mortality is a warning sign for the risk of excessive H2 accumulation in the large implants such as fixation plates. Nonetheless, due to the very light mass and negligible surface area of fine magnesium wire having sub-millimeter diameter there should not be that much of concern regarding the risk of H2 gas evolution. However, it is still an estimation that needs to be investigated precisely by more in vitro and in vivo studies.
2.2. Fe and Its Alloys
2.2.1. Advantages of Fe and Its Alloys
Iron (Fe) as the fourth most abundant element on earth is significantly necessary for the human body and takes part in many enzymatic systems. The hemoglobin uses the largest part of total Fe (about 60–70%). Whereas, only about 10% of it is stored in bone marrow [44]. Fe has an essential role in the function of red blood cells and oxygen transport throughout the body. Fe deficiency may decrease the number of healthy oxygen-carrying red blood cells, thus has a negative effect on physical activity and increases susceptibility to infections [45]. Fe has a crucial role in bone metabolism by participating in two main biological processes including collagen synthesis and vitamin D activation and deactivation [46]. The clinical observations have shown that both Fe overload and deficiency (with or without anemia) could happen for the patients who suffered from osteoporosis [45,46]. The link between Fe and bone metabolism, especially in the homeostasis of bone ageing to maintain a balance between bone formation and resorption, is still in a need of further investigation, especially for elderly people to increase the quality of their life.
Almost all of the previous in vivo studies in animal models have been mainly focused on the application of Fe and its alloys as suitable degradable implant materials in the fabrication of cardiovascular stents [47]. While there are few studies in literature related to the bone application of Fe and its alloys. Kraus et al. [48] followed up the degradation behavior of Fe-based wires implanted into the femur of 38 rats for 52 weeks. Regardless of some results [48] showing that Fe ions could release from the implanted wires into the surrounding tissues, there is no clear information about its benefits on bone regeneration process.
2.2.2. Disadvantages of Fe and Its Alloys
The standard electrode potential for the reaction of Fe(s) ↔ Fe2+(aq) + 2e− is relatively high (−0.444 V) [49]. Furthermore, owing to including a high concentration of CO2 gas in blood causing to create a uniform, compact and dense manganese carbonate crystals the degradation rate of Fe in vivo is slower than in vitro [50] and in most of the cases is longer than clinical needs [51]. Additionally, because of the low rate of blood circulation near the implants, utilization of Fe and its alloys for bone reconstruction purposes would be definitely lower than their corrosion rate. Adding some alloying elements to pure Fe has been reported to be one of the most effective methods to accelerate the degradation rate of Fe to an acceptable level for practical clinical usage [12,44]. Among all of the Fe-based alloys, Fe–Mn alloys have been proved to be the most promising ones in accelerating the corrosion rate of Fe with similar mechanical properties (i.e., Young’s modulus and ultimate tensile strength) to 316L SS [51]. Moreover, Mn can play an important role in promoting the growth of new bone and connective tissues as well as reducing bone loss [52,53] which could increase its bioactivity in orthopedic and dental applications. However, Fe and its alloys have much higher mechanical properties than those of the human cortical bone (see Table 1), which keeps the stress shielding effect as a challenging issue to select them as a suitable candidate in the load-bearing locations, especially as bulk temporary implants.
2.3. Zn and Its Alloys
2.3.1. Advantages of Zn and Its Alloys
Zinc (Zn) as the second most abundant transition metal element in the human body is found in all organs, tissues, fluids, and body secretions [54,55]. It is considered to be one of the vital mineral elements participating in a variety of fundamental biological functions, including signal transduction, apoptosis regulation as well as nucleic acid metabolism, DNA and RNA polymerase, and organic ligands interactions [56,57,58]. Approximately 85% of the Zn content of body exists in bone and muscle [14] which serves a crucial role in the improvement of cell proliferation and osteo-related gene expressions of osteoblasts affecting bone in growth [59,60]. Li et al. [56] investigated the biological effects of the Zn-1X(Mg, Ca and Sr) binary alloys using thin pin shape implants inserted into the bone tunnel created along the axis of the femoral shaft from the distal femur of mice. They reported that the Zn-1X binary alloys with nutrient alloying elements improved new bone formation around the pins effectively. Other in vivo and in vitro studies have shown that Zn affects the osteoclastic bone resorption metabolism [61,62]. The Zn content in the bone matrix of patients suffering from skeletal diseases such as osteoporosis (commonly in elderly people) and bone cancer is less than that of normal people [56,63]. In summary, having a healthy bone with sufficient density is correlated with the balancing of Zn content in the human body.
It has been well established that Zn ions (Zn2+) show antibacterial property [64,65,66]. Recently, Zhu et al. [59] introduced plasma immersion ion implantation (PIII) process as a promising method for Zn-incorporation on Ti alloy, which is beneficial to both osteogenic and antibacterial abilities to enhance osseointegration while decreases implant-associated infections. Zn2+ are released directly from the corrosion of Zn and its possible alloys when in contact with the human body fluids through electrochemical corrosion. Drelich et al. proposed [67] the hypothetical mechanism happening during the degradation of Zn in the physiological environment (Figure 3). The reaction between some of Zn2+ with hydroxyl ions (OH−) forms Zn oxide (ZnO). In addition to the wide range of dental and orthopedic applications of ZnO, due to its desirable antibacterial and osteogenic abilities, the anti-cancer property of ZnO has been also approved as a beneficial material to cure osteosarcoma [68,69].
The standard potential for the cathodic reaction of Zn is −0.762 V [49], which is between that of Mg and Fe. Therefore, the moderate degradation rate of Zn is faster than Fe but slower than Mg, which could be an ideal option for clinical applications, especially in terms of mechanical stability [55]. More recently, Yang et al. [57] implanted pure Zn stents into the abdominal aorta of rabbits for 12 months. They reported that the stent was capable to serve mechanical stability for the first 6 months and degraded 41.75 ± 29.72% of the stent volume after 12 months of implantation without any severe inflammations, platelet aggregation, and thrombosis formation. Furthermore, in the matter of accumulation of H2 during the degradation, there is less concern in the application of Zn and its alloys in bone applications than that of Mg and its alloys. Because it seems that the corrosion rate of Zn is low enough to prepare a time for the dissolving of H2 in the body without the creation of any gas cavities.
2.3.2. Disadvantages of Zn and Its Alloys
Generally, pure Zn is soft, brittle with low strength (Table 1). Therefore, it seems impossible to apply pure zinc in load-bearing applications. The addition of alloying elements has been recognized as one of the most effective methods to improve the mechanical properties of pure Zn [56]. Even adding a little amount of alloying elements can improve its mechanical properties considerably. Briefly, depending on the composition of the Zn alloys the ultimate tensile strength (UTS) has been achieved in a wide range of 87 to 399 MPa till now [55,70]. Moreover, other parameters such as using different metalworking processes such as rolling, extortion, and post-processing heat treatments can definitely affect the strength, ductility, and degradation behavior of Zn-based alloys. However, Young’s modulus (E) of Zn is about twice as that of Mg, which indicates that the stress shielding effect is more challenging in Zn-based implants.
Non-uniform corrosion behavior of Zn compared to uniform corrosion of both Mg and Fe is another problem. Chen et al. [15] compared the corrosion behavior of Zn, Fe and Mg in a long-term course in vitro. They observed that by increasing immersion time the corrosion rate of Zn developed faster than Fe and Mg, which is justified by the occurrence of localized corrosion in the surface of Zn samples. Similar behavior was reported in vivo [57]. The localized corrosion causes to lose the strength uniformity of an implant which makes its failure behavior more ambiguous. Drelich et al. [67] claimed that coating of Zn with a passive layer of ZnO film could be an effective approach to delay the degradation rate and decrease the corrosion non-uniformity. However, Törne et al. [71] claimed that the corrosion behavior of Zn is affected by the types of examined solution. They proposed that whole blood or real plasma are suitable solutions for short-term in vitro studies which can resemble in vivo situation, while Ringer’s solution is more suitable for long-term degradation studies. Collectively, more in vivo and in vitro investigations should be conducted for the better understanding of the corrosion behavior of Zn in bone applications to address those contradicting results.
3. Current Orthopedic and Dental Implant Applications of Metallic Wires
The skeletal system of the human body as a complex three-dimensional structure plays two main roles, supporting the many body organs and their related tissues and attaching the numerous muscle groups which are needed for body movements. Bone as the hard part of the skeleton is a natural two- phase organic-inorganic ceramic composite. The organic phase gives bone its flexibility, while the inorganic phase provides bone with its structural rigidity [72]. The combination of organic and inorganic phases in the matrix provides bone with the unique mechanical properties such as toughness, strength, and stiffness. These properties give the ability to withstand against various mechanical loads applied during the normal and intense physical activities. Despite the remarkable mechanical and structural characteristics, the bone may fracture due to various loads resulting from sudden injuries and repeated cyclic loads. An effective solution in restoring the functionality of damaged bone is surgical implantation of artificial biomaterials. Several types of bone fixation devices in the form of screws, plates, nails, staples, and wires are produced for orthopedic and dental implant applications. The selection of biomaterials for these devices is highly dependent on the specific medical application. The new biomaterials which were introduced and developed for implant applications should have excellent biocompatibility, comparable strength to natural bone and produce no cytotoxicity effects [73]. The present review paper focuses on the bone application of wires; therefore, in this section, bone fixation devices which are made from wires are introduced first and then the evolution of the biomaterials to be compatible with natural bone are explained.
3.1. K-Wires
Martin Krischner (1879–1942) was a German surgeon who developed a device that allowed him to insert chromed piano wire from 0.7 to 1.5 mm in diameter into fractured bones to be used as a traction anchor instead of the large Steinmann pins [74]. Krischner wires (K-wires) were never used by their inventor for fracture fixation and orthopedic implants [75]. Otto Lowe [74] in 1932 published the first paper describing the use of K-wires for fracture fragment stabilization. Nowadays, these wires with different sizes have been used to hold bone fragments together (pin fixation) or to provide an anchor for skeletal traction. K-wires can also serve as guide pins for the placement of cannulated screws and can be placed in bone either by hand or at low speed with a power drill [75,76]. Figure 4a shows radiographic picture of K-wires used to repair a fracture of the medial epicondyle in the elbow.
3.2. Cerclage Wires
The other application of thinner orthopedic wire is as a means of stabilizing fracture fragments. Cerclage wiring refers to encircling fragments and tensioning the wire to hold fragments in alignment [76]. A single or double strand of the wire is placed around the bone, and then the ends are twisted together. Cerclage wires are usually used in combination with other types of fixation devices such as plates or nails, but can also be used alone in special situations [76]. The radiograph in Figure 4b shows cerclage wiring used to contain bone fragments in a fracture around the stem of a femoral prosthesis.
3.3. Tension-Band Wires
The tension band technique converts a tensile force to the compression one. Tension banding is particularly useful in the setting of fractures where a muscle pull produces distraction of the fracture fragments, such as fracture of the patella [76]. Parallel K-wires are placed to provide rotational stability and reduce shearing forces between the fragments. Figure 5 presents an application of tension band wiring in repairing of an olecranon fracture.
3.4. Orthodontic Archwires
An orthodontic archwire is a wire conforming the dental arch and exerts forces to correct irregularities in the position of teeth. An archwire can be used with dental braces as a source of force. Orthodontic wires release the energy stored upon its placement by applying forces and torque to the teeth through the appliances placed on them [77]. The forces are applied to move the teeth to a targeted position. Another application of these wires is maintaining the existing dental position; in this case, they have a retentive purpose [77].
3.5. Ligature Wires
3.6. Staples
The bone staple is essentially simple in design and use. This device is made up two or more points of entry into bone that are attached to each other. They can be fabricated by double bending a pin or wire that is biased cut to create the sharp ends or tips [10]. The bone staples are fixed into the bone to help stabilize a fracture to promote bone healing. Bone staples can be used as adjuncts to other forms of fixations or as single or multiple bone staples at one site.
3.7. Sutures
Metallic sutures are available in many sizes and in two forms: monofilament or multi-strand. Most surgeons find the multi-strand wires are easier to handle since they are pliable and ties like silk [79].
4. The evolution of Metallic Wires in Bone Fixation Devices
K-wires as a versatile tool in the hand of orthopedic surgeons have been used for temporary or definitive osteosynthesis, temporary joint transfixation or for the guidance of other implants such as cannulated screws. K-wires are present in different forms and designs. Traditional K-wires have a circular cross-section and two tip designs (diamond and trocar tips). Diamond tip K-wires require the least axial force to penetrate the bone and consequently generate low heat during drilling, while the trocar tip wires need a greater force and generate higher temperature on insertion [80]. According to a surgical instrumentation catalogue, the diameter of standard K-wires based on their applications varies between 0.4 and 3.5 mm. Besides the strengthening of K-wires by enhancing the mechanical properties of their materials, the configuration of them has been studied in some researches [81,82]. Different K-wire fixation techniques contained two or four K-wires with different diameter were investigated and it was observed that the type of configuration was an effective parameter in increasing of the rigidity and stability of the fractured bone [81,82].
The first usage of wires in fracture fixation was reported in 1775 when Fe wires were used in a bone surgery [27]. In 1906, Lambotte used a combination of a Fe wire cerclage, Mg plate and steel screws to stabilize the fracture of the lower leg [17]. The occurrence of an electrochemical reaction between Mg and Fe caused extensive subcutaneous gas cavities, local swelling and pain one-day post-surgery [27]. By observing these symptoms, Lambotte learned that to avoid galvanic corrosion of the Mg, it should not be implanted with other metals [17]. Lambotte also used pure Mg nails alone to fix supracondylar fractures of four children. He observed the formation of gas cavities due to the high corrosion rate of magnesium in vivo [37]. Mainly, because of this problem, the application of Mg wires was restricted, and SS wires were introduced instead. The biometals used in wire bone fixation devices are classified into two categories, permanent and biodegradable metals. Among permanent metallic wires, surgical SS, cobalt-chromium (CoCr) alloys and Ti alloys are the most common ones. In the following sections, the application of these two groups was described in wire bone fixation devices.
4.1. Permanent Metallic Wires
In 1920, the first type of SS namely 18-8 was used as a bone implant. This alloy showed higher corrosion resistant and mechanical strength in comparison with that of pure Fe. Since then, various types of SSs were developed and some of them were used as a proper material for K-wires and cerclage wires. In 1962, the American Society for Testing and Materials (ASTM) has formed committee F04 on medical and surgical materials and devices to standardized metals for medical applications. Table 2 shows the differently registered biomaterials for bone wires in the ASTM standard.
In 1988, Stark et al. were the first researchers to recommend the use of SS K-wires in all grafted fractures, since they were easy to accomplish and required short operating time [83]. They also achieved 97% union of long-standing ununited fractures of the scaphoid by examining 151 patients through 22 years, which was a great achievement with K-wires [83]. SS K-wires provide strong fixation but can be difficult to manipulate and often requires a secondary operation to remove the wire. Due to the mismatch between the mechanical properties of the wires and the natural bone, mechanical forces and loads are retained by the wires and are not transferred to the damaged bone. Consequently, stress shielding happens and results in bone resorption and wire loosening. In addition to stress shielding effect as well as need for the second surgery, K-wires may cause percutaneous pin tract infection and wire migration [84,85].
The most basic materials used in K-wires are SSs, Co-Cr alloys, Ti and its alloys and nitinol. It should be noted that the nitinol is an alloy of nickel and titanium elements where the two elements are present in roughly equal atomic percentages. Since 1930, it has been known that Co-based alloys due to their excellent wear resistance which is higher than SS, are proper candidates for bone repair devices [87]. These alloys possess excellent mechanical properties. CoCr alloys also have one order of magnitude greater corrosion resistance in comparison with SSs. Mainly, due to these properties, cobalt and its alloys specially, MP35N, modified 35NLT and Elgiloy, have achieved wide attention for fabrication of K-wires, cerclage wires and guide wires [86].
The performance of medical grade Ti alloys is superior to that of SS and cobalt alloys, due to the 50% greater strength to weight ratio of the former. These alloys have a lower modulus, higher corrosion resistance and better biocompatibility in comparison with SSs and cobalt-based alloys. These advantages make the Ti and its alloys a better-suited alternative for bone applications with higher loading rates [88]. As compared to commercial unalloyed Ti, Ti-6Al-4V alloy has greater strength, it has been selected as a proper material for K-wires and cerclage wires. The application of this alloy has been approved by the ASTM for wire bone fixation. Therefore, various medical device manufacturers utilize Ti-6Al-4V alloy for producing K-wires in a wide range of diameters. Clauss et al. have treated 135 toe deformities using both SS K-wires and Ti K-wires for one year. They observed that the Ti K-wires represent less recurrence of deformity, pain, and biofilm formation than SS k-wires. Hence, the authors suggested utilization of Ti K-wires instead of SS ones for transfixation of toe deformities [89]. Despite the lower density of Ti alloys, their wear resistance and bending strength are lower than cobalt alloys [87].
Nitinol has proper mechanical stability, lower stiffness, and thermo-elasticity as well as acceptable corrosion resistance. These properties make it a suitable substitution for SS implants [88]. Fracture fixation by SS K-wires provides more bending stiffness in comparison with the nitinol wires, while nitinol wires are more durable. Additionally, nitinol typically costs about 4 times as much as SS with all else equal.
4.2. Biodegradable Polymeric (BP) Wires
In order to eliminate the secondary surgery and resolve the shortcomings of permanent metallic wires, the fracture fixation with biodegradable wires made of polymeric materials was suggested and applied in the clinical trials [90,91]. The wires made of biodegradable synthetic polymers were applied in the fracture fixation of the knee [91], wrist [92], elbow [84] olecranon and patella [93] and small bones of hand [90] and their usage were compared with the metallic K-wires. It was concluded that in both cases the healing time was the same and polymeric wires were suitable alternatives for the metallic ones [84,90,91,93]. Despite the high cost of polymeric biomaterials, the total expenses of treatment by polymeric wires was estimated lower than the metallic ones, since there is no need for the second surgery [93]. In the fixation of wrist fracture, treatment by BP wires was not recommended, because of high complication rate in patients [92]. In other cases, it was suggested to use polymeric wires as an adjunct to metal fixations [94,95]. It has been reported that BP materials have a common disadvantage in load-bearing applications according to their innate mechanical properties. Considering a proper mechanical strength, biodegradable metals are promising candidates in load-bearing situations, where a high mechanical strength and a suitable Young’s modulus are required.
5. Recent Developments of BM Wires in Bone Applications
Although the idea of deployment of BM wires has been presented more than a century ago, their development has been retarded until nearly a decade ago. In this section, the evolution of BM wires has been introduced with the only focus on Mg, Fe, and Zn and their alloys.
The first experimentally employed Mg wires were used as sutures to anchor nerves and muscles. During the early attempts, the lack of ductility prevented the use of Mg wires as suture [19]. Although the pure Mg as a suture wire presented an adequate degradation rate [19], rapid degradation was an obstacle to develop the usage of Mg as an implant in bone surgery. In orthopedic applications, implants usually undertake a certain load during the healing of injured bone. Due to the rapid degradation, the mechanical strength and integrity of the Mg-based implants will be deteriorated seriously. Hence, the implants lose their load-bearing ability during their service time. Pits or cracks created by the rapid corrosion might result in sudden failure, even at the initial stage after implantation [96]. Therefore, it can be concluded that as a bone fixation wire material, two main drawbacks of Mg could be low ductility and high degradation rate.
Recent studies on Mg-based BMs have focused on the improvement of mechanical properties and corrosion resistance of Mg and its alloys. In this regard, various methods such as selection on alloying elements [97,98,99,100], microstructural adjustment [101,102,103,104] and surface modification [96,105] have been applied. All the mentioned methods have been widely investigated for examining the in vivo and in vitro characteristics of common implant devices such as screws, plates, and pins [106,107,108]. In addition to the clinical trials of McBride and Verbrugge [109], at the first half of the 20th century, to employ Mg screws, plates and nails, recently, a few researchers [110,111] developed Mg-based implant devices and utilized them in patients’0 body to fix the bone fractures. Although plenty of studies has investigated the application of BP materials for manufacturing K-wires and cerclage wires, less attention has been paid to develop BMs for these wire bone fixation devices. By analyzing the plenty of publications about biodegradable Mg-based materials, it has been found that just a few pieces of research have investigated the development of the Mg alloys in the form of wires for bone fraction surgeries. As it was mentioned, the diameter of K-wires and cerclage wires vary between 0.4 and 3.5 mm. Hence, in this section, only the wires in this range of diameters were considered.
Various alloying elements were added to pure Mg to reduce the corrosion rate and concurrently keep the biocompatibility of the alloy for bone surgery. Among these alloys, Mg-calcium (Ca) alloys were biocompatible but degraded quite rapidly [97]. The combination of Mg with rare earth metals decreased the corrosion rate but also created cytotoxic effects [97,99]. Tie et al. [112] introduced a novel Mg alloy containing 2% silver (Mg2Ag) and showed that the alloy possessed appropriate mechanical properties and a rather low degradation rate in vitro. In order to assess the in vivo behavior of the alloy, Jahn et al. [113] implanted Mg2Ag intramedullary wires into mice with and without a femoral shaft fracture. The wires with the final diameter of 0.8 mm were produced via the cold rolling following the hot extrusion. To avoid the loss of ductility, heat treatment between the mentioned metal forming processes were employed. As a matter of biological effects, Mg2Ag alloy does not have any side effects on the growth rate of the bone or on inner organ morphology that represents the high biocompatibility of this alloy. They have examined the degradation rate of the alloy both in vitro and in vivo. Although the corrosion rate of Mg2Ag alloy in vivo was three times faster than in vitro, the alloy still showed sufficient rate of biodegradability which maintained proper mechanical stability while supporting fracture healing. Figure 6 illustrates the X-ray images of fractured bone fixed by steel and Mg2Ag wires during 133 days in mice [113]. Finally, they have concluded that Mg2Ag might be a promising material that has a potential application in musculoskeletal medicine.
In another attempt, Bian et al. introduced Mg-based BMs with dietary trace element germanium (Ge) for orthopedic implant application [114]. They added various mass percentages of Ge to Mg but in a limited range because of biosafety concerns. The MgGe samples with a diameter of 2.2 mm were prepared by hot rolling and machining. The highest strength and elongation were reported for Mg3Ge alloy with the yield tensile strength (YTS) of 135 MPa, UTS of 236 MPa and 17.7% elongation. It could be concluded that in comparison to other Mg-X alloy (X represents for essential/possibly essential element in human health) Mg-3Ge exhibits the highest strength and significantly improves elongation and serves the lowest in vivo corrosion rate. Figure 7 gives a comparative diagram to assess the strength and elongation of various biodegradable Mg-X alloys manufactured in different process conditions [114].
Drawing and extrusion are the most common industrial processes for the fabrication of wires based on the desired diameters. Bian et al. [114] have produced the Mg3Ge wires by machining following hot rolling process which is not a proper method for manufacturing wires. It is clear from Figure 7 that extruded parts for most of the Mg alloys have a higher ductility and strength in comparison with rolled and casted parts. Considering the last two points, one can conclude that more ductility and higher strength would be achieved by the fabrication of Mg3Ge wires via wire extrusion.
The relevance between the manufacturing process and the corrosion rate for Mg alloys have been investigated by Koo et al. [115]. They fabricated as-cast Mg-Zn-Mn and as-extruded Mg-Zn-Mn wires with a diameter of 1.6 mm. Both the alloys were examined in vivo and in vitro. It was observed that as-cast Mg-Zn-Mn alloy had higher corrosion rate with severely localized pattern in comparison with the extruded one which had the uniformly localized pattern. This observation has been attributed to the larger grains boundary and the lower mechanical strength of the as-cast alloy compared to the extruded one which had smaller grain size and higher mechanical strength [115]. This research highlighted the effect of the manufacturing process on the mechanical properties and the corrosion rate of the BM alloys. Therefore, it can be stated that by imposing higher strains during the manufacturing process of wires, finer microstructure could be achieved, which in turn improves the mechanical properties and corrosion rate of BMs. Despite the limited studies about Mg wires applied in bone fixation devices, it could be stated that Mg wires have a high potential for utilization as K-wires and guide wires in orthopedic surgeries.
In order to overcome the low corrosion rate of pure Fe, various alloying elements such as Mn, Co, Al, W, Sn, B, C, S and Si have been introduced to accelerate its degradation rate [116,117,118]. After adding Mn and Si into pure Fe (Fe30Mn6Si), its corrosion rate was increased [118], while adding Co, Al, W, Sn, B, C and S have no appreciable influences on the degradation rate of pure Fe [116]. All the mentioned elements can increase the strength of the base metal except Sn which decreases the mechanical properties [116]. Fe-based alloys also have high strength and high ductility, making them suitable candidates for utilization as wire fixation devices. Additionally, the superior mechanical properties of these alloys are favored for making fine wires even in sub-micron sizes which could be beneficial for the plenty of clinical operations. However, the high Young’s modulus of these alloys offers an inadequate match to those of natural bone and potentially causes stress shielding.
Hermawan et al. [119] reported the corrosion rate of Fe-Mn alloy which was finally one order of magnitude lower than that of Mg and its alloys. To achieve high degradation rates, Fe-Mn-Pd alloys were produced and showed higher corrosion rate compared to pure Fe and Fe-Mn alloys [51]. It is worth mentioning that these researchers obtained the corrosion rate of those alloys in vitro, which in fact are different from in vivo results. Kraus et al. [48] examined Fe-Mn-Pd alloy wires in vivo to perform a feasibility study of these alloys in osteosynthesis applications. They produced the wires with a diameter of 1.6 mm by casting and machining processes. The degradation rate of Fe-Mn-Pd wires was not significantly higher than that of Fe and Fe-Mn alloys (see Figure 8).
Attempting to find a proper Fe-based alloy with suitable degradation rate, some researchers achieved novel Fe alloys such as Fe-Pd [120], Fe-Mn-C-S [121] and Fe-Ga [122] which showed higher corrosion rate compared to pure Fe in vitro. Capek et al. [120] stated that the preparation route significantly influenced material properties such as mechanical strength and corrosion rate. In spite of numerous studies for improving the degradation rate of Fe-based alloys have been reported, only one research in the literature [48] has applied Fe-based wires in vivo experiments in the rats’ long bone.
As discussed in Section 2.3, Zn and its alloys have moderate corrosion rate and biologically beneficial corrosion products thus have been considered as one of the first priorities in the material selection for the regeneration of bone defects. However, there is no in vivo studies in the literature about the utilization of Zn-based wires in the orthopedic or dental applications. Actually, the contribution of Zn-based wires in vivo experiments has been mostly limited to the cardiovascular stent application which has different biological environment compared to bone tissues. Anyway, the alloying elements, process conditions for wire drawing, mechanical properties, and the corrosion behavior of Zn-based stents could be an initial guidance for the future use of this kind wires in the bone regeneration purposes.
5.1. Medical Sutures and Staples
In 1849, Sims successfully used a fine structure of drawn silver wires by a jeweler to close a large vesicovaginal fistula [123]. In 1947 Babcock et al. [123] published their experimental results for utilization of tantalum (Ta) and SS wires as sutures. They found that both the materials were suitable candidates for suturing but the 18-8 SS which had a reasonable price could be more applicable [123]. For many years and until now, SS sutures have gained a lot of attentions. Permanent metals adopted for utilization as sutures were mentioned in Table 2. Since the beginning of the 2nd world war, BP materials were introduced. The BP materials could be classified in two groups, synthetic polymers (nylon, polyester and propylene) and natural polymers (catgut and collagen) [124]. Materials that were introduced for suture applications should have high mechanical strength and integrity and should be biocompatible. It has been reported that polymers cannot withstand high loads securely and exhibit a low creep and stress relaxation resistance which limits their range of application [13]. Metallic sutures possess, in general, the higher strength and more advantageous creep and relaxation behavior than polymers, and they also show, in most of cases, good biocompatibility. Therefore, metallic sutures are preferred to polymeric ones especially when a biodegradable metallic suture is applied. Mg, Fe and Zn as biodegradable metals could attract more attention for suture applications.
The first usage of Mg as a suture material dates to the beginning of the 20th century. There were some attempts to use Mg wires for osteosynthesis and in vascular surgeries. The low ductility of pure Mg due to its close-packed hexagonal structure has prevented their usage as suture materials. In 1924, Seeling produced high purity Mg in a distillation process to overcome the low ductility of the material [13]. The high purity Mg did not exhibit adequate mechanical properties to allow a defect-free kinking and knotting of the wires. Seeling also tried to increase the ductility of Mg by adding some alloying elements [13]. The corrosion rate of Mg as suturing material was reported to be adequate. Hence, Seeling focused on the improvement of its mechanical properties. As it was mentioned earlier, Mg and its alloys have high corrosion rate which is inappropriate for most of the applications. Therefore, decreasing the degradation rate of Mg by some methods such as adding alloying elements were carried out. Researches in this field were retarded until the beginning of 21th century.
Seitz et al. [125,126] were the first researchers produced Mg wires for suture applications. They selected four Mg alloys, ZEK100, MgCa0.8, AL36 and AX30, which were previously reported to be biocompatible. Mg suture wires of 0.3 to 0.5 mm in diameter were fabricated by hot extrusion [125] and their diameter was further decreased via multiple drawing [126]. Despite low mechanical properties of the extruded wires, they could meet the parameters required for a surgical suture. As an extruded suture, the AL36 wire had the greatest ductility which allowed for tightening knots (Figure 9). With the aid of multiple wires drawing process, the Mg wires were reduced to monofilament wire possessing diameters between 0.5 and 0.1 mm and they also twisted into polyfilament sutures using stranding. Compared to monofilament strands, polyfilament alloy materials possessed significantly lower tensile strengths but higher fracture strains [126]. More ductility along with the adequate strength of polyfilament alloy materials made them suitable candidates for suture applications.
The previously mentioned studies have investigated pure Mg in combination with aluminum (Al) as the alloying element. It has been shown that it could be detrimental to the body. In high doses, Al has been shown to cause neurotoxicity [26]. Considering the neurotoxicity of element Al, Mg-Al-based alloys are not recommended candidates for biodegradable implant material [27]. However, recently, Al-free Mg alloys with better biological performance such as Mg-RE (rare earth element) alloys have been developed and investigated in vivo and in vitro [98,99,127]. Bai et al. [127] employed hot extrusion and cold drawing with intermediate annealing process to prepare fine wires with final diameters less than 0.4 mm of three kinds of ternary Mg-4%RE (Gd/Y/Nd)-0.4%Zn alloys. High yield strength along with moderate and adequate ductility was reported for all the fine wires. The in vitro degradation performance of the finished fine wires was evaluated, and the results indicated that Mg-4Gd-0.4Zn and Mg-4Nd-0.4Zn wires showed a similar good corrosion resistance and a uniform corrosion behavior in simulated body fluid (SBF) solution. In contrast, Mg-4Y-0.4Zn fine wires exhibited a relatively high degradation rate and pitting corrosion behavior [127]. All the studies dedicated to wires with the diameter of less than 1 mm have been reviewed in this section. Generally, one can conclude that Mg-based fine wires might be good candidates for suture applications with adequate mechanical properties and adequate degradation rate. Another application of fine wires is as staples. Staples made of pure Mg [128,129] and its alloys [130] were recently investigated for gastric anastomosis. Although the examined staples have exhibited enough closure strength, homogeneous corrosion behavior, and desirable biodegradation rate both in vivo and in vitro [128,129,130], their usage as a bone staple were not evaluated in any researches yet.
In the 18th century, Icart successfully employed Fe wires for the first time to support the healing of fractured human bone [13]. At that time, Fe was not considered to be a degradable implant material and was selected only due to its sufficient mechanical properties. It was just at the beginning of the 21st century that Fe attracted researchers’ attention as a biodegradable and more importantly nutrient implant material in bone surgeries. However, the use of pure Fe and Fe-based alloys as a nutrient suture material were not reported in the literature. Table 3 summarizes all the applications of biodegradable metallic wires.
5.2. Bone Tissue Engineering
Bone grafting is known as an operation aiming to replace diseased or injured bones with grafting materials. The bone graft could be taken from the patient (autograft) or donors (allograft) or utilized synthetic materials [131]. Even though both of autograft and allograft have some significant advantages, owing to some clinical problems such as the necessity of performing additional surgery on the donor site as well as size and geometry limitations of autograft and inconsistency with host tissue, and the possibility of disease transmission from donated allograft, a growing demand for synthetic materials as bone substitutes is received from clinicians [132]. Rely on the diamond concept for the bone healing process, synthetic bone materials could play an important role as a scaffold because it can keep mechanical stability. In addition, a combination of these materials with osteogenic cells and growth factors could accelerate the new bone formation [132,133].
Among the wide range of synthetic materials, calcium phosphate cement (CPC) is known to be the most resemble synthetic material to natural bone thus is clinically suitable for the repair of bone defects in a variety of orthopedic and dental applications [134,135]. Although CPCs are biodegradable, biocompatible, osteoconductive and have proper compression strength, because of their low bending and tensile strength and low fracture toughness their applications are limited to non-load bearing areas such as small cranial and maxillo-facial surgeries [136,137]. Generally, the mechanical strength of CPC is similar to that of trabecular bone, or one-fifth of that of cortical bone [138]. Reinforcement of CPC with fibers is one of the most promising approaches for its application in thin and large bone defects as well as stress-bearing locations [135]. The fiber reinforced calcium phosphate cement (FRCPC) concept was firstly introduced by Gonten et al. in 2000 [139]. They utilized a fiber-mesh made from poly (galectin) to reinforce CPC. Their results showed that the knitted fiber-mesh could enhance the flexural and toughness of CPCs. Then, in 2002, Xu et al. [140] incorporated two types of resorbable fibers into CPC with a fiber volume fraction of 25%. Their FRCPC increased the flexural strength threefold, and work-of-fracture toughness nearly 100 times than those of unreinforced CPC. They also claimed that resorption of the fiber during the regeneration process could facilitate vacuolization and consequently rapid bone-ingrowth. In a same period of time, Dos Santos et al. [138] followed up this field using non-degradable fibers including carbon, nylon which were not suitable for clinical applications. They just tried to enhance the mechanical properties which CPC is weak at.
In the next generation of FRCPC, biocompatible and biodegradable polymeric fibers such as poly (lactic-co-glycolic) acid (PLGA) [141] and biopolymers such as chitosan and gelatin [142] were used. Owing to the lower Young’s modulus and strength of these fibers than those of the cement matrix, they are not successful enough as a reinforcement element for the strengthening of CPC. The bending strength of 40–45 MPa is the best mechanical properties have been reported for FRCPC achieved by PLGA fibers up to now. Furthermore, in physiological environment, fast degradation rate of PLGA fibers results in the concern of mechanical stability only after 3–4 weeks [143]. In 2013, the new generation of FRCPC was introduced by Kruger et al. [144]. They utilized AZ31 and ZEK100 Mg wires with 0.6 and 0.228 mm in diameter respectively. It was for the first time that BM wires were used as a reinforcement element for the strengthening of CPC which was successful to improve the bending strength of FRCPC up to 139 ± 41 MPa. They stated that regarding the fracture of the FRCPC initiated by shearing of the matrix at or near the biodegradable metallic wire surface, hybrid reinforcement of CPC with both metal and fine polymer fibers such as polylactic acid (PLA) could postpone the crack initiation and further enhance the mechanical properties of FRCPC (Figure 10). Additionally, in vitro tests with osteoblasts validated cytocompatibility of wire-reinforced CPC composites with BM.
However, there is only one pilot study for the use of FRCPC composites. Further investigations need to be done to optimize the mechanical properties of the BM wire reinforced CPC composites by applying a vast range of diameters, plenty types of biodegradable alloys and different fiber dispositions. Moreover, assessment of the mechanical stability should be conducted in much longer time in vitro (several months or even a year), and finally in vivo animal tests should be performed to examine all of the positive and negative biological effects and structural changing during the degradation of these kind of composites before any clinical applications for the grafting of human bone defects in the load-bearing locations.
6. Future Work
Generally, for BM wires and especially for Mg and its alloys, controlling the degradation rate for implant applications is quite important. It becomes more critical for the application of fine BM wires in stress-bearing areas, because the mechanical properties of such wires can be significantly influenced by high corrosion rate. Therefore, the first priority in the application of BM wires is controlling the corrosion rate to a logical rate, at least in the initial stage after implantation. In this regard, methods such as selection of alloying elements, microstructure adjustments and surface modification will be effective. It is worth mentioning that these corrosion controlling methods have some intrinsic differences. Various surface modification techniques create a protective layer on the material which resist against corrosion. In some cases, this layer also increases the osteoinductivity and osteoconductivity of the material while in other cases only controls the corrosion rate on the surface. In general, surface modification methods affect the surface corrosion. Selecting proper alloying elements in combination with the base metal could adjust the volume degradation rate of the material and concurrently could enhance mechanical properties of an alloy. The third corrosion controlling method, by employing a proper fabrication process, creates a fine and uniform microstructure which in turn influences the mechanical properties of the material. Hence, it is obvious that selecting alloying elements and refining microstructure methods will have another beneficial effect on mechanical characteristics of the materials. These two mentioned techniques, except in some special cases, are preferred to surface modification methods.
6.1. Alloying Elements
6.1.1. Magnesium
Common alloying elements used for pure Mg are mentioned in Table 4. Biological and mechanical advantages and disadvantages of the elements are summarized in this table. Since Al and Cu may cause neurotoxicity in the body, their usage in recent studies has been limited. It is obvious from the table that Cu also accelerates the corrosion rate of Mg [26] and hence, it is not suitable for implants. Adding Ca, Si and Li elements could deteriorate the degradation rate of Mg [97]. Therefore, these elements cannot play their role as a corrosion controlling element. It can be seen that other alloying elements, such as Zn, Zr, Mn and RE improve the corrosion resistance of Mg and simultaneously increase the strength and ductility of the obtained alloy. Additionally, for the mentioned elements in standard dosage, harmful side effects were not reported [97]. In recent literature it can be found that newly introduced biocompatible Mg alloys mostly contain these elements [145,146,147,148]. Therefore, in designing and developing of new Mg biomaterials the potentials of these alloying elements should be considered.
6.1.2. Iron
Alloying elements such as Mn, Co, Al, W, Sn, B, C, S and Si were added into Fe-based alloys to accelerate their degradation rate. It has been found that adding Co, Al, W, Sn, B, C and S have no influence on the degradation behavior of pure Fe [116], while the alloy Fe30Mn6Si had a relatively more corrosion rate compared to pure Fe [118]. There are two main criteria regarding increase in the corrosion rate of Fe-based alloys which affect the corrosion susceptibility of this kind of alloys: (1) the addition of less noble alloying elements within the solubility limit in Fe to cause the matrix more susceptible to corrosion; and (2) the addition of noble alloying elements to generate small and finely dispersed intermetallic phases (IMPs). Mn and Pd have been shown to be suitable alloying elements according to both of the mentioned approaches [51]. Fe-Mn-Pd alloy has investigated and suggested as a Fe-based alloy which could improve the degradation rate of the base metal [48]. Inspecting the effect of alloying elements on the corrosion behavior of Fe-based alloys is still a challenging and ongoing research area.
6.1.3. Zinc
Zinc as a newly introduced biodegradable metal with a moderate degradation rate has attracted some attention. Alloying elements of Zn have the role of strengthening the matrix since Zn-based alloys suffer from low mechanical properties. To improve the mechanical properties of pure Zn, some elements such as Mg, Ca, Sr, Sn and Fe were added into Zn-based alloys [56,70,117,149]. Vojtech et al. [70] developed as cast Zn-Mg alloys and studied their mechanical properties and corrosion behavior. Their results showed a significantly improvement in the tensile strength of Zn modifying by 1% Mg. The elongation of Zn-1% Mg alloy was much greater than that of pure Zn but was only 2%, which is quite low for medical usage [70]. Combination of Mg as an alloying element with Zn-based alloys especially about 1% is newly introduced and investigated by several researchers [54,55]. Shen et al. [150] produced Zn-1.2% Mg alloy and achieved the high ultimate strength of 362 MPa and elongation of 21%, which is the highest ductility obtained for biodegradable Zn alloys. The combination of Zn with other alloying elements is still a challenging topic for researchers.
6.2. Surface Modification
6.2.1. Magnesium
Numerous studies have proved that the functional and mechanical behaviors as well as chemical and physical properties of biomaterials can be affected by different surface modification techniques [151]. Although plenty of coating methods such as electrodeposition [152], sol-gel and dipping [153], chemical conversion [154], anodization [155], vapor deposition [156], spin [157], and alkali treatment [158] have been proposed to inhibit rapid corrosion of Mg and its alloys, just few of them are effective and flexible enough for the formation of a uniform coating with desired thickness on the non-flat surfaces such as wires. Simultaneously, the adhesion between the substrate and the coating film is another concern that should be considered. Finally, prevention from deteriorating the mechanical properties of the substrate as much as possible is the third consideration in the selection of an adequate coating method. To summarize, it is claimed that only sol-gel preparation combined with dip coating and alkali treatment can meet all of the three mentioned requirements which make them suitable and cost-effective methods for the coating of Mg-based wires [151,159].
The composition of the coating is another critically important parameter. An ideal coating material for bone applications should be able to enhance the biocompatibility and osteointegration properties of Mg-based alloys and simultaneously increase the corrosion resistance. As discussed in Section 2.1.1, coating with Mg(OH)2 [159,160] could enhance bone formation and passivate the Mg-based wires to decrease the corrosion rate as well. The synthetic calcium phosphate coatings [151,161,162] can definitely facilitate the new bone formation. The biomimetic coating with pure collagen [163] and collagen-based composites [164] is another promising approach that can be applied in the future studies of Mg-based wires in bone tissue regeneration.
6.2.2. Iron
Despite numerous investigations focused on the surface treatment methods for Mg-based alloys, only few research can be found for surface treatment of pure Fe. Chen et al. [165] suggested using micro-patterned Au disc arrays to accelerate degradation of pure Fe. The proposed approach relied on the galvanic corrosion caused by the Au array [165]. In another research, Fe-O thin films were prepared on pure Fe by plasma immersion ion implantation and deposition in order to improve the biodegradability and biocompatibility [166]. The prepared thin films decreased the degradation rate and enhanced the corrosion behavior [166]. Sandblasting method has been proposed by Zhou et al. [167] as a successful surface treatment for increasing the degradation rate of pure Fe in SBF. The reasons for increasing the corrosion rate were the change of surface composition (in the early stage), high roughness and high density of dislocations [167]. The limited number of researches in the surface treatment methods for Fe-based BM wires indicates that more studies is required to introduce and reveal the potentials of various surface treatments approaches.
6.3. Fabrication Processes
As stated before, microstructure adjustment is one of the corrosion control methods. In this regard, selection of a proper fabrication process could effectively influence the microstructure. In case of Mg-Zn-Mn alloy, it has been reported that the extruded alloy compared to casted material had fine grain size and accordingly slower degradation rate. Therefore, selection of the manufacturing process of the alloy needs more attention. There are several common manufacturing processes such as rolling, extrusion, forging, drawing, and continuous casting. Recently severe plastic deformation (SPD) processes such as equal channel angular extrusion (ECAP), multi-axial forging (MAF) and high-pressure torsion (HPT) were introduced. These SPD methods by imposing large shear strains or huge compressive strains decrease the grain size of the materials. Dobatkin et al. [168] employed three different SPD processes (ECAP, MAF, and rotary swaging (RS)) to investigate the effects on the microstructure and corrosion behavior of WE43 Mg alloy. They observed that all the processes could decrease the grain size and create ultra-fine grained (UFG) microstructure. The biodegradation rate of the UFG WE43 was examined in vitro and it was concluded that ECAP and MAF caused some deceleration of biodegradation rate by slowing down the gas formation in the biological fluid and improved the biocompatibility of the WE43 alloy [168]. This research shows the potential of SPD method in controlling the corrosion of Mg alloys which can be spread to other biodegradable metals as well.
7. Conclusions
Application of biodegradable metals (magnesium, iron, and zinc) as promising biodegradable materials is spreading in various biomedical devices especially for dental and orthopedic applications. Wire is one of the most popular forms of these materials that can be easily formed by drawing and other methods. Although currently biodegradable metallic wires have some drawbacks such as unsatisfactory degradation rate and mechanical properties when used in bone surgeries, many methods can be adopted to control their corrosion behavior and tailor their mechanical properties. Owing to the proper mechanical properties, controllable degradation rate, and the release of nutrient ions, which will significantly be beneficial to bone cells and bone tissue regeneration, we firmly believe that in the near future BM wires will be used broadly in dental and orthopedic fields.
Author Contributions
Mohammad Asgari, Zhiyong Li and Yin Xiao conceptualized the paper and gave instructions; Mohammad Asgari wrote the paper; Ruiqiang Hang, Zhiyong Li and Yin Xiao edited the paper; Mohammad Asgari, Zhiyong Li and Yin Xiao revised the paper; Chang Wang and Zhentao Yu gave idea and advice; Zhiyong Li and Yin Xiao gave directions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Griebel, A.J.; Schaffer, J.E. Absorbable filament technologies: Wire-drawing to enable next-generation medical devices. In Magnesium Technology 2016; Springer: Berlin, Germany, 2016; pp. 323–327. [Google Scholar]
- Sardeshmukh, A.; Reddy, S.; Gautham, B.; Joshi, A.; Panchal, J. A data science approach for analysis of multi-pass wire drawing. In Proceedings of the ASME 2017 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Cleveland, OH, USA, 6–9 August 2017; American Society of Mechanical Engineers: New York, NY, USA, 2017; p. V001T002A071. [Google Scholar] [CrossRef]
- Griebel, A.J.; Schaffer, J.E.; Hopkins, T.M.; Alghalayini, A.; Mkorombindo, T.; Ojo, K.O.; Xu, Z.; Little, K.J.; Pixley, S.K. An in vitro and in vivo characterization of fine WE43B magnesium wire with varied thermomechanical processing conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017. [Google Scholar] [CrossRef] [PubMed]
- Duerig, T.; Pelton, A.; Stöckel, D. An overview of nitinol medical applications. Mater. Sci. Eng. A 1999, 273, 149–160. [Google Scholar] [CrossRef]
- Welch, J.M.; Sutton, G. Coronary Guide Catheter. Google Patents WO2017020012 A1, 29 July 2016. [Google Scholar]
- Henkes, H.; Bose, A.; Felber, S.; Miloslavski, E.; Berg-Dammer, E.; Kühne, D. Endovascular coil occlusion of intracranial aneurysms assisted by a novel self-expandable nitinol microstent (neuroform). Int. Neuroradiol. 2002, 8, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Sun, D.-H.; Yu, T.; Wang, L.; Zhu, D.; Li, Y.-H. Death due to intra-aortic migration of kirschner wire from the clavicle: A case report and review of the literature. Medicine 2016, 95, e3741. [Google Scholar] [CrossRef] [PubMed]
- Bravo, L.A.; de Cabañes, A.G.; Manero, J.M.; Rúperez, E.; Gil, F.J. NiTi superelastic orthodontic archwires with polyamide coating. J. Mater. Sci. Mater. Med. 2014, 25, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, B. Configured ligature wire for quick conventional and overtie lingual archwire ligations. APOS Trends Orthod. 2017, 7, 108–110. [Google Scholar] [CrossRef]
- Iavazzo, C.; Gkegkes, I.D.; Vouloumanou, E.K.; Mamais, I.; Peppas, G.; Falagas, M.E. Sutures versus staples for the management of surgical wounds: A meta-analysis of randomized controlled trials. Am. Surg. 2011, 77, 1206–1221. [Google Scholar] [PubMed]
- Bowen, P.K.; Shearier, E.R.; Zhao, S.; Guillory, R.J.; Zhao, F.; Goldman, J.; Drelich, J.W. Biodegradable metals for cardiovascular stents: From clinical concerns to recent Zn-alloys. Adv. Healthc. Mater. 2016, 5, 1121–1140. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zheng, Y.; Qin, L. Progress of biodegradable metals. Prog. Natl. Sci. Mater. Int. 2014, 24, 414–422. [Google Scholar] [CrossRef]
- Seitz, J.-M.; Durisin, M.; Goldman, J.; Drelich, J.W. Recent advances in biodegradable metals for medical sutures: A critical review. Adv. Healthc. Mater. 2015, 4, 1915–1936. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yang, H.T.; Li, X.; Zheng, Y.F. In vitro evaluation of the feasibility of commercial Zn alloys as biodegradable metals. J. Mater. Sci. Technol. 2016, 32, 909–918. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, W.; Maitz, M.F.; Chen, M.; Zhang, H.; Mao, J.; Zhao, Y.; Huang, N.; Wan, G. Comparative corrosion behavior of Zn with Fe and Mg in the course of immersion degradation in phosphate buffered saline. Corros. Sci. 2016, 111, 541–555. [Google Scholar] [CrossRef]
- Li, H.; Yang, H.; Zheng, Y.; Zhou, F.; Qiu, K.; Wang, X. Design and characterizations of novel biodegradable ternary Zn-based alloys with IIA nutrient alloying elements Mg, Ca and Sr. Mater. Des. 2015, 83, 95–102. [Google Scholar] [CrossRef]
- Witte, F. Reprint of: The history of biodegradable magnesium implants: A review. Acta Biomater. 2015, 23, S28–S40. [Google Scholar] [CrossRef] [PubMed]
- Andrews, E.W. Absorbable metal clips as substitutes for ligatures and deep sutures in wound closure. J. Am. Med. Assoc. 1917, 69, 278–281. [Google Scholar] [CrossRef]
- Seelig, M. A study of magnesium wire as an absorbable suture and ligature material. Arch. Surg. 1924, 8, 669–680. [Google Scholar] [CrossRef]
- Hou, L.-D.; Li, Z.; Pan, Y.; Sabir, M.; Zheng, Y.-F.; Li, L. A review on biodegradable materials for cardiovascular stent application. Front. Mater. Sci. 2016, 10, 238–259. [Google Scholar] [CrossRef]
- Li, X.; Chu, C.; Zhou, L.; Bai, J.; Guo, C.; Xue, F.; Lin, P.; Chu, P.K. Fully degradable PLA-based composite reinforced with 2D-braided Mg wires for orthopedic implants. Compos. Sci. Technol. 2017, 142, 180–188. [Google Scholar] [CrossRef]
- Staiger, M.P.; Pietak, A.M.; Huadmai, J.; Dias, G. Magnesium and its alloys as orthopedic biomaterials: A review. Biomaterials 2006, 27, 1728–1734. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Zhu, D. Application of Mg-based alloys for cardiovascular stents. Int. J. Biomed. Eng. Technol. 2013, 12, 382–398. [Google Scholar] [CrossRef]
- Liu, A.; Sun, M.; Shao, H.; Yang, X.; Ma, C.; He, D.; Gao, Q.; Liu, Y.; Yan, S.; Xu, S. The outstanding mechanical response and bone regeneration capacity of robocast dilute magnesium-doped wollastonite scaffolds in critical size bone defects. J. Mater. Chem. B 2016, 4, 3945–3958. [Google Scholar] [CrossRef]
- Wu, L.; Feyerabend, F.; Schilling, A.F.; Willumeit-Römer, R.; Luthringer, B.J. Effects of extracellular magnesium extract on the proliferation and differentiation of human osteoblasts and osteoclasts in coculture. Acta Biomater. 2015, 27, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Persaud-Sharma, D.; McGoron, A. Biodegradable magnesium alloys: A review of material development and applications. J. Biomim. Biomater. Tissue Eng. 2012, 12, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.F.; Gu, X.N.; Witte, F. Biodegradable metals. Mater. Sci. Eng. R Rep. 2014, 77, 1–34. [Google Scholar] [CrossRef]
- Pilarska, A.A.; Klapiszewski, Ł.; Jesionowski, T. Recent development in the synthesis, modification and application of Mg(OH)2 and MgO: A review. Powder Technol. 2017, 319, 373–407. [Google Scholar] [CrossRef]
- Guo, M.; Muhammad, F.; Wang, A.; Qi, W.; Wang, N.; Guo, Y.; Wei, Y.; Zhu, G. Magnesium hydroxide nanoplates: A pH-responsive platform for hydrophobic anticancer drug delivery. J. Mater. Chem. B 2013, 1, 5273–5278. [Google Scholar] [CrossRef]
- Janning, C.; Willbold, E.; Vogt, C.; Nellesen, J.; Meyer-Lindenberg, A.; Windhagen, H.; Thorey, F.; Witte, F. Magnesium hydroxide temporarily enhancing osteoblast activity and decreasing the osteoclast number in peri-implant bone remodelling. Acta Biomater. 2010, 6, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Weizbauer, A.; Kieke, M.; Rahim, M.I.; Angrisani, G.L.; Willbold, E.; Diekmann, J.; Flörkemeier, T.; Windhagen, H.; Müller, P.P.; Behrens, P.; et al. Magnesium-containing layered double hydroxides as orthopaedic implant coating materials—An in vitro and in vivo study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Hickey, D.J.; Ercan, B.; Chung, S.; Webster, T.J.; Sun, L.; Geilich, B. Mgo nanocomposites as new antibacterial materials for orthopedic tissue engineering applications. In Proceedings of the 2014 40th Annual Northeast Bioengineering Conference (NEBEC), Boston, MA, USA, 25–27 April 2014; pp. 1–2. [Google Scholar]
- Huang, L.; Li, D.-Q.; Lin, Y.-J.; Wei, M.; Evans, D.G.; Duan, X. Controllable preparation of Nano-MgO and investigation of its bactericidal properties. J. Inorg. Biochem. 2005, 99, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Haghshenas, M. Mechanical characteristics of biodegradable magnesium matrix composites: A review. J. Magn. Alloys 2017, 5, 189–201. [Google Scholar] [CrossRef]
- Gu, X.-N.; Zheng, Y.-F. A review on magnesium alloys as biodegradable materials. Front. Mater. Sci. China 2010, 4, 111–115. [Google Scholar] [CrossRef]
- Yusop, A.; Bakir, A.; Shaharom, N.; Abdul Kadir, M.; Hermawan, H. Porous biodegradable metals for hard tissue scaffolds: A review. Int. J. Biomater. 2012, 2012, 641430. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Witte, F.; Lu, F.; Wang, J.; Li, J.; Qin, L. Current status on clinical applications of magnesium-based orthopaedic implants: A review from clinical translational perspective. Biomaterials 2017, 112, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Haynes, W.M. CRC Handbook of Chemistry and Physics; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Feyerabend, F.; Wendel, H.-P.; Mihailova, B.; Heidrich, S.; Agha, N.A.; Bismayer, U.; Willumeit-Römer, R. Blood compatibility of magnesium and its alloys. Acta Biomater. 2015, 25, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Harandi, S.E.; Banerjee, P.C.; Easton, C.D.; Singh Raman, R.K. Influence of bovine serum albumin in hanks’ solution on the corrosion and stress corrosion cracking of a magnesium alloy. Mater. Sci. Eng. C 2017, 80, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Noviana, D.; Paramitha, D.; Ulum, M.F.; Hermawan, H. The effect of hydrogen gas evolution of magnesium implant on the postimplantation mortality of rats. J. Orthop. Transl. 2016, 5, 9–15. [Google Scholar] [CrossRef]
- Tang, J.; Wang, J.; Xie, X.; Zhang, P.; Lai, Y.; Li, Y.; Qin, L. Surface coating reduces degradation rate of magnesium alloy developed for orthopaedic applications. J. Orthop. Transl. 2013, 1, 41–48. [Google Scholar] [CrossRef]
- Kraus, T.; Fischerauer, S.F.; Hänzi, A.C.; Uggowitzer, P.J.; Löffler, J.F.; Weinberg, A.M. Magnesium alloys for temporary implants in osteosynthesis: In vivo studies of their degradation and interaction with bone. Acta Biomater. 2012, 8, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Xu, X.; Xu, Z.; Wang, J.; Cai, H. Development of Fe-based degradable metallic biomaterials. Metallic Biomater. New Direct. Technol. 2017, 113–160. [Google Scholar]
- Zimmermann, M.B.; Hurrell, R.F. Nutritional iron deficiency. Lancet 2007, 370, 511–520. [Google Scholar] [CrossRef]
- Toxqui, L.; Vaquero, M.P. Chronic iron deficiency as an emerging risk factor for osteoporosis: A hypothesis. Nutrients 2015, 7, 2324–2344. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.; Yang, Y.; Virtanen, S.; Boccaccini, A.R. Iron and Iron-based alloys for temporary cardiovascular applications. J. Mater. Sci. Mater. Med. 2015, 26, 138. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.; Moszner, F.; Fischerauer, S.; Fiedler, M.; Martinelli, E.; Eichler, J.; Witte, F.; Willbold, E.; Schinhammer, M.; Meischel, M. Biodegradable Fe-based alloys for use in osteosynthesis: Outcome of an in vivo study after 52 weeks. Acta Biomater. 2014, 10, 3346–3353. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Zheng, Y.; Han, Y. Accelerating degradation rate of pure iron by Zinc Ion implantation. Regener. Biomater. 2016, 3, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Mouzou, E.; Paternoster, C.; Tolouei, R.; Chevallier, P.; Biffi, C.A.; Tuissi, A.; Mantovani, D. CO2-rich atmosphere strongly affects the degradation of Fe-21Mn-1C for biodegradable metallic implants. Mater. Lett. 2016, 181, 362–366. [Google Scholar] [CrossRef]
- Schinhammer, M.; Hanzi, A.C.; Loffler, J.F.; Uggowitzer, P.J. Design strategy for biodegradable Fe-based alloys for medical applications. Acta Biomater. 2010, 6, 1705–1713. [Google Scholar] [CrossRef] [PubMed]
- Keen, C.L.; Zidenberg-Cherr, S. Manganese A2—Caballero, benjamin. In Encyclopedia of Food Sciences and Nutrition, 2nd ed.; Academic Press: Oxford, UK, 2003; pp. 3686–3691. [Google Scholar]
- Dermience, M.; Lognay, G.; Mathieu, F.; Goyens, P. Effects of thirty elements on bone metabolism. J. Trace Elements Med. Biol. 2015, 32, 86–106. [Google Scholar] [CrossRef] [PubMed]
- Sikora-Jasinska, M.; Mostaed, E.; Mostaed, A.; Beanland, R.; Mantovani, D.; Vedani, M. Fabrication, mechanical properties and in vitro degradation behavior of newly developed Zn Ag alloys for degradable implant applications. Mater. Sci. Eng. C 2017, 77, 1170–1181. [Google Scholar] [CrossRef] [PubMed]
- Katarivas Levy, G.; Goldman, J.; Aghion, E. The prospects of zinc as a structural material for biodegradable implants—A review paper. Metals 2017, 7, 402. [Google Scholar] [CrossRef]
- Li, H.F.; Xie, X.H.; Zheng, Y.F.; Cong, Y.; Zhou, F.Y.; Qiu, K.J.; Wang, X.; Chen, S.H.; Huang, L.; Tian, L.; et al. Development of biodegradable Zn-1X binary alloys with nutrient alloying elements Mg, Ca and Sr. Sci. Rep. 2015, 5, 10719. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Wang, C.; Liu, C.; Chen, H.; Wu, Y.; Han, J.; Jia, Z.; Lin, W.; Zhang, D.; Li, W.; et al. Evolution of the degradation mechanism of pure Zinc stent in the one-year study of rabbit abdominal aorta model. Biomaterials 2017, 145, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Sun, J.; Yang, Y.; Zhou, F.; Pu, Z.; Li, L.; Zheng, Y. Microstructure, mechanical properties, in vitro degradation behavior and hemocompatibility of novel Zn–Mg–Sr alloys as biodegradable metals. Mater. Lett. 2016, 162, 242–245. [Google Scholar] [CrossRef]
- Zhu, H.; Jin, G.; Cao, H.; Qiao, Y.; Liu, X. Influence of implantation voltage on the biological properties of Zinc-implanted titanium. Surf. Coat. Technol. 2017, 312, 75–80. [Google Scholar] [CrossRef]
- Seo, H.-J.; Cho, Y.-E.; Kim, T.; Shin, H.-I.; Kwun, I.-S. Zinc may increase bone formation through stimulating cell proliferation, alkaline phosphatase activity and collagen synthesis in osteoblastic MC3T3-E1 cells. Nutr. Res. Pract. 2010, 4, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Moonga, B.S.; Dempster, D.W. Zinc is a potent inhibitor of osteoclastic bone resorption in vitro. J. Bone Min. Res. 1995, 10, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, P.; Rai, D.V.; Garg, M.L. Zinc inhibits ovariectomy induced microarchitectural changes in the bone tissue. J. Nutr. Intermed. Metab. 2016, 3, 33–40. [Google Scholar] [CrossRef]
- Yamaguchi, M. Role of nutritional zinc in the prevention of osteoporosis. Mol. Cell. Biochem. 2010, 338, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Pasquet, J.; Chevalier, Y.; Pelletier, J.; Couval, E.; Bouvier, D.; Bolzinger, M.-A. The contribution of zinc ions to the antimicrobial activity of zinc oxide. Colloids Surf. A Physicochem. Eng. Asp. 2014, 457, 263–274. [Google Scholar] [CrossRef]
- Boyd, D.; Li, H.; Tanner, D.A.; Towler, M.R.; Wall, J.G. The antibacterial effects of zinc ion migration from Zinc-based glass polyalkenoate cements. J. Mater. Sci. Mater. Med. 2006, 17, 489–494. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, T.J.; Zeelie, J.J.; Krause, D.J. The antimicrobial action of Zinc ion/antioxidant combinations. J. Clin. Pharm. Ther. 1992, 17, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Drelich, A.J.; Bowen, P.K.; LaLonde, L.; Goldman, J.; Drelich, J.W. Importance of oxide film in endovascular biodegradable Zinc stents. Surf. Innov. 2016, 4, 133–140. [Google Scholar] [CrossRef]
- Moon, S.-H.; Choi, W.J.; Choi, S.-W.; Kim, E.H.; Kim, J.; Lee, J.-O.; Kim, S.H. Anti-cancer activity of ZnO chips by sustained Zinc Ion release. Toxicol. Rep. 2016, 3, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-W.; Choi, W.J.; Kim, E.H.; Moon, S.-H.; Park, S.-J.; Lee, J.-O.; Kim, S.H. Inflammatory bone resorption and antiosteosarcoma potentials of Zinc Ion sustained release ZnO chips: Friend or foe? ACS Biomater. Sci. Eng. 2016, 2, 494–500. [Google Scholar] [CrossRef]
- Vojtech, D.; Kubasek, J.; Serak, J.; Novak, P. Mechanical and corrosion properties of newly developed biodegradable Zn-based alloys for bone fixation. Acta Biomater. 2011, 7, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Törne, K.; Larsson, M.; Norlin, A.; Weissenrieder, J. Degradation of Zinc in saline solutions, plasma, and whole blood. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Katz, E.P.; Li, S.-T. Structure and function of bone collagen fibrils. J. Mol. Biol. 1973, 80, 1–15. [Google Scholar] [CrossRef]
- Tan, L.; Yu, X.; Wan, P.; Yang, K. Biodegradable materials for bone repairs: A review. J. Mater. Sci. Technol. 2013, 29, 503–513. [Google Scholar] [CrossRef]
- Huber, W. Historical remarks on martin kirschner and the development of the kirschner (K)-wire. Indian J. Plast. Surg. 2008, 41, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Harasen, G. Orthopedic hardware and equipment for the beginner: Part 1. Pins and wires. Can. Vet. J. 2011, 52, 1025–1026. [Google Scholar] [PubMed]
- Ricbard, M.; Slone, M.M.H.; Vander Griend Robert, A.; William, J. Montgomery Orthopaedic fixation devices. RadioGraphics 1991, 11, 823–847. [Google Scholar]
- Rudolph, D.J.; Willes, M.G.; Sameshima, G.T. A finite element model of apical force distribution from orthodontic tooth movement. Angle Orthod. 2001, 71, 127–131. [Google Scholar] [PubMed]
- Henriques, J.F.C.; Higa, R.H.; Semenara, N.T.; Janson, G.; Fernandes, T.M.F.; Sathler, R. Evaluation of deflection forces of orthodontic wires with different ligation types. Braz. Oral Res. 2017, 31, e49. [Google Scholar] [CrossRef] [PubMed]
- Cowley, L.L. Wire sutures: Braided or monofilament? Am. J. Surg. 1967, 113, 472–474. [Google Scholar] [CrossRef]
- Karmani, S.; Lam, F. The design and function of surgical drills and k-wires. Curr. Orthop. 2004, 18, 484–490. [Google Scholar] [CrossRef]
- Massengill, J.B.; Alexander, H.; Parson, J.R.; Schecter, M.J. Mechanical analysis of kirschner wire fixation in a phalangeal model. J. Hand Surg. 1979, 4, 351–356. [Google Scholar] [CrossRef]
- Viegas, S.F.; Ferren, E.L.; Self, J.; Tencer, A.F. Comparative mechanical properties of various kirschner wire configurations in transverse and oblique phalangeal fractures. J. Hand Surg. 1988, 13, 246–253. [Google Scholar] [CrossRef]
- Stark, H.H.; Rickard, T.; Zemel, N.; Ashworth, C. Treatment of ununited fractures of the scaphoid by iliac bone grafts and kirschner-wire fixation. J. Bone Jt. Surg. Am. 1988, 70, 982–991. [Google Scholar] [CrossRef]
- Hope, P.G.; Williamson, D.M.; Coates, C.J.; Cole, W.G. Biodegradable pin fixation of elbow fractures in children. A randomised trial. J. Bone Jt. Surg. Br. Vol. 1991, 73, 965–968. [Google Scholar] [CrossRef]
- Leppilahti, J.; Jalovaara, P. Migration of kirschner wires following fixation of the clavicle—A report of 2 cases. Acta Orthop. Scand. 1999, 70, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Gbur, J.L.; Lewandowski, J.J. Fatigue and fracture of wires and cables for biomedical applications. Int. Mater. Rev. 2016, 61, 231–314. [Google Scholar] [CrossRef]
- Chen, Q.; Thouas, G.A. Metallic implant biomaterials. Mater. Sci. Eng. R Rep. 2015, 87, 1–57. [Google Scholar] [CrossRef]
- Prasad, K.; Bazaka, O.; Chua, M.; Rochford, M.; Fedrick, L.; Spoor, J.; Symes, R.; Tieppo, M.; Collins, C.; Cao, A.; et al. Metallic biomaterials: Current challenges and opportunities. Materials 2017, 10, 884. [Google Scholar] [CrossRef] [PubMed]
- Clauss, M.; Graf, S.; Gersbach, S.; Hintermann, B.; Ilchmann, T.; Knupp, M. Material and biofilm load of k wires in toe surgery: Titanium versus stainless steel. Clin. Orthop. Relat. Res. 2013, 471, 2312–2317. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; Jensen, C. Biodegradable pins versus kirschner wires in hand surgery. J. Hand Surg. Br. Eur. Vol. 1996, 21, 507–510. [Google Scholar] [CrossRef]
- Plaga, B.; Royster, R.; Donigian, A.; Wright, G.; Caskey, P. Fixation of osteochondral fractures in rabbit knees. A comparison of kirschner wires, fibrin sealant, and polydioxanone pins. Bone Jt. J. 1992, 74, 292–296. [Google Scholar] [CrossRef]
- Casteleyn, P.P.; Handelberg, F.; Haentjens, P. Biodegradable rods versus kirschner wire fixation of wrist fractures. A randomised trial. J. Bone Jt. Surg. Br. Vol. 1992, 74, 858–861. [Google Scholar] [CrossRef]
- Juutilainen, T.; Patiälä, H.; Rokkanen, P.; Törmälä, P. Biodegradable wire fixation in olecranon and patella fractures combined with biodegradable screws or plugs and compared with metallic fixation. Arch. Orthop. Trauma Surg. 1995, 114, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Lurate, B.; Mukherjee, D.; Kruse, R.; Albright, J. Fixation of osteochondral fractures with absorbable pins. In Proceedings of the 1995 Fourteenth Southern Biomedical Engineering Conference, Shreveport, LA, USA, 7–9 April 1995; pp. 57–58. [Google Scholar]
- Maruyama, T.; Saha, S.; Mongiano, D.O.; Mudge, K. Metacarpal fracture fixation with absorbable polyglycolide rods and stainless steel k wires: A biomechanical comparison. J. Biomed. Mater. Res. Part A 1996, 33, 9–12. [Google Scholar] [CrossRef]
- Tian, P.; Liu, X. Surface modification of biodegradable magnesium and its alloys for biomedical applications. Regen. Biomater. 2015, 2, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Witte, F.; Hort, N.; Vogt, C.; Cohen, S.; Kainer, K.U.; Willumeit, R.; Feyerabend, F. Degradable biomaterials based on magnesium corrosion. Curr. Opin. Solid State Mater. Sci. 2008, 12, 63–72. [Google Scholar] [CrossRef]
- Hanzi, A.C.; Gerber, I.; Schinhammer, M.; Loffler, J.F.; Uggowitzer, P.J. On the in vitro and in vivo degradation performance and biological response of new biodegradable Mg-Y-Zn alloys. Acta Biomater. 2010, 6, 1824–1833. [Google Scholar] [CrossRef] [PubMed]
- KubÁSek, J.; VojtĚCh, D. Structural and corrosion characterization of biodegradable Mg–Re (Re = Gd, Y, Nd) alloys. Trans. Nonferrous Met. Soc. China 2013, 23, 1215–1225. [Google Scholar] [CrossRef]
- Chen, L.; Bin, Y.; Zou, W.; Wang, X.; Li, W. The influence of Sr on the microstructure, degradation and stress corrosion cracking of the Mg alloys—ZK40xSr. J. Mech. Behav. Biomed. Mater. 2017, 66, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Gu, X.; Lou, S.; Zheng, Y. The development of binary Mg-Ca alloys for use as biodegradable materials within bone. Biomaterials 2008, 29, 1329–1344. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Zheng, Y.; Cheng, Y.; Zhong, S.; Xi, T. In vitro corrosion and biocompatibility of binary magnesium alloys. Biomaterials 2009, 30, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Lietaert, K.; Weber, L.; Van Humbeeck, J.; Mortensen, A.; Luyten, J.; Schrooten, J. Open cellular magnesium alloys for biodegradable orthopaedic implants. J. Magn. Alloys 2013, 1, 303–311. [Google Scholar] [CrossRef]
- Mutlu, I.; Oktay, E. Influence of fluoride content of artificial saliva on metal release from 17-4 PH stainless steel foam for dental implant applications. J. Mater. Sci. Technol. 2013, 29, 582–588. [Google Scholar] [CrossRef]
- Cui, W.; Beniash, E.; Gawalt, E.; Xu, Z.; Sfeir, C. Biomimetic coating of magnesium alloy for enhanced corrosion resistance and calcium phosphate deposition. Acta Biomater. 2013, 9, 8650–8659. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, N.; Angrisani, N.; Reifenrath, J.; Lucas, A.; Thorey, F.; Bormann, D.; Meyer-Lindenberg, A. Biomechanical testing and degradation analysis of MgCa0.8 alloy screws: A comparative in vivo study in rabbits. Acta Biomater. 2011, 7, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Schilling, M.; Eifler, R.; Hering, B.; Reifenrath, J.; Besdo, S.; Windhagen, H.; Willbold, E.; Weizbauer, A. Corrosion behavior, biocompatibility and biomechanical stability of a prototype magnesium-based biodegradable intramedullary nailing system. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Chaya, A.; Yoshizawa, S.; Verdelis, K.; Myers, N.; Costello, B.J.; Chou, D.T.; Pal, S.; Maiti, S.; Kumta, P.N.; Sfeir, C. In vivo study of magnesium plate and screw degradation and bone fracture healing. Acta Biomater. 2015, 18, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Mc, B.E. Absorbable metal in bone surgery: A further report on the use of magnesium alloys. J. Am. Med. Assoc. 1938, 111, 2464–2467. [Google Scholar]
- Windhagen, H.; Radtke, K.; Weizbauer, A.; Diekmann, J.; Noll, Y.; Kreimeyer, U.; Schavan, R.; Stukenborg-Colsman, C.; Waizy, H. Biodegradable magnesium-based screw clinically equivalent to titanium screw in hallux valgus surgery: Short term results of the first prospective, randomized, controlled clinical pilot study. Biomed. Eng. Online 2013, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Ezechieli, M.; Ettinger, M.; Konig, C.; Weizbauer, A.; Helmecke, P.; Schavan, R.; Lucas, A.; Windhagen, H.; Becher, C. Biomechanical characteristics of bioabsorbable magnesium-based (mgyrezr-alloy) interference screws with different threads. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3976–3981. [Google Scholar] [CrossRef] [PubMed]
- Tie, D.; Feyerabend, F.; Muller, W.D.; Schade, R.; Liefeith, K.; Kainer, K.U.; Willumeit, R. Antibacterial biodegradable Mg-Ag alloys. Eur. Cells Mater. 2013, 25, 284–298. [Google Scholar] [CrossRef]
- Jahn, K.; Saito, H.; Taipaleenmaki, H.; Gasser, A.; Hort, N.; Feyerabend, F.; Schluter, H.; Rueger, J.M.; Lehmann, W.; Willumeit-Romer, R.; et al. Intramedullary Mg2Ag nails augment callus formation during fracture healing in mice. Acta Biomater. 2016, 36, 350–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, D.; Zhou, W.; Deng, J.; Liu, Y.; Li, W.; Chu, X.; Xiu, P.; Cai, H.; Kou, Y.; Jiang, B.; et al. Development of magnesium-based biodegradable metals with dietary trace element germanium as orthopaedic implant applications. Acta Biomater. 2017, 64, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.; Lee, H.B.; Dong, Z.; Kotoka, R.; Sankar, J.; Huang, N.; Yun, Y. The effects of static and dynamic loading on biodegradable magnesium pins in vitro and in vivo. Sci. Rep. 2017, 7, 14710. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Zheng, Y.F. Effects of alloying elements (Mn, Co, Al, W, Sn, B, C and S) on biodegradability and in vitro biocompatibility of pure iron. Acta Biomater. 2011, 7, 1407–1420. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Zhou, C.; Fan, H.; Fan, Y.; Jiang, Q.; Song, P.; Fan, H.; Chen, Y.; Zhang, X. Bio-functional design, application and trends in metallic biomaterials. Int. J. Mol. Sci. 2017, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Zheng, Y.F.; Ruan, L. In vitro investigation of Fe30Mn6Si shape memory alloy as potential biodegradable metallic material. Mater. Lett. 2011, 65, 540–543. [Google Scholar] [CrossRef]
- Hermawan, H.; Dube, D.; Mantovani, D. Developments in metallic biodegradable stents. Acta Biomater. 2010, 6, 1693–1697. [Google Scholar] [CrossRef] [PubMed]
- Capek, J.; Msallamova, S.; Jablonska, E.; Lipov, J.; Vojtech, D. A novel high-strength and highly corrosive biodegradable Fe-Pd alloy: Structural, mechanical and in vitro corrosion and cytotoxicity study. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 79, 550–562. [Google Scholar] [CrossRef] [PubMed]
- Hufenbach, J.; Wendrock, H.; Kochta, F.; Kühn, U.; Gebert, A. Novel biodegradable Fe-Mn-C-S alloy with superior mechanical and corrosion properties. Mater. Lett. 2017, 186, 330–333. [Google Scholar] [CrossRef]
- Wang, H.; Zheng, Y.; Liu, J.; Jiang, C.; Li, Y. In vitro corrosion properties and cytocompatibility of Fe-Ga alloys as potential biodegradable metallic materials. Mater. Sci. Eng. C 2017, 71, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Babcock, W.W. Metallic sutures and ligatures. Surg. Clin. N. Am. 1947, 27, 1435–1460. [Google Scholar] [CrossRef]
- Chellamani, K.; Veerasubramanian, D.; Balaji, R. Surgical Sutures: An Overview. J. Acad. Ind. Res. 2013, 1, 778–782. [Google Scholar]
- Seitz, J.-M.; Wulf, E.; Freytag, P.; Bormann, D.; Bach, F.-W. The manufacture of resorbable suture material from magnesium. Adv. Eng. Mater. 2010, 12, 1099–1105. [Google Scholar] [CrossRef]
- Seitz, J.-M.; Utermöhlen, D.; Wulf, E.; Klose, C.; Bach, F.-W. The manufacture of resorbable suture material from magnesium—Drawing and stranding of thin wires. Adv. Eng. Mater. 2011, 13, 1087–1095. [Google Scholar] [CrossRef]
- Bai, J.; Yin, L.; Lu, Y.; Gan, Y.; Xue, F.; Chu, C.; Yan, J.; Yan, K.; Wan, X.; Tang, Z. Preparation, microstructure and degradation performance of biomedical magnesium alloy fine wires. Prog. Natl. Sci. Mater. Int. 2014, 24, 523–530. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, J.; Yan, J.; Chen, Y.; Zhao, C.; Zhang, Y.; Jiang, M.; Xu, H.; Ni, J.; Zhang, X. In vivo degradation and biocompatibility of linear cutter staples made of high purity magnesium. Eur. Cells Mater. 2014, 28, 76. [Google Scholar]
- Wu, H.; Zhao, C.; Ni, J.; Zhang, S.; Liu, J.; Yan, J.; Chen, Y.; Zhang, X. Research of a novel biodegradable surgical staple made of high purity magnesium. Bioact. Mater. 2016, 1, 122–126. [Google Scholar] [CrossRef]
- Cao, J.; Jiang, K.W.; Yang, X.D.; Shen, Z.L.; Guo, P.; Yan, Y.C.; Cui, Y.C.; Han, L.; Lv, Y.; Ye, Y.J.; et al. [animal experimental study of biodegradable magnesium alloy stapler for gastrointestinal anastomosis]. Zhonghua Wei Chang Wai Ke Za Zhi Chin. J. Gastrointest. Surg. 2013, 16, 772–776. [Google Scholar]
- Moore, W.R.; Graves, S.E.; Bain, G.I. Synthetic bone graft substitutes. ANZ J. Surg. 2001, 71, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, W.; Schnitzler, V.; Tancret, F.; Bouler, J.-M. Calcium phosphate cements for bone substitution: Chemistry, handling and mechanical properties. Acta Biomater. 2014, 10, 1035–1049. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, G.; Moghaddam, A. Allograft bone matrix versus synthetic bone graft substitutes. Injury 2011, 42, S16–S21. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.; Hoellen, I.; Ignatius, A. Biodegradable bone cements. Der Orthop. 1997, 26, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Geffers, M.; Groll, J.; Gbureck, U. Reinforcement strategies for load-bearing calcium phosphate biocements. Materials 2015, 8, 2700–2717. [Google Scholar] [CrossRef]
- Vaishya, R.; Chauhan, M.; Vaish, A. Bone cement. J. Clin. Orthop. Trauma 2013, 4, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M. Design of ceramic-based cements and putties for bone graft substitution. Eur. Cells Mater. 2010, 20, 3–10. [Google Scholar] [CrossRef]
- Dos Santos, L.A.; Carrodéguas, R.G.; Boschi, A.O.; Fonseca de Arruda, A.C. Fiber-enriched double-setting calcium phosphate bone cement. J. Biomed. Mater. Res. Part A 2003, 65, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Von Gonten, A.; Kelly, J.; Antonucci, J.M. Load-bearing behavior of a simulated craniofacial structure fabricated from a hydroxyapatite cement and bioresorbable fiber-mesh. J. Mater. Sci. Mater. Med. 2000, 11, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.H.K.; Quinn, J.B. Calcium phosphate cement containing resorbable fibers for short-term reinforcement and macroporosity. Biomaterials 2002, 23, 193–202. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, H.H. Effects of synergistic reinforcement and absorbable fiber strength on hydroxyapatite bone cement. J. Biomed. Mater. Res. Part A 2005, 75, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Jiang, P.; Fan, Q.; Ma, B.; Cai, H. Mechanical and biocompatible influences of chitosan fiber and gelatin on calcium phosphate cement. J. Biomed. Mater. Res. Part B Appl. Biomater. 2007, 82, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Krüger, R.; Groll, J. Fiber reinforced calcium phosphate cements–on the way to degradable load bearing bone substitutes? Biomaterials 2012, 33, 5887–5900. [Google Scholar] [CrossRef] [PubMed]
- Krüger, R.; Seitz, J.-M.; Ewald, A.; Bach, F.-W.; Groll, J. Strong and tough magnesium wire reinforced phosphate cement composites for load-bearing bone replacement. J. Mech. Behav. Biomed. Mater. 2013, 20, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; He, Y.; Zhou, J.; Tang, S.; Yang, Y.; Wang, X. Effects of scandium addition on biocompatibility of biodegradable Mg–1.5Zn–0.6Zr alloy. Mater. Lett. 2018, 215, 200–202. [Google Scholar] [CrossRef]
- Salleh, E.M.; Ramakrishnan, S.; Hussain, Z. Synthesis of biodegradable Mg-Zn alloy by mechanical alloying: Effect of milling time. Procedia Chem. 2016, 19, 525–530. [Google Scholar] [CrossRef]
- Gui, Z.; Kang, Z.; Li, Y. Mechanical and corrosion properties of Mg-Gd-Zn-Zr-Mn biodegradable alloy by hot extrusion. J. Alloys Compd. 2016, 685, 222–230. [Google Scholar] [CrossRef]
- Dai, J.; Zhang, X.; Yin, Q.; Ni, S.; Ba, Z.; Wang, Z. Friction and wear behaviors of biodegradable Mg-6Gd-0.5Zn-0.4Zr alloy under simulated body fluid condition. J. Magn. Alloys 2017, 5, 448–453. [Google Scholar] [CrossRef]
- Kubásek, J.; Vojtěch, D.; Jablonská, E.; Pospíšilová, I.; Lipov, J.; Ruml, T. Structure, mechanical characteristics and in vitro degradation, cytotoxicity, genotoxicity and mutagenicity of novel biodegradable Zn–Mg alloys. Mater. Sci. Eng. C 2016, 58, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Liu, X.; Fan, B.; Lan, P.; Zhou, F.; Li, X.; Wang, H.; Xiao, X.; Li, L.; Zhao, S. Mechanical properties, in vitro degradation behavior, hemocompatibility and cytotoxicity evaluation of Zn–1.2Mg alloy for biodegradable implants. RSC Adv. 2016, 6, 86410–86419. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphate coatings on magnesium and its biodegradable alloys. Acta Biomater. 2014, 10, 2919–2934. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.W.; Shan, D.Y.; Han, E.H. Electrodeposition of hydroxyapatite coating on AZ91D magnesium alloy for biomaterial application. Mater. Lett. 2008, 62, 3276–3279. [Google Scholar] [CrossRef]
- Rojaee, R.; Fathi, M.; Raeissi, K. Controlling the degradation rate of AZ91 magnesium alloy via sol–gel derived nanostructured hydroxyapatite coating. Mater. Sci. Eng. C 2013, 33, 3817–3825. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Li, G.; Lian, J. A chemical conversion hydroxyapatite coating on AZ60 magnesium alloy and its electrochemical corrosion behaviour. Int. J. Electrochem. Sci. 2012, 7, 11497–11511. [Google Scholar]
- Zhang, Y.; Ma, Y.; Chen, M.; Wei, J. Effects of anodizing biodegradable Mg–Zn–Zr alloy on the deposition of Ca–P coating. Surf. Coat. Technol. 2013, 228, S111–S115. [Google Scholar] [CrossRef]
- Tsubakino, H.; Yamamoto, A.; Fukumoto, S.; Watanabe, A.; Sugahara, K.; Inoue, H. High-purity magnesium coating on magnesium alloys by vapor deposition technique for improving corrosion resistance. Mater. Trans. 2003, 44, 504–510. [Google Scholar] [CrossRef]
- Johnson, I.; Akari, K.; Liu, H. Nanostructured hydroxyapatite/poly (lactic-co-glycolic acid) composite coating for controlling magnesium degradation in simulated body fluid. Nanotechnology 2013, 24, 375103. [Google Scholar] [CrossRef] [PubMed]
- Butev, E.; Esen, Z.; Bor, S. In vitro bioactivity investigation of alkali treated Ti6Al7Nb alloy foams. Appl. Surf. Sci. 2015, 327, 437–443. [Google Scholar] [CrossRef]
- Tang, H.; Wu, T.; Xu, F.; Tao, W.; Jian, X. Fabrication and characterization of Mg(OH)2 films on AZ31 magnesium alloy by alkali treatment. Int. J. Electrochem. Sci. 2017, 12, 1377–1388. [Google Scholar] [CrossRef]
- Feng, J.; Chen, Y.; Liu, X.; Liu, T.; Zou, L.; Wang, Y.; Ren, Y.; Fan, Z.; Lv, Y.; Zhang, M. In-situ hydrothermal crystallization Mg(Oh)2 films on magnesium alloy AZ91 and their corrosion resistance properties. Mater. Chem. Phys. 2013, 143, 322–329. [Google Scholar] [CrossRef]
- Shadanbaz, S.; Dias, G.J. Calcium phosphate coatings on magnesium alloys for biomedical applications: A review. Acta Biomater. 2012, 8, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Harun, W.S.W.; Asri, R.I.M.; Alias, J.; Zulkifli, F.H.; Kadirgama, K.; Ghani, S.A.C.; Shariffuddin, J.H.M. A comprehensive review of hydroxyapatite-based coatings adhesion on metallic biomaterials. Ceram. Int. 2018, 44, 1250–1268. [Google Scholar] [CrossRef]
- Zhao, N.; Zhu, D. Collagen self-assembly on orthopedic magnesium biomaterials surface and subsequent bone cell attachment. PLoS ONE 2014, 9, e110420. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.-L.; Yan, Y.-H.; Wan, T.; Yang, H. Poly (l-lactic acid)/hydroxyapatite/collagen composite coatings on AZ31 magnesium alloy for biomedical application. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2013, 227, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Z.; Shi, X.-H.; Zhang, P.-C.; Bai, B.; Leng, Y.-X.; Huang, N. The microstructure and properties of commercial pure iron modified by plasma nitriding. Solid State Ion. 2008, 179, 971–974. [Google Scholar] [CrossRef]
- Zhu, S.; Huang, N.; Xu, L.; Zhang, Y.; Liu, H.; Lei, Y.; Sun, H.; Yao, Y. Biocompatibility of Fe–O films synthesized by plasma immersion ion implantation and deposition. Surf. Coat. Technol. 2009, 203, 1523–1529. [Google Scholar] [CrossRef]
- Zhou, J.; Yang, Y.; Alonso Frank, M.; Detsch, R.; Boccaccini, A.R.; Virtanen, S. Accelerated degradation behavior and cytocompatibility of pure iron treated with sandblasting. ACS Appl. Mater. Interfaces 2016, 8, 26482–26492. [Google Scholar] [CrossRef] [PubMed]
- Dobatkin, S.V.; Lukyanova, E.A.; Martynenko, N.S.; Anisimova, N.Y.; Kiselevskiy, M.V.; Gorshenkov, M.V.; Yurchenko, N.Y.; Raab, G.I.; Yusupov, V.S.; Birbilis, N.; et al. Strength, corrosion resistance, and biocompatibility of ultrafine-grained mg alloys after different modes of severe plastic deformation. IOP Conf. Ser. Mater. Sci. Eng. 2017, 194, 012004. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of a typical pass in the wire drawing process.

Figure 2.
(a) Porous pure-magnesium implantation; (b) survival rate of the group of rats with magnesium implants compared with control group; (c) gas cavity formation; and (d) subcutaneous opening of the implantation area at Day 7, reproduced with permission from [41], Elsevier, 2016.
Figure 2.
(a) Porous pure-magnesium implantation; (b) survival rate of the group of rats with magnesium implants compared with control group; (c) gas cavity formation; and (d) subcutaneous opening of the implantation area at Day 7, reproduced with permission from [41], Elsevier, 2016.

Figure 3.
Schematic diagram of degradation mechanism of Zn in a physiological environment.

Figure 4.
(a) Radiographic picture of K-wires used to repair a fracture of the medial epicondyle in the elbow and (b) radiograph shows cerclage wiring used to contain bone fragments in a fracture around the stem of a femoral prosthesis, reproduced with permission from [76], The Radiological Society of North America (RSNA®), 1991.
Figure 4.
(a) Radiographic picture of K-wires used to repair a fracture of the medial epicondyle in the elbow and (b) radiograph shows cerclage wiring used to contain bone fragments in a fracture around the stem of a femoral prosthesis, reproduced with permission from [76], The Radiological Society of North America (RSNA®), 1991.

Figure 5.
The radiograph shows tension band wiring used to repair an olecranon fracture, reproduced with permission from [76], The Radiological Society of North America (RSNA®), 1991.
Figure 5.
The radiograph shows tension band wiring used to repair an olecranon fracture, reproduced with permission from [76], The Radiological Society of North America (RSNA®), 1991.

Figure 6.
X-ray images to determine degradation of intramedullary Mg2Ag wires during 133 days in mice compared to a steel pin (scale bar = 5 mm), reproduced with permission from [113], Elsevier, 2016.
Figure 6.
X-ray images to determine degradation of intramedullary Mg2Ag wires during 133 days in mice compared to a steel pin (scale bar = 5 mm), reproduced with permission from [113], Elsevier, 2016.

Figure 7.
Comparison of the mechanical properties among various biodegradable Mg-X alloys (X: essential/possibly essential element in human health). Different symbols represent different alloy systems and symbol color reflects the process condition, reproduced with permission from [114], Elsevier, 2017.
Figure 7.
Comparison of the mechanical properties among various biodegradable Mg-X alloys (X: essential/possibly essential element in human health). Different symbols represent different alloy systems and symbol color reflects the process condition, reproduced with permission from [114], Elsevier, 2017.

Figure 8.
Optical micrographs of the wires after implantation for (a–c) 4 weeks and (d–f) 52 weeks of (a,d) pure Fe, (b,e) Fe–10Mn–1Pd and (c,f) Fe–21Mn–0.7C–1Pd, reproduced with permission from [48], Elsevier, 2014.
Figure 8.
Optical micrographs of the wires after implantation for (a–c) 4 weeks and (d–f) 52 weeks of (a,d) pure Fe, (b,e) Fe–10Mn–1Pd and (c,f) Fe–21Mn–0.7C–1Pd, reproduced with permission from [48], Elsevier, 2014.

Figure 9.
Knotted noose made of the alloy AL36, reproduced with permission from [125], WILEY, 2010.
Figure 9.
Knotted noose made of the alloy AL36, reproduced with permission from [125], WILEY, 2010.

Figure 10.
Comparison between three different compositions of FRCPC including AZ31, PLA and hybrid (both AZ31 and PLA). (a) Load-displacement curves; (b) Bending strength and (c) Fracture images of the composites, reproduced with permission from [114], Elsevier, 2013.
Figure 10.
Comparison between three different compositions of FRCPC including AZ31, PLA and hybrid (both AZ31 and PLA). (a) Load-displacement curves; (b) Bending strength and (c) Fracture images of the composites, reproduced with permission from [114], Elsevier, 2013.


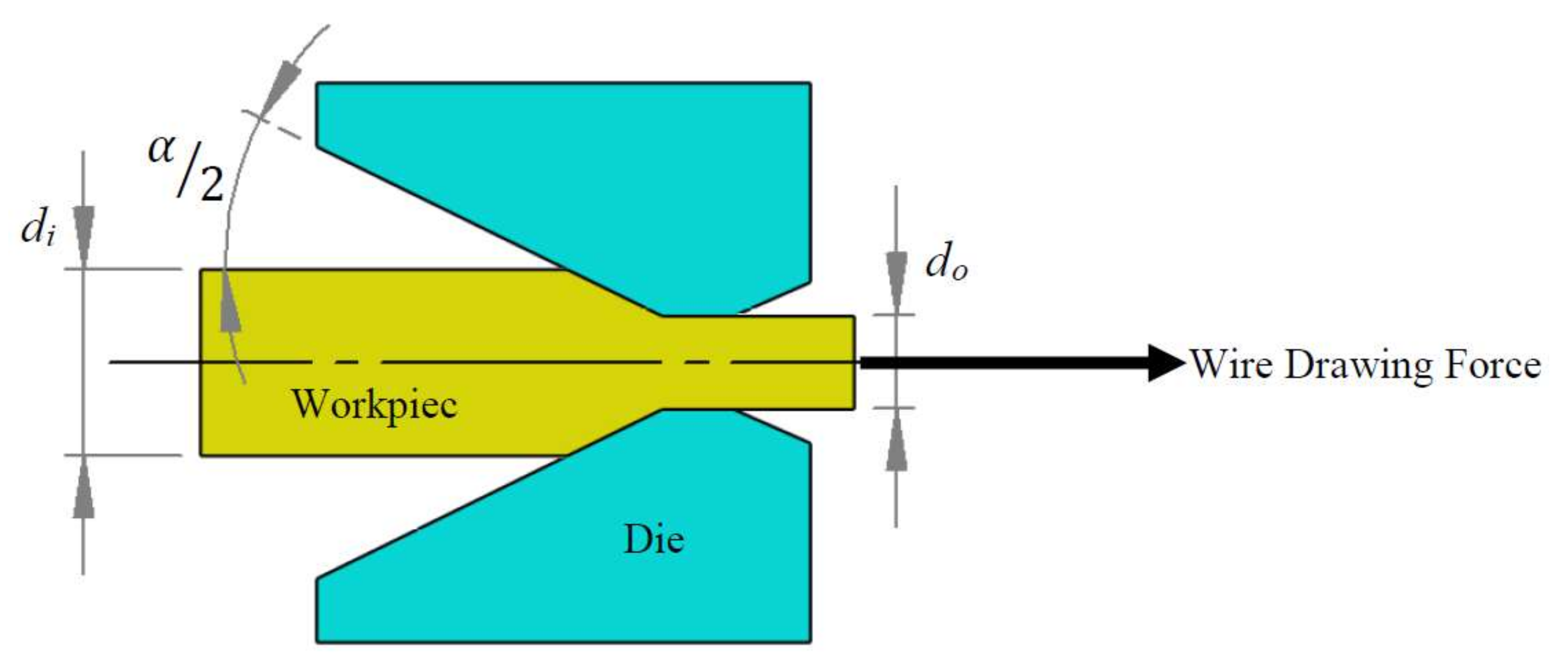{kind=link}
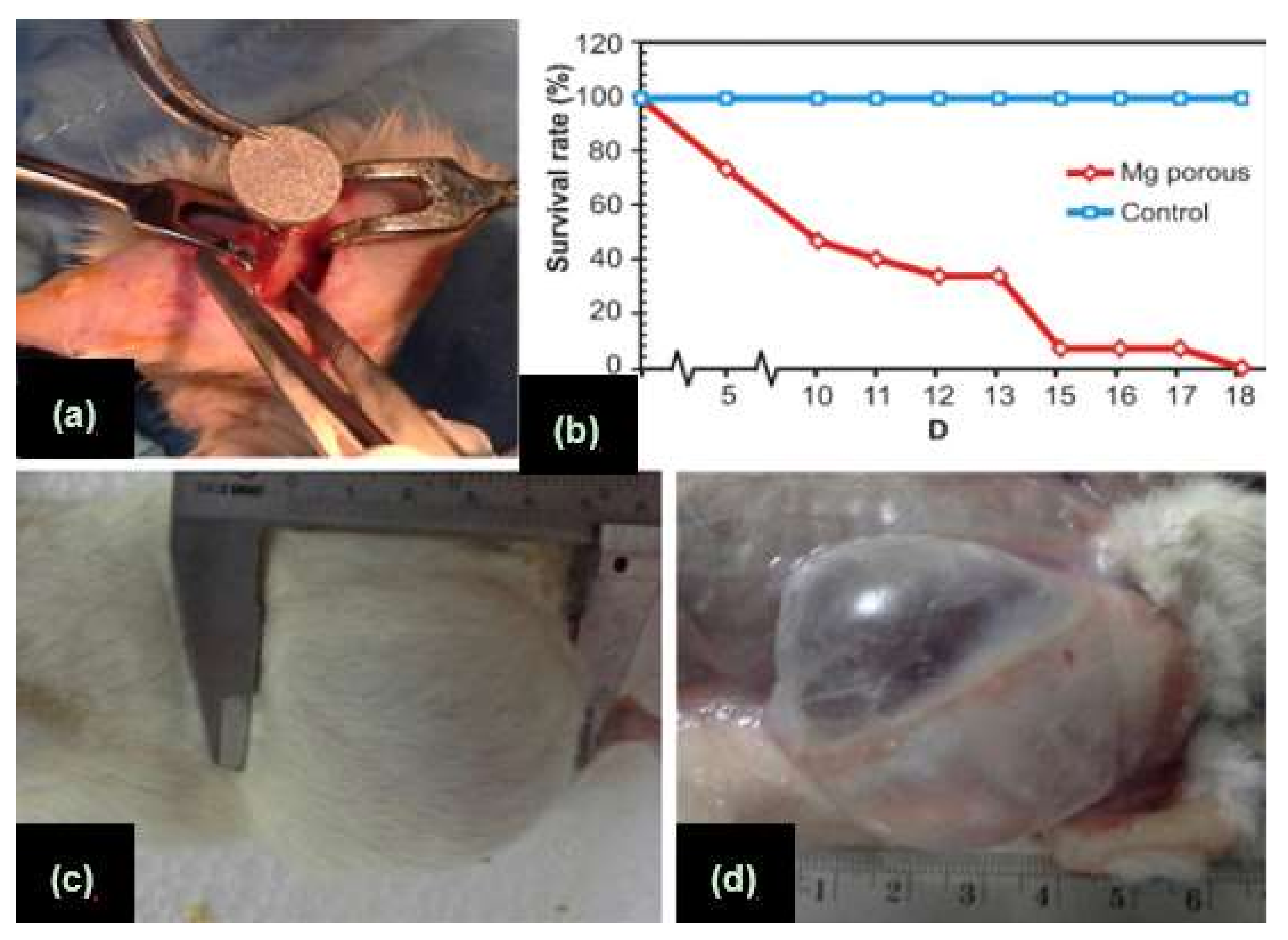{kind=link}
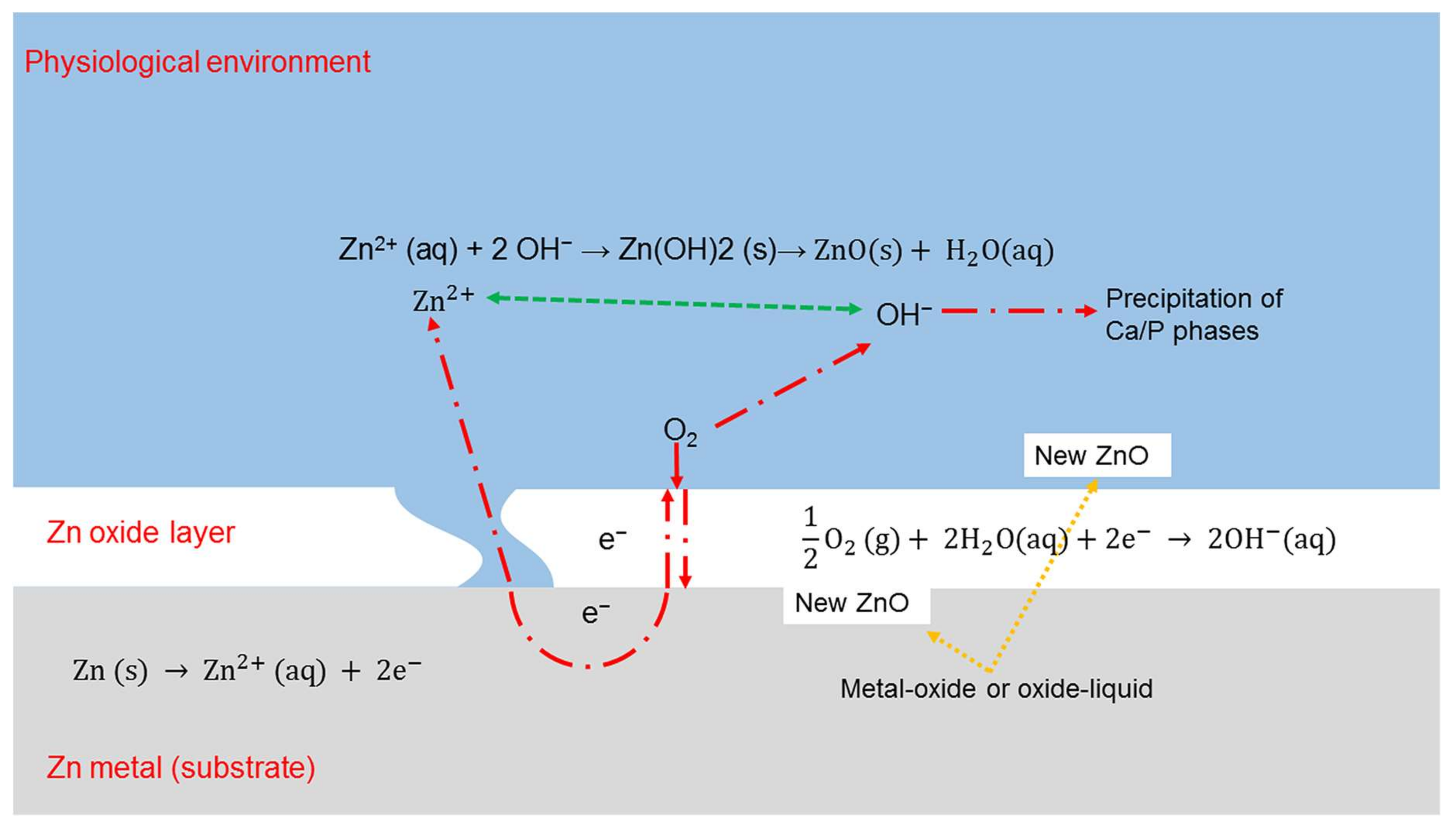{kind=link}
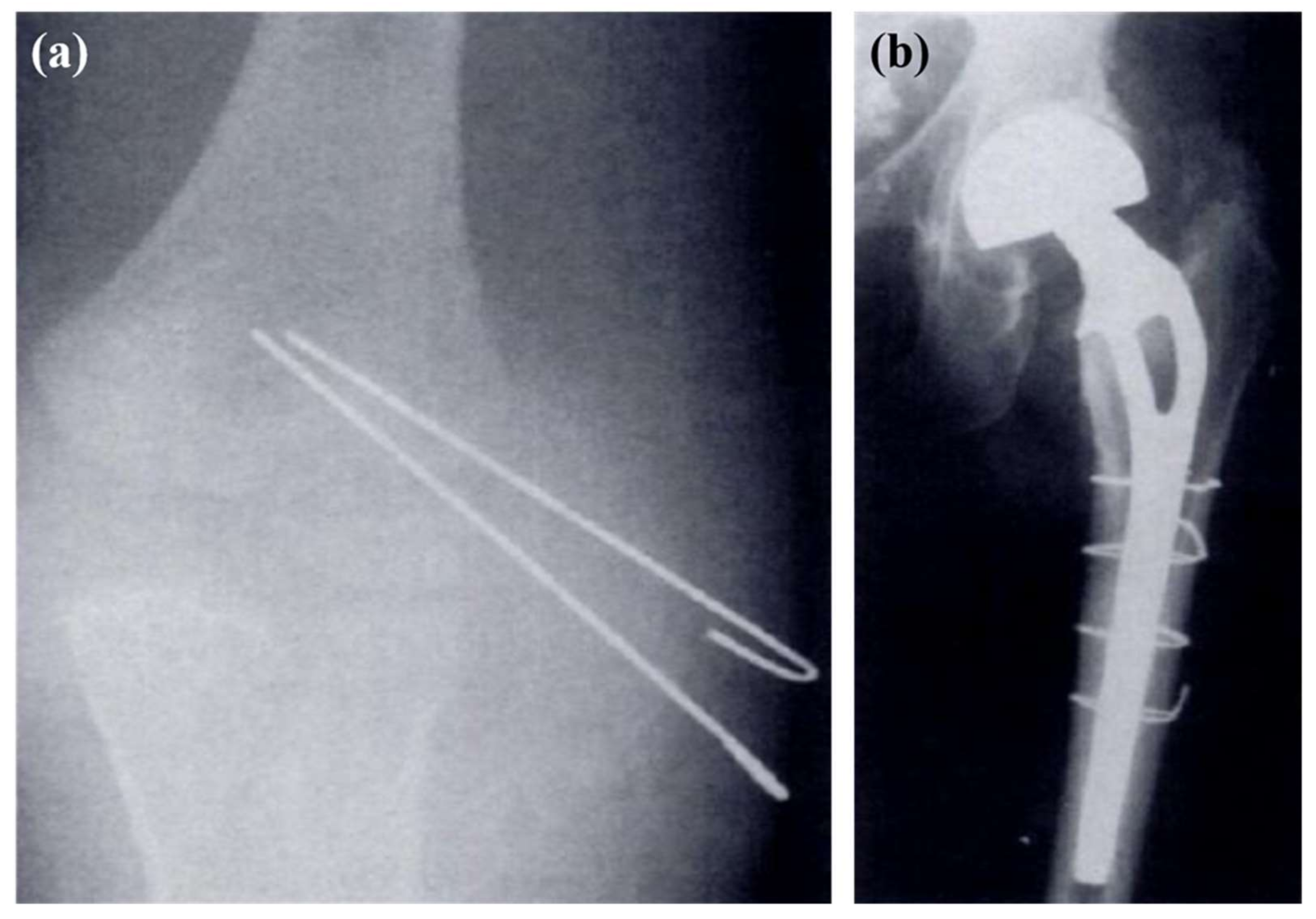{kind=link}
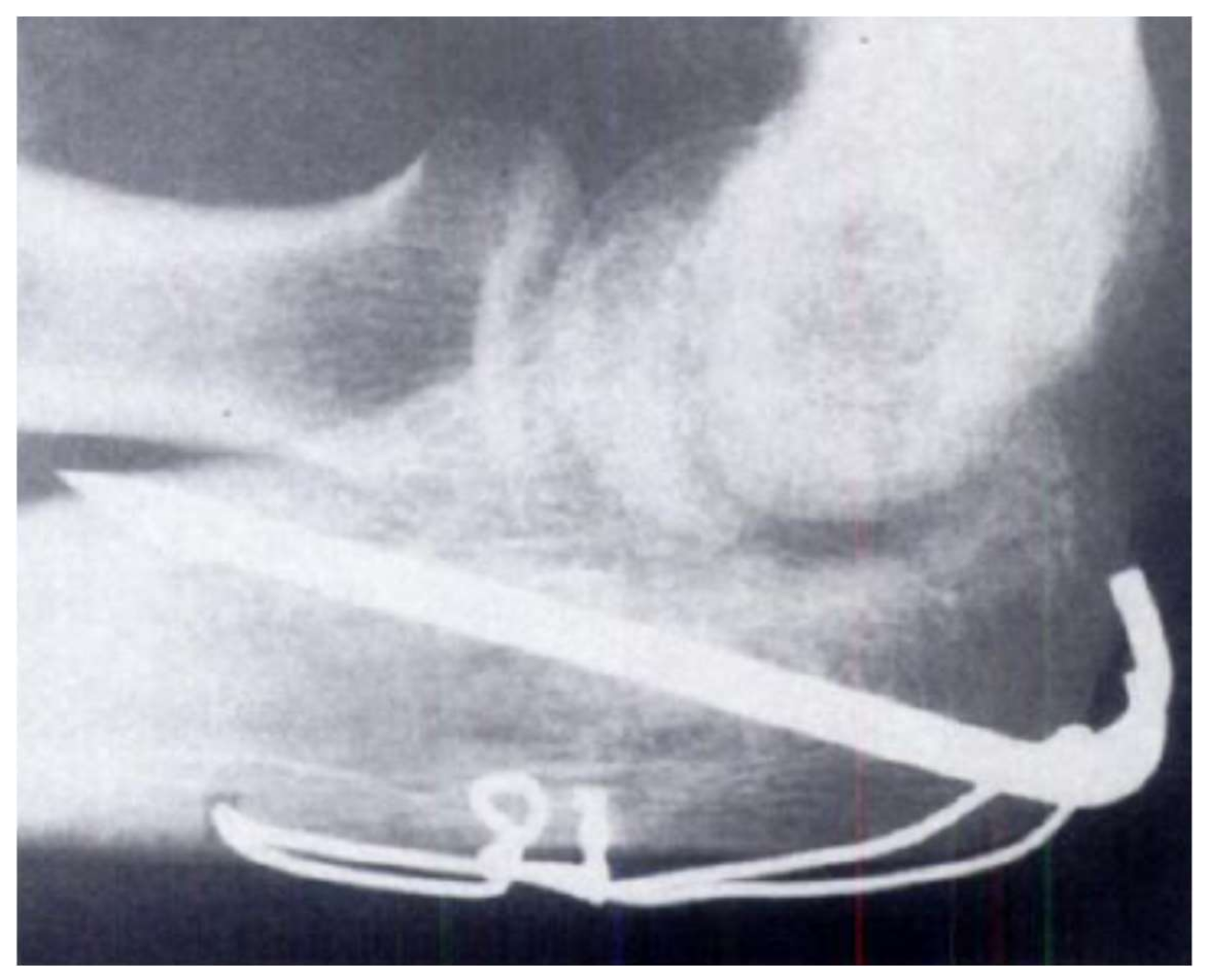{kind=link}
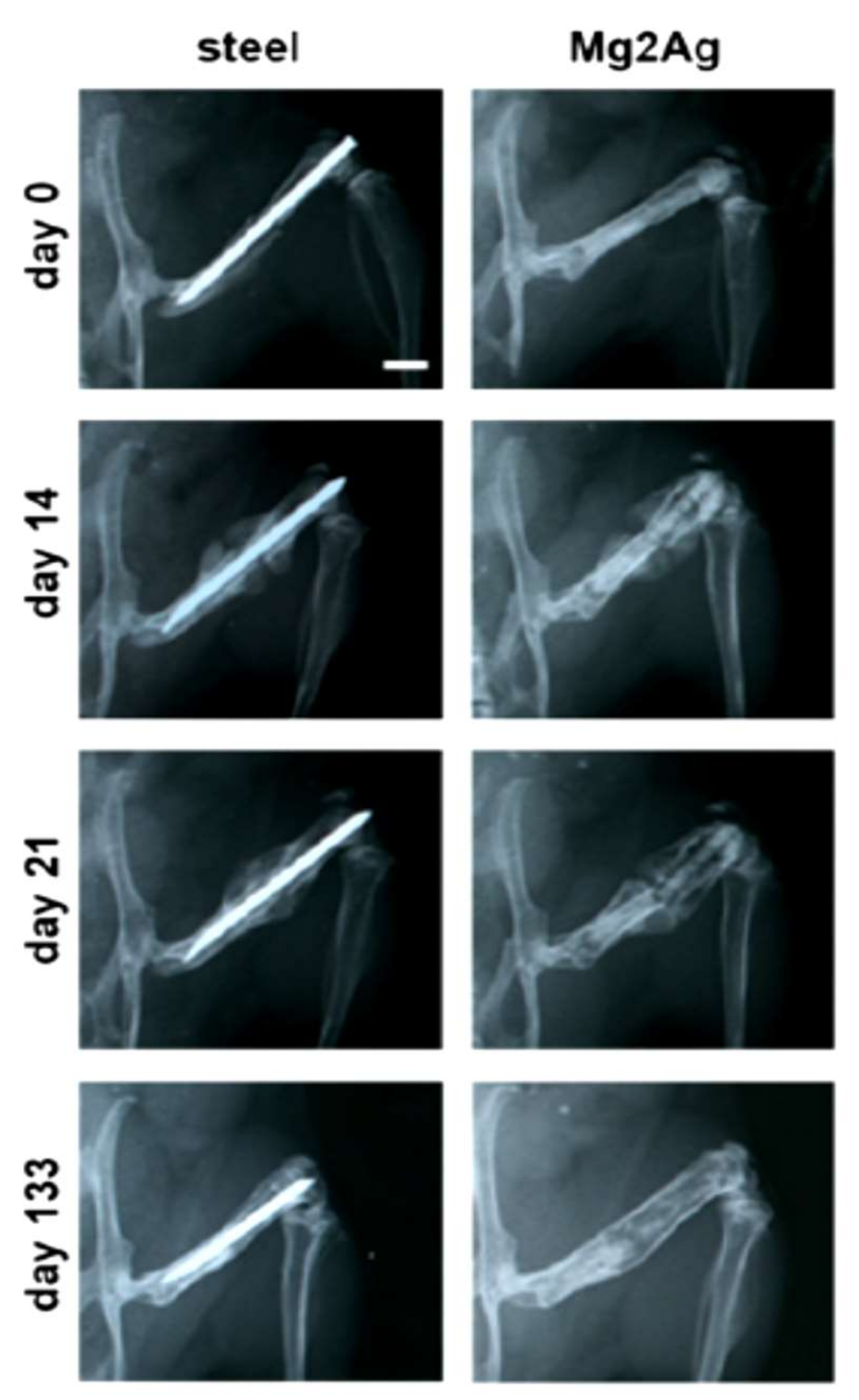{kind=link}
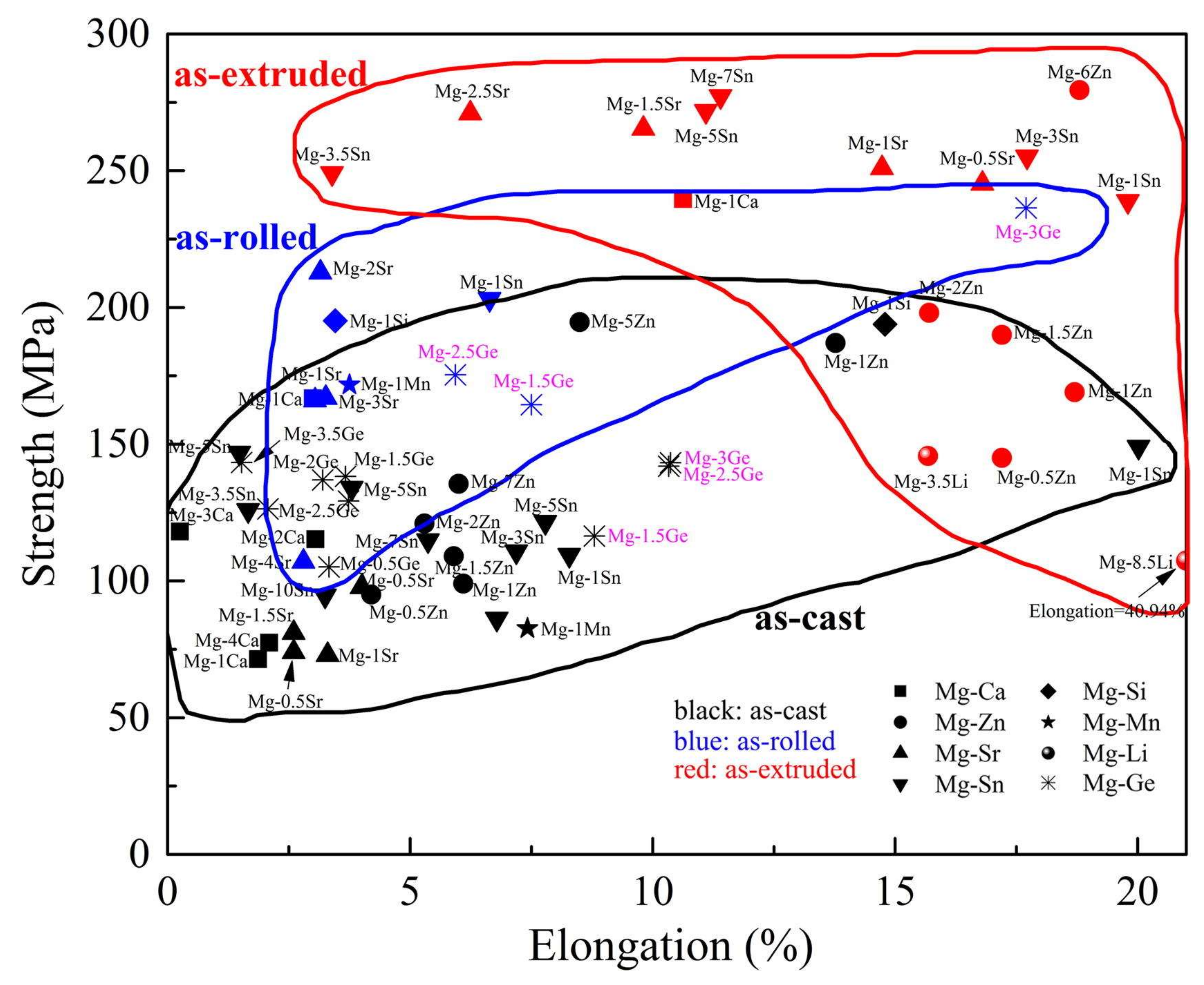{kind=link}
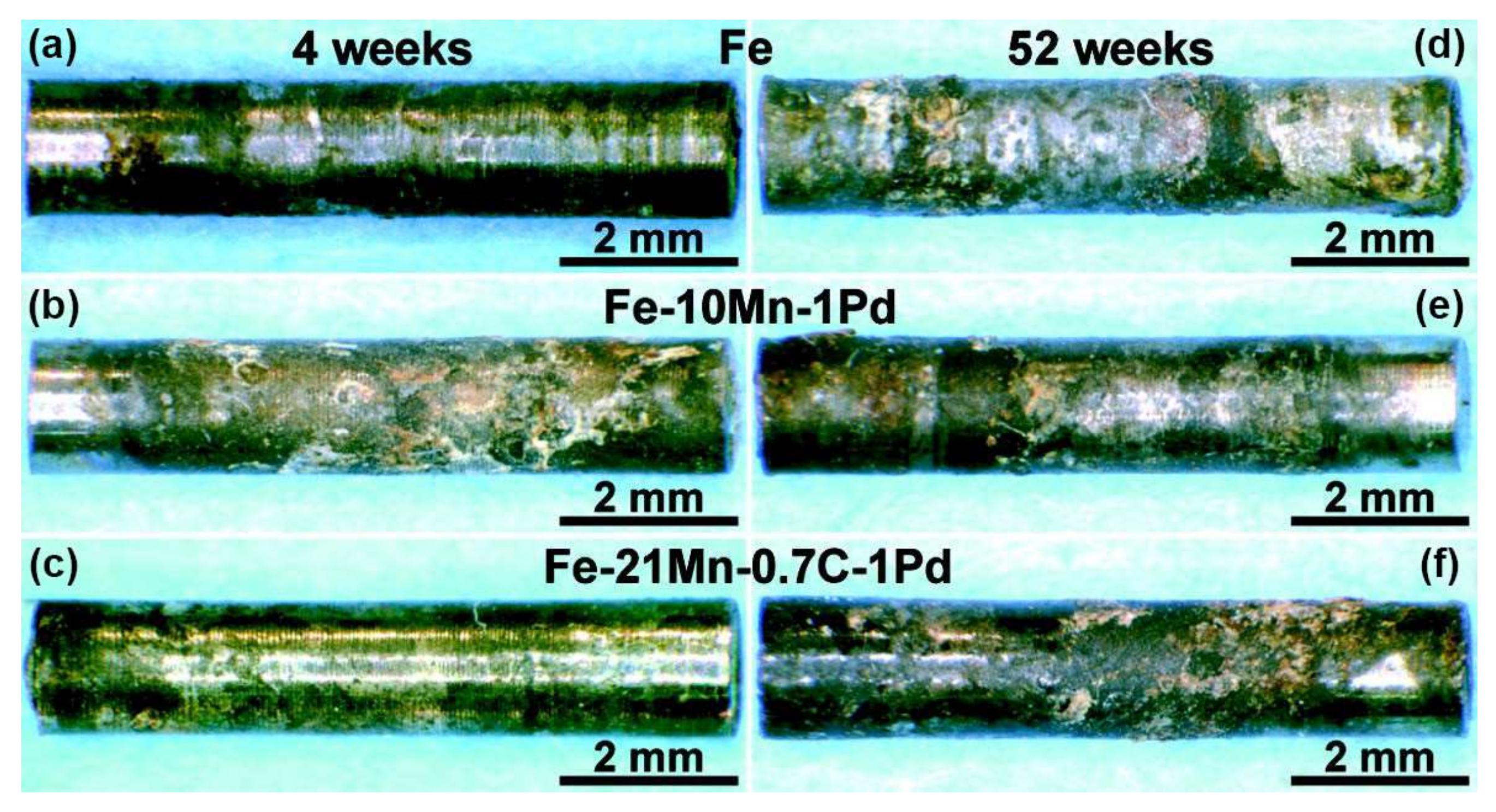{kind=link}
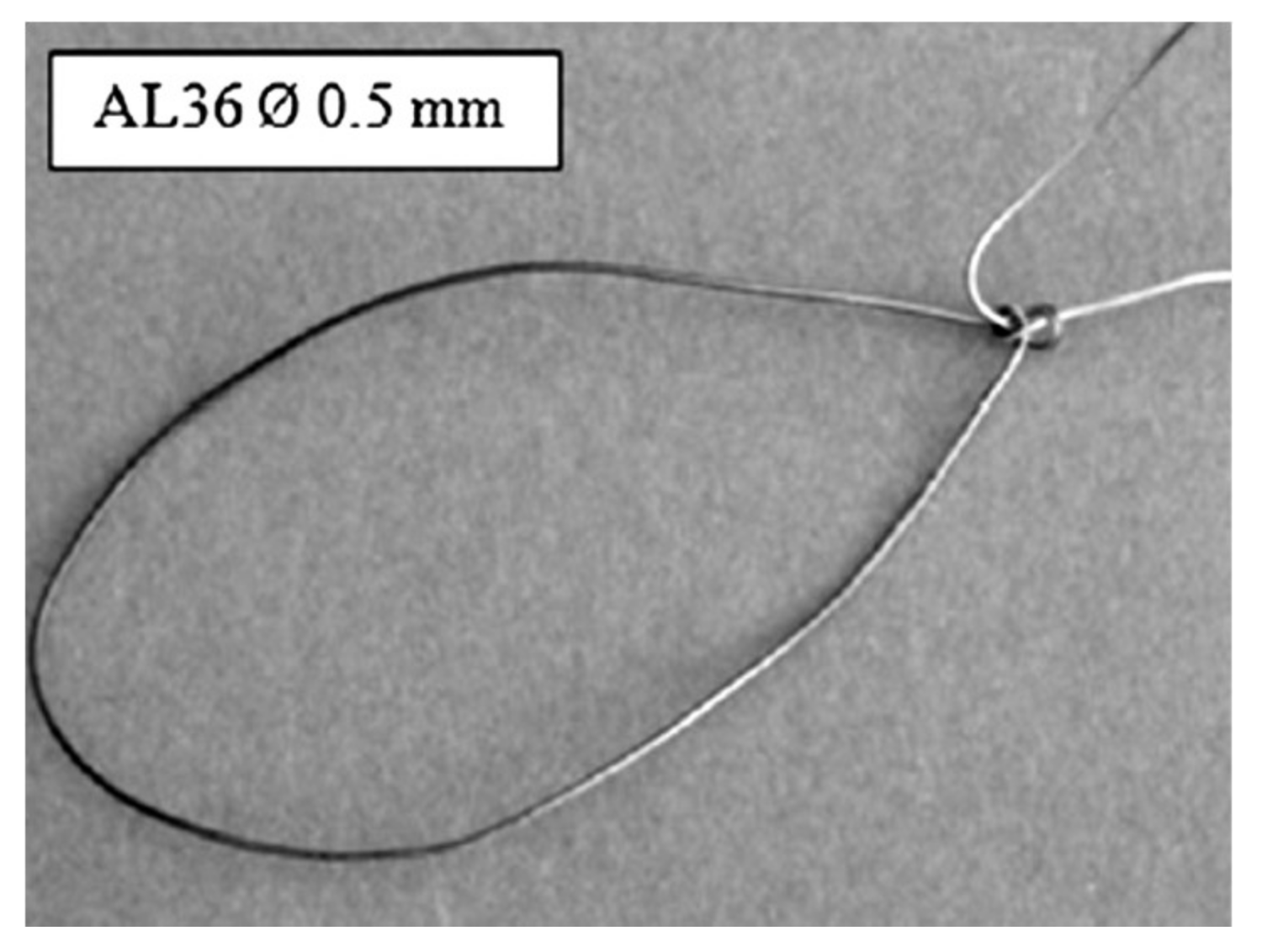{kind=link}
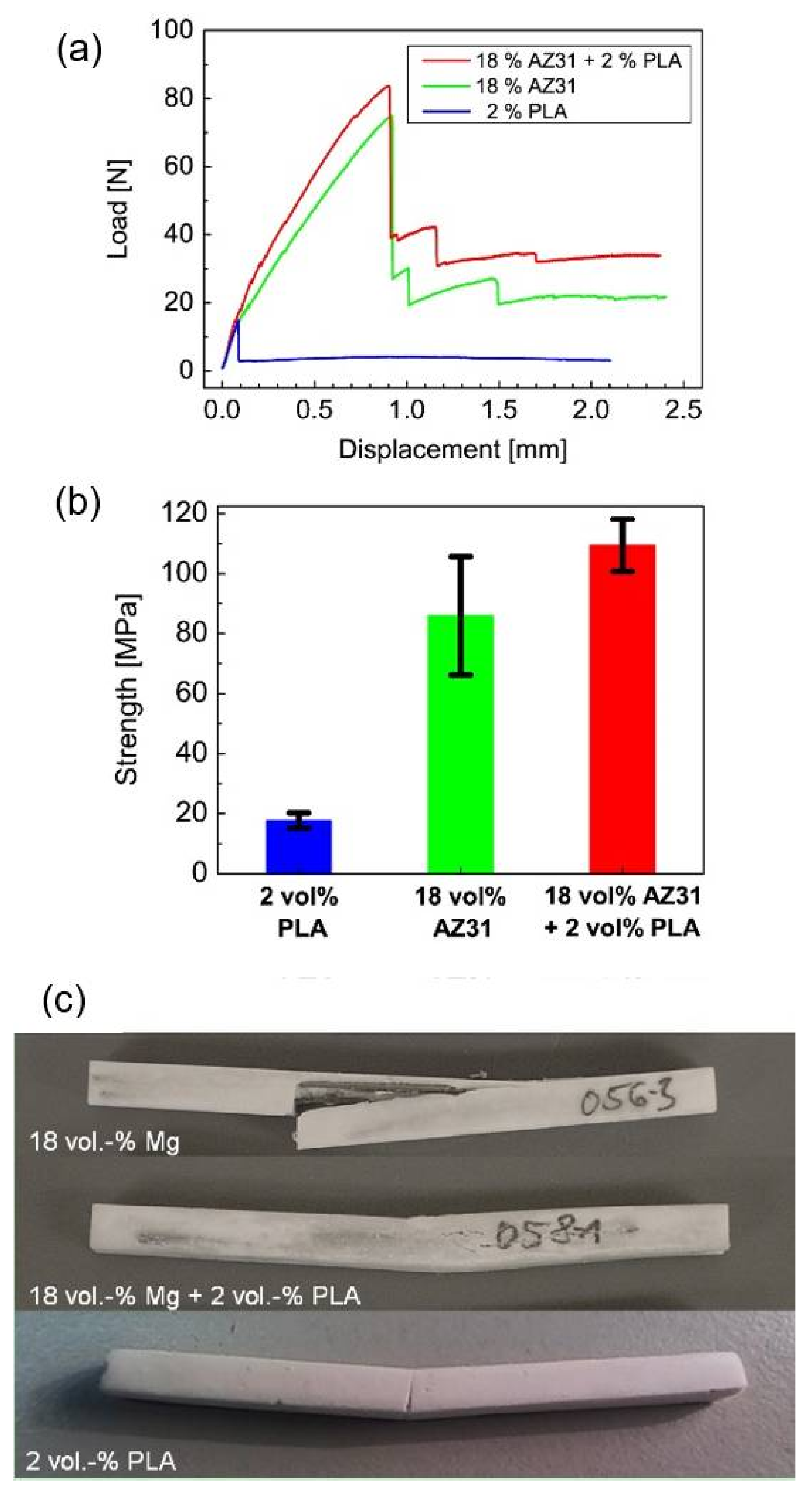{kind=link}
Table 1.
Comparison of typical mechanical properties of cortical bone and commonly used metallic biomaterials, data from [35,36,37].
| Tissue/Material | Young’s Modulus, E (GPa) | Yield Tensile Strength (MPa) | Ultimate Tensile Strength (MPa) | Density (g/cm3) |
|---|---|---|---|---|
| Cortical bone | 5–23 | 104.9–114.3 | 35–283 | 1.8–2.0 |
| Pure Mg, wrought | 41–45 | 100 | 180 | 1.74 |
| Pure Zn, as cast | 90 | 10 | 20 | 7.13 |
| Pure Fe | 211.4 | 50 | 540 | 7.87 |
| Ti-6Al-4V, as cast | 114 | 760–880 | 830–1025 | 4.43 |
| 316L stainless steel | 193 | 200–300 | 450–650 | 8 |
| Co-Cr alloy | 240 | 500–1500 | 900–1540 | 8.3 |
Table 2.
Common permanent biomaterials used for bone wires, data from [86].
Table 2.
Common permanent biomaterials used for bone wires, data from [86].
| Chemical Composition | Alloy | ASTM Number | Application |
|---|---|---|---|
| Fe-18Cr-14Ni-2.5Mo (C < 0.03) | 316 L | F138-08/F139-08/F1350-08 | Kirschner wires, cerclage wires |
| Fe-19Cr-10Ni-2Mn | 302 | A313/F899 | guidewires |
| Fe-20Cr-10.5Ni-2Mn | - | A313/F899 | Guidewires, orthodontic wires |
| Fe-20Cr-10.5Ni-2Mn (C < 0.03) | - | A580 | Guidewires, Orthodontic wires |
| 35Co-35Ni-20Cr-10Mo (Ti = 0.7) | MP35N | F562 | Orthopedic wires |
| 35Co-35Ni-10Mo (Ti = 0.01) | 35NLT | F562 | Orthopedic wires |
| 40Co-20Cr-16Fe-15Ni-7Mo | Elgiloy | F1058–08 | Surgical wires |
| Ti-6Al-4V | - | F136 | Kirschner-wires |
| Ti-Ni | Nitinol | F2063 | Archwires, Kirschner-wires |
Table 3.
Biodegradable metallic wires in bone applications.
| Base Metal | Alloy | Wire Diameter (mm) | Fabrication Process | Application | Type of Biological Experiments | Published Time |
|---|---|---|---|---|---|---|
| Mg | ZEK100 [125] | 0.3–0.5 | Hot extrusion | Suture | - | 2010 |
| MgCa0.8 [125] | 0.3–0.5 | Hot extrusion | Suture | - | 2010 | |
| AL36 [125] | 0.3–0.5 | Hot extrusion | Suture | - | 2010 | |
| AX30 [125] | 0.3–0.5 | Hot extrusion | Suture | - | 2010 | |
| ZEK100 [126] | 0.274 m–0.822 p | Hot extrusion + Cold drawing + Intermediate annealing | Suture | - | 2011 | |
| MgCa0.8 [126] | 0.274 m–0.822 p | Hot extrusion + Cold drawing + Intermediate annealing | Suture | - | 2011 | |
| AL36 [126] | 0.274 m–0.822 p | Hot extrusion + Cold drawing + Intermediate annealing | Suture | - | 2011 | |
| AX30 [126] | 0.274 m–0.822 p | Hot extrusion + Cold drawing + Intermediate annealing | Suture | - | 2011 | |
| Mg-4Gd-0.4Zn [127] | 0.3 | Hot extrusion + Cold drawing + Intermediate annealing | Suture | in vitro | 2014 | |
| Mg-4Y-0.4Zn [127] | 0.3 | Hot extrusion + Cold drawing + Intermediate annealing | Suture | in vitro | 2014 | |
| Mg-4Nd-0.4Zn [127] | 0.3 | Hot extrusion + Cold drawing + Intermediate annealing | Suture | in vitro | 2014 | |
| Mg2Ag [113] | 0.8 | Hot extrusion + Cold drawing + Intermediate annealing | Guide wire-thin pin | in vitro-in vivo (mouse) | 2016 | |
| Mg3Ge [114] | 2.2 | Hot rolling + Machining | Guide wire-thin pin | in vitro-in vivo (rabbit) | 2017 | |
| Mg-Zn-Mn [115] | 1.6 | Hot extrusion | Guide wire-thin pin | in vitro-in vivo (mouse) | 2017 | |
| Fe | Fe–10Mn–1Pd [48] | 1.6 | Casting + Machining | Guide wire-thin pin | in vitro-in vivo (rat) | 2014 |
| Fe–21Mn–0.7C–1Pd [48] | 1.6 | Casting + Machining | Guide wire-thin pin | in vitro-in vivo (rat) | 2014 |
m: Monofilament, p: polyfilament.
Table 4.
Biological and mechanical advantages and disadvantages of alloying elements for Mg.
| Alloying Element | Advantages | Disadvantages |
|---|---|---|
| Al | Increase the strength and ductility and decrease the corrosion rate [26]. | Neurotoxicity and accumulation in bone [87]. |
| Ca | Most abundant mineral and mainly stored in bone and teeth; activator or stabilizer of enzymes [87]. | Calcium metabolism disorder; kidney stones; increasing corrosion rate [97]. |
| Cu | Increase the ductility [97]. | Neurodegenerative diseases including Alzheimer’s, Menkes, and Wilson disease; accelerate corrosion and decrease the strength [26]. |
| Zn | Essential trace element; appear in all enzyme classes; increase the strength and improve corrosion resistance [87]. | Euro toxic and hinder bone development at higher concentration [87]. |
| Mn | Improve corrosion resistance, strength and ductility; essential trace element; activator of enzyme; Mn deficiency is related to osteoporosis, diabetes mellitus, and atherosclerosis [87]. | Excessive Mn results in neurotoxicity [87]. |
| Si | Cross linking agent of connective tissue basement membrane structures; necessary for bone calcification [87]. | Excessive SiO2 causes lung diseases [87]; decreasing the ductility and increasing corrosion rate [97]. |
| Li | Used in the treatment of manic-depressive psychoses [87]. | Decrease the strength and increasing corrosion rate [97]. |
| Zr | Increase the strength and ductility [97]. | High concentration in liver and gall bladder [87]. |
| RE | Compound of drugs for treatment of cancer; improve the mechanical properties and corrosion resistance [87]. | Accumulation in bone and liver [87]. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Asgari, M.; Hang, R.; Wang, C.; Yu, Z.; Li, Z.; Xiao, Y. Biodegradable Metallic Wires in Dental and Orthopedic Applications: A Review. Metals 2018, 8, 212. https://doi.org/10.3390/met8040212
AMA Style
Asgari M, Hang R, Wang C, Yu Z, Li Z, Xiao Y. Biodegradable Metallic Wires in Dental and Orthopedic Applications: A Review. Metals. 2018; 8(4):212. https://doi.org/10.3390/met8040212
Chicago/Turabian StyleAsgari, Mohammad, Ruiqiang Hang, Chang Wang, Zhentao Yu, Zhiyong Li, and Yin Xiao. 2018. "Biodegradable Metallic Wires in Dental and Orthopedic Applications: A Review" Metals 8, no. 4: 212. https://doi.org/10.3390/met8040212
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.