
Changes in T2 Relaxation Time Mapping of Intervertebral Discs Adjacent to Vertebrae after Kyphoplasty Correlate with the Physical Clinical Outcome of Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Procedure
2.2. Image Acquisition
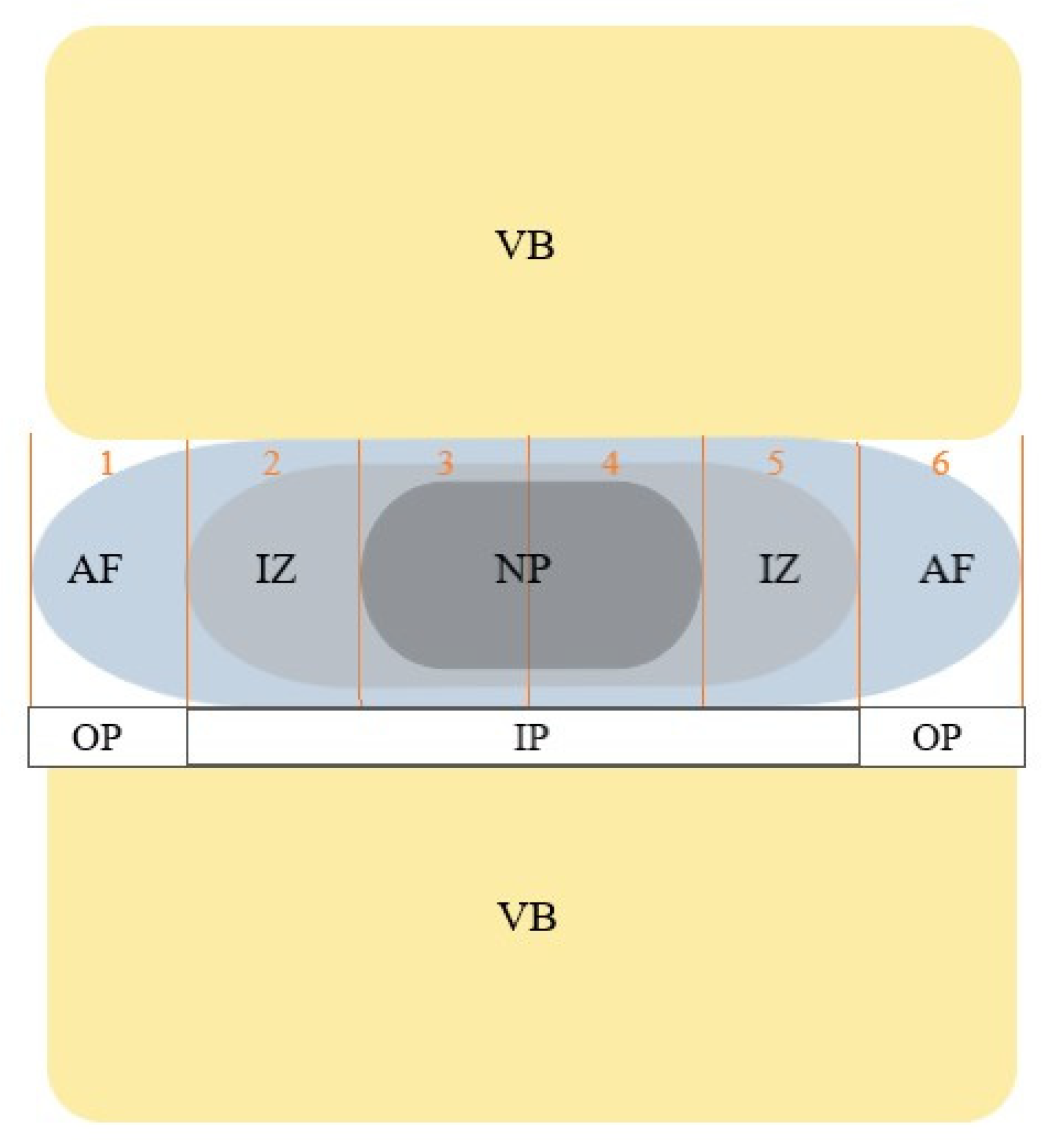
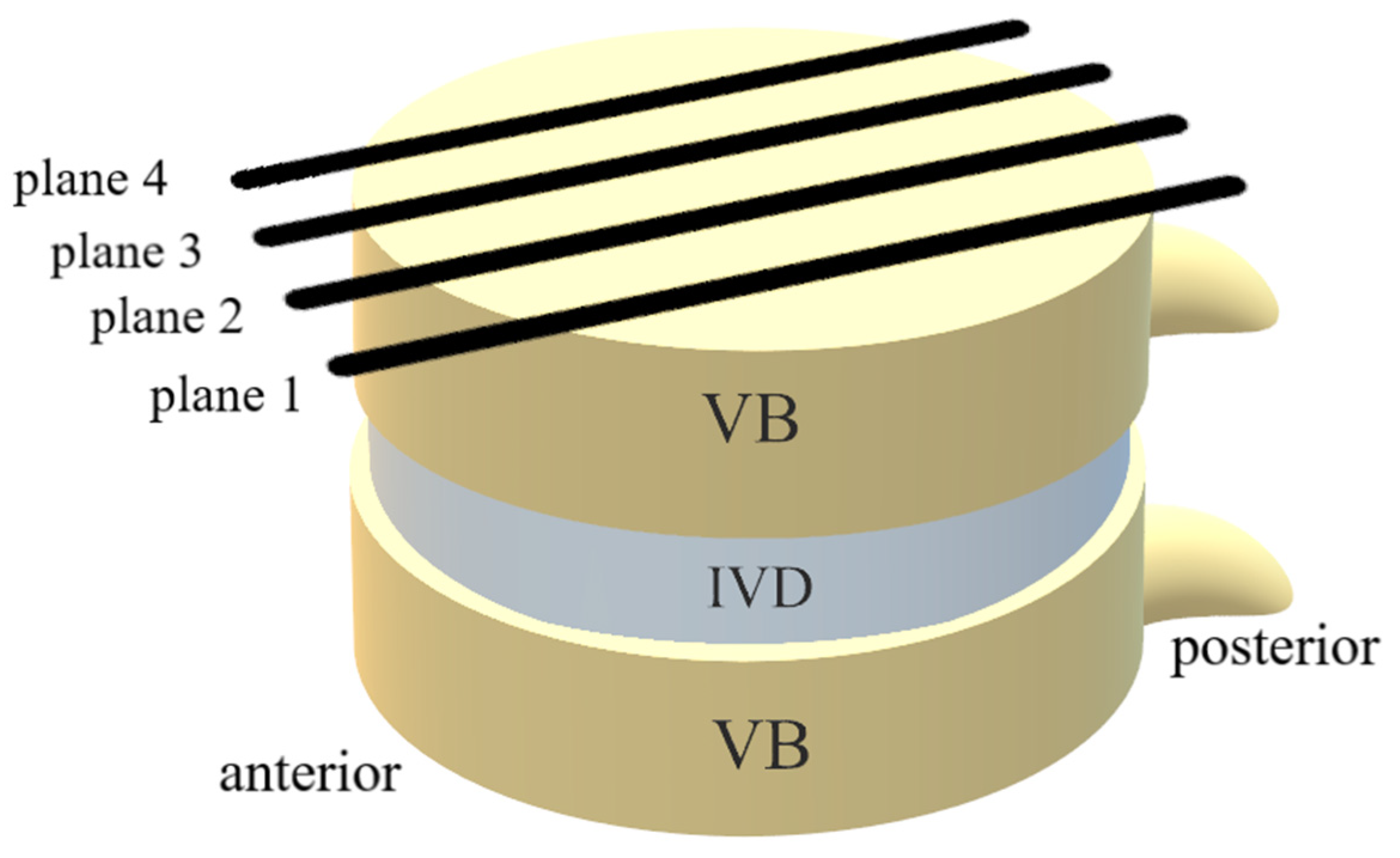
2.3. Image Analysis
2.4. Quality of Life Analysis
2.4.1. 36-Item Short Form Survey (SF-36)
2.4.2. Oswestry Low Back Pain Disability Questionnaire (ODQ)
2.4.3. Numerical Rating Scale (NRS)
2.5. Statistical Analysis
3. Results
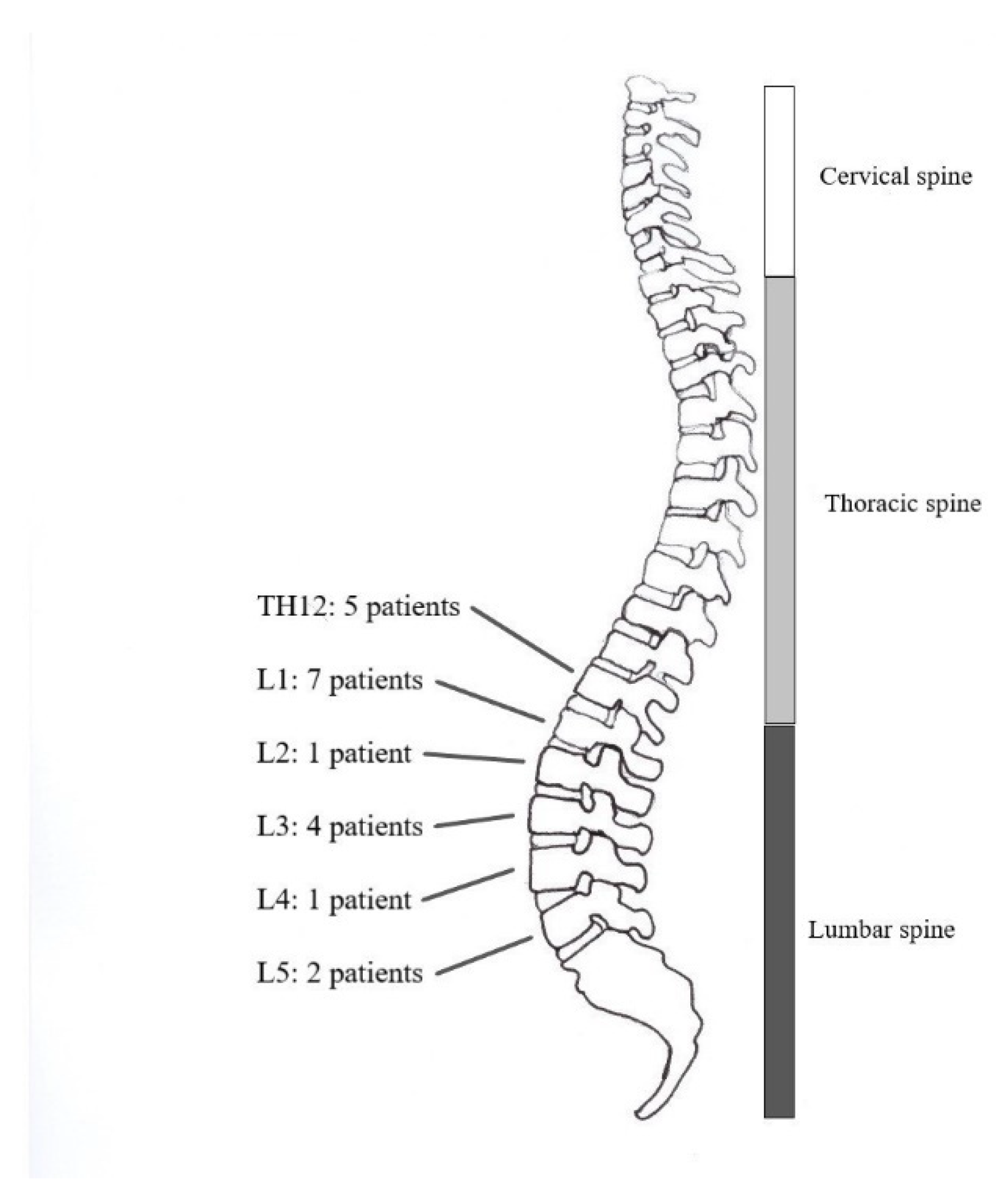
3.1. Patient Characteristics
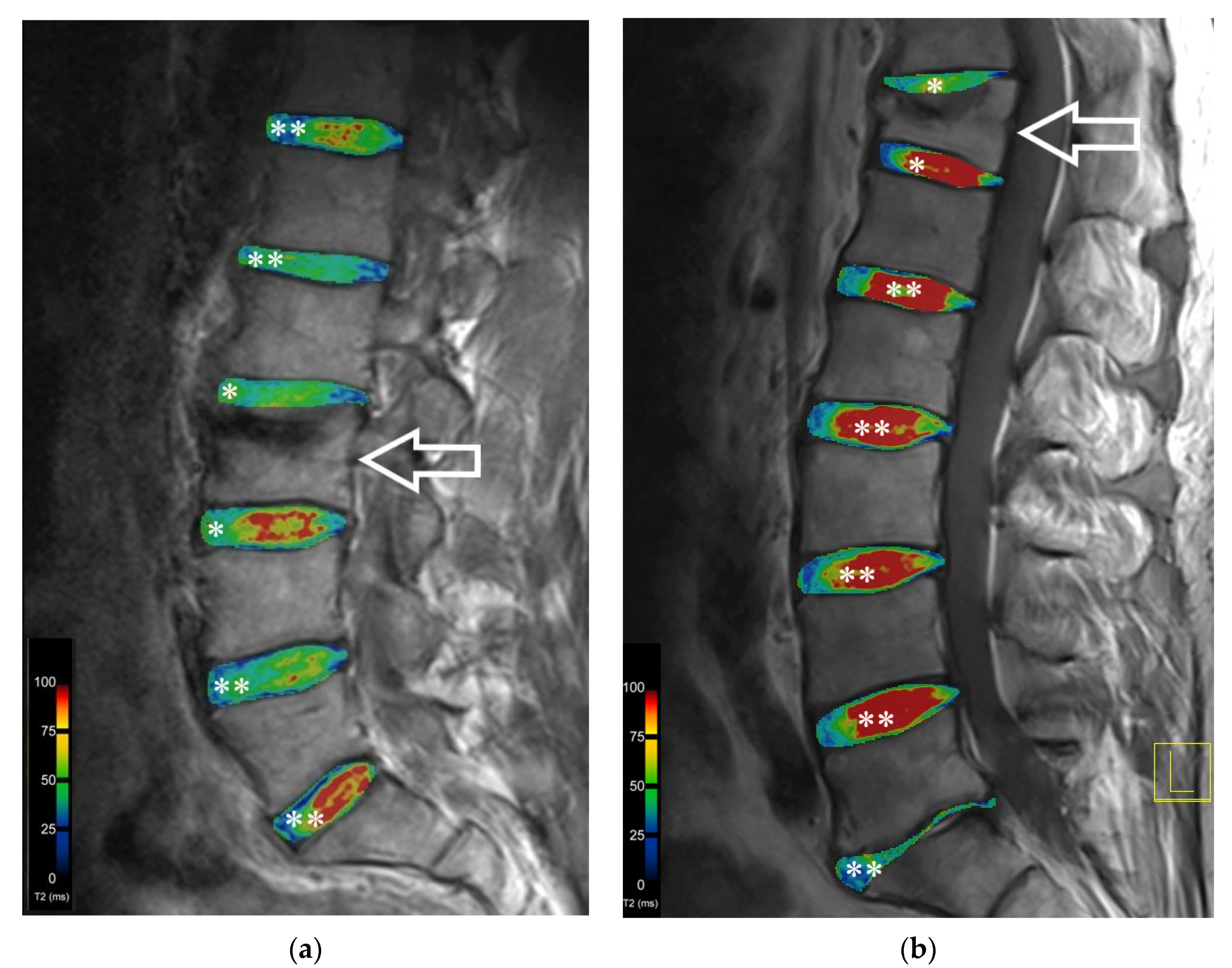
3.2. T2 Mapping
3.3. Quality of Life Analysis
3.3.1. 36-Item Short Form Survey
3.3.2. Oswestry Low Back Pain Disability Questionnaire and Disability Score
3.3.3. Numeric Rating Scale (NRS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner Res. 2007, 22, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Luca, D.L. The Global Demography of Aging: Facts, Explanations, Future. In Handbook of the Economics of Population Aging; Piggott, J., Woodland, A., Eds.; Elsevier B.V.: North-Holland, The Netherlands, 2016; Chapter 1; Volume 1, pp. 3–56. [Google Scholar]
- HealthQualityOntario. Vertebral Augmentation Involving Vertebroplasty or Kyphoplasty for Cancer-Related Vertebral Compression Fractures: A Systematic Review. Ont. Health Technol. Assess. Ser. 2016, 16, 1–202. [Google Scholar]
- Shayganfar, A.; Khodayi, M.; Ebrahimian, S.; Tabrizi, Z. Quantitative diagnosis of osteoporosis using lumbar spine signal intensity in magnetic resonance imaging. Br. J. Radiol. 2019, 92, 20180774. [Google Scholar] [CrossRef]
- Filippiadis, D.K.; Marcia, S.; Masala, S.; Deschamps, F.; Kelekis, A. Percutaneous Vertebroplasty and Kyphoplasty: Current Status, New Developments and Old Controversies. Cardiovasc. Interv. Radiol. 2017, 40, 1815–1823. [Google Scholar] [CrossRef]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsoumakidou, G.; Too, C.W.; Koch, G.; Caudrelier, J.; Cazzato, R.L.; Garnon, J.; Gangi, A. CIRSE Guidelines on Percutaneous Vertebral Augmentation. Cardiovasc. Interv. Radiol. 2017, 40, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Chandra, R.V.; Maingard, J.; Asadi, H.; Slater, L.A.; Mazwi, T.L.; Marcia, S.; Barr, J.; Hirsch, J.A. Vertebroplasty and Kyphoplasty for Osteoporotic Vertebral Fractures: What Are the Latest Data? AJNR. Am. J. Neuroradiol. 2018, 39, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Sribastav, S.S.; Ye, F.; Yang, C.; Wang, J.; Liu, H.; Zheng, Z. Comparison of Percutaneous Vertebroplasty and Balloon Kyphoplasty for the Treatment of Single Level Vertebral Compression Fractures: A Meta-analysis of the Literature. Pain Phys. 2015, 18, 209–222. [Google Scholar]
- Liu, J.-T.; Li, C.-S.; Chang, C.-S.; Liao, W.-J. Long-term follow-up study of osteoporotic vertebral compression fracture treated using balloon kyphoplasty and vertebroplasty. J. Neurosurg. Spine 2015, 23, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Zitka, R.; Gakhar, H.; Clamp, J.; Bommireddy, R.; Klezl, Z. Kyphoplasty Augmentation in Thoracolumbar Spine-Clinical Outcomes after 2 Years. Acta Chirurgiae Orthop. Traumatol. Cechoslov. 2019, 86, 188–192. [Google Scholar]
- König, M.A.; Panzer, S.; Schulz, J.; Bierschneider, M.; Boszczyk, B.M. Magnetic resonance imaging changes of intervertebral discs after kyphoplasty. Eur. Spine J. 2015, 24, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Michelini, G.; Corridore, A.; Torlone, S.; Bruno, F.; Marsecano, C.; Capasso, R.; Caranci, F.; Barile, A.; Masciocchi, C.; Splendiani, A. Dynamic MRI in the evaluation of the spine: State of the art. Acta Bio-Med. Atenei Parm. 2018, 89, 89–101. [Google Scholar] [CrossRef]
- Colosimo, C.; Gaudino, S.; Alexandre, A.M. Imaging in degenerative spine pathology. Acta Neurochir. Suppl. 2011, 108, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Pabst, D.M.C. Magnetresonanz-Tomographie. Available online: https://www.ukgm.de/ugm_2/deu/umr_rdi/Teaser/Grundlagen_der_Magnetresonanztomographie_MRT_2013.pdf (accessed on 21 September 2020).
- Stelzeneder, D.; Welsch, G.H.; Kovács, B.K.; Goed, S.; Paternostro-Sluga, T.; Vlychou, M.; Friedrich, K.; Mamisch, T.C.; Trattnig, S. Quantitative T2 evaluation at 3.0T compared to morphological grading of the lumbar intervertebral disc: A standardized evaluation approach in patients with low back pain. Eur. J. Radiol. 2012, 81, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Hesper, T.; Hosalkar, H.S.; Bittersohl, D.; Welsch, G.H.; Krauspe, R.; Zilkens, C.; Bittersohl, B. T2* mapping for articular cartilage assessment: Principles, current applications, and future prospects. Skelet. Radiol. 2014, 43, 1429–1445. [Google Scholar] [CrossRef]
- Marano, M.; Vespasiani Gentilucci, U.; Altamura, C.; Siotto, M.; Squitti, R.; Bucossi, S.; Quintiliani, L.; Migliore, S.; Greco, F.; Scarciolla, L.; et al. Altered metal metabolism in patients with HCV-related cirrhosis and hepatic encephalopathy. Metab. Brain Dis. 2015, 30, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Berton, A.; Longo, U.G.; Candela, V.; Greco, F.; Martina, F.M.; Quattrocchi, C.C.; Denaro, V. Quantitative Evaluation of Meniscal Healing Process of Degenerative Meniscus Lesions Treated with Hyaluronic Acid: A Clinical and MRI Study. J. Clin. Med. 2020, 9, 2280. [Google Scholar] [CrossRef]
- Schenk, H.; Simon, D.; Waldenmeier, L.; Evers, C.; Janka, R.; Welsch, G.H.; Pachowsky, M.L. Regions at Risk in the Knee Joint of Young Professional Soccer Players: Longitudinal Evaluation of Early Cartilage Degeneration by Quantitative T2 Mapping in 3 T MRI. Cartilage 2021, 13, 595s–603s. [Google Scholar] [CrossRef]
- Welsch, G.H.; Apprich, S.; Zbyn, S.; Mamisch, T.C.; Mlynarik, V.; Scheffler, K.; Bieri, O.; Trattnig, S. Biochemical (T2, T2* and magnetisation transfer ratio) MRI of knee cartilage: Feasibility at ultra-high field (7T) compared with high field (3T) strength. Eur. Radiol. 2011, 21, 1136–1143. [Google Scholar] [CrossRef]
- Stelzeneder, D.; Kovács, B.K.; Goed, S.; Welsch, G.H.; Hirschfeld, C.; Paternostro-Sluga, T.; Friedrich, K.M.; Mamisch, T.C.; Trattnig, S. Effect of short-term unloading on T2 relaxation time in the lumbar intervertebral disc—in vivo magnetic resonance imaging study at 3.0 tesla. Spine J. 2012, 12, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Pachowsky, M.L.; Kleyer, A.; Wegener, L.; Langenbach, A.; Simon, D.; Janka, R.; May, M.; Welsch, G.H. Quantitative T2 Mapping Shows Increased Degeneration in Adjacent Intervertebral Discs Following Kyphoplasty. Cartilage 2020, 11, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Schnake, K.J.; Blattert, T.R.; Hahn, P.; Franck, A.; Hartmann, F.; Ullrich, B.; Verheyden, A.; Mörk, S.; Zimmermann, V.; Gonschorek, O.; et al. Classification of Osteoporotic Thoracolumbar Spine Fractures: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Glob. Spine J. 2018, 8, 46s–49s. [Google Scholar] [CrossRef] [PubMed]
- Grevitt, M.; Khazim, R.; Webb, J.; Mulholland, R.; Shepperd, J. The short form-36 health survey questionnaire in spine surgery. J. Bone Jt. Surg. Br. Vol. 1997, 79, 48–52. [Google Scholar] [CrossRef]
- Ellert, U.; Kurth, B.-M. Methodische Betrachtungen zu den Summenscores des SF-36 anhand der erwachsenen bundesdeutschen Bevölkerung. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2004, 47, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smeets, R.; Köke, A.; Lin, C.-W.; Ferreira, M.; Demoulin, C. Measures of function in low back pain/disorders: Low Back Pain Rating Scale (LBPRS), Oswestry Disability Index (ODI), Progressive Isoinertial Lifting Evaluation (PILE), Quebec Back Pain Disability Scale (QBPDS), and Roland-Morris Disability Questionnaire (RDQ). Arthritis Care Res. 2011, 63, S158–S173. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [Green Version]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Huang, L.; Liu, Y.; Ding, Y.; Wu, X.; Zhang, N.; Lai, Q.; Zeng, X.; Wan, Z.; Dai, M.; Zhang, B. Quantitative evaluation of lumbar intervertebral disc degeneration by axial T2∗ mapping. Medicine 2017, 96, e9393. [Google Scholar] [CrossRef]
- Müller-Lutz, A.; Schleich, C.; Schmitt, B.; Antoch, G.; Matuschke, F.; Quentin, M.; Wittsack, H.J.; Miese, F. Gender, BMI and T2 dependencies of glycosaminoglycan chemical exchange saturation transfer in intervertebral discs. Magn. Reson. Imaging 2016, 34, 271–275. [Google Scholar] [CrossRef]
- Silagi, E.S.; Shapiro, I.M.; Risbud, M.V. Glycosaminoglycan synthesis in the nucleus pulposus: Dysregulation and the pathogenesis of disc degeneration. Matrix biol. J. Int. Soc. Matrix Biol. 2018, 71–72, 368–379. [Google Scholar] [CrossRef]
- Zhou, X.; Haudenschild, A.K.; Sherlock, B.E.; Hu, J.C.; Leach, J.K.; Athanasiou, K.A.; Marcu, L. Detection of glycosaminoglycan loss in articular cartilage by fluorescence lifetime imaging. J. Biomed. Opt. 2018, 23, 126002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haneder, S.; Ong, M.M.; Budjan, J.M.; Schmidt, R.; Konstandin, S.; Morelli, J.N.; Schad, L.R.; Schoenberg, S.O.; Kerl, U.H. 23Na-magnetic resonance imaging of the human lumbar vertebral discs: In vivo measurements at 3.0 T in healthy volunteers and patients with low back pain. Spine J. Off. J. N. Am. Spine Soc. 2014, 14, 1343–1350. [Google Scholar] [CrossRef]
- Hoshino, M.; Takahashi, S.; Yasuda, H.; Terai, H.; Watanabe, K.; Hayashi, K.; Tsujio, T.; Kono, H.; Suzuki, A.; Tamai, K.; et al. Balloon Kyphoplasty Versus Conservative Treatment for Acute Osteoporotic Vertebral Fractures With Poor Prognostic Factors: Propensity Score Matched Analysis Using Data From Two Prospective Multicenter Studies. Spine 2019, 44, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Dario, A.B.; Ferreira, M.L.; Refshauge, K.M.; Lima, T.S.; Ordoñana, J.R.; Ferreira, P.H. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: A systematic review of twin studies. Spine J. 2015, 15, 1106–1117. [Google Scholar] [CrossRef] [PubMed]
- Hangai, M.; Kaneoka, K.; Kuno, S.; Hinotsu, S.; Sakane, M.; Mamizuka, N.; Sakai, S.; Ochiai, N. Factors associated with lumbar intervertebral disc degeneration in the elderly. Spine J. Off. J. N. Am. Spine Soc. 2008, 8, 732–740. [Google Scholar] [CrossRef] [Green Version]
- Liuke, M.; Solovieva, S.; Lamminen, A.; Luoma, K.; Leino-Arjas, P.; Luukkonen, R.; Riihimäki, H. Disc degeneration of the lumbar spine in relation to overweight. Int. J. Obes. 2005, 29, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Samartzis, D.; Karppinen, J.; Mok, F.; Fong, D.Y.; Luk, K.D.; Cheung, K.M. A population-based study of juvenile disc degeneration and its association with overweight and obesity, low back pain, and diminished functional status. J. Bone Jt. Surg. Am. 2011, 93, 662–670. [Google Scholar] [CrossRef] [Green Version]
- Ellingson, A.M.; Mehta, H.; Polly, D.W.; Ellermann, J.; Nuckley, D.J. Disc degeneration assessed by quantitative T2* (T2 star) correlated with functional lumbar mechanics. Spine 2013, 38, E1533–E1540. [Google Scholar] [CrossRef] [Green Version]
- Welsch, G.H.; Trattnig, S.; Paternostro-Sluga, T.; Bohndorf, K.; Goed, S.; Stelzeneder, D.; Mamisch, T.C. Parametric T2 and T2* mapping techniques to visualize intervertebral disc degeneration in patients with low back pain: Initial results on the clinical use of 3.0 Tesla MRI. Skelet. Radiol. 2011, 40, 543–551. [Google Scholar] [CrossRef]
- Middendorp, M.; Vogl, T.J.; Kollias, K.; Kafchitsas, K.; Khan, M.F.; Maataoui, A. Association between intervertebral disc degeneration and the Oswestry Disability Index. J. Back Musculoskelet. Rehabilit. 2017, 30, 819–823. [Google Scholar] [CrossRef]
- Beall, D.P.; Chambers, M.R.; Thomas, S.; Amburgy, J.; Webb, J.R., Jr.; Goodman, B.S.; Datta, D.K.; Easton, R.W.; Linville, D., 2nd; Talati, S.; et al. Prospective and Multicenter Evaluation of Outcomes for Quality of Life and Activities of Daily Living for Balloon Kyphoplasty in the Treatment of Vertebral Compression Fractures: The EVOLVE Trial. Neurosurgery 2019, 84, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Dohm, M.; Black, C.M.; Dacre, A.; Tillman, J.B.; Fueredi, G. A randomized trial comparing balloon kyphoplasty and vertebroplasty for vertebral compression fractures due to osteoporosis. AJNR Am. J. Neuroradiol. 2014, 35, 2227–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.R.; Ehrhardt, K.P.; Ripoll, J.G.; Sharma, B.; Padnos, I.W.; Kaye, R.J.; Kaye, A.D. Pain in the Elderly. Curr. Pain Headache Rep. 2016, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, J.; Allaire, B.; Fein, P.M.; Lu, D.; Jarraya, M.; Guermazi, A.; Demissie, S.; Samelson, E.J.; Bouxsein, M.L.; Morgan, E.F. Correspondence between bone mineral density and intervertebral disc degeneration across age and sex. Arch. Osteoporos. 2018, 13, 123. [Google Scholar] [CrossRef]
- De Schepper, E.I.; Damen, J.; van Meurs, J.B.; Ginai, A.Z.; Popham, M.; Hofman, A.; Koes, B.W.; Bierma-Zeinstra, S.M. The association between lumbar disc degeneration and low back pain: The influence of age, gender, and individual radiographic features. Spine 2010, 35, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Pachowsky, M.L.; Werner, S.; Marlovits, S.; Stelzeneder, D.; Renner, N.; Trattnig, S.; Welsch, G.H. 3D-isotropic high-resolution morphological imaging and quantitative T2 mapping as biomarkers for gender related differences after matrix-associated autologous chondrocyte transplantation (MACT). J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2014, 32, 1341–1348. [Google Scholar] [CrossRef]
- Song, X.X.; Yu, Y.J.; Li, X.F.; Liu, Z.D.; Yu, B.W.; Guo, Z. Estrogen receptor expression in lumbar intervertebral disc of the elderly: Gender- and degeneration degree-related variations. Jt. Bone Spine 2014, 81, 250–253. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Segment | Adjacent Vertebral Disc (ms) | Nonadjacent Vertebral Disc (ms) | p-Value Difference | |
|---|---|---|---|---|
| ROI 2 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 74.59 ± 44.99 52.01 ± 15.10 51.66 ± 12.54 48.05 ± 12.86 54.02 ± 16.73 53.01 ± 12.75 56.38 ± 14.89 | 62.78 ± 21.20 42.38 ± 7.75 60.15 ± 40.61 63.42 ± 42.67 57.71 ± 15.95 54.82 ± 12.00 56.19 ± 15.08 | 0.920 0.001 0.662 0.001 0.251 0.465 0.991 |
| ROI 3 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 92.81 ± 70.18 62.56 ± 26.75 58.48 ± 14.11 53.12 ± 12.88 56.60 ± 10.70 55.76 ± 9.12 65.83 ± 31.12 | 66.10 ± 19.49 55.77 ± 11.46 65.72 ± 31.99 71.85 ± 32.78 65.74 ± 16.39 62.14 ± 14.75 71.44 ± 27.13 | 0.533 0.514 0.610 0.001 0.031 0.139 0.262 |
| ROI 4 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 101.87 ± 64.60 64.41 ± 21.02 58.41 ± 12.19 55.99 ± 12.23 53.84 ± 10.75 55.20 ± 7.29 56.46 ± 20.06 | 68.63 ± 19.62 58.59 ± 14.01 63.71 ± 19.48 74.21 ± 35.20 68.12 ± 22.92 63.67 ± 15.41 68.25 ± 22.32 | 0.262 0.391 0.456 0.002 0.008 0.069 0.052 |
| ROI 5 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 108.07 ± 97.42 59.69 ± 18.95 50.54 ± 11.65 48.28 ± 9.51 49.50 ± 9.55 54.58 ± 4.65 55.28 ± 16.15 | 69.88 ± 14.93 54.83 ± 10.91 55.10 ± 13.05 59.61 ± 12.78 57.04 ± 11.68 57.56 ± 10.43 65.86 ± 17.65 | 0.516 0.514 0.169 0.000 0.007 0.388 0.075 |
| Segment | Adjacent Vertebral Disc (ms) | Nonadjacent Vertebral Disc (ms) | p-Value Difference | |
|---|---|---|---|---|
| ROI 1 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 80.75 ± 48.62 59.99 ± 45.25 51.27 ± 13.51 53.81 ± 14.73 56.33 ± 29.40 53.65 ± 14.78 49.36 ± 8.40 | 67.04 ± 22.11 45.33 ± 15.43 55.43 ± 24.11 62.89 ± 37.41 68.19 ± 47.84 52.74 ± 18.70 51.63 ± 19.31 | 0.867 0.001 0.882 0.646 0.063 0.516 0.829 |
| ROI 6 | TH11/TH12 TH12/L1 L1/L2 L2/L3 L3/L4 L4/L5 L5/S1 | 109.69 ± 113.61 69.80 ± 42.13 58.04 ± 21.98 48.50 ± 12.32 49.31 ± 12.39 60.05 ± 17.75 64.31 ± 21.69 | 73.32 ± 27.57 70.34 ± 75.77 54.87 ± 25.69 56.93 ± 30.46 60.18 ± 39.46 54.68 ± 17.43 70.75 ± 56.65 | 0.899 0.044 0.416 0.542 0.324 0.232 0.866 |
| SF-36 Subscale | Minimum | Maximum | Mean Value | SD |
|---|---|---|---|---|
| VT | 15 | 100 | 56.25 | 24.60 |
| PF | 20 | 100 | 50.00 | 27.74 |
| BP | 33 | 100 | 59.25 | 23.41 |
| GH | 30 | 95 | 56.75 | 17.72 |
| RP | 0 | 100 | 50.00 | 46.60 |
| RE | 0 | 100 | 78.33 | 36.31 |
| SF | 13 | 100 | 80.62 | 27.35 |
| MH | 48 | 100 | 75.20 | 15.82 |
| PCS | 33 | 70 | 50.00 | 10.77 |
| MCS | 29 | 61 | 50.00 | 8.97 |
| ODQ Subscale | n | Minimum | Maximum | Mean Value | SD |
|---|---|---|---|---|---|
| Pain intensity | 20 | 0 | 3 | 1.05 | 1.15 |
| Personal care | 20 | 0 | 2 | 0.60 | 0.598 |
| Lifting | 20 | 0 | 4 | 1.75 | 1.55 |
| Walking | 20 | 0 | 5 | 1.30 | 1.49 |
| Sitting | 20 | 0 | 5 | 1.10 | 1.37 |
| Standing | 20 | 0 | 4 | 1.85 | 1.57 |
| Sleeping | 20 | 0 | 3 | 0.40 | 0.75 |
| Sex life | 12 | 0 | 5 | 0.75 | 1.60 |
| Social life | 20 | 0 | 4 | 1.00 | 1.34 |
| Travelling | 20 | 0 | 5 | 1.45 | 1.79 |
| ODI | 20 | 0 | 73.33 | 28.09 | 22.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wegener, L.C.; Werner, F.; Kleyer, A.; Simon, D.; Uder, M.; Janka, R.; Trattnig, S.; Welsch, G.H.; Pachowsky, M.L. Changes in T2 Relaxation Time Mapping of Intervertebral Discs Adjacent to Vertebrae after Kyphoplasty Correlate with the Physical Clinical Outcome of Patients. Diagnostics 2022, 12, 605. https://doi.org/10.3390/diagnostics12030605
Wegener LC, Werner F, Kleyer A, Simon D, Uder M, Janka R, Trattnig S, Welsch GH, Pachowsky ML. Changes in T2 Relaxation Time Mapping of Intervertebral Discs Adjacent to Vertebrae after Kyphoplasty Correlate with the Physical Clinical Outcome of Patients. Diagnostics. 2022; 12(3):605. https://doi.org/10.3390/diagnostics12030605
Chicago/Turabian StyleWegener, Lisa C., Felix Werner, Arnd Kleyer, David Simon, Michael Uder, Rolf Janka, Siegfried Trattnig, Goetz H. Welsch, and Milena L. Pachowsky. 2022. "Changes in T2 Relaxation Time Mapping of Intervertebral Discs Adjacent to Vertebrae after Kyphoplasty Correlate with the Physical Clinical Outcome of Patients" Diagnostics 12, no. 3: 605. https://doi.org/10.3390/diagnostics12030605