
Flow Cytometric Analysis of Macrophages and Cytokines Profile in the Bronchoalveolar Lavage Fluid in Patients with Lung Cancer
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Material
2.3. Cell Count and Flow Cytometry Analysis
2.4. Cytokines Concentration Measurement
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristic of Study Group
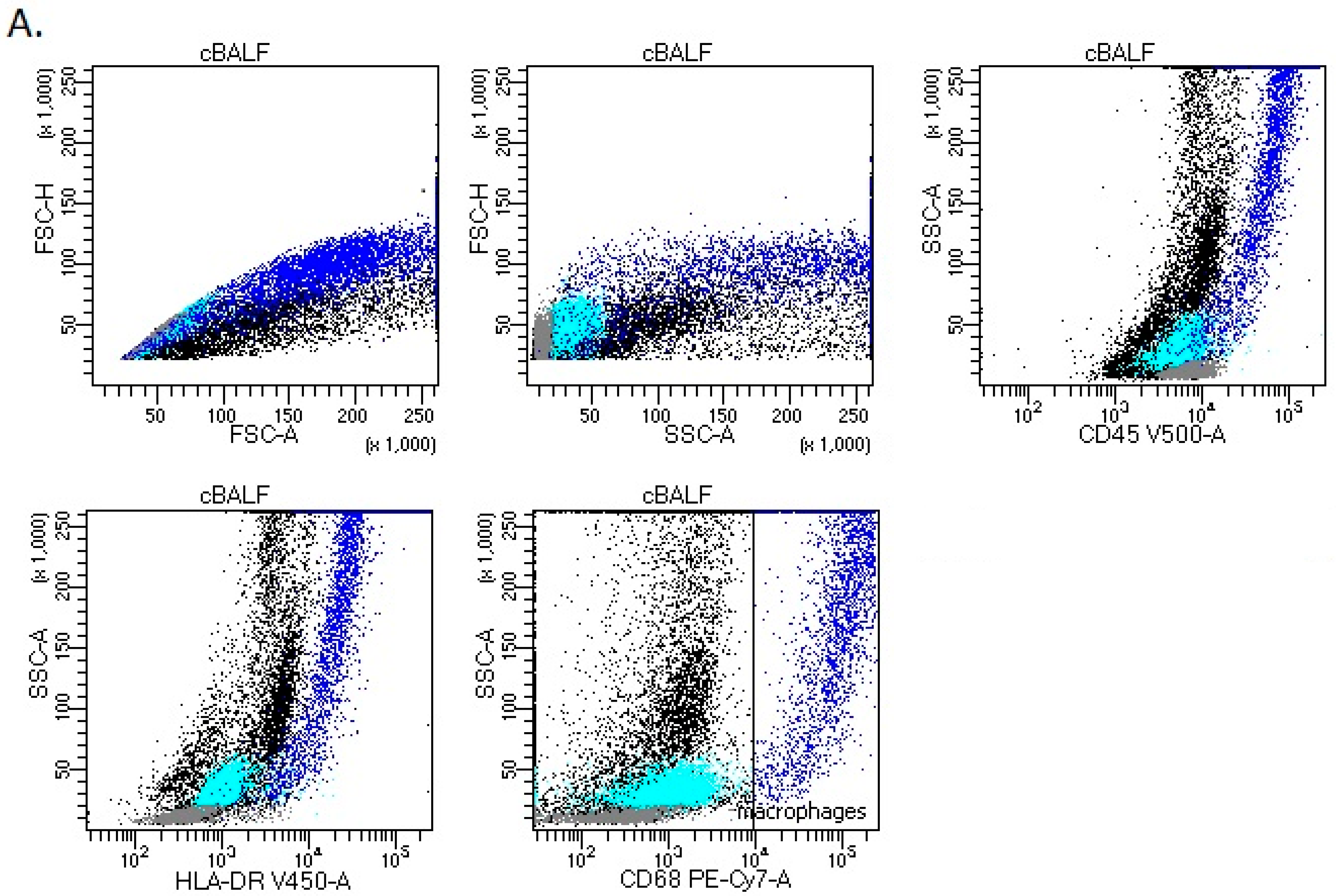
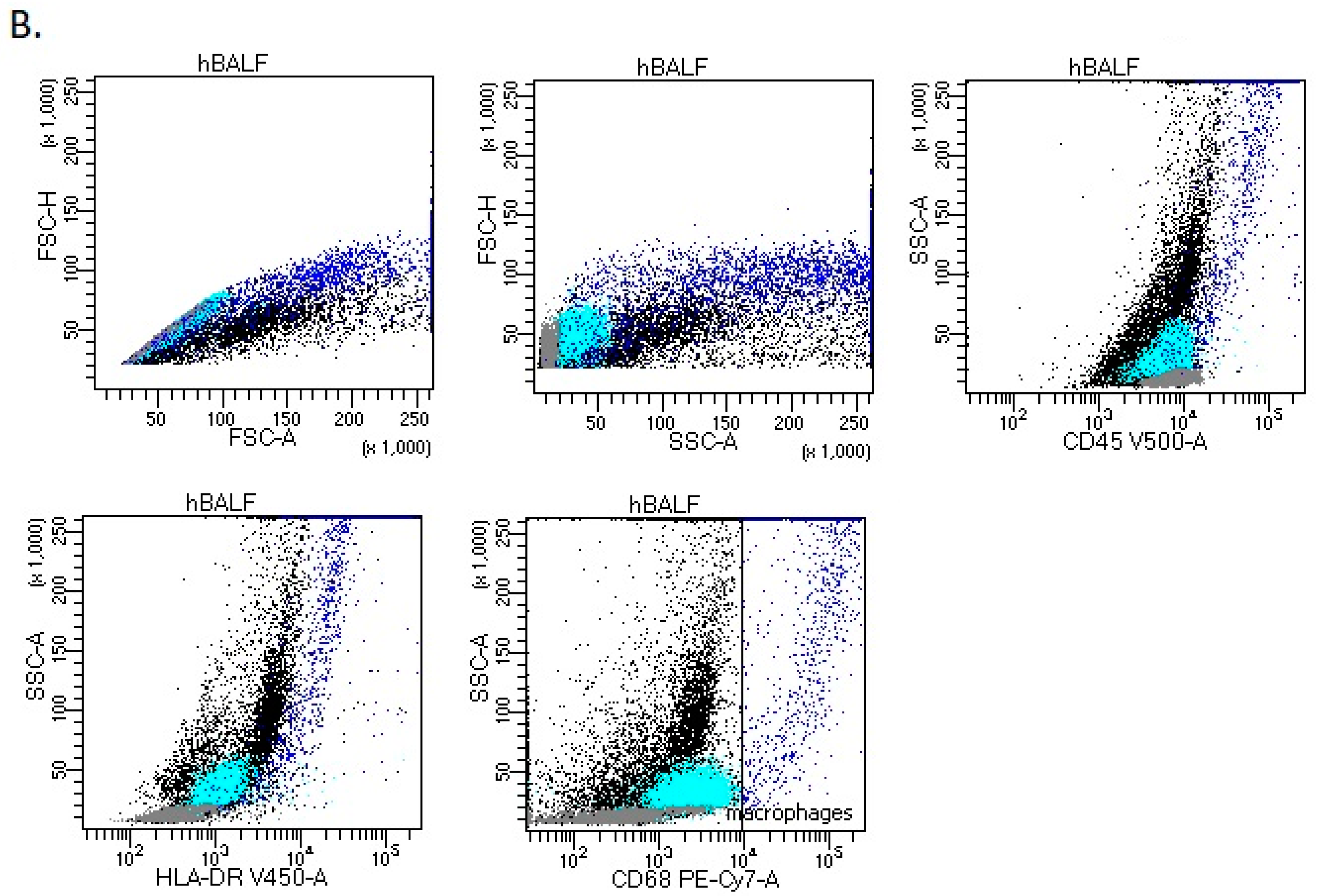
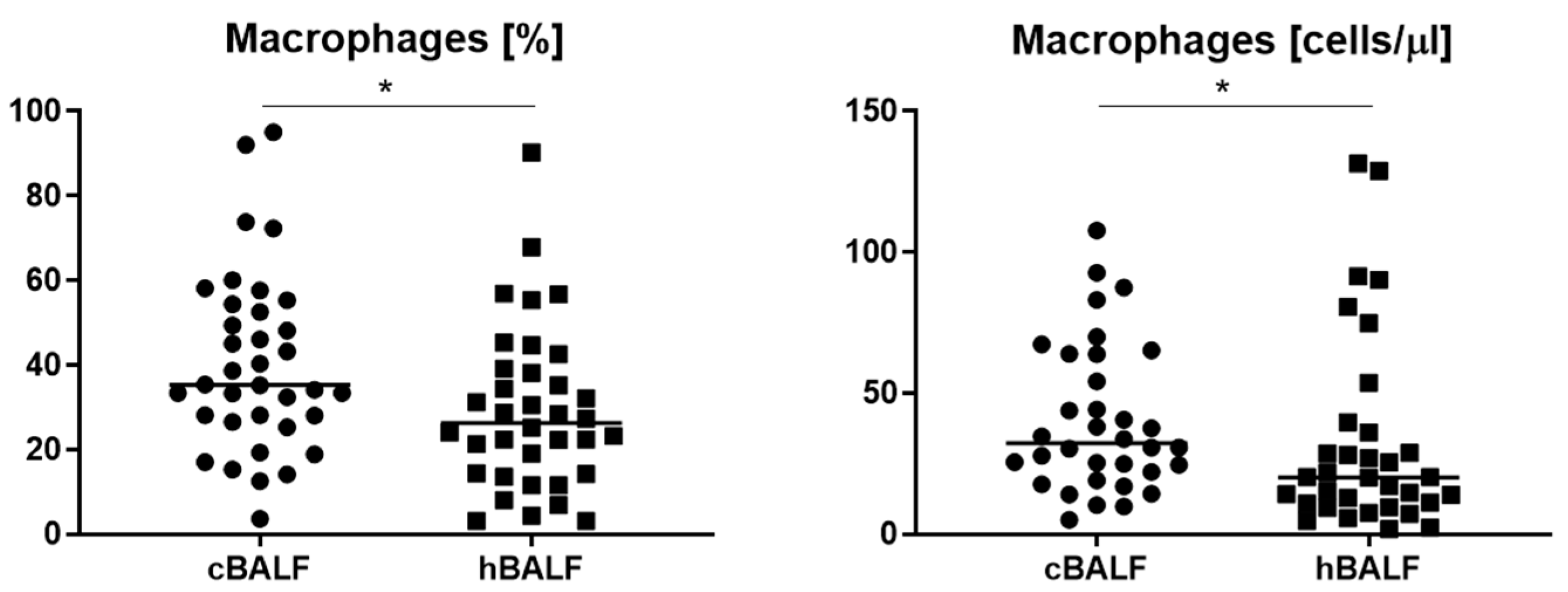
3.2. Leukocytes Subpopulation in cBALF and hBALF
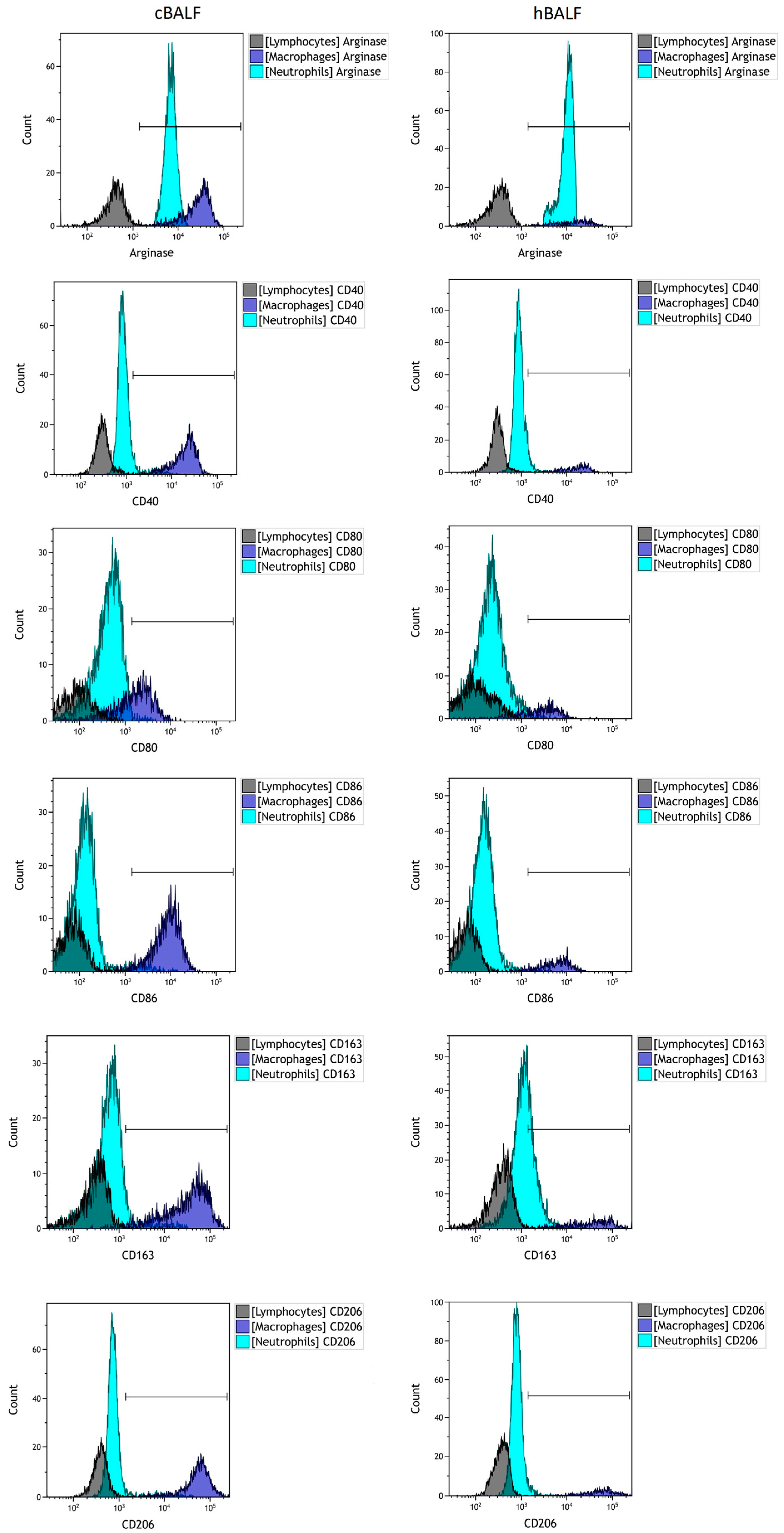
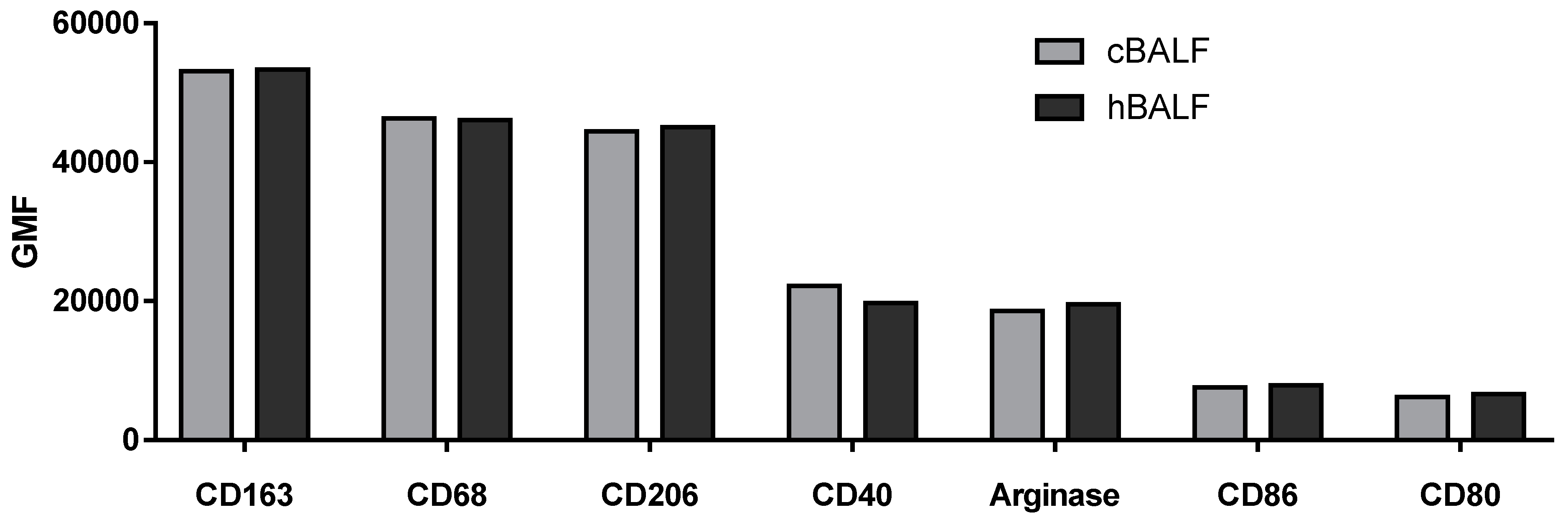
3.3. Macrophages Phenotype in cBALF and hBALF
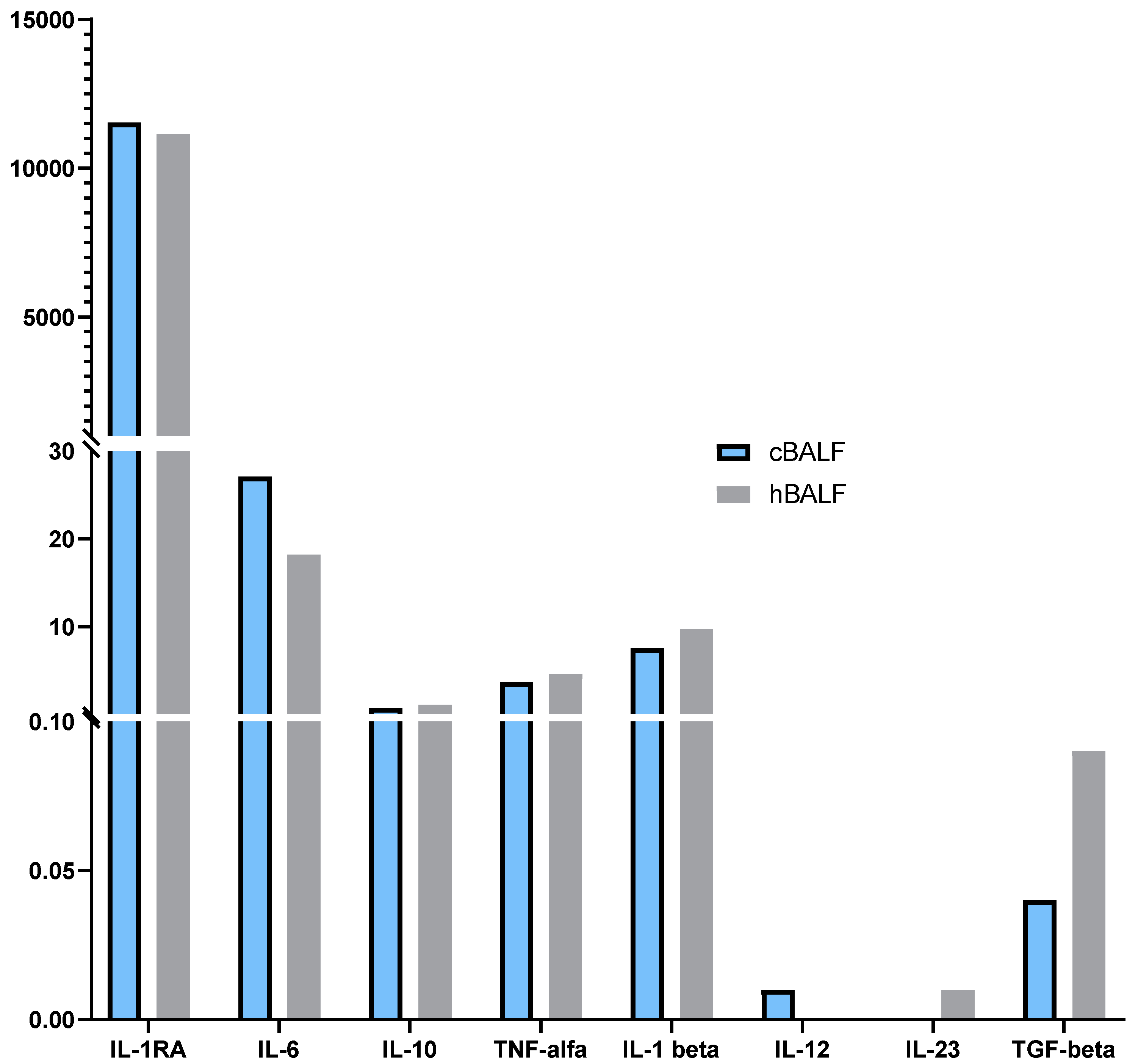
3.4. Cytokines Profile in cBALF and hBALF
4. Discussion
4.1. Macrophages Count in Bronchoalveolar Lavage Fluid
4.2. Usefulness of Macrophage Phenotype Assessment
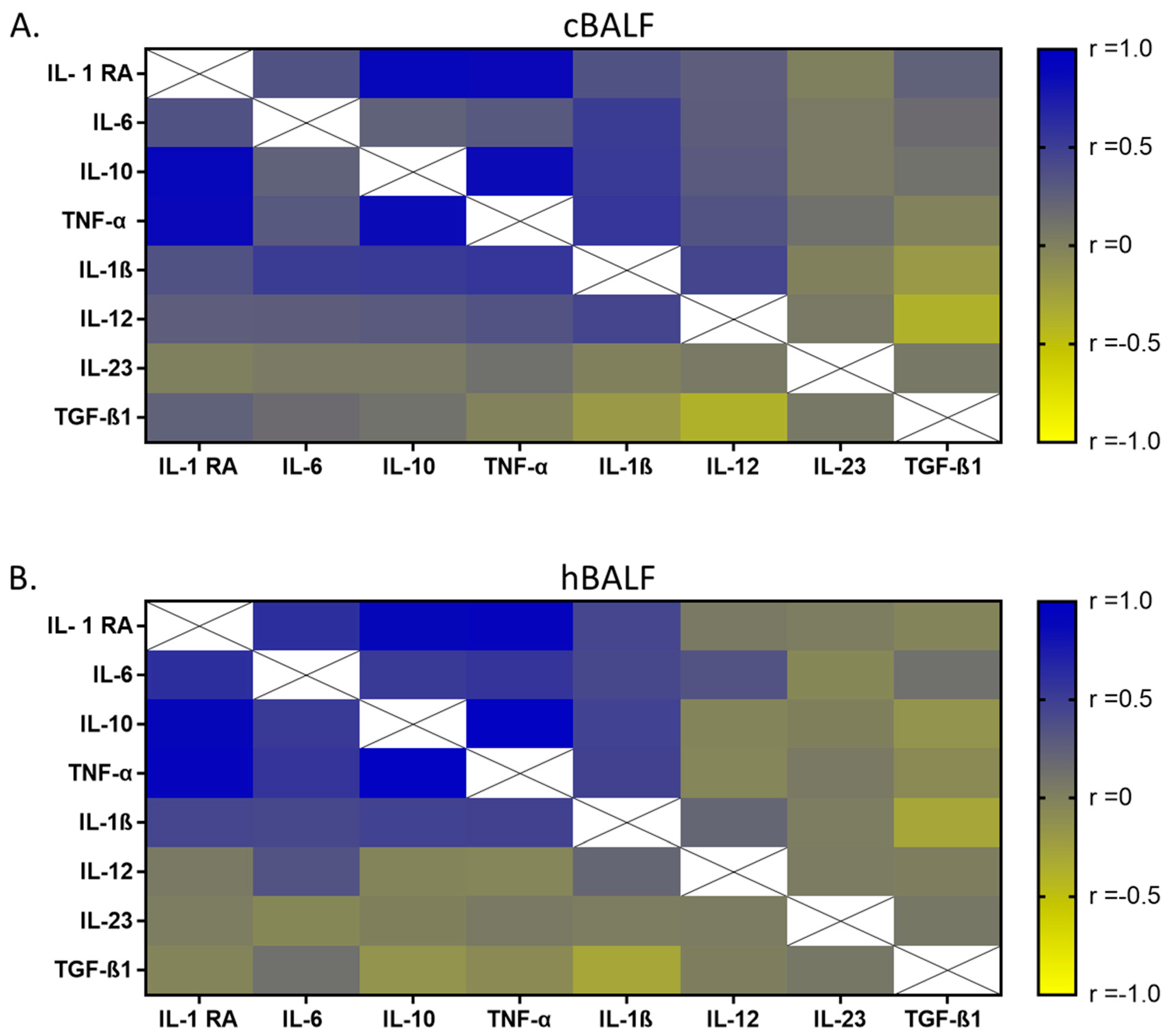
4.3. Cytokines Profile Correleted with Macrophages Phenotype
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Aga | Lung Segments | Diagnosis | Histological Type | Stage | TNM |
|---|---|---|---|---|---|---|---|
| 1 | m | 69 | B1-2L | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 2 | m | 73 | B6L | no cancer cells | - | - | - |
| 3 | m | 67 | B6L | NSCLC | squamous cell carcinoma | IB | pT2aN0 |
| 4 | f | 70 | B8L | NSCLC | adenocarcinoma | IB | pT2aN0M0 |
| 5 | m | 57 | B1R | NSCLC | Large cell neuroendocrine carcinoma | IIIA | pT4N0 |
| 6 | m | 84 | B3R | no cancer cells | - | - | - |
| 7 | m | 69 | B6L | NSCLC | adenocarcinoma | IA3 | pT1cN0 |
| 8 | f | 73 | B5L | NSCLC | squamous cell carcinoma | IA1 | pT1aN0Mx |
| 9 | f | 53 | B1-2L i B3L | NSCLC | adenocarcinoma | IIIA | pT1cN2 |
| 10 | m | 62 | B6L | metastatic cells | - | - | - |
| 11 | f | 61 | B8L | no cancer cells | - | - | - |
| 12 | f | 67 | B10L | NSCLC | squamous cell carcinoma | IIIB | pT4N2 |
| 13 | f | 62 | B6L | metastatic cells | - | - | - |
| 14 | f | 72 | B8,10R | no cancer cells | - | - | - |
| 15 | f | 63 | B5L | no continuity of diagnosis | - | - | - |
| 16 | m | 80 | B6L | no cancer cells | - | - | - |
| 17 | m | 72 | B2R | metastatic cells | - | - | - |
| 18 | f | 66 | B6R | NSCLC | Large cell neuroendocrine carcinoma | IIB | pT2aN1 |
| 19 | f | 72 | B1R | NSCLC | adenocarcinoma | IIIA | pT1aN2 |
| 20 | f | 68 | B6L | NSCLC | adenocarcinoma | IIB | pT2aN1 |
| 21 | f | 69 | B6L | NSCLC | adenocarcinoma | IB | pT2aN0Mx |
| 22 | f | 72 | B5L | no continuity of diagnosis | - | - | - |
| 23 | f | 73 | B9L/B8L | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 24 | m | 83 | B1-2L | NSCLC | adenocarcinoma | IB | pT2aN0M0 |
| 25 | m | 69 | B3R | NSCLC | adenocarcinoma-squamous cell carcinoma | IB | pT2aN0Mx |
| 26 | f | 46 | B10R | metastatic cells | - | - | - |
| 27 | m | 66 | B3L | no cancer cells | - | - | - |
| 28 | m | 80 | B6R | NSCLC | adenocarcinoma | IA3 | pT1cN0 |
| 29 | m | 65 | B9L | NSCLC | squamous cell carcinoma | IB | pT2aN0 |
| 30 | f | 73 | B3R | NSCLC | squamous cell carcinoma | IB | pT2aN0 |
| 31 | m | 66 | B3R | NSCLC | adenocarcinoma | IA2 | pT1bN0 |
| 32 | f | 77 | B3R | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 33 | m | 62 | B6R | carcinoid | - | - | - |
| 34 | m | 81 | B3R | no cancer cells | - | - | - |
| 35 | f | 63 | B2R | NSCLC | adenocarcinoma | IA2 | pT1bN0 |
| 36 | f | 73 | B3L | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 37 | f | 70 | B3L | NSCLC | adenocarcinoma | IA2 | pT1bN0 |
| 38 | f | 71 | B2R | NSCLC | squamous cell carcinoma | IA3 | PT1cN0M0 |
| 39 | m | 66 | B3R | NSCLC | squamous cell carcinoma | IA2 | pT1bN0 |
| 40 | m | 67 | B2R | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 41 | m | 72 | B1R | NSCLC | adenocarcinoma | IB | pT2aN0M0 |
| 42 | m | 69 | B9L | NSCLC | Large cell neuroendocrine carcinoma | IA3 | pT1cN0Mx |
| 43 | f | 72 | B5L | NSCLC | squamous cell carcinoma | IIB | pT2aN1Mx |
| 44 | m | 42 | B6L | no continuity of diagnosis | - | - | - |
| 45 | f | 62 | B3R | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 46 | m | 71 | B6L | NSCLC | squamous cell carcinoma | IIA | pT2bN0Mx |
| 47 | f | 82 | B3L | NSCLC | adenocarcinoma | IA2 | pT1bN0Mx |
| 48 | m | 71 | B6R | NSCLC | adenocarcinoma | IA3 | pT1cN0 |
| 49 | m | 66 | B1R | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 50 | f | 54 | B6 8 9 L | no cancer cells | - | - | - |
| 51 | m | 62 | B6L | no cancer cells | - | - | - |
| 52 | f | 68 | B3R | hamartoma | - | - | - |
| 53 | f | 71 | B3R | no continuity of diagnosis | - | - | - |
| 54 | m | 71 | B3R | no cancer cells | - | - | - |
| 55 | m | 72 | B9 B10R | NSCLC | adenocarcinoma | IB | pT2aN0 |
| 56 | m | 73 | B1R | NSCLC | adenocarcinoma | IA3 | pT1cN0Mx |
| 57 | m | 74 | B9 B10L | no cancer cells | - | - | - |
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Singh, P.; Ahmad, S.; Ahmad, T.; Dohare, R.; Almatroodi, S.A.; Alrumaihi, F.; Rahmani, A.H.; Syed, M.A. Comprehensive Integrative Analysis Reveals the Association of KLF4 with Macrophage Infiltration and Polarization in Lung Cancer Microenvironment. Cells 2021, 10, 2091. [Google Scholar] [CrossRef] [PubMed]
- Casal-Mourino, A.; Valdes, L.; Barros-Dios, J.M.; Ruano-Ravina, A. Lung cancer survival among never smokers. Cancer Lett. 2019, 451, 142–149. [Google Scholar] [CrossRef]
- Zugazagoitia, J.; Paz-Ares, L. Extensive-Stage Small-Cell Lung Cancer: First-Line and Second-Line Treatment Options. J. Clin. Oncol. 2022, 40, 671–680. [Google Scholar] [CrossRef]
- Ruiz-Cordero, R.; Devine, W.P. Targeted Therapy and Checkpoint Immunotherapy in Lung Cancer. Surg. Pathol. Clin. 2020, 13, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Remon, J.; Hellmann, M.D. First-Line Immunotherapy for Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Martin, E.M.; Mellows, T.W.P.; Clarke, J.; Ganesan, A.P.; Wood, O.; Cazaly, A.; Seumois, G.; Chee, S.J.; Alzetani, A.; King, E.V.; et al. M1(hot) tumor-associated macrophages boost tissue-resident memory T cells infiltration and survival in human lung cancer. J. Immunother. Cancer 2020, 8, e000778. [Google Scholar] [CrossRef]
- Neophytou, C.M.; Panagi, M.; Stylianopoulos, T.; Papageorgis, P. The Role of Tumor Microenvironment in Cancer Metastasis: Molecular Mechanisms and Therapeutic Opportunities. Cancers 2021, 13, 2053. [Google Scholar] [CrossRef]
- Dong, Y.; Wan, Z.; Gao, X.; Yang, G.; Liu, L. Reprogramming Immune Cells for Enhanced Cancer Immunotherapy: Targets and Strategies. Front. Immunol. 2021, 12, 609762. [Google Scholar] [CrossRef]
- Wang, S.; Liu, G.; Li, Y.; Pan, Y. Metabolic Reprogramming Induces Macrophage Polarization in the Tumor Microenvironment. Front. Immunol. 2022, 13, 840029. [Google Scholar] [CrossRef]
- Xu, F.; Wei, Y.; Tang, Z.; Liu, B.; Dong, J. Tumor-associated macrophages in lung cancer: Friend or foe? (Review). Mol. Med. Rep. 2020, 22, 4107–4115. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Geng, X.; Hou, J.; Wu, G. New insights into M1/M2 macrophages: Key modulators in cancer progression. Cancer Cell. Int. 2021, 21, 389. [Google Scholar] [CrossRef] [PubMed]
- Jayasingam, S.D.; Citartan, M.; Thang, T.H.; Mat Zin, A.A.; Ang, K.C.; Ch’ng, E.S. Evaluating the Polarization of Tumor-Associated Macrophages Into M1 and M2 Phenotypes in Human Cancer Tissue: Technicalities and Challenges in Routine Clinical Practice. Front. Oncol. 2019, 9, 1512. [Google Scholar] [CrossRef]
- Lin, Y.; Xu, J.; Lan, H. Tumor-associated macrophages in tumor metastasis: Biological roles and clinical therapeutic applications. J. Hematol. Oncol. 2019, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Yu, Y.; Wang, X.; Zhang, T. Tumor-Associated Macrophages in Tumor Immunity. Front. Immunol. 2020, 11, 583084. [Google Scholar] [CrossRef] [PubMed]
- Okeke, E.B.; Uzonna, J.E. The Pivotal Role of Regulatory T Cells in the Regulation of Innate Immune Cells. Front. Immunol. 2019, 10, 680. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, K.A.; Amici, S.A.; Webb, L.M.; de Ruiz-Rosado, J.D.; Popovich, P.G.; Partida-Sanchez, S.; Guerau-de-Arellano, M. Novel Markers to Delineate Murine M1 and M2 Macrophages. PLoS ONE 2015, 10, e0145342. [Google Scholar] [CrossRef]
- Kong, X.; Zhu, M.; Wang, Z.; Xu, Z.; Shao, J. Characteristics and clinical significance of CD163+/CD206+M2 mono-macrophage in the bladder cancer microenvironment. Turk. J. Biol. 2021, 45, 624–632. [Google Scholar] [CrossRef]
- Juhas, U.; Ryba-Stanislawowska, M.; Szargiej, P.; Mysliwska, J. Different pathways of macrophage activation and polarization. Postepy Hig. Med. Dosw. 2015, 69, 496–502. [Google Scholar] [CrossRef]
- Locati, M.; Curtale, G.; Mantovani, A. Diversity, Mechanisms, and Significance of Macrophage Plasticity. Annu. Rev. Pathol. 2020, 15, 123–147. [Google Scholar] [CrossRef]
- Kashfi, K.; Kannikal, J.; Nath, N. Macrophage Reprogramming and Cancer Therapeutics: Role of iNOS-Derived NO. Cells 2021, 10, 3194. [Google Scholar] [CrossRef] [PubMed]
- Sharifiaghdam, M.; Shaabani, E.; Faridi-Majidi, R.; De Smedt, S.C.; Braeckmans, K.; Fraire, J.C. Macrophages as a therapeutic target to promote diabetic wound healing. Mol. Ther. 2022, 30, 2891–2908. [Google Scholar] [CrossRef] [PubMed]
- Domagala-Kulawik, J.; Raniszewska, A. How to evaluate the immune status of lung cancer patients before immunotherapy. Breathe 2017, 13, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Osinska, I.; Wolosz, D.; Domagala-Kulawik, J. Association between M1 and M2 macrophages in bronchoalveolar lavage fluid and tobacco smoking in patients with sarcoidosis. Pol. Arch. Med. Wewn. 2014, 124, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Grunewaldt, A.; Hugel, C.; Hermann, E.; Wagner, T.O. Possible Significance of Bronchoalveolar Lavage Cytology at Initial Diagnosis and Follow-up of Lung Cancer. Pneumologie 2017, 71, 106–110. [Google Scholar] [CrossRef]
- Osinska, I.; Stelmaszczyk-Emmel, A.; Polubiec-Kownacka, M.; Dziedzic, D.; Domagala-Kulawik, J. CD4+/CD25(high)/FoxP3+/CD127-regulatory T cells in bronchoalveolar lavage fluid of lung cancer patients. Hum. Immunol. 2016, 77, 912–915. [Google Scholar] [CrossRef]
- Domagala-Kulawik, J. The relevance of bronchoalveolar lavage fluid analysis for lung cancer patients. Expert Rev. Respir. Med. 2020, 14, 329–337. [Google Scholar] [CrossRef]
- Domagala-Kulawik, J.; Kwiecien, I.; Pankowski, J.; Pasieka-Lis, M.; Wolosz, D.; Zielinski, M. Elevated Foxp3/CD8 Ratio in Lung Adenocarcinoma Metastatic Lymph Nodes Resected by Transcervical Extended Mediastinal Lymphadenectomy. Biomed Res. Int. 2017, 2017, 5185034. [Google Scholar] [CrossRef]
- Osinska, I.; Domagala-Kulawik, J. Bronchoalveolar lavage in lung cancer–diagnostic value and assessment of the anti-cancer immune response. Postepy Hig. Med. Dosw. 2013, 67, 1119–1127. [Google Scholar] [CrossRef]
- Domagala-Kulawik, J.; Skirecki, T.; Maskey-Warzechowska, M.; Grubek-Jaworska, H.; Chazan, R. Bronchoalveolar lavage total cell count in interstitial lung diseases--does it matter? Inflammation 2012, 35, 803–809. [Google Scholar] [CrossRef]
- Detterbeck, F.C. The eighth edition TNM stage classification for lung cancer: What does it mean on main street? J. Thorac. Cardiovasc. Surg. 2018, 155, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Chcialowski, A.; Chorostowska-Wynimko, J.; Fal, A.; Pawlowicz, R.; Domagala-Kulawik, J. Recommendation of the Polish Respiratory Society for bronchoalveolar lavage (BAL) sampling, processing and analysis methods. Pneumonol. Alergol. Pol. 2011, 79, 75–89. [Google Scholar] [PubMed]
- Kwiecien, I.; Rutkowska, E.; Polubiec-Kownacka, M.; Raniszewska, A.; Rzepecki, P.; Domagala-Kulawik, J. Identification of PD-1 ligands: PD-L1 and PD-L2 on macrophages in lung cancer milieu by flow cytometry. Transl. Lung Cancer Res. 2021, 10, 1679–1689. [Google Scholar] [CrossRef] [PubMed]
- Lendeckel, U.; Venz, S.; Wolke, C. Macrophages: Shapes and functions. ChemTexts 2022, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Kwiecien, I.; Stelmaszczyk-Emmel, A.; Polubiec-Kownacka, M.; Dziedzic, D.; Domagala-Kulawik, J. Elevated regulatory T cells, surface and intracellular CTLA-4 expression and interleukin-17 in the lung cancer microenvironment in humans. Cancer Immunol. Immunother. 2017, 66, 161–170. [Google Scholar] [CrossRef]
- Kwiecien, I.; Skirecki, T.; Polubiec-Kownacka, M.; Raniszewska, A.; Domagala-Kulawik, J. Immunophenotype of T Cells Expressing Programmed Death-1 and Cytotoxic T Cell Antigen-4 in Early Lung Cancer: Local vs. Systemic Immune Response. Cancers 2019, 11, 567. [Google Scholar] [CrossRef]
- Domagala-Kulawik, J. Difficulties in the interpretation BALF and induced sputum cell smears. Pneumonol. Alergol. Pol. 2007, 75, 261–267. [Google Scholar]
- Wojtan, P.; Mierzejewski, M.; Osinska, I.; Domagala-Kulawik, J. Macrophage polarization in interstitial lung diseases. Cent. Eur. J. Immunol. 2016, 41, 159–164. [Google Scholar] [CrossRef]
- Mantovani, A.; Marchesi, F.; Malesci, A.; Laghi, L.; Allavena, P. Tumour-associated macrophages as treatment targets in oncology. Nat. Rev. Clin. Oncol. 2017, 14, 399–416. [Google Scholar] [CrossRef]
- Cassetta, L.; Pollard, J.W. Targeting macrophages: Therapeutic approaches in cancer. Nat. Rev. Drug. Discov. 2018, 17, 887–904. [Google Scholar] [CrossRef]
- Chen, L.; Li, Q.; Zhou, X.D.; Shi, Y.; Yang, L.; Xu, S.L.; Chen, C.; Cui, Y.H.; Zhang, X.; Bian, X.W. Increased pro-angiogenic factors, infiltrating neutrophils and CD163(+) macrophages in bronchoalveolar lavage fluid from lung cancer patients. Int. Immunopharmacol. 2014, 20, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Sarode, P.; Schaefer, M.B.; Grimminger, F.; Seeger, W.; Savai, R. Macrophage and Tumor Cell Cross-Talk Is Fundamental for Lung Tumor Progression: We Need to Talk. Front. Oncol. 2020, 10, 324. [Google Scholar] [CrossRef] [PubMed]
- Balazova, K.; Clevers, H.; Dost, A.F.M. The role of macrophages in non-small cell lung cancer and advancements in 3D co-cultures. Elife 2023, 12, e82998. [Google Scholar] [CrossRef]
- Li, J.; Li, J.; Wang, L.; Hao, J.; Wu, L.; Tao, H.; Zhang, S.; Cui, P.; Li, X.; Zhang, X.; et al. Alveolar macrophages in patients with non-small cell lung cancer. Int. J. Clin. Exp. Pathol. 2020, 13, 1867–1872. [Google Scholar] [PubMed]
- Aras, S.; Zaidi, M.R. TAMeless traitors: Macrophages in cancer progression and metastasis. Br. J. Cancer 2017, 117, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Sreejit, G.; Fleetwood, A.J.; Murphy, A.J.; Nagareddy, P.R. Origins and diversity of macrophages in health and disease. Clin. Transl. Immunol. 2020, 9, e1222. [Google Scholar] [CrossRef]
- Rodero, M.P.; Poupel, L.; Loyher, P.L.; Hamon, P.; Licata, F.; Pessel, C.; Hume, D.A.; Combadiere, C.; Boissonnas, A. Immune surveillance of the lung by migrating tissue monocytes. Elife 2015, 4, e07847. [Google Scholar] [CrossRef]
- Lin, M.W.; Yang, C.Y.; Kuo, S.W.; Wu, C.T.; Chang, Y.L.; Yang, P.C. The Prognostic Significance of pSTAT1 and CD163 Expressions in Surgically Resected Stage 1 Pulmonary Squamous Cell Carcinomas. Ann. Surg. Oncol. 2016, 23, 3071–3081. [Google Scholar] [CrossRef]
- Zhang, B.; Yao, G.; Zhang, Y.; Gao, J.; Yang, B.; Rao, Z.; Gao, J. M2-polarized tumor-associated macrophages are associated with poor prognoses resulting from accelerated lymphangiogenesis in lung adenocarcinoma. Clinics 2011, 66, 1879–1886. [Google Scholar] [CrossRef]
- Wynn, T.A.; Chawla, A.; Pollard, J.W. Macrophage biology in development, homeostasis and disease. Nature 2013, 496, 445–455. [Google Scholar] [CrossRef]
- Kowalski, B.; Valaperti, A.; Bezel, P.; Steiner, U.C.; Scholtze, D.; Wieser, S.; Vonow-Eisenring, M.; Widmer, A.; Kohler, M.; Franzen, D. Analysis of cytokines in serum and bronchoalveolar lavage fluid in patients with immune-checkpoint inhibitor-associated pneumonitis: A cross-sectional case-control study. J. Cancer Res. Clin. Oncol. 2022, 148, 1711–1720. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Charles, K.A.; Mantovani, A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell 2005, 7, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Pushalkar, S.; Hundeyin, M.; Daley, D.; Zambirinis, C.P.; Kurz, E.; Mishra, A.; Mohan, N.; Aykut, B.; Usyk, M.; Torres, L.E.; et al. The Pancreatic Cancer Microbiome Promotes Oncogenesis by Induction of Innate and Adaptive Immune Suppression. Cancer Discov. 2018, 8, 403–416. [Google Scholar] [CrossRef]
- Gonzalez-Santiago, A.E.; Mendoza-Topete, L.A.; Sanchez-Llamas, F.; Troyo-Sanroman, R.; Gurrola-Diaz, C.M. TGF-beta1 serum concentration as a complementary diagnostic biomarker of lung cancer: Establishment of a cut-point value. J. Clin. Lab. Anal. 2011, 25, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Ilonidis, G.; Parapanisiou, E.; Anogeianaki, A.; Giavazis, I.; Theofilogiannakos, E.K.; Tsekoura, P.; Kidonopoulou, K.; Trakatelli, C.; Polimenidis, Z.; Conti, P.; et al. Interleukin-1beta (IL-1 beta), interleukin 6 (IL-6) and tumor necrosis factor (TNF) in plasma and pleural fluid of pneumonia, lung cancer and tuberculous pleuritis. J. Biol. Regul. Homeost. Agents 2006, 20, 41–46. [Google Scholar]
- Chen, Z.; Xu, Z.; Sun, S.; Yu, Y.; Lv, D.; Cao, C.; Deng, Z. TGF-beta1, IL-6, and TNF-alpha in bronchoalveolar lavage fluid: Useful markers for lung cancer? Sci. Rep. 2014, 4, 5595. [Google Scholar] [CrossRef]
- Dinarello, C.A. The IL-1 family of cytokines and receptors in rheumatic diseases. Nat. Rev. Rheumatol. 2019, 15, 612–632. [Google Scholar] [CrossRef]
- Garon, E.B.; Chih-Hsin Yang, J.; Dubinett, S.M. The Role of Interleukin 1beta in the Pathogenesis of Lung Cancer. JTO Clin. Res. Rep. 2020, 1, 100001. [Google Scholar] [CrossRef]
- Gabay, C.; Lamacchia, C.; Palmer, G. IL-1 pathways in inflammation and human diseases. Nat. Rev. Rheumatol. 2010, 6, 232–241. [Google Scholar] [CrossRef]







| n | Age (Years) Mean ± SD | Sex m/f | Stage I/II/III/IV | Subtypes AD/SQCC/LCC/AS | |
|---|---|---|---|---|---|
| Cancer | 36 | 69.6 ± 5.9 | 18/18 | 28/4/4/0 | 23/9/3/1 |
| X no cancer cells | 11 | 70.7 ± 8.9 | 7/4 | - | - |
| X metastatic cells | 4 | 60.5 ± 10.8 | 2/2 | - | - |
| X no continuity of diagnosis | 4 | 62.0 ± 13.9 | 1/3 | - | - |
| X other diagnosis | 2 | 65.0 ± 5.5 | 1/1 | - | - |
| cBALF Median (Q1–Q3) | hBALF Median (Q1–Q3) | * p < 0.05 Mann–Whitney U Test) | |
|---|---|---|---|
| Lymhocytes [%] | 10.5 (7.0–17.3) | 13.7 (7.6–20.3) | 0.310101 |
| Lymhocytes [cells/µL] | 9.3 (4.2–15.8) | 10.4 (5.1–21.7) | 0.373551 |
| Lymphocytes T CD3+ [%] | 6.7 (3.5–12.0) | 10.6 (5.3–16.2) | 0.070508 |
| Lymphocytes T CD3+ [cells/µL] | 5.8 (2.5–10.0) | 6.8 (3.3–12.6) | 0.170413 |
| Lymphocytes T CD3+ CD4+ [%] | 1.8 (1.1–3.4) | 2.7 (1.3–4.8) | 0.142350 |
| Lymphocytes T CD3+ CD4+ [cells/µL] | 1.3 (0.8–3.2) | 2.1 (0.9–4.7) | 0.224691 |
| Lymphocytes T CD3+ CD8+ [%] | 3.9 (2.3–7.3) | 5.8 (2.9–11.0) | 0.183149 |
| Lymphocytes T CD3+ CD8+ [cells/µL] | 3.0 (1.7–6.3) | 0.1 (0.0–0.4) | 0.318384 |
| Ratio CD4/CD8 | 0.4 (0.2–1.1) | 0.6 (0.2–1.1) | 0.959834 |
| Lymphocytes B CD19+ [%] | 0.2 (0.0–0.4) | 0.1 (0.0–0.3) | 0.809831 |
| Lymphocytes B CD19+ [cells/µL] | 0.1 (0.0–0.3) | 0.1 (0.0–0.4) | 0.806871 |
| Natural killer (NK) cells [%] | 0.3 (0.0–1.5) | 0.4 (0.0–2.1) | 0.337706 |
| Natural killer (NK) cells [cells/µL] | 0.2 (0.0–1.6) | 0.6 (0.0–1.4) | 0.844019 |
| Neutrophils [%] | 44.4 (32.9–61.4) | 54.3 (45.6–70.4) | 0.070508 |
| Neutrophils [cells/µL] | 32.7 (17.6–66.3) | 45.1 (26.7–83.9) | 0.354547 |
| Macrophages [%] | 35.3 (27.3–53.5) | 26.3 (14.3–38.6) | * 0.013236 |
| Macrophages [cells/µL] | 32.2 (22.1–63.9) | 20.1 (10.8–36.1) | * 0.037162 |
| cBALF Median (Q1–Q3) | hBALF Median (Q1–Q3) | * p < 0.05 Mann–Whitney U Test) | |
|---|---|---|---|
| % CD206 | 97.1 (92.4–98.6) | 97.7 (90.2–99.4) | 0.888623 |
| % Arginase | 98.1 (95.9–99.2) | 98.2 (95.9–99.3) | 0.888623 |
| % CD163 | 96.3 (93.1–98.9) | 96.6 (92.6–99.3) | 0.934892 |
| % CD68 | 100.0 (100.0–100.0) | 100.0 (100.0–100.0) | 0.842726 |
| % CD86 | 96.8 (91.6–99.5) | 98.0 (91.7–99.6) | 0.648868 |
| % CD80 | 87.4 (78.5–94.1) | 87.4 (74.3–93.2) | 0.440583 |
| % CD40 | 98.8 (95.4–99.7) | 98.9 (95.9–99.8) | 0.879409 |
| GMF CD206 | 44,438 (28,803–66,189) | 45,054 (28,663–67,334) | 0.972072 |
| GMF Arginase | 18,646 (12,110–31,417) | 19,572 (10,700–38,081) | 0.717447 |
| GMF CD163 | 53,134 (34,389–72,585) | 53,340 (26,831–84,638) | 0.925616 |
| GMF CD68 | 46,344 (34,389–71,585) | 46,080 (30,582–77,574) | 0.916350 |
| GMF CD86 | 7564 (5070–12,816) | 7874 (5896–12,332) | 0.861031 |
| GMF CD80 | 6175 (4084–10,921) | 6631 (3268–10,683) | 0.833605 |
| GMF CD40 | 22,213 (11,152–28,548) | 19,702 (9424–31,888) | 0.761523 |
| Cytokines [pg/mL] | cBALF Median (Q1–Q3) | hBALF Median (Q1–Q3) | * p < 0.05 Mann–Whitney U Test) |
|---|---|---|---|
| IL-1 RA | 11,535.57 (6294.640–15,332.25) | 11,130.85 (7791.798–14,822.15) | 0.977679 |
| IL-6 | 27.09 (11.934–42.04) | 18.19 (9.569–37.08) | 0.299483 |
| IL-10 | 0.80 (0.531–1.34) | 1.12 (0.584–1.45) | 0.366820 |
| TNF-α | 3.69 (1.89–6.26) | 4.63 (2.159–6.13) | 0.835963 |
| IL-1β | 7.60 (3.00–15.80) | 9.76 (2.255–18.86) | 0.871082 |
| IL-12 | 0.01 (0.004–0.01) | 0.00 (0.004–0.01) | 0.085922 |
| IL-23 | 0.00 (0.00–0.01) | 0.01 (0.00–0.01) | 0.715991 |
| TGF-β | 0.04 (0.00–0.48) | 0.09 (0.00–0.27) | 0.758215 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiecień, I.; Rutkowska, E.; Raniszewska, A.; Rzeszotarska, A.; Polubiec-Kownacka, M.; Domagała-Kulawik, J.; Korsak, J.; Rzepecki, P. Flow Cytometric Analysis of Macrophages and Cytokines Profile in the Bronchoalveolar Lavage Fluid in Patients with Lung Cancer. Cancers 2023, 15, 5175. https://doi.org/10.3390/cancers15215175
Kwiecień I, Rutkowska E, Raniszewska A, Rzeszotarska A, Polubiec-Kownacka M, Domagała-Kulawik J, Korsak J, Rzepecki P. Flow Cytometric Analysis of Macrophages and Cytokines Profile in the Bronchoalveolar Lavage Fluid in Patients with Lung Cancer. Cancers. 2023; 15(21):5175. https://doi.org/10.3390/cancers15215175
Chicago/Turabian StyleKwiecień, Iwona, Elżbieta Rutkowska, Agata Raniszewska, Agnieszka Rzeszotarska, Małgorzata Polubiec-Kownacka, Joanna Domagała-Kulawik, Jolanta Korsak, and Piotr Rzepecki. 2023. "Flow Cytometric Analysis of Macrophages and Cytokines Profile in the Bronchoalveolar Lavage Fluid in Patients with Lung Cancer" Cancers 15, no. 21: 5175. https://doi.org/10.3390/cancers15215175