
Induction of Bystander and Abscopal Effects after Electroporation-Based Treatments

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. In Vitro Experiments and Cell Preparation for Tumor Injections
2.1.1. In Vitro Cell Electroporation
2.1.2. In Vitro Cell Viability Evaluation of Cells Directly Treated with Bleomycin Electrotransfer or Calcium Electroporation
2.1.3. In Vitro Cell Viability Evaluation of Cells Indirectly Treated with Cell Medium Taken from the Directly Treated Cells (Evaluation of Bystander Effect)
2.2. In Vivo Experiments
2.2.1. Electrochemotherapy and Calcium Electroporation
2.2.2. Electrotransfection
2.2.3. Electroporation Parameters
2.2.4. Tumor Size Measurements
2.2.5. Serum Preparation and ELISA
2.3. Statistical Analysis
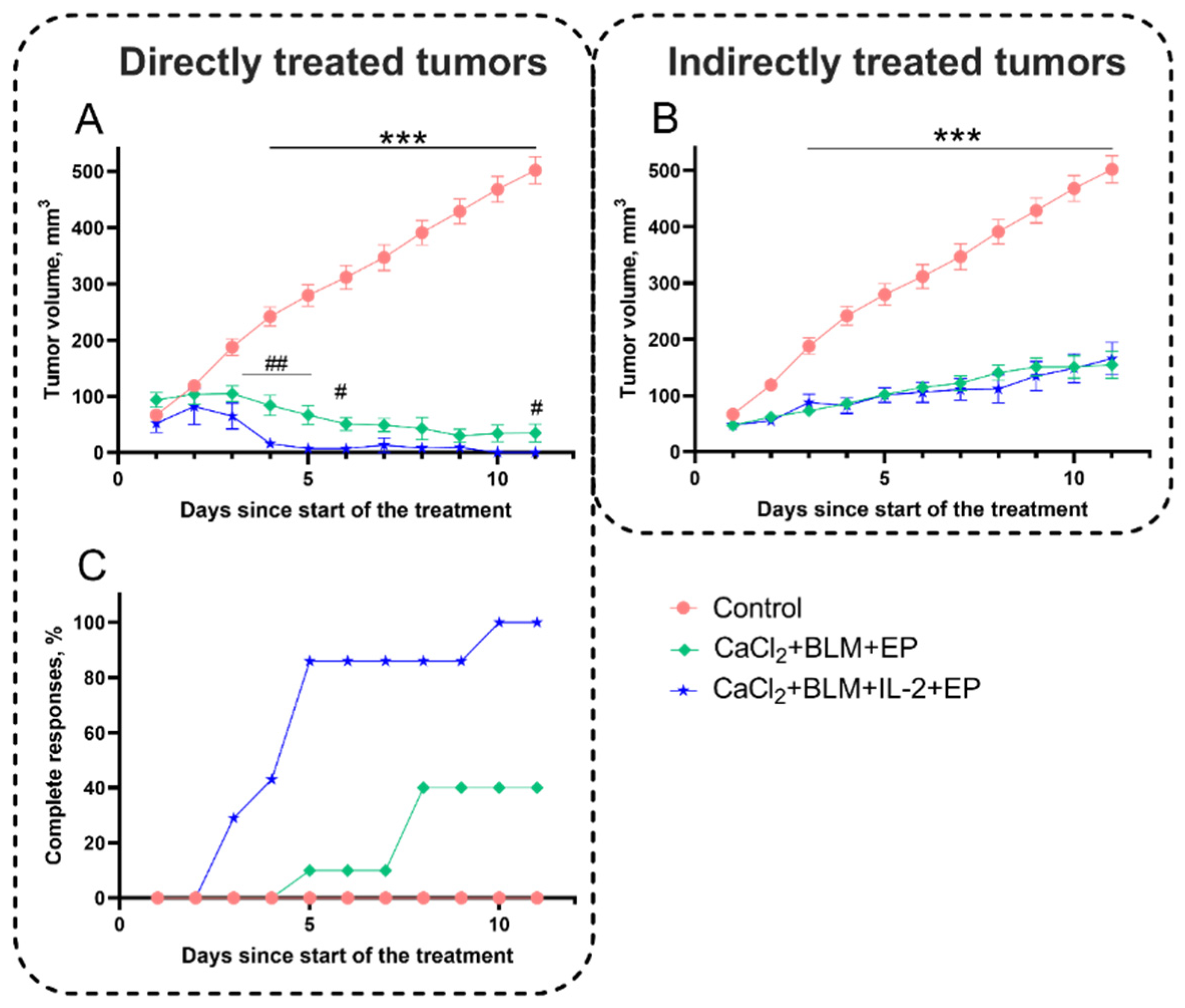
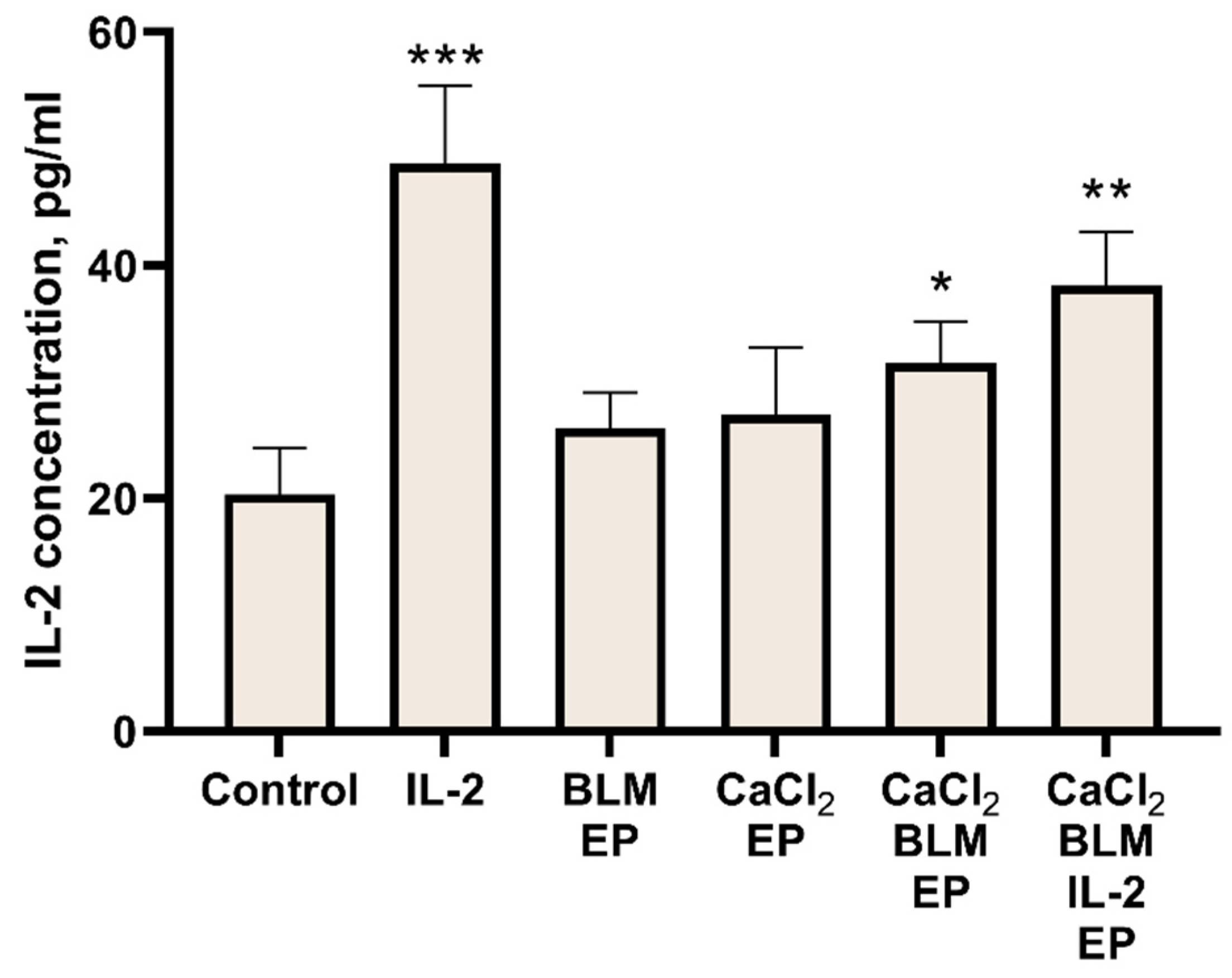
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Batista Napotnik, T.; Polajžer, T.; Miklavčič, D. Cell Death Due to Electroporation—A Review. Bioelectrochemistry 2021, 141, 107871. [Google Scholar] [CrossRef] [PubMed]
- Mir, L.M.; Orlowski, S.; Belehradek, J.; Paoletti, C. Electrochemotherapy Potentiation of Antitumour Effect of Bleomycin by Local Electric Pulses. Eur. J. Cancer Clin. Oncol. 1991, 27, 68–72. [Google Scholar] [CrossRef]
- Davalos, R.V.; Mir, I.L.M.; Rubinsky, B. Tissue Ablation with Irreversible Electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Šatkauskas, S.; Batiuškaite, D.; Šalomskaite-Davalgiene, S.; Venslauskas, M.S. Effectiveness of Tumor Electrochemotherapy as a Function of Electric Pulse Strength and Duration. Bioelectrochemistry 2005, 65, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Cadossi, R.; Ronchetti, M.; Cadossi, M. Locally Enhanced Chemotherapy by Electroporation: Clinical Experiences and Perspective of Use of Electrochemotherapy. Future Oncol. 2014, 10, 877–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belehradek, M.; Domenge, C.; Luboinski, B.; Orlowski, S.; Belehradek, J.; Mir, L.M. Electrochemotherapy, a New Antitumor Treatment. First Clinical Phase I–II Trial. Cancer 1993, 72, 3694–3700. [Google Scholar] [CrossRef]
- Al-Sakere, B.; André, F.; Bernat, C.; Connault, E.; Opolon, P.; Davalos, R.V.; Rubinsky, B.; Mir, L.M. Tumor Ablation with Irreversible Electroporation. PLoS ONE 2007, 2, e1135. [Google Scholar] [CrossRef] [Green Version]
- Falk, H.; Matthiessen, L.W.; Wooler, G.; Gehl, J. Calcium Electroporation for Treatment of Cutaneous Metastases; a Randomized Double-Blinded Phase II Study, Comparing the Effect of Calcium Electroporation with Electrochemotherapy. Acta Oncol. 2018, 57, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; Gissel, H.; Hojman, P.; Eriksen, J.; Gehl, J. Calcium Electroporation in Three Cell Lines: A Comparison of Bleomycin and Calcium, Calcium Compounds, and Pulsing Conditions. Biochim. Biophys. Acta 2014, 1840, 1204–1208. [Google Scholar] [CrossRef] [Green Version]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D.; et al. Electrochemotherapy—An Easy, Highly Effective and Safe Treatment of Cutaneous and Subcutaneous Metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) Study. Eur. J. Cancer Suppl. 2006, 4, 3–13. [Google Scholar] [CrossRef]
- Gehl, J.; Sersa, G.; Matthiessen, L.W.; Muir, T.; Soden, D.; Occhini, A.; Quaglino, P.; Curatolo, P.; Campana, L.G.; Kunte, C.; et al. Updated Standard Operating Procedures for Electrochemotherapy of Cutaneous Tumours and Skin Metastases. Acta Oncol. 2018, 57, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Sersa, G.; Stabuc, B.; Cemazar, M.; Miklavcic, D.; Rudolf, Z. Electrochemotherapy with Cisplatin: Clinical Experience in Malignant Melanoma Patients. Clin. Cancer Res. 2000, 6, 863–867. [Google Scholar] [PubMed]
- Gudvangen, E.; Kim, V.; Novickij, V.; Battista, F.; Pakhomov, A.G. Electroporation and Cell Killing by Milli- to Nanosecond Pulses and Avoiding Neuromuscular Stimulation in Cancer Ablation. Sci. Rep. 2022, 12, 1763. [Google Scholar] [CrossRef] [PubMed]
- Edd, J.F.; Horowitz, L.; Davalos, R.V.; Mir, L.M.; Rubinsky, B. In Vivo Results of a New Focal Tissue Ablation Technique: Irreversible Electroporation. IEEE Trans. Biomed. Eng. 2006, 53, 1409–1415. [Google Scholar] [CrossRef] [PubMed]
- Rai, Z.L.; Feakins, R.; Pallett, L.J.; Manas, D.; Davidson, B.R. Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy. J. Clin. Med. 2021, 10, 1609. [Google Scholar] [CrossRef]
- Ruarus, A.H.; Barabasch, A.; Catalano, O.; Leen, E.; Narayanan, G.; Nilsson, A.; Padia, S.A.; Wiggermann, P.; Scheffer, H.J.; Meijerink, M.R. Irreversible Electroporation for Hepatic Tumors: Protocol Standardization Using the Modified Delphi Technique. J. Vasc. Interv. Radiol. 2020, 31, 1765–1771.e15. [Google Scholar] [CrossRef] [PubMed]
- Vroomen, L.G.P.H.; Petre, E.N.; Cornelis, F.H.; Solomon, S.B.; Srimathveeravalli, G. Irreversible Electroporation and Thermal Ablation of Tumors in the Liver, Lung, Kidney and Bone: What Are the Differences? Diagn. Interv. Imaging 2017, 98, 609–617. [Google Scholar] [CrossRef]
- Jiang, C.; Davalos, R.V.; Bischof, J.C. A Review of Basic to Clinical Studies of Irreversible Electroporation Therapy. IEEE Trans. Biomed. Eng. 2015, 62, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, H.J.; Nielsen, K.; de Jong, M.C.; van Tilborg, A.A.J.M.; Vieveen, J.M.; Bouwman, A.R.A.; Meijer, S.; van Kuijk, C.; van den Tol, P.M.P.; Meijerink, M.R. Irreversible Electroporation for Nonthermal Tumor Ablation in the Clinical Setting: A Systematic Review of Safety and Efficacy. J. Vasc. Interv. Radiol. 2014, 25, 997–1011. [Google Scholar] [CrossRef] [PubMed]
- Heller, L.; Pottinger, C.; Jaroszeski, M.J.; Gilbert, R.; Heller, R. In Vivo Electroporation of Plasmids Encoding GM-CSF or Interleukin-2 into Existing B16 Melanomas Combined with Electrochemotherapy Induces Long-Term Antitumour Immunity. Melanoma Res. 2000, 10, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Sedlar, A.; Dolinsek, T.; Markelc, B.; Prosen, L.; Kranjc, S.; Bosnjak, M.; Blagus, T.; Cemazar, M.; Sersa, G. Potentiation of Electrochemotherapy by Intramuscular IL-12 Gene Electrotransfer in Murine Sarcoma and Carcinoma with Different Immunogenicity. Radiol. Oncol. 2012, 46, 302–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hribernik, A.; Cemazar, M.; Sersa, G.; Bosnjak, M.; Snoj, M. Effectiveness of Electrochemotherapy after IFN-α Adjuvant Therapy of Melanoma Patients. Radiol. Oncol. 2016, 50, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Cemazar, M.; Todorovic, V.; Scancar, J.; Lampreht, U.; Stimac, M.; Kamensek, U.; Kranjc, S.; Coer, A.; Sersa, G. Adjuvant TNF-α Therapy to Electrochemotherapy with Intravenous Cisplatin in Murine Sarcoma Exerts Synergistic Antitumor Effectiveness. Radiol. Oncol. 2015, 49, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mir, L.M.; Roth, C.; Orlowski, S.; Quintin-Colonna, F.; Fradelizi, D.; Belehradek, J.; Kourilsky, P. Systemic Antitumor Effects of Electrochemotherapy Combined with Histoincompatible Cells Secreting Interleukin-2. J. Immunother. 1995, 17, 30–38. [Google Scholar] [CrossRef]
- Heppt, M.V.; Eigentler, T.K.; Kähler, K.C.; Herbst, R.A.; Göppner, D.; Gambichler, T.; Ulrich, J.; Dippel, E.; Loquai, C.; Schell, B.; et al. Immune Checkpoint Blockade with Concurrent Electrochemotherapy in Advanced Melanoma: A Retrospective Multicenter Analysis. Cancer Immunol. Immunother. 2016, 65, 951–959. [Google Scholar] [CrossRef]
- Falk, H.; Forde, P.F.; Bay, M.L.; Mangalanathan, U.M.; Hojman, P.; Soden, D.M.; Gehl, J. Calcium Electroporation Induces Tumor Eradication, Long-Lasting Immunity and Cytokine Responses in the CT26 Colon Cancer Mouse Model. OncoImmunology 2017, 6, e1301332. [Google Scholar] [CrossRef] [Green Version]
- Neal, R.E.; Rossmeisl, J.H.; Robertson, J.L.; Arena, C.B.; Davis, E.M.; Singh, R.N.; Stallings, J.; Davalos, R.V. Improved Local and Systemic Anti-Tumor Efficacy for Irreversible Electroporation in Immunocompetent versus Immunodeficient Mice. PLoS ONE 2013, 8, e64559. [Google Scholar] [CrossRef]
- Li, X.; Xu, K.; Li, W.; Qiu, X.; Ma, B.; Fan, Q.; Li, Z. Immunologic Response to Tumor Ablation with Irreversible Electroporation. PLoS ONE 2012, 7, e48749. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Ren, Z.; Yin, S.; Xu, Y.; Guo, D.; Xie, H.; Zhou, L.; Wu, L.; Jiang, J.; Li, H.; et al. The Local Liver Ablation with Pulsed Electric Field Stimulate Systemic Immune Reaction against Hepatocellular Carcinoma (HCC) with Time-Dependent Cytokine Profile. Cytokine 2017, 93, 44–50. [Google Scholar] [CrossRef]
- Zhao, J.; Wen, X.; Tian, L.; Li, T.; Xu, C.; Wen, X.; Melancon, M.P.; Gupta, S.; Shen, B.; Peng, W.; et al. Irreversible Electroporation Reverses Resistance to Immune Checkpoint Blockade in Pancreatic Cancer. Nat. Commun. 2019, 10, 899. [Google Scholar] [CrossRef] [Green Version]
- Shi, X.; O’Neill, C.; Wang, X.; Chen, Y.; Yu, Y.; Tan, M.; Lv, G.; Li, Y.; Martin, R.C. Irreversible Electroporation Enhances Immunotherapeutic Effect in the Off-Target Tumor in a Murine Model of Orthotopic HCC. Am. J. Cancer Res. 2021, 11, 3304–3319. [Google Scholar] [PubMed]
- Nuccitelli, R.; Berridge, J.C.; Mallon, Z.; Kreis, M.; Athos, B.; Nuccitelli, P. Nanoelectroablation of Murine Tumors Triggers a CD8-Dependent Inhibition of Secondary Tumor Growth. PLoS ONE 2015, 10, e0134364. [Google Scholar] [CrossRef] [Green Version]
- He, C.; Huang, X.; Zhang, Y.; Lin, X.; Li, S. T-cell Activation and Immune Memory Enhancement Induced by Irreversible Electroporation in Pancreatic Cancer. Clin. Transl. Med. 2020, 10, e39. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Du, F.; Liu, Q.; Guo, Y.; Wang, Q.; Huang, W.; Wang, Z.; Ding, X.; Wu, Z. Immunological Effect of Irreversible Electroporation on Hepatocellular Carcinoma. BMC Cancer 2021, 21, 443. [Google Scholar] [CrossRef]
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-Sensing Receptors in Sterile Inflammation and Inflammatory Diseases. Nat. Rev. Immunol. 2020, 20, 95–112. [Google Scholar] [CrossRef] [PubMed]
- Jakstys, B.; Jakutaviciute, M.; Uzdavinyte, D.; Satkauskiene, I.; Satkauskas, S. Correlation between the Loss of Intracellular Molecules and Cell Viability after Cell Electroporation. Bioelectrochemistry 2020, 135, 107550. [Google Scholar] [CrossRef]
- Ruzgys, P.; Barauskaitė, N.; Novickij, V.; Novickij, J.; Šatkauskas, S. The Evidence of the Bystander Effect after Bleomycin Electrotransfer and Irreversible Electroporation. Molecules 2021, 26, 6001. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji—An Open Source Platform for Biological Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Guzmán, C.; Bagga, M.; Kaur, A.; Westermarck, J.; Abankwa, D. ColonyArea: An ImageJ Plugin to Automatically Quantify Colony Formation in Clonogenic Assays. PLoS ONE 2014, 9, 92444. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, S.K.; Krüger, M.B.; Mangalanathan, U.M.; Tramm, T.; Mahmood, F.; Novak, I.; Gehl, J. Normal and Malignant Cells Exhibit Differential Responses to Calcium Electroporation. Cancer Res. 2017, 77, 4389–4401. [Google Scholar] [CrossRef] [Green Version]
- Baba, K.; Nomura, M.; Ohashi, S.; Hiratsuka, T.; Nakai, Y.; Saito, T.; Kondo, Y.; Fukuyama, K.; Kikuchi, O.; Yamada, A.; et al. Experimental Model for the Irradiation-Mediated Abscopal Effect and Factors Influencing This Effect. Am. J. Cancer Res. 2020, 10, 440. [Google Scholar] [PubMed]
- Daguenet, E.; Louati, S.; Wozny, A.S.; Vial, N.; Gras, M.; Guy, J.B.; Vallard, A.; Rodriguez-Lafrasse, C.; Magné, N. Radiation-Induced Bystander and Abscopal Effects: Important Lessons from Preclinical Models. Br. J. Cancer 2020, 123, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Sawal, H.; Asghar, K.; Bureik, M.; Jalal, N. Bystander Signaling via Oxidative Metabolism. Onco. Targets Ther. 2017, 10, 3925–3940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widel, M. Radiation Induced Bystander Effect: From in Vitro Studies to Clinical Application. Int. J. Med. Phys. Clin. Eng. Radiat. Oncol. 2016, 5, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Justesen, T.F.; Orhan, A.; Raskov, H.; Nolsoe, C.; Gögenur, I. Electroporation and Immunotherapy—Unleashing the Abscopal Effect. Cancers 2022, 14, 2876. [Google Scholar] [CrossRef]
- Mukhopadhyay, A.; Wright, J.; Shirley, S.; Canton, D.A.; Burkart, C.; Connolly, R.J.; Campbell, J.S.; Pierce, R.H. Characterization of Abscopal Effects of Intratumoral Electroporation-Mediated IL-12 Gene Therapy. Gene Ther. 2018, 26, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.K. The Surprising Story of IL-2. Am. J. Pathol. 2020, 190, 1776–1781. [Google Scholar] [CrossRef]
- Komel, T.; Bosnjak, M.; Kranjc Brezar, S.; de Robertis, M.; Mastrodonato, M.; Scillitani, G.; Pesole, G.; Signori, E.; Sersa, G.; Cemazar, M. Gene Electrotransfer of IL-2 and IL-12 Plasmids Effectively Eradicated Murine B16.F10 Melanoma. Bioelectrochemistry 2021, 141, 107843. [Google Scholar] [CrossRef]
- Heller, L.C.; Heller, R. Electroporation Gene Therapy Preclinical and Clinical Trials for Melanoma. Curr. Gene Ther. 2010, 10, 312–317. [Google Scholar] [CrossRef]
- Horton, H.M.; Lalor, P.A.; Rolland, A.P. IL-2 Plasmid Electroporation: From Preclinical Studies to Phase I Clinical Trial; Humana Press: Totowa, NJ, USA, 2008; pp. 361–372. [Google Scholar]
- Jin, G.-H.; Hirano, T.; Murakami, M. Combination Treatment with IL-2 and Anti-IL-2 MAbs Reduces Tumor Metastasis via NK Cell Activation. Int. Immunol. 2008, 20, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillis, S.; Ferm, M.M.; Ou, W.; Smith, K.A. T Cell Growth Factor Parameters of Production and a Quantitative Microassay for Activity. J. Immunol. 1978, 120, 2027–2032. Available online: https://scirp.org/reference/referencespapers.aspx?referenceid=1622535 (accessed on 22 June 2022).
- Morgan, D.A.; Ruscetti, F.W.; Gallo, R. Selective in Vitro Growth of T Lymphocytes from Normal Human Bone Marrows. Science 1976, 193, 1007–1008. [Google Scholar] [CrossRef]
- Smith, K.A. Interleukin-2: Inception, Impact, and Implications. Science 1988, 240, 1169–1176. [Google Scholar] [CrossRef]
- Herberman, R.B.; Nunn, M.E.; Lavrin, D.H. Natural Cytotoxic Reactivity of Mouse Lymphoid Cells against Syngeneic and Allogeneic Tumors. I. Distribution of Reactivity and Specificity. Int. J. Cancer 1975, 16, 216–229. [Google Scholar] [CrossRef]
- Biron, C.A.; Young, H.A.; Kasaian, M.T. Interleukin 2-Induced Proliferation of Murine Natural Killer Cells In Vivo. J. Exp. Med. 1990, 171, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Induction of NK Cell Activity against Fresh Human Leukemia in Culture with Interleukin 2. Available online: https://pubmed.ncbi.nlm.nih.gov/3494084/ (accessed on 22 June 2022).
- Sitrin, J.; Ring, A.; Christopher Garcia, K.; Benoist, C.; Mathis, D. Regulatory T Cells Control NK Cells in an Insulitic Lesion by Depriving Them of IL-2. J. Exp. Med. 2013, 210, 1153–1165. [Google Scholar] [CrossRef] [Green Version]
- Bugaut, H.; Bruchard, M.; Berger, H.; Derangère, V.; Odoul, L.; Euvrard, R.; Ladoire, S.; Chalmin, F.; Végran, F.; Rébé, C.; et al. Bleomycin Exerts Ambivalent Antitumor Immune Effect by Triggering Both Immunogenic Cell Death and Proliferation of Regulatory T Cells. PLoS ONE 2013, 8, e65181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvet, C.Y.; Famin, D.; André, F.M.; Mir, L.M. Electrochemotherapy with Bleomycin Induces Hallmarks of Immunogenic Cell Death in Murine Colon Cancer Cells. OncoImmunology 2014, 3, e28131. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Adjemian, S.; Yang, H.; Catani, J.P.P.; Hannani, D.; Martins, I.; Michaud, M.; Kepp, O.; Sukkurwala, A.Q.; Vacchelli, E.; et al. ATP-Dependent Recruitment, Survival and Differentiation of Dendritic Cell Precursors in the Tumor Bed after Anticancer Chemotherapy. OncoImmunology 2013, 2, e24568. [Google Scholar] [CrossRef] [Green Version]
- Entin, I.; Plotnikov, A.; Korenstein, R.; Keisari, Y. Tumor Growth Retardation, Cure, and Induction of Antitumor Immunity in B16 Melanoma-Bearing Mice by Low Electric Field-Enhanced Chemotherapy. Clin. Cancer Res. 2003, 9, 3190–3197. [Google Scholar] [PubMed]
- Tremble, L.F.; O’Brien, M.A.; Soden, D.M.; Forde, P.F. Electrochemotherapy with Cisplatin Increases Survival and Induces Immunogenic Responses in Murine Models of Lung Cancer and Colorectal Cancer. Cancer Lett. 2019, 442, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Bigi, L.; Galdo, G.; Cesinaro, A.M.; Vaschieri, C.; Marconi, A.; Pincelli, C.; Fantini, F. Electrochemotherapy Induces Apoptotic Death in Melanoma Metastases: A Histologic and Immunohistochemical Investigation. Clin. Cosmet. Investig. Dermatol. 2016, 9, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendix, M.B.; Houston, A.; Forde, P.F.; Brint, E. Electrochemotherapy and Immune Interactions; A Boost to the System? Eur. J. Surg. Oncol. 2022; in press. [Google Scholar] [CrossRef]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruzgys, P.; Navickaitė, D.; Palepšienė, R.; Uždavinytė, D.; Barauskaitė, N.; Novickij, V.; Girkontaitė, I.; Šitkauskienė, B.; Šatkauskas, S. Induction of Bystander and Abscopal Effects after Electroporation-Based Treatments. Cancers 2022, 14, 3770. https://doi.org/10.3390/cancers14153770
Ruzgys P, Navickaitė D, Palepšienė R, Uždavinytė D, Barauskaitė N, Novickij V, Girkontaitė I, Šitkauskienė B, Šatkauskas S. Induction of Bystander and Abscopal Effects after Electroporation-Based Treatments. Cancers. 2022; 14(15):3770. https://doi.org/10.3390/cancers14153770
Chicago/Turabian StyleRuzgys, Paulius, Diana Navickaitė, Rūta Palepšienė, Dovilė Uždavinytė, Neringa Barauskaitė, Vitalij Novickij, Irutė Girkontaitė, Brigita Šitkauskienė, and Saulius Šatkauskas. 2022. "Induction of Bystander and Abscopal Effects after Electroporation-Based Treatments" Cancers 14, no. 15: 3770. https://doi.org/10.3390/cancers14153770