Solid Organ Transplantation Is Associated with an Increased Rate of Mismatch Repair Deficiency and PIK3CA Mutations in Colorectal Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jorge, A.; Wallace, Z.S.; Lu, N.; Zhang, Y.; Choi, H.K. Renal Transplantation and Survival Among Patients with Lupus Nephritis: A Cohort Study. Ann. Intern. Med. 2019, 170, 240–247. [Google Scholar] [CrossRef]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krisl, A.; Stampf, S.; Hauri, D.; Binet, I.; Mueller, T.; Sidler, D.; Hadaya, K.; Golshayan, D.; Pascual, M.; Koller, M.; et al. Immunosuppression management in renal transplant recipients with normal-immunological risk: 10-year results from the Swiss Transplant Cohort Study. Swiss Med. Wkly. 2020, 150, w20354. [Google Scholar] [CrossRef]
- Nedredal, G.I.; Picon, R.V.; Chedid, M.F.; Foss, A. Immunosuppression in Liver Transplantation: State of the Art and Future Perspectives. Curr. Pharm. Des. 2020, 26, 3389–3401. [Google Scholar] [CrossRef]
- Au, E.; Wong, G.; Chapman, J.R. Cancer in kidney transplant recipients. Nat. Rev. Nephrol. 2018, 14, 508–520. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008-A Swedish population-based study. Int. J. Cancer 2013, 132, 1429–1438. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/ijc.27765 (accessed on 10 January 2022). [CrossRef]
- Collett, D.; Mumford, L.; Banner, N.R.; Neuberger, J.; Watson, C. Comparison of the Incidence of Malignancy in Recipients of Different Types of Organ: A UK Registry Audit. Am. J. Transplant. 2010, 10, 1889–1896. [Google Scholar] [CrossRef]
- Imamura, R.; Nakazawa, S.; Yamanaka, K.; Kakuta, Y.; Tsutahara, K.; Taniguchi, A.; Kawamura, M.; Kato, T.; Abe, T.; Uemura, M.; et al. Cumulative cancer incidence and mortality after kidney transplantation in Japan: A long-term multicenter cohort study. Cancer Med. 2021, 10, 2205–2215. [Google Scholar] [CrossRef]
- Huo, Z.; Li, C.; Xu, X.; Ge, F.; Wang, R.; Wen, Y.; Peng, H.; Wu, X.; Liang, H.; Peng, G.; et al. Cancer Risks in Solid Organ Transplant Recipients: Results from a Comprehensive Analysis of 72 Cohort Studies. OncoImmunology 2020, 9, 1848068. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Santi, I.; Weires, M.; Thomsen, H.; Sundquist, J.; Bermejo, J.L. Tumor location and patient characteristics of colon and rectal adenocarcinomas in relation to survival and TNM classes. BMC Cancer 2010, 10, 688. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, Y.; Dai, Y.; Cheng, J.-N.; Gong, Z.; Feng, Y.; Sun, C.; Jia, Q.; Zhu, B. Immune Landscape of Colorectal Cancer Tumor Microenvironment from Different Primary Tumor Location. Front. Immunol. 2018, 9, 1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowacki, F.; Al Morabiti, M.; Lionet, A.; Labalette, M.; Provot, F.; Noel, C.; Hazzan, M. Long-Term Kinetics of a T-Lymphocytes Subset in Kidney Transplant Recipients: Relationship With Posttransplant Malignancies. Transplant. Proc. 2009, 41, 3323–3325. [Google Scholar] [CrossRef] [PubMed]
- Luque, Y.; Jamme, M.; Rabant, M.; DeWolf, S.; Noël, L.-H.; Thervet, E.; Chatenoud, L.; Snanoudj, R.; Anglicheau, D.; Legendre, C.; et al. Long-term CD4 lymphopenia is associated with accelerated decline of kidney allograft function. Nephrol. Dial. Transplant. 2016, 31, 487–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dujardin, A.; Lorent, M.; Foucher, Y.; Legendre, C.; Kerleau, C.; Brouard, S.; Giral, M.; Blancho, G.; Branchereau, J.; Cantarovich, D.; et al. Time-dependent lymphocyte count after transplantation is associated with higher risk of graft failure and death. Kidney Int. 2021, 99, 1189–1201. [Google Scholar] [CrossRef]
- Safaeian, M.; Robbins, H.A.; Berndt, S.I.; Lynch, C.F.; Fraumeni, J.F., Jr.; Engels, E.A. Risk of Colorectal Cancer After Solid Organ Transplantation in the United States. Am. J. Transplant. 2016, 16, 960–967. [Google Scholar] [CrossRef] [Green Version]
- Merchea, A.; Shahjehan, F.; Croome, K.P.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Kasi, P.M. Colorectal Cancer Characteristics and Outcomes after Solid Organ Transplantation. J. Oncol. 2019, 2019, 5796108. Available online: https://www.hindawi.com/journals/jo/2019/5796108/ (accessed on 5 October 2022). [CrossRef] [Green Version]
- Hsu, Y.-L.; Lin, C.-C.; Jiang, J.-K.; Lin, H.-H.; Lan, Y.-T.; Wang, H.-S.; Yang, S.-H.; Chen, W.-S.; Lin, T.-C.; Lin, J.-K.; et al. Clinicopathological and molecular differences in colorectal cancer according to location. Int. J. Biol. Markers 2019, 34, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.A.; Turner, E.H.; Beightol, M.B.; Jacobson, A.; Gooley, T.A.; Salipante, S.J.; Haraldsdottir, S.; Smith, C.; Scroggins, S.; Tait, J.F.; et al. Frequent PIK3CA Mutations in Colorectal and Endometrial Tumors With 2 or More Somatic Mutations in Mismatch Repair Genes. Gastroenterology 2016, 151, 440–447.e1. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Wahab, N.; Safa, H.; Abudayyeh, A.; Johnson, D.H.; Trinh, V.A.; Zobniw, C.M.; Lin, H.; Wong, M.K.; Abdelrahim, M.; Gaber, A.O.; et al. Checkpoint inhibitor therapy for cancer in solid organ transplantation recipients: An institutional experience and a systematic review of the literature. J. Immunother. Cancer 2019, 7, 106. [Google Scholar] [CrossRef] [Green Version]
- Manohar, S.; Thongprayoon, C.; Cheungpasitporn, W.; Markovic, S.N.; Herrmann, S.M. Systematic Review of the Safety of Immune Checkpoint Inhibitors Among Kidney Transplant Patients. Kidney Int. Rep. 2020, 5, 149–158. [Google Scholar] [CrossRef]
- Lipson, E.J.; Bagnasco, S.M.; Moore, J.; Jang, S.; Patel, M.J.; Zachary, A.A.; Pardoll, D.M.; Taube, J.M.; Drake, C.G. Tumor Regression and Allograft Rejection after Administration of Anti-PD-1. N. Engl. J. Med. 2016, 374, 896–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schenk, K.M.; Stein, J.E.; Chandra, S.; Davar, D.; Eroglu, Z.; Khushalani, N.I.; Luke, J.J.; Ott, P.A.; Sosman, J.A.; Aggarwal, V.; et al. Nivolumab (NIVO) + tacrolimus (TACRO) + prednisone (PRED) +/− ipilimumab (IPI) for kidney transplant recipients (KTR) with advanced cutaneous cancers. J. Clin. Orthod. 2022, 40, 9507. [Google Scholar] [CrossRef]
- Sugie, N.; Fujii, N.; Danno, K. Cyclosporin-A suppresses p53-dependent repair DNA synthesis and apoptosis following ultraviolet-B irradiation. Photodermatol. Photoimmunol. Photomed. 2002, 18, 163–168. [Google Scholar] [CrossRef]
- Hojo, M.; Morimoto, T.; Maluccio, M.; Asano, T.; Morimoto, K.; Lagman, M.; Shimbo, T.; Suthanthiran, M. Cyclosporine induces cancer progression by a cell-autonomous mechanism. Nature 1999, 397, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.-Y.; Hao, M. Mammalian Target of Rapamycin (mTOR) Regulates Transforming Growth Factor-β1 (TGF-β1)-Induced Epithelial-Mesenchymal Transition via Decreased Pyruvate Kinase M2 (PKM2) Expression in Cervical Cancer Cells. Med. Sci. Monit. 2017, 23, 2017–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, S.; Hoffmann, V.S.; Habicht, A.; Kauke, T.; Bucher, J.; Schoenberg, M.; Werner, J.; Guba, M.; Andrassy, J. Effects of mTOR-Is on malignancy and survival following renal transplantation: A systematic review and meta-analysis of randomized trials with a minimum follow-up of 24 months. PLoS ONE 2018, 13, e0194975. [Google Scholar] [CrossRef] [Green Version]
- Murray, S.L.; Daly, F.E.; O’Kelly, P.; O’Leary, E.; Deady, S.; O’Neill, J.P.; Dudley, A.; Rutledge, N.R.; McCormick, A.; Houlihan, D.D.; et al. The impact of switching to mTOR inhibitor-based immunosuppression on long-term non-melanoma skin cancer incidence and renal function in kidney and liver transplant recipients. Ren. Fail. 2020, 42, 607–612. [Google Scholar] [CrossRef]
- Sinicrope, F.A.; Mahoney, M.R.; Yoon, H.H.; Smyrk, T.C.; Thibodeau, S.N.; Goldberg, R.M.; Nelson, G.D.; Sargent, D.J.; Alberts, S.R. Analysis of Molecular Markers by Anatomic Tumor Site in Stage III Colon Carcinomas from Adjuvant Chemotherapy Trial NCCTG N0147 (Alliance). Clin. Cancer Res. 2015, 21, 5294–5304. [Google Scholar] [CrossRef] [Green Version]
- Uhlig, J.; Cecchini, M.; Sheth, A.; Stein, S.; Lacy, J.; Kim, H.S. Microsatellite Instability and KRAS Mutation in Stage IV Colorectal Cancer: Prevalence, Geographic Discrepancies, and Outcomes From the National Cancer Database. J. Natl. Compr. Cancer Netw. 2021, 19, 307–318. [Google Scholar] [CrossRef]
- El-Jawhari, J.J.; El-Sherbiny, Y.M.; Scott, G.B.; Morgan, R.S.; Prestwich, R.; Bowles, P.A.; Blair, G.E.; Tanaka, T.; Rabbitts, T.H.; Meade, J.L.; et al. Blocking oncogenic RAS enhances tumour cell surface MHC class I expression but does not alter susceptibility to cytotoxic lymphocytes. Mol. Immunol. 2014, 58, 160–168. [Google Scholar] [CrossRef]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.E.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the cBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 29) | Kidney (n = 18) | Liver (n = 8) | KLT (n = 3) | ||
|---|---|---|---|---|---|
| Age in years (range) | 60 (31–82) | 51 (31–77) | 62.5 (54–73) | 73 (66–82) | |
| Sex (%) | Male | 16 (55) | 10 (56) | 4 (50) | 2 (67) |
| Female | 13 (45) | 8 (44) | 4 (50) | 1 (33) | |
| Time from transplant to CRC diagnosis in years | 9 (2–35) | 11 (3–35) | 3.5 (2–13) | 6 (2–12) | |
| TMB median (range) | 21.98 (3.52–53.7) | 14.07 (3.52–31.7) | 45.8 (37.8–53.7) | 37 | |
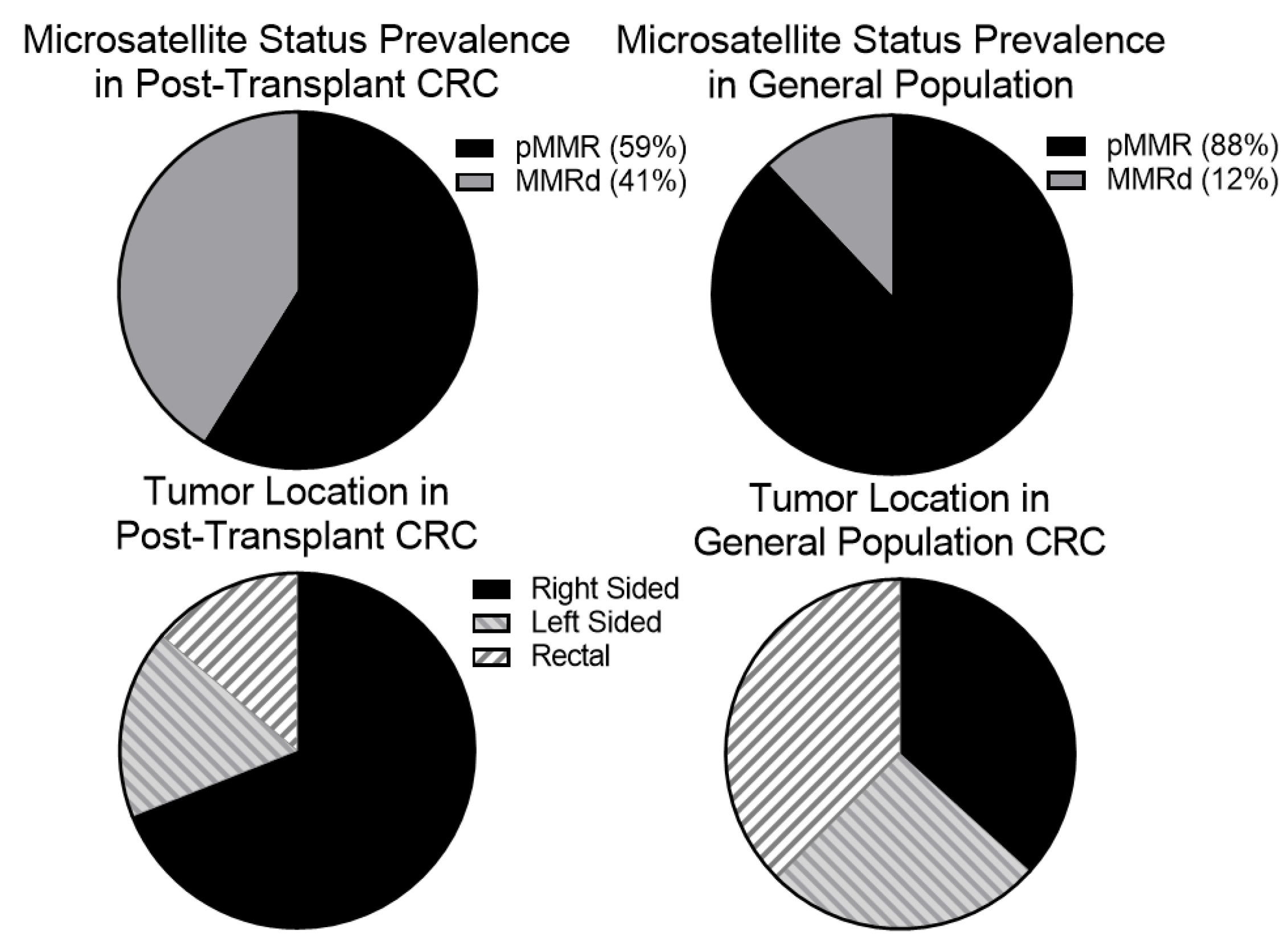
| Mismatch Repair Status (%) | MMRd | 7 (41) | 3 (27) | 2 (50) | 2 (100) |
| pMMR | 10 (59) | 8 (63) | 2 (50) | 0 | |
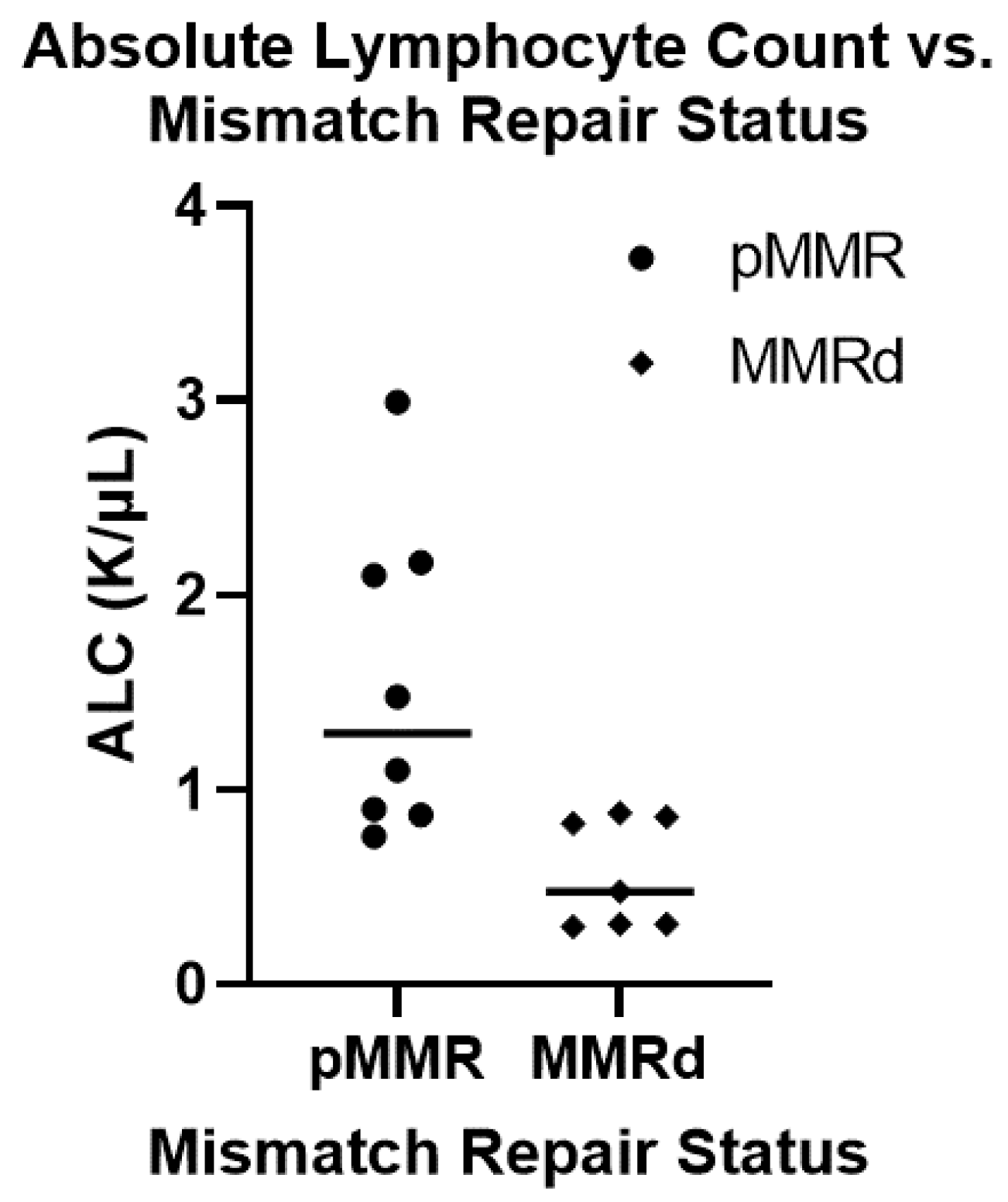
| ALC at CRC dx (K/μL) median/range | 1.1 (0.25–2.99) | 1.2 (0.48–2.99) | 0.84 (0.25–2.1) | 0.86 (0.83–1.43) | |
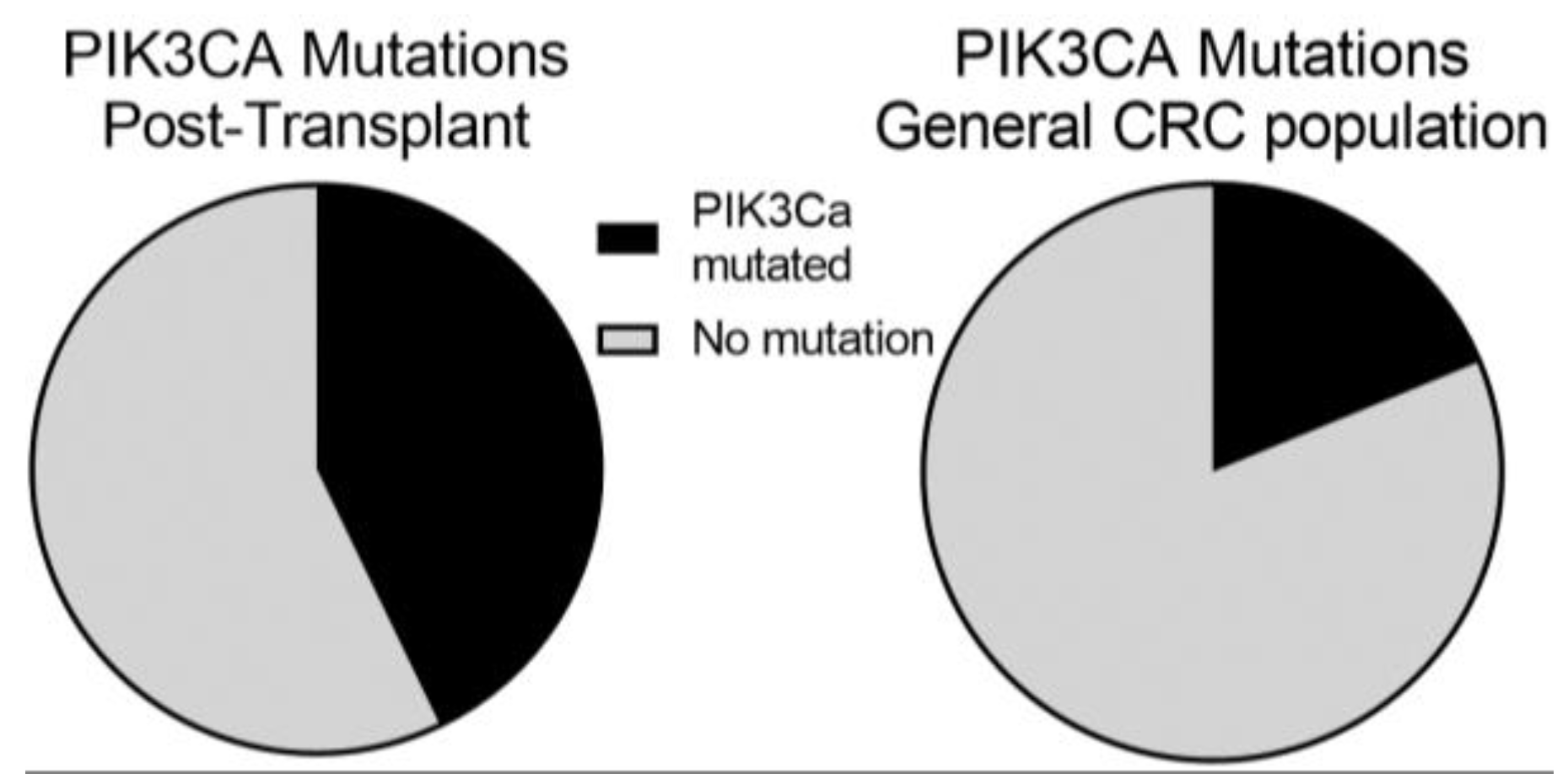
| PIK3CA status (%) | Mutant | 6 (43) | 3 (38) | 2 (50) | 1 (50) |
| Wild type | 8 (57) | 5 (62) | 2 (50) | 1 (50) | |
| KRAS status (%) | Mutant | 3 (21) | 2 (25) | 0 | 1 (50) |
| Wild type | 11 (79) | 6 (75) | 2 (100) | 1 (50) | |
| BRAF status (%) | Mutant | 4 (31) | 1 (14) | 2 (50) | 1 (50) |
| Wild type | 9 (69) | 6 (86) | 2 (50) | 1 (50) | |
| APC status (%) | Mutant | 5 (42) | 4 (57) | 0 | 1 (100) |
| Wild type | 7 (58) | 3 (43) | 4 (100) | 0 | |
| TP53 status (%) | Mutant | 5 (42) | 3 (43) | 2 (50) | 0 |
| Wild type | 7 (58) | 4 (57) | 2 (50) | 1 (100) | |
| Immunosuppression at the time of CRC diagnosis (%) | none | 2 (7) | 2 (11) | 0 | 0 |
| CNI | 6 (21) | 1 (6) | 5 (62) | 0 | |
| CNI + MMF | 1 (3) | 0 | 1 (12) | 0 | |
| CNI + Pred | 7 (24) | 6 (33) | 0 | 1 (33) | |
| CNI + MMF + Pred | 9 (30) | 7 (39) | 0 | 2 (67) | |
| CNI + Pred + 6-MP | 1 (3) | 0 | 1 (12) | 0 | |
| mTORi + MMF | 1 (3) | 0 | 1 (12) | 0 | |
| mTORi + Pred | 1 (3) | 1 (6) | 0 | 0 | |
| AZA + Pred | 1 (3) | 1 (6) | 0 | 0 | |
| Cause of Liver Transplant (%) | HCV | 3 (27) | N/A | 2 (25) | 1 (33) |
| ETOH | 3 (27) | N/A | 2 (25) | 1 (33) | |
| NASH | 3 (27) | N/A | 2 (25) | 1 (33) | |
| Primary Sclerosing Cholangitis | 1 (9) | N/A | 1 (12) | 0 | |
| Alpha-1-Antitrypsin | 1 (9) | N/A | 1 (12) | 0 | |
| Cause of Renal Transplant (%) | atypical HUS | 1 (5) | 1 (6) | N/A | 0 |
| CNI toxicity | 1 (5) | 0 | N/A | 1(33) | |
| diarrhea 2/2 short gut | 1 (5) | 0 | N/A | 1 (33) | |
| DM | 4 (19) | 4 (22) | N/A | 0 | |
| DM/HTN | 1 (5) | 1 (6) | N/A | 0 | |
| DM/FSGS | 1 (5) | 1 (6) | N/A | 0 | |
| FSGS | 2 (10) | 2 (11) | N/A | 0 | |
| GPA | 1 (5) | 1 (6) | N/A | 0 | |
| HTN | 4 (19) | 3 (17) | N/A | 1 (33) | |
| IgA nephropathy | 1 (5) | 1 (6) | N/A | 0 | |
| oligomeganephronia | 1 (5) | 1 (6) | N/A | 0 | |
| PKD | 1 (5) | 1 (6) | N/A | 0 | |
| SLE | 2 (10) | 2 (11) | N/A | 0 | |
| Stage at diagnosis (%) | Stage 0/1 | 7 (24) | 5 (28) | 2 (25) | 0 |
| Stage 2 | 9 (31) | 6 (33) | 1 (12) | 2 (67) | |
| Stage 3 | 10 (34) | 5 (28) | 4 (50) | 1 (33) | |
| Stage 4 | 3 (10) | 2 (11) | 1 (12) | 0 | |
| Recurrence (%) | Yes | 7 (24) | 6 (33) | 0 | 1 (33) |
| No | 22 (76) | 12 (67) | 8 (100) | 2 (67) | |
| Tumor location | Right | 20 (69) | 12 (67) | 5 (62) | 3 (100) |
| Left | 5 (17) | 3 (17) | 2 (25) | 0 | |
| Rectal | 4 (14) | 3 (17) | 1 (12) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christenson, E.S.; Lee, V.; Wang, H.; Yarchoan, M.; De Jesus-Acosta, A.; Azad, N.; Gurakar, A.; Lin, M.-T.; Le, D.T.; Brennan, D.C.; et al. Solid Organ Transplantation Is Associated with an Increased Rate of Mismatch Repair Deficiency and PIK3CA Mutations in Colorectal Cancer. Curr. Oncol. 2023, 30, 75-84. https://doi.org/10.3390/curroncol30010006
Christenson ES, Lee V, Wang H, Yarchoan M, De Jesus-Acosta A, Azad N, Gurakar A, Lin M-T, Le DT, Brennan DC, et al. Solid Organ Transplantation Is Associated with an Increased Rate of Mismatch Repair Deficiency and PIK3CA Mutations in Colorectal Cancer. Current Oncology. 2023; 30(1):75-84. https://doi.org/10.3390/curroncol30010006
Chicago/Turabian StyleChristenson, Eric S., Valerie Lee, Hao Wang, Mark Yarchoan, Ana De Jesus-Acosta, Nilo Azad, Ahmet Gurakar, Ming-Tseh Lin, Dung T. Le, Daniel C. Brennan, and et al. 2023. "Solid Organ Transplantation Is Associated with an Increased Rate of Mismatch Repair Deficiency and PIK3CA Mutations in Colorectal Cancer" Current Oncology 30, no. 1: 75-84. https://doi.org/10.3390/curroncol30010006