Intraoperative Positive Pancreatic Parenchymal Resection Margin: Is It a True Indication of Completion Total Pancreatectomy after Partial Pancreatectomy for Pancreatic Ductal Adenocarcinoma?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Statistical Analysis
3. Results
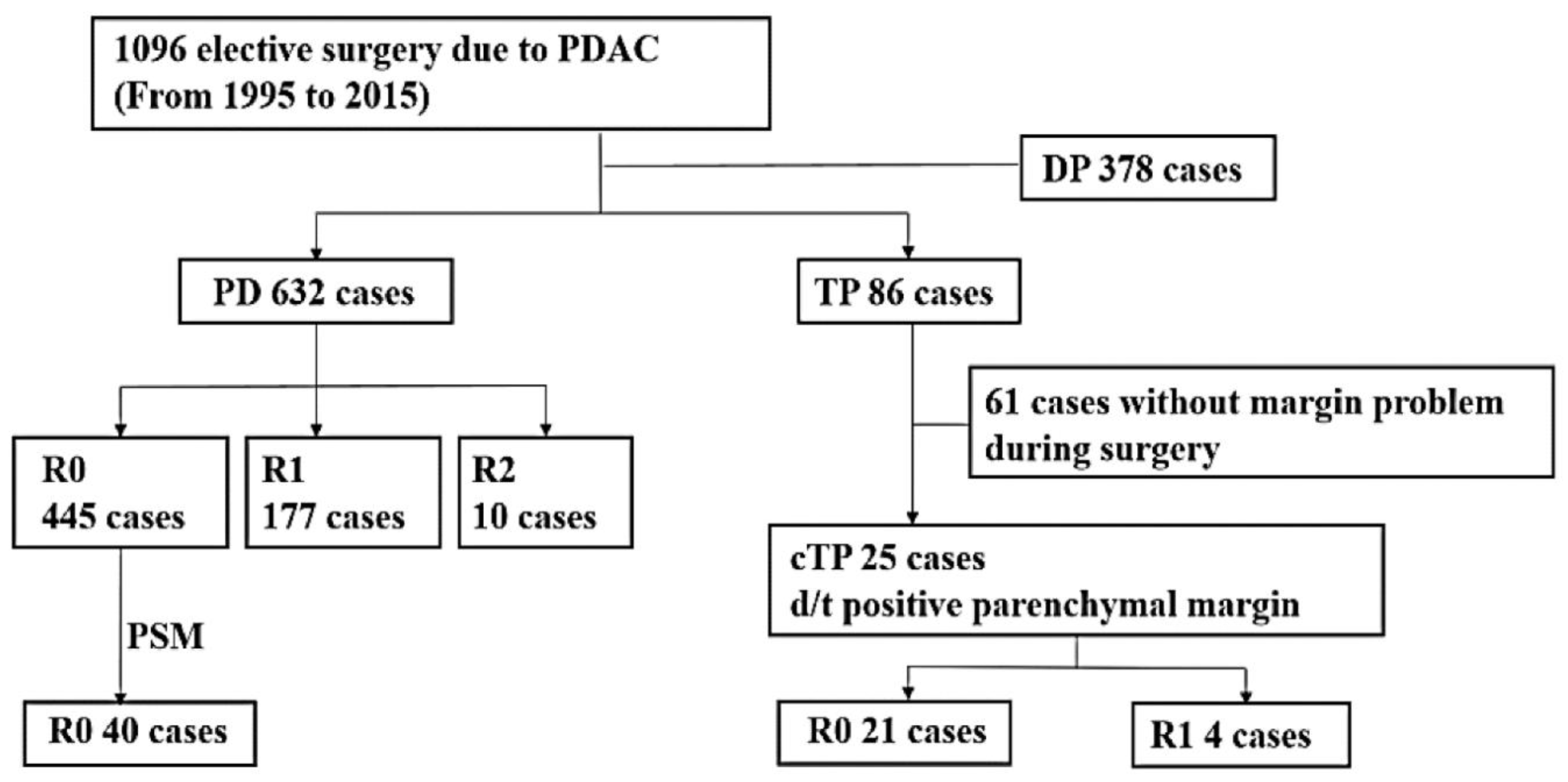
3.1. Clinical, Operative, and Pathological Characteristics
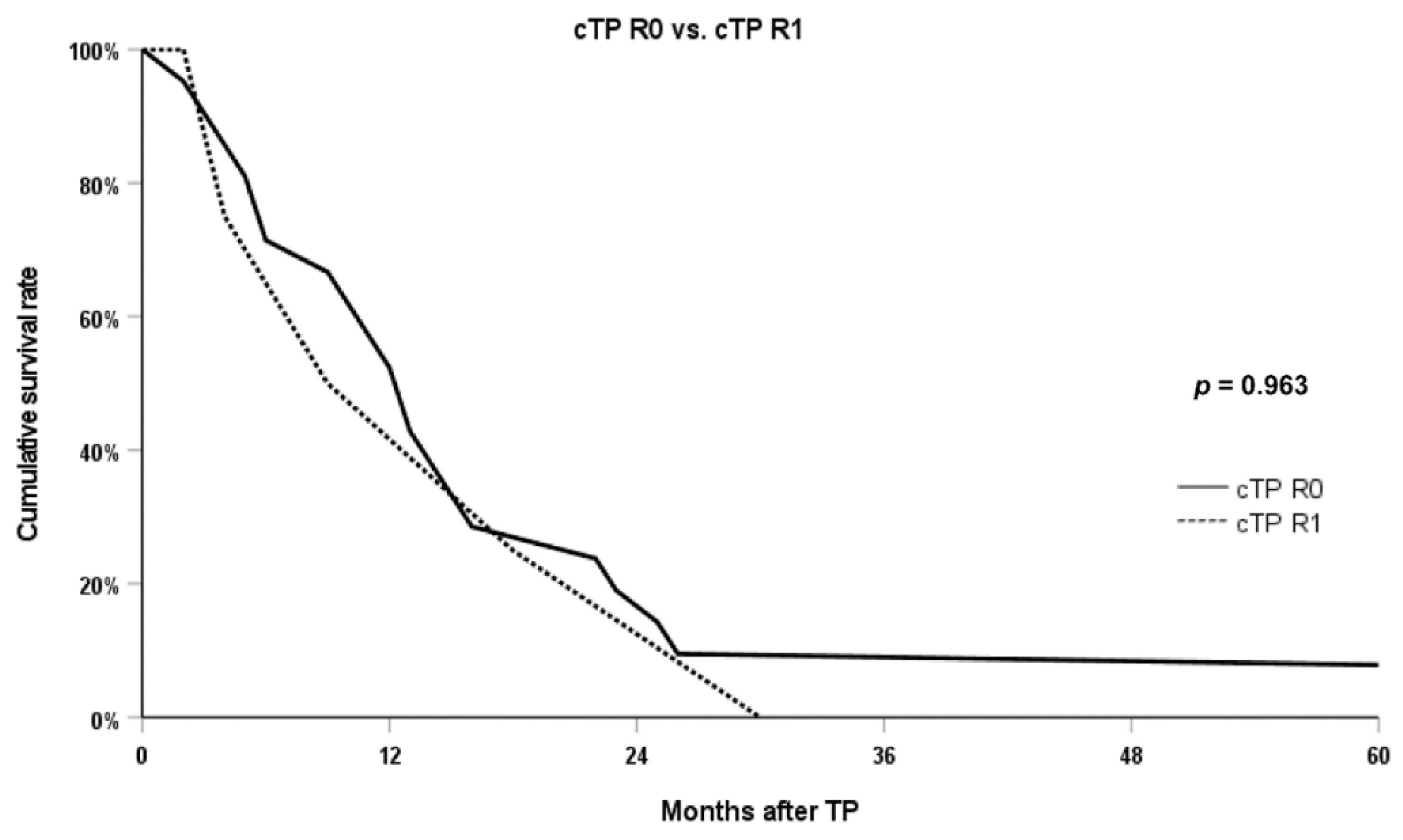
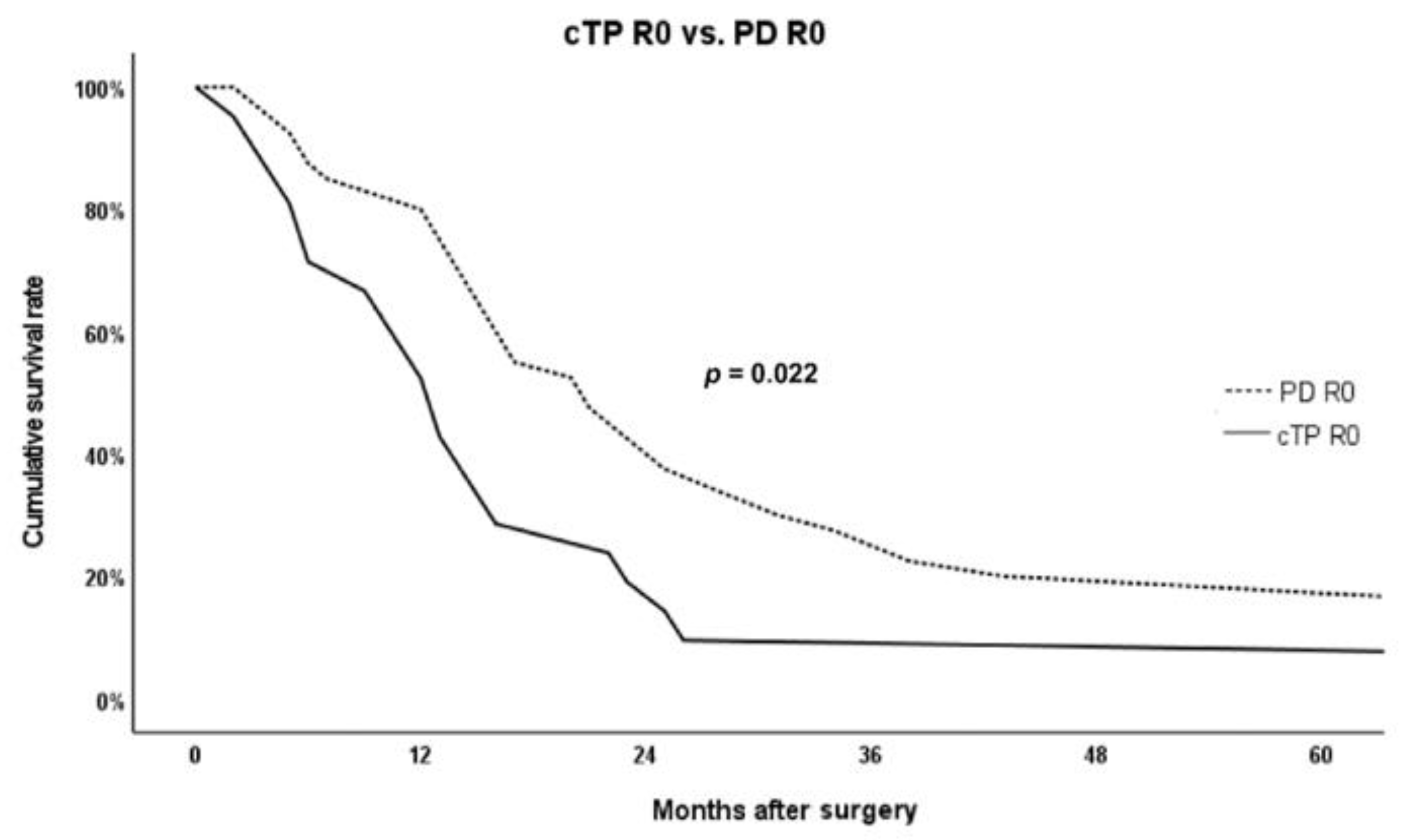
3.2. Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strobel, O.; Neoptolemos, J.; Jäger, D.; Büchler, M.W. Optimizing the outcomes of pancreatic cancer surgery. Nat. Rev. Clin. Oncol. 2019, 16, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Warschkow, R.; Widmann, B.; Beutner, U.; Marti, L.; Steffen, T.; Schiesser, M.; Schmied, B.M. The More the Better-Lower Rate of Stage Migration and Better Survival in Patients with Retrieval of 20 or More Regional Lymph Nodes in Pancreatic Cancer: A Population-Based Propensity Score Matched and Trend SEER Analysis. Pancreas 2017, 46, 648–657. [Google Scholar] [CrossRef]
- Kumar, R.; Herman, J.M.; Wolfgang, C.L.; Zheng, L. Multidisciplinary Management of Pancreatic Cancer. Surg. Oncol. Clin. N. Am. 2013, 22, 265–287. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Stewart, A.K.; Winchester, D.P.; Talamonti, M.S. National Failure to Operate on Early Stage Pancreatic Cancer. Ann. Surg. 2007, 246, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Tomlinson, J.S.; Ma, A.K.S.; Winchester, D.P.; Talamonti, M.S. Multimodality therapy for pancreatic cancer in the U.S.: Utilization, outcomes, and the effect of hospital volume. Cancer 2007, 110, 1227–1234. [Google Scholar] [CrossRef]
- Imamura, M.; Doi, R.; Imaizumi, T.; Funakoshi, A.; Wakasugi, H.; Sunamura, M.; Ogata, Y.; Hishinuma, S.; Asano, T.; Aikou, T.; et al. A randomized multicenter trial comparing resection and radiochemotherapy for resectable locally invasive pancreatic cancer. Surgery 2004, 136, 1003–1011. [Google Scholar] [CrossRef]
- Niesen, W.; Hank, T.; Büchler, M.; Strobel, O. Local radicality and survival outcome of pancreatic cancer surgery. Ann. Gastroenterol. Surg. 2019, 3, 464–475. [Google Scholar] [CrossRef]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Springfeld, C.; Jäger, D.; Schirmacher, P.; Hackert, T.; Büchler, M.W. Pancreatic Cancer Surgery: The New R-status Counts. Ann. Surg. 2016, 265, 565–573. [Google Scholar] [CrossRef]
- Hank, T.; Hinz, U.; Tarantino, I.; Kaiser, J.; Niesen, W.; Bergmann, F.; Hackert, T.; Büchler, M.W.; Strobel, O. Validation of at least 1 mm as cut-off for resection margins for pancreatic adenocarcinoma of the body and tail. Br. J. Surg. 2018, 105, 1171–1181. [Google Scholar] [CrossRef]
- Nitta, T.; Mitsuhashi, T.; Asano, T.; Okamura, K.; Tamoto, E.; Murakami, S.; Kurashima, Y.; Ebihara, Y.; Nakanishi, Y.; Nakamura, T.; et al. The impact of margin status determined by the one-millimeter rule on tumor recurrence and survival following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. Surg. Today 2016, 47, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Casadei, R.; Monari, F.; Buscemi, S.; Laterza, M.; Ricci, C.; Rega, D.; D’Ambra, M.; Pezzilli, R.; Calculli, L.; Santini, D.; et al. Total pancreatectomy: Indications, operative technique, and results: A single centre experience and review of literature. Updates Surg. 2010, 62, 41–46. [Google Scholar] [CrossRef]
- Crippa, S.; Tamburrino, D.; Partelli, S.; Salvia, R.; Germenia, S.; Bassi, C.; Pederzoli, P.; Falconi, M. Total pancreatectomy: Indications, different timing, and perioperative and long-term outcomes. Surgery 2011, 149, 79–86. [Google Scholar] [CrossRef]
- Pulvirenti, A.; Pea, A.; Rezaee, N.; Gasparini, C.; Malleo, G.; Weiss, M.J.; Cameron, J.L.; Wolfgang, C.L.; He, J.; Salvia, R. Perioperative outcomes and long-term quality of life after total pancreatectomy. Br. J. Surg. 2019, 106, 1819–1828. [Google Scholar] [CrossRef]
- Stoop, T.F.; Ateeb, Z.; Ghorbani, P.; Scholten, L.; Arnelo, U.; Besselink, M.G.; Del Chiaro, M. Surgical Outcomes After Total Pancreatectomy: A High-Volume Center Experience. Ann. Surg. Oncol. 2021, 28, 1543–1551. [Google Scholar] [CrossRef]
- Hayama, S.; Ambo, Y.; Takeuchi, S.; Takada, M.; Nakamura, F.; Kashimura, N.; Hirano, S. Clinical Outcomes after Total Pancreatectomy for Malignant Neoplasms; A Single Center Retrospective Study of 26 Cases. 2020. Available online: https://www.researchsquare.com/article/rs-17343/v1 (accessed on 1 July 2021).
- Muller, M.W.; Friess, H.; Kleeff, J.; Dahmen, R.; Wagner, M.; Hinz, U.; Breisch-Girbig, D.; Ceyhan, G.O.; Buchler, M.W. Is there still a role for total pancreatectomy? Ann. Surg. 2007, 246, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Wolfgang, C.L.; Cameron, J.L.; Eckhauser, F.; Choti, M.A.; Schulick, R.D.; Edil, B.H.; Pawlik, T.M. Total pancreatectomy for pancreatic adenocarcinoma: Evaluation of morbidity and long-term survival. Ann. Surg. 2009, 250, 282–287. [Google Scholar] [CrossRef]
- Casadei, R.; Ricci, C.; Taffurelli, G.; Guariniello, A.; Di Gioia, A.; Di Marco, M.; Pagano, N.; Serra, C.; Calculli, L.; Santini, D.; et al. Is total pancreatectomy as feasible, safe, efficacious, and cost-effective as pancreaticoduodenectomy? A single center, prospective, observational study. J. Gastrointest. Surg. 2016, 20, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Petrucciani, N.; Nigri, G.; Giannini, G.; Sborlini, E.; Antolino, L.; de’Angelis, N.; Gavriilidis, P.; Valente, R.; Lainas, P.; Dagher, I.; et al. Total Pancreatectomy for Pancreatic Carcinoma: When, Why, and What Are the Outcomes? Results of a Systematic Review. Pancreas 2020, 49, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Häberle, L.; Esposito, I. Circumferential resection margin (CRM) in pancreatic cancer. Surg. Pract. Sci. 2020, 1, 100006. [Google Scholar] [CrossRef]
- Raut, C.P.; Tseng, J.F.; Sun, C.C.; Wang, H.; Wolff, R.A.; Crane, C.H.; Vauthey, J.-N.; Abdalla, E.K.; Lee, J.E.; Pisters, P.W.T.; et al. Impact of Resection Status on Pattern of Failure and Survival After Pancreaticoduodenectomy for Pancreatic Adenocarcinoma. Ann. Surg. 2007, 246, 52–60. [Google Scholar] [CrossRef]
- Butturini, G.; Stocken, D.D.; Wente, M.N.; Jeekel, H.; Klinkenbijl, J.H.; Bakkevold, K.E.; Takada, T.; Amano, H.; Dervenis, C.; Bassi, C.; et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: Meta-analysis of randomized controlled trials. Arch. Surg. 2008, 143, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strobel, O.; Berens, V.; Hinz, U.; Hartwig, W.; Hackert, T.; Bergmann, F.; Debus, J.; Jäger, D.; Büchler, M.W.; Werner, J. Resection after neoadjuvant therapy for locally advanced, “unresectable” pancreatic cancer. Surgery 2012, 152, S33–S42. [Google Scholar] [CrossRef]
- Delpero, J.R.; Bachellier, P.; Regenet, N.; Le Treut, Y.P.; Paye, F.; Carrere, N.; Sauvanet, A.; Autret, A.; Turrini, O.; Monges-Ranchin, G.; et al. Pancreaticoduodenectomy for pancreatic ductal adenocarcinoma: A French multicentre prospective evaluation of resection margins in 150 evaluable specimens. HPB 2014, 16, 20–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikmen, K.; Kerem, M.; Bostanci, H.; Sare, M.; Ekinci, O. Intra-Operative Frozen Section Histology of the Pancreatic Resection Margins and Clinical Outcome of Patients with Adenocarcinoma of the Head of the Pancreas Undergoing Pancreaticoduodenectomy. Med Sci. Monit. 2018, 24, 4905–4913. [Google Scholar] [CrossRef]
- Yin, Z.; Zhou, Y.; Hou, B.; Ma, T.; Yu, M.; Zhang, C.; Lu, X.; Jian, Z. Revision of Surgical Margin under Frozen Section to Achieve R0 Status on Survival in Patients with Pancreatic Cancer. J. Gastrointest. Surg. 2018, 22, 1565–1575. [Google Scholar] [CrossRef] [PubMed]
- Petrucciani, N.; Nigri, G.; Debs, T.; Giannini, G.; Sborlini, E.; Antolino, L.; Aurello, P.; D’Angelo, F.; Gugenheim, J.; Ramacciato, G. Frozen section analysis of the pancreatic margin during pancreaticoduodenectomy for cancer: Does extending the resection to obtain a secondary R0 provide a survival benefit? Results of a systematic review. Pancreatology 2016, 16, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.; Smith, A.R.; Whelan, P.; Sutton, R.; Raraty, M.; Neoptolemos, J.; Ghaneh, P. Classification of R1 resections for pancreatic cancer: The prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology 2009, 55, 277–283. [Google Scholar] [CrossRef]
- Verbeke, C.S.; Leitch, D.; Menon, K.V.; McMahon, M.J.; Guillou, P.J.; Anthoney, A. Redefining the R1 resection in pancreatic cancer. Br. J. Surg. 2006, 93, 1232–1237. [Google Scholar] [CrossRef]
- Mathur, A.; Ross, S.B.; Luberice, K.; Kurian, T.; Vice, M.; Toomey, P.; Rosemurgy, A.S. Margin Status Impacts Survival after Pancreaticoduodenectomy but Negative Margins Should Not be Pursued. Am. Surg. 2014, 80, 353–360. [Google Scholar] [CrossRef]
- Springfeld, C.; Jager, D.; Buchler, M.W.; Strobel, O.; Hackert, T.; Palmer, D.H.; Neoptolemos, J.P. Chemotherapy for pancreatic cancer. Presse Med. 2019, 48, e159–e174. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Asbun, H.; Bain, A.; Behrman, S.W.; Benson, A.B., 3rd; Binder, E.; Cardin, D.B.; Cha, C.; et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2017, 15, 1028–1061. [Google Scholar] [CrossRef] [PubMed]
- Hirai, I.; Kimura, W.; Ozawa, K.; Kudo, S.; Suto, K.; Kuzu, H.; Fuse, A. Perineural Invasion in Pancreatic Cancer. Pancreas 2002, 24, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Crippa, S.; Pergolini, I.; Javed, A.A.; Honselmann, K.C.; Weiss, M.J.; Di Salvo, F.; Burkhart, R.; Zamboni, G.; Belfiori, G.; Ferrone, C.R.; et al. Implications of Perineural Invasion on Disease Recurrence and Survival After Pancreatectomy for Pancreatic Head Ductal Adenocarcinoma. Ann. Surg. 2022, 276, 378–385. [Google Scholar] [CrossRef]
- Takahashi, H.; Katsuta, E.; Yan, L.; Tokumaru, Y.; Katz, M.H.; Takabe, K. Transcriptomic Profile of Lymphovascular Invasion, a Known Risk Factor of Pancreatic Ductal Adenocarcinoma Metastasis. Cancers 2020, 12, 2033. [Google Scholar] [CrossRef] [PubMed]
- Heidt, D.G.; Burant, C.; Simeone, D.M. Total Pancreatectomy: Indications, Operative Technique, and Postoperative Sequelae. J. Gastrointest. Surg. 2007, 11, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Coco, D.; Leanza, S.; Guerra, F. Total Pancreatectomy: Indications, Advantages and Disadvantages—A Review. Maedica 2019, 14, 391–396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| cTP R0 (n = 21) | cTP R1 (n = 4) | p-Value | |
|---|---|---|---|
| Age (median, years) | 62.0 | 71.5 | 0.144 |
| Sex | 0.656 | ||
| Male | 13 (61.9) | 2 (50.0) | |
| Female | 8 (38.1) | 2 (50.0) | |
| BMI (kg/m2) | 23.0 ± 2.8 | 21.9 ± 1.4 | 0.499 |
| Preoperative DM | 0.238 | ||
| No | 9 (42.9) | 3 (75.0) | |
| Yes | 12 (57.1) | 1 (25.0) | |
| ASA score | 0.367 | ||
| 1 | 1 (4.8) | 1 (25.0) | |
| 2 | 19 (90.4) | 3 (75.0) | |
| 3 | 1 (4.8) | 0 (0.0) | |
| PreOP albumin (g/dL) | 4.1 ± 0.4 | 4.1 ± 0.3 | 0.779 |
| PreOP total protein (g/dL) | 6.9 ± 0.5 | 6.7 ± 0.7 | 0.470 |
| PreOP CA19-9 (U/mL) | 0.524 | ||
| 37 or below | 7 (33.3) | 2 (50.0) | |
| Higher than 37 | 14 (66.7) | 2 (50.0) | |
| PreOP total bilirubin (mg/dL) | 2.8 ± 3.7 | 6.2 ± 7.2 | 0.163 |
| PreOP biliary drainage | 0.656 | ||
| No | 13 (61.9) | 2 (50.0) | |
| Yes | 8 (38.1) | 2 (50.0) | |
| Neoadjuvant treatment | - | ||
| No | 21 (100.0) | 4 (100.0) | |
| Yes | 0 (0.0) | 0 (0.0) | |
| Other organ resection | - | ||
| No | 21 (100.0) | 4 (100.0) | |
| Yes | 0 (0.0) | 0 (0.0) | |
| Combined vascular surgery | 0.184 | ||
| No | 17 (81.0) | 2 (50.0) | |
| Yes | 4 (19.0) | 2 (50.0) | |
| Operation time (minutes) | 366.9 ± 57.8 | 456.0 ± 185.1 | 0.408 |
| Estimated blood loss (mL) | 728.6 ± 398.0 | 825.0 ± 623.8 | 0.688 |
| cTP R0 (n = 21) | PD R0 (n = 40) | p-Value | |
|---|---|---|---|
| Age (median, years) | 62.0 | 60.5 | 0.893 |
| Sex | 0.885 | ||
| Male | 13 (61.9) | 24 (60.0) | |
| Female | 8 (38.1) | 16 (40.0) | |
| BMI (kg/m2) | 22.9 ± 2.8 | 22.7 ± 3.9 | 0.471 |
| Preoperative DM | 0.202 | ||
| No | 9 (42.9) | 24 (60.0) | |
| Yes | 12 (57.1) | 16 (40.0) | |
| ASA score | 1.000 | ||
| 1 | 1 (4.8) | 2 (5.0) | |
| 2 | 19 (90.4) | 36 (90.0) | |
| 3 | 1 (4.8) | 2 (5.0) | |
| PreOP albumin (g/dL) | 4.1 ± 0.4 | 3.9 ± 0.4 | 0.025 |
| PreOP total protein (g/dL) | 6.9 ± 0.5 | 6.5 ± 0.5 | 0.006 |
| PreOP CA19-9 (U/mL) | 0.789 | ||
| 37 or below | 7 (33.3) | 12 (30.0) | |
| Higher than 37 | 14 (66.7) | 28 (70.0) | |
| PreOP total bilirubin (mg/dL) | 2.8 ± 3.7 | 5.9 ± 6.2 | 0.011 |
| PreOP biliary drainage | 0.016 | ||
| No | 13 (61.9) | 12 (30.0) | |
| Yes | 8 (38.1) | 28 (70.0) | |
| Neoadjuvant treatment | 0.465 | ||
| No | 21 (100.0) | 39 (97.5) | |
| Yes | 0 (0.0) | 1 (2.5) | |
| Other organ resection | 0.198 | ||
| No | 21 (100.0) | 37 (92.5) | |
| Yes | 0 (0.0) | 3 (7.5) | |
| Combined vascular surgery | 1.000 | ||
| No | 17 (81.0) | 33 (82.5) | |
| Yes | 4 (19.0) | 7 (17.5) | |
| Operation time (minutes) | 366.9 ± 57.8 | 340.7 ± 61.1 | 0.075 |
| Estimated blood loss (mL) | 728.6 ± 398.0 | 732.8 ± 629.2 | 0.225 |
| cTP R0 (n = 21) | PD R0 (n = 40) | p-Value | |
|---|---|---|---|
| T stage | 0.964 | ||
| T2 | 13 (61.9) | 25 (62.5) | |
| T3 | 8 (38.1) | 15 (37.5) | |
| Tumor size (cm) | 4.5 ± 3.4 | 3.8 ± 1.3 | 0.206 |
| N stage | 0.919 | ||
| N0 | 7 (33.3) | 14 (35.0) | |
| N1 | 10 (47.6) | 17 (42.5) | |
| N2 | 4 (19.1) | 9 (22.5) | |
| Harvested LN | 28.6 ± 14.5 | 22.7 ± 10.9 | 0.080 |
| Metastatic LN | 2.0 ± 2.5 | 3.1 ± 5.8 | 0.732 |
| M stage | - | ||
| M0 | 21 (100.0) | 40 (100.0) | |
| M1 | 0 (0.0) | 0 (0.0) | |
| Differentiation | 0.591 | ||
| Well | 1 (4.8) | 5 (12.5) | |
| Moderate | 12 (57.1) | 21 (52.5) | |
| Poor | 7 (33.3) | 9 (22.5) | |
| Unknown | 1 (4.8) | 5 (12.5) | |
| PNI | 1.000 | ||
| No | 0 (0.0) | 1 (2.5) | |
| Yes | 15 (71.4) | 27 (67.5) | |
| Unknown | 6 (28.6) | 12 (30.0) | |
| LVI | 1.000 | ||
| No | 1 (4.8) | 3 (7.5) | |
| Yes | 7 (33.3) | 11 (27.5) | |
| Unknown | 13 (61.9) | 26 (65.0) |
| cTP R0 (n = 21) | PD R0 (n = 40) | p-Value | |
|---|---|---|---|
| Clavien-Dindo classification | 0.323 | ||
| No complication | 15 (71.4) | 26 (65.0) | |
| I | 1 (4.8) | 3 (7.5) | |
| II | 1 (4.8) | 7 (17.5) | |
| IIIa | 3 (14.2) | 1 (2.5) | |
| IIIb | 1 (4.8) | 1 (2.5) | |
| IVa | 0 (0.0) | 2 (5.0) | |
| IVb | 0 (0.0) | 0 (0.0) | |
| V | 0 (0.0) | 0 (0.0) | |
| Length of stay (days) | 16.1 ± 6.3 | 16.5 ± 15.9 | 0.051 |
| Postoperative ICU stay (days) | 1.9 ± 2.0 | 1.2 ± 1.0 | 0.151 |
| In-hospital mortality | 0 (0.0) | 0 (0.0) | - |
| 90-day mortality | 1 (4.8) | 0 (0.0) | 0.344 |
| Re-admission within 90 days | 0 (0.0) | 2 (5.0) | 0.541 |
| Adjuvant treatment | 0.993 | ||
| No | 10 (47.6) | 19 (47.5) | |
| Yes | 11 (52.4) | 21 (52.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-H.; Yoon, S.-J.; Lee, O.-J.; Shin, S.-H.; Heo, J.-S.; Han, I.-W. Intraoperative Positive Pancreatic Parenchymal Resection Margin: Is It a True Indication of Completion Total Pancreatectomy after Partial Pancreatectomy for Pancreatic Ductal Adenocarcinoma? Curr. Oncol. 2022, 29, 5295-5305. https://doi.org/10.3390/curroncol29080420
Jung J-H, Yoon S-J, Lee O-J, Shin S-H, Heo J-S, Han I-W. Intraoperative Positive Pancreatic Parenchymal Resection Margin: Is It a True Indication of Completion Total Pancreatectomy after Partial Pancreatectomy for Pancreatic Ductal Adenocarcinoma? Current Oncology. 2022; 29(8):5295-5305. https://doi.org/10.3390/curroncol29080420
Chicago/Turabian StyleJung, Ji-Hye, So-Jeong Yoon, Ok-Joo Lee, Sang-Hyun Shin, Jin-Seok Heo, and In-Woong Han. 2022. "Intraoperative Positive Pancreatic Parenchymal Resection Margin: Is It a True Indication of Completion Total Pancreatectomy after Partial Pancreatectomy for Pancreatic Ductal Adenocarcinoma?" Current Oncology 29, no. 8: 5295-5305. https://doi.org/10.3390/curroncol29080420