
Is 20 Hz Whole-Body Vibration Training Better for Older Individuals than 40 Hz?

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. WBV Training
2.3. Measurement of the EMG Signals of Rectus Femoris Muscle
2.3.1. Measurement of the EMG Signals of Maximal Voluntary Isometric Contraction (MVIC)
2.3.2. Measurement of the Muscle Activity during Static Standing and WBV
2.3.3. Frequency Spectrum Analysis of the EMG Signals
2.4. Statistical Analysis
3. Results
3.1. Comparison between Different Age Groups during Same Frequency WBV
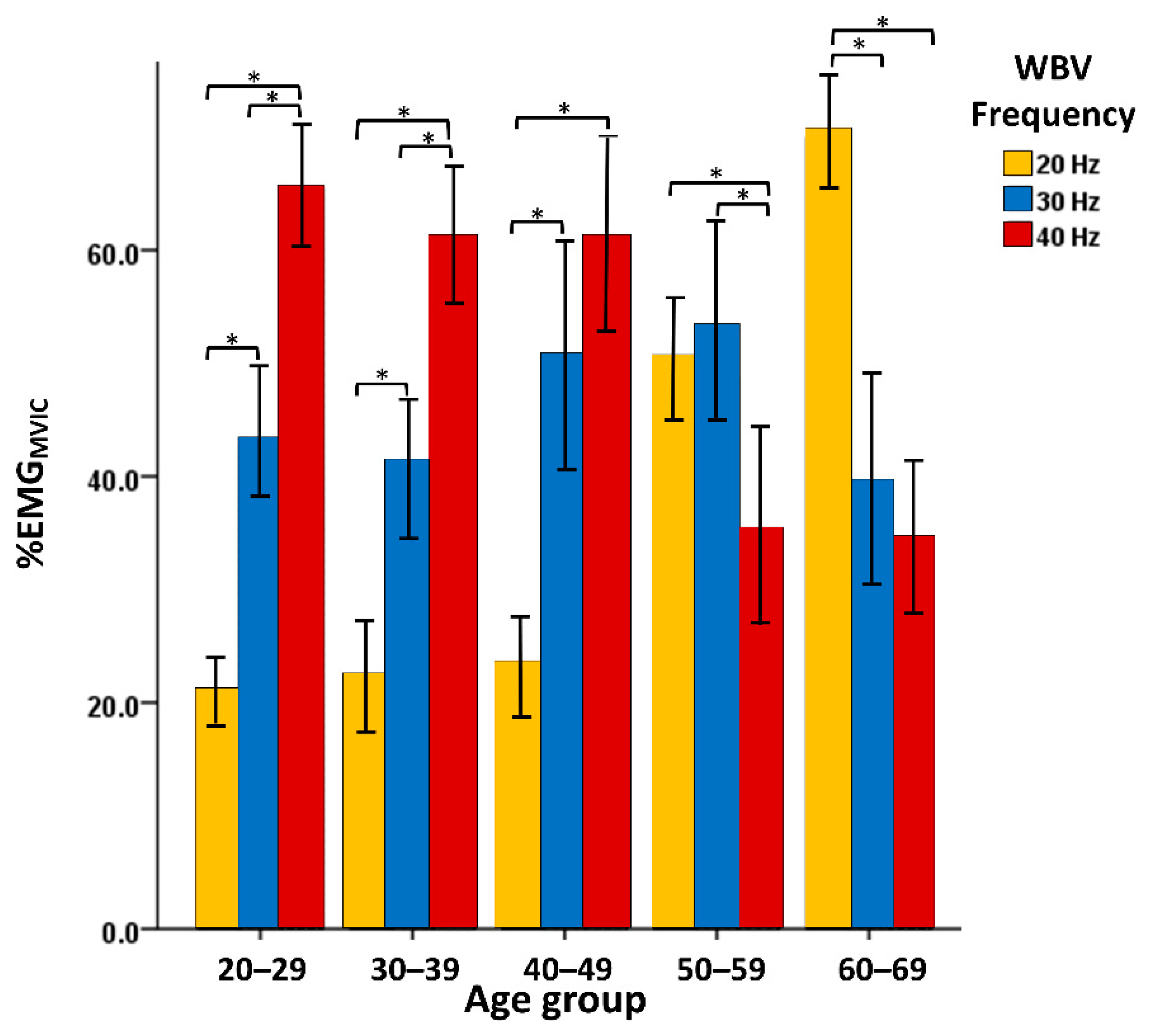
3.2. Interactions of Different Age Groups during WBV at Different Frequencies
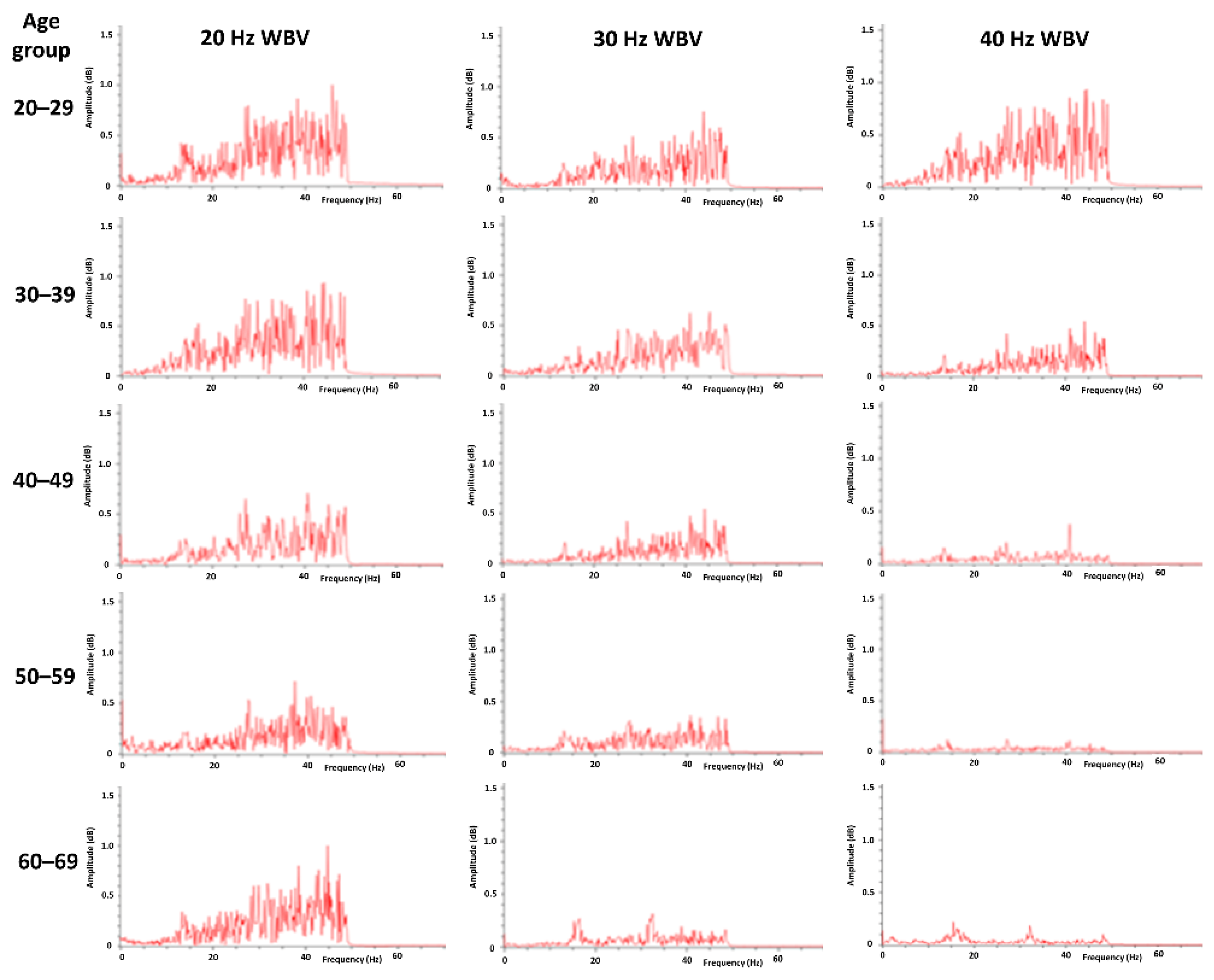
3.3. Frequency Spectrum Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alam, M.M.; Khan, A.A.; Farooq, M. Effect of whole-body vibration on neuromuscular performance: A literature review. Work 2018, 59, 571–583. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Sartor, F.; Winwood, K.; Stannard, S.R.; Narici, M.V.; Rittweger, J. A Comparison of the Physiologic Effects of Acute Whole-Body Vibration Exercise in Young and Older People. Arch. Phys. Med. Rehabil. 2008, 89, 815–821. [Google Scholar] [CrossRef]
- Nam, S.-S.; Sunoo, S.; Park, H.-Y.; Moon, H.-W. The effects of long-term whole-body vibration and aerobic exercise on body composition and bone mineral density in obese middle-aged women. J. Exerc. Nutr. Biochem. 2016, 20, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Tu, Y.-K.; Wang, T.-G.; Huang, Y.-T.; Chien, K.-L. Effects of resistance training, endurance training and whole-body vibration on lean body mass, muscle strength and physical performance in older people: A systematic review and network meta-analysis. Age Ageing 2018, 47, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Ritzmann, R.; Krämer, A.; Bernhardt, S.; Gollhofer, A. Whole Body Vibration Training—Improving Balance Control and Muscle Endurance. PLoS ONE 2014, 9, e89905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardinale, M.; Lim, J. Electromyography Activity of Vastus Lateralis Muscle During Whole-Body Vibrations of Different Frequencies. J. Strength Cond. Res. 2003, 17, 621–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, B.; Zurfluh, S.; Müller, R. Acute effects of whole-body vibration on trunk muscles in young healthy adults. J. Electromyogr. Kinesiol. 2011, 21, 450–457. [Google Scholar] [CrossRef]
- Bosco, C.; Cardinale, M.; Tsarpela, O. Influence of vibration on mechanical power and electromyogram activity in human arm flexor muscles. Graefe’s Arch. Clin. Exp. Ophthalmol. 1999, 79, 306–311. [Google Scholar] [CrossRef]
- Bazett-Jones, D.M.; Finch, H.W.; Dugan, E.L. Comparing the Effects of Various Whole-Body Vibration Accelerations on Counter-Movement Jump Performance. J. Sports Sci. Med. 2008, 7, 144–150. [Google Scholar]
- Luo, J.; McNamara, B.; Moran, K. The Use of Vibration Training to Enhance Muscle Strength and Power. Sports Med. 2005, 35, 23–41. [Google Scholar] [CrossRef]
- Pollock, R.D.; Woledge, R.; Mills, K.R.; Martin, F.C.; Newham, D. Muscle activity and acceleration during whole body vibration: Effect of frequency and amplitude. Clin. Biomech. 2010, 25, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Borges, D.T.; Macedo, L.; Lins, C.A.A.; Sousa, C.; Brasileiro, J.S. Effects of Whole Body Vibration on the Neuromuscular Amplitude of Vastus Lateralis Muscle. J. Sports Sci. Med. 2017, 16, 414–420. [Google Scholar] [PubMed]
- Hazell, T.J.; Jakobi, J.M.; Kenno, K.A. The effects of whole-body vibration on upper- and lower-body EMG during static and dynamic contractions. Appl. Physiol. Nutr. Metab. 2007, 32, 1156–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Süüden, E.; Ereline, J.; Gapeyeva, H.; Pääsuke, M. Low back muscle fatigue during Sørensen endurance test in patients with chronic low back pain: Relationship between electromyographic spectral compression and anthropometric characteristics. Electromyogr. Clin. Neurophysiol. 2008, 48, 185–192. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Krishnan, C.; Allen, E.J.; Ms, P.E.J.A. Effect of knee position on quadriceps muscle force steadiness and activation strategies. Muscle Nerve 2011, 43, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Girard, O.; Brocherie, F.; Millet, G.P. High Altitude Increases Alteration in Maximal Torque but Not in Rapid Torque Development in Knee Extensors after Repeated Treadmill Sprinting. Front. Physiol. 2016, 7, 97. [Google Scholar] [CrossRef] [Green Version]
- Andersen, L.L.; Magnusson, S.P.; Nielsen, M.; Haleem, J.; Poulsen, K.; Aagaard, P. Neuromuscular Activation in Conventional Therapeutic Exercises and Heavy Resistance Exercises: Implications for Rehabilitation. Phys. Ther. 2006, 86, 683–697. [Google Scholar] [CrossRef] [Green Version]
- Abercromby, A.F.J.; Amonette, W.E.; Layne, C.S.; Mcfarlin, B.K.; Hinman, M.R.; Paloski, W.H. Variation in Neuromuscular Responses during Acute Whole-Body Vibration Exercise. Med. Sci. Sports Exerc. 2007, 39, 1642–1650. [Google Scholar] [CrossRef] [Green Version]
- Macadam, P.; Feser, E.H. Examination of Gluteus Maximus Electromyographic Excitation Associated with Dynamic Hip Extension During Body Weight Exercise: A Systematic Review. Int. J. Sports Phys. Ther. 2019, 14, 14–31. [Google Scholar] [CrossRef] [Green Version]
- Boren, K.; Conrey, C.; Le Coguic, J.; Paprocki, L.; Voight, M.; Robinson, T.K. Electromyographic Analysis of Gluteus Medius And Gluteus Maximus During Rehabilitation Exercises. Int. J. Sports Phys. Ther. 2011, 6, 206–223. [Google Scholar] [PubMed]
- Ritzmann, R.; Kramer, A.; Gruber, M.; Gollhofer, A.; Taube, W. EMG activity during whole body vibration: Motion artifacts or stretch reflexes? Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 110, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, R.D.; Woledge, R.; Martin, F.C.; Newham, D. Effects of whole body vibration on motor unit recruitment and threshold. J. Appl. Physiol. 2012, 112, 388–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, S.Y.; Hsu, P.S.; Lai, C.L.; Liao, W.C.; Lee, M.C.; Wang, C.H. Effect of Two Frequencies of Whole-Body Vibration Training on Balance and Flexibility of the Elderly: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2016, 95, 730–737. [Google Scholar] [CrossRef]
- Jakobsson, F.; Borg, K. Fibre-type composition, structure and cytoskeletal protein location of fibres in anterior tibial muscle. Comparison between young adults and physically active aged humans. Acta Neuropathol. 1990, 80, 459–468. [Google Scholar] [CrossRef]
- Verdijk, L.B.; Koopman, R.; Schaart, G.; Meijer, K.; Savelberg, H.H.C.M.; van Loon, L.J.C. Satellite cell content is specifically reduced in type II skeletal muscle fibers in the elderly. Am. J. Physiol. Metab. 2007, 292, E151–E157. [Google Scholar] [CrossRef] [Green Version]
- Marín, P.J.; Herrero, A.J.; García-López, D.; Rhea, M.R.; López-Chicharro, J.; González-Gallego, J.; Garatachea, N. Acute Effects of Whole-Body Vibration on Neuromuscular Responses in Older Individuals: Implications for Prescription of Vibratory Stimulation. J. Strength Cond. Res. 2012, 26, 232–239. [Google Scholar] [CrossRef]
- Lienhard, K.; Cabasson, A.; Meste, O.; Colson, S.S. Comparison of sEMG processing methods during whole-body vibration exercise. J. Electromyogr. Kinesiol. 2015, 25, 833–840. [Google Scholar] [CrossRef]
- Fratini, A.; Cesarelli, M.; Bifulco, P.; Romano, M. Relevance of motion artifact in electromyography recordings during vibration treatment. J. Electromyogr. Kinesiol. 2009, 19, 710–718. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 20–29 Years Old Group (n = 21) | 30–39 Years Old Group (n = 18) | 40–49 Years Old Group (n = 18) | 50–59 Years Old Group (n = 20) | 60–69 Years Old Group (n = 21) | p-Value | |
|---|---|---|---|---|---|---|
| Age (years) | 24.2 (22.9–25.5) | 34.7 (33.3–36.1) | 46.1 (44.9–47.3) | 54.0 (52.6–55.4) | 65.7 (64.7–66.7) | <0.001 * |
| Sex (Male/Female) | 12/9 | 9/9 | 11/7 | 10/10 | 9/12 | 0.811 |
| Height (cm) | 168.6 (164.0–173.3) | 162.3 (157.5–167.0) | 164.1 (160.4–167.9) | 164.0 (160.8–167.2) | 160.2 (157.2–163.2) | 0.024 * |
| Body Mass (kg) | 62.0 (56.4–67.7) | 61.2 (54.5–67.9) | 68.2 (62.8–73.6) | 64.8 (58.9–70.6) | 61.9 (57.3–66.5) | 0.357 |
| Body Mass Index | 21.6 (20.5–22.7) | 23.0 (21.4–24.6) | 25.3 (23.6–27.0) | 23.9 (22.3–25.6) | 23.6 (22.7–25.3) | 0.007 * |
| EMGMVIC (μV) | 321.4 (289.5–353.4) | 296.4 (273.5–369.6) | 275.0 (226.0–324.0) | 210.8 (167.8–253.8) | 182.8 (156.2–209.4) | <0.001 * |
| SS_EMGMVIC (%) | 7.6 (6.0–9.24) | 8.5 (6.6–10.4) | 8.1 (6.2–9.9) | 15.3 (11.8–18.9) | 19.0 (15.8–22.1) | <0.001 * |
| WBV Frequency | 20–29 Years Old Group (n = 21) | 30–39 Years Old Group (n = 18) | 40–49 Years Old Group (n = 18) | 50–59 Years Old Group (n = 20) | 60–69 Years Old Group (n = 21) | p-Value |
|---|---|---|---|---|---|---|
| 20 Hz | 21.4 d,e (18.0–24.7) | 22.2 d,e (17.1–27.3) | 22.7 d,e (18.3–27.1) | 49.7 a,b,c,e (44.4–54.9) | 69.2 a,b,c,d (62.8–75.7) | <0.001 * |
| 30 Hz | 43.7 (38.0–49.4) | 40.3 (34.1–46.6) | 50.0 (40.4–59.7) | 53.3 (44.2–62.3) | 39.9 (30.8–49.0) | 0.058 |
| 40 Hz | 64.7 d,e (58.9–70.6) | 60.6 d,e (54.4–66.8) | 60.4 d,e (51.7–69.1) | 35.6 a,b,c (26.8–44.4) | 34.4 a,b,c (27.2–41.6) | <0.001 * |
| p-Value | <0.001 * | <0.001 * | <0.001 * | 0.006 * | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, S.-Y.; Ko, C.-P.; Tseng, C.-Y.; Huang, W.-C.; Lai, C.-L.; Wang, C.-H. Is 20 Hz Whole-Body Vibration Training Better for Older Individuals than 40 Hz? Int. J. Environ. Res. Public Health 2021, 18, 11942. https://doi.org/10.3390/ijerph182211942
Tseng S-Y, Ko C-P, Tseng C-Y, Huang W-C, Lai C-L, Wang C-H. Is 20 Hz Whole-Body Vibration Training Better for Older Individuals than 40 Hz? International Journal of Environmental Research and Public Health. 2021; 18(22):11942. https://doi.org/10.3390/ijerph182211942
Chicago/Turabian StyleTseng, Shiuan-Yu, Chung-Po Ko, Chin-Yen Tseng, Wei-Ching Huang, Chung-Liang Lai, and Chun-Hou Wang. 2021. "Is 20 Hz Whole-Body Vibration Training Better for Older Individuals than 40 Hz?" International Journal of Environmental Research and Public Health 18, no. 22: 11942. https://doi.org/10.3390/ijerph182211942