
Nasopharyngeal and Peripheral Blood Type II Interferon Signature Evaluation in Infants during Respiratory Syncytial Virus Infection
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. mRNA Isolation and Real-Time PCR
2.3. IFN Signature Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Populations
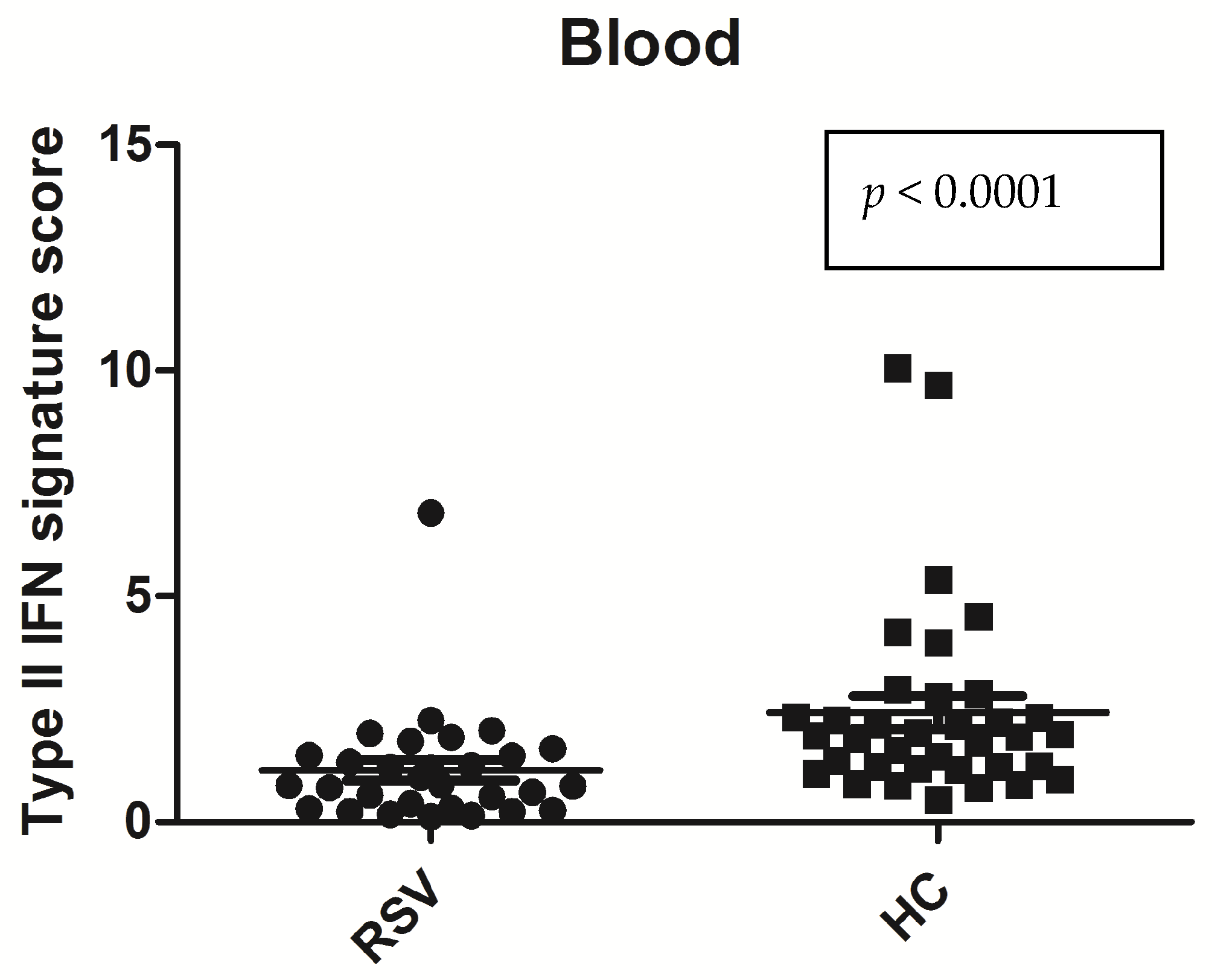
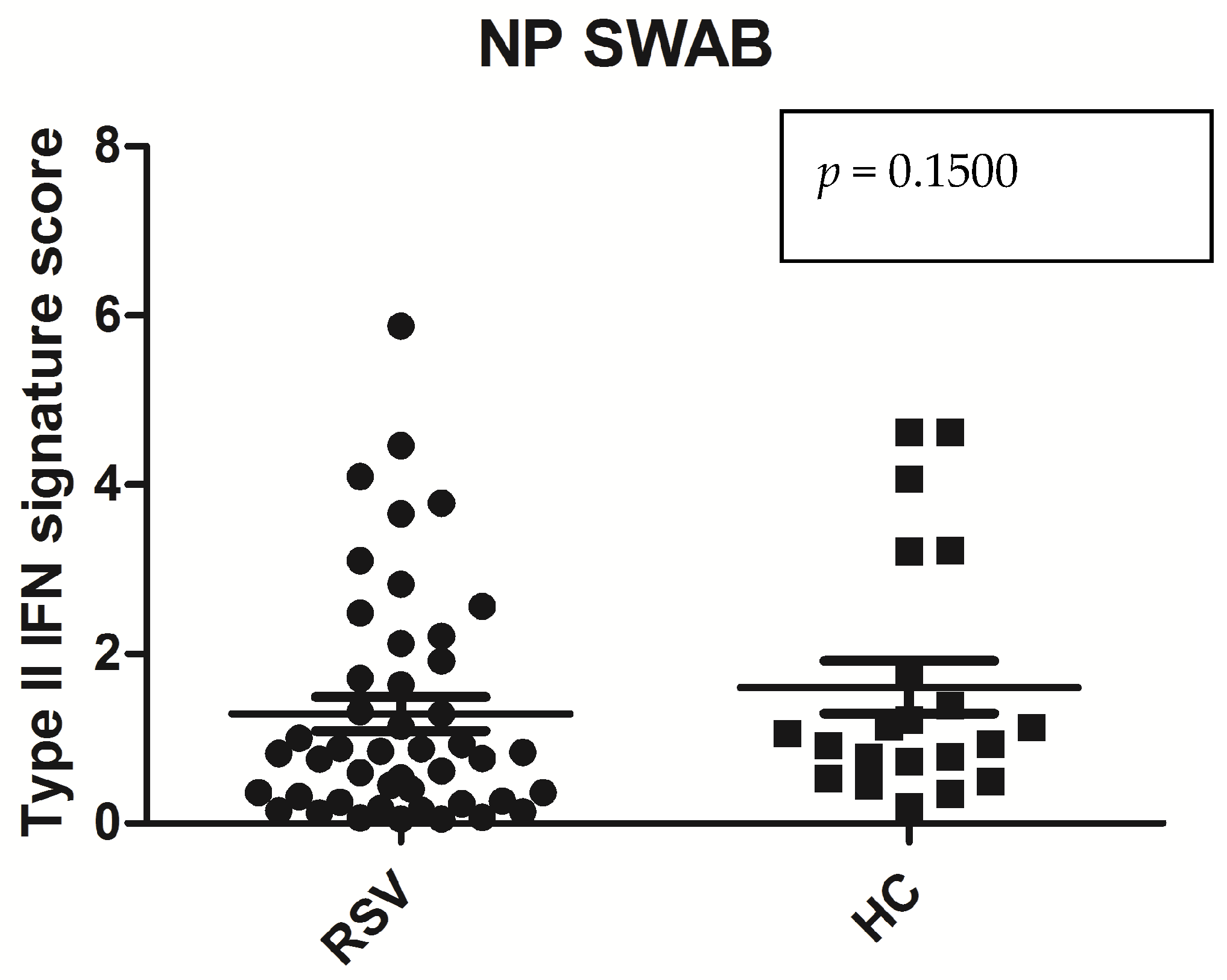
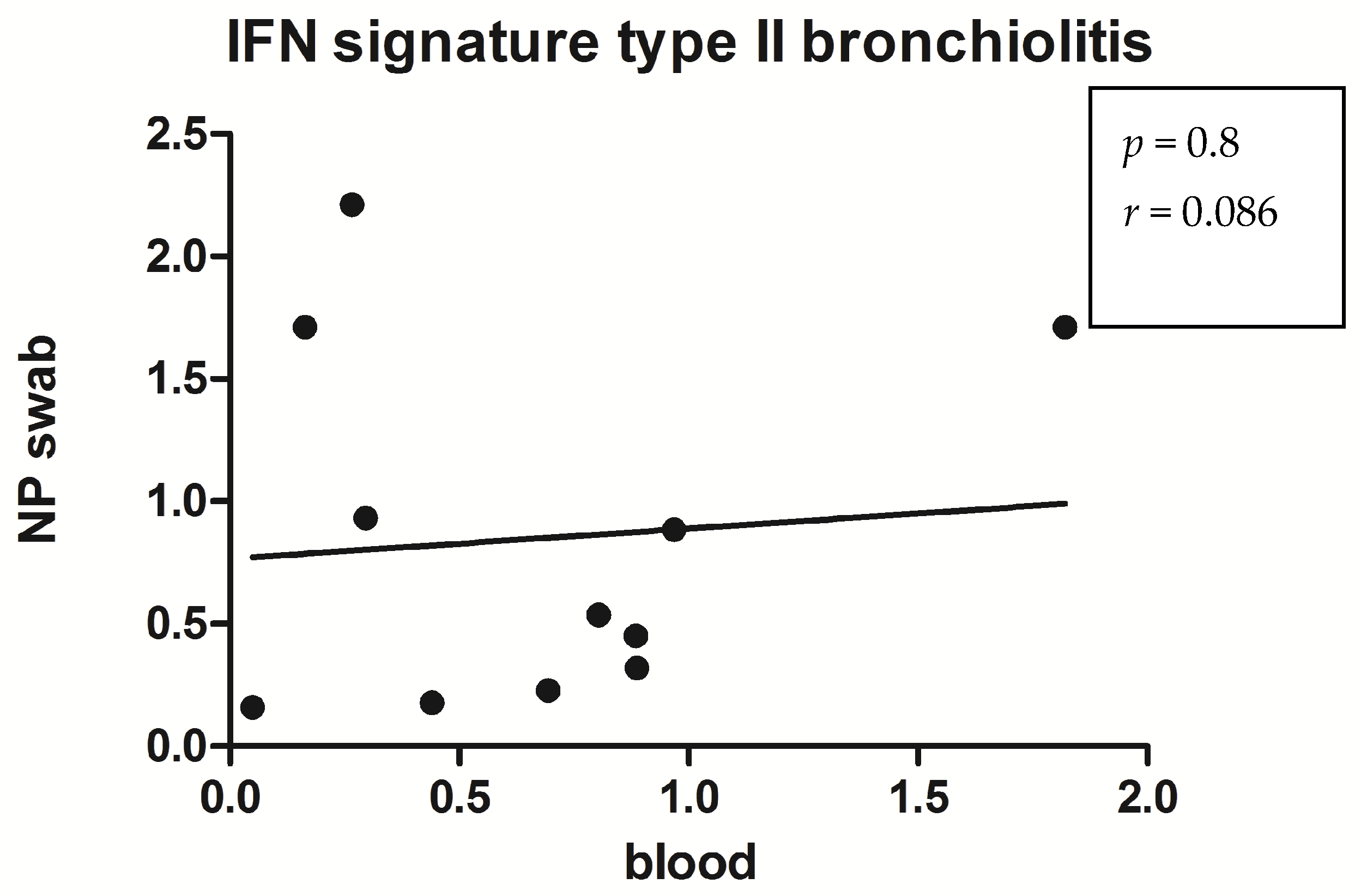
3.2. IFN-Stimulated Genes Expression Evaluated by qPCR
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hall, C.B.; Weinberg, G.A.; Iwane, M.K.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Auinger, P.; Griffin, M.R.; Poehling, K.A.; Erdman, D.; et al. The burden of respiratory syncytial virus infection in young children. N. Engl. J. Med. 2009, 360, 588–598. [Google Scholar] [CrossRef]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Vennard, S.; Mahdy, S.; Nair, H.; RESCEU investigators. Risk Factors for Poor Outcome or Death in Young Children With Respiratory Syncytial Virus-Associated Acute Lower Respiratory Tract Infection: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2022, 226 (Suppl. 1), S10–S16. [Google Scholar] [CrossRef] [PubMed]
- Kuhdari, P.; Brosio, F.; Malaventura, C.; Stefanati, A.; Orsi, A.; Icardi, G.; Gabutti, G. Human respiratory syncytial virus and hospitalization in young children in Italy. Ital. J. Pediatr. 2018, 44, 50. [Google Scholar] [CrossRef] [PubMed]
- Rima, B.; Collins, P.; Easton, A.; Fouchier, R.; Kurath, G.; Lamb, R.A.; Lee, B.; Maisner, A.; Rota, P.; Wang, L.; et al. ICTV virus taxonomy profile: Pneumoviridae. J. Gen. Virol. 2017, 98, 2912–2913. [Google Scholar] [CrossRef]
- Peri, F.; Lorenzon, B.; Cason, C.; Amaddeo, A.; Norbedo, S.; Comar, M.; Barbi, E.; Cozzi, G. Urgent Hospitalizations Related to Viral Respiratory Disease in Children during Autumn and Winter Seasons 2022/2023. Viruses 2023, 15, 2425. [Google Scholar] [CrossRef]
- Rector, A.; Bloemen, M.; Thijssen, M.; Pussig, B.; Beuselinck, K.; Van Ranst, M.; Wollants, E. Respiratory Viruses in Wastewater Compared with Clinical Samples, Leuven, Belgium. Emerg. Infect. Dis. 2024, 30, 141–145. [Google Scholar] [CrossRef]
- Morgan, N.; Buys, H.; Muloiwa, R. RSV infection in children hospitalised with severe lower respiratory tract infection in a low-middle-income setting: A cross-sectional observational study. PLoS ONE 2023, 18, e0291433. [Google Scholar] [CrossRef]
- Feiler, M.O.; Yucel, R.; Liu, Z.; Caserta, M.; Lawrence, B.P.; Pason, C.H.; Hardy, D.J.; Thevenet-Morrison, K.; Dozier, A.; Jusko, T.A. Trends and Non-Clinical Predictors of Respiratory Syncytial Virus (RSV) and Influenza Diagnosis in an Urban Pediatric Population. Int. J. Pediatr. Res. 2023, 9, 112. [Google Scholar] [CrossRef]
- Schreiber, G. The molecular basis for differential type I interferon signaling. J. Biol. Chem. 2017, 292, 7285–7294. [Google Scholar] [CrossRef]
- Park, A.; Iwasaki, A. Type I and type III interferons—Induction, signaling, evasion, and application to combat COVID-19. Cell Host Microbe 2020, 27, 870–878. [Google Scholar] [CrossRef]
- Nile, S.H.; Nile, A.; Qiu, J.; Li, L.; Jia, X.; Kai, G. COVID-19: Pathogenesis, cytokine storm and therapeutic potential of interferons. Cytokine Growth Factor. Rev. 2020, 53, 66–70. [Google Scholar] [CrossRef]
- Chen, S.; Bonifati, S.; Qin, Z.; St Gelais, C.; Kodigepalli, K.M.; Barrett, B.S.; Kim, S.H.; Antonucci, J.M.; Ladner, K.J.; Buzovetsky, O.; et al. SAMHD1 suppresses innate immune responses to viral infections and inflammatory stimuli by inhibiting the NF-κB and interferon pathways. Proc. Natl. Acad. Sci. USA 2018, 115, E3798–E3807. [Google Scholar] [CrossRef] [PubMed]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef]
- Salaun, B.; De Smedt, J.; Vernhes, C.; Moureau, A.; Öner, D.; Bastian, A.R.; Janssens, M.; Balla-Jhagjhoorsingh, S.; Aerssens, J.; Lambert, C.; et al. T cells, more than antibodies, may prevent symptoms developing from respiratory syncytial virus infections in older adults. Front. Immunol. 2023, 14, 1260146. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, L.F.; Xu, J.L.; Shang, S.Q. Epidemiological and Immunological Features of Influenza Viruses in Hospitalized Children with Influenza Illness in Hangzhou. Fetal Pediatr. Pathol. 2020, 39, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Gut, W.; Pancer, K.; Abramczuk, E.; Cześcik, A.; Dunal-Szczepaniak, M.; Lipka, B.; Litwińska, B. RSV respiratory infection in children under 5 y.o.--dynamics of the immune response Th1/Th2 and IgE. Przegl. Epidemiol. 2013, 67, 17–22. [Google Scholar] [PubMed]
- Tovo, P.A.; Garazzino, S.; Daprà, V.; Pruccoli, G.; Calvi, C.; Mignone, F.; Alliaudi, C.; Denina, M.; Scolfaro, C.; Zoppo, M.; et al. COVID-19 in Children: Expressions of Type I/II/III Interferons, TRIM28, SETDB1, and Endogenous Retroviruses in Mild and Severe Cases. Int. J. Mol. Sci. 2021, 22, 7481. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Ashkar, A.A. The Dual Nature of Type I and Type II Interferons. Front. Immunol. 2018, 9, 2061. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Li, Z.; Hyseni, X.; Schmitt, M.; Devlin, R.B.; Karoly, E.D.; Soukup, J.M. Identification of gene biomarkers for respiratory syncytial virus infection in a bronchial epithelial cell line. Genom. Med. 2008, 2, 113–125. [Google Scholar] [CrossRef]
- Yamada, Y.; Matsumoto, K.; Hashimoto, N.; Saikusa, M.; Homma, T.; Yoshihara, S.; Saito, H. Effect of Th1/Th2 cytokine pretreatment on RSV-induced gene expression in airway epithelial cells. Int. Arch. Allergy Immunol. 2011, 154, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Martínez, I.; Lombardía, L.; García-Barreno, B.; Domínguez, O.; Melero, J.A. Distinct gene subsets are induced at different time points after human respiratory syncytial virus infection of A549 cells. J. Gen. Virol. 2007, 88, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; San Juan, H.; Kumar, M.; Behera, A.K.; Mohapatra, A.; Hellermann, G.R.; Mane, S.; Lockey, R.F.; Mohapatra, S.S. Respiratory syncytial virus infection activates STAT signaling in human epithelial cells. Biochem. Biophys. Res. Commun. 2003, 306, 616–622. [Google Scholar] [CrossRef]
- Tian, B.; Zhang, Y.; Luxon, B.A.; Garofalo, R.P.; Casola, A.; Sinha, M.; Brasier, A.R. Identification of NF-kappaB-dependent gene networks in respiratory syncytial virus-infected cells. J. Virol. 2002, 76, 6800–6814. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luxon, B.A.; Casola, A.; Garofalo, R.P.; Jamaluddin, M.; Brasier, A.R. Expression of respiratory syncytial virus-induced chemokine gene networks in lower airway epithelial cells revealed by cDNA microarrays. J. Virol. 2001, 75, 9044–9058. [Google Scholar] [CrossRef]
- Rudd, B.D.; Burstein, E.; Duckett, C.S.; Li, X.; Lukacs, N.W. Differential role for TLR3 in respiratory syncytial virus-induced chemokine expression. J. Virol. 2005, 79, 3350–3357. [Google Scholar] [CrossRef]
- Bhoj, V.G.; Sun, Q.; Bhoj, E.J.; Somers, C.; Chen, X.; Torres, J.P.; Mejias, A.; Gomez, A.M.; Jafri, H.; Ramilo, O.; et al. MAVS and MyD88 are essential for innate immunity but not cytotoxic T lymphocyte response against respiratory syncytial virus. Proc. Natl. Acad. Sci. USA 2008, 105, 14046–14051. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.; Pennings, J.; Hodemaekers, H.; Buisman, A.; van Oosten, M.; de Rond, L.; Oztürk, K.; Dormans, J.; Kimman, T.; Hoebee, B. Host transcription profiles upon primary respiratory syncytial virus infection. J. Virol. 2007, 81, 5958–5967. [Google Scholar] [CrossRef]
- Schuurhof, A.; Bont, L.; Pennings, J.L.; Hodemaekers, H.M.; Wester, P.W.; Buisman, A.; de Rond, L.C.; Widjojoatmodjo, M.N.; Luytjes, W.; Kimpen, J.L.; et al. Gene expression differences in lungs of mice during secondary immune responses to respiratory syncytial virus infection. J. Virol. 2010, 84, 9584–9594. [Google Scholar] [CrossRef]
- Culley, F.J.; Pennycook, A.M.; Tregoning, J.S.; Hussell, T.; Openshaw, P.J. Differential chemokine expression following respiratory virus infection reflects Th1- or Th2-biased immunopathology. J. Virol. 2006, 80, 4521–4527. [Google Scholar] [CrossRef]
- Pennings, J.L.; Schuurhof, A.; Hodemaekers, H.M.; Buisman, A.; de Rond, L.C.; Widjojoatmodjo, M.N.; Luytjes, W.; Kimpen, J.L.; Bont, L.; Janssen, R. Systemic signature of the lung response to respiratory syncytial virus infection. PLoS ONE 2011, 6, e21461. [Google Scholar] [CrossRef] [PubMed]
- Bendelja, K.; Vojvoda, V.; Aberle, N.; Cepin-Bogovic, J.; Gagro, A.; Mlinaric-Galinovic, G.; Rabatic, S. Decreased Toll-like receptor 8 expression and lower TNF-alpha synthesis in infants with acute RSV infection. Respir. Res. 2011, 11, 143. [Google Scholar] [CrossRef] [PubMed]
- Fjaerli, H.O.; Bukholm, G.; Krog, A.; Skjaeret, C.; Holden, M.; Nakstad, B. Whole blood gene expression in infants with respiratory syncytial virus bronchiolitis. BMC Infect. Dis. 2006, 6, 175. [Google Scholar] [CrossRef] [PubMed]
- Fjaerli, H.O.; Bukholm, G.; Skjaeret, C.; Holden, M.; Nakstad, B. Cord blood gene expression in infants hospitalized with respiratory syncytial virus bronchiolitis. J. Infect. Dis. 2007, 196, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Zaas, A.K.; Chen, M.; Varkey, J.; Veldman, T.; Hero, A.O., 3rd; Lucas, J.; Huang, Y.; Turner, R.; Gilbert, A.; Lambkin-Williams, R.; et al. Gene expression signatures diagnose influenza and other symptomatic respiratory viral infections in humans. Cell Host Microbe 2009, 6, 207–217. [Google Scholar] [PubMed]
- Scagnolari, C.; Midulla, F.; Pierangeli, A.; Moretti, C.; Bonci, E.; Berardi, R.; De Angelis, D.; Selvaggi, C.; Di Marco, P.; Girardi, E.; et al. Gene expression of nucleic acid-sensing pattern recognition receptors in children hospitalized for respiratory syncytial virus-associated acute bronchiolitis. Clin. Vaccine Immunol. 2009, 16, 816–823. [Google Scholar] [CrossRef]
- Bucasas, K.L.; Mian, A.I.; Demmler-Harrison, G.J.; Caviness, A.C.; Piedra, P.A.; Franco, L.M.; Shaw, C.A.; Zhai, Y.; Wang, X.; Bray, M.S.; et al. Global gene expression profiling in infants with acute respiratory syncytial virus broncholitis demonstrates systemic activation of interferon signaling networks. Pediatr. Infect. Dis. J. 2013, 32, e68–e76. [Google Scholar] [CrossRef]
- Mejias, A.; Dimo, B.; Suarez, N.M.; Garcia, C.; Suarez-Arrabal, M.C.; Jartti, T.; Blankenship, D.; Jordan-Villegas, A.; Ardura, M.I.; Xu, Z.; et al. Whole blood gene expression profiles to assess pathogenesis and disease severity in infants with respiratory syncytial virus infection. PLoS Med. 2013, 10, e1001549. [Google Scholar] [CrossRef]
- van den Kieboom, C.H.; Ahout, I.M.; Zomer, A.; Brand, K.H.; de Groot, R.; Ferwerda, G.; de Jonge, M.I. Nasopharyngeal gene expression, a novel approach to study the course of respiratory syncytial virus infection. Eur. Respir. J. 2015, 45, 718–725. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- van Bleek, G.M.; Osterhaus, A.D.M.E.; de Swart, R.L. RSV 2010: Recent advances in research on respiratory syncytial virus and other pneumoviruses. Vaccine 2011, 29, 7285–7291. [Google Scholar] [CrossRef]
- Baker, K.A.; Ryan, M.E. Rsv infection in infants and young children. Postgrad. Med. 1999, 106, 97–111. [Google Scholar] [CrossRef]
- Mejías, A.; Chávez-Bueno, S.; Jafri, H.S.; Ramilo, O. Respiratory syncytial virus infections: Old challenges and new opportunities. Pediatr. Infect. Dis. J. 2005, 24, S189–S197. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Braciale, T.J. Respiratory syncytial virus infection suppresses lung CD8+ T-cell effector activity and peripheral CD8+ T-cell memory in the respiratory tract. Nat. Med. 2002, 8, 54–60. [Google Scholar] [CrossRef] [PubMed]
- González, P.A.; Prado, C.E.; Leiva, E.D.; Carreño, L.J.; Bueno, S.M.; Riedel, C.A.; Kalergis, A.M. Respiratory syncytial virus impairs T cell activation by preventing synapse assembly with dendritic cells. Proc. Natl. Acad. Sci. USA 2008, 105, 14999–15004. [Google Scholar] [CrossRef] [PubMed]
- Openshaw, P.J.; Chiu, C. Protective and dysregulated T cell immunity in RSV infection. Curr. Opin. Virol. 2013, 3, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Semple, M.G.; Dankert, H.M.; Ebrahimi, B.; Correia, J.B.; Booth, J.A.; Stewart, J.P.; Smyth, R.L.; Hart, C.A. Severe respiratory syncytial virus bronchiolitis in infants is associated with reduced airway interferon gamma and substance P. PLoS ONE 2007, 2, e1038. [Google Scholar] [CrossRef] [PubMed]
- Thwaites, R.S.; Coates, M.; Ito, K.; Ghazaly, M.; Feather, C.; Abdulla, F.; Tunstall, T.; Jain, P.; Cass, L.; Rapeport, G.; et al. Reduced nasal viral load and IFN responses in infants with respiratory syncytial virus bronchiolitis and respiratory failure. Am. J. Respir. Crit. Care Med. 2018, 198, 1074–1084. [Google Scholar] [CrossRef]
- Chen, Z.M.; Mao, J.H.; Du, L.Z.; Tang, Y.M. Association of cytokine responses with disease severity in infants with respiratory syncytial virus infection. Acta Paediatr. 2002, 91, 914–922. [Google Scholar] [CrossRef]
- Öner, D.; Drysdale, S.B.; McPherson, C.; Lin, G.L.; Janet, S.; Broad, J.; Pollard, A.J.; Aerssens, J.; RESCEU Investigators. Biomarkers for Disease Severity in Children Infected With Respiratory Syncytial Virus: A Systematic Literature Review. J. Infect. Dis. 2020, 222 (Suppl. 7), S648–S657. [Google Scholar] [CrossRef]
- Lopez, J.; Mommert, M.; Mouton, W.; Pizzorno, A.; Brengel-Pesce, K.; Mezidi, M.; Pizzorno, A.; Brengel-Pesce, K.; Mezidi, M.; Villard, M.; et al. Early nasal type I IFN immunity against SARS-CoV-2 is compromised in patients with autoantibodies against type I IFNs. J. Exp. Med. 2021, 218, e20211211. [Google Scholar] [CrossRef]
- Zedan, A.; Winters, A.D.; Yu, W.; Wang, S.; Ren, Y.; Takeshita, A.; Gong, Q. Antiviral Functions of Type I and Type III Interferons in the Olfactory Epithelium. Biomolecules 2023, 13, 1762. [Google Scholar] [CrossRef] [PubMed]
- Aberle, J.H.; Aberle, S.W.; Rebhandl, W.; Pracher, E.; Kundi, M.; Popow-Kraupp, T. Decreased interferon-gamma response in respiratory syncytial virus compared to other respiratory viral infections in infants. Clin. Exp. Immunol. 2004, 137, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.; Shaw, A.; Kakakios, A.; Isaacs, D. Interferon-gamma levels in nasopharyngeal secretions of infants with respiratory syncytial virus and other respiratory viral infections. Clin. Exp. Immunol. 2003, 131, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Renzi, P.M.; Turgeon, J.P.; Marcotte, J.E.; Drblik, S.P.; Bérubé, D.; Gagnon, M.F.; Spier, S. Reduced IFN-g production in infants with bronchiolitis and asthma. Am. J. Respir. Crit. Care Med. 1999, 159, 1417–1422. [Google Scholar] [CrossRef]
- Bendelja, K.; Gagro, A.; Bace, A.; Lokar-Kolbas, R.; Krsulovic-Hresic, V.; Drazenovic, V.; Mlinaric-Galinovic, G.; Rabatic, S. Predominant type-2 response in infants with respiratory syncytial virus (RSV) infection demonstrated by cytokine flow cytometry. Clin. Exp. Immunol. 2000, 121, 332–338. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Bronchiolitis (30) * | Healthy Controls (36) * | p Value § |
|---|---|---|---|
| Age (days) | 86 ± 84 | 92 ± 101 | 0.585 |
| White blood cells count (cells × 109/L) | 9670 ± 650 | 8830 ± 992 | 0.386 |
| Neutrophils (cells × 109/L) | 2834 ± 1129 | 3228 ± 1010 | 0.545 |
| Lymphocytes (cells × 109/L) | 5400 ± 1998 | 4180 ± 1883 | 0.032 ° |
| Eosinophils (cells × 109/L) | 302 ± 100 | 443 ± 80 | 0.310 |
| Monocytes (cells × 109/L) | 1503 ± 1030 | 632 ± 301 | <0.0001 ° |
| CXCL9 | CXCL10 | Ido1 | IFN | IFN Score |
|---|---|---|---|---|
| 0.157065 | 8.18543 | 0.286978 | 0.164163 | 0.22557 |
| 0.624713 | 0.679134 | 0.553085 | 0.197167 | 0.588899 |
| 0.061826 | 0.16016 | 0.069976 | 0.311058 | 0.115068 |
| 0.931124 | 2.576414 | 1.962246 | 0.549406 | 1.446685 |
| 0.587774 | 2.936548 | 4.420878 | 0.804047 | 1.870297 |
| 1.766501 | 3.628207 | 1.800975 | 0.693805 | 1.783738 |
| 0.302649 | 1.540725 | 1.108899 | 2.195808 | 1.324812 |
| 0.58293 | 1.376756 | 1.961242 | 0.326026 | 0.979843 |
| 0.937127 | 35.02627 | 1.534166 | 0.776836 | 1.235647 |
| 0.728682 | 143.6117 | 12.19011 | 1.500456 | 6.845283 |
| 0.09159 | 25.39361 | 2.204072 | 0.203047 | 1.203559 |
| 0.660717 | 51.14568 | 3.818783 | 0.229422 | 2.23975 |
| 0.068105 | 0.242614 | 0.109202 | 0.234683 | 0.171942 |
| 0.127123 | 0.490703 | 0.448894 | 0.170006 | 0.30945 |
| 0.457043 | 9.124063 | 0.856635 | 0.262696 | 0.656839 |
| 1.638153 | 6.903458 | 0.736292 | 0.049596 | 1.187223 |
| 2.700755 | 6.703653 | 0.173626 | 1.332774 | 2.016765 |
| 0.282434 | 0.369647 | 0.176321 | 0.295971 | 0.289203 |
| 0.470063 | 14.85163 | 1.255824 | 1.693257 | 1.474541 |
| 0.802751 | 270.6202 | 3.105014 | 0.606671 | 1.953883 |
| 0.229872 | 3.890983 | 0.424244 | 0.382459 | 0.403351 |
| 0.693212 | 4.8035 | 0.830444 | 0.321862 | 0.761828 |
| 0.159718 | 0.358076 | 0.063926 | 0.44009 | 0.258897 |
| 0.372456 | 1.831377 | 0.710723 | 0.885488 | 0.798105 |
| 1.423442 | 1.934601 | 0.320828 | 1.820754 | 1.622098 |
| 0.276544 | 1.094884 | 0.69411 | 0.886863 | 0.790487 |
| 0.189038 | 0.331033 | 0.059418 | 0.266275 | 0.227656 |
| 0.060295 | 0.15324 | 0.119145 | 0.968841 | 0.136193 |
| 0.174432 | 0.771439 | 0.319235 | 0.974291 | 0.545337 |
| 0.45667 | 13.39745 | 0.651593 | 0.98962 | 0.820607 |
| CXCL9 | CXCL10 | Ido1 | IFN | IFN Score |
|---|---|---|---|---|
| 0.927221 | 5.927591 | 2.814915 | 1.059956 | 1.937436 |
| 0.807148 | 0.578726 | 1.007283 | 0.800781 | 0.803965 |
| 0.961704 | 2.670438 | 0.346059 | 0.938156 | 0.94993 |
| 0.553646 | 3.473331 | 2.624912 | 1.69073 | 2.157821 |
| 0.558547 | 3.529864 | 1.485558 | 0.880558 | 1.183058 |
| 1.166531 | 6.642831 | 3.234286 | 1.094232 | 2.200409 |
| 0.574403 | 0.930456 | 0.491075 | 0.977094 | 0.752429 |
| 0.703173 | 3.167205 | 2.206281 | 1.306828 | 1.756554 |
| 0.593752 | 2.681653 | 2.472985 | 1.178443 | 1.825714 |
| 0.526364 | 2.241326 | 2.699156 | 0.94144 | 1.591383 |
| 0.789334 | 16.15611 | 1.675641 | 0.349211 | 1.232488 |
| 0.449238 | 1.028112 | 1.120321 | 2.891309 | 1.074216 |
| 3.026584 | 33.28678 | 3.15599 | 4.782118 | 3.969054 |
| 1.415051 | 6.074084 | 2.684512 | 1.954509 | 2.31951 |
| 1.233968 | 5.30949 | 3.012727 | 2.855546 | 2.934137 |
| 1.818892 | 54.26082 | 2.671744 | 1.829073 | 2.250408 |
| 1.482601 | 7.572696 | 3.070401 | 5.337788 | 4.204095 |
| 0.198741 | 1.123516 | 7.019939 | 1.755256 | 1.439386 |
| 0.246297 | 2.135114 | 2.707466 | 1.617702 | 1.876408 |
| 0.315997 | 3.798261 | 1.361492 | 0.123542 | 0.838745 |
| 0.547174 | 2.802106 | 3.099739 | 2.73358 | 2.767843 |
| 0.299992 | 31.17147 | 14.73604 | 5.374277 | 10.05516 |
| 0.62112 | 1.344691 | 3.800596 | 1.08666 | 1.215676 |
| 0.927419 | 12.62865 | 9.230163 | 1.47954 | 5.354851 |
| 0.525293 | 3.374039 | 2.958201 | 2.699701 | 2.828951 |
| 0.473346 | 7.375175 | 1.825008 | 1.997246 | 1.911127 |
| 0.831074 | 5.225671 | 0.523769 | 1.607206 | 1.21914 |
| 0.667976 | 1.468509 | 0.821468 | 0.810344 | 0.815906 |
| 1.640676 | 11.53084 | 1.537516 | 2.962262 | 2.301469 |
| 4.472612 | 44.21708 | 10.61164 | 8.757177 | 9.684408 |
| 0.422769 | 1.28918 | 1.027396 | 2.246802 | 1.158288 |
| 0.554591 | 2.148308 | 2.335841 | 0.387631 | 1.35145 |
| 4.242832 | 20.40956 | 2.606556 | 4.880706 | 4.561769 |
| 0.927105 | 3.324605 | 0.747185 | 3.002083 | 1.964594 |
| 1.444508 | 2.796676 | 1.462326 | 3.054695 | 2.129501 |
| 0.192616 | 0.748958 | 0.230515 | 1.446799 | 0.489737 |
| IFNg | CXCL9 | CXCL10 | IDO1 | IFN Score |
|---|---|---|---|---|
| 1.685659 | 0.106575 | 0.060205 | 0.190854 | 0.177204 |
| 0.199817 | 0.450834 | 0.357298 | 0.520083 | 0.450208 |
| 0.6063 | 0.114727 | 0.115976 | 2.218294 | 0.847529 |
| 2.364469 | 1.466056 | 1.387023 | 3.230586 | 1.915262 |
| 1.629892 | 0.515913 | 0.334127 | 1.168483 | 0.884869 |
| 2.218103 | 0.494326 | 0.552003 | 2.591719 | 2.211611 |
| 0.742426 | 3.30203 | 7.521585 | 61.60443 | 5.878039 |
| 0.288555 | 0.349889 | 0.12762 | 0.980016 | 0.319222 |
| 0.937276 | 0.708254 | 0.318651 | 3.882854 | 0.822765 |
| 2.629424 | 3.740852 | 2.294862 | 25.64459 | 4.465884 |
| 8.459833 | 0.68337 | 2.678824 | 24.66566 | 3.105226 |
| 0.116979 | 0.333878 | 0.191974 | 0.371062 | 0.262926 |
| 1.939566 | 1.338197 | 0.955549 | 12.77733 | 1.638882 |
| 4.688201 | 0.820236 | 1.056642 | 30.713 | 3.659446 |
| // | 0.711009 | 0.875694 | 7.346527 | 2.825088 |
| 0.042141 | 0.051571 | 0.025111 | 0.01295 | 0.046856 |
| 0.357725 | 0.264255 | 0.155025 | 3.177838 | 0.36583 |
| 2.861291 | 1.714959 | 2.135358 | 14.25268 | 2.485898 |
| 2.379219 | 0.3004 | 0.203204 | 2.950032 | 0.754847 |
| 0.989339 | 2.618225 | 0.873043 | 3.202769 | 2.563137 |
| 0.05656 | 0.025731 | 0.016338 | 0.130882 | 0.062945 |
| 0.590727 | 1.039541 | 0.494817 | 1.226243 | 0.764687 |
| // | 1.674171 | 0.778514 | 2.732303 | 1.142535 |
| 1.114745 | 0.356293 | 1.091995 | 18.2477 | 1.293056 |
| 3.358902 | 1.725384 | 1.169357 | 2.415619 | 2.123589 |
| // | // | // | 7.065799 | 3.783915 |
| 0.033014 | 0.017777 | 0.028004 | 2.806203 | 0.071856 |
| 3.286032 | 1.858926 | 9.757487 | 45.052 | 4.096859 |
| // | // | // | 2.414923 | 1.316748 |
| // | 0.060658 | 0.041742 | // | 0.052629 |
| // | 0.159294 | 0.03838 | 1.285106 | 0.159294 |
| 2.72743 | 1.535855 | 0.419061 | 1.133716 | 0.93273 |
| 1.111062 | 0.075519 | 0.066413 | // | 0.252402 |
| 0.228895 | 0.020628 | 0.01378 | 1.211771 | 0.148608 |
| 0.772693 | 0.185458 | // | 0.599208 | 0.599208 |
| 1.345381 | 0.09437 | 0.119168 | // | 0.125718 |
| 3.47402 | 0.311783 | 0.234453 | 2.285236 | 0.536745 |
| // | 1.710044 | 0.532687 | 1.712725 | 1.711384 |
| // | // | 0.124275 | 4.711086 | 0.617166 |
| // | // | 0.164969 | 4.244882 | 0.364803 |
| // | 0.272361 | 1.167929 | 6.361056 | 0.878366 |
| // | 0.672684 | 0.285985 | 0.403993 | 0.403993 |
| // | // | 0.262111 | // | 0.229 |
| // | // | 0.08179 | // | 0.134591 |
| 1.749853 | 0.583862 | 0.332689 | 0.660082 | 0.83433 |
| IFNg | CXCL9 | CXCL10 | IDO1 | IFN Score |
|---|---|---|---|---|
| 0.119396 | 0.365331 | 0.212938 | 0.454007 | 0.351945 |
| // | // | // | 4.354237 | 3.21977 |
| 2.396478 | 3.402945 | 11.74381 | 21.757 | 4.622528 |
| 1.084336 | 0.501719 | 0.324502 | 0.174045 | 0.396846 |
| 1.370674 | 1.186268 | 0.581905 | 0.50408 | 0.732686 |
| 1.941057 | 1.744747 | 0.761611 | 0.479918 | 0.777233 |
| 0.900624 | 1.081239 | 0.490691 | 0.45876 | 0.530976 |
| // | 0.067341 | 0.494851 | // | 0.494851 |
| 0.570475 | 0.233015 | 0.373023 | 0.449391 | 0.449391 |
| // | 6.473846 | 7.796893 | // | 4.625882 |
| 4.727643 | 4.158529 | 2.109328 | // | 3.227281 |
| 0.478495 | 0.471916 | 1.254819 | 3.87319 | 0.919472 |
| 0.12972 | 0.0641 | 0.110914 | 2.88078 | 0.199274 |
| 3.129895 | 1.368325 | 1.13171 | 1.313043 | 1.222377 |
| 0.485004 | 1.065 | 0.874331 | 1.552961 | 1.132574 |
| 0.78607 | 1.009494 | 0.807926 | 0.295926 | 0.7852 |
| 1.857269 | 1.117105 | 0.639395 | 0.215011 | 0.936784 |
| 0.320975 | 1.104835 | 3.47792 | 3.986919 | 1.145811 |
| 0.84222 | 1.283846 | 0.833621 | 1.326317 | 1.063033 |
| 1.786934 | 3.155041 | 2.117417 | 0.710685 | 1.805562 |
| 7.505436 | 7.622924 | 4.274014 | 0.492337 | 4.072474 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savino, F.; Dini, M.; Clemente, A.; Calvi, C.; Pau, A.; Galliano, I.; Gambarino, S.; Bergallo, M. Nasopharyngeal and Peripheral Blood Type II Interferon Signature Evaluation in Infants during Respiratory Syncytial Virus Infection. Medicina 2024, 60, 259. https://doi.org/10.3390/medicina60020259
Savino F, Dini M, Clemente A, Calvi C, Pau A, Galliano I, Gambarino S, Bergallo M. Nasopharyngeal and Peripheral Blood Type II Interferon Signature Evaluation in Infants during Respiratory Syncytial Virus Infection. Medicina. 2024; 60(2):259. https://doi.org/10.3390/medicina60020259
Chicago/Turabian StyleSavino, Francesco, Maddalena Dini, Anna Clemente, Cristina Calvi, Anna Pau, Ilaria Galliano, Stefano Gambarino, and Massimiliano Bergallo. 2024. "Nasopharyngeal and Peripheral Blood Type II Interferon Signature Evaluation in Infants during Respiratory Syncytial Virus Infection" Medicina 60, no. 2: 259. https://doi.org/10.3390/medicina60020259