
The Impact of Socio-Demographic Factors on Breastfeeding: Findings from the “Mamma & Bambino” Cohort

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analyses
3. Results
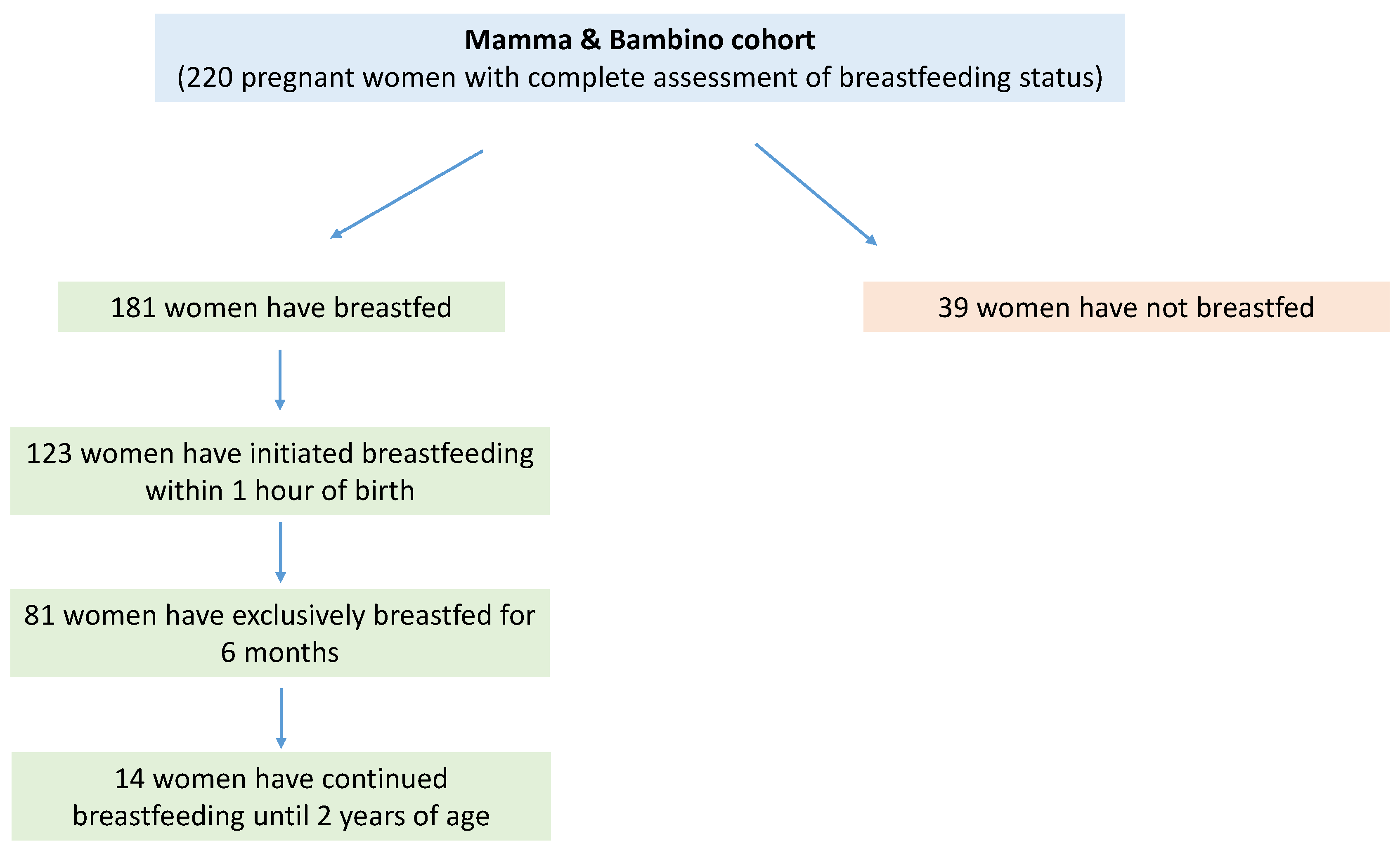
3.1. Characteristics of Study Population
3.2. Association between Maternal Characteristics and Breastfeeding Status
3.3. Association between Maternal Characteristics and Exclusive Breastfeeding for the First Six Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Health Topics: Breastfeeding. 2020. Available online: https://www.who.int/health-topics/breastfeeding (accessed on 15 December 2020).
- WHO Multicentre Growth Reference Study (WMGRS). Breastfeeding in the WHO Multicentre Growth Reference Study. Acta Pædiatrica 2006. [Google Scholar] [CrossRef]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington D.C., US. 2008. Available online: https://apps.who.int/iris/handle/10665/43895 (accessed on 15 December 2020).
- Andreas, N.J.; Kampmann, B.; Mehring Le-Doare, K. Human breast milk: A review on its composition and bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations International Children’s Emergency Fund (UNICEF). Breastfeeding: A mother’s Gift for Every Child. 2018. Available online: https://www.unicef.org/publications/index_102824.html (accessed on 15 December 2020).
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 96–113. [Google Scholar] [CrossRef] [Green Version]
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O'Hare, D.; Schanler, R.J.; Eidelman, A.I.; American Academy of Pediatrics Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2005, 115, 496–506. [Google Scholar] [CrossRef] [Green Version]
- Taveras, E.M.; Capra, A.M.; Braveman, P.A.; Jensvold, N.G.; Escobar, G.J.; Lieu, T.A. Clinician support and psychosocial risk factors associated with breastfeeding discontinuation. Pediatrics 2003, 112, 108–115. [Google Scholar] [CrossRef]
- Tarrant, M.; Fong, D.Y.; Wu, K.M.; Lee, I.L.; Wong, E.M.; Sham, A.; Lam, C.; Dodgson, J.E. Breastfeeding and weaning practices among Hong Kong mothers: A prospective study. BMC Pregnancy Childbirth 2010, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Bick, D.E.; MacArthur, C.; Lancashire, R.J. What influences the uptake and early cessation of breast feeding? Midwifery 1998, 14, 242–247. [Google Scholar] [CrossRef]
- McCarter-Spaulding, D.; Lucas, J.; Gore, R. Employment and breastfeeding outcomes in a sample of black women in the United States. J. Natl. Black Nurses Assoc. 2011, 22, 38–45. [Google Scholar]
- Schwartz, K.; D'Arcy, H.J.; Gillespie, B.; Bobo, J.; Longeway, M.; Foxman, B. Factors associated with weaning in the first 3 months postpartum. J. Fam. Pract. 2002, 51, 439–444. [Google Scholar] [PubMed]
- Cameron, A.J.; Hesketh, K.; Ball, K.; Crawford, D.; Campbell, K.J. Influence of peers on breastfeeding discontinuation among new parents: The Melbourne InFANT Program. Pediatrics 2010, 126, e601–e607. [Google Scholar] [CrossRef] [PubMed]
- Nkrumah, J. Maternal work and exclusive breastfeeding practice: A community based cross-sectional study in Efutu Municipal, Ghana. Int. Breastfeed. J. 2016, 12, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertini, G.; Perugi, S.; Dani, C.; Pezzati, M.; Tronchin, M.; Rubaltelli, F.F. Maternal education and the incidence and duration of breast feeding: A prospective study. J. Pediatr. Gastroenterol. Nutr. 2003, 37, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.; Davanzo, R.; Ronfani, L. Are data on the prevalence and duration of breastfeeding reliable? The case of Italy. Acta Paediatr. 2000, 89, 88–93. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Nutrition Targets 2025: Breastfeeding Policy Brief. 2014. Available online: https://www.who.int/nutrition/publications/globaltargets2025_policybrief_breastfeeding/en (accessed on 15 December 2020).
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; Magnano San Lio, R.; Favara, G.; Panella, M.; Cianci, A.; Agodi, A. Single Nucleotide Polymorphisms in Vitamin D Receptor Gene Affect Birth Weight and the Risk of Preterm Birth: Results From the "Mamma & Bambino" Cohort and A Meta-Analysis. Nutrients 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, A.; Barchitta, M.; Agrifoglio, O.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Panella, M.; Cianci, A.; Agodi, A. The impact of social determinants and lifestyles on dietary patterns during pregnancy: Evidence from the "Mamma & Bambino" study. Ann. Ig. 2019, 31, 81–89. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Agodi, A. Dietary Folate Intake and Folic Acid Supplements among Pregnant Women from Southern Italy: Evidence from the “Mamma & Bambino” Cohort. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Magnano San Lio, R.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Agodi, A.; Barchitta, M.; Quattrocchi, A.; Maugeri, A.; Canto, C.; Marchese, A.E.; Vinciguerra, M. Low fruit consumption and folate deficiency are associated with LINE-1 hypomethylation in women of a cancer-free population. Genes Nutr. 2015, 10, 480. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Quattrocchi, A.; Agodi, A. Dietary Patterns are Associated with Leukocyte LINE-1 Methylation in Women: A Cross-Sectional Study in Southern Italy. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maugeri, A.; Barchitta, M.; Fiore, V.; Rosta, G.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Agodi, A. Determinants of Adherence to the Mediterranean Diet: Findings from a Cross-Sectional Study in Women from Southern Italy. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchitta, M.; Maugeri, A.; La Mastra, C.; Rosa, M.C.; Favara, G.; Lio, R.M.S.; Agodi, A. Dietary Antioxidant Intake and Human Papillomavirus Infection: Evidence from a Cross-Sectional Study in Italy. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Barchitta, M.; Valenti, G.; Marzagalli, R.; Frontini, V.; Marchese, A.E. Increase in the prevalence of the MTHFR 677 TT polymorphism in women born since 1959: Potential implications for folate requirements. Eur. J. Clin. Nutr. 2011, 65, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.C.; Tjønneland, A.; Olsen, A.; Clavel-Chapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Barone, G.; Mazzoleni, P.; Catalfo, A.; De Guidi, G.; Iemmolo, M.G.; Crimi, N.; Agodi, A. Mediterranean Diet and Particulate Matter Exposure Are Associated With LINE-1 Methylation: Results From a Cross-Sectional Study in Women. Front. Genet. 2018, 9, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchitta, M.; Quattrocchi, A.; Adornetto, V.; Marchese, A.E.; Agodi, A. Tumor necrosis factor-alpha -308 G>A polymorphism, adherence to Mediterranean diet, and risk of overweight/obesity in young women. BioMed. Res. Int. 2014, 2014, 742620. [Google Scholar] [CrossRef]
- Eveleth, P.B.; Andres, R.; Chumlea, W.C.; Eiben, O.; Ge, K.; Harris, T.; Heymsfield, S.B.; Launer, L.J.; Rosenberg, I.H.; Solomons, N.W.; et al. Uses and interpretation of anthropometry in the elderly for the assessment of physical status. Report to the Nutrition Unit of the World Health Organization: The Expert Subcommittee on the Use and Interpretation of Anthropometry in the Elderly. J. Nutr. Health Aging 1998, 2, 5–17. [Google Scholar]
- Moore Simas, T.A.; Waring, M.E.; Sullivan, G.M.; Liao, X.; Rosal, M.C.; Hardy, J.R.; Berry, R.E. Institute of medicine 2009 gestational weight gain guideline knowledge: Survey of obstetrics/gynecology and family medicine residents of the United States. Birth 2013, 40, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries; Evidence Report/Technology Assessment (Full Report); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2007; pp. 1–186. [Google Scholar]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Agrifoglio, O.; Agodi, A. The Role of miRNAs as Biomarkers for Pregnancy Outcomes: A Comprehensive Review. Int. J. Genom. 2017, 2017, 8067972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddinott, P.; Tappin, D.; Wright, C. Breast feeding. BMJ 2008, 336, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Sámano, R.; Martínez-Rojano, H.; Godínez Martínez, E.; Sánchez Jiménez, B.; Villeda Rodríguez, G.P.; Pérez Zamora, J.; Casanueva, E. Effects of breastfeeding on weight loss and recovery of pregestational weight in adolescent and adult mothers. Food Nutr. Bull. 2013, 34, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia Pac. J. Public Health 2016, 28, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Platt, R.W.; Dahhou, M.; Kramer, M.S. Do population-based interventions widen or narrow socioeconomic inequalities? The case of breastfeeding promotion. Int. J. Epidemiol. 2014, 43, 1284–1292. [Google Scholar] [CrossRef] [Green Version]
- Webb, A.L.; Sellen, D.W.; Ramakrishnan, U.; Martorell, R. Maternal years of schooling but not academic skills is independently associated with infant-feeding practices in a cohort of rural Guatemalan women. J. Hum. Lact. 2009, 25, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Menon, S.T. Toward a model of psychological health empowerment: Implications for health care in multicultural communities. Nurse Educ. Today 2002, 22, 28–39. [Google Scholar] [CrossRef]
- Dubois, L.; Girard, M. Social determinants of initiation, duration and exclusivity of breastfeeding at the population level: The results of the Longitudinal Study of Child Development in Quebec (ELDEQ 1998-2002). Can. J. Public Health 2003, 94, 300–305. [Google Scholar] [CrossRef]
- Mangrio, E.; Persson, K.; Bramhagen, A.C. Sociodemographic, physical, mental and social factors in the cessation of breastfeeding before 6 months: A systematic review. Scand. J. Caring Sci. 2018, 32, 451–465. [Google Scholar] [CrossRef]
- Verret-Chalifour, J.; Giguère, Y.; Forest, J.C.; Croteau, J.; Zhang, P.; Marc, I. Breastfeeding initiation: Impact of obesity in a large Canadian perinatal cohort study. PLoS ONE 2015, 10, e0117512. [Google Scholar] [CrossRef] [Green Version]
- Mäkelä, J.; Vaarno, J.; Kaljonen, A.; Niinikoski, H.; Lagström, H. Maternal overweight impacts infant feeding patterns—The STEPS Study. Eur. J. Clin. Nutr. 2014, 68, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Donath, S.M.; Amir, L.H.; Team, A.S. The relationship between maternal smoking and breastfeeding duration after adjustment for maternal infant feeding intention. Acta Paediatr. 2004, 93, 1514–1518. [Google Scholar] [CrossRef] [PubMed]
- Vio, F.; Salazar, G.; Infante, C. Smoking during pregnancy and lactation and its effects on breast-milk volume. Am. J. Clin. Nutr. 1991, 54, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Kramer, M.S.; Platt, R.W. Maternal smoking and the risk of early weaning: A meta-analysis. Am. J. Public Health 2001, 91, 304–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giglia, R.; Binns, C.W.; Alfonso, H. Maternal cigarette smoking and breastfeeding duration. Acta Paediatr. 2006, 95, 1370–1374. [Google Scholar] [CrossRef] [PubMed]
- Clifford, T.J.; Campbell, M.K.; Speechley, K.N.; Gorodzinsky, F. Factors influencing full breastfeeding in a southwestern ontario community: Assessments at 1 week and at 6 months postpartum. J. Hum. Lact. 2006, 22, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Rosenberg, K.D.; Sandoval, A.P. Breastfeeding duration and perinatal cigarette smoking in a population-based cohort. Am. J. Public Health 2006, 96, 309–314. [Google Scholar] [CrossRef]
- Hauck, Y.L.; Fenwick, J.; Dhaliwal, S.S.; Butt, J. A Western Australian survey of breastfeeding initiation, prevalence and early cessation patterns. Matern. Child Health J. 2011, 15, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Ayton, J.; van der Mei, I.; Wills, K.; Hansen, E.; Nelson, M. Cumulative risks and cessation of exclusive breast feeding: Australian cross-sectional survey. Arch. Dis. Child. 2015, 100, 863–868. [Google Scholar] [CrossRef]
- Agboado, G.; Michel, E.; Jackson, E.; Verma, A. Factors associated with breastfeeding cessation in nursing mothers in a peer support programme in Eastern Lancashire. BMC Pediatr. 2010, 10, 3. [Google Scholar] [CrossRef] [Green Version]
- Prior, E.; Santhakumaran, S.; Gale, C.; Philipps, L.H.; Modi, N.; Hyde, M.J. Breastfeeding after cesarean delivery: A systematic review and meta-analysis of world literature. Am. J. Clin. Nutr. 2012, 95, 1113–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.; Jordan, S. Impact of birth complications on breastfeeding duration: An internet survey. J. Adv. Nurs. 2013, 69, 828–839. [Google Scholar] [CrossRef] [PubMed]
- Oakley, L.L.; Henderson, J.; Redshaw, M.; Quigley, M.A. The role of support and other factors in early breastfeeding cessation: An analysis of data from a maternity survey in England. BMC Pregnancy Childbirth 2014, 14, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronborg, H.; Vaeth, M.; Rasmussen, K.M. Obesity and early cessation of breastfeeding in Denmark. Eur. J. Public Health 2013, 23, 316–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartok, C.J.; Schaefer, E.W.; Beiler, J.S.; Paul, I.M. Role of body mass index and gestational weight gain in breastfeeding outcomes. Breastfeed. Med. 2012, 7, 448–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulaiman, Z.; Liamputtong, P.; Amir, L.H. Timing of return to work and women's breastfeeding practices in urban Malaysia: A qualitative study. Health Soc. Care Commun. 2018, 26, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Ogbuanu, C.; Glover, S.; Probst, J.; Liu, J.; Hussey, J. The effect of maternity leave length and time of return to work on breastfeeding. Pediatrics 2011, 127, e1414–e1427. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Overall (n = 220) | Breastfeeding (n = 181) | Not Breastfeeding (n = 39) | p-Value |
|---|---|---|---|---|
| Age (Years) | 37.0 (5.0) | 37.0 (4.0) | 38.0 (4.0) | 0.656 |
| Educational Level | ||||
| Low | 33 (15.0%) | 20 (11.0%) | 13 (33.3%) | 0.001 |
| Medium | 106 (48.2%) | 89 (49.2%) | 17 (43.6%) | |
| High | 81 (36.8%) | 72 (39.8%) | 9 (23.1%) | |
| Employment Status | ||||
| Full-time employed | 88 (40.0%) | 77 (42.5%) | 11 (28.2%) | 0.240 |
| Part-time employed | 36 (16.4%) | 29 (16.0%) | 7 (17.9%) | |
| Unemployed | 96 (43.6%) | 75 (41.4%) | 21 (53.8%) | |
| Smoking Status | ||||
| Current | 38 (17.4%) | 30 (16.8%) | 8 (20.5%) | 0.601 |
| Former | 52 (23.9%) | 45 (25.1%) | 7 (17.9%) | |
| Never | 128 (58.7%) | 104 (58.1%) | 24 (61.5%) | |
| Pre-Gestational BMI | 22.7 (4.5) | 22.6 (4.5) | 23.2 (4.9) | 0.768 |
| Gestational Weight Gain a | ||||
| Reduced | 86 (39.3%) | 72 (40.0%) | 14 (35.9%) | 0.291 |
| Adequate | 81 (37.0%) | 69 (38.3%) | 12 (30.8%) | |
| Excessive | 52 (23.7%) | 39 (21.7%) | 13 (33.3%) | |
| Having Children b | ||||
| Yes | 138 (66.7%) | 115 (68.5%) | 23 (59.0%) | 0.258 |
| No | 69 (33.3%) | 53 (31.5%) | 16 (41.0%) | |
| Adherence to Mediterranean Diet | ||||
| Low | 76 (34.7%) | 61 (33.9%) | 15 (38.5%) | 0.638 |
| Medium | 131 (59.8%) | 110 (61.1%) | 21 (53.8%) | |
| High | 12 (5.5%) | 9 (5.0%) | 3 (7.7%) | |
| Type of Delivery | ||||
| Natural | 121 (57.3%) | 100 (57.8%) | 21 (55.3%) | 0.774 |
| Caesarean | 90 (42.7%) | 73 (42.2%) | 17 (44.7%) |
| Characteristics | OR | 95% CI | p-Value |
|---|---|---|---|
| Educational Level | |||
| Low | ref | ||
| Medium | 3.171 | 1.285–7.822 | 0.012 |
| High | 4.549 | 1.525–13.570 | 0.007 |
| Employment Status | |||
| Unemployed | ref | ||
| Part-time employed | 0.922 | 0.339–2.508 | 0.874 |
| Full-time employed | 1.206 | 0.489–2.977 | 0.684 |
| Characteristics | Adherent (n = 81) | Non-Adherent (n = 100) | p-Value |
|---|---|---|---|
| Age (Years) | 37.0 (4.0) | 38.0 (4.0) | 0.293 |
| Educational Level | |||
| Low | 3 (3.7%) | 17 (17.0%) | 0.018 |
| Medium | 43 (53.1%) | 46 (46.0%) | |
| High | 35 (43.2%) | 37 (37.0%) | |
| Employment Status | |||
| Full-time employed | 41 (50.6%) | 36 (36.0%) | 0.015 |
| Part-time employed | 16 (19.8%) | 13 (13.0%) | |
| Unemployed | 24 (29.6%) | 51 (51.0%) | |
| Smoking Status | |||
| Current | 13 (16.3%) | 17 (16.3%) | 0.983 |
| Former | 20 (25.0%) | 25 (25.3%) | |
| Never | 47 (58.8%) | 57 (57.6%) | |
| Pre-gestational BMI | 22.3 (4.2) | 22.7 (4.8) | 0.236 |
| Gestational Weight Gain a | |||
| Reduced | 37 (46.3%) | 35 (35.0%) | 0.304 |
| Adequate | 27 (33.8%) | 42 (42.0%) | |
| Excessive | 16 (20.0%) | 23 (23.0%) | |
| Having Children b | |||
| Yes | 48 (66.7%) | 67 (69.8%) | 0.666 |
| No | 24 (33.3%) | 29 (30.2%) | |
| Adherence to Mediterranean Diet | |||
| Low | 25 (30.9%) | 36 (36.4%) | 0.730 |
| Medium | 52 (64.2%) | 58 (58.6%) | |
| High | 4 (4.9%) | 5 (5.1%) | |
| Type of Delivery | |||
| Natural | 45 (58.4%) | 55 (57.3%) | 0.879 |
| Caesarean | 32 (41.6%) | 41 (42.7%) |
| Characteristics | OR | 95% CI | p-Value |
| Educational Level | |||
| Low | ref | ||
| Medium | 4.632 | 1.227–17.484 | 0.024 |
| High | 3.727 | 0.925–15.009 | 0.064 |
| Employment Status | |||
| Unemployed | ref | ||
| Part-time employed | 2.423 | 0.978–5.999 | 0.056 |
| Full-time employed | 2.158 | 1.033–4.508 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnano San Lio, R.; Maugeri, A.; La Rosa, M.C.; Cianci, A.; Panella, M.; Giunta, G.; Agodi, A.; Barchitta, M. The Impact of Socio-Demographic Factors on Breastfeeding: Findings from the “Mamma & Bambino” Cohort. Medicina 2021, 57, 103. https://doi.org/10.3390/medicina57020103
Magnano San Lio R, Maugeri A, La Rosa MC, Cianci A, Panella M, Giunta G, Agodi A, Barchitta M. The Impact of Socio-Demographic Factors on Breastfeeding: Findings from the “Mamma & Bambino” Cohort. Medicina. 2021; 57(2):103. https://doi.org/10.3390/medicina57020103
Chicago/Turabian StyleMagnano San Lio, Roberta, Andrea Maugeri, Maria Clara La Rosa, Antonio Cianci, Marco Panella, Giuliana Giunta, Antonella Agodi, and Martina Barchitta. 2021. "The Impact of Socio-Demographic Factors on Breastfeeding: Findings from the “Mamma & Bambino” Cohort" Medicina 57, no. 2: 103. https://doi.org/10.3390/medicina57020103