
Peripheral Blood DNA Methylation Profiles Do Not Predict Endoscopic Post-Operative Recurrence in Crohn’s Disease Patients
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
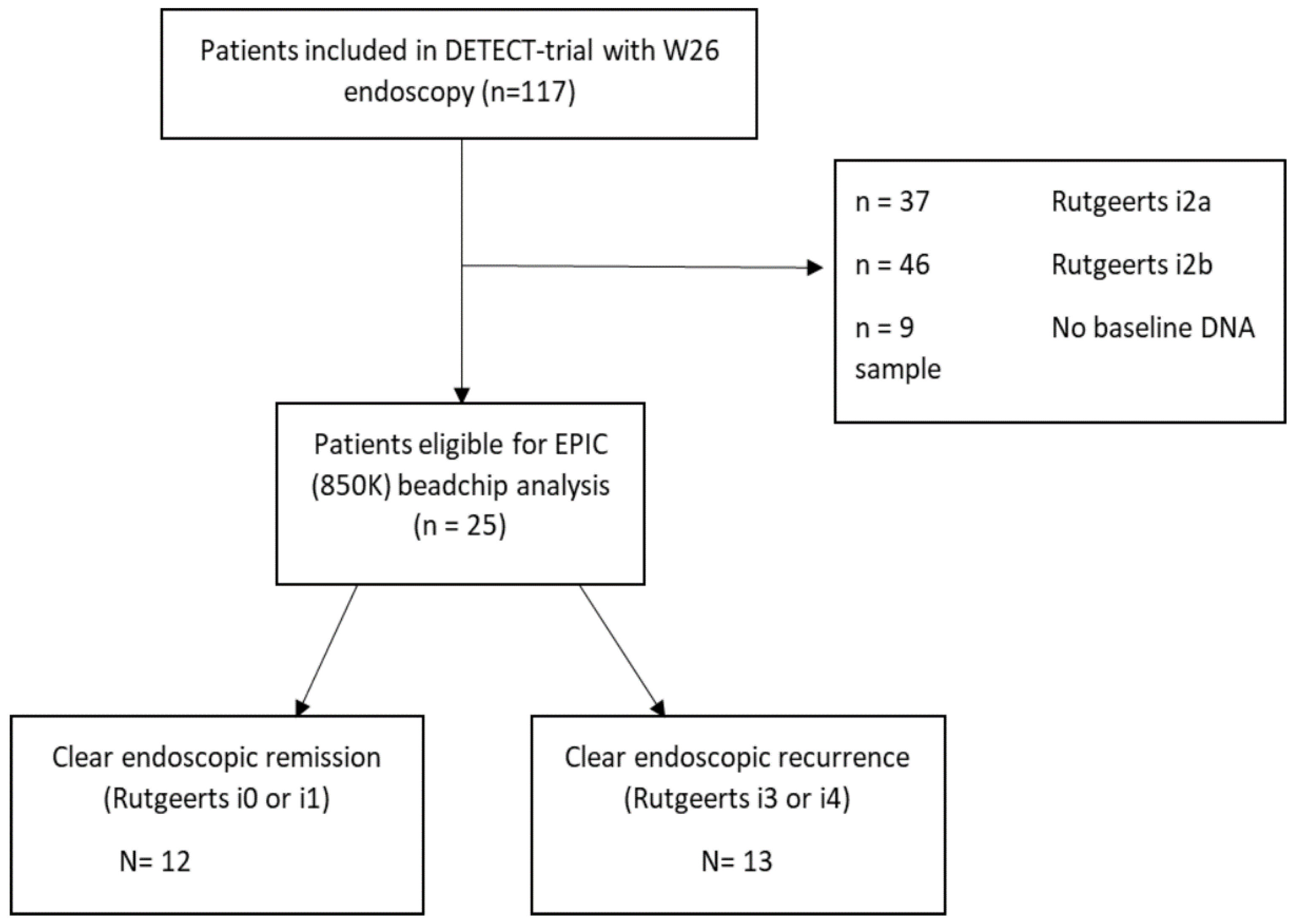
2.1. Patient Characteristics and Clinical Parameters
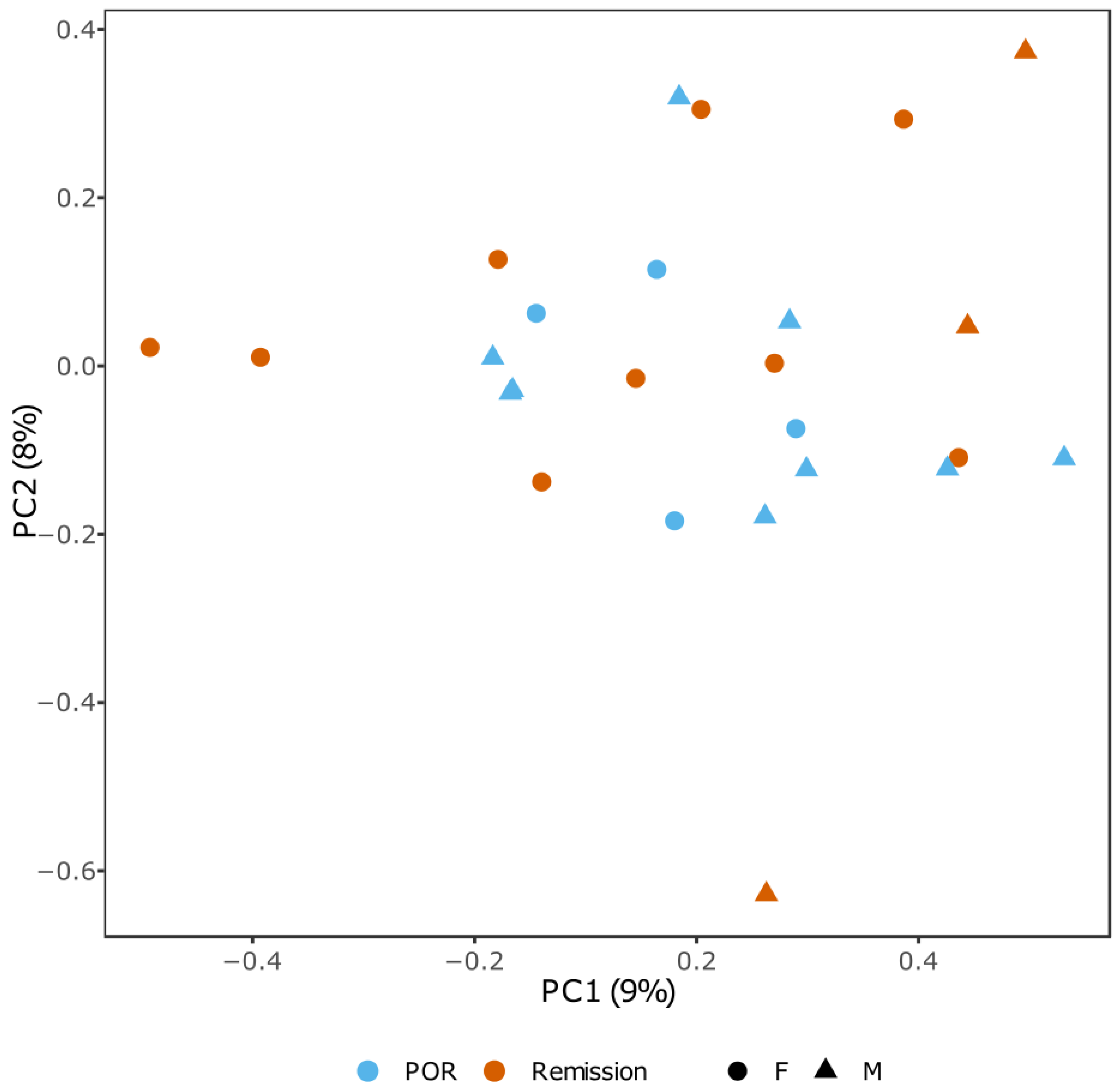
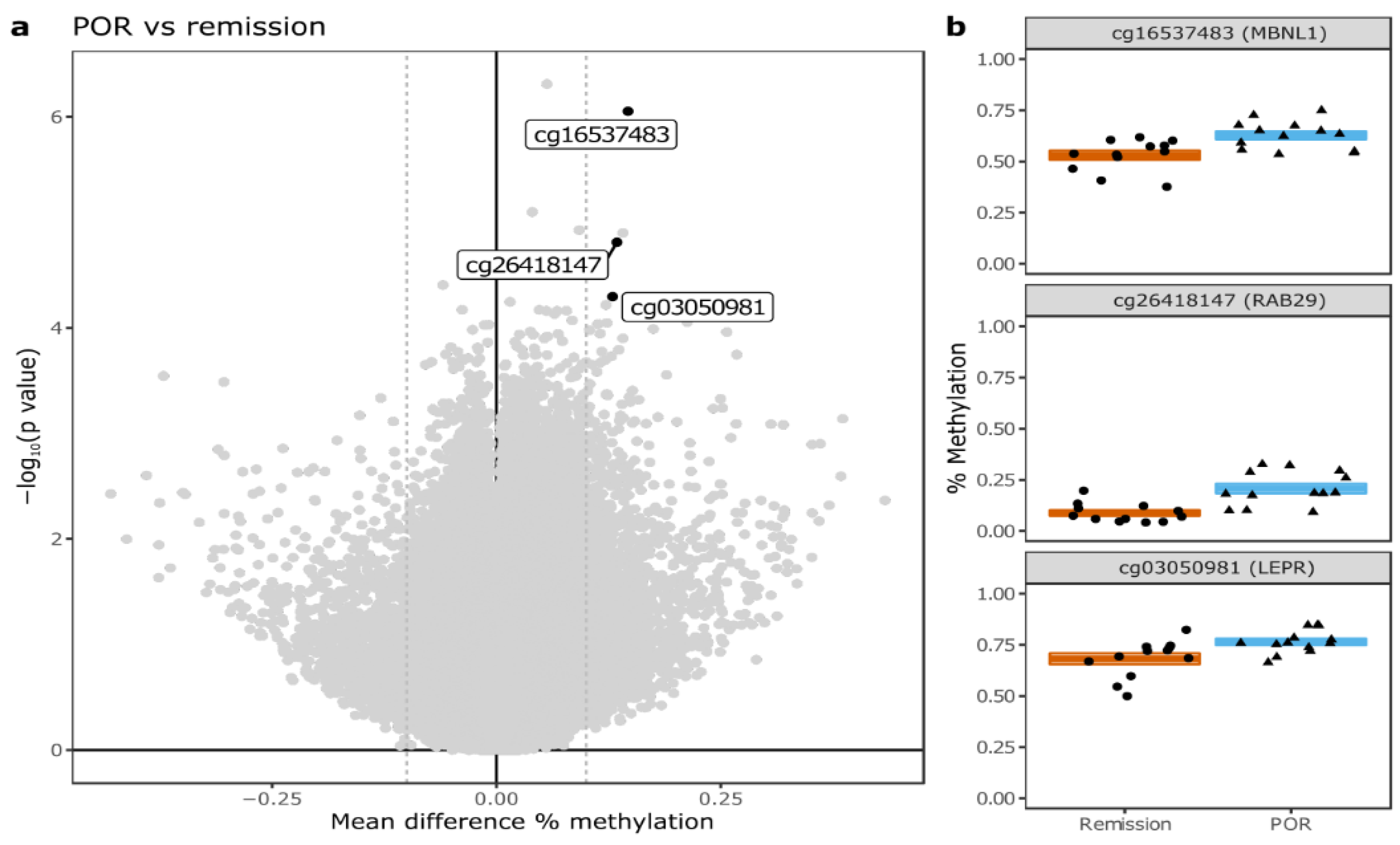
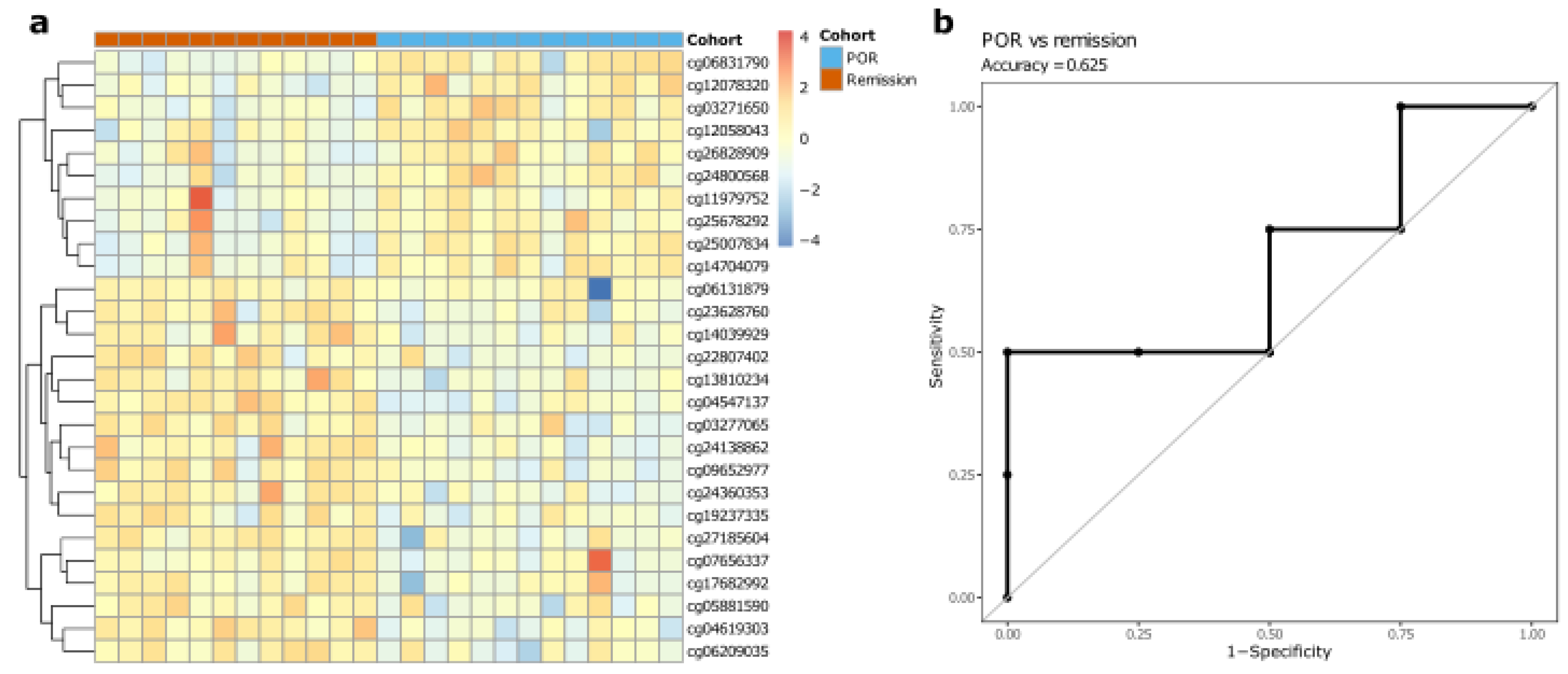
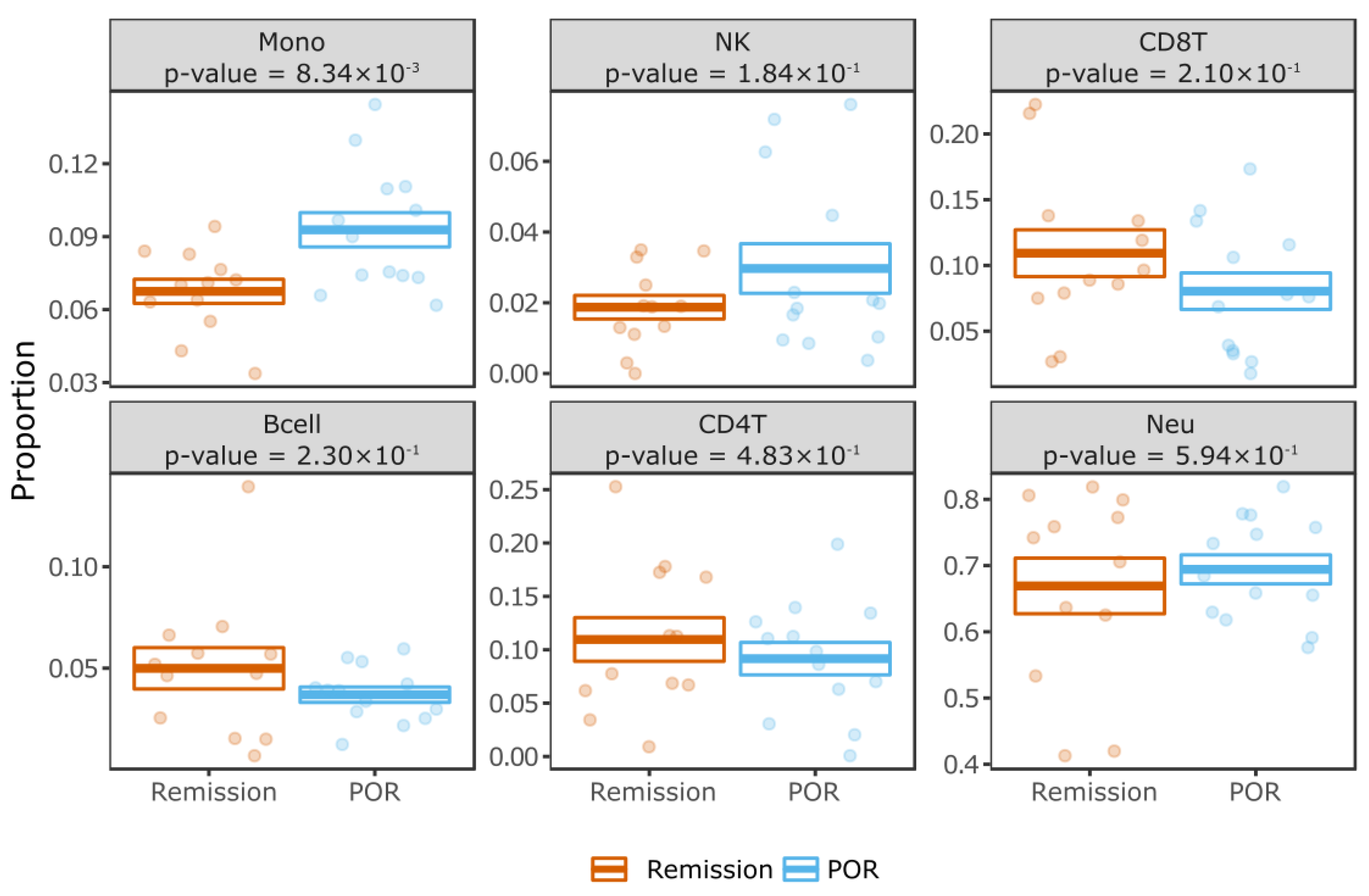
2.2. Differential Methylation Analysis
3. Discussion
4. Materials and Methods
4.1. Patient Cohort Selection
4.2. DNA Isolation, Quality Control and Bisulfite Conversion
4.3. Clinical Analysis
4.4. Methylation Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| POR | Post-operative recurrence |
| ICR | Ileocolonic resection |
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Frolkis, A.D.; Dykeman, J.; Negrón, M.E.; Debruyn, J.; Jette, N.; Fiest, K.M.; Frolkis, T.; Barkema, H.; Rioux, K.P.; Panaccione, R.; et al. Risk of surgery for inflammatory bowel diseases has decreased over time: A systematic review and meta-analysis of population-based studies. Gastroenterology 2013, 145, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Vermeire, S.; Irles-Depe, M.; van Assche, G.; Rutgeerts, P.; Denost, Q.; Wolthuis, A.; D’Hoore, A.; Laharie, D.; Ferrante, M. Rates of Post-operative Recurrence of Crohn’s Disease and Effects of Immunosuppressive and Biologic Therapies. Clin. Gastroenterol. Hepatol. 2020, 19, 713–720.e1. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Beyls, J.; Kerremans, R.; Hiele, M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990, 99, 956–963. [Google Scholar] [CrossRef]
- Gionchetti, P.; Dignass, A.; Danese, S.; Dias, F.J.M.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 2: Surgical Management and Special Situations. J. Crohns Colitis 2017, 11, 135–149. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Loftus, E.; Hirano, I.; Falck–Ytter, Y.; Singh, S.; Sultan, S.; Flamm, S.L.; Lim, J.K.; Rubenstein, J.H.; Smalley, W.E.; et al. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease After Surgical Resection. Gastroenterology 2017, 152, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Marlicz, W.; Skonieczna-Żydecka, K.; Dabos, K.J.; Łoniewski, I.; Koulaouzidis, A. Emerging concepts in non-invasive monitoring of Crohn’s disease. Ther. Adv. Gastroenterol. 2018, 11, 1756284818769076. [Google Scholar] [CrossRef]
- Hatzimichael, E.; Lagos, K.; Sim, V.R.; Briasoulis, E.; Crook, T. Epigenetics in diagnosis, prognostic assessment and treatment of cancer: An update. EXCLI J. 2014, 13, 954–976. [Google Scholar]
- Duruisseaux, M.; Martínez-Cardús, A.; Calleja-Cervantes, M.E.; Moran, S.; de Moura, M.C.; Davalos, V.; Piñeyro, D.; Sanchez-Cespedes, M.; Girard, N.; Brevet, M.; et al. Epigenetic prediction of response to anti-PD-1 treatment in non-small-cell lung cancer: A multicentre, retrospective analysis. Lancet Respir. Med. 2018, 6, 771–781. [Google Scholar] [CrossRef]
- Jung, G.; Hernández-Illán, E.; Moreira, L.; Balaguer, F.; Goel, A. Epigenetics of colorectal cancer: Biomarker and therapeutic potential. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 111–130. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Concepcion, A.N.; Vianen, M.; Marijnissen, A.C.A.; Lafeber, F.P.G.J.; Radstake, T.R.D.J.; Pandit, A. Multiomics and Machine Learning Accurately Predict Clinical Response to Adalimumab and Etanercept Therapy in Patients With Rheumatoid Arthritis. Arthritis Rheumatol. 2021, 73, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.P. Epigenetics: Principles and practice. Dig. Dis. 2011, 29, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Somineni, H.K.; Venkateswaran, S.; Kilaru, V.; Marigorta, U.M.; Mo, A.; Okou, D.T.; Kellermayer, R.; Mondal, K.; Cobb, D.; Walters, T.D.; et al. Blood-Derived DNA Methylation Signatures of Crohn’s Disease and Severity of Intestinal Inflammation. Gastroenterology 2019, 156, 2254–2265.e3. [Google Scholar] [CrossRef] [PubMed]
- Yim, A.Y.F.L.; de Bruyn, J.R.; Duijvis, N.W.; Sharp, C.; Ferrero, E.; de Jonge, W.J.; Wildenberg, M.E.; Mannens, M.M.A.M.; Buskens, C.J.; D’Haens, G.R.; et al. A distinct epigenetic profile distinguishes stenotic from non-inflamed fibroblasts in the ileal mucosa of Crohn’s disease patients. PLoS ONE 2018, 13, e0209656. [Google Scholar]
- Li Yim, A.Y.F.; Duijvis, N.W.; Zhao, J.; de Jonge, W.J.; D’Haens, G.R.A.M.; Mannens, M.M.A.M.; Mul, A.N.P.M.; Velde, A.A.; Henneman, P. Peripheral blood methylation profiling of female Crohn’s disease patients. Clin. Epigenet. 2016, 8, 65. [Google Scholar] [CrossRef]
- McDermott, E.; Ryan, E.J.; Tosetto, M.; Gibson, D.; Burrage, J.; Keegan, D.; Byrne, K.; Crowe, E.; Sexton, G.; Malone, K.; et al. DNA Methylation Profiling in Inflammatory Bowel Disease Provides New Insights into Disease Pathogenesis. J. Crohn’s Colitis 2016, 10, 77–86. [Google Scholar] [CrossRef]
- Adams, A.T.; Kennedy, N.A.; Hansen, R.; Hansen, R.; Ventham, N.T.; O’Leary, K.R.; Drummond, H.E.; Noble, C.L.; El-Omar, E.; Russell, R.K.; et al. Two-stage Genome-wide Methylation Profiling in Childhood-onset Crohn’s Disease Implicates Epigenetic Alterations at the VMP1/MIR21 and HLA Loci. Inflamm. Bowel Dis. 2014, 20, 1784–1793. [Google Scholar] [CrossRef]
- Ventham, N.T.; IBD BIOM Consortium; Kennedy, N.; Adams, A.T.; Kalla, R.; Heath, S.C.; O’Leary, K.R.; Drummond, H.E.; Wilson, D.C.; Gut, I.G.; et al. Integrative epigenome-wide analysis demonstrates that DNA methylation may mediate genetic risk in inflammatory bowel disease. Nat. Commun. 2016, 7, 13507. [Google Scholar] [CrossRef]
- Karatzas, P.S.; Mantzaris, G.J.; Safioleas, M.; Gazouli, M. DNA methylation profile of genes involved in inflammation and autoimmunity in inflammatory bowel disease. Medicine 2014, 93, e309. [Google Scholar] [CrossRef]
- Relton, C.L.; Hartwig, F.P.; Davey Smith, G. From stem cells to the law courts: DNA methylation, the forensic epigenome and the possibility of a biosocial archive. Int. J. Epidemiol. 2015, 44, 1083–1093. [Google Scholar] [CrossRef] [PubMed]
- Altucci, L.; Rots, M.G. Epigenetic drugs: From chemistry via biology to medicine and back. Clin. Epigenet. 2016, 8, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koestler, D.C.; Jones, M.J.; Usset, J.; Christensen, B.C.; Butler, R.A.; Kobor, M.S.; Wiencke, J.K.; Kelsey, K.T. Improving cell mixture deconvolution by identifying optimal DNA methylation libraries (IDOL). BMC Bioinform. 2016, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Cardani, R.; Baldassa, S.; Botta, A.; Rinaldi, F.; Novelli, G.; Mancinelli, E.; Meola, G. Ribonuclear inclusions and MBNL1 nuclear sequestration do not affect myoblast differentiation but alter gene splicing in myotonic dystrophy type 2. Neuromuscul. Disord. 2009, 19, 335–343. [Google Scholar] [CrossRef]
- Wang, P.-Y.; Lin, Y.-M.; Wang, L.-H.; Kuo, T.-Y.; Cheng, S.-J.; Wang, G.-S. Reduced cytoplasmic MBNL1 is an early event in a brain-specific mouse model of myotonic dystrophy. Hum. Mol. Genet. 2017, 26, 2247–2257. [Google Scholar] [CrossRef]
- Sellier, C.; Cerro-Herreros, E.; Blatter, M.; Freyermuth, F.; Gaucherot, A.; Ruffenach, F.; Sarkar, P.; Puymirat, J.; Udd, B.; Day, J.W.; et al. rbFOX1/MBNL1 competition for CCUG RNA repeats binding contributes to myotonic dystrophy type 1/type 2 differences. Nat. Commun. 2018, 9, 2009. [Google Scholar] [CrossRef]
- Song, K.-Y.; Guo, X.-M.; Wang, H.-Q.; Zhang, L.; Huang, S.-Y.; Huo, Y.-C.; Zhang, G.; Feng, J.-Z.; Zhang, R.-R.; Ma, Y.; et al. MBNL1 reverses the proliferation defect of skeletal muscle satellite cells in myotonic dystrophy type 1 by inhibiting autophagy via the mTOR pathway. Cell Death Dis. 2020, 11, 545. [Google Scholar] [CrossRef]
- Itskovich, S.S.; Gurunathan, A.; Clark, J.; Burwinkel, M.; Wunderlich, M.; Berger, M.R.; Kulkarni, A.; Chetal, K.; Venkatasubramanian, M.; Salomonis, N.; et al. MBNL1 regulates essential alternative RNA splicing patterns in MLL-rearranged leukemia. Nat. Commun. 2020, 11, 2369. [Google Scholar] [CrossRef]
- Chen, Y.-S.; Liu, C.-W.; Lin, Y.-C.; Tsai, C.-Y.; Yang, C.-H.; Lin, J.-C. The SRSF3-MBNL1-Acin1 circuit constitutes an emerging axis to lessen DNA fragmentation in colorectal cancer via an alternative splicing mechanism. Neoplasia 2020, 22, 702–713. [Google Scholar] [CrossRef]
- Davis, J.; Salomonis, N.; Ghearing, N.; Lin, S.-C.J.; Kwong, J.Q.; Mohan, A.; Swanson, M.; Molkentin, J.D. MBNL1-mediated regulation of differentiation RNAs promotes myofibroblast transformation and the fibrotic response. Nat. Commun. 2015, 6, 10084. [Google Scholar] [CrossRef]
- Sznajder, J.; Scotti, M.M.; Shin, J.; Taylor, K.; Ivankovic, F.; Nutter, C.A.; Aslam, F.; Subramony, S.H.; Ranum, L.P.W.; Swanson, M.S. Loss of MBNL1 induces RNA misprocessing in the thymus and peripheral blood. Nat. Commun. 2020, 11, 2022. [Google Scholar] [CrossRef] [PubMed]
- LeMasters, K.E.; Blech-Hermoni, Y.; Stillwagon, S.J.; Vajda, N.A.; Ladd, A.N. Loss of muscleblind-like 1 promotes invasive mesenchyme formation in endocardial cushions by stimulating autocrine TGFbeta3. BMC Dev. Biol. 2012, 12, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vajda, N.A.; Brimacombe, K.R.; LeMasters, K.E.; Ladd, A.N. Muscleblind-like 1 is a negative regulator of TGF-beta-dependent epithelial-mesenchymal transition of atrioventricular canal endocardial cells. Dev. Dyn. 2009, 238, 3266–3272. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Rieder, F.; Fiocchi, C.; Achkar, J.-P. Pathogenesis of postoperative recurrence in Crohn’s disease. Gut 2011, 60, 553–562. [Google Scholar] [CrossRef]
- Scarpa, M.; Bortolami, M.; Morgan, S.L.; Kotsafti, A.; Ferraro, S.; Ruffolo, C.; D’Incà, R.; Polese, L.; Barollo, M.; D’Amico, D.F.; et al. TGF-beta1 and IGF-1 production and recurrence of Crohn’s disease after ileo-colonic resection. J. Surg. Res. 2009, 152, 26–34. [Google Scholar] [CrossRef]
- Boschetti, G.; Nancey, S.; Moussata, D.; Cotte, E.; Francois, Y.; Flourié, B.; Kaiserlian, D. Enrichment of Circulating and Mucosal Cytotoxic CD8+ T Cells Is Associated with Postoperative Endoscopic Recurrence in Patients with Crohn’s Disease. J. Crohns Colitis 2016, 10, 338–345. [Google Scholar] [CrossRef]
- Kuwahara, T.; Inoue, K.; D’Agati, V.D.; Fujimoto, T.; Eguchi, T.; Saha, S.; Wolozin, B.; Iwatsubo, T.; Abeliovich, A. LRRK2 and RAB7L1 coordinately regulate axonal morphology and lysosome integrity in diverse cellular contexts. Sci. Rep. 2016, 6, 29945. [Google Scholar] [CrossRef]
- Eguchi, T.; Kuwahara, T.; Sakurai, M.; Komori, T.; Fujimoto, T.; Ito, G.; Yoshimura, S.-I.; Harada, A.; Fukuda, M.; Koike, M.; et al. LRRK2 and its substrate Rab GTPases are sequentially targeted onto stressed lysosomes and maintain their homeostasis. Proc. Natl. Acad. Sci. USA 2018, 115, E9115–E9124. [Google Scholar] [CrossRef]
- Berwick, D.C.; Heaton, G.R.; Azeggagh, S.; Harvey, K. LRRK2 Biology from structure to dysfunction: Research progresses, but the themes remain the same. Mol. Neurodegener. 2019, 14, 49. [Google Scholar] [CrossRef]
- Kuwahara, T.; Funakawa, K.; Komori, T.; Sakurai, M.; Yoshii, G.; Eguchi, T.; Fukuda, M.; Iwatsubo, T. Roles of lysosomotropic agents on LRRK2 activation and Rab10 phosphorylation. Neurobiol. Dis. 2020, 145, 105081. [Google Scholar] [CrossRef]
- Liu, J.Z.; Van Sommeren, S.; Huang, H.; Ng, S.C.; Alberts, R.; Takahashi, A.; Ripke, S.; Lee, J.C.; Jostins, L.; Shah, T.; et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat. Genet. 2015, 47, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Lee, J.; Krummey, S.; Lu, W.; Cai, H.; Lenardo, M.J. The kinase LRRK2 is a regulator of the transcription factor NFAT that modulates the severity of inflammatory bowel disease. Nat. Immunol. 2011, 12, 1063–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maekawa, T.; Shimayama, H.; Tsushima, H.; Kawakami, F.; Kawashima, R.; Kubo, M.; Ichikawa, T. LRRK2: An Emerging New Molecule in the Enteric Neuronal System That Quantitatively Regulates Neuronal Peptides and IgA in the Gut. Dig. Dis. Sci. 2017, 62, 903–912. [Google Scholar] [CrossRef]
- Takagawa, T.; Kitani, A.; Fuss, I.; Levine, B.; Brant, S.R.; Peter, I.; Tajima, M.; Nakamura, S.; Strober, W. An increase in LRRK2 suppresses autophagy and enhances Dectin-1-induced immunity in a mouse model of colitis. Sci. Transl. Med. 2018, 10, eaan8162. [Google Scholar] [CrossRef]
- Liu, Z.; Lenardo, M.J. The role of LRRK2 in inflammatory bowel disease. Cell Res. 2012, 22, 1092–1094. [Google Scholar] [CrossRef]
- Wallings, R.L.; Tansey, M.G. LRRK2 regulation of immune-pathways and inflammatory disease. Biochem. Soc. Trans. 2019, 47, 1581–1595. [Google Scholar] [CrossRef] [PubMed]
- Mackey-Lawrence, N.M.; Petri, W.A., Jr. Leptin and mucosal immunity. Mucosal. Immunol. 2012, 5, 472–479. [Google Scholar] [CrossRef]
- Fantuzzi, G.; Faggioni, R. Leptin in the regulation of immunity, inflammation, and hematopoiesis. J. Leukoc. Biol. 2000, 68, 437–446. [Google Scholar]
- Frank, S.; Stallmeyer, B.; Kämpfer, H.; Kolb, N.; Pfeilschifter, J. Leptin enhances wound re-epithelialization and constitutes a direct function of leptin in skin repair. J. Clin. Investig. 2000, 106, 501–509. [Google Scholar] [CrossRef]
- Ring, B.D.; Scully, S.; Davis, C.R.; Baker, M.B.; Cullen, M.J.; Pelleymounter, M.A.; Danilenko, D.M. Systemically and topically administered leptin both accelerate wound healing in diabetic ob/ob mice. Endocrinology 2000, 141, 446–449. [Google Scholar] [CrossRef]
- Sukhotnik, I.; Helou, H.; Lurie, M.; Khateeb, K.; Bejar, J.; Coran, A.G.; Mogilner, J.G.; Shiloni, E. The effect of leptin on intestinal recovery following ischemia-reperfusion injury in a rat. Pediatr. Surg. Int. 2007, 23, 473–478. [Google Scholar] [CrossRef]
- Umeki, H.; Tokuyama, R.; Ide, S.; Okubo, M.; Tadokoro, S.; Tezuka, M.; Tatehara, S.; Satomura, K. Leptin promotes wound healing in the oral mucosa. PLoS ONE 2014, 9, e101984. [Google Scholar]
- Matsumura, S.; Kurashima, Y.; Murasaki, S.; Morimoto, M.; Arai, F.; Saito, Y.; Katayama, N.; Kim, D.; Inagaki, Y.; Kudo, T.; et al. Stratified layer analysis reveals intrinsic leptin stimulates cryptal mesenchymal cells for controlling mucosal inflammation. Sci. Rep. 2020, 10, 18351. [Google Scholar] [CrossRef] [PubMed]
- de Bruyn, J.R.; Bossuyt, P.; Ferrante, M.; West, R.L.; Dijkstra, G.; Witteman, B.J.; Wildenberg, M.; Hoentjen, F.; Franchimont, D.; Clasquin, E.; et al. High-Dose Vitamin D Does Not Prevent Postoperative Recurrence of Crohn’s Disease in a Randomized Placebo-Controlled Trial. Clin. Gastroenterol. Hepatol. 2020, 19, 1573–1582.e5. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.C.; Bell, J.T. Power and sample size estimation for epigenome-wide association scans to detect differential DNA methylation. Int. J. Epidemiol. 2015, 44, 1429–1441. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-S.; Song, E.-J.; Nam, Y.-D. Dysbiosis of Gut Microbiome and Its Impact on Epigenetic Regulation. J. Clin. Epigenet. 2017, 3, 14. [Google Scholar]
- Hamilton, A.L.; Kamm, M.A.; De Cruz, P.; Wright, E.K.; Feng, H.; Wagner, J.; Sung, J.J.Y.; Kirkwood, C.D.; Inouye, M.; Teo, S.-M. Luminal microbiota related to Crohn’s disease recurrence after surgery. Gut Microbes 2020, 11, 1713–1728. [Google Scholar] [CrossRef]
- Machiels, K.; Del Río, M.P.; La Torre, A.M.-D.; Xie, Z.; Andreu, V.P.; Sabino, J.; Santiago, A.; Campos, D.; Wolthuis, A.; D’Hoore, A.; et al. Early Postoperative Endoscopic Recurrence in Crohn’s Disease Is Characterised by Distinct Microbiota Recolonisation. J. Crohns Colitis 2020, 14, 1535–1546. [Google Scholar] [CrossRef]
- Bachour, S.P.; Shah, R.S.; Lyu, R.; Rieder, F.; Qazi, T.; Lashner, B.; Achkar, J.P.; Philpott, J.; Barnes, E.L.; Axelrad, J.; et al. Mild neoterminal ileal post-operative recurrence of Crohn’s disease conveys higher risk for severe endoscopic disease progression than isolated anastomotic lesions. Aliment. Pharmacol. Ther. 2022, 55, 1139–1150. [Google Scholar] [CrossRef]
- Ma, C.; Gecse, K.B.; Duijvestein, M.; Sandborn, W.J.; Zou, G.; Shackelton, L.M.; Stitt, L.W.; Parker, C.E.; Bossuyt, P.; Löwenberg, M.; et al. Reliability of Endoscopic Evaluation of Postoperative Recurrent Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 2139–2141.e2. [Google Scholar] [CrossRef]
- Rivière, P.; Vermeire, S.; Irles-Depe, M.; Van Assche, G.; Rutgeerts, P.; Overstraeten, A.D.B.V.; Denost, Q.; Wolthuis, A.; D’Hoore, A.; Laharie, D.; et al. No Change in Determining Crohn’s Disease Recurrence or Need for Endoscopic or Surgical Intervention With Modification of the Rutgeerts’ Scoring System. Clin. Gastroenterol. Hepatol. 2019, 17, 1643–1645. [Google Scholar] [CrossRef] [PubMed]
- Gecse, K.; Lowenberg, M.; Bossuyt, P.; Rutgeerts, P.J.; Vermeire, S.; Stitt, L.; Vandervoort, M.K.; Sandborn, W.; Feagan, B.G.; Samaan, M.A.; et al. Sa1198 Agreement Among Experts in the Endoscopic Evaluation of Postoperative Recurrence in Crohn’s Disease Using the Rutgeerts Score. Gastroenterology 2014, 146, S-227. [Google Scholar] [CrossRef]
- Ihaka, R.; Gentleman, R. R: A Language for Data Analysis and Graphics. J. Comput. Graph. Stat. 1996, 5, 299–314. [Google Scholar]
- Aryee, M.J.; Jaffe, A.E.; Corrada-Bravo, H.; Ladd-Acosta, C.; Feinberg, A.P.; Hansen, K.D.; Irizarry, R.A. Minfi: A flexible and comprehensive Bioconductor package for the analysis of Infinium DNA methylation microarrays. Bioinformatics 2014, 30, 1363–1369. [Google Scholar] [CrossRef]
- Fortin, J.-P.; Labbe, A.; Lemire, M.; Zanke, B.W.; Hudson, T.J.; Fertig, E.J.; Greenwood, C.M.; Hansen, K.D. Functional normalization of 450k methylation array data improves replication in large cancer studies. Genome Biol. 2014, 15, 503. [Google Scholar] [CrossRef]
- Van Iterson, M.; Tobi, E.W.; Slieker, R.C.; Den Hollander, W.; Luijk, R.; Slagboom, P.E.; Heijmans, B.T. MethylAid: Visual and interactive quality control of large Illumina 450k datasets. Bioinformatics 2014, 30, 3435–3437. [Google Scholar] [CrossRef]
- Du, P.; Zhang, X.; Huang, C.-C.; Jafari, N.; Kibbe, W.A.; Hou, L.; Lin, S.M. Comparison of Beta-value and M-value methods for quantifying methylation levels by microarray analysis. BMC Bioinform. 2010, 11, 587. [Google Scholar] [CrossRef]
- Smyth, G.K. Linear models and empirical bayes methods for assessing differential expression in microarray experiments. Stat. Appl. Genet. Mol. Biol. 2004, 3, 3. [Google Scholar] [CrossRef]
- Ritchie, M.E.; Belinda, P.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Peters, T.J.; Buckley, M.J.; Statham, A.L.; Pidsley, R.; Samaras, K.; Lord, R.V.; Clark, S.J.; Molloy, P.L. De novo identification of differentially methylated regions in the human genome. Epigenet. Chromatin 2015, 8, 6. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentleman, R.; Carey, V.; Huber, W.; Hahne, F. Genefilter: Methods for filtering genes from high-throughput experiments. R Package Version 1.72.1. 2021. [Google Scholar]
- Wickam, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Endoscopic Remission (n = 12) | Endoscopic Recurrence (n = 13) | p-Value | |
|---|---|---|---|
| Female, n (%) | 9 (75) | 4 (30.8) | 0.03 |
| Age, years, median (IQR) | 30 (21–42) | 31 (25–53) | 0.51 |
| Ethnic background, n (%) - Caucasian | 10 (83.3) | 10 (76.9) | 0.72 |
| C-reactive protein, mg/L, median (IQR) | 25.5 (3–84.5) | 62.6 (13.6–104) | 0.28 |
| Faecal calprotectin, ug/g, median (IQR) | 454.5 (111–1650.5) | 805 (303.8–1602.5) | 0.39 |
| Baseline CDAI score, median (IQR) | 104.5 (62.3–161.3) | 144 (101–292) | 0.11 |
| Disease location, n (%) - Ileal disease (L1) - Ileocolonic disease (L3) | 10 (83.3) 2 (16.7) | 6 (46.2) 7 (53.8) | 0.048 |
| Disease behavior, n (%) - Non stricturing/penetrating (B1) - Stricturing (B2) - Penetrating (B3) - Perianal disease (p) | 3 (25) 7 (58.3) 2 (16.7) - | 3 (27.3) 5 (45.5) 3 (27.3) 2 (15.4) | 0.78 |
| Previous IBD related surgery, n (%) | 1 (8.3) | 4 (30.8) | 0.15 |
| Previous medical treatment, n (%) - Immunomodulator (AZA, 6MP, MTX) - Anti-TNF (IFX and/or ADA) | 7 (58.3) 5 (41.7) | 7 (58.3) 7 (58.3) | 0.82 0.54 |
| Smoking, n (%) - Active - Non-smoker | 5 (41.7) 7 (58.3) | 2 (15.4) 11 (84.6) | 0.14 |
| CpG ID | p Value | adj. p Value | Beta | Annotated Genes |
|---|---|---|---|---|
| cg22681074 | 4.89 × 10−7 | 0.375 | 0.056 | GJC2 |
| cg16537483 | 8.85 × 10−7 | 0.375 | 0.147 | MBNL1 |
| cg15599437 | 7.97 × 10−6 | 0.966 | 0.040 | |
| cg20677058 | 1.18 × 10−5 | 0.966 | 0.092 | AKR7L |
| cg22120095 | 1.26 × 10−5 | 0.966 | 0.141 | CACNA2D2 |
| cg26418147 | 1.54 × 10−5 | 0.966 | 0.134 | RAB29 |
| cg25215028 | 2.06 × 10−5 | 0.966 | 0.108 | |
| cg05128623 | 3.92 × 10−5 | 0.966 | −0.060 | SLC43A2 |
| cg03050981 | 5.05 × 10−5 | 0.966 | 0.129 | LEPR |
| cg12919469 | 5.68 × 10−5 | 0.966 | 0.015 | TMC4 |
| cg07528209 | 6.05 × 10−5 | 0.966 | 0.122 | |
| cg01094108 | 6.75 × 10−5 | 0.966 | −0.038 | GLI3 |
| cg11551901 | 6.76 × 10−5 | 0.966 | 0.048 | SEC31B |
| cg22995183 | 6.87 × 10−5 | 0.966 | 0.078 | MRTFB |
| cg01543603 | 6.90 × 10−5 | 0.966 | 0.056 | ANKRD11 |
| cg08514511 | 6.91 × 10−5 | 0.966 | 0.068 | FRK |
| cg14574579 | 7.37 × 10−5 | 0.966 | 0.064 | UMODL1 |
| cg05725940 | 8.50 × 10−5 | 0.966 | 0.084 | GSDMB |
| cg00871238 | 8.81 × 10−5 | 0.966 | 0.212 | |
| cg14219900 | 8.96 × 10−5 | 0.966 | 0.123 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joustra, V.W.; Li Yim, A.Y.F.; de Bruyn, J.R.; Duijvestein, M.; Hageman, I.L.; de Jonge, W.J.; Henneman, P.; Wildenberg, M.; D’Haens, G. Peripheral Blood DNA Methylation Profiles Do Not Predict Endoscopic Post-Operative Recurrence in Crohn’s Disease Patients. Int. J. Mol. Sci. 2022, 23, 10467. https://doi.org/10.3390/ijms231810467
Joustra VW, Li Yim AYF, de Bruyn JR, Duijvestein M, Hageman IL, de Jonge WJ, Henneman P, Wildenberg M, D’Haens G. Peripheral Blood DNA Methylation Profiles Do Not Predict Endoscopic Post-Operative Recurrence in Crohn’s Disease Patients. International Journal of Molecular Sciences. 2022; 23(18):10467. https://doi.org/10.3390/ijms231810467
Chicago/Turabian StyleJoustra, Vincent W., Andrew Y. F. Li Yim, Jessica R. de Bruyn, Marjolijn Duijvestein, Ishtu L. Hageman, Wouter J. de Jonge, Peter Henneman, Manon Wildenberg, and Geert D’Haens. 2022. "Peripheral Blood DNA Methylation Profiles Do Not Predict Endoscopic Post-Operative Recurrence in Crohn’s Disease Patients" International Journal of Molecular Sciences 23, no. 18: 10467. https://doi.org/10.3390/ijms231810467