
Role of Vitamin D in Liver Disease and Complications of Advanced Chronic Liver Disease

 , ,
, ,
Abstract
:1. Introduction
2. Data Sources and Searches
3. The Biochemistry and Physiology of Vitamin
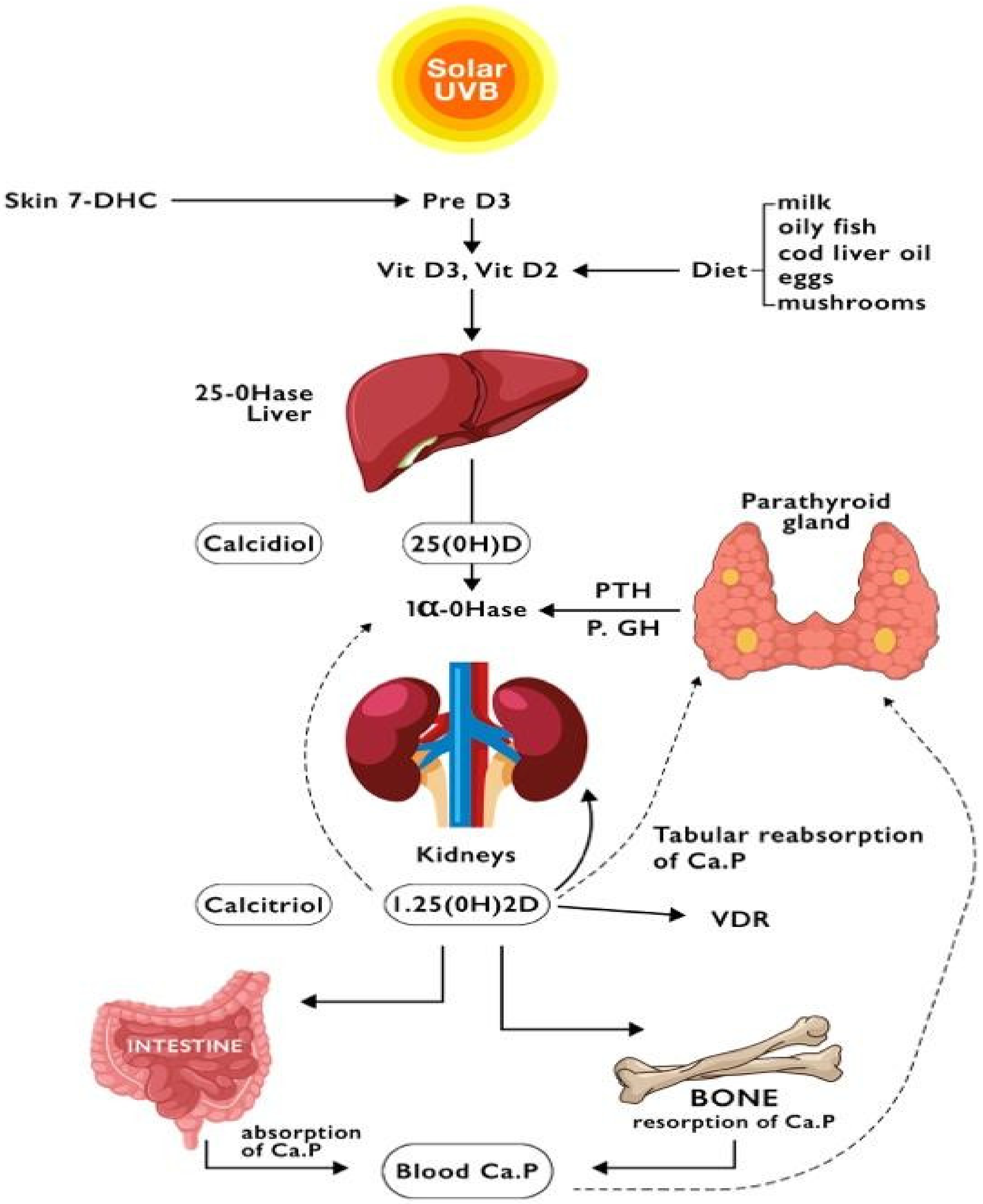
3.1. Sources of Vitamin D
3.2. Metabolism of Vitamin D
3.3. Vitamin D Binding Protein (DBP)
3.4. Mechanism of Action of Vitamin D
3.5. Vitamin D Deficiency
4. Vitamin D in the Chronic Liver Diseases
4.1. Viral Hepatitis
4.1.1. Hepatitis B Virus (HBV)
4.1.2. Hepatitis Delta Virus (HDV)
4.1.3. Hepatitis C Virus (HCV)
4.2. Alcoholic Liver Disease (ALD)
4.3. Non-Alcoholic Fatty Liver Disease (NAFLD)
4.4. Autoimmune and Cholestatic Liver Disease
4.4.1. Vitamin D and Autoimmunity
4.4.2. Autoimmune Hepatitis
4.4.3. Primary Biliary Cholangitis (PBC) and Primary Sclerosing Cholangitis (PSC)
5. Vitamin D in Advanced Chronic Liver Disease (ACLD) and Complications
5.1. Hepatic Encephalopathy
5.2. Gastro-Esophageal Varices and Variceal Bleeding
5.3. Bacterial Infections and Spontaneous Bacterial Peritonitis
5.4. Sarcopenia
6. Vitamin D and HepatoCellular Carcinoma (HCC)
6.1. Vitamin D in Hepatocarcinogenesis
6.2. Vitamin D as Biomarkers in HCC
6.3. Vitamin D Supplementation Therapy in HCC
7. Conclusions and Future Perspective
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Holick, M.F.; Chen, T.C.; Lu, Z.; Sauter, E. Vitamin D and Skin Physiology: A D-Lightful Story. J. Bone Miner. Res. 2007, 22, V28–V33. [Google Scholar] [CrossRef] [PubMed]
- Kühn, J.; Schröter, A.; Hartmann, B.M.; Stangl, G.I. Cocoa and chocolate are sources of vitamin D2. Food Chem. 2018, 269, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-W.; Lee, H.-C. Vitamin D and health—The missing vitamin in humans. Pediatr. Neonatol. 2019, 60, 237–244. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021; Giugno 2016; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Nakamura, K.; Nashimoto, M.; Okuda, Y.; Ota, T.; Yamamoto, M. Fish as a major source of vitamin D in the Japanese diet. Nutrition 2002, 18, 415–416. [Google Scholar] [CrossRef]
- Pellegrino, L.; Marangoni, F.; Muscogiuri, G.; D’Incecco, P.; Duval, G.T.; Annweiler, C.; Colao, A. Vitamin D Fortification of Consumption Cow’s Milk: Health, Nutritional and Technological Aspects. A Multidisciplinary Lecture of the Recent Scientific Evidence. Molecules 2021, 26, 5289. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- White, P.; Cooke, N. The Multifunctional Properties and Characteristics of Vitamin D-binding Protein. Trends Endocrinol. Metab. 2000, 11, 320–327. [Google Scholar] [CrossRef]
- Cooke, N.E.; Haddad, J.G. Vitamin D Binding Protein (Gc-Globulin). Endocr. Rev. 1989, 10, 294–307. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J. Vitamin D Insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, A.; Malki, A. Vitamin D Signaling in Inflammation and Cancer: Molecular Mechanisms and Therapeutic Implications. Molecules 2020, 25, 3219. [Google Scholar] [CrossRef] [PubMed]
- Gorham, E.D.; Garland, C.F.; Garland, F.C.; Grant, W.B.; Mohr, S.B.; Lipkin, M.; Newmark, H.L.; Giovannucci, E.; Wei, M.; Holick, M.F. Vitamin D and prevention of colorectal cancer. J. Steroid Biochem. Mol. Biol. 2005, 97, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yan, J.; Liu, B. Targeting VEGF/VEGFR to Modulate Antitumor Immunity. Front. Immunol. 2018, 9, 978. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Islam, M.N.; Dakshanamurthy, S.; Rizvi, I.; Rao, M.; Herrell, R.; Zinser, G.; Valrance, M.; Aranda, A.; Moras, D.; et al. The Molecular Basis of Vitamin D Receptor and β-Catenin Crossregulation. Mol. Cell 2006, 21, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Morelli, M.E.; Caruso, P. Vitamin D in Neurological Diseases: A Rationale for a Pathogenic Impact. Int. J. Mol. Sci. 2018, 19, 2245. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Christakos, S. Mechanisms Underlying the Regulation of Innate and Adaptive Immunity by Vitamin D. Nutrients 2015, 7, 8251–8260. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef]
- Kitson, M.T.; Roberts, S.K. D-livering the message: The importance of vitamin D status in chronic liver disease. J. Hepatol. 2012, 57, 897–909. [Google Scholar] [CrossRef]
- Zhao, X.; Li, J.; Wang, J.; Habib, S.; Wei, W.; Sun, S.; Strobel, H.W.; Jia, J. Vitamin D serum level is associated with Child–Pugh score and metabolic enzyme imbalances, but not viral load in chronic hepatitis B patients. Medicine 2016, 95, e3926. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Tan, D.; Ning, Q.; Niu, J.; Bai, X.; Chen, S.; Cheng, J.; Yu, Y.; Wang, H.; Xu, M.; et al. Association of baseline vitamin D level with genetic determinants and virologic response in patients with chronic hepatitis B. Hepatol. Res. 2018, 48, E213–E221. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, A.K.; Amento, E.P.; Clemens, T.L.; Holick, M.F.; Krane, S.M. Specific High-Affinity Receptors for 1,25-Dihydroxyvitamin D3 in Human Peripheral Blood Mononuclear Cells: Presence in Monocytes and Induction in T Lymphocytes Following Activation. J. Clin. Endocrinol. Metab. 1983, 57, 1308–1310. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Bitetto, D.; Fattovich, G.; Fabris, C.; Ceriani, E.; Falleti, E.; Fornasiere, E.; Pasino, M.; Ieluzzi, D.; Cussigh, A.; Cmet, S.; et al. Complementary role of vitamin D deficiency and the interleukin-28B rs12979860 C/T polymorphism in predicting antiviral response in chronic hepatitis C. Hepatology 2011, 53, 1118–1126. [Google Scholar] [CrossRef]
- Petta, S.; Cammà, C.; Scazzone, C.; Tripodo, C.; Marco, V.D.; Bono, A.; Cabibi, D.; Licata, G.; Porcasi, R.; Marchesini, G.; et al. Low vitamin D serum level is related to severe fibrosis and low responsiveness to interferon-based therapy in genotype 1 chronic hepatitis C. Hepatology 2010, 51, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Terrier, B.; Carrat, F.; Geri, G.; Pol, S.; Piroth, L.; Halfon, P.; Poynard, T.; Souberbielle, J.-C.; Cacoub, P. Low 25-OH vitamin D serum levels correlate with severe fibrosis in HIV-HCV co-infected patients with chronic hepatitis. J. Hepatol. 2011, 55, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Timms, P.M.; Mannan, N.; Hitman, G.A.; Noonan, K.; Mills, P.G.; Syndercombe-Court, D.; Aganna, E.; Price, C.P.; Boucher, B.J. Circulating MMP9, vitamin D and variation in the TIMP-1 response with VDR genotype: Mechanisms for inflammatory damage in chronic disorders? QJM Mon. J. Assoc. Physicians 2002, 95, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.-P. Matrix metalloproteinases, the pros and cons, in liver fibrosis. J. Gastroenterol. Hepatol. 2006, 21 (Suppl. 3), S88–S91. [Google Scholar] [CrossRef]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Siddiqui, M.; Manansala, J.S.; Abdulrahman, H.A.; Nasrallah, G.K.; Smatti, M.K.; Younes, N.; Althani, A.A.; Yassine, H.M. Immune Modulatory Effects of Vitamin D on Viral Infections. Nutrients 2020, 12, 2879. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.-C.; Kao, J.-H. Clinical utility of quantitative HBsAg in natural history and nucleos(t)ide analogue treatment of chronic hepatitis B: New trick of old dog. J. Gastroenterol. 2013, 48, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.-Q.; Shi, Y.; Tang, H. New insight of vitamin D in chronic liver diseases. Hepatobiliary Pancreat. Dis. Int. HBPD Int. 2014, 13, 580–585. [Google Scholar] [CrossRef]
- Hoan, N.X.; Khuyen, N.; Binh, M.T.; Giang, D.P.; Tong, H.V.; Hoan, P.Q.; Trung, N.T.; Anh, D.T.; Toan, N.L.; Meyer, C.G.; et al. Association of vitamin D deficiency with hepatitis B virus—Related liver diseases. BMC Infect. Dis. 2016, 16, 507. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.-Q.; Bai, L.; Zhou, T.-Y.; Fe, M.; Zhang, D.-M.; Tang, H. Sustained suppression of viral replication in improving vitamin D serum concentrations in patients with chronic hepatitis B. Sci. Rep. 2015, 5, 15441. [Google Scholar] [CrossRef]
- Farnik, H.; Bojunga, J.; Berger, A.; Allwinn, R.; Waidmann, O.; Kronenberger, B.; Keppler, O.T.; Zeuzem, S.; Sarrazin, C.; Lange, C.M. Low vitamin D serum concentration is associated with high levels of hepatitis B virus replication in chronically infected patients. Hepatology 2013, 58, 1270–1276. [Google Scholar] [CrossRef]
- Mohamadkhani, A.; Bastani, F.; Khorrami, S.; Ghanbari, R.; Eghtesad, S.; Sharafkhah, M.; Montazeri, G.; Poustchi, H. Negative Association of Plasma Levels of Vitamin D and miR-378 With Viral Load in Patients With Chronic Hepatitis B Infection. Hepat. Mon. 2015, 15, e28315. [Google Scholar] [CrossRef]
- Teymoori-Rad, M.; Shokri, F.; Salimi, V.; Marashi, S.M. The interplay between vitamin D and viral infections. Rev. Med. Virol. 2019, 29, e2032. [Google Scholar] [CrossRef]
- He, L.-J.; Zhang, H.-P.; Li, H.-J.; Wang, J.; Chang, D.-D. Effect of Serum Vitamin D Levels on Cellular Immunity and Antiviral Effects in Chronic Hepatitis B Patients. Clin. Lab. 2016, 62, 1933–1939. [Google Scholar] [CrossRef]
- Beard, J.A.; Bearden, A.; Striker, R. Vitamin D and the anti-viral state. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2011, 50, 194–200. [Google Scholar] [CrossRef]
- Alves, C.; Branco, C.; Cunha, C. Hepatitis delta virus: A peculiar virus. Adv. Virol. 2013, 2013, 560105. [Google Scholar] [CrossRef] [PubMed]
- Uçmak, F.; YIlmaz, A.; Ekin, N.; Ekinci, A.; Solmaz, İ.; Şenateş, E. Vitamin D deficiency in patients with chronic hepatitis D viral infection. Clin. Exp. Hepatol. 2021, 7, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, M.P.; Ones, D.S. A century of research on conscientiousness at work. Proc. Natl. Acad. Sci. USA 2019, 116, 23004–23010. [Google Scholar] [CrossRef]
- Sriphoosanaphan, S.; Thanapirom, K.; Kerr, S.J.; Suksawatamnuay, S.; Thaimai, P.; Sittisomwong, S.; Sonsiri, K.; Srisoonthorn, N.; Teeratorn, N.; Tanpowpong, N.; et al. Effect of vitamin D supplementation in patients with chronic hepatitis C after direct-acting antiviral treatment: A randomized, double-blind, placebo-controlled trial. PeerJ 2021, 9, e10709. [Google Scholar] [CrossRef] [PubMed]
- Curry, M.P.; O’Leary, J.G.; Bzowej, N.; Muir, A.J.; Korenblat, K.M.; Fenkel, J.M.; Reddy, K.R.; Lawitz, E.; Flamm, S.L.; Schiano, T.; et al. Sofosbuvir and Velpatasvir for HCV in Patients with Decompensated Cirrhosis. N. Engl. J. Med. 2015, 373, 2618–2628. [Google Scholar] [CrossRef]
- Sriphoosanaphan, S.; Thanapirom, K.; Suksawatamnuay, S.; Thaimai, P.; Sittisomwong, S.; Sonsiri, K.; Srisoonthorn, N.; Teeratorn, N.; Tanpowpong, N.; Chaopathomkul, B.; et al. Changes in hepatic fibrosis and vitamin D levels after viral hepatitis C eradication using direct-acting antiviral therapy. BMC Gastroenterol. 2020, 20, 346. [Google Scholar] [CrossRef]
- Villar, L.M.; Campo, J.A.D.; Ranchal, I.; Lampe, E.; Romero-Gomez, M. Association between vitamin D and hepatitis C virus infection: A meta-analysis. World J. Gastroenterol. 2013, 19, 5917–5924. [Google Scholar] [CrossRef]
- Murayama, A.; Saitoh, H.; Takeuchi, A.; Yamada, N.; Matsumura, T.; Shiina, M.; Muramatsu, M.; Wakita, T.; Imawari, M.; Kato, T. Vitamin D derivatives inhibit hepatitis C virus production through the suppression of apolipoprotein. Antivir. Res. 2018, 160, 55–63. [Google Scholar] [CrossRef]
- Fukuhara, T.; Wada, M.; Nakamura, S.; Ono, C.; Shiokawa, M.; Yamamoto, S.; Motomura, T.; Okamoto, T.; Okuzaki, D.; Yamamoto, M.; et al. Amphipathic α-helices in apolipoproteins are crucial to the formation of infectious hepatitis C virus particles. PLoS Pathog. 2014, 10, e1004534. [Google Scholar] [CrossRef]
- Lương, K.V.Q. Theoretical basis of a beneficial role for vitamin D in viral hepatitis. World J. Gastroenterol. 2012, 18, 5338. [Google Scholar] [CrossRef]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Thursz, M.; Gual, A.; Lackner, C.; Mathurin, P.; Moreno, C.; Spahr, L.; Sterneck, M.; Cortez-Pinto, H. EASL Clinical Practice Guidelines: Management of alcohol-related liver disease. J. Hepatol. 2018, 69, 154–181. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.K.; Bataller, R.; Ahn, J.; Kamath, P.S.; Shah, V.H. ACG Clinical Guideline: Alcoholic Liver Disease. Am. J. Gastroenterol. 2018, 113, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Meng, Q.-H. Current understanding of the metabolism of micronutrients in chronic alcoholic liver disease. World J. Gastroenterol. 2020, 26, 4567–4578. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, C.; Farías, J.; Zamorano, M.; Herrera, C. Vitamin Supplements as a Nutritional Strategy against Chronic Alcohol Consumption? An Updated Review. Antioxidants 2022, 11, 564. [Google Scholar] [CrossRef]
- Trépo, E.; Ouziel, R.; Pradat, P.; Momozawa, Y.; Quertinmont, E.; Gervy, C.; Gustot, T.; Degré, D.; Vercruysse, V.; Deltenre, P.; et al. Marked 25-hydroxyvitamin D deficiency is associated with poor prognosis in patients with alcoholic liver disease. J. Hepatol. 2013, 59, 344–350. [Google Scholar] [CrossRef]
- Anty, R.; Canivet, C.M.; Patouraux, S.; Ferrari-Panaia, P.; Saint-Paul, M.C.; Huet, P.-M.; Lebeaupin, C.; Iannelli, A.; Gual, P.; Tran, A. Severe Vitamin D Deficiency May be an Additional Cofactor for the Occurrence of Alcoholic Steatohepatitis. Alcohol. Clin. Exp. Res. 2015, 39, 1027–1033. [Google Scholar] [CrossRef]
- Malham, M.; Peter Jørgensen, S.; Lauridsen, A.L.; Ott, P.; Glerup, H.; Dahlerup, J.F. The effect of a single oral megadose of vitamin D provided as either ergocalciferol (D2) or cholecalciferol (D3) in alcoholic liver cirrhosis: Eur. J. Gastroenterol. Hepatol. 2012, 24, 172–178. [Google Scholar] [CrossRef]
- Savić, Ž.; Vračarić, V.; Milić, N.; Nićiforović, D.; Damjanov, D.; Pellicano, R.; Medić-Stojanoska, M.; Abenavoli, L. Vitamin D supplementation in patients with alcoholic liver cirrhosis: A prospective study. Minerva Med. 2018, 109, 352–357. [Google Scholar] [CrossRef]
- González-Reimers, E. Bone changes in alcoholic liver disease. World J. Hepatol. 2015, 7, 1258. [Google Scholar] [CrossRef]
- López-Larramona, G.; Lucendo, A.J.; González-Delgado, L. Alcoholic liver disease and changes in bone mineral density. Rev. Esp. Enferm. Dig. 2013, 105, 609–621. [Google Scholar] [CrossRef]
- Savic, Z.; Damjanov, D.; Curic, N.; Kovacev-Zavisic, B.; Hadnadjev, L.; Novakovic-Paro, J.; Nikolic, S. Vitamin D status, bone metabolism and bone mass in patients with alcoholic liver cirrhosis. Bratisl. Med. J. 2014, 115, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- EASL–EASD–EASO. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Ratziu, V.; Bellentani, S.; Cortez-Pinto, H.; Day, C.; Marchesini, G. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J. Hepatol. 2010, 53, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Drzewoski, J.; Śliwińska, A. The Molecular Mechanisms by Which Vitamin D Prevents Insulin Resistance and Associated Disorders. Int. J. Mol. Sci. 2020, 21, 6644. [Google Scholar] [CrossRef]
- Barchetta, I.; Carotti, S.; Labbadia, G.; Gentilucci, U.V.; Muda, A.O.; Angelico, F.; Silecchia, G.; Leonetti, F.; Fraioli, A.; Picardi, A.; et al. Liver vitamin D receptor, CYP2R1, and CYP27A1 expression: Relationship with liver histology and vitamin D3 levels in patients with nonalcoholic steatohepatitis or hepatitis C virus. Hepatology 2012, 56, 2180–2187. [Google Scholar] [CrossRef]
- Barchetta, I.; Cimini, F.A.; Chiappetta, C.; Bertoccini, L.; Ceccarelli, V.; Capoccia, D.; Gaggini, M.; Di Cristofano, C.; Della Rocca, C.; Silecchia, G.; et al. Relationship between hepatic and systemic angiopoietin-like 3, hepatic Vitamin D receptor expression and NAFLD in obesity. Liver Int. 2020, 40, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Cimini, F.A.; Barchetta, I.; Carotti, S.; Bertoccini, L.; Baroni, M.G.; Vespasiani-Gentilucci, U.; Cavallo, M.-G.; Morini, S. Relationship between adipose tissue dysfunction, vitamin D deficiency and the pathogenesis of non-alcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 3407–3417. [Google Scholar] [CrossRef]
- Borges-Canha, M.; Neves, J.S.; Mendonça, F.; Silva, M.M.; Costa, C.; Cabral, P.M.; Guerreiro, V.; Lourenço, R.; Meira, P.; Salazar, D.; et al. The Impact of Vitamin D in Non-Alcoholic Fatty Liver Disease: A Cross-Sectional Study in Patients with Morbid Obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 487–495. [Google Scholar] [CrossRef]
- Bennouar, S.; Cherif, A.B.; Kessira, A.; Bennouar, D.E.; Abdi, S. Association and interaction between vitamin D level and metabolic syndrome for non-alcoholic fatty liver disease. J. Diabetes Metab. Disord. 2021, 20, 1309–1317. [Google Scholar] [CrossRef]
- Heo, N.J.; Park, H.E.; Yoon, J.W.; Kwak, M.-S.; Yang, J.I.; Chung, S.J.; Yim, J.Y.; Chung, G.E. The Association between Vitamin D and Nonalcoholic Fatty Liver Disease Assessed by Controlled Attenuation Parameter. J. Clin. Med. 2021, 10, 2611. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.S.; Bril, F.; Cusi, K.; Newsome, P.N. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 70, 711–724. [Google Scholar] [CrossRef]
- Kwok, R.M.; Torres, D.M.; Harrison, S.A. Vitamin D and nonalcoholic fatty liver disease (NAFLD): Is it more than just an association?: Hepatology. Hepatology 2013, 58, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef] [PubMed]
- Sakpal, M.; Satsangi, S.; Mehta, M.; Duseja, A.; Bhadada, S.; Das, A.; Dhiman, R.K.; Chawla, Y.K. Vitamin D supplementation in patients with nonalcoholic fatty liver disease: A randomized controlled trial. JGH Open 2017, 1, 62–67. [Google Scholar] [CrossRef]
- Sharifi, N.; Amani, R.; Hajiani, E.; Cheraghian, B. Does vitamin D improve liver enzymes, oxidative stress, and inflammatory biomarkers in adults with non-alcoholic fatty liver disease? A randomized clinical trial. Endocrine 2014, 47, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Zanko, V.L.; Domislovic, V.; Trkulja, V.; Krznaric-Zrnic, I.; Turk-Wensveen, T.; Krznaric, Z.; Kanizaj, T.F.; Radic-Kristo, D.; Bilic-Zulle, L.; Orlic, L.; et al. Vitamin D for treatment of non-alcoholic fatty liver disease detected by transient elastography: A randomized, double-blind, placebo-controlled trial. Diabetes Obes. Metab. 2020, 22, 2097–2106. [Google Scholar] [CrossRef] [PubMed]
- Sindhughosa, D.A.; Wibawa, I.D.N.; Mariadi, I.K.; Somayana, G. Additional treatment of vitamin D for improvement of insulin resistance in non-alcoholic fatty liver disease patients: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 7716. [Google Scholar] [CrossRef]
- Hussain, M.; Iqbal, J.; Malik, S.A.; Waheed, A.; Shabnum, S.; Akhtar, L.; Saeed, H. Effect of vitamin D supplementation on various parameters in non-alcoholic fatty liver disease patients. Pak. J. Pharm. Sci. 2019, 32, 1343–1348. [Google Scholar]
- Guo, X.; Wang, C.; Yang, T.; Li, S.; Li, K.; Li, D. Vitamin D and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 7389–7399. [Google Scholar] [CrossRef] [PubMed]
- Kitson, M.T.; Pham, A.; Gordon, A.; Kemp, W.; Roberts, S.K. High-dose vitamin D supplementation and liver histology in NASH. Gut 2016, 65, 717–718. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Moosazadeh, M.; Lankarani, K.B.; Akbari, M.; Heydari, S.T.; Kolahdooz, F.; Samimi, M.; Asemi, Z. The effects of vitamin D supplementation on metabolic profiles and liver function in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S975–S982. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Theodor, E.; Segal, R.M.; Shoenfeld, Y. Vitamin D in Systemic and Organ-Specific Autoimmune Diseases. Clin. Rev. Allergy Immunol. 2013, 45, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Montano-Loza, A.J. Evolving Role of Vitamin D in Immune-Mediated Disease and Its Implications in Autoimmune Hepatitis. Dig. Dis. Sci. 2019, 64, 324–344. [Google Scholar] [CrossRef]
- Shoenfeld, N.; Amital, H.; Shoenfeld, Y. The effect of melanism and vitamin D synthesis on the incidence of autoimmune disease. Nat. Clin. Pract. Rheumatol. 2009, 5, 99–105. [Google Scholar] [CrossRef]
- EASL. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]
- Efe, C.; Kav, T.; Aydin, C.; Cengiz, M.; Imga, N.N.; Purnak, T.; Smyk, D.S.; Torgutalp, M.; Turhan, T.; Ozenirler, S.; et al. Low Serum Vitamin D Levels Are Associated with Severe Histological Features and Poor Response to Therapy in Patients with Autoimmune Hepatitis. Dig. Dis. Sci. 2014, 59, 3035–3042. [Google Scholar] [CrossRef]
- Abe, K.; Fujita, M.; Hayashi, M.; Takahashi, A.; Ohira, H. Association of serum 25-hydroxyvitamin D levels with severe necroinflammatory activity and inflammatory cytokine production in type I autoimmune hepatitis. PLoS ONE 2020, 15, e0239481. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Bhanji, R.A.; Mazurak, V.C.; Lytvyak, E.; Mason, A.; Czaja, A.J.; Montano-Loza, A.J. Severe vitamin D deficiency is a prognostic biomarker in autoimmune hepatitis. Aliment. Pharmacol. Ther. 2019, 49, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Leung, D.Y.M.; Goleva, E. Vitamin D Enhances Glucocorticoid Action in Human Monocytes. J. Biol. Chem. 2013, 288, 14544–14553. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Ip, S.; Lytvyak, E.; Asghari, S.; Rider, E.; Mason, A.; Montano-Loza, A.J. Vitamin D is Associated with Clinical Outcomes in Patients with Primary Biliary Cholangitis. Nutrients 2022, 14, 878. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Kopilov, R.; Selmi, C.; Nussinovitch, U.; Sánchez-Castañón, M.; López-Hoyos, M.; Amital, H.; Kivity, S.; Gershwin, E.M.; Shoenfeld, Y. Vitamin D in primary biliary cirrhosis, a plausible marker of advanced disease. Immunol. Res. 2015, 61, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Adorini, L. Vitamin D receptor polymorphisms in primary biliary cirrhosis: A functional connection? J. Hepatol. 2009, 50, 1071–1073. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Nezu, S.; Uegaki, S.; Kikuchi, K.; Shibuya, A.; Miyakawa, H.; Takahashi, S.; Bianchi, I.; Zermiani, P.; Podda, M.; et al. Vitamin D receptor polymorphisms are associated with increased susceptibility to primary biliary cirrhosis in Japanese and Italian populations. J. Hepatol. 2009, 50, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Halmos, B.; Szalay, F.; Cserniczky, T.; Nemesanszky, E.; Lakatos, P.; Barlage, S.; Schmitz, G.; Romics, L.; Csaszar, A. Association of Primary Biliary Cirrhosis with Vitamin D Receptor BsmI Genotype Polymorphism in a Hungarian Population. Dig. Dis. Sci. 2000, 45, 5. [Google Scholar] [CrossRef]
- Fan, L.; Tu, X.; Zhu, Y.; Zhou, L.; Pfeiffer, T.; Feltens, R.; Stoecker, W.; Zhong, R. Genetic association of vitamin D receptor polymorphisms with autoimmune hepatitis and primary biliary cirrhosis in the Chinese. J. Gastroenterol. Hepatol. 2005, 20, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Strassburg, C.P.; Manns, M.P. Genetic association of vitamin D receptor polymorphisms with primary biliary cirrhosis and autoimmune hepatitis: Genetic Association of Vitamin D Receptor Polymorphisms with Primary Biliary Cirrhosis and Autoimmune Hepatitis. Hepatology 2002, 35, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Mo, C.; Lu, Y.; Deng, Y.; Wang, J.; Xie, L.; Li, T.; He, Y.; Qin, X.; Li, S. Lack of association between vitamin D receptor gene ApaI, BsmI, and TaqI polymorphisms and primary biliary cirrhosis risk: A meta-analysis. Tumor Biol. 2014, 35, 4913–4920. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, R.A.; Lindor, K.D.; Sartin, J.S.; LaRusso, N.F.; Wiesner, R.H. Serum Lipid and Fat-Soluble Vitamin Levels in Primary Sclerosing Cholangitis. J. Clin. Gastroenterol. 1995, 20, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Malham, M. Vitamin D deficiency in cirrhosis relates to liver dysfunction rather than aetiology. World J. Gastroenterol. 2011, 17, 922. [Google Scholar] [CrossRef] [PubMed]
- Stokes, C.S.; Volmer, D.A.; Grünhage, F.; Lammert, F. Vitamin D in chronic liver disease. Liver Int. 2013, 33, 338–352. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.C.; Yang, Y.Y.; Lee, W.P.; Lee, K.C.; Hsieh, Y.C.; Lee, T.Y.; Lin, H.C. Comparative portal hypotensive effects as propranolol of vitamin D3 treatment by decreasing intrahepatic resistance in cirrhotic rats. J. Gastroenterol. Hepatol. 2015, 30, 628–637. [Google Scholar] [CrossRef]
- Paternostro, R.; Wagner, D.; Reiberger, T.; Mandorfer, M.; Schwarzer, R.; Ferlitsch, M.; Trauner, M.; Peck-Radosavljevic, M.; Ferlitsch, A. Low 25-OH-vitamin D levels reflect hepatic dysfunction and are associated with mortality in patients with liver cirrhosis. Wien. Klin. Wochenschr. 2017, 129, 8–15. [Google Scholar] [CrossRef]
- Putz-Bankuti, C.; Pilz, S.; Stojakovic, T.; Scharnagl, H.; Pieber, T.R.; Trauner, M.; Obermayer-Pietsch, B.; Stauber, R.E. Association of 25-hydroxyvitamin D levels with liver dysfunction and mortality in chronic liver disease. Liver Int. 2012, 32, 845–851. [Google Scholar] [CrossRef]
- Bjelakovic, M.; Nikolova, D.; Bjelakovic, G.; Gluud, C. Vitamin D supplementation for chronic liver diseases in adults. Cochrane Database Syst. Rev. 2021, 2021, CD011564. [Google Scholar] [CrossRef]
- Kumar, P.; Chaudhry, S.; Dev, N.; Kumar, R.; Singh, G. Serum 25-hydroxyvitamin D level in patients with chronic liver disease and its correlation with hepatic encephalopathy: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 798–803. [Google Scholar]
- Vidot, H.; Potter, A.; Cheng, R.; Allman-Farinelli, M.; Shackel, N. Serum 25-hydroxyvitamin D deficiency and hepatic encephalopathy in chronic liver disease. World J. Hepatol. 2017, 9, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Afifi, M.A.E.; Hussein, A.M.; Rizk, M. Low Serum 25-Hydroxy Vitamin D (25-OHD) and Hepatic Encephalopathy in HCV-Related Liver Cirrhosis. Int. J. Hepatol. 2021, 8, CD011564. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.Y.; Wu, X.R.; Li, H.X.; Li, S.W.; Lu, T.; Zhong, Y.M.; Yu, M.F. Study on correlation between serum 25-hydroxyvitamin D3 level and esophageal variceal bleeding in cirrhotic patients. Zhonghua Gan Zang Bing Za Zhi Chin. J. Hepatol. 2019, 27, 358–362. [Google Scholar]
- Lima, T.B.; Santos, L.A.A.; de Carvalho Nunes, H.R.; Silva, G.F.; Caramori, C.A.; Qi, X.; Romeiro, F.G. Safety and efficacy of risedronate for patients with esophageal varices and liver cirrhosis: A non-randomized clinical trial. Sci. Rep. 2019, 9, 18958. [Google Scholar] [CrossRef]
- Anty, R.; Tonohouan, M.; Ferrari-Panaia, P.; Piche, T.; Pariente, A.; Anstee, Q.M.; Gual, P.; Tran, A. Low levels of 25-hydroxy vitamin D are independently associated with the risk of bacterial infection in cirrhotic patients. Clin. Transl. Gastroenterol. 2014, 5, e56. [Google Scholar] [CrossRef]
- Buonomo, A.R.; Arcopinto, M.; Scotto, R.; Zappulo, E.; Pinchera, B.; Sanguedolce, S.; Perruolo, G.; Formisano, P.; Cittadini, A.; Gentilucc, U.V.; et al. The serum-ascites vitamin D gradient (SADG): A novel index in spontaneous bacterial peritonitis. Clin. Res. Hepatol. Gastroenterol. 2019, 43, e57–e60. [Google Scholar] [CrossRef]
- Hafez, H.A.; Madani, H.; Alem, S.A.; Farrag, A.; Fathy, W.; Abdo, M. Is Serum-Ascites Vitamin D Gradient a Valid Marker for Diagnosing Spontaneous Bacterial Peritonitis in Patients with Cirrhotic Ascites? Lab. Med. 2021, 52, 567–573. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, L.; Ma, L.; Lv, C.; Ding, Y.; Xia, T.; Wang, J.; Dou, X. Vitamin D status and expression of vitamin D receptor and LL-37 in patients with spontaneous bacterial peritonitis. Dig. Dis. Sci. 2012, 57, 182–188. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Al-Karmalawy, A.A.; El-Kholy, A.A.; El-Damas, D.A.; Abostate, H.M.; Mostafa, S.M.; Hamada, M.; Elkady, M.A.K.; Hassan, Y.; AL-Hussain, E.; et al. Effect of Vitamin D supplementation in patients with liver cirrhosis having spontaneous bacterial peritonitis: A randomized controlled study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6908–6919. [Google Scholar]
- Marasco, G.; Dajti, E.; Ravaioli, F.; Brocchi, S.; Rossini, B.; Alemanni, L.V.; Peta, G.; Bartalena, L.; Golfieri, R.; Festi, D.; et al. Clinical impact of sarcopenia assessment in patients with liver cirrhosis. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 377–388. [Google Scholar] [CrossRef]
- Marasco, G.; Serenari, M.; Renzulli, M.; Alemanni, L.V.; Rossini, B.; Pettinari, I.; Dajti, E.; Ravaioli, F.; Golfieri, R.; Cescon, M.; et al. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J. Gastroenterol. 2020, 55, 927–943. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Girgis, C.M.; Cha, K.M.; So, B.; Tsang, M.; Chen, J.; Houweling, P.J.; Schindeler, A.; Stokes, R.; Swarbrick, M.M.; Evesson, F.J.; et al. Mice with myocyte deletion of vitamin D receptor have sarcopenia and impaired muscle function. J. Cachexia Sarcopenia Muscle 2019, 10, 1228–1240. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Atsukawa, M.; Tsubota, A.; Ono, H.; Kawano, T.; Yoshida, Y.; Arai, T.; Hayama, K.; Itokawa, N.; Kondo, C.; et al. Effect of vitamin d supplementation on skeletal muscle volume and strength in patients with decompensated liver cirrhosis undergoing branched chain amino acids supplementation: A prospective, randomized, controlled pilot trial. Nutrients 2021, 13, 1874. [Google Scholar] [CrossRef]
- Uchitomi, R.; Oyabu, M.; Kamei, Y. Vitamin d and sarcopenia: Potential of vitamin D supplementation in sarcopenia prevention and treatment. Nutrients 2020, 12, 3189. [Google Scholar] [CrossRef]
- Colombo, M.; de Franchis, R.; Del Ninno, E.; Sangiovanni, A.; De Fazio, C.; Tommasini, M.; Donato, M.F.; Piva, A.; Di Carlo, V.; Dioguardi, N. Hepatocellular carcinoma in Italian patients with cirrhosis. N. Engl. J. Med. 1991, 325, 675–680. [Google Scholar] [CrossRef]
- Fedirko, V.; Duarte-Salles, T.; Bamia, C.; Trichopoulou, A.; Aleksandrova, K.; Trichopoulos, D.; Trepo, E.; Tjønneland, A.; Olsen, A.; Overvad, K.; et al. Prediagnostic circulating vitamin D levels and risk of hepatocellular carcinoma in European populations: A nested case-control study. Hepatology 2014, 60, 1222–1230. [Google Scholar] [CrossRef]
- Gaksch, M.; Jorde, R.; Grimnes, G.; Joakimsen, R.; Schirmer, H.; Wilsgaard, T.; Mathiesen, E.B.; Njølstad, I.; Løchen, M.-L.; März, W.; et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE 2017, 12, e0170791. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, X.; Li, X.; Găman, M.-A.; Kord-Varkaneh, H.; Rahmani, J.; Salehi-Sahlabadi, A.; Day, A.S.; Xu, Y. Serum Vitamin D Levels and Risk of Liver Cancer: A Systematic Review and Dose-Response Meta-Analysis of Cohort Studies. Nutr. Cancer 2021, 73, 1–9. [Google Scholar] [CrossRef]
- Fang, A.; Long, J.; Zhang, Y.; Liu, Z.; Li, Q.; Zhang, D.; Luo, Y.; Zhong, R.; Zhou, Z.; Xu, Y.; et al. Serum Bioavailable, Rather Than Total, 25-hydroxyvitamin D Levels Are Associated With Hepatocellular Carcinoma Survival. Hepatology 2020, 72, 169–182. [Google Scholar] [CrossRef]
- Liu, H.; Jiang, X.; Qiao, Q.; Chen, L.; Matsuda, K.; Jiang, G.; Yu, T.; Wang, Y.; Lin, H.; Liang, X.; et al. Association of circulating 25-Hydroxyvitamin D and its related genetic variations with hepatocellular carcinoma incidence and survival. Ann. Transl. Med. 2020, 8, 1080. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, L.; Xu, H.-J.; Li, Y.; Hu, C.-M.; Yang, J.-Y.; Sun, M.-Y. The Anti-Inflammatory Effects of Vitamin D in Tumorigenesis. Int. J. Mol. Sci. 2018, 19, 2736. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Chung, F.-L. Oxidative stress and hepatocarcinogenesis. Hepatoma Res. 2018, 4, 39. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, R.; Banik, S.; Chatterjee, M. Inhibitory effect of vitamin D 3 on 3′methyl-4-dimethyl-amino-azobenzene-induced rat hepatocarcinogenesis: A study on Antioxidant Defense Enzymes. J. Exp. Ther. Oncol. 2002, 2, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, A.R.; El-Mesery, M.; El-Karef, A.; Eissa, L.A. Vitamin D potentiates anti-tumor activity of 5-fluorouracil via modulating caspase-3 and TGF-β1 expression in hepatocellular carcinoma-induced in rats. Can. J. Physiol. Pharmacol. 2018, 96, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Katz, L.H.; Muñoz, N.M.; Gu, S.; Shin, J.; Jogunoori, W.S.; Lee, M.-H.; Belkin, M.D.; Kim, S.-B.; White, J.C.; et al. Vitamin D Deficiency Promotes Liver Tumor Growth in Transforming Growth Factor-β/Smad3-Deficient Mice through Wnt and Toll-like Receptor 7 Pathway Modulation. Sci. Rep. 2016, 6, 30217. [Google Scholar] [CrossRef] [PubMed]
- Iseki, K.; Tatsuta, M.; Uehara, H.; Iishi, H.; Yano, H.; Sakai, N.; Ishiguro, S. Inhibition of angiogenesis as a mechanism for inhibition by 1alpha-hydroxyvitamin D3 and 1,25-dihydroxyvitamin D3 of colon carcinogenesis induced by azoxymethane in Wistar rats. Int. J. Cancer 1999, 81, 730–733. [Google Scholar] [CrossRef]
- Arteh, J.; Narra, S.; Nair, S. Prevalence of Vitamin D Deficiency in Chronic Liver Disease. Dig. Dis. Sci. 2010, 55, 2624–2628. [Google Scholar] [CrossRef]
- Finkelmeier, F.; Kronenberger, B.; Köberle, V.; Bojunga, J.; Zeuzem, S.; Trojan, J.; Piiper, A.; Waidmann, O. Severe 25-hydroxyvitamin D deficiency identifies a poor prognosis in patients with hepatocellular carcinoma—A prospective cohort study. Aliment. Pharmacol. Ther. 2014, 39, 1204–1212. [Google Scholar] [CrossRef]
- Falleti, E. Vitamin D receptor gene polymorphisms and hepatocellular carcinoma in alcoholic cirrhosis. World J. Gastroenterol. 2010, 16, 3016. [Google Scholar] [CrossRef]
- Abdel-Mohsen, M.A.; El-Braky, A.A.-A.; Ghazal, A.A.E.-R.; Shamseya, M.M. Autophagy, apoptosis, vitamin D, and vitamin D receptor in hepatocellular carcinoma associated with hepatitis C virus. Medicine 2018, 97, e0172. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Yang, S.; Lao, X.; Li, R.; Chen, Z.; Wang, J.; Qin, X.; Li, S. Association of Single Nucleotide Polymorphisms in VDR and DBP Genes with HBV-Related Hepatocellular Carcinoma Risk in a Chinese Population. PLoS ONE 2014, 9, e116026. [Google Scholar] [CrossRef] [PubMed]
- Whitcomb, B.P.; Mutch, D.G.; Herzog, T.J.; Rader, J.S.; Gibb, R.K.; Goodfellow, P.J. Frequent HOXA11 and THBS2 promoter methylation, and a methylator phenotype in endometrial adenocarcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 2277–2287. [Google Scholar]
- Marik, R.; Fackler, M.; Gabrielson, E.; Zeiger, M.A.; Sukumar, S.; Stearns, V.; Umbricht, C.B. DNA methylation-related vitamin D receptor insensitivity in breast cancer. Cancer Biol. Ther. 2010, 10, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Smirnoff, P.; Liel, Y.; Gnainsky, J.; Shany, S.; Schwartz, B. The protective effect of estrogen against chemically induced murine colon carcinogenesis is associated with decreased CpG island methylation and increased mRNA and protein expression of the colonic vitamin D receptor. Oncol. Res. 1999, 11, 255–264. [Google Scholar] [PubMed]
- Abdalla, M.; Khairy, E.; Louka, M.L.; Ali-Labib, R.; Ibrahim, E.A.-S. Vitamin D receptor gene methylation in hepatocellular carcinoma. Gene 2018, 653, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Dalhoff, K.; Dancey, J.; Astrup, L.; Skovsgaard, T.; Hamberg, K.J.; Lofts, F.J.; Rosmorduc, O.; Erlinger, S.; Hansen, J.B.; Steward, W.P.; et al. A phase II study of the vitamin D analogue Seocalcitol in patients with inoperable hepatocellular carcinoma. Br. J. Cancer 2003, 89, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Finlay, I.G.; Stewart, G.J.; Ahkter, J.; Morris, D.L. A phase one study of the hepatic arterial administration of 1,25-dihydroxyvitamin D 3 for liver cancers. J. Gastroenterol. Hepatol. 2001, 16, 333–337. [Google Scholar] [CrossRef]
- Wu, Y.-Q.; Fan, W.-Z.; Xue, M.; Guo, J.; Wei, J.-L.; Wang, Y.; Yao, W.; Zhao, Y.; Li, J.-P. 25-OH-vitamin D deficiency identifies poor tumor response in hepatocellular carcinoma treated with transarterial chemoembolization. Clin. Transl. Oncol. 2020, 22, 70–80. [Google Scholar] [CrossRef]
- Morris, D.; Jourdan, J.-L.; Finlay, I.; Gruenberger, T.; The, M.; Pourgholami, M. Hepatic intra-arterial injection of 1,25-dihydroxyvitamin D3 in lipiodol: Pilot study in patients with hepatocellular carcinoma. Int. J. Oncol. 2002, 21, 901–906. [Google Scholar] [CrossRef]
- Matsuda, A.; Ishiguro, K.; Yan, I.K.; Patel, T. Therapeutic Efficacy of Vitamin D in Experimental c-MET-β-Catenin-Driven Hepatocellular Cancer. Gene Expr. 2019, 19, 151–159. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Target | Action |
|---|---|
| Non-Liver Diseases | |
| IMMUNE SYSTEM | Reduced risk of respiratory infection, such as tuberculosis and COVID-19 and sepsis. |
| Improved response to steroid treatment in autoimmune disease, like psoriasis, type 1 diabetes, multiple sclerosis, rheumatoid arthritis. | |
| INSULIN SENSITIVITY | Better control of insulin secretion of pancreatic β-cell. Improved insulin resistance, marked by a decrease in HOMA-IR |
| CARCINOGENESIS | Reduced risk of breast, colon, pancreatic and prostate cancer |
| Liver Disease | |
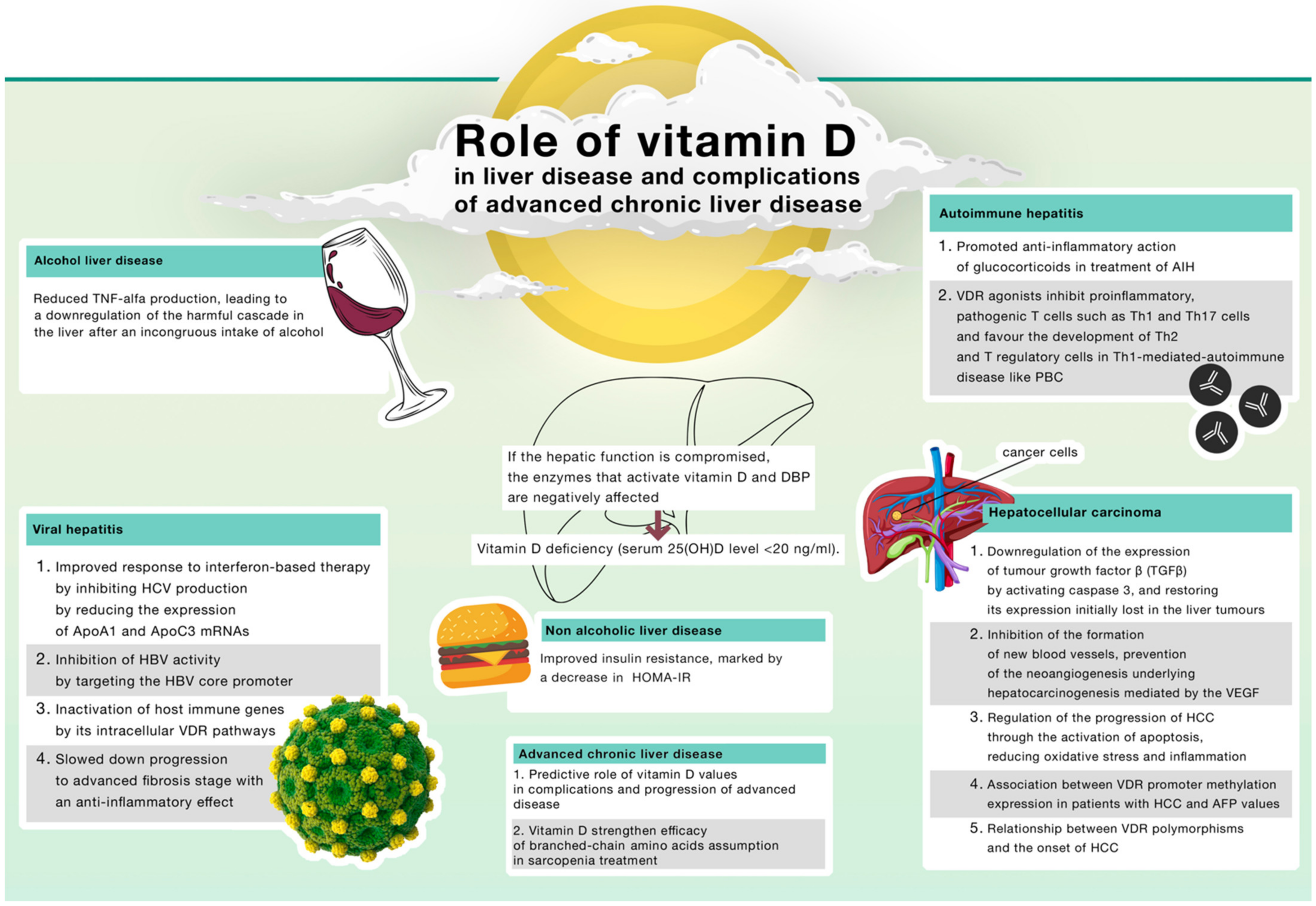
| VIRAL HEPATITIS | Improved response to interferon-based therapy by inhibiting HCV production by reducing the expression of ApoA1 and ApoC3 mRNAs |
| Inhibition of HBV activity by targeting the HBV core promoter | |
| Inactivation of host immune genes by its intracellular VDR pathways | |
| Slowed down progression to advanced fibrosis stage with an anti-inflammatory effect | |
| NAFLD | Improved insulin resistance, marked by a decrease in Homeostasis Model Assessment Insulin Resistance (HOMA-IR) |
| ALD | Reduced TNF-alfa production, leading to a downregulation of the harmful cascade in the liver after an incongruous intake of alcohol |
| AIH | Promoted anti-inflammatory action of glucocorticoids in treatment of AIH |
| VDR agonists inhibit proinflammatory, pathogenic T cells such as Th1 and Th17 cells and favour the development of Th2 and T regulatory cells in Th1-mediated-autoimmune disease like PBC | |
| ACLD | Antibacterial immune response to SBP of VDR system and its downstream gene LL-37 |
| More significant increase in the skeletal mass index compared with only branched-chain amino acids assumption in sarcopenia treatment | |
| HCC | Downregulation of the expression of tumour growth factor β (TGFβ) by activating caspase 3, and restoring its expression initially lost in the liver tumours |
| Inhibition of the formation of new blood vessels, prevention of the neoangiogenesis underlying hepatocarcinogenesis mediated by the VEGF | |
| Regulation of the progression of HCC through the activation of apoptosis, reducing oxidative stress and inflammation | |
| Relationship between VDR polymorphisms and the onset of HCC | |
| Association between VDR promoter methylation expression in patients with HCC and AFP values | |
| Identifier | Study Title | Study Tipe | Intervention | Status |
|---|---|---|---|---|
| NCT01575717 | The Effect of Vitamin D Repletion in Patients with Hepatocellular Carcinoma on the Orthotopic Liver Transplant List Interventional | Interventional | Drug: Vitamin D3 4000 IU Drug: Vitamin D3 2000 IU | Unknown |
| NCT02779465 | Oral Vitamin D Treatment for the Prevention of Hepatocellular Carcinoma Interventional | Interventional | Drug: Vitamin D3 | Not yet recruiting |
| NCT01956864 | Study of High-Dose Oral Vitamin D for the Prevention of Liver Cancer Interventional | Interventional | Drug: Vitamin D | Withdrawn |
| NCT02461979 | The Role of the Vitamin D Receptor Gene Polymorphisms in Hepatocarcinogenesis Interventional | Interventional | Other: The VDR genotype | Recruiting |
| IU: International Unit | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ravaioli, F.; Pivetti, A.; Di Marco, L.; Chrysanthi, C.; Frassanito, G.; Pambianco, M.; Sicuro, C.; Gualandi, N.; Guasconi, T.; Pecchini, M.; et al. Role of Vitamin D in Liver Disease and Complications of Advanced Chronic Liver Disease. Int. J. Mol. Sci. 2022, 23, 9016. https://doi.org/10.3390/ijms23169016
Ravaioli F, Pivetti A, Di Marco L, Chrysanthi C, Frassanito G, Pambianco M, Sicuro C, Gualandi N, Guasconi T, Pecchini M, et al. Role of Vitamin D in Liver Disease and Complications of Advanced Chronic Liver Disease. International Journal of Molecular Sciences. 2022; 23(16):9016. https://doi.org/10.3390/ijms23169016
Chicago/Turabian StyleRavaioli, Federico, Alessandra Pivetti, Lorenza Di Marco, Christou Chrysanthi, Gabriella Frassanito, Martina Pambianco, Chiara Sicuro, Noemi Gualandi, Tomas Guasconi, Maddalena Pecchini, and et al. 2022. "Role of Vitamin D in Liver Disease and Complications of Advanced Chronic Liver Disease" International Journal of Molecular Sciences 23, no. 16: 9016. https://doi.org/10.3390/ijms23169016