
























{%comp-FFFFFF-bl%}
Angela Bordeaux had always been on the high end of functioning for someone with Down syndrome. She could read and write, and once even won a contest for her poem about an otter at the Oregon Zoo. But when she started having behavior issues at her day program in Portland, her parents, Nancy and David Bordeaux, became concerned. By her late 20s, she was having trouble reading, and by 31, Angela could no longer read or write her name.
The staff at the day program urged her parents to take her to a specialist, who gave them a surprising diagnosis. Angela had a condition that typically affects individuals more than twice her age.
Angela was one of the youngest patients he’d ever seen with Alzheimer’s disease.
There’s a growing recognition among families and caregivers of what researchers had discovered years ago, that individuals with Down syndrome will invariably develop the pathology of Alzheimer’s disease starting as early as their second decade of life. And if they live long enough, most will develop the dementia and clinical symptoms as well.
Now that their life expectancy has been stretched into the 50s and 60s, individuals with Down syndrome represents the single largest group with a genetic predisposition for Alzheimer’s disease. As such, they have become the primary study group for new Alzheimer’s tests, preventive treatments and potential cures. {%qr-Their great gift to the world will be the curing of Alzheimer’s disease.%em Huntington Potter, Linda Crnic Institute for Down Syndrome%}
It now appears these individuals, who historically have been undervalued and unappreciated to the point that expectant parents often decide to terminate their pregnancies rather than have a child with Down syndrome, might hold the key to unlocking the mysteries of arguably the most feared disease of aging.
“Their great gift to the world,” said Huntington Potter, a researcher with the Linda Crnic Center for Down Syndrome in Denver, “will be the curing of Alzheimer’s disease.”
The Bordeauxs, who moved to Redmond four years ago, had felt called as Christians to adopt three children with Down syndrome.
“In the ’70s, it was a very disposable society,” David, a former Multnomah County parole officer, said. “And we decided that God put in our hearts to adopt these kids.”
Nancy had been in nursing school, and the last baby born during her training program had Down syndrome. They adopted Zach, now 39, when he was 7 days old, and Angela, 38, four years later. LaToyya, 31, came to them from Kansas in the late 1980s. Angela’s diagnosis came almost by coincidence. The staff had just completed a training on Down syndrome and Alzheimer’s around the time her issues began to emerge.
{%pl-3366409%}
“If a normal person suddenly couldn’t read, you would realize something was wrong,” Nancy said. “But a person with Down syndrome, they already have deficits, so when they get Alzheimer’s, it’s not as obvious.”
Doctors put Angela on the Alzheimer’s medication Aricept, and initially it seemed to help.
“Mom, I can read again,” she proclaimed after several months, but the recovery was short-lived. Now she can only write her name by copying the letters or if someone spells it out for her.
Nobody had ever told the Bordeauxs to look out for Alzheimer’s as their children aged. And while Angela’s diagnosis caught them off guard, they recognized the symptoms when LaToyya started having similar issues. She began to forget things, such as asking when they were going to have dinner just after they had eaten. At times, she would break out in gibberish. Soon, doctors gave LaToyya the same diagnosis, and now Nancy wonders whether Zach is similarly affected. A bout of meningitis when he was 4 years old further sapped his limited cognitive abilities, making an accurate diagnosis difficult.
“He probably does have Alzheimer’s because he has the gene for it,” she said. “But he functions so low because of his meningitis that we don’t know.”
The Bordeauxs say they will continue to care for all three at home as long as they can do so safely.
“I really don’t know what the future is,” Nancy said. “Other than I expect them to continue to decline.”
New connections
The life expectancy for someone with Down syndrome born in 1907 was a mere 9 years. Today, they routinely live into their 60s, mainly due to better treatment of congenital heart defects and infection. Mainstreaming rather than institutionalizing individuals with Down syndrome also has allowed them to live healthier, more productive lives and is paying huge dividends in terms of longevity. But that has pushed more of them into the decades of life where Alzheimer’s becomes more probability than possibility.
Researchers estimate that about 10 to 35 percent of those with Down syndrome will develop dementia in their 40s, and 40 to 75 percent in their 60s. If they live longer, the rate might get closer to universal.
Down syndrome occurs when an individual is born with an extra full or partial copy of chromosome 21, resulting in common physical traits such as small stature, poor muscle tone and a distinct facial appearance, and intellectual deficits ranging from mild to moderate. The condition also appears to prematurely age individuals, leading them to show the classic signs of aging up to 20 years earlier than the general population.
But what few people realize is that Alzheimer’s disease occurs by essentially the same process. And it was Potter who first proposed this connection.
{%pf-3420116%}
In the 1960s, pathologists examining the brains of individuals with Down syndrome found the same plaques and tangles that characterize Alzheimer’s disease. By the late 1980s, Alzheimer’s researchers discovered the amyloid precursor protein gene, which produces a protein that, when cleaved, forms the amyloid beta peptide that accumulates to form plaques and tangles.
The APP gene is located on chromosome 21, the very chromosome of which individuals with Down syndrome have an extra copy. It’s why Down syndrome is also called trisomy 21, meaning having three copies of the chromosome. But that means they also have an extra copy of the APP gene and so produce and accumulate much more amyloid beta.
In 1991, Potter, then a young associate professor at Harvard University, proposed a provocative theory that Alzheimer’s and Down syndrome were, in fact, the same phenomenon. He suggested that as some individuals age, through genetic mutations, they develop cells with three copies of chromosome 21. They become what geneticists call mosaic, with some of their cells having two copies and some having three copies. The cells with three copies would produce more of the amyloid beta peptide that leads to Alzheimer’s.
The theory seemed crazy at first. Potter and his colleagues submitted a paper describing the theory for publication and received a four-line rejection letter, opening with, “I would not recommend publishing this paper anytime, anywhere.”
But in 1999, a post-doc student in Potter’s lab showed that 6 to 8 percent of skin cells in people with typical age-related Alzheimer’s disease contained three copies of chromosome 21, and subsequent research showed similar results for brain cells. And when researchers looked at MRIs of brains affected by Down syndrome they looked identical to those with Alzheimer’s.
“That started out as a hypothesis and over the past 20 years, the hypothesis is proving to be correct,” Potter said. “The data are pretty incontrovertible now.”
The great divide
The link to a condition as high profile as Alzheimer’s disease has brought new attention, new resources and new grants to Down syndrome research.
But in local communities, for the most part, the support structures for individuals dealing with those conditions have remained separate. Down syndrome and Alzheimer’s disease organizations did not have a history of working together, and local and state agencies for developmental disabilities and aging have for most part remained separate. As a result, families and caregivers for aging individuals with Down syndrome often fall through the cracks, their needs not fully served or understood by either side.
“That’s a real challenge, and to be honest, I don’t think the care systems, the agencies that exist in the community are really geared up to face this kind of issue,” said Matt Janicki, a professor of Disability and Human Development at the University of Illinois at Chicago. “There’s just not a lot of communication between the aging system and the disability system.”
Moreover, the lack of resources puts extra pressure on parents who have cared for a son or daughter with Down syndrome all their lives, only to find that the demands for their caregiving increase just as their ability to meet them begins to wane.
{%pl-3377626%}
Richard Marshall, 49, came to stay with Betty and Frank Kodera in York, Nebraska, in 1971 when he was just 5 years old. They had already raised two boys, one of whom was working a summer job with a local agency for the developmentally disabled. The staff was desperately searching for a family to take a young boy with Down syndrome. If they couldn’t find a home for him within a few weeks, the boy would be put in an institution.
“Leave him here until you find someone,” Frank recalls telling his son. “Well, they didn’t find someone.”
The Koderas knew little about Down syndrome at the time. They had only seen one other person with the condition, a man who never ventured beyond the fence surrounding his front yard.
“We just figured we’d treat him like our two boys,” Betty said. “We just figured it would take longer.”
For more than 40 years, they cared for Richard, shepherding him through school and work programs as they moved from Nebraska to Washington to Montana and back again. He worked various jobs operating a drill press, processing seafood, sorting recyclables. Then several years ago, on a family trip to Wyoming, they awoke one night to find Richard confused and trying to open the door of their motel room. It was one of the first signs that something was wrong.
He started having trouble at work as well, confused about how to perform the simple tasks he had done hundreds of times before. His doctor advised them to rule out more benign possibilities but eventually in 2010, a neurologist in Lincoln, Nebraska, confirmed Richard had Alzheimer’s disease.
“He spent 15 minutes with us and said, ‘This is what you’ve got. I’ll give you some pills, and there’s nothing else I can do,’” Betty recalled. “They drop a time bomb in your lap and say, ‘Go home.’”
Richard began to decline quickly. He wouldn’t sleep at night and developed seizures and hallucinations. His behavior became erratic. He became terrified of a hallway mirror and once wrapped a blanket around it to hide its reflection. He took family photos off the refrigerator and hid or destroyed them. {%pl-3377625%}
Having reached their 80s and starting to slow down themselves, Frank and Betty realized they could no longer care for Richard at home. When they found a care home that could take Richard an hour away in Hebron, Nebraska, they sold their house and moved there to be closer to him.
“We’re getting too old to be driving 50 miles on a regular basis. We wanted to see him more than once a month,” Frank said. “After someone has been with you for 43 years, you’re pretty much loving the guy.”
Richard entered the care home in April 2013. By July he could no longer walk or talk and developed swallowing difficulties. The Koderas visit regularly, often at lunch time to help feed him. They would like to take him home for visits but are no longer up to the task. Even leaning him in his wheelchair to tie a bib on him is a difficult challenge for the couple.
“He has to have help with everything that he does,” Betty said. “Between the two of us, we couldn’t do it.”
The shadow looms
The average age of onset of dementia among individuals with Down syndrome is 52, which means parents are generally in their 70s or 80s when it hits. Often, one of the parents has started to show signs of dementia as well, leaving the other to care for two individuals.
It’s a fear that Judy Marick, of Portland, faces now on a daily basis. Her husband, Jim, has Alzheimer’s and is in a group home. Her son Jason, 39, has Down syndrome and lives at home with her.
“At this point, Jason doesn’t have Alzheimer’s, but it looms very close to my heart. It just sounds like he’s going to get it,” she said. “It seems every time Jason repeats a question two or three times I automatically think, ‘Oh no, am I seeing the first signs of Alzheimer’s now?’”
{%pr-3377554%}
Marick had never expected her son to make it to 40. She hasn’t told Jason of his increased risk but has told him his father has an illness that is affecting his brain.
“Jason has a real fear of ‘getting what Daddy has,’” she said. “He is seeing Jim deteriorate, and Jim had gone through a segment of being aggressive and combative. And that was very scary for him.”
Marick, 75, has sought information and support from other parents she’s come to know over the decades as their children came up together through the disability system, schools and day programs.
“Alzheimer’s and Down syndrome is something that parents just really fear,” she said. “This is a topic that comes up a lot. Have you heard any more? Have you heard the latest? It’s just a real, real fear.”
One of those friends is Yvonne Jordan, of Lake Oswego, whose son, Michael, is 41.
“The secret words are people with Down syndrome ‘have a higher incidence of …’” she said. “And they just throw those at you all the way through your life, this just whole heck of a long list of things.”
Michael lived with his mother until moving to a group home three years ago. He still works four days a week, and volunteers with the Red Cross on Fridays. But the Jordans have a family history of Alzheimer’s, so she worries that could double his genetic risk.
“Anytime we would see something about Down syndrome and Alzheimer’s, you’re shaking in your boots a little bit,” she said. “Mainly because all of us have some base of what Alzheimer’s is all about.”
Often, by the time dementia hits, parents have died or are in no shape to provide additional care. It can then fall to siblings to pick up the slack, creating a sandwich generation like no other.
“We kind of joke that we’re sort of the club sandwich generation,” said Sarah Jurcyk, of Kansas City, Kansas, who is the legal guardian of her sister, Lucy. “Because we’re not only caring for our parents and we have kids, now we have a sibling to take care of. It’s like a triple-decker thing, supporting three generations of people.”
Still, individuals with Down syndrome tend to unite a family, rather than divide it. Statistically, parents of children with Down syndrome are less likely to get divorced, and brothers and sisters routinely respond in surveys that their lives are richer for the experience.
Father Francis Hilton, a Jesuit priest from Metuchen, New Jersey, took over as legal guardian of his younger sister, Judith, who had Down syndrome after their mother died in 2006. The family had begun to suspect something was wrong with Judith three years earlier, when her boss expressed some concerns. The family attributed it to stress over losing her father to lung cancer and seeing her mom decline after breaking a hip. In the summer of 2003, Hilton took Judith, then 41, to see specialists at Rutgers University Medical Center. By the third visit, the doctors told him there was no other explanation: Judith had Alzheimer’s.
{%pl-3377536%}
When they returned to their parents’ house, Judith bounded up the stairs and told her mother how nice the doctors had been and about the lunch with her brother by the ocean shore. When she left the room, her mother asked Hilton what he had learned.
“Judith has Alzheimer’s, and I can’t figure out why she’s so happy right now,” he told her.
“At some level, she knows she’s going to be in good hands,” his mother replied.
In that moment, Hilton realized he had just inherited the responsibility of ensuring his sister’s well-being.
“My parents had given their lives to making Judith’s world. It was time for them to move on and pass the torch,” he said. “And there’s no torch I would rather have received.”
Judith was the youngest of eight children in the Hilton family.
“She was born at a time when there really wasn’t a lot going on for kids with intellectual disabilities,” Hilton said. “So Judith really lived her whole life on the edge of whatever good stuff was going on.”
She was part of the movement in New Jersey at the time for greater inclusion of the developmentally disabled, and Judith accumulated a number of firsts along the way: attending the first classes for individuals with developmental disabilities, being the first student with Down syndrome at her high school, and the first with Down syndrome at her worksite.
“She was the first person with Down syndrome to go on a cruise to Bermuda on her own,” Hilton said.
When she was diagnosed with Alzheimer’s, the doctors told him what to expect. The first thing that will happen, they said, is she will break one or both of her feet as she struggles to adapt to her changing perceptions of the world around her. In short order, Judith broke one foot, and then the week her mother died, she broke the other stepping awkwardly off the stairs.
Much to her family’s chagrin, Judith’s favorite movie was “Dirty Dancing,” and she would annoy the Catholic family by reciting lines from the racy film. But “The Wizard of Oz” ran a close second, and she rarely missed an opportunity to watch it.
“I feel like the scarecrow,” she told her brother six months after her diagnosis. “My head is full of straw.”
Hilton eventually quit his job as a department chair at Rutgers University and took a sabbatical to spend more time with Judith. She had several bouts of aspirational pneumonia, a common problem for individuals with Down syndrome and Alzheimer’s as swallowing becomes more difficult. Judith had lost the ability to walk and spent much of her day in bed. She had continued to decline steadily over the five years after her diagnosis, until a weekend in November 2011.
Hilton was grading papers at her bedside and they were watching the Giants football game on the TV. For reasons still unclear, Judith seemed to make a remarkable rally. She noticed for the first time the feeding tube in her nose. She questioned why her brother was giving the students all those red marks on their papers, and when the Wicked Witch of the West appeared on the television screen, Judith became animated.
“She was really acting like the Alzheimer’s had gone away,” Hilton said. Her nurses couldn’t believe the difference, asking Hilton what he had done to precipitate such a drastic change.
Then late Tuesday night, at a time when it’s never good news, Hilton’s phone rang.
Judith had felt so good that, for the first time in years, she had tried to get out of bed. She caught her foot on the bedsheet and fell, breaking her neck.
“That was the end of life as I knew it,” Hilton said. “I was there for her life, but I wasn’t there for her final day. Judith died all by herself.”
{%pc-3377545%}
Hilton said his family knew little of the increased risk for Alzheimer’s. They had always been told Judith would have heart problems, but it wasn’t until she was in her 40s that anyone mentioned the risk of dementia. News of the link has been slow to filter through to families, and even when it does, they often are in denial.
“It’s hard for families to accept that this is inevitable, because you’ve worked so long and hard to change the school systems and get them integrated, and then you get hit with this at the end,” said Leone Murphy, a nurse practitioner working with individuals with developmental disabilities and an instructor at Rutgers University. “So many families are still not even able to accept that this is coming.”
Murphy’s daughter, Michelle, has Down syndrome and watched two of her closest friends, including Judith Hilton, as they declined and ultimately died from Alzheimer’s. Michelle spoke at a conference two years ago about what it was like to see her best friends fade away, lose the ability to feed themselves, and forget her name.
Michelle has shown no signs of dementia, but having seen it firsthand, Murphy knows she must prepare for that likelihood. But there are few provisions in the community for those with intellectual disabilities and dementia. Neither day programs nor the group homes are prepared for it, nor are there many specialized facilities to meet their unique needs. Murphy said individuals often end up in nursing homes surrounded by elderly residents.
“Every time I go to a nursing home, I see people with Down syndrome just sitting, vegetating in the corner,” she said. “It’s really sad. We need to come up with a place where we can take care of them, where they could possibly age in place.”
Gains and losses
Just east of the parkway running through Bend sits a nondescript apartment complex that was born of parents’ hopes and dreams but now harbors more than its fair share of fears. More than 20 years ago, a group of parents with children with developmental disabilities banded together under the name Central Oregon Transition Plus with the goal of mapping out a better future for their children. When it was time for their children to leave home and lead more independent lives, they wanted to find safe and secure housing for them but realized no such place existed. {%pr-3382880%}
Through a partnership with Cascades Community Development, they opened two apartment complexes and a group home with just enough staffing to help the residents live on their own. The three units now house a combined 29 residents with developmental disabilities ranging in age from 29 to 58, including six individuals with Down syndrome.
That means several of the residents, such at Matt Wilson, 33, are reaching the age when Alzheimer’s symptoms typically appear for the first time.
“Matt’s grandmother died of Alzheimer’s in 2000,” his mother, Pam Wilson, said. “Ever since then I’ve watched for it very closely.”
Wilson hopes that even if her son starts to show signs of dementia, he will be able to stay at the complex with additional support services. But there is also an understanding among the parents that residents must be able to live relatively independently to stay there.
“If he became unstable in his living environment, where he would be a danger to himself, then there would have to be a decision made,” Wilson said. “He would have to go live in an environment where it would be safer for him.”
While the COTP parents have made individual plans to ensure their children will have ongoing support after they’re gone, they also take solace in knowing that the community of parents will look out for all of the residents.
“When one of the kids needs help, we all come together,” said Karen Blanford, whose 42-year-old daughter, Jenny, has Down syndrome. “So hopefully someone in the group can help them find the services they might need.”
For many parents and siblings, the looming threat of Alzheimer’s represents a cruel twist of fate for individuals who were born at a disadvantage and have been trying all their lives to catch up. The very families that fought for inclusion and acceptance over the past three to four decades are now among the first to face the stark reality that Alzheimer’s threatens to unravel all of their hard work.
“When Jason was born, it was all about early intervention,” Marick said. “We all absorbed information and wanted to push our kids. We did everything and offered them everything for that reason. They were just going to be super people with Down syndrome. And in the last 10 years, we’ve realized that it can all be taken from them.”
The nation is already struggling with how it will take care of the millions of additional cases of Alzheimer’s disease as the baby boomer generation ages. But within that larger demographic wave there exists a more intense riptide of individuals with Down syndrome facing the same issue. With gains in longevity, the number of individuals living with Down syndrome is expected to double from 642,000 in 2000 to 1.2 million by 2030. With no reliable treatments for Alzheimer’s, efforts to help affected individuals now focus on early diagnosis to help accommodate their diminishing skills.
But families, providers and caregivers will have to get much better at recognizing the early signs of Alzheimer’s in order to help. Individuals with Down syndrome face myriad health issues as they age. Separating what is Alzheimer’s disease from what is a thyroid problem or sleep apnea or a B12 deficiency is often impossible.
“I think the important thing is to make sure you’re not attributing Alzheimer’s disease to something else,” said Dr. Brian Chicoine, co-founder and medical director of the Adult Down Syndrome Center of Lutheran General Hospital in Park Ridge, Illinois. “We certainly see folks who have depression that looks like Alzheimer’s disease that got better when you treated the depression.”
The center was launched in 2012 and has seen more than 5,500 adolescents and adults with Down syndrome, whose symptoms of aging are often overlooked by less experienced eyes. The clinic’s providers are careful to rule out other conditions before settling on an Alzheimer’s diagnosis.
“But there are certainly patients that see me for the first time that have enough of a pattern that I’d be pretty flabbergasted if I found something else,” Chicoine said. {%pc-3377560%}
When normal adults start to forget or act erratically in their later years, family and friends are quick to suspect Alzheimer’s. But when individuals with Down syndrome act similarly, it’s often attributed to their intellectual disabilities instead.
“When symptoms start, it’s too easy to blame the person because you don’t know what’s happening,” said Sharon Miller, of Burbank, California.
Miller’s sister, Robin Trocki, came to live with her more than 20 years ago, after their mother died in New Jersey. For years, Robin worked in a bakery and a supermarket. She had her artwork published in a book and played Sue Sylvester’s sister on the television show “Glee.”
Her first symptoms of Alzheimer’s began to appear about age 50.
“She would have trouble with forgetting things, trouble with confusion. She would make little mistakes,” Miller said. “And then that began to escalate.”
Robin began complaining about problems at work, which Miller attributed to having a new supervisor. She told Robin she had to try harder. When Robin had a series of falls, the staff at her program claimed she was merely doing it for attention, not realizing that gait issues are often the first sign of Alzheimer’s. And when she became overly emotional, it was chalked up to menopause or a disagreement with her friend.
“Everything was easily explained away, misunderstood and then blamed on her,” Miller said.
One night, Robin took everything out of her freezer and put it her sock drawer. Despite living in housing for individuals with developmental disabilities, the staff had no idea how to deal with her emerging dementia.
Then, two years ago, Robin’s condition began to deteriorate rapidly. She became terrified of the dark and would have psychotic breaks. She stopped walking or feeding herself. Miller brought her home in December 2013 fully prepared it would be her sister’s last Christmas.
But somehow, close to her family, in a environment where she felt safe and loved, her condition improved.
“She got happier,” Miller said. “She just wanted to be with me.”
Even as recently as a decade ago, learning about dementia in someone with a developmental disability was a daunting task. Miller reached out to Down syndrome and Alzheimer’s advocacy groups with little success. She tracked down a friend whose son with Down syndrome had died of Alzheimer’s. She met with her three weeks in a row, sitting on the woman’s porch absorbing all of her hard-gained experience.
“You have to tell me everything from the first sign to everything that happened at the end,” she recalls telling her.
“I don’t want to tell you about the end,” her friend replied. “I don’t want to scare you.”
It’s information they haven’t been able to get until recently from national Down syndrome advocacy groups. These groups got their start in helping families dealing with the first diagnosis of Down syndrome and so not surprisingly have focused primarily on issues of early intervention and inclusion.
“I think it’s been slow to come to the table from a national standpoint because that’s a negative thing,” said Dr. Seth Keller, a neurologist from Cherry Hill, New Jersey. “You’re talking to these young parents with children with Down syndrome, do you really want to tell them that when their children get to be 40, 50 or 60, they’re going to get Alzheimer’s and die?”
So until recently, there was little guidance from these groups on the realities of aging with Down syndrome.
“I believe there are families that have their heads in the sand, who don’t want to know what’s going on,” Miller said. “To me, it’s scary not knowing.”
There’s a similar disconnect among the medical professionals. While physicians who specialize in Down syndrome may have a greater understanding of the link with Alzheimer’s, primary care physicians or specialists who see such individuals less frequently aren’t always aware of the connection. “Doctors and nurses who care for people with developmental disabilities don’t know what normative aging is,” Keller said. {%pl-3377632%}
When Robin developed bladder issues and required a catheter, for example, her doctor told Miller she would have to have the catheter changed under general anesthesia every month.
“To me, that’s unacceptable. My question is always, ‘Would you do that to me?’” Miller said. “I found another urologist who changed her catheter using kindness instead.”
To help improve care for individuals with intellectual disabilities and dementia, Keller, Janicki and others involved with the American Academy of Developmental Medicine and Dentistry formed the National Task Group on Intellectual Disabilities and Dementia Practices. The group has developed guidelines for care and has served as a voice at the table, ensuring the medical establishment considers the unique needs of the disabled population when putting policies and actions plans in place. Most recently, they advocated for greater consideration within the National Alzheimer’s Plan for individuals with all sorts of intellectual disabilities.
Such efforts are starting to have an impact. Down syndrome and Alzheimer’s organizations are starting to collaborate and share information with families about aging and dementia. A recent restructuring within the federal Department of Health and Human Services created the Administration on Community Living, bridging the Administration on Aging and the Administration on Intellectual and Developmental Disabilities.
Keller has also been working with Special Olympics to increase the visibility of aging issues among its athletes. The group has long had a program called Healthy Athletes, in which they screen participants for medical issues. But in some states, officials have noticed the rise of dementia in its older athletes and are now working to integrate screening and referral for potential Alzheimer’s cases as well.
“For people with intellectual disabilities, I don’t think we have a true blueprint of what aging looks like,” said Jim Balamaci, president and CEO of Special Olympics Alaska. “So we want to help put that blueprint together by working with the provider agencies, the hospital and the school of nursing to come up with a solution that might beneficial.”
Recognizing those subtle, early changes can be challenging in real time and often emerge only with the clarity of hindsight. Mary Hogan, family coordinator for the National Task Group, said she missed many of the clues in her brother, Bill Hogan, who died of Alzheimer’s in 2010 at the age of 49.
“We would give lip service to the idea that people with Down syndrome will develop Alzheimer’s, but we really didn’t do our homework, and we didn’t really understand the disease itself,” Hogan said. “We didn’t understand the progression of the disease.”
Bill had been methodical with his calendar all of his life, dutifully recording whether each day was a good day or a bad day, coloring in the days and marking them with his intricate system of symbols.
“When he lost interest in that kind of activity, that should have been an immediate alarm for us,” she said. “That’s a really profound change, and we didn’t connect that with where we were heading.”
Over time, the subtle changes seemed to come more frequently and the losses became more noticeable. Bill’s last 15 months, she said, were ones of rapid decline. There’s some debate over whether Alzheimer’s moves at a quicker pace in Down syndrome or whether it just seems that way because the initial signs are so often masked by their cognitive deficits.
Hogan said keeping track of the changes is particularly difficult when individuals live in group homes, which can have frequent turnover in staff. There’s often no one there with the historical knowledge of an individual’s habits and tendencies to pick up on significant differences in behavior.{%pr-3417343%}
Tracking change
Evelyn Fella was moving her sister, Irma Fella, into a new care home in 2001 when she heard for the first time a social worker tell the new caregivers Irma had signs of dementia.
“Who decided that? Why would they say something like that?” she recalls thinking at the time. “But I’m going to say they were right.”
Irma was born in Detroit in 1945. After three sons, her mother was ecstatic to finally have a baby girl to take home. She was so excited, doctors couldn’t bring themselves to tell her the baby girl had Down syndrome.
Within two months, however, she knew something was wrong. Irma wasn’t developing the same way her brothers had. Doctors broke the news and told her to put Irma in an institution.
“My mother went to visit one and it was horrible, just a horrible experience,” Fella said. “So my sister just continued to be part of the family, and my mother’s expectations weren’t any less than for any of her other children.”
In the early 1950s, her mother saw an ad in the newspaper from a mother looking to find other families of children with disabilities. The parents got together and created a program for their children, renting space from the parks and recreation department. It was just one of the groups being formed around the country by parents whose children were denied access to public school. Eventually some of these parent groups joined forces in the National Association for Retarded Children, which now operates throughout the country under the acronym ARC.
The program served as a nursery school for Evelyn as well, who was four years younger than Irma. The public school system had no programs available for children with intellectual disabilities, but at age 16, Irma attended a live-in school run by Catholic nuns who taught individuals with disabilities academic and life skills. At age 26, she came back home and lived with her mother until 1992. After their mother’s death, Evelyn brought Irma to San Diego and helped her choose a group home.
Although she couldn’t read, Irma always insisted she had to have a subscription to TV Guide. She would bury her head in it, perusing the listings with great concentration. Her siblings would often call her out on it: “Oh Irmy, you can’t read.” But when they tested her, asking her to find a given word on the page, she would locate it. Irma had a talent for matching, and having seen and heard the words on the TV screen, she had begun to recognize the show titles, days, times and channels. All her life, she loved word search puzzles, and puzzle books were a standard birthday gift. She would dutifully find and circle every word in book after book. But after Irma turned 60, Evelyn discovered one day she could no longer find the hidden words. She had taken to merely circling every letter.
There were other clues of her slow decline. One year for Christmas, Irma’s brother had bought sketchbooks for everyone in the family, asking them to do a doodle each day and then return the books to him the following Christmas.
“And the only person who did it was my sister,” Evelyn said.
But her brother was so pleased, the sketchbook became an annual gift. Irma would draw what she saw freehand, filling page after page, before exchanging the full book for a fresh one the following holidays.
With time, she could no longer draw, so Evelyn transitioned her to coloring books. She impressed the others at her day program with how well she could color within the lines. That skill soon faded as well, and she took to drawing first circles and then only straight lines.
Evelyn realized her sister was backtracking through normal childhood development. While infants progress from straight lines to circles, to coloring, to freehand drawing, Irma was doing just the opposite. She was slowly but steadily regressing.{%pl-3421752%}
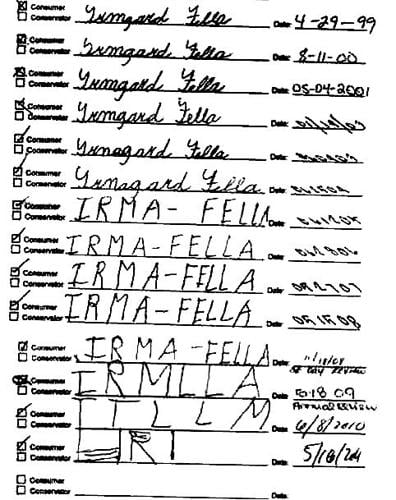
In 2011, Evelyn happened upon an even more stark demonstration of her sister’s decline. Each year, they would meet with the staff at the local day program, and Irma would sign her name at the bottom of her paperwork. At one of her last meetings, Evelyn glanced at the years of documents in her sister’s file dating back to 1999. Then she noticed something remarkable. As she lined up the papers up, she could see the visual representation of how Alzheimer’s disease was affecting Irma. The signatures had gone from a tight, neat cursive of her full name, Irmagard Fella, to increasingly more chaotic block printing of her shortened name. After 12 years, she could barely get a few letters down on the line.
Evelyn took a copy of the signatory timeline and shared it with Down syndrome researchers at the University of California, San Diego. After a news report including a photo of the signatures, the image went viral garnering tens of thousands of hits and hundreds of pointed comments.
“What was pushing everybody’s buttons,” Evelyn said, “was the realization of ‘Look what’s happening to us all.’”
The image had been circulating without the accompanying article and most of those responding online didn’t know that Irma had Down syndrome. Evelyn realized that, for a brief moment, Irma was being treated just like anybody else’s sister, mother or grandmother with Alzheimer’s disease. “Finally,” she thought to herself, “she is equal.”
New hopes
In fact, the fates of those with Alzheimer’s, whether due to Down syndrome or normal aging, are becoming increasingly intertwined. Researchers have found many treatments for Alzheimer’s disease that work well in mice but have been hard to translate into humans, says Dr. Bill Mobley, chair of neuroscience at the University of California, San Diego.
“One of the reasons we think that is, is that we haven’t been able to start early enough,” he said. “By the time people have clinical symptoms they’ve had the disease probably 20 years. We need to get to them earlier. And the people with Down syndrome offer that opportunity.”
In the general population, about 17 percent of women who reach age 65 and about 9 percent of men will develop Alzheimer’s disease. That means studies testing preventive treatments would have to enroll many more individuals to get the numbers of Alzheimer’s cases needed to see a meaningful effect. Among those with Down syndrome, the lifetime risk is higher than 50 percent, so researchers would need to enroll fewer overall participants to get the same number of people who ultimately develop Alzheimer’s.
Mobley recalls a discussion at a research conference eight years ago over the need for a cheap, reliable diagnostic test that would identify much earlier in life the patients destined to develop Alzheimer’s.
“If those are the criteria, the answer is Down syndrome,” Mobley recalls saying. “I can make the diagnosis even in utero. The test I use is my eyesight and my brain, and I know 50 years before the onset of dementia that this person is going to get dementia with a very high probability.”
At the time, nobody seemed to get it. But that has changed now, Mobley said.
“I think the reason why is that they now understand it may be absolutely necessary to prevent Alzheimer’s disease if we want to treat it,” he said. “So then the genetically predisposed populations become the ones you want to test, because you can make the diagnosis (so much earlier).”
Previously, much of Alzheimer’s research had focused on families with a genetic defect that causes early onset Alzheimer’s. Affected family members have a 50-50 chance of passing that defect on to their children. But while scores of those families have been identified around the world, there are many more individuals with Down syndrome.
“There’s not even any comparison,” Mobley said. “In the U.S., there are 200,000 Down syndrome people. There aren’t 200,000 people in all of those (familial Alzheimer’s disease families) in this universe.”
Including individuals with cognitive deficits in research studies can be challenging, because of concerns that they may not truly understand the risks involved. Researchers have been collaborating on standards for how to best explain the process and to make sure they understand they don’t have to participate. {%pr-3377548%}
Justine Dyer, a 27-year old with Down syndrome from Maine, was a participant in a recent clinical trial for an experimental drug to improve memory.
Dyer said she wanted to be in the study “to help my brain” and to help others.
“Her grandmother died of Alzheimer’s,” her mother, Betsy Dyer, said. “So we as a family are very anxious to participate in this kind of a study.”
Dyer said the researchers did a wonderful job explaining the study to Justine, using pictures to help her understand.
“The bottom line is she trusts me, and she believes that I wouldn’t ask her to do something that isn’t safe,” she said. “We definitely went through the risks.”
Justine said the researchers were “really nice,” and called Dr. Brian Skotko, the co-director of the Mass General Down Syndrome Program and one of the principal investigators of the study, “awesome.”
Skotko was also a researcher in a clinical trial conducted by Transitions Therapeutics for the drug ELND005. The compound is believed to play a role in preventing the build-up of amyloid beta in the brain. The drug is being tested both for its ability to improve cognitive function in individuals with Down syndrome and as a treatment for Alzheimer’s disease.
The Phase II study was primarily aimed at testing the safety of the drugs in young adults with Down syndrome, and the 23 test subjects reported no serious problems. Skotko said there was also a statistically significant change in patient- and caregiver-reported symptoms among those on the medication, compared to placebo. The company is now planning a Phase III trial to test the drugs in a larger group of patients.
{%qc-If we succeed in preventing or curing Alzheimer’s disease first in Down syndrome, then bully for those individuals as well as for us. I think that’s what’s pushing the public to pay attention to it. The reality is they’ve had this wonderful value as human beings all along.%em Dr. Bill Mobley, University of California, San Diego%}
“For me, it’s a human-rights issue,” Skotko said. “You and I could sign up if we wanted to for clinical drug trials and now individuals with Down syndrome, with the guidance of their trustees or caregivers, can sign up in they want to. And I think it’s an exciting time for them.”
There is also concern over whether individuals with Down syndrome are now being viewed as “guinea pigs,” exposing them to the risks involved in clinical trials in order to benefit healthy individuals who might develop late-onset Alzheimer’s.
Many of the family members of individuals with Down syndrome don’t see it that way.
“It’s about improving the quality of life of people with Down syndrome,” Hogan said. “If you know the pathology is going to be there, isn’t it in their best interest to try to find something that would slow down the progression for them as well as for the general population?”
It would be an ironic turn of events for a group of individuals known more their infectious happy personalities than their contributions to science.
“If we succeed in preventing or curing Alzheimer’s disease first in Down syndrome, then bully for those individuals as well as for us,” Mobley said. “I think that’s what’s pushing the public to pay attention to it. The reality is they’ve had this wonderful value as human beings all along.” •
Editor’s note: This article has been corrected. The original version misstated the name of the Linda Crnic Institute for Down Syndrome. Also, Jennifer Dyer was a participant in a clinical trial for a drug to improve memory. The original version of this story misstated the trial in which she was involved.













(0) comments
Welcome to the discussion.
Log In
Keep it Clean. Please avoid obscene, vulgar, lewd, racist or sexually-oriented language.
PLEASE TURN OFF YOUR CAPS LOCK.
Don't Threaten. Threats of harming another person will not be tolerated.
Be Truthful. Don't knowingly lie about anyone or anything.
Be Nice. No racism, sexism or any sort of -ism that is degrading to another person.
Be Proactive. Use the 'Report' link on each comment to let us know of abusive posts.
Share with Us. We'd love to hear eyewitness accounts, the history behind an article.