Thursday, May 30, 2024
As an organization accredited by the ACCME, Medscape, LLC, requires everyone who is in a position to control the content of an education activity to disclose all relevant financial relationships with any commercial interest. The ACCME defines "relevant financial relationships" as financial relationships in any amount, occurring within the past 12 months, including financial relationships of a spouse or life partner, that could create a conflict of interest.
Medscape, LLC, encourages Authors to identify investigational products or off-label uses of products regulated by the US Food and Drug Administration, at first mention and where appropriate in the content.

Professor of Medicine, Duke University School of Medicine; Co-Director, Solid Tumor Therapeutics Program, Duke Cancer Institute, Durham, North Carolina

Assistant Professor, Department of Clinical Pharmacy and Outcomes Sciences, South Carolina College of Pharmacy, Columbia, South Carolina
This activity is intended for hematologists, oncologists, pathologists, pharmacists, and medical geneticists.
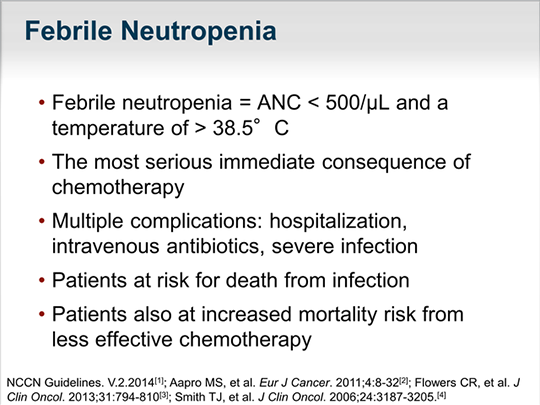
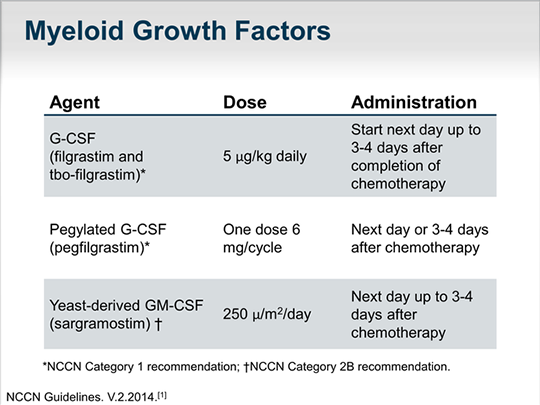
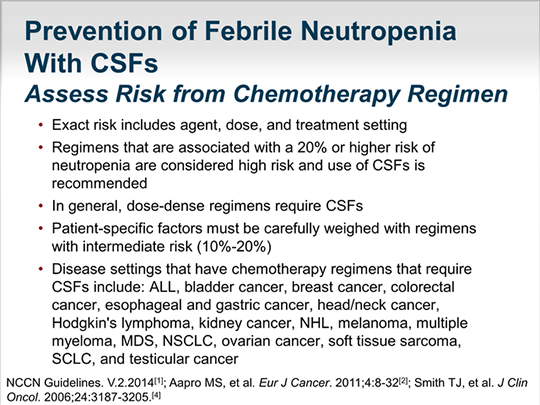
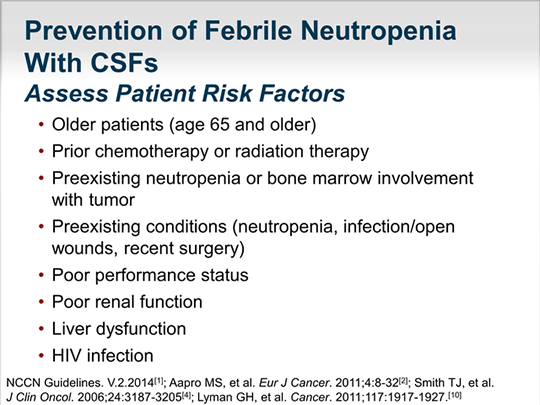
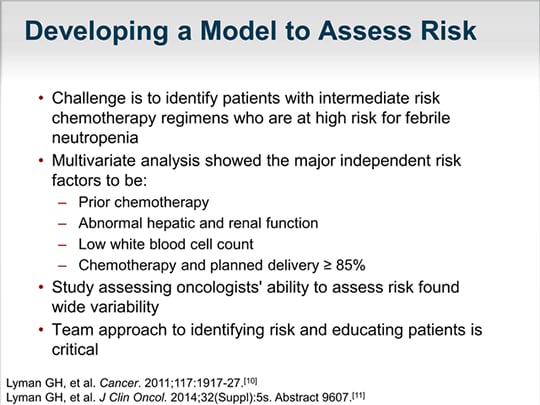
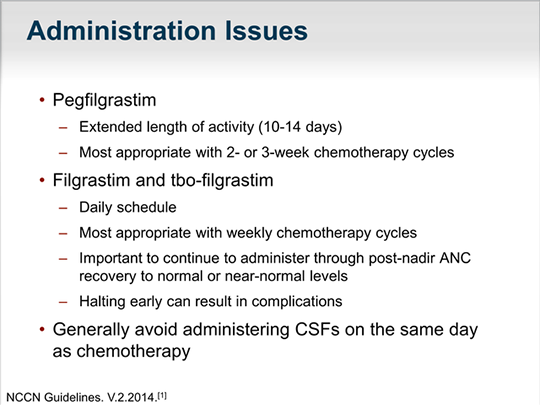
The goal of this activity is to discuss the optimal use of myeloid growth factors in the prevention of chemotherapy-induced neutropenia.
Upon completion of this activity, participants will be able to:
As an organization accredited by the ACCME, Medscape, LLC, requires everyone who is in a position to control the content of an education activity to disclose all relevant financial relationships with any commercial interest. The ACCME defines "relevant financial relationships" as financial relationships in any amount, occurring within the past 12 months, including financial relationships of a spouse or life partner, that could create a conflict of interest.
Medscape, LLC, encourages Authors to identify investigational products or off-label uses of products regulated by the US Food and Drug Administration, at first mention and where appropriate in the content.
Professor of Medicine, Duke University School of Medicine; Co-Director, Solid Tumor Therapeutics Program, Duke Cancer Institute, Durham, North Carolina
Assistant Professor, Department of Clinical Pharmacy and Outcomes Sciences, South Carolina College of Pharmacy, Columbia, South Carolina
Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
Medscape, LLC designates this enduring material for a maximum of 0.50
AMA PRA Category 1 Credit(s)™
. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Medscape, LLC staff have disclosed that they have no relevant financial relationships.
Medscape, LLC is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
Medscape, LLC designates this continuing education activity for 0.50 contact hour(s) (0.05 CEUs) (Universal Activity Number 0461-0000-14-045-H01-P).
For questions regarding the content of this activity, contact the accredited provider for this CME/CE activity noted above. For technical assistance, contact [email protected]
There are no fees for participating in or receiving credit for this online educational activity. For information on applicability
and acceptance of continuing education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those
credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the
activity online during the valid credit period that is noted on the title page. To receive AMA PRA Category 1 Credit™, you must receive a minimum score of 70% on the post-test.
Follow these steps to earn CME/CE credit*:
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannot alter it.
Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time period you can print
out the tally as well as the certificates from the CME/CE Tracker.
*The credit that you receive is based on your user profile.
CME/CE Released: 7/31/2014
Valid for credit through: 7/31/2015, 11:59 PM EST
processing....

This transcript has been edited for style and clarity.
