
The Efficacy of Expiratory Muscle Training during Inspiratory Load in Healthy Adult Males: A Randomized Controlled Trial

Abstract
:1. Introduction
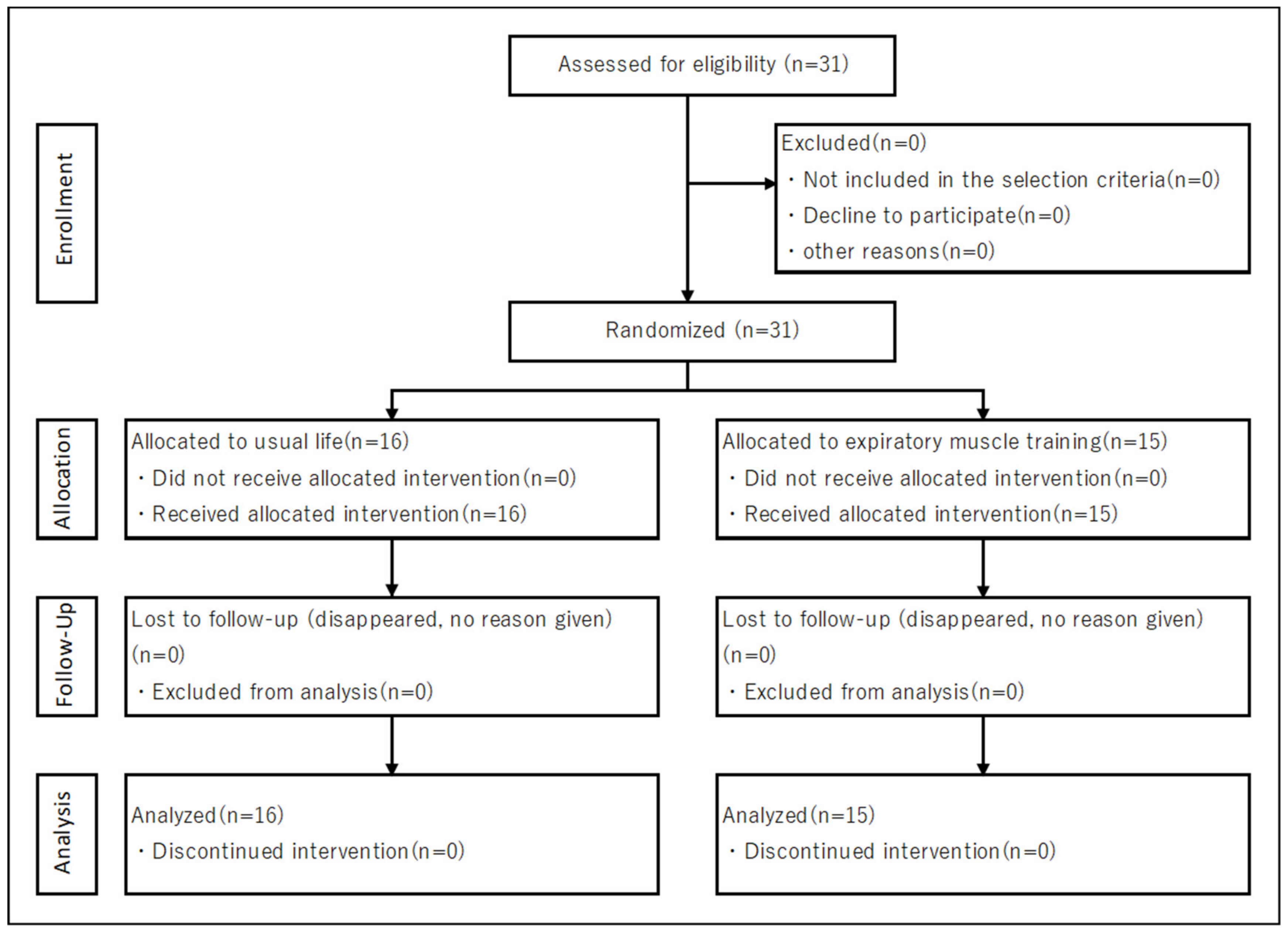
2. Methods
2.1. Subjects
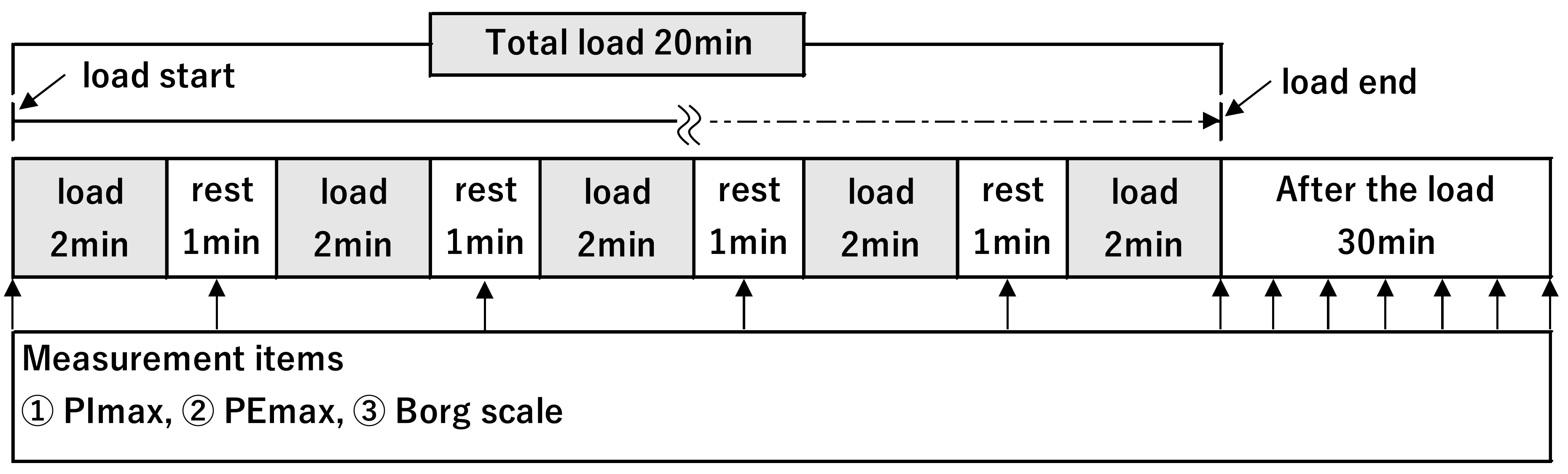
2.2. Research Protocol and EMT
2.3. Measurement Items
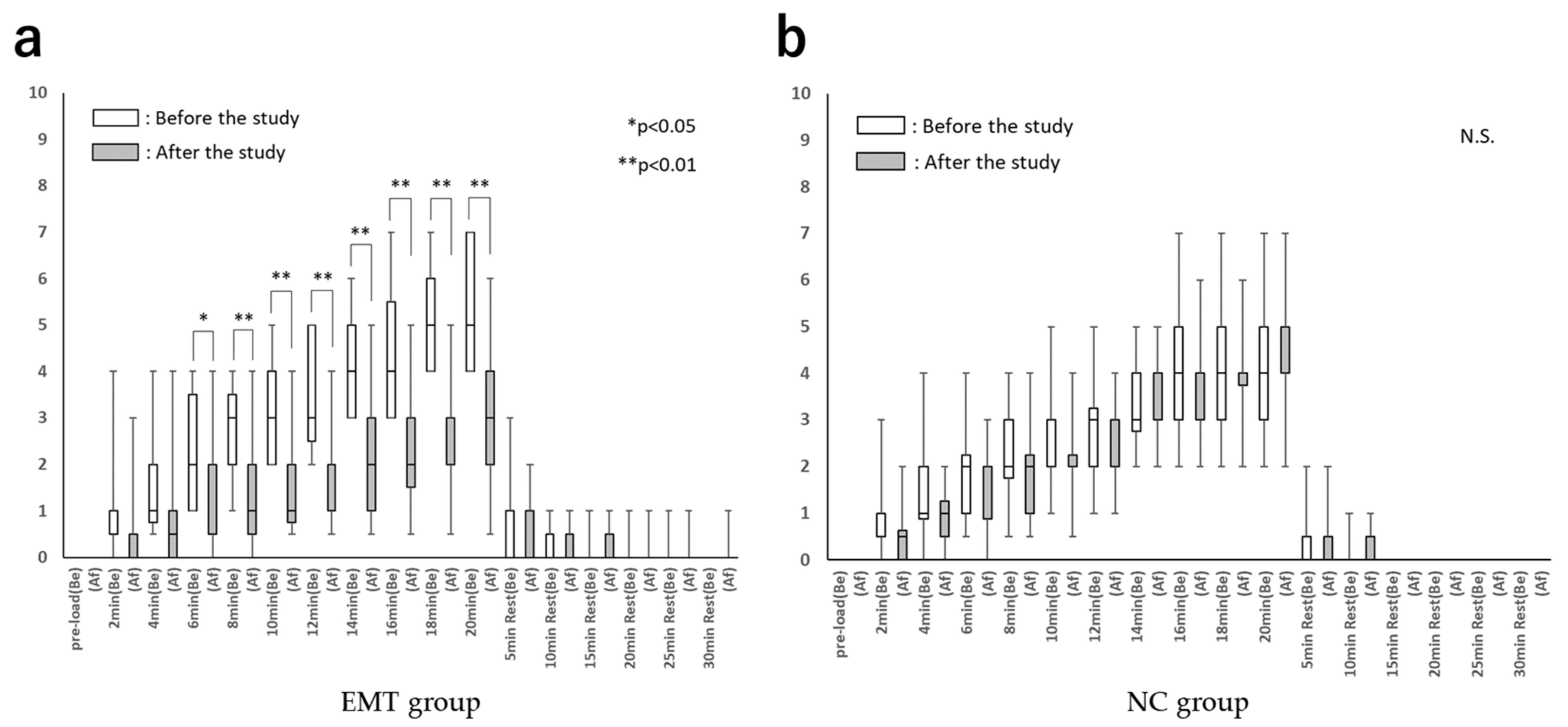
2.3.1. Respiratory Muscle Fatigue
2.3.2. Respiratory Distress
2.3.3. Respiratory Functions
2.4. Sample Size
2.5. Statistical Analysis
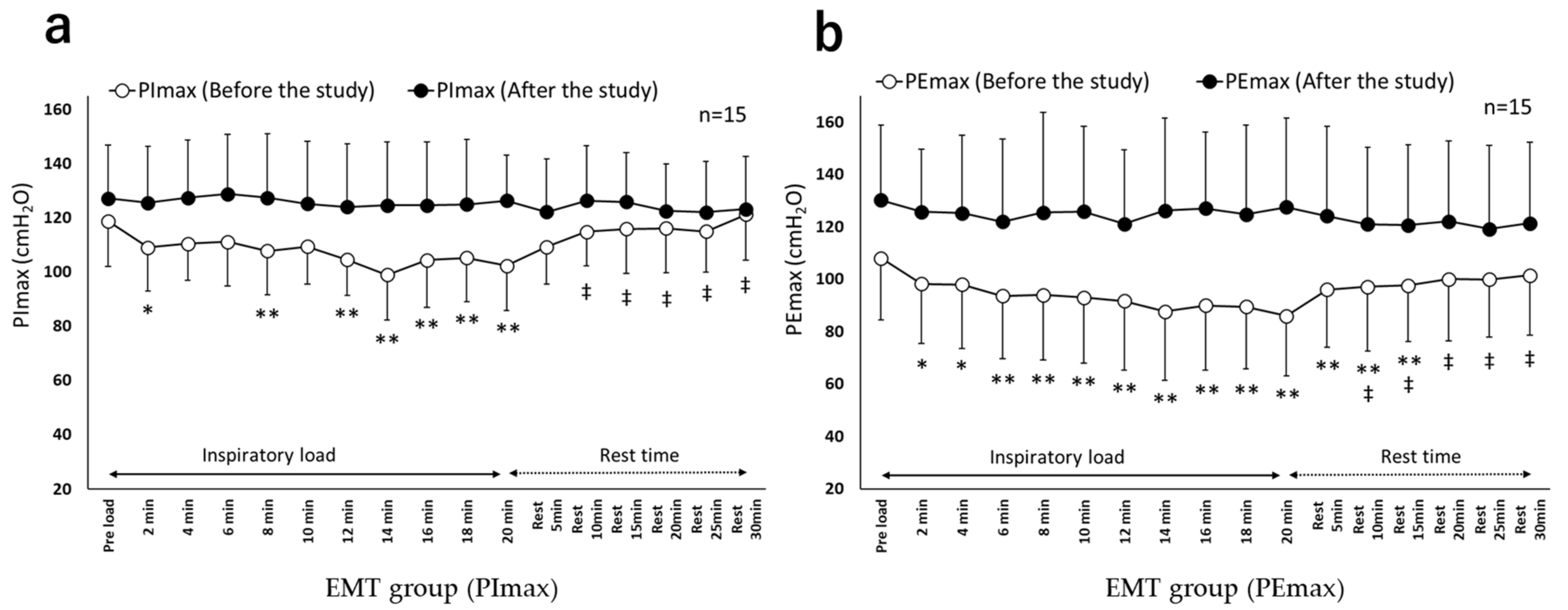
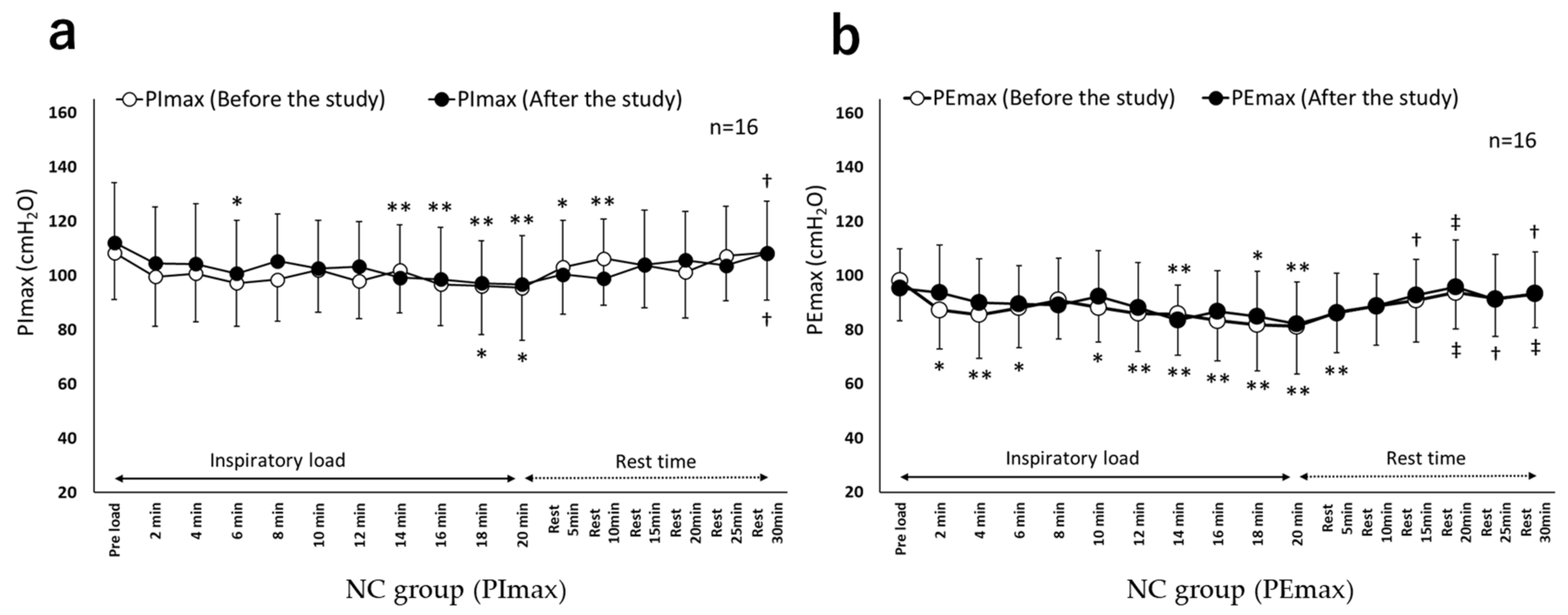
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gosselink, R.; Troosters, T.; Decramer, M. Distribution of Muscle Weakness in Patients with Stable Chronic Obstructive Pulmonary Disease. J. Cardiopulm. Rehabil. 2000, 20, 353–360. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; Bertley, J.C.; Chau, L.K.; Webb, K.A. Qualitative aspects of exertional breathlessness in chronic airflow limitation: Pathophysiologic mechanisms. Am. J. Respir. Crit. Care Med. 1997, 155, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Gosselink, R.; Vos, J.D.; Heuvel, S.P.; Segers, J.; Decramer, M.; Kwakkel, G. Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur. Respir. J. 2011, 37, 416–425. [Google Scholar] [CrossRef] [PubMed]
- McSweeny, A.J.; Grant, I.; Heaton, R.K.; Adams, K.M.; Timms, R.M. Life Quality of Patients with Chronic Obstructive Pulmonary Disease. Arch. Intern. Med. 1982, 142, 473–478. [Google Scholar] [CrossRef]
- Borge, C.R.; Hagen, K.B.; Mengshoel, A.M.; Omenaas, E.; Moum, T.; Wahl, A.K. Effects of controlled breathing exercises and respiratory muscle training in people with chronic obstructive pulmonary disease: Results from evaluating the quality of evi-dence in systematic reviews. BMC Pulm. Med. 2014, 14, 184. [Google Scholar] [CrossRef]
- Weiner, P.; Magadle, R.; Beckerman, M.; Weiner, M.; Berar-Yanay, N. Comparison of Specific Expiratory, Inspiratory, and Combined Muscle Training Programs in COPD. Chest 2003, 124, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Hodgev, V.A.; Kostianev, S.S. Maximal inspiratory pressure predicts mortality in patients with chronic obstructive pulmonary disease in a five-year fllow-up. Folia Med. 2006, 48, 36–41. [Google Scholar]
- Puhan, M.A.; Gimeno-Santos, E.; Scharplatz, M.; Troosters, T.; Walters, E.H.; Steurer, J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2011, 5, CD005305. [Google Scholar]
- Geddes, E.L.; O’Brien, K.; Reid, W.D.; Brooks, D.; Crowe, J. Inspiratory muscle training in adults with chronic obstructive pulmonary disease: An update of a systematic review. Respir. Med. 2008, 102, 1715–1729. [Google Scholar] [CrossRef] [Green Version]
- Crowe, J.; Reid, W.D.; Geddes, E.L.; O’Brien, K.; Brooks, D. Inspiratory muscle training compared with other rehabilitation interventions in adults with chronic obstructive pulmonary disease: A systematic literature review and meta-analysis. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 319–329. [Google Scholar] [CrossRef]
- Martin, J.; Aubier, M.; Engel, L. Effects of inspiratory loading on respiratory muscle activity during expiration. Am. Rev. Respir. Dis. 1982, 125, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, T.; Maruyama, H.; Kato, M.; Uchida, M.; Kubo, A. Characteristics of respiratory muscle fatigue upon inhalation resistance with a maximal inspiratory mouth pressure of 50%. J. Phys. Ther. Sci. 2019, 31, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crisafulli, E.; Costi, S.; Fabbri, L.M.; Clini, E.M. Respiratory muscles training in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2007, 2, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, S.; Güell, R.; Barreiro, E.; Solanes, I.; Ramírez-Sarmiento, A.; Orozco-Levi, M.; Casan, P.; Gea, J.; Sanchis, J. Clinical outcomes of expiratory muscle training in severe COPD patients. Respir. Med. 2007, 101, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ninane, V.; Rypens, F.; Yernault, J.C.; Troyer, A.D. Abdominal muscle use during breathing in patients with chronic air-flow obstruction. Am. Rev. Respir. Dis. 1992, 146, 16–21. [Google Scholar] [CrossRef]
- Mesquita, R.; Donaria, L.; Genz, I.C.H.; Pitta, F.; Probst, V.S. Respiratory muscle strength during and after hospitaliza-tion for COPD exacerbation. Respir. Care 2013, 58, 2142–2149. [Google Scholar] [CrossRef] [Green Version]
- Neves, L.F.; Reis, M.H.; Plentz, R.; Matte, D.L.; Coronel, C.C.; Sbruzzi, G. Expiratory and Expiratory Plus Inspiratory Muscle Training Improves Respiratory Muscle Strength in Subjects With COPD: Systematic Review. Respir. Care 2014, 59, 1381–1388. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- NHLBI Workshop. Respiratory muscle fatigue. Report of the Respiratory Muscle Fatigue Workshop Group. Am. Rev. Respir. Dis. 1990, 142, 474–480. [Google Scholar] [CrossRef]
- American Thoracic Society. Standardization of Spirometry, 1994 Update. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [Google Scholar] [CrossRef]
- Suzuki, S.; Sato, M.; Okubo, T. Expiratory muscle training and sensation of respiratory effort during exercise in normal subjects. Thorax 1995, 50, 366–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, S.; Suzuki, J.; Ishii, T.; Akahori, T.; Okubo, T. Relationship of Respiratory Effort Sensation to Expiratory Muscle Fatigue during Expiratory Threshold Loading. Am. Rev. Respir. Dis. 1992, 145, 461–466. [Google Scholar] [CrossRef]
- Black, L.F.; Hyatt, R.E. Maximal respiratory pressures: Normal values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; European Respiratory Society. ATS/ERS statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Hershenson, M.B.; Kikuchi, Y.; Loring, S.H. Relative strengths of the chest wall muscles. J. Appl. Physiol. 1988, 65, 852–862. [Google Scholar] [CrossRef]
- Kojima, H.; Yamada, T.; Takeda, M.; Itou, Y.; Yoshida, M.; Kimura, M. Effectiveness of Cough Exercise and Expiratory Muscle Training: A Meta-analysis. J. Phys. Ther. Sci. 2006, 18, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Freitas, F.S.; Ibiapina, C.C.; Alvim, C.G.; Britto, R.R.; Parreira, V.F. Relationship between cough strength and functional level in elderly. Rev. Bras. Fisioter. 2010, 14, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Morrow, B.M.; Angelil, L.; Forsyth, J.; Huisamen, A.; Juries, E.; Corten, L. The utility of using peak expiratory flow and forced vital capacity to predict poor expiratory cough flow in children with neuromuscular disorders. S. Afr. J. Physiother. 2019, 75, 8. [Google Scholar] [CrossRef]
- Ramirez-Sarmiento, A.; Orozco-Levi, M.; Guell, R.; Barreiro, E.; Hernandez, N.; Mota, S.; Sangenis, M.; Broquetas, J.M.; Casan, P.; Gea, J. Inspiratory muscle training in patients with chronic obstructive pulmonary disease structural adaptation and physiologic outcomes. Am. J. Respir. Crit. Care Med. 2002, 166, 1491–1497. [Google Scholar] [CrossRef]
- Killian, K.J.; Gandevia, S.; Summers, E.; Campbell, E.J. Effect of increased lung volume on perception of breathlessness, effort, and tension. J. Appl. Physiol. 1984, 57, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Campbell, E.J.; Gandevia, S.; Killian, K.J.; Mahutte, C.K.; Rigg, J.R. Changes in the perception of inspiratory resistive loads during partial curarization. J. Physiol. 1980, 309, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandevia, S.; Killian, K.J.; Campbell, E.J.M. The Effect of Respiratory Muscle Fatigue on Respiratory Sensations. Clin. Sci. 1981, 60, 463–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EMT n = 15 | NC n = 16 | |||
|---|---|---|---|---|
| Before the Study | After the Study | Before the Study | After the Study | |
| Male sex, n (%) | 15 (100) | - | 16 (100) | - |
| Age, years | 27.3 ± 2.4 | - | 26.7 ± 5.1 | - |
| Height, cm | 173.2 ± 5.0 | - | 170.5 ± 5.4 | - |
| Body weight, kg | 64.8 ± 7.4 | 64.5 ± 7.3 | 67.0 ± 7.0 | 66.6 ± 6.9 |
| Body mass index, kg/m2 | 21.5 ± 1.5 | 21.5 ± 1.8 | 23.1 ± 2.1 | 22.9 ± 2.1 |
| Respiratory function | ||||
| FVC, L | 4.5 ± 0.5 | 4.6 ± 0.6 | 4.4 ± 0.4 | 4.4 ± 0.4 |
| %FVC, % | 106.3 ± 10.7 | 107.3 ± 11.6 | 104.5 ± 9.8 | 104.6 ± 10.3 |
| FEV1.0, L | 4.0 ± 0.4 | 4.0 ± 0.4 | 3.8 ± 0.4 | 3.8 ± 0.4 |
| FEV1.0%, % | 88.2 ± 5.9 | 87.8 ± 6.2 | 87.1 ± 4.2 | 86.7 ± 3.7 |
| PEF, L/s | 9.5 ± 1.1 | 10.2 ± 1.1 * | 9.8 ± 1.1 | 9.6 ± 0.9 |
| Respiratory muscle strength | ||||
| PImax, cmH2O | 118.8 ± 16.8 | 127.1 ± 19.7 | 108.4 ± 17.3 | 112.1 ± 22.1 |
| PEmax, cmH2O | 108.0 ± 23.7 | 130.1 ± 28.6 ** | 98.1 ± 14.8 | 95.3 ± 14.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukamoto, T.; Kato, M.; Kurita, Y.; Uchida, M.; Kubo, A.; Maruyama, H. The Efficacy of Expiratory Muscle Training during Inspiratory Load in Healthy Adult Males: A Randomized Controlled Trial. Healthcare 2022, 10, 933. https://doi.org/10.3390/healthcare10050933
Tsukamoto T, Kato M, Kurita Y, Uchida M, Kubo A, Maruyama H. The Efficacy of Expiratory Muscle Training during Inspiratory Load in Healthy Adult Males: A Randomized Controlled Trial. Healthcare. 2022; 10(5):933. https://doi.org/10.3390/healthcare10050933
Chicago/Turabian StyleTsukamoto, Toshiya, Michitaka Kato, Yasunari Kurita, Masaki Uchida, Akira Kubo, and Hitoshi Maruyama. 2022. "The Efficacy of Expiratory Muscle Training during Inspiratory Load in Healthy Adult Males: A Randomized Controlled Trial" Healthcare 10, no. 5: 933. https://doi.org/10.3390/healthcare10050933