
Apparent Lack of Benefit of Combining Repetitive Transcranial Magnetic Stimulation with Internet-Delivered Cognitive Behavior Therapy for the Treatment of Resistant Depression: Patient-Centered Randomized Controlled Pilot Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Institutional Review Board Approval
2.3. Inclusion and Exclusion Criteria
- A neurological disorder, including a history of seizures, cerebrovascular disease, primary or secondary tumors in the central nervous system, stroke, cerebral aneurysm, movement disorder, or any lifetime history of loss of consciousness due to head injury.
- Any current personality disorder that would interfere with participation in the study or might affect cognition and ability to participate meaningfully, as well as mental retardation identified through medical history or by the investigator.
- A current amnestic disorder, dementia, or delirium, as defined by a Montreal Cognitive Assessment score of ≤16, or any other neurological or mental disease that might affect cognition or the ability to participate in CBT meaningfully.
- Participation in any drug or device clinical trial in the six weeks (42 days) prior to the screening visit and/or participation in another clinical trial for the duration of the study.
- Participants who are pregnant/breastfeeding.
- Discovery and/or the sudden appearance of any condition or circumstance from the above list that, in the opinion of the investigator, has the potential to prevent study completion and/or to have a confounding effect on outcome assessments.
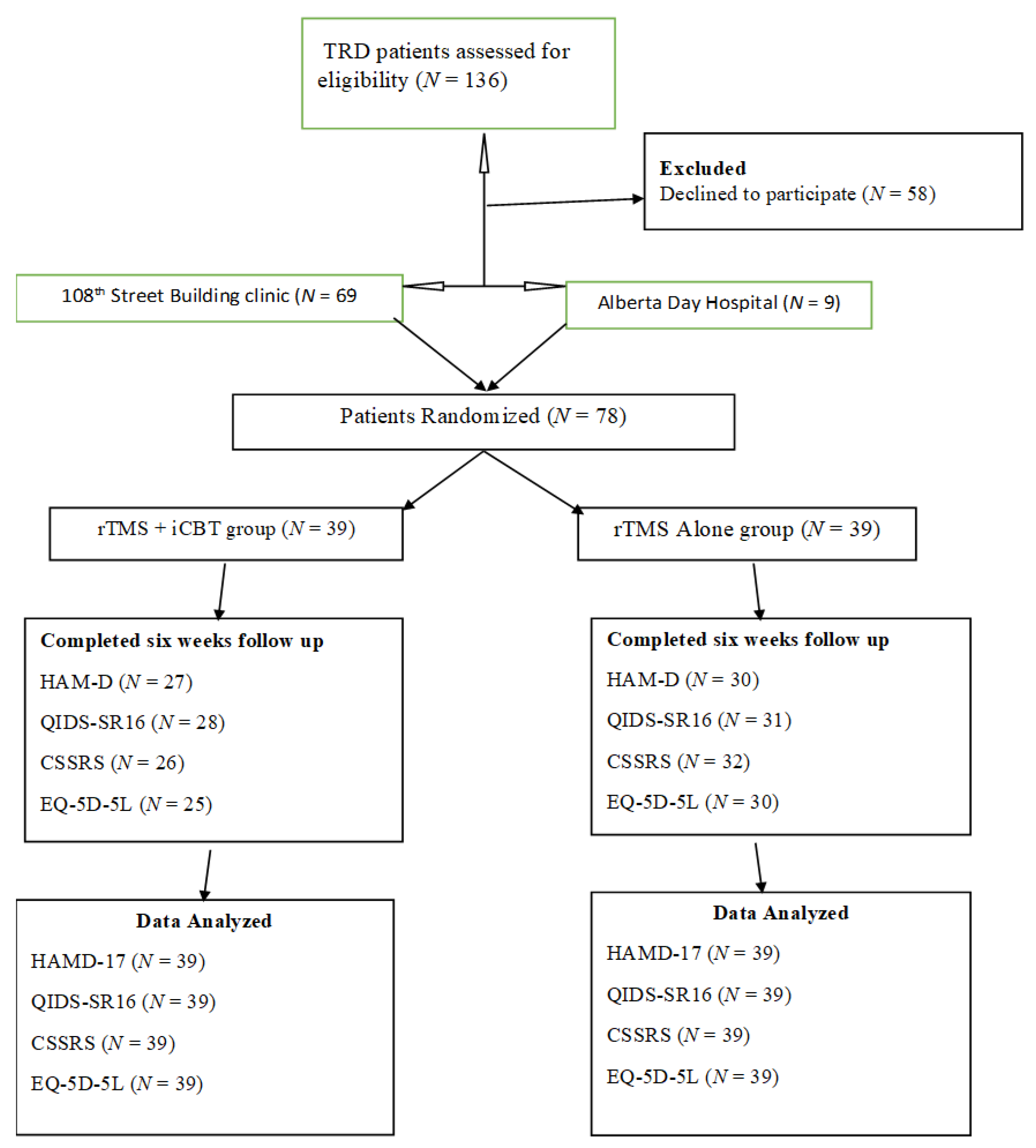
2.4. Recruitment Procedures
2.5. Randomization and Blinding
2.6. Intervention
2.7. Sample Size Calculation
2.8. Data Collection
2.9. Primary Outcome Measure
2.10. Secondary Outcome Measures
2.11. Exploratory Outcomes
2.12. Statistical Analysis
3. Results
3.1. Primary Outcome Measures
3.2. Secondary Outcome Measures
3.3. Exploratory Outcomes
4. Discussion
4.1. Principal Findings
4.2. Interpreting Findings against the Literature
4.3. Strengths of This Study
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR* D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Bourin, M. Developing Therapies for Treatment-Resistant Depressive Disorder in Animal Models. In Treatment Resistance in Psychiatry; Springer: Berlin/Heidelberg, Germany, 2019; pp. 79–86. [Google Scholar]
- Ventriglio, A.; Bhugra, D.; Sampogna, G.; Luciano, M.; De Berardis, D.; Sani, G.; Fiorillo, A. From dysthymia to treatment-resistant depression: Evolution of a psychopathological construct. Int. Rev. Psychiatry 2020, 32, 471–476. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, D.; Tomasetti, C.; Pompili, M.; Serafini, G.; Vellante, F.; Fornaro, M.; Valchera, A.; Perna, G.; Volpe, U.; Martinotti, G.; et al. An Update on Glutamatergic System in Suicidal Depression and on the Role of Esketamine. Curr. Top. Med. Chem. 2020, 20, 554–584. [Google Scholar] [CrossRef] [PubMed]
- Sackeim, H.A. The definition and meaning of treatment-resistant depression. J. Clin. Psychiatry 2001, 62, 10–17. [Google Scholar] [PubMed]
- Souery, D.; Papakostas, G.I.; Trivedi, M.H. Treatment-resistant depression. J. Clin. Psychiatry 2006, 67, 16. [Google Scholar]
- Berlim, M.T.; Turecki, G. What is the meaning of treatment resistant/refractory major depression (TRD)? A systematic review of current randomized trials. Eur. Neuropsychopharmacol. 2007, 17, 696–707. [Google Scholar] [CrossRef]
- Berlim, M.T.; Turecki, G. Definition, assessment, and staging of treatment—Resistant refractory major depression: A review of current concepts and methods. Can. J. Psychiatry 2007, 52, 46–54. [Google Scholar] [CrossRef]
- Gelenberg, A.J.; Freeman, M.P.; Markowitz, J.C.; Rosenbaum, J.F.; Thase, M.E.; Trivedi, M.H.; Van Rhoads, R.S. American Psychiatric Association practice guidelines for the treatment of patients with major depressive disorder. Am. J. Psychiatry 2010, 167 (Suppl. 10), 9–118. [Google Scholar]
- Gibson, T.B.; Jing, Y.; Carls, G.S.; Kim, E.; Bagalman, J.E.; Burton, W.N.; Tran, Q.-V.; Pikalov, A.; Goetzel, R.Z. Cost burden of treatment resistance in patients with depression. Am. J. Manag. Care 2010, 16, 370–377. [Google Scholar] [CrossRef]
- Olchanski, N.; Myers, M.M.; Halseth, M.; Cyr, P.L.; Bockstedt, L.; Goss, T.F.; Howland, R.H. The Economic Burden of Treatment-Resistant Depression. Clin. Ther. 2013, 35, 512–522. [Google Scholar] [CrossRef]
- Dunner, D.L.; Rush, A.J.; Russell, J.M.; Burke, M.; Woodard, S.; Wingard, P.; Allen, J. Prospective, Long-Term, Multicenter Study of the Naturalistic Outcomes of Patients with Treatment-Resistant Depression. J. Clin. Psychiatry 2006, 67, 688–695. [Google Scholar] [CrossRef]
- Hantouche, E.; Angst, J.; Azorin, J.-M. Explained factors of suicide attempts in major depression. J. Affect. Disord. 2010, 127, 305–308. [Google Scholar] [CrossRef]
- Bernal, M.; Haro, J.; Bernert, S.; Brugha, T.; de Graaf, R.; Bruffaerts, R.; Lépine, J.; de Girolamo, G.; Vilagut, G.; Gasquet, I.; et al. Risk factors for suicidality in Europe: Results from the ESEMED study. J. Affect. Disord. 2007, 101, 27–34. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Dilsaver, S.C. Lifetime rates of suicide attempts among subjects with bipolar and unipolar disorders relative to subjects with other axis I disorders. Biol. Psychiatry 1996, 39, 896–899. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Alonso, J.; Angermeyer, M.; Beautrais, A.; Bruffaerts, R.; Chiu, W.T.; de Girolamo, G.; Gluzman, S.; et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br. J. Psychiatry 2008, 192, 98–105. [Google Scholar] [CrossRef]
- Shelton, R.C.; Osuntokun, O.; Heinloth, A.N.; Corya, S.A. Therapeutic Options for Treatment-Resistant Depression. CNS Drugs 2010, 24, 131–161. [Google Scholar] [CrossRef]
- Nierenberg, A.A.; Katz, J.; Fava, M. A Critical Overview of the Pharmacologic Management of Treatment-Resistant Depression. Psychiatr. Clin. N. Am. 2007, 30, 13–29. [Google Scholar] [CrossRef]
- McPherson, S.; Cairns, P.; Carlyle, J.; Shapiro, D.A.; Richardson, P.; Taylor, D. The effectiveness of psychological treatments for treatment-resistant depression: A systematic review. Acta Psychiatr. Scand. 2005, 111, 331–340. [Google Scholar] [CrossRef]
- Schatzberg, A.F.; Demitrack, M.A.; O’Reardon, J.P.; Richelson, M.; Thase, M.E. Transcranial magnetic stimulation: Potential new treatment for resistant depression. J. Clin. Psychiatry 2007, 68, 315–330. [Google Scholar] [CrossRef]
- Lam, R.W.; Chan, P.; Wilkins-Ho, M.; Yatham, L.N. Repetitive Transcranial Magnetic Stimulation for Treatment-Resistant Depression: A Systematic Review and Metaanalysis. Can. J. Psychiatry 2008, 53, 621–631. [Google Scholar] [CrossRef]
- Hallett, M. Transcranial magnetic stimulation and the human brain. Nature 2000, 406, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Rossi, S. Transcranial magnetic stimulation: Diagnostic, therapeutic, and research potential. Neurology 2007, 68, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Nahas, Z.; Lomarev, M.; Roberts, D.R.; Shastri, A.; Lorberbaum, J.P.; Teneback, C.; McConnell, K.; Vincent, D.J.; Li, X.; George, M.S.; et al. Unilateral left prefrontal transcranial magnetic stimulation (TMS) produces intensity-dependent bilateral effects as measured by interleaved BOLD fMRI. Biol. Psychiatry 2001, 50, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Machado, S.; Arias-Carrion, O.; Paes, F.; Vieira, R.T.; Caixeta, L.; Novaes, F.; Marinho, T.; Almada, L.F.; Silva, A.C.; Nardi, A.E. Repetitive Transcranial Magnetic Stimulation for Clinical Applications in Neurological and Psychiatric Disorders: An Overview. Eurasian J. Med. 2013, 45, 191–206. [Google Scholar] [CrossRef]
- Grimm, S.; Beck, J.; Schuepbach, D.; Hell, D.; Boesiger, P.; Bermpohl, F.; Niehaus, L.; Boeker, H.; Northoff, G. Imbalance between Left and Right Dorsolateral Prefrontal Cortex in Major Depression Is Linked to Negative Emotional Judgment: An fMRI Study in Severe Major Depressive Disorder. Biol. Psychiatry 2008, 63, 369–376. [Google Scholar] [CrossRef]
- George, M.S.; Nahas, Z.; Molloy, M.; Speer, A.M.; Oliver, N.C.; Li, X.-B.; Arana, G.W.; Risch, S.C.; Ballenger, J.C. A controlled trial of daily left prefrontal cortex TMS for treating depression. Biol. Psychiatry 2000, 48, 962–970. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Andersson, G.; van Oppen, P. Psychotherapy for depression in adults: A meta-analysis of comparative outcome studies. J. Consult. Clin. Psychol. 2008, 76, 909–922. [Google Scholar] [CrossRef]
- Cavanagh, K. Geographic Inequity in the Availability of Cognitive Behavioural Therapy in England and Wales: A 10-Year Update. Behav. Cogn. Psychother. 2013, 42, 497–501. [Google Scholar] [CrossRef]
- Murray, E.; Khadjesari, Z.; White, I.; Kalaitzaki, E.; Godfrey, C.; McCambridge, J.; Thompson, S.G.; Wallace, P.; Riper, M.; Eapen, B.; et al. Methodological Challenges in Online Trials. J. Med. Internet Res. 2009, 11, e9. [Google Scholar] [CrossRef]
- Cross, M. How the internet is changing health care. BMJ 2008, 337, a883. [Google Scholar] [CrossRef]
- Spek, V.; Cuijpers, P.; Nyklícek, I.; Riper, H.; Keyzer, J.; Pop, V. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: A meta-analysis. Psychol. Med. 2006, 37, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Kiropoulos, L.A.; Klein, B.; Austin, D.W.; Gilson, K.; Pier, C.; Mitchell, J.; Ciechomski, L. Is internet-based CBT for panic disorder and agoraphobia as effective as face-to-face CBT? J. Anxiety Disord. 2008, 22, 1273–1284. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H. Review of randomised controlled trials of Internet interventions for mental disorders and related conditions. Clin. Psychol. 2006, 10, 16–29. [Google Scholar] [CrossRef]
- Cuijpers, P.; Riper, H.; Andersson, G. Internet-based treatment of depression. Curr. Opin. Psychol. 2015, 4, 131–135. [Google Scholar] [CrossRef]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Cipriani, A.; Furukawa, T.A. Effectiveness and acceptability of cognitive behavior therapy delivery formats in adults with depression: A network meta-analysis. JAMA Psychiatry 2019, 76, 700–707. [Google Scholar] [CrossRef]
- Clark, D.M. Implementing NICE guidelines for the psychological treatment of depression and anxiety disorders: The IAPT experience. Int. Rev. Psychiatry 2011, 23, 318–327. [Google Scholar] [CrossRef]
- Vlaescu, G.; Alasjö, A.; Miloff, A.; Carlbring, P.; Andersson, G. Features and functionality of the Iterapi platform for internet-based psychological treatment. Internet Interv. 2016, 6, 107–114. [Google Scholar] [CrossRef]
- Proudfoot, J.; Goldberg, D.; Mann, A.; Everitt, B.; Marks, I.; Gray, J.A. Computerized, interactive, multimedia cognitive-behavioural program for anxiety and depression in general practice. Psychol. Med. 2003, 33, 217–227. [Google Scholar] [CrossRef]
- Proudfoot, J.; Ryden, C.; Everitt, B.; Shapiro, D.A.; Goldberg, D.; Mann, A.; Tylee, A.; Marks, I.; Gray, J.A. Clinical efficacy of computerised cognitive-behavioural therapy for anxiety and depression in primary care: Randomised controlled trial. Br. J. Psychiatry 2004, 185, 46–54. [Google Scholar] [CrossRef]
- Christensen, H.; Griffiths, K.M.; Korten, A.; Powell, J. Web-based Cognitive Behavior Therapy: Analysis of Site Usage and Changes in Depression and Anxiety Scores. J. Med. Internet Res. 2002, 4, e3. [Google Scholar] [CrossRef] [PubMed]
- Karasouli, E.; Adams, A. Assessing the Evidence for e-Resources for Mental Health Self-Management: A Systematic Literature Review. JMIR Ment. Health 2014, 1, e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, G.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; Titov, N. Computer Therapy for the Anxiety and Depressive Disorders Is Effective, Acceptable and Practical Health Care: A Meta-Analysis. PLoS ONE 2010, 5, e13196. [Google Scholar] [CrossRef] [PubMed]
- Kaltenthaler, E.; Shackley, P.; Stevens, K.; Beverley, C.; Parry, G.; Chilcott, J. A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety. Health Technol. Assess. 2002, 6, 1–89. [Google Scholar] [CrossRef]
- Kaltenthaler, E.; Brazier, J.; De Nigris, E.; Tumur, I.; Ferriter, M.; Beverley, C.; Parry, G.; Rooney, G.; Sutcliffe, P. Computerised cognitive behaviour therapy for depression and anxiety update: A systematic review and economic evaluation. Health Technol. Assess. 2006, 10, 1–168. [Google Scholar] [CrossRef]
- Kaltenthaler, E.; Parry, G.; Beverley, C.; Ferriter, M. Computerised cognitive-behavioural therapy for depression: Systematic review. Br. J. Psychiatry 2008, 193, 181–184. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health Action Plan 2013–2020. 2017. Available online: http://apps.who.int/iris/bitstream/10665/89966/1/9789241506021_eng.pdf (accessed on 4 April 2022).
- Abou El-Magd, R.M.; Obuobi-Donkor, G.; Adu, M.K.; Lachowski, C.; Duddumpudi, S.; Lawal, M.A.; Sapara, A.O.; Achor, M.; Kouzehgaran, M.; Hegde, R.; et al. Repetitive Transcranial Magnetic Stimulation (rTMS) with and without Internet-Delivered Cognitive Behavior Therapy (iCBT) for the Treatment of Resistant Depression (TRD): Protocol for patient-centred Randomized Controlled Pilot Trial. JMIR Res. Protoc. 2020, 9, e18843. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Haynes, R.B. Clinical Epidemiology: How to Do Clinical Practice Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56. [Google Scholar] [CrossRef]
- Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Fisher, P.; Zelazny, J.; Burke, A.; Oquendo, M.; et al. Columbia-Suicide Severity Rating Scale; Columbia University: New York, NY, USA, 2008. [Google Scholar]
- American Psychological Association. DSM 5 diagnostic and statistical manual of mental disorders. In DSM 5 Diagnostic and Statistical Manual of Mental Disorders; The Association: Washington, DC, USA, 2013; p. 947. [Google Scholar]
- van Reenen, M.; Janssen, B. EQ-5D-5L User Guide: Basic Information on How to Use the EQ-5D-5L Instrument; EuroQol Research Foundation: Rotterdam, The Netherlands, 2015. [Google Scholar]
- Leucht, S.; Fennema, H.; Engel, R.; Kaspers–Janssen, M.; Lepping, P.; Szegedi, A. What does the HAMD mean? J. Affect. Disord. 2013, 148, 243–248. [Google Scholar] [CrossRef]
- Schmitt, N. Uses and abuses of coefficient alpha. Psychol. Assess. 1996, 8, 350. [Google Scholar] [CrossRef]
- Briggs, S.R.; Cheek, J.M. The role of factor analysis in the development and evaluation of personality scales. J. Pers. 1986, 54, 106–148. [Google Scholar] [CrossRef]
- Kobak, K.A.; Reynolds, W.M. The Hamilton Depression Inventory. 2004. Available online: https://psycnet.apa.org/record/2004-14941-010 (accessed on 4 April 2022).
- Sharp, R. The Hamilton rating scale for depression. Occup. Med. 2015, 65, 340. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, M.H.; Rush, A.J.; Ibrahim, H.M.; Carmody, T.J.; Biggs, M.M.; Suppes, T.; Crismon, M.L.; Shores-Wilson, K.; Toprac, M.G.; Dennehy, E.B.; et al. The Inventory of Depressive Symptomatology, Clinician Rating (IDS-C) and Self-Report (IDS-SR), and the Quick Inventory of Depressive Symptomatology, Clinician Rating (QIDS-C) and Self-Report (QIDS-SR) in public sector patients with mood disorders: A psychometric evaluation. Psychol. Med. 2004, 34, 73–82. [Google Scholar] [CrossRef]
- Doraiswamy, P.M.; Bernstein, I.H.; Rush, A.J.; Kyutoku, Y.; Carmody, T.J.; MacLeod, L.; Venkatraman, S.; Burks, M.; Stegman, D.; Witte, B.; et al. Diagnostic utility of the Quick Inventory of Depressive Symptomatology (QIDS-C16 and QIDS-SR16) in the elderly. Acta Psychiatr. Scand. 2010, 122, 226–234. [Google Scholar] [CrossRef]
- Bernstein, I.H.; Rush, A.J.; Trivedi, M.H.; Hughes, C.W.; Macleod, L.; Witte, B.P.; Jain, S.; Mayes, T.L.; Emslie, G.J. Psychometric properties of the Quick Inventory of Depressive Symptomatology in adolescents. Int. J. Methods Psychiatr. Res. 2010, 19, 185–194. [Google Scholar] [CrossRef]
- Rush, A.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein, D.N.; Markowitz, J.C.; Ninan, P.T.; Kornstein, S.; Manber, R.; et al. The 16-Item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 2003, 54, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Bilbao, A.; Martín-Fernández, J.; García-Pérez, L.; Mendezona, J.I.; Arrasate, M.; Candela, R.; Acosta, F.J.; Estebanez, S.; Retolaza, A. Psychometric properties of the EQ-5D-5L in patients with major depression: Factor analysis and Rasch analysis. J. Ment. Health 2021, 31, 506–516. [Google Scholar] [CrossRef]
- Kavanaugh, B.C.; Aaronson, S.T.; Clarke, G.N.; Holtzheimer, P.E.; Johnson, C.W.; McDonald, W.M.; Schneider, M.B.; Carpenter, L.L. Neurocognitive Effects of Repetitive Transcranial Magnetic Stimulation With a 2-Coil Device in Treatment-Resistant Major Depressive Disorder. J. ECT 2018, 34, 258–265. [Google Scholar] [CrossRef]
- Carpenter, L.L.; Aaronson, S.T.; Clarke, G.N.; Holtzheimer, P.E.; Johnson, C.W.; McDonald, W.M.; Stannard, E.L.; Schneider, M.B. rTMS with a two-coil array: Safety and efficacy for treatment resistant major depressive disorder. Brain Stimul. 2017, 10, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Kito, S.; Matsuda, Y.; Sewaki, Y.; Sekiya, J.; Fujii, T.; Noda, T.; Ikezawa, S.; Takano, H.; Nakazawa, K.; Nomura, M.; et al. A 6-Month Follow-up Case Study of Low-Frequency Right Prefrontal Repetitive Transcranial Magnetic Stimulation in Treatment-Resistant Bipolar Depression. J. ECT 2017, 33, e43–e44. [Google Scholar] [CrossRef] [PubMed]
- Johansson, R.; Sjöberg, E.; Sjögren, M.; Johnsson, E.; Carlbring, P.; Andersson, T.; Rousseau, A.; Andersson, G. Tailored vs. Standardized Internet-Based Cognitive Behavior Therapy for Depression and Comorbid Symptoms: A Randomized Controlled Trial. PLoS ONE 2012, 7, e36905. [Google Scholar] [CrossRef] [Green Version]
- Barbini, B.; Attanasio, F.; Manfredi, E.; Cavallini, M.C.; Zanardi, R.; Colombo, C. Bright light therapy accelerates the antidepressant effect of repetitive transcranial magnetic stimulation in treatment resistant depression: A pilot study. Int. J. Psychiatry Clin. Pract. 2021, 25, 375–377. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P.; Carlbring, P.; Riper, H.; Hedman, E. Guided Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: A systematic review and meta-analysis. World Psychiatry 2014, 13, 288–295. [Google Scholar] [CrossRef]
- Hedman, E.; Ljótsson, B.; Kaldo, V.; Hesser, H.; El Alaoui, S.; Kraepelien, M.; Andersson, E.; Rück, C.; Svanborg, C.; Andersson, G.; et al. Effectiveness of Internet-based cognitive behaviour therapy for depression in routine psychiatric care. J. Affect. Disord. 2014, 155, 49–58. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Warmerdam, L. Behavioral activation treatments of depression: A meta-analysis. Clin. Psychol. Rev. 2007, 27, 318–326. [Google Scholar] [CrossRef]
- Richards, D.; Richardson, T. Computer-based psychological treatments for depression: A systematic review and meta-analysis. Clin. Psychol. Rev. 2012, 32, 329–342. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P. Internet-Based and Other Computerized Psychological Treatments for Adult Depression: A Meta-Analysis. Cogn. Behav. Ther. 2009, 38, 196–205. [Google Scholar] [CrossRef]
- Twomey, C.; O’Reilly, G. Effectiveness of a freely available computerised cognitive behavioural therapy programme (MoodGYM) for depression: Meta-analysis. Aust. N. Z. J. Psychiatry 2016, 51, 260–269. [Google Scholar] [CrossRef]
- Orman, J.; O’Dea, B.; Shand, F.; Berk, M.; Proudfoot, J.; Christensen, H. Patients and technology: E-mental health for mood and anxiety disorders in general practice. Aust. Fam. Physician 2014, 43, 832–837. [Google Scholar] [PubMed]


{kind=link}
| Variables | rTMS | iCBT + rTMS | Total | Chi-Square/t-Test | p-Value |
|---|---|---|---|---|---|
| n = 39 | n = 39 | ||||
| Gender | |||||
| Male | 17 (43.6%) | 11 (28.2%) | 28 (35.9%) | ||
| Female | 22 (56.4%) | 28 (71.8%) | 50 (64.1%) | χ2(1) = 2.01 | 0.24 |
| Age (Years) | |||||
| ≤25 | 3 (7.7%) | 3 (7.7) | 6 (7.7%) | ||
| 26–40 | 19 (48.7%) | 14 (35.9%) | 33 (42.3%) | ||
| >40 | 17 (43.6%) | 22 (56.4%) | 39 (50.0%) | 1.47 * | 0.54 |
| Educational level | |||||
| Elementary | 1 (2.8%) | 1 (2.8%) | 2 (2.7%) | ||
| High school | 8 (22.2%) | 10 (26.3%) | 18 (24.3%) | ||
| College/University | 27 (75.0%) | 27 (71.1%) | 54 (73.0%) | 0.43 * | 0.89 |
| MDD at baseline | |||||
| At most mild depression | 18 (54.5%) | 16 (43.2%) | 34 (48.8%) | ||
| Moderate-to-severe depression | 15 (45.5%) | 21 (56.8%) | 36 (51.4%) | ||
| χ2(1) = 0.89 | 0.47 | ||||
| Suicidal ideation at baseline | |||||
| No suicidal ideation | 14 (40.0) | 7 (18.4) | 21 (28.8) | ||
| Present suicidal ideation | 21 (60.0) | 31 (81.6) | 52 (71.2) | χ2(1) = 4.14 | 0.07 |
| Subjective depression at baseline (QIDS) | |||||
| At most mild depression | |||||
| Moderate-to-severe depression | 4 (11.8) | 3 (8.1) | 7 (9.9) | ||
| 30 (88.2) | 34 (91.9) | 64 (90.1) | χ2(1) = 0.27 | 0.7 | |
| EQ-5D-5L at baseline | |||||
| Mobility: | |||||
| No problems walking | |||||
| Slight problems walking | 22 (64.7) | 28 (75.7) | 50 (70.4) | ||
| Moderate problems walking | 8 (23.5) | 2 (5.4) | 10 (14.1) | ||
| Severe problems walking | 3 (8.8) | 5 (13.5) | 8 (11.3) | ||
| Unable to walk | 1 (2.9) | 2 (5.4) | 3 (4.2) | 5.01 * | 0.15 |
| Self-care: | |||||
| No problems washing/dressing | |||||
| Slight problems washing/dressing | 18 (52.9) | 21 (56.8) | 39 (54.9) | ||
| Moderate problems washing/dressing | 10 (29.4) | 5 (13.5) | 15 (21.1) | ||
| Severe problems washing/dressing | 5 (14.7) | 7 (18.9) | 12 (16.9) | ||
| Unable to washing/dressing | 1 (2.9) | 4 (10.8) | 5 (7.0) | 3.91 | 0.27 |
| Usual activities | |||||
| No problems doing usual activities | 7 (20.6) | 2 (5.4) | 9 (12.7) | ||
| Slight problems doing usual activities | 7 (20.6) | 9 (24.3) | 16 (22.5) | ||
| Moderate problems doing usual activities | 12 (35.3) | 9 (24.3) | 21 (29.6) | ||
| Severe problems doing usual activities | |||||
| Unable to do usual activities | 7 (20.6) | 15 (40.5) | 22 (31.0) | 6.51 * | 0.15 |
| 1 (2.9) | 2 (5.4) | 3 (4.2) | |||
| Pain/discomfort | |||||
| No pain or discomfort | 13 (38.2) | 7 (18.9) | 20 (28.2) | ||
| Slight pain or discomfort | 6 (17.6) | 14 (37.8) | 20 (28.2) | ||
| Moderate pain or discomfort | 10 (29.4) | 11 (29.7) | 21 (29.6) | ||
| Severe pain or discomfort | 4 (11.8) | 5 (13.5) | 9 (12.7) | ||
| Extreme pain or discomfort | 1 (2.9) | 0 (0.0) | 1 (1.4) | 5.95 * | 0.17 |
| Anxiety/depression | |||||
| Not anxious or depressed | 1 (2.9) | 1 (2.7) | 2 (2.8) | ||
| Slightly anxious or depressed | 4 (11.8) | 0 (0.0) | 4 (5.6) | ||
| Moderately anxious or depressed | 13 (38.2) | 13 (35.1) | 26 (36.6) | ||
| Severely anxious or depressed | 10 (29.4) | 18 (48.6) | 28 (39.4) | ||
| Extremely anxious or depressed | 6 (17.6) | 5 (13.5) | 11 (15.5) | 6.22 * | 0.15 |
| Total score HAMD at baseline | n = 33 | n = 37 | - | ||
| Mean score (SD) | 15.73 (6.03) | 17.43 (4.79) | t (68) = 1.32 | 0.19 | |
| Total score CSSRS baseline | n = 35 | n = 38 | - | ||
| Mean score (SD) | 1.57 (1.70) | 1.79 (1.44) | t (71) = 0.59 | 0.56 | |
| Total score QIDS baseline | n = 34 | n = 37 | - | ||
| Mean score (SD) | 16.62 (4.59) | 17.59 (4.15) | t (69) = 0.94 | 0.35 | |
| EQ-VAS at baseline mean score (SD) | n = 33 | n = 37 | - | ||
| 47.48 (18.42) | 45.27 (18.36) | - | t (68) = 0.50 | 0.62 | |
| Measure | Descriptive | ANCOVA Parameters | |||||
|---|---|---|---|---|---|---|---|
| Baseline, Mean (SD) | Discharge Means (SD) | F Value (df) | p-Value | Partial Eta | |||
| rTMS | rTMS + iCBT | rTMS | rTMS + iCBT | ||||
| HAM-D-17 | 15.73 (6.03) | 17.43 (4.79) | 8.89 (5.83) | 9.97 (7.03) | 0.15 (1) | 0.70 | 0.003 |
| CSSRS | 1.57 (1.70) | 1.79 (1.44) | 0.96 (1.45) | 1.03 (1.11) | 0.04 (1) | 0.85 | 0.001 |
| QIDS-16 | 16.62 (4.59) | 17.59 (4.15) | 10.08 (4.36) | 11.34 (5.72) | 0.26 (1) | 0.61 | 0.005 |
| EQ-VAS | 65.80 (17.06) | 59.76 (21.72) | 64.42 (18.13) | 60.90 (21.45) | 0.46 (1) | 0.50 | 0.009 |
| Measures | rTMS | iCBT + rTMS | Total | Chi-Square/Fischer Exact | p-Value |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| MDD at discharge | n = 27 | n = 30 | |||
| At most mild depression | 24 (88.9) | 25 (83.3) | 49 (86.0) | * | 0.71 |
| Moderate-to-severe depression | 3 (11.1) | 5 (16.7) | 8 (14.0) | ||
| Suicidal ideation at discharge | n = 28 | n = 31 | |||
| No suicidal ideation | 16 (57.1) | 12 (38.7) | 28 (47.5) | 2.01 | |
| Present suicidal ideation | 12 (42.9) | 19 (61.3) | 31 (52.5) | 0.2 | |
| Likely depression at discharge (QIDS) | |||||
| At most mild depression | n = 26 | n = 32 | |||
| Moderate-to-severe depression | 13 (50.0) | 19 (59.4) | 32 (55.2) | ||
| 13 (50.0) | 13 (40.6) | 26 (44.8) | 0.51 | 0.6 | |
| EQ-5D-5L at discharge | |||||
| Mobility: | |||||
| No problems walking | 17 (65.4) | 23 (74.2) | 40 (70.2) | ||
| Slight problems walking | 7 (26.9) | 5 (16.1) | 12 (21.1) | ||
| Moderate problems walking | 1 (3.8) | 1 (3.2) | 2 (3.5) | ||
| Severe problems walking | 1 (3.8) | 2 (6.5) | 3 (5.3) | ||
| Unable to walk | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.48 * | 0.81 |
| Self-care: | |||||
| No problems washing/dressing | |||||
| Slight problems washing/dressing | 17 (65.4) | 19 (61.3) | 36 (63.2) | ||
| Moderate problems washing/dressing | 7 (26.9) | 8 (25.8) | 15 (26.3) | ||
| Severe problems washing/dressing | 1 (3.8) | 3 (9.7) | 4 (7.0) | ||
| Unable to washing/dressing | 1 (3.8) | 1 (3.2) | 2 (3.5) | 0.98 | 0.91 |
| Usual activities | |||||
| No problems doing usual activities | 7 (26.9) | 4 (12.9) | 11 (19.3) | ||
| Slight problems doing usual activities | 9 (34.6) | 15 (48.4) | 24 (42.1) | ||
| Moderate problems doing usual activities | 6 (23.1) | 6 (19.4) | 12 (21.1) | ||
| Severe problems doing usual activities | 3 (11.5) | 5 (16.1) | 8 (14.0) | ||
| Unable to do usual activities | 1 (3.8) | 1 (3.2) | 2 (3.5) | 2.66 | 0.67 |
| Pain/discomfort | |||||
| No pain or discomfort | 12 (46.2) | 13 (41.9) | 25 (43.9) | ||
| Slight pain or discomfort | 7 (26.9) | 9 (29.0) | 16 (28.1) | ||
| Moderate pain or discomfort | 6 (23.1) | 6 (19.4) | 12 (21.1) | ||
| Severe pain or discomfort | 0 (0.0) | 2 (6.5) | 2 (3.5) | ||
| Extreme pain or discomfort | 1 (3.8) | 1 (3.2) | 2 (3.5) | 1.83 * | 0.87 |
| Anxiety/depression | |||||
| Not anxious or depressed | 4 (15.4) | 4 (12.9) | 8 (14.0) | ||
| Slightly anxious or depressed | 6 (23.1) | 11 (35.5) | 17 (29.8) | ||
| Moderately anxious or depressed | 10 (38.5) | 8 (25.8) | 18 (31.6) | 0.59 | |
| Severely anxious or depressed | 5 (19.2) | 8 (25.8) | 13 (22.8) | ||
| Extremely anxious or depressed | 1 (3.8) | 0 (0.0) | 1 (1.8) | 2.95 * | |
| Measure | Responses, n | Scores | Mean Difference (95% CI) | p-Value | t Value | Effect Size (Cohen d) | ||
|---|---|---|---|---|---|---|---|---|
| Baseline Score, Mean (SD) | Six-Week Score, Mean (SD) | Change from Baseline, % | ||||||
| HAMD | 56 | 16.25 (5.29) | 9.45 (6.44) | 41.8 | 6.80 (4.98–8.63) | <0.001 | 7.46 | 1.15 |
| CSSRS | 59 | 1.69 (1.59) | 1.00 (1.27) | 40.8 | 0.69 (0.35–1.04) | <0.001 | 4.06 | 0.48 |
| QIDS | 56 | 16.79(4.45) | 10.88 (5.22) | 35.2 | 5.91 (4.66–7.16) | <0.001 | 9.45 | 1.23 |
| EQ-VAS | 54 | 47.67 (18.45) | 62.56 (19.75) | 61.56 | 14.89 (−19.62)–(−10.16) | <0.001 | 6.31 | 0.78 |
| Condition | Prevalence, n/Total Responses (%) | Change in Prevalence (the Sixth Week from Baseline), % | χ2 (df) | p-Value | |
|---|---|---|---|---|---|
| Baseline | Sixth Week | ||||
| MDD clinical diagnosis | 27/56 (48.2) | 8/56 (14.3) | −33.9 | 15.00 (1) | <0.001 |
| Suicidal ideations | 42/59 (71.2) | 31/59 (52.5) | −18.7 | 4.35 (1) | 0.004 |
| Subjective depression (QIDS-16) | 49/56 (87.5) | 26/56 (46.4) | −41.1 | 21.35 (1) | <0.001 |
| EQ-5D-5L | |||||
| Mobility: | |||||
| No problems walking | −3.6 | ||||
| Slight problems walking | 41/55 (74.5) | 39/55 (70.9) | 10.9 | ||
| Moderate problems walking | 6/55 (10.9) | 12/55 (21.8) | −7.3 | ||
| Severe problems walking | 5/55 (9.1) | 1/55 (1.8) | 0 | 4.72(1) | 0.194 |
| Unable to walk | 3/55 (5.5) | 3/55 (5.5) | |||
| Self-care: | |||||
| No problems washing/dressing | 32/55 (58.2) | 35/55 (63.6) | |||
| Slight problems washing/dressing | 11/55 (20.0) | 14/55 (25.5) | 5.4 | ||
| Moderate problems washing/dressing | 11/55 (20.0) | 4/55 (7.3) | 5.5 | ||
| Severe problems washing/dressing | 1/55 (1.8) | 2/55 (3.6) | −12.7 | 4.09 (1) | 0.252 |
| Unable to washing/dressing | 1.8 | ||||
| Usual activities | |||||
| No problems doing usual activities | 8/55 (14.5) | 11/55(20.0) | 5.5 | ||
| Slight problems doing usual activities | 14/55 (25.5) | 23/55 (41.8) | 16.3 | ||
| Moderate problems doing usual activities | 16/55 (29.1) | 11/55 (20.0) | −9.1 | ||
| Severe problems doing usual activities | 15/55 (27.3) | 8/55 (14.5) | −12.8 | 5.72 (1) | 0.221 |
| Unable to do usual activities | 2/55 (3.6) | 2/55 (3.6) | 0 | ||
| Pain/discomfort | |||||
| No pain or discomfort | 15/55 (27.3) | 24/55 (43.6) | 16.3 | ||
| Slight pain or discomfort | 18/55 (32.7) | 16/55 (29.1) | -3.6 | ||
| Moderate pain or discomfort | 16/55 (29.1) | 11/55 (20.0) | -9.1 | ||
| Severe pain or discomfort | 5/55 (9.1) | 2/55 (3.6) | -5.5 | 4.74 (1) | 0.315 |
| Extreme pain or discomfort | 1/55 (1.8) | 2/55 (3.6) | 1.8 | ||
| Anxiety/depression | |||||
| Not anxious or depressed | 2/55 (3.6) | 7/55 (12.7) | 9.1 | ||
| Slightly anxious or depressed | 3/55 (5.5) | 16/55 (29.1) | 23.6 | ||
| Moderately anxious or depressed | 18/55 (32.7) | 18/55 (32.7) | 0 | ||
| Severely anxious or depressed | 21/55 (38.2 | 13/55 (23.6) | −14.6 | 21.89 (1) | <0.001 |
| Extremely anxious or depressed | 11/55 (20.0) | 1/55 (3.6) | −16.6 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adu, M.K.; Shalaby, R.; Eboreime, E.; Sapara, A.; Lawal, M.A.; Chew, C.; Daubert, S.; Urichuck, L.; Surood, S.; Li, D.; et al. Apparent Lack of Benefit of Combining Repetitive Transcranial Magnetic Stimulation with Internet-Delivered Cognitive Behavior Therapy for the Treatment of Resistant Depression: Patient-Centered Randomized Controlled Pilot Trial. Brain Sci. 2023, 13, 293. https://doi.org/10.3390/brainsci13020293
Adu MK, Shalaby R, Eboreime E, Sapara A, Lawal MA, Chew C, Daubert S, Urichuck L, Surood S, Li D, et al. Apparent Lack of Benefit of Combining Repetitive Transcranial Magnetic Stimulation with Internet-Delivered Cognitive Behavior Therapy for the Treatment of Resistant Depression: Patient-Centered Randomized Controlled Pilot Trial. Brain Sciences. 2023; 13(2):293. https://doi.org/10.3390/brainsci13020293
Chicago/Turabian StyleAdu, Medard Kofi, Reham Shalaby, Ejemai Eboreime, Adegboyega Sapara, Mobolaji A. Lawal, Corina Chew, Shelley Daubert, Liana Urichuck, Shireen Surood, Daniel Li, and et al. 2023. "Apparent Lack of Benefit of Combining Repetitive Transcranial Magnetic Stimulation with Internet-Delivered Cognitive Behavior Therapy for the Treatment of Resistant Depression: Patient-Centered Randomized Controlled Pilot Trial" Brain Sciences 13, no. 2: 293. https://doi.org/10.3390/brainsci13020293