

Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Right Heart Catheterization: Principles and Methodology
3. Right Heart Catheterization in HFpEF
4. Right Heart Catheterization in AdHF
4.1. The Role of RHC in Advanced HFrEF and Candidacy for LVAD or Heart Replacement Therapy
4.2. The Role of RHC in Post-Heart Replacement Therapy and LVAD Management
5. Right Heart Catheterization in Acute HF (AHF) and Cardiogenic Shock (CS)
5.1. The Diagnostic Role of RHC
5.2. The Role of RHC in Guiding Therapy
5.3. The Prognostic Role of RHC
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACS | acute coronary syndrome |
| AdHF | advanced heart failure |
| AHF | acute heart failure |
| AMI | acute myocardial infarction |
| APE | acute pulmonary edema |
| BMI | body mass index |
| BP | blood pressure |
| BSA | body surface area |
| BTD | bridge to decision |
| BTT | bridge to transplantation |
| CAD | coronary artery disease |
| CFR | coronary flow reserve |
| CI | cardiac index |
| CMD | coronary microvascular dysfunction |
| CMR | cardiac magnetic resonance |
| CPET | cardiopulmonary exercise test |
| CO | cardiac output |
| COPD | chronic obstructive pulmonary disease |
| CPI | cardiac power index |
| CPO | cardiac power output |
| CS | cardiogenic shock |
| CVP | central venous pressure |
| HFA | Heart Failure Association |
| ECG | electrocardiogram |
| ECMO | extracorporeal membrane oxygenation |
| ESC | European Society of Cardiology |
| ERS | European Respiratory Society |
| HF | heart failure |
| HFpEF | heart failure with a preserved ejection fraction |
| HFrEF | heart failure with reduced ejection fraction |
| HR | heart rate |
| IABP | intra-aortic balloon pump |
| ICU | intensive care unit |
| IHM | invasive hemodynamic monitoring |
| IMR | microvascular resistance |
| LA | left atrium |
| LHC | left heart catheterization |
| LV | left ventricle |
| LVAD | left ventricular assist device |
| LVEDP | left ventricular end-diastolic pressure |
| LVESP | left ventricular end-systolic pressure |
| LVEF | left ventricular ejection fraction |
| MAP | mean arterial pressure |
| MCS | mechanical circulatory support |
| MI | myocardial infarction |
| MR | mitral regurgitation |
| mPAP | mean pulmonary artery pressure. |
| NRD | Nationwide Readmissions Database |
| sPAP | systolic pulmonary artery pressure |
| NP | natriuretic peptides |
| PA | pulmonary artery |
| PAC | pulmonary artery catheter |
| PAP | pulmonary artery pressure |
| PAPi | pulmonary artery pulsatility index |
| PCWP | pulmonary capillary wedge pressure |
| PGD | primary graft dysfunction |
| PH | pulmonary hypertension |
| PLR | passive leg raise |
| PV | pressure-volume |
| PVR | pulmonary vascular resistance |
| QoL | Quality of Life |
| RA | right atrium |
| RAP | right atrial pressure |
| RHC | right heart catheterization |
| RV | right ventricle |
| RVAD | right ventricular assist device |
| RVP | right ventricular pressure |
| RVSWI | RV stroke work index |
| SCAI | Society for Cardiovascular Angiography and Interventions |
| S-G | Swan–Ganz |
| SV | stroke volume |
| SvO2 | mixed venous oxygen saturation |
| SVR | systemic vascular resistance |
| TAPSE | tricuspid annular plane systolic excursion |
| TPG | transpulmonary gradient |
| TR | tricuspid regurgitation |
| VAD | ventricular assist device |
| VA-ECMO | Venoarterial extracorporeal membrane oxygenation |
| VO2 | maximal oxygen consumption |
| WU | wood unit |
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Binanay, C.; Califf, R.M.; Hasselblad, V.; O’Connor, C.M.; Shah, M.R.; Sopko, G.; Stevenson, L.W.; Francis, G.S.; Leier, C.V.; Miller, L.W.; et al. Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness: The ESCAPE Trial. JAMA 2005, 294, 1625–1633. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Panjrath, G.S.; Amancherla, K.; Davis, L.L.; Deswal, A.; Dixon, D.L.; Januzzi, J.L.; Yancy, C.W. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure with Preserved Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2023, 81, 1835–1878. [Google Scholar] [CrossRef] [PubMed]
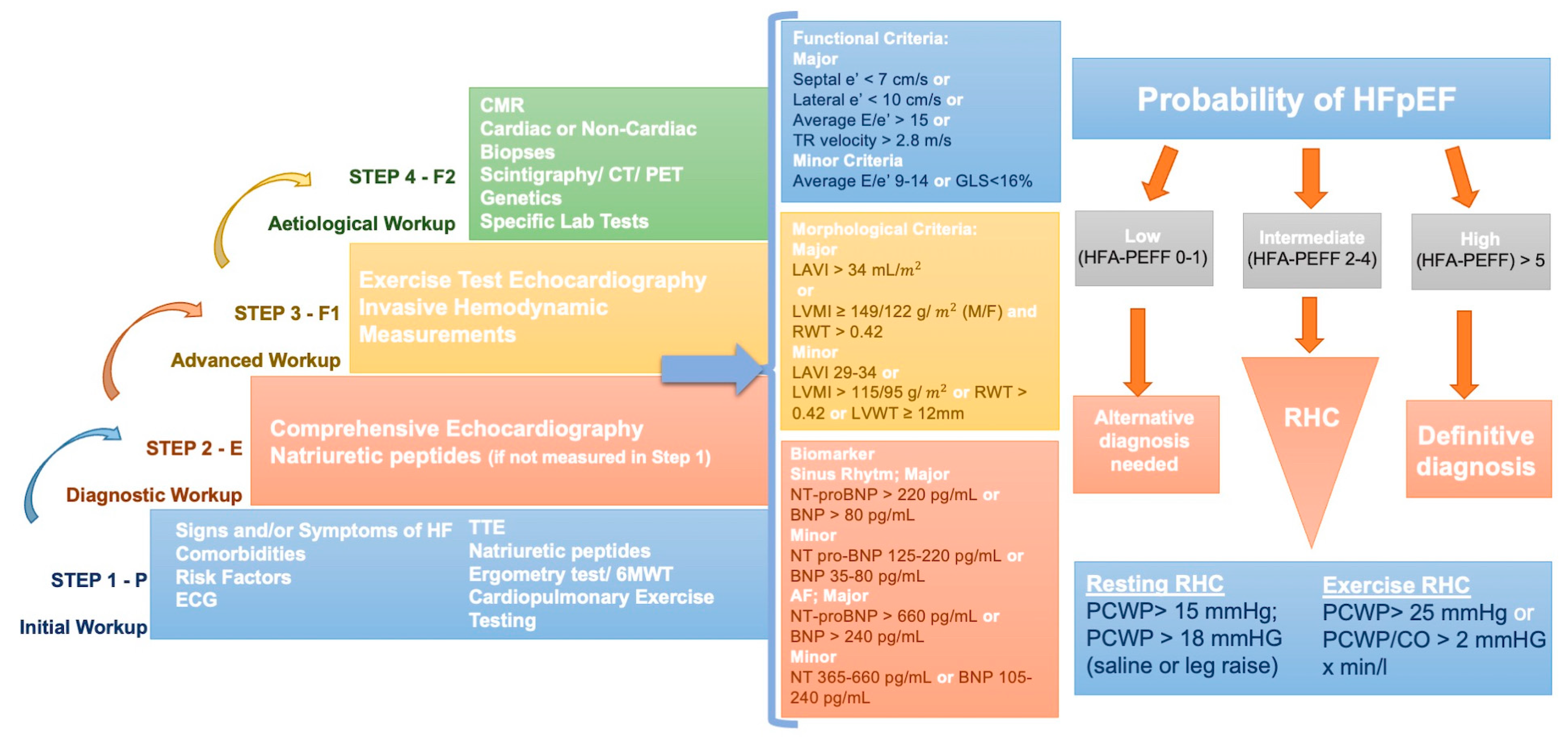
- Pieske, B.; Tschöpe, C.; de Boer, R.A.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to Diagnose Heart Failure with Preserved Ejection Fraction: The HFA-PEFF Diagnostic Algorithm: A Consensus Recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 40, 3297–3317. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, A.B.; Desai, S.P. Swan, Ganz, and Their Catheter: Its Evolution Over the Past Half Century. Ann. Intern. Med. 2018, 169, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, G.M.; Ciarka, A.; Biniecka, M.; Ceranowicz, P. Right Heart Catheterization-Background, Physiological Basics, and Clinical Implications. J. Clin. Med. 2019, 8, 1331. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.S. A Tale of Serendipity, Ingenuity, and Chance: 50th Anniversary of Creation of the Swan-Ganz Catheter. J. Am. Coll. Cardiol. 2019, 74, 100–103. [Google Scholar] [CrossRef]
- Chokkalingam Mani, B.; Chaudhari, S.S. Right Heart Cardiac Catheterization; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- De Backer, D.; Vincent, J.-L. The Pulmonary Artery Catheter: Is It Still Alive? Curr. Opin. Crit. Care 2018, 24, 204–208. [Google Scholar] [CrossRef]
- Hsu, S.; Fang, J.C.; Borlaug, B.A. Hemodynamics for the Heart Failure Clinician: A State-of-the-Art Review. J. Card. Fail. 2022, 28, 133–148. [Google Scholar] [CrossRef]
- Krishnan, A.; Markham, R.; Savage, M.; Wong, Y.-W.; Walters, D. Right Heart Catheterisation: How to Do It. Heart Lung Circ. 2019, 28, e71–e78. [Google Scholar] [CrossRef]
- Saugel, B.; Scheeren, T.W.L.; Teboul, J.-L. Ultrasound-Guided Central Venous Catheter Placement: A Structured Review and Recommendations for Clinical Practice. Crit. Care 2017, 21, 225. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.-T.; Kwan, G.N.C.; Evans-Barns, H.; Rophael, J.A.; van Driel, M.L. Venous Cutdown versus the Seldinger Technique for Placement of Totally Implantable Venous Access Ports. Cochrane Database Syst. Rev. 2016, 2016, CD008942. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Ziccardi, M.; Khalid, N. Pulmonary Artery Catheterization; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kovacs, G.; Avian, A.; Pienn, M.; Naeije, R.; Olschewski, H. Reading Pulmonary Vascular Pressure Tracings. How to Handle the Problems of Zero Leveling and Respiratory Swings. Am. J. Respir. Crit. Care Med. 2014, 190, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, S.; Preston, I.R. Right Heart Catheterisation: Best Practice and Pitfalls in Pulmonary Hypertension. Eur. Respir. Rev. 2015, 24, 642–652. [Google Scholar] [CrossRef] [PubMed]
- D’Alto, M.; Dimopoulos, K.; Coghlan, J.G.; Kovacs, G.; Rosenkranz, S.; Naeije, R. Right Heart Catheterization for the Diagnosis of Pulmonary Hypertension: Controversies and Practical Issues. Heart Fail. Clin. 2018, 14, 467–477. [Google Scholar] [CrossRef]
- Saxena, A.; Garan, A.R.; Kapur, N.K.; O’Neill, W.W.; Lindenfeld, J.; Pinney, S.P.; Uriel, N.; Burkhoff, D.; Kern, M. Value of Hemodynamic Monitoring in Patients with Cardiogenic Shock Undergoing Mechanical Circulatory Support. Circulation 2020, 141, 1184–1197. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Borlaug, B.A.; Kitzman, D.W.; McCulloch, A.D.; Blaxall, B.C.; Agarwal, R.; Chirinos, J.A.; Collins, S.; Deo, R.C.; Gladwin, M.T.; et al. Research Priorities for Heart Failure with Preserved Ejection Fraction: National Heart, Lung, and Blood Institute Working Group Summary. Circulation 2020, 141, 1001–1026. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure with Preserved Ejection Fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef]
- Kasner, M.; Aleksandrov, A.S.; Westermann, D.; Lassner, D.; Gross, M.; von Haehling, S.; Anker, S.D.; Schultheiss, H.-P.; Tschöpe, C. Functional Iron Deficiency and Diastolic Function in Heart Failure with Preserved Ejection Fraction. Int. J. Cardiol. 2013, 168, 4652–4657. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.; Ebner, N.; Valentova, M.; Sandek, A.; Doehner, W.; Cleland, J.G.; Lainscak, M.; Schulze, P.C.; et al. Iron Deficiency in Patients with Heart Failure with Preserved Ejection Fraction and Its Association with Reduced Exercise Capacity, Muscle Strength and Quality of Life. Clin. Res. Cardiol. 2019, 108, 203–211. [Google Scholar] [CrossRef]
- Buckley, L.F.; Canada, J.M.; Del Buono, M.G.; Carbone, S.; Trankle, C.R.; Billingsley, H.; Kadariya, D.; Arena, R.; Van Tassell, B.W.; Abbate, A. Low NT-ProBNP Levels in Overweight and Obese Patients Do Not Rule out a Diagnosis of Heart Failure with Preserved Ejection Fraction. ESC Heart Fail. 2018, 5, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Reddy, Y.N.V.; Pislaru, S.V.; Melenovsky, V.; Borlaug, B.A. Evidence Supporting the Existence of a Distinct Obese Phenotype of Heart Failure with Preserved Ejection Fraction. Circulation 2017, 136, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.-W.; Park, S.-J.; Cho, E.J.; Kim, E.K.; Lee, G.Y.; Chang, S.-A.; Choi, J.-O.; Lee, S.-C.; Park, S.W. Relation of N-Terminal Pro-B-Type Natriuretic Peptide and Left Ventricular Diastolic Function to Exercise Tolerance in Patients with Significant Valvular Heart Disease and Normal Left Ventricular Systolic Function. Am. J. Cardiol. 2017, 119, 1846–1853. [Google Scholar] [CrossRef] [PubMed]
- Hummel, Y.M.; Liu, L.C.Y.; Lam, C.S.P.; Fonseca-Munoz, D.F.; Damman, K.; Rienstra, M.; van der Meer, P.; Rosenkranz, S.; van Veldhuisen, D.J.; Voors, A.A.; et al. Echocardiographic Estimation of Left Ventricular and Pulmonary Pressures in Patients with Heart Failure and Preserved Ejection Fraction: A Study Utilizing Simultaneous Echocardiography and Invasive Measurements. Eur. J. Heart Fail. 2017, 19, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Lam, C.S.P.; Svedlund, S.; Saraste, A.; Hage, C.; Tan, R.-S.; Beussink-Nelson, L.; Ljung Faxén, U.; Fermer, M.L.; Broberg, M.A.; et al. Prevalence and Correlates of Coronary Microvascular Dysfunction in Heart Failure with Preserved Ejection Fraction: PROMIS-HFpEF. Eur. Heart J. 2018, 39, 3439–3450. [Google Scholar] [CrossRef]
- Hwang, S.-J.; Melenovsky, V.; Borlaug, B.A. Implications of Coronary Artery Disease in Heart Failure with Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2014, 63, 2817–2827. [Google Scholar] [CrossRef]
- Phan, T.T.; Shivu, G.N.; Abozguia, K.; Davies, C.; Nassimizadeh, M.; Jimenez, D.; Weaver, R.; Ahmed, I.; Frenneaux, M. Impaired Heart Rate Recovery and Chronotropic Incompetence in Patients with Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2010, 3, 29–34. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Nishimura, R.A.; Sorajja, P.; Lam, C.S.P.; Redfield, M.M. Exercise Hemodynamics Enhance Diagnosis of Early Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2010, 3, 588–595. [Google Scholar] [CrossRef]
- Simonneau, G.; Montani, D.; Celermajer, D.S.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic Definitions and Updated Clinical Classification of Pulmonary Hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Nair, N. Invasive Hemodynamics in Heart Failure with Preserved Ejection Fraction: Importance of Detecting Pulmonary Vascular Remodeling and Right Heart Function. Heart Fail. Clin. 2021, 17, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Paulus, W.J.; Tschöpe, C.; Sanderson, J.E.; Rusconi, C.; Flachskampf, F.A.; Rademakers, F.E.; Marino, P.; Smiseth, O.A.; De Keulenaer, G.; Leite-Moreira, A.F.; et al. How to Diagnose Diastolic Heart Failure: A Consensus Statement on the Diagnosis of Heart Failure with Normal Left Ventricular Ejection Fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur. Heart J. 2007, 28, 2539–2550. [Google Scholar] [CrossRef]
- Bilak, J.M.; Alam, U.; Miller, C.A.; McCann, G.P.; Arnold, J.R.; Kanagala, P. Microvascular Dysfunction in Heart Failure with Preserved Ejection Fraction: Pathophysiology, Assessment, Prevalence and Prognosis. Card. Fail. Rev. 2022, 8, e24. [Google Scholar] [CrossRef] [PubMed]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.H.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur. Heart J. 2021, 16, 1049–1069. [Google Scholar] [CrossRef]
- Prasad, S.B.; Holland, D.J.; Atherton, J.J. Diastolic Stress Echocardiography: From Basic Principles to Clinical Applications. Heart 2018, 104, 1739–1748. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. J. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Guazzi, M.; Wilhelm, M.; Halle, M.; Van Craenenbroeck, E.; Kemps, H.; de Boer, R.A.; Coats, A.J.S.; Lund, L.; Mancini, D.; Borlaug, B.; et al. Exercise Testing in Heart Failure with Preserved Ejection Fraction: An Appraisal through Diagnosis, Pathophysiology and Therapy—A Clinical Consensus Statement of the Heart Failure Association and European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 1327–1345. [Google Scholar] [CrossRef]
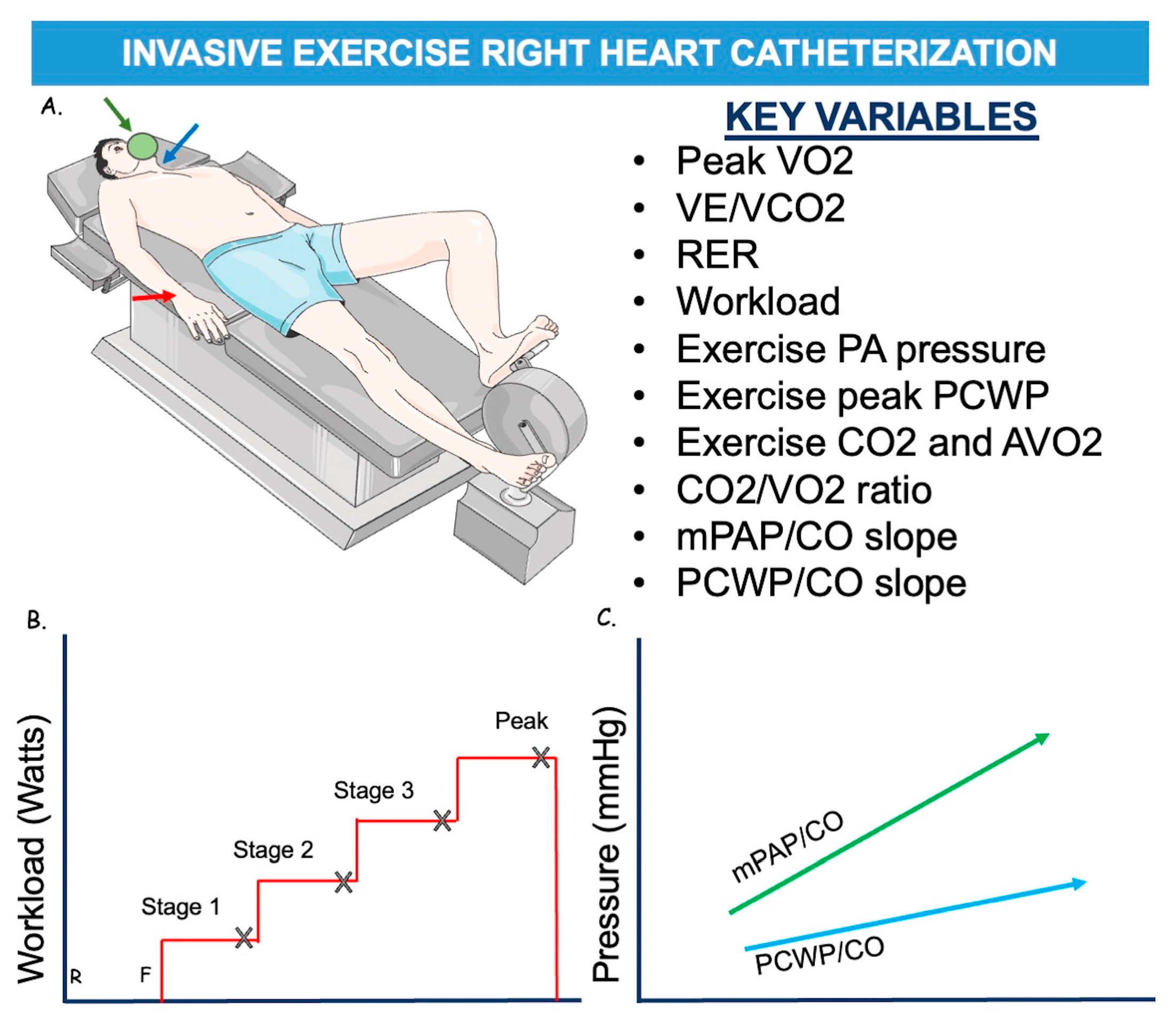
- Jain, C.C.; Borlaug, B.A. Performance and Interpretation of Invasive Hemodynamic Exercise Testing. Chest 2020, 158, 2119–2129. [Google Scholar] [CrossRef]
- Pandey, A.; Khera, R.; Park, B.; Haykowsky, M.; Borlaug, B.A.; Lewis, G.D.; Kitzman, D.W.; Butler, J.; Berry, J.D. Relative Impairments in Hemodynamic Exercise Reserve Parameters in Heart Failure with Preserved Ejection Fraction: A Study-Level Pooled Analysis. JACC Heart Fail. 2018, 6, 117–126. [Google Scholar] [CrossRef]
- Rieth, A.; Richter, M.J.; Gall, H.; Seeger, W.; Ghofrani, H.A.; Mitrovic, V.; Hamm, C.W. Hemodynamic Phenotyping Based on Exercise Catheterization Predicts Outcome in Patients with Heart Failure and Reduced Ejection Fraction. J. Heart Lung Transplant. 2017, 36, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Olson, T.P.; Reddy, Y.N.V.; Melenovsky, V.; Kane, G.C.; Borlaug, B.A. Haemodynamics, Dyspnoea, and Pulmonary Reserve in Heart Failure with Preserved Ejection Fraction. Eur. Heart J. 2018, 39, 2810–2821. [Google Scholar] [CrossRef] [PubMed]
- Dorfs, S.; Zeh, W.; Hochholzer, W.; Jander, N.; Kienzle, R.-P.; Pieske, B.; Neumann, F.J. Pulmonary Capillary Wedge Pressure during Exercise and Long-Term Mortality in Patients with Suspected Heart Failure with Preserved Ejection Fraction. Eur. Heart J. 2014, 35, 3103–3112. [Google Scholar] [CrossRef] [PubMed]
- Finet, J.E.; Van Iterson, E.H.; Wilson Tang, W.H. Invasive Hemodynamic and Metabolic Evaluation of HFpEF. Curr. Treat. Options Cardiovasc. Med. 2021, 23, 32. [Google Scholar] [CrossRef] [PubMed]
- Wolsk, E.; Bakkestrøm, R.; Thomsen, J.H.; Balling, L.; Andersen, M.J.; Dahl, J.S.; Hassager, C.; Møller, J.E.; Gustafsson, F. The Influence of Age on Hemodynamic Parameters during Rest and Exercise in Healthy Individuals. JACC Heart Fail. 2017, 5, 337–346. [Google Scholar] [CrossRef]
- Naeije, R.; Vanderpool, R.; Dhakal, B.P.; Saggar, R.; Saggar, R.; Vachiery, J.-L.; Lewis, G.D. Exercise-Induced Pulmonary Hypertension: Physiological Basis and Methodological Concerns. Am. J. Respir. Crit. Care Med. 2013, 187, 576–583. [Google Scholar] [CrossRef]
- Eisman, A.S.; Shah, R.V.; Dhakal, B.P.; Pappagianopoulos, P.P.; Wooster, L.; Bailey, C.; Cunningham, T.F.; Hardin, K.M.; Baggish, A.L.; Ho, J.E.; et al. Pulmonary Capillary Wedge Pressure Patterns during Exercise Predict Exercise Capacity and Incident Heart Failure. Circ. Heart Fail. 2018, 11, e004750. [Google Scholar] [CrossRef]
- Ho, J.E.; Zern, E.K.; Wooster, L.; Bailey, C.S.; Cunningham, T.; Eisman, A.S.; Hardin, K.M.; Zampierollo, G.A.; Jarolim, P.; Pappagianopoulos, P.P.; et al. Differential Clinical Profiles, Exercise Responses, and Outcomes Associated with Existing HFpEF Definitions. Circulation 2019, 140, 353–365. [Google Scholar] [CrossRef]
- D’Alto, M.; Romeo, E.; Argiento, P.; Motoji, Y.; Correra, A.; Di Marco, G.M.; Iacono, A.M.; Barracano, R.; D’Andrea, A.; Rea, G.; et al. Clinical Relevance of Fluid Challenge in Patients Evaluated for Pulmonary Hypertension. Chest 2017, 151, 119–126. [Google Scholar] [CrossRef]
- Andersen, M.J.; Olson, T.P.; Melenovsky, V.; Kane, G.C.; Borlaug, B.A. Differential Hemodynamic Effects of Exercise and Volume Expansion in People with and without Heart Failure. Circ. Heart Fail. 2015, 8, 41–48. [Google Scholar] [CrossRef]
- van de Bovenkamp, A.A.; Wijkstra, N.; Oosterveer, F.P.T.; Vonk Noordegraaf, A.; Bogaard, H.J.; van Rossum, A.C.; de Man, F.S.; Borlaug, B.A.; Handoko, M.L. The Value of Passive Leg Raise during Right Heart Catheterization in Diagnosing Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2022, 15, e008935. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Kane, G.C.; Reddy, Y.N.V.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure with Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation 2017, 135, 825–838. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.A.; Gelijns, A.C.; Moskowitz, A.J.; Heitjan, D.F.; Stevenson, L.W.; Dembitsky, W.; Long, J.W.; Ascheim, D.D.; Tierney, A.R.; Levitan, R.G.; et al. Long-Term Use of a Left Ventricular Assist Device for End-Stage Heart Failure. N. Engl. J. Med. 2001, 345, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Ammar, K.A.; Jacobsen, S.J.; Mahoney, D.W.; Kors, J.A.; Redfield, M.M.; Burnett, J.C.; Rodeheffer, R.J. Prevalence and Prognostic Significance of Heart Failure Stages: Application of the American College of Cardiology/American Heart Association Heart Failure Staging Criteria in the Community. Circulation 2007, 115, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Xanthakis, V.; Enserro, D.M.; Larson, M.G.; Wollert, K.C.; Januzzi, J.L.; Levy, D.; Aragam, J.; Benjamin, E.J.; Cheng, S.; Wang, T.J.; et al. Prevalence, Neurohormonal Correlates, and Prognosis of Heart Failure Stages in the Community. JACC Heart Fail. 2016, 4, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Giustiniano, E.; Padua, E.; Negri, K.; Bragato, R.M.; Cecconi, M. Echocardiography during Prone-Position Mechanical Ventilation in Patients with COVID-19: A Proposal for a New Approach. J. Am. Soc. Echocardiogr. 2020, 33, 905–906. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Danziger-Isakov, L.; Kirklin, J.K.; Kirk, R.; Kushwaha, S.S.; et al. The 2016 International Society for Heart Lung Transplantation Listing Criteria for Heart Transplantation: A 10-Year Update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Parker, W.F.; Chung, K.; Anderson, A.S.; Siegler, M.; Huang, E.S.; Churpek, M.M. Practice Changes at U.S. Transplant Centers After the New Adult Heart Allocation Policy. J. Am. Coll. Cardiol. 2020, 75, 2906–2916. [Google Scholar] [CrossRef]
- Gonzalez, J.; Callan, P. Invasive Haemodynamic Assessment before and after Left Ventricular Assist Device Implantation: A Guide to Current Practice. Interv. Cardiol. 2021, 16, e34. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D.; Hsich, E.; Meiser, B.; Potena, L.; Robinson, A.; Rossano, J.W.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-Sixth Adult Heart Transplantation Report—2019; Focus Theme: Donor and Recipient Size Match. J. Heart Lung Transplant. 2019, 38, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Costard-Jäckle, A.; Fowler, M.B. Influence of Preoperative Pulmonary Artery Pressure on Mortality after Heart Transplantation: Testing of Potential Reversibility of Pulmonary Hypertension with Nitroprusside Is Useful in Defining a High-Risk Group. J. Am. Coll. Cardiol. 1992, 19, 48–54. [Google Scholar] [CrossRef]
- Ghio, S.; Crimi, G.; Houston, B.; Montalto, C.; Garascia, A.; Boffini, M.; Temporelli, P.L.; La Rovere, M.T.; Pacileo, G.; Panneerselvam, K.; et al. Nonresponse to Acute Vasodilator Challenge and Prognosis in Heart Failure with Pulmonary Hypertension. J. Card. Fail. 2021, 27, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Bellettini, M.; Frea, S.; Pidello, S.; Boffini, M.; Boretto, P.; Gallone, G.; Bongiovanni, F.; Masetti, M.; Sabatino, M.; Raineri, C.; et al. Pretransplant Right Ventricular Dysfunction Is Associated with Increased Mortality after Heart Transplantation: A Hard Inheritance to Overcome. J. Card. Fail. 2022, 28, 259–269. [Google Scholar] [CrossRef] [PubMed]
- de Groote, P.; Delobelle, M.; Hebbar, E.; Mercier, T.; Fertin, M.; Goéminne, C.; Duva Pentiah, A.; Vincentelli, A.; Bauters, C.; Lamblin, N. Right Heart Catheterization in Advanced Systolic Heart Failure. What Are the Most Useful Haemodynamic Parameters for Risk Stratification? Arch. Cardiovasc. Dis. 2022, 115, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Benge, W.; Litchfield, R.L.; Marcus, M.L. Exercise Capacity in Patients with Severe Left Ventricular Dysfunction. Circulation 1980, 61, 955–959. [Google Scholar] [CrossRef]
- Mancini, D.M.; Eisen, H.; Kussmaul, W.; Mull, R.; Edmunds, L.H.; Wilson, J.R. Value of Peak Exercise Oxygen Consumption for Optimal Timing of Cardiac Transplantation in Ambulatory Patients with Heart Failure. Circulation 1991, 83, 778–786. [Google Scholar] [CrossRef]
- Deis, T.; Balling, L.; Rossing, K.; Wolsk, E.; Perch, M.; Gustafsson, F. Lung Diffusion Capacity in Advanced Heart Failure: Relation to Central Haemodynamics and Outcome. ESC Heart Fail. 2019, 6, 379–387. [Google Scholar] [CrossRef]
- Sutcliffe, P.D.; Aaronson, K.D.; Cody, R.J.; Koelling, T.M. Impact of Serial Changes in Cardiac Hemodynamics on Exercise Performance in Patients with Heart Failure Due to Ischemic and Nonischemic Cardiomyopathy. Am. J. Cardiol. 2003, 91, 164–168. [Google Scholar] [CrossRef]
- Barrett-O’Keefe, Z.; Lee, J.F.; Berbert, A.; Witman, M.A.H.; Nativi-Nicolau, J.; Stehlik, J.; Richardson, R.S.; Wray, D.W. Hemodynamic Responses to Small Muscle Mass Exercise in Heart Failure Patients with Reduced Ejection Fraction. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H1512–H1520. [Google Scholar] [CrossRef]
- Pugliese, N.R.; Fabiani, I.; Mandoli, G.E.; Guarini, G.; Galeotti, G.G.; Miccoli, M.; Lombardo, A.; Simioniuc, A.; Bigalli, G.; Pedrinelli, R.; et al. Echo-Derived Peak Cardiac Power Output-to-Left Ventricular Mass with Cardiopulmonary Exercise Testing Predicts Outcome in Patients with Heart Failure and Depressed Systolic Function. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Koshy, A.; Green, T.; Toms, A.; Cassidy, S.; Schueler, S.; Jakovljevic, D.; MacGowan, G.A. The Role of Exercise Hemodynamics in Assessing Patients with Chronic Heart Failure and Left Ventricular Assist Devices. Expert Rev. Med. Devices 2019, 16, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Berry, N.C.; Manyoo, A.; Oldham, W.M.; Stephens, T.E.; Goldstein, R.H.; Waxman, A.B.; Tracy, J.A.; Leary, P.J.; Leopold, J.A.; Kinlay, S.; et al. Protocol for Exercise Hemodynamic Assessment: Performing an Invasive Cardiopulmonary Exercise Test in Clinical Practice. Pulm. Circ. 2015, 5, 610–618. [Google Scholar] [CrossRef] [PubMed]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement from the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Kapur, N.K.; Esposito, M.L.; Bader, Y.; Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Burkhoff, D. Mechanical Circulatory Support Devices for Acute Right Ventricular Failure. Circulation 2017, 136, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Lala, A.; Guo, Y.; Xu, J.; Esposito, M.; Morine, K.; Karas, R.; Katz, S.D.; Hochman, J.S.; Burkhoff, D.; Kapur, N.K. Right Ventricular Dysfunction in Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Hemodynamic Analysis of the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) Trial and Registry. J. Card. Fail. 2018, 24, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Korabathina, R.; Heffernan, K.S.; Paruchuri, V.; Patel, A.R.; Mudd, J.O.; Prutkin, J.M.; Orr, N.M.; Weintraub, A.; Kimmelstiel, C.D.; Kapur, N.K. The Pulmonary Artery Pulsatility Index Identifies Severe Right Ventricular Dysfunction in Acute Inferior Myocardial Infarction. Catheter. Cardiovasc. Interv. 2012, 80, 593–600. [Google Scholar] [CrossRef]
- Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Paruchuri, V.; Denofrio, D.; Kapur, N.K. Pulmonary Artery Pulsatility Index Is Associated with Right Ventricular Failure after Left Ventricular Assist Device Surgery. J. Card. Fail. 2016, 22, 110–116. [Google Scholar] [CrossRef]
- Kang, G.; Ha, R.; Banerjee, D. Pulmonary Artery Pulsatility Index Predicts Right Ventricular Failure after Left Ventricular Assist Device Implantation. J. Heart Lung Transplant. 2017, 35, 67–73. [Google Scholar] [CrossRef]
- Kormos, R.L.; Teuteberg, J.J.; Pagani, F.D.; Russell, S.D.; John, R.; Miller, L.W.; Massey, T.; Milano, C.A.; Moazami, N.; Sundareswaran, K.S.; et al. Right Ventricular Failure in Patients with the HeartMate II Continuous-Flow Left Ventricular Assist Device: Incidence, Risk Factors, and Effect on Outcomes. J. Thorac. Cardiovasc. Surg. 2010, 139, 1316–1324. [Google Scholar] [CrossRef]
- Drakos, S.G.; Janicki, L.; Horne, B.D.; Kfoury, A.G.; Reid, B.B.; Clayson, S.; Horton, K.; Haddad, F.; Li, D.Y.; Renlund, D.G.; et al. Risk Factors Predictive of Right Ventricular Failure after Left Ventricular Assist Device Implantation. Am. J. Cardiol. 2010, 105, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Baumwol, J.; Macdonald, P.S.; Keogh, A.M.; Kotlyar, E.; Spratt, P.; Jansz, P.; Hayward, C.S. Right Heart Failure and “Failure to Thrive” after Left Ventricular Assist Device: Clinical Predictors and Outcomes. J. Heart Lung Transplant. 2011, 30, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Lietz, K.; Long, J.W.; Kfoury, A.G.; Slaughter, M.S.; Silver, M.A.; Milano, C.A.; Rogers, J.G.; Naka, Y.; Mancini, D.; Miller, L.W. Outcomes of Left Ventricular Assist Device Implantation as Destination Therapy in the Post-REMATCH Era: Implications for Patient Selection. Circulation 2007, 116, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Prestinenzi, P.; Potena, L. Right Heart Catheterization in Patients with Advanced Heart Failure: When to Perform? How to Interpret? Heart Fail. Clin. 2021, 17, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.O.; Stehlik, J.; Edwards, L.B.; Aurora, P.; Christie, J.D.; Dobbels, F.; Kirk, R.; Kucheryavaya, A.Y.; Rahmel, A.O.; Hertz, M.I. Registry of the International Society for Heart and Lung Transplantation: Twenty-Sixth Official Adult Heart Transplant Report-2009. J. Heart Lung Transplant. 2009, 28, 1007–1022. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Zuckermann, A.; Macdonald, P.; Leprince, P.; Esmailian, F.; Luu, M.; Mancini, D.; Patel, J.; Razi, R.; Reichenspurner, H.; et al. Report from a Consensus Conference on Primary Graft Dysfunction after Cardiac Transplantation. J. Heart Lung Transplant. 2014, 33, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Milligan, G.P.; Joseph, S.M. Reconsidering the Diagnostic Criteria of Right Ventricular Primary Graft Dysfunction. J. Card Fail. 2020, 26, 985–986. [Google Scholar] [CrossRef]
- Deng, M.C.; Eisen, H.J.; Mehra, M.R.; Billingham, M.; Marboe, C.C.; Berry, G.; Kobashigawa, J.; Johnson, F.L.; Starling, R.C.; Murali, S.; et al. Noninvasive Discrimination of Rejection in Cardiac Allograft Recipients Using Gene Expression Profiling. Am. J. Transplant. 2006, 6, 150–160. [Google Scholar] [CrossRef]
- Mehra, M.R.; Kobashigawa, J.; Starling, R.; Russell, S.; Uber, P.A.; Parameshwar, J.; Mohacsi, P.; Augustine, S.; Aaronson, K.; Barr, M. Listing Criteria for Heart Transplantation: International Society for Heart and Lung Transplantation Guidelines for the Care of Cardiac Transplant Candidates-2006. J. Heart Lung Transplant. 2006, 25, 1024–1042. [Google Scholar] [CrossRef]
- Frankfurter, C.; Molinero, M.; Vishram-Nielsen, J.K.K.; Foroutan, F.; Mak, S.; Rao, V.; Billia, F.; Orchanian-Cheff, A.; Alba, A.C. Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation: A Systematic Review. Circ. Heart Fail. 2020, 13, e006994. [Google Scholar] [CrossRef]
- Rajapreyar, I.; Soliman, O.; Brailovsky, Y.; Tedford, R.J.; Gibson, G.; Mohacsi, P.; Hajduczok, A.G.; Tchantchaleishvili, V.; Wieselthaler, G.; Rame, J.E.; et al. Late Right Heart Failure After Left Ventricular Assist Device Implantation: Contemporary Insights and Future Perspectives. JACC Heart Fail. 2023, 11, 865–878. [Google Scholar] [CrossRef] [PubMed]
- Dridi, N.P.; Vishram-Nielsen, J.K.K.; Gustafsson, F. Exercise Tolerance in Patients Treated with a Durable Left Ventricular Assist Device: Importance of Myocardial Recovery. J. Card. Fail. 2021, 27, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Bellavia, D.; Iacovoni, A.; Scardulla, C.; Moja, L.; Pilato, M.; Kushwaha, S.S.; Senni, M.; Clemenza, F.; Agnese, V.; Falletta, C.; et al. Prediction of Right Ventricular Failure after Ventricular Assist Device Implant: Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Heart Fail. 2017, 19, 926–946. [Google Scholar] [CrossRef] [PubMed]
- Kochav, S.M.; Flores, R.J.; Truby, L.K.; Topkara, V.K. Prognostic Impact of Pulmonary Artery Pulsatility Index (PAPi) in Patients with Advanced Heart Failure: Insights from the ESCAPE Trial. J. Card. Fail. 2018, 24, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Muslem, R.; Ong, C.S.; Tomashitis, B.; Schultz, J.; Ramu, B.; Craig, M.L.; Van Bakel, A.B.; Gilotra, N.A.; Sharma, K.; Hsu, S.; et al. Pulmonary Arterial Elastance and INTERMACS-Defined Right Heart Failure Following Left Ventricular Assist Device. Circ. Heart Fail. 2019, 12, e005923. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Sayer, G.; Addetia, K.; Fedson, S.; Kim, G.H.; Rodgers, D.; Kruse, E.; Collins, K.; Adatya, S.; Sarswat, N.; et al. Hemodynamic Ramp Tests in Patients with Left Ventricular Assist Devices. JACC Heart Fail. 2016, 4, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Morrison, K.A.; Garan, A.R.; Kato, T.S.; Yuzefpolskaya, M.; Latif, F.; Restaino, S.W.; Mancini, D.M.; Flannery, M.; Takayama, H.; et al. Development of a Novel Echocardiography Ramp Test for Speed Optimization and Diagnosis of Device Thrombosis in Continuous-Flow Left Ventricular Assist Devices: The Columbia Ramp Study. J. Am. Coll. Cardiol. 2012, 60, 1764–1775. [Google Scholar] [CrossRef]
- Imamura, T.; Jeevanandam, V.; Kim, G.; Raikhelkar, J.; Sarswat, N.; Kalantari, S.; Smith, B.; Rodgers, D.; Besser, S.; Chung, B.; et al. Optimal Hemodynamics During Left Ventricular Assist Device Support Are Associated with Reduced Readmission Rates. Circ. Heart Fail. 2019, 12, e005094. [Google Scholar] [CrossRef]
- Tehrani, D.M.; Grinstein, J.; Kalantari, S.; Kim, G.; Sarswat, N.; Adatya, S.; Sayer, G.; Uriel, N. Cardiac Output Assessment in Patients Supported with Left Ventricular Assist Device: Discordance Between Thermodilution and Indirect Fick Cardiac Output Measurements. ASAIO J. 2017, 63, 433–437. [Google Scholar] [CrossRef]
- Sayer, G.; Jeevanandam, V.; Ota, T.; Uriel, N. Invasive Hemodynamic Echocardiographic Ramp Test in the HeartAssist5 LVAD: Insights into Device Performance. ASAIO J. 2017, 63, e10–e12. [Google Scholar] [CrossRef]
- Imamura, T.; Chung, B.; Nguyen, A.; Sayer, G.; Uriel, N. Clinical Implications of Hemodynamic Assessment during Left Ventricular Assist Device Therapy. J. Cardiol. 2018, 71, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.H.; Hansen, P.B.; Sander, K.; Olsen, P.S.; Rossing, K.; Boesgaard, S.; Russell, S.D.; Gustafsson, F. Effect of Increasing Pump Speed during Exercise on Peak Oxygen Uptake in Heart Failure Patients Supported with a Continuous-Flow Left Ventricular Assist Device. A Double-Blind Randomized Study. Eur. J. Heart Fail. 2014, 16, 403–408. [Google Scholar] [CrossRef] [PubMed]
- McDiarmid, A.; Gordon, B.; Wrightson, N.; Robinson-Smith, N.; Pillay, T.; Parry, G.; Schueler, S.; MacGowan, G.A. Hemodynamic, Echocardiographic, and Exercise-Related Effects of the HeartWare Left Ventricular Assist Device in Advanced Heart Failure. Congest. Heart Fail. 2013, 19, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Martina, J.; de Jonge, N.; Rutten, M.; Kirkels, J.H.; Klöpping, C.; Rodermans, B.; Sukkel, E.; Hulstein, N.; Mol, B.; Lahpor, J. Exercise Hemodynamics during Extended Continuous Flow Left Ventricular Assist Device Support: The Response of Systemic Cardiovascular Parameters and Pump Performance. Artif. Organs 2013, 37, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.V.; Muthiah, K.; Robson, D.; Prichard, R.; Walker, R.; Pin Lim, C.; Wang, L.W.; Macdonald, P.S.; Jansz, P.; Hayward, C.S. Impact of Pump Speed on Hemodynamics with Exercise in Continuous Flow Ventricular Assist Device Patients. ASAIO J. 2020, 66, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Brassard, P.; Jensen, A.S.; Nordsborg, N.; Gustafsson, F.; Møller, J.E.; Hassager, C.; Boesgaard, S.; Hansen, P.B.; Olsen, P.S.; Sander, K.; et al. Central and Peripheral Blood Flow during Exercise with a Continuous-Flow Left Ventricular Assist Device: Constant versus Increasing Pump Speed: A Pilot Study. Circ. Heart Fail. 2011, 4, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Chioncel, O.; Mebazaa, A.; Maggioni, A.P.; Harjola, V.-P.; Rosano, G.; Laroche, C.; Piepoli, M.F.; Crespo-Leiro, M.G.; Lainscak, M.; Ponikowski, P.; et al. Acute Heart Failure Congestion and Perfusion Status—Impact of the Clinical Classification on in-Hospital and Long-Term Outcomes; Insights from the ESC-EORP-HFA Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2019, 21, 1338–1352. [Google Scholar] [CrossRef]
- Miró, Ò.; García Sarasola, A.; Fuenzalida, C.; Calderón, S.; Jacob, J.; Aguirre, A.; Wu, D.M.; Rizzi, M.A.; Malchair, P.; Haro, A.; et al. Departments Involved during the First Episode of Acute Heart Failure and Subsequent Emergency Department Revisits and Rehospitalisations: An Outlook through the NOVICA Cohort. Eur. J. Heart Fail. 2019, 21, 1231–1244. [Google Scholar] [CrossRef]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.-P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A Survey on Hospitalized Acute Heart Failure Patients: Description of Population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) With the Special Contribution of the Heart Failure Association (HFA) of the ESC. Rev. Esp. Cardiol. 2022, 75, 523. [Google Scholar] [CrossRef]
- Chioncel, O.; Mebazaa, A.; Harjola, V.-P.; Coats, A.J.; Piepoli, M.F.; Crespo-Leiro, M.G.; Laroche, C.; Seferovic, P.M.; Anker, S.D.; Ferrari, R.; et al. Clinical Phenotypes and Outcome of Patients Hospitalized for Acute Heart Failure: The ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1242–1254. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.R.; Hasselblad, V.; Stevenson, L.W.; Binanay, C.; O’Connor, C.M.; Sopko, G.; Califf, R.M. Impact of the Pulmonary Artery Catheter in Critically Ill Patients: Meta-Analysis of Randomized Clinical Trials. JAMA 2005, 294, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, G.A.; Lemor, A.; Blumer, V.; Rueda, C.A.; Zalawadiya, S.; Stevenson, L.W.; Lindenfeld, J. Trends in Utilization and Outcomes of Pulmonary Artery Catheterization in Heart Failure with and without Cardiogenic Shock. J. Card. Fail. 2019, 25, 364–371. [Google Scholar] [CrossRef] [PubMed]
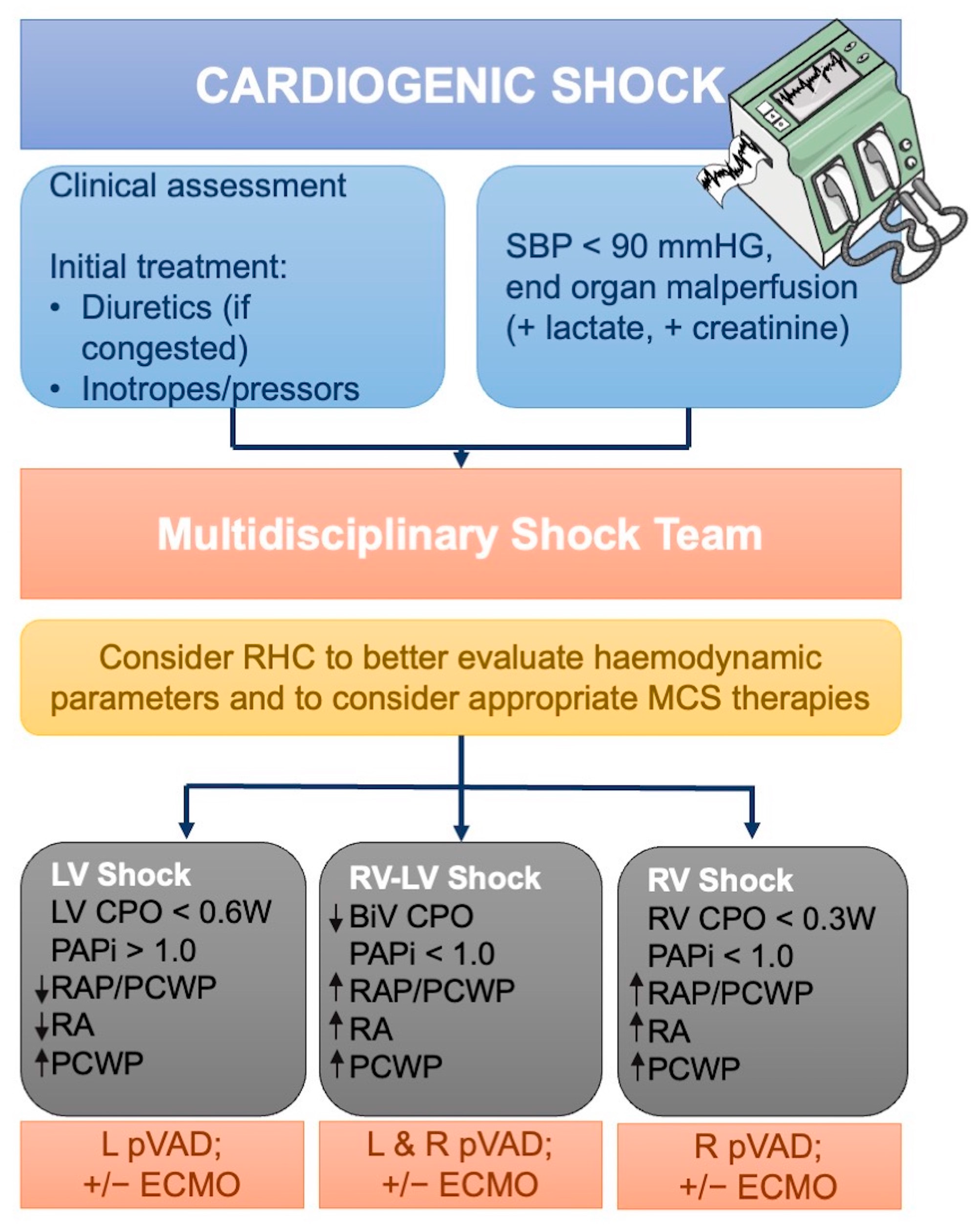
- Chioncel, O.; Parissis, J.; Mebazaa, A.; Thiele, H.; Desch, S.; Bauersachs, J.; Harjola, V.-P.; Antohi, E.-L.; Arrigo, M.; Ben Gal, T.; et al. Epidemiology, Pathophysiology and Contemporary Management of Cardiogenic Shock—A Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1315–1341. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; de Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of Cardiogenic Shock Complicating Myocardial Infarction: An Update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Combes, A.; van Diepen, S.; Hollinger, A.; Katz, J.N.; Landoni, G.; Hajjar, L.A.; Lassus, J.; Lebreton, G.; Montalescot, G.; et al. Management of Cardiogenic Shock Complicating Myocardial Infarction. Intensive Care Med. 2018, 44, 760–773. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.D.; Bohula, E.A.; van Diepen, S.; Katz, J.N.; Alviar, C.L.; Baird-Zars, V.M.; Barnett, C.F.; Barsness, G.W.; Burke, J.A.; Cremer, P.C.; et al. Epidemiology of Shock in Contemporary Cardiac Intensive Care Units. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005618. [Google Scholar] [CrossRef]
- Aissaoui, N.; Puymirat, E.; Tabone, X.; Charbonnier, B.; Schiele, F.; Lefèvre, T.; Durand, E.; Blanchard, D.; Simon, T.; Cambou, J.-P.; et al. Improved Outcome of Cardiogenic Shock at the Acute Stage of Myocardial Infarction: A Report from the USIK 1995, USIC 2000, and FAST-MI French Nationwide Registries. Eur. Heart J. 2012, 33, 2535–2543. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation: The Task Force for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Jentzer, J.C.; van Diepen, S.; Barsness, G.W.; Henry, T.D.; Menon, V.; Rihal, C.S.; Naidu, S.S.; Baran, D.A. Cardiogenic Shock Classification to Predict Mortality in the Cardiac Intensive Care Unit. J. Am. Coll. Cardiol. 2019, 74, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Iannaccone, M.; Albani, S.; Giannini, F.; Colangelo, S.; Boccuzzi, G.G.; Garbo, R.; Brilakis, E.S.; D’ascenzo, F.; de Ferrari, G.M.; Colombo, A. Short Term Outcomes of Impella in Cardiogenic Shock: A Review and Meta-Analysis of Observational Studies. Int. J. Cardiol. 2021, 324, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Bertaina, M.; Ferraro, I.; Omedè, P.; Conrotto, F.; Saint-Hilary, G.; Cavender, M.A.; Claessen, B.E.; Henriques, J.P.S.; Frea, S.; Usmiani, T.; et al. Meta-Analysis Comparing Complete or Culprit Only Revascularization in Patients with Multivessel Disease Presenting with Cardiogenic Shock. Am. J. Cardiol. 2018, 122, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Bueno, H.; Granger, C.B.; Hochman, J.; Huber, K.; Lettino, M.; Price, S.; Schiele, F.; Tubaro, M.; Vranckx, P.; et al. Acute Cardiovascular Care Association Position Statement for the Diagnosis and Treatment of Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Document of the Acute Cardiovascular Care Association of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 183–197. [Google Scholar] [CrossRef]
- Jentzer, J.C.; Wiley, B.M.; Anavekar, N.S.; Pislaru, S.V.; Mankad, S.V.; Bennett, C.E.; Barsness, G.W.; Hollenberg, S.M.; Holmes, D.R.; Oh, J.K. Noninvasive Hemodynamic Assessment of Shock Severity and Mortality Risk Prediction in the Cardiac Intensive Care Unit. JACC Cardiovasc. Imaging 2021, 14, 321–332. [Google Scholar] [CrossRef]
- Suess, E.M.; Pinsky, M.R. Hemodynamic Monitoring for the Evaluation and Treatment of Shock: What Is the Current State of the Art? Semin. Respir. Crit. Care Med. 2015, 36, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI Clinical Expert Consensus Statement on the Classification of Cardiogenic Shock: This Document Was Endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter. Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar] [CrossRef]
- Forrester, J.S.; Diamond, G.; Chatterjee, K.; Swan, H.J. Medical Therapy of Acute Myocardial Infarction by Application of Hemodynamic Subsets (First of Two Parts). N. Engl. J. Med. 1976, 295, 1356–1362. [Google Scholar] [CrossRef]
- Kohsaka, S.; Menon, V.; Lowe, A.M.; Lange, M.; Dzavik, V.; Sleeper, L.A.; Hochman, J.S.; SHOCK Investigators. Systemic Inflammatory Response Syndrome after Acute Myocardial Infarction Complicated by Cardiogenic Shock. Arch. Intern. Med. 2005, 165, 1643–1650. [Google Scholar] [CrossRef]
- Sorajja, P.; Borlaug, B.A.; Dimas, V.V.; Fang, J.C.; Forfia, P.R.; Givertz, M.M.; Kapur, N.K.; Kern, M.J.; Naidu, S.S. SCAI/HFSA Clinical Expert Consensus Document on the Use of Invasive Hemodynamics for the Diagnosis and Management of Cardiovascular Disease. Catheter. Cardiovasc. Interv. 2017, 89, E233–E247. [Google Scholar] [CrossRef]
- Jacobs, A.K.; Leopold, J.A.; Bates, E.; Mendes, L.A.; Sleeper, L.A.; White, H.; Davidoff, R.; Boland, J.; Modur, S.; Forman, R.; et al. Cardiogenic Shock Caused by Right Ventricular Infarction: A Report from the SHOCK Registry. J. Am. Coll. Cardiol. 2003, 41, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Brodie, B.R.; Stuckey, T.D.; Hansen, C.; Bradshaw, B.H.; Downey, W.E.; Pulsipher, M.W. Comparison of Late Survival in Patients with Cardiogenic Shock due to Right Ventricular Infarction versus Left Ventricular Pump Failure Following Primary Percutaneous Coronary Intervention for ST-Elevation Acute Myocardial Infarction. Am. J. Cardiol. 2007, 99, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Miranda, C.Y.; Hall, S.A. Cardiogenic Shock in Patients with Advanced Chronic Heart Failure. Methodist DeBakey Cardiovasc. J. 2020, 16, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Mimoz, O.; Rauss, A.; Rekik, N.; Brun-Buisson, C.; Lemaire, F.; Brochard, L. Pulmonary Artery Catheterization in Critically Ill Patients: A Prospective Analysis of Outcome Changes Associated with Catheter-Prompted Changes in Therapy. Crit. Care Med. 1994, 22, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Ranka, S.; Mastoris, I.; Kapur, N.K.; Tedford, R.J.; Rali, A.; Acharya, P.; Weidling, R.; Goyal, A.; Sauer, A.J.; Gupta, B.; et al. Right Heart Catheterization in Cardiogenic Shock Is Associated with Improved Outcomes: Insights from the Nationwide Readmissions Database. J. Am. Heart Assoc. 2021, 10, e019843. [Google Scholar] [CrossRef] [PubMed]
- Osman, M.; Syed, M.; Patel, B.; Munir, M.B.; Kheiri, B.; Caccamo, M.; Sokos, G.; Balla, S.; Basir, M.B.; Kapur, N.K.; et al. Invasive Hemodynamic Monitoring in Cardiogenic Shock Is Associated with Lower In-Hospital Mortality. J. Am. Heart Assoc. 2021, 10, e021808. [Google Scholar] [CrossRef] [PubMed]
- Burkhoff, D.; Sayer, G.; Doshi, D.; Uriel, N. Hemodynamics of Mechanical Circulatory Support. J. Am. Coll. Cardiol. 2015, 66, 2663–2674. [Google Scholar] [CrossRef]
- Basir, M.B.; Kapur, N.K.; Patel, K.; Salam, M.A.; Schreiber, T.; Kaki, A.; Hanson, I.; Almany, S.; Timmis, S.; Dixon, S.; et al. Improved Outcomes Associated with the Use of Shock Protocols: Updates from the National Cardiogenic Shock Initiative. Catheter. Cardiovasc. Interv. 2019, 93, 1173–1183. [Google Scholar] [CrossRef]
- Osman, M.; Balla, S.; Dupont, A.; O’Neill, W.W.; Basir, M.B. Reviving Invasive Hemodynamic Monitoring in Cardiogenic Shock. Invasive Hemodynamic Monitoring in Cardiogenic Shock. Am. J. Cardiol. 2021, 150, 128–129. [Google Scholar] [CrossRef]
- Fincke, R.; Hochman, J.S.; Lowe, A.M.; Menon, V.; Slater, J.N.; Webb, J.G.; LeJemtel, T.H.; Cotter, G.; SHOCK Investigators. Cardiac Power Is the Strongest Hemodynamic Correlate of Mortality in Cardiogenic Shock: A Report from the SHOCK Trial Registry. J. Am. Coll. Cardiol. 2004, 44, 340–348. [Google Scholar] [CrossRef]
- Morrow, D.A.; Antman, E.M.; Charlesworth, A.; Cairns, R.; Murphy, S.A.; de Lemos, J.A.; Giugliano, R.P.; McCabe, C.H.; Braunwald, E. TIMI Risk Score for ST-Elevation Myocardial Infarction: A Convenient, Bedside, Clinical Score for Risk Assessment at Presentation: An Intravenous NPA for Treatment of Infarcting Myocardium Early II Trial Substudy. Circulation 2000, 102, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.S.; Paniagua, D.; Denktas, A.E.; Jneid, H.; Kar, B.; Chan, W.; Bozkurt, B. Usefulness of the Sum of Pulmonary Capillary Wedge Pressure and Right Atrial Pressure as a Congestion Index That Prognosticates Heart Failure Survival (from the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness Trial). Am. J. Cardiol. 2016, 118, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Garan, A.R.; Kanwar, M.; Thayer, K.L.; Whitehead, E.; Zweck, E.; Hernandez-Montfort, J.; Mahr, C.; Haywood, J.L.; Harwani, N.M.; Wencker, D.; et al. Complete Hemodynamic Profiling with Pulmonary Artery Catheters in Cardiogenic Shock Is Associated with Lower In-Hospital Mortality. JACC Heart Fail. 2020, 8, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Vila, M.; Rivas-Lasarte, M.; Ferrero-Gregori, A.; Sans-Roselló, J.; Duran-Cambra, A.; Sionis, A. Impact of Pulmonary Artery Catheter Use on Short- and Long-Term Mortality in Patients with Cardiogenic Shock. Cardiology 2017, 136, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Sionis, A.; Rivas-Lasarte, M.; Mebazaa, A.; Tarvasmäki, T.; Sans-Roselló, J.; Tolppanen, H.; Varpula, M.; Jurkko, R.; Banaszewski, M.; Silva-Cardoso, J.; et al. Current Use and Impact on 30-Day Mortality of Pulmonary Artery Catheter in Cardiogenic Shock Patients: Results from the CardShock Study. J. Intensive Care Med. 2020, 35, 1426–1433. [Google Scholar] [CrossRef]
- Hsu, S.; Kambhampati, S.; Sciortino, C.M.; Russell, S.D.; Schulman, S.P. Predictors of Intra-Aortic Balloon Pump Hemodynamic Failure in Non-Acute Myocardial Infarction Cardiogenic Shock. Am. Heart J. 2018, 199, 181–191. [Google Scholar] [CrossRef]
- Sintek, M.A.; Gdowski, M.; Lindman, B.R.; Nassif, M.; Lavine, K.J.; Novak, E.; Bach, R.G.; Silvestry, S.C.; Mann, D.L.; Joseph, S.M. Intra-Aortic Balloon Counterpulsation in Patients with Chronic Heart Failure and Cardiogenic Shock: Clinical Response and Predictors of Stabilization. J. Card Fail. 2015, 21, 868–876. [Google Scholar] [CrossRef]
- O’Neill, W.W.; Grines, C.; Schreiber, T.; Moses, J.; Maini, B.; Dixon, S.R.; Ohman, E.M. Analysis of Outcomes for 15,259 US Patients with Acute Myocardial Infarction Cardiogenic Shock (AMICS) Supported with the Impella Device. Am. Heart J. 2018, 202, 33–38. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
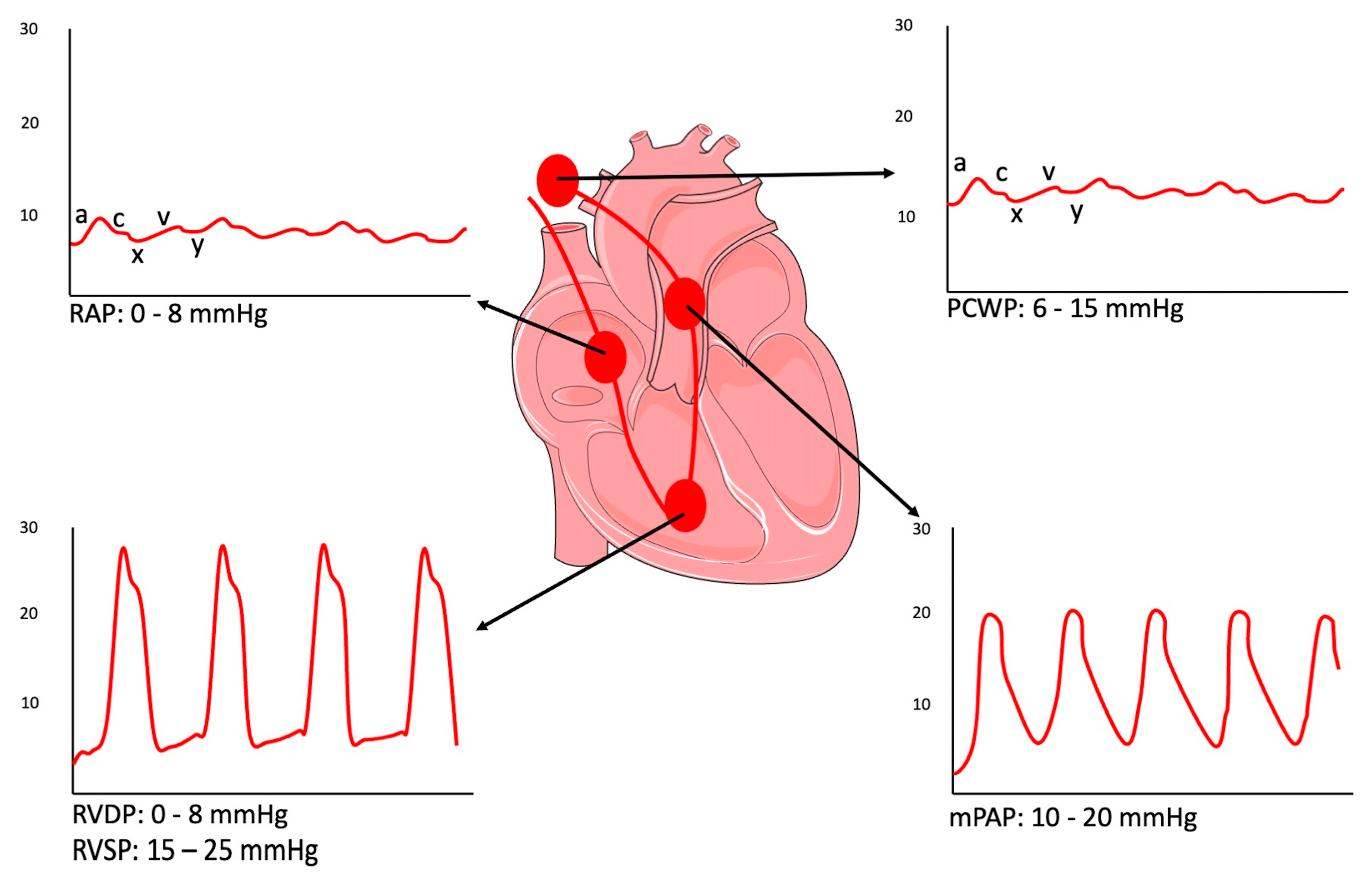
| HEMODYNAMIC PARAMETERS | NORMAL RANGE |
|---|---|
| Central venous pressure (CVP) | 2–6 mmHg |
| Right atrial pressure (RAP) | 0–8 mmHg |
| Right ventricular systolic pressure (RVSP) | 15–25 mmHg |
| Right ventricular diastolic pressure (RVDP) | 0–8 mmHg |
| Pulmonary artery systolic/diastolic pressure (PASP/PADP) | 15–25 mmHg; 8–15 mmHg |
| Mean pulmonary artery pressure (mPAP: PADP + [PASP − PADP/3]) | 10–20 mmHg |
| Pulmonary capillary wedge pressure (PCWP) | 6–15 mmHg |
| Diastolic pulmonary gradient (DPG: PADP − PCWP) | <7 mmHg |
| PAPi ([PASP − PADP]/RAP) | >2 |
| Transpulmonary gradient (TPG: mPAP − PCWP) | <12 mmHg |
| Mean systemic arterial pressure (mSAP: DBP + 1/3[SBP − DBP]) | 65–110 mmHg |
| Cardiac output (CO) | 4–8 L/min |
| Cardiac index (CI: CO/BSA) | 2.5–4 L/min/m2 |
| Stroke volume (SV) | 60–100 mL/beat |
| Stroke volume index (SVI: SV/BSA) | 33–47 mL/m2/beat |
| Systemic vascular resistance (SVR: [mSAP − RAP]/CO × 80) | 700–1600 dyn·s/cm5 |
| SVR index (SVRI: SVR/CI) | 1330–3040 dyn·s/cm5·m2 |
| Pulmonary vascular resistance (PVR: [mPAP − PCWP]/CO × 80) | 20–120 dyn·s/cm5 |
| PVR index (PVRI: PVR/CI) | 38–228 dyn·s/cm5·m2 |
| H2FPEF | ||
|---|---|---|
| Clinical Variable | Values | Pts |
| H—Heavy | BMI > 30 Kg/m2 | 2 |
| H—Hypertensive | ≥2 antihypertensive drugs | 1 |
| F—Atrial Fibrillation | Paroxysmal or Persistent | 3 |
| P—Pulmonary hypertension | * sPAP > 35 mmHG | 1 |
| E—Elder | Age > 60 years | 1 |
| F—Filling pressure | * E/e′ > 9 | 1 |
| Clinical Scenario | Application | Parameters |
|---|---|---|
| Acute decompensated HF |
| CI, CPO, CO, mPAP, PCWP, RAP, sVO2, TPG |
| Heart Transplant eligibility |
| CI, CO, mPAP, PAC, PAPi, sPAP, PVR, RAP, TPG |
| Post-Heart Transplant Evaluation |
| CI, sPAP, PCWP, PVR, RAP, TPG |
| VAD candidacy |
| CI, CPO, CO, mPAP, PAPi, PCWP, RAP, RVSWI, sVO2, TPG |
| Post-VAD Evaluation |
| CI, CPO, CO, mPAP, PAC, PAPi, PCWP, PVR, RAP, sVO2, TPG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manzi, L.; Sperandeo, L.; Forzano, I.; Castiello, D.S.; Florimonte, D.; Paolillo, R.; Santoro, C.; Mancusi, C.; Di Serafino, L.; Esposito, G.; et al. Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure. Diagnostics 2024, 14, 136. https://doi.org/10.3390/diagnostics14020136
Manzi L, Sperandeo L, Forzano I, Castiello DS, Florimonte D, Paolillo R, Santoro C, Mancusi C, Di Serafino L, Esposito G, et al. Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure. Diagnostics. 2024; 14(2):136. https://doi.org/10.3390/diagnostics14020136
Chicago/Turabian StyleManzi, Lina, Luca Sperandeo, Imma Forzano, Domenico Simone Castiello, Domenico Florimonte, Roberta Paolillo, Ciro Santoro, Costantino Mancusi, Luigi Di Serafino, Giovanni Esposito, and et al. 2024. "Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure" Diagnostics 14, no. 2: 136. https://doi.org/10.3390/diagnostics14020136