


Real-Life Assessment of the Ability of an Ultraviolet C Lamp (SanificaAria 200, Beghelli) to Inactivate Airborne Microorganisms in a Healthcare Environment
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sanitation Device
2.2. Air Samplers
2.3. Sampling Settings
2.4. Sample Analysis
3. Results
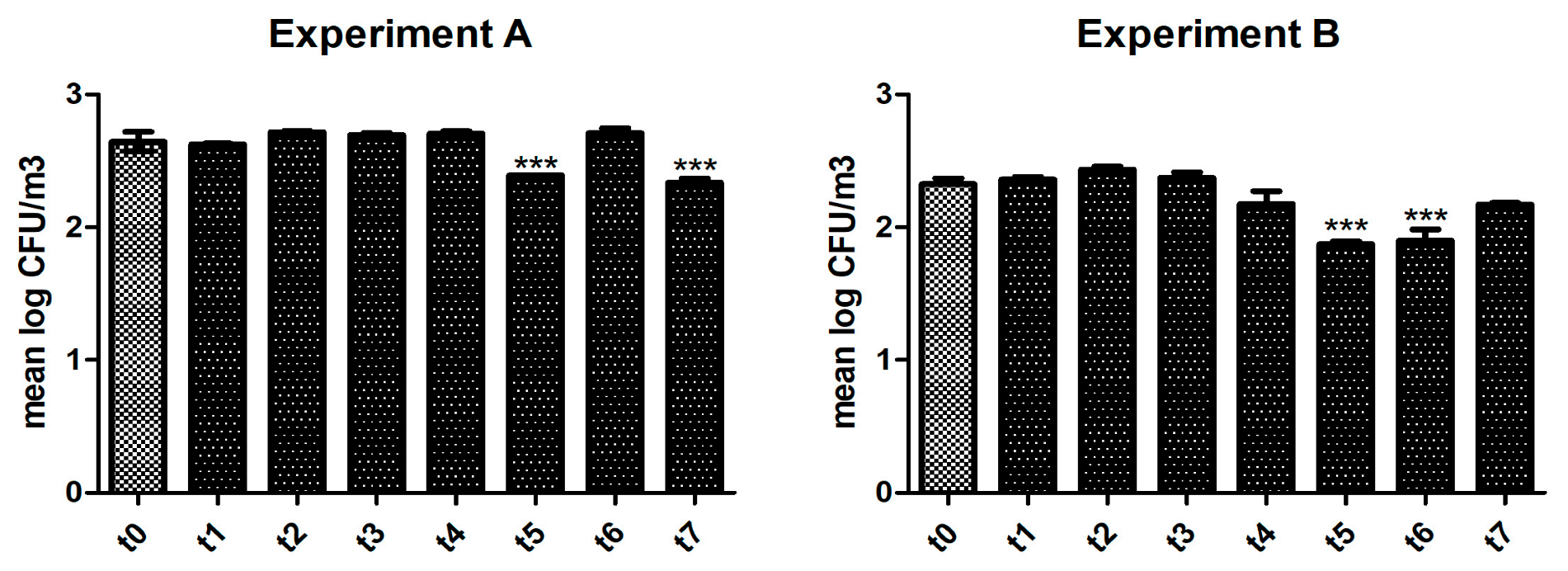
3.1. Activity of the UVC Device in Reducing Bacterial Levels
3.2. Antiviral Activity of the UVC Device
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wyon, D.P. The effects of indoor air quality on performance and productivity. Indoor Air 2004, 14, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Welch, D.; Buonanno, M.; Grilj, V.; Shuryak, I.; Crickmore, C.; Bigelow, A.W.; Randers-Pehrson, G.; Johnson, G.W.; Brenner, D.J. Far-UVC light: A new tool to control the spread of airborne-mediated microbial diseases. Sci. Rep. 2018, 8, 2752, Erratum in Sci. Rep. 2021, 11, 18122. [Google Scholar] [CrossRef]
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544, Erratum in Lancet 2017, 389, e1. [Google Scholar]
- Vardakas, K.Z.; Rafailidis, P.I.; Konstantelias, A.A.; Falagas, M.E. Predictors of mortality in patients with infections due to multi-drug resistant Gram negative bacteria: The study, the patient, the bug or the drug? J. Infect. 2013, 66, 401–414. [Google Scholar] [CrossRef]
- Bridges, C.B.; Kuehnert, M.J.; Hall, C.B. Transmission of influenza: Implications for control in health care settings. Clin. Infect. Dis. 2003, 37, 1094–1101. [Google Scholar]
- Bale, R.; Iida, A.; Yamakawa, M.; Li, C.; Tsubokura, M. Quantifying the COVID-19 infection risk due to droplet/aerosol inhalation. Sci. Rep. 2022, 12, 11186. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob. Resist. Infect. Control 2016, 5, 10. [Google Scholar] [CrossRef]
- Katara, G.; Hemvani, N.; Chitnis, S.; Chitnis, V.; Chitnis, D.S. Surface disinfection by exposure to germicidal UV light. Indian J. Med. Microbiol. 2008, 26, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Conner-Kerr, T.A.; Sullivan, P.K.; Gaillard, J.; Franklin, M.E.; Jones, R.M. The effects of ultraviolet radiation on antibiotic-resistant bacteria in vitro. Ostomy/Wound Manag. 1998, 44, 50–56. [Google Scholar]
- Budowsky, E.I.; Bresler, S.E.; Friedman, E.A.; Zheleznova, N.V. Principles of selective inactivation of viral genome. I. UV-induced inactivation of influenza virus. Arch. Virol. 1981, 68, 239–247. [Google Scholar] [CrossRef]
- Gurzadyan, G.G.; Görner, H.; Schulte-Frohlinde, D. Ultraviolet (193, 216 and 254 nm) photoinactivation of Escherichia coli strains with different repair deficiencies. Radiat. Res. 1995, 141, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Memarzadeh, F.; Olmsted, R.N.; Bartley, J.M. Applications of ultraviolet germicidal irradiation disinfection in health care facilities: Effective adjunct, but not stand-alone technology. Am. J. Infect. Control 2010, 38, S13–S24. [Google Scholar] [CrossRef] [PubMed]
- Setlow, P. Spores of Bacillus subtilis: Their resistance and to killing by radiation, heat and chemicals. J. Appl. Microbiol. 2006, 101, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, W.G.; McClelland, T.L.; Neu, D.T.; Martin, S.B., Jr.; Mead, K.R.; Thewlis, R.E.; Noti, J.D. Ambulance disinfection using Ultraviolet Germicidal Irradiation (UVGI): Effects of fixture location and surface reflectivity. J. Occup. Environ. Hyg. 2018, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Narita, K.; Asano, K.; Naito, K.; Ohashi, H.; Sasaki, M.; Morimoto, Y.; Igarashi, A.; Nakane, A. Ultraviolet C light with wavelength of 222 nm inactivates a wide spectrum of microbial pathogens. J. Hosp. Infect. 2020, 105, 459–467. [Google Scholar] [CrossRef]
- Szeto, W.; Yam, W.C.; Huang, H.; Leung, D.Y.C. The efficacy of vacuum-ultraviolet light disinfection of some common environmental pathogens. BMC Infect. Dis. 2020, 20, 127. [Google Scholar] [CrossRef]
- Eadie, E.; Hiwar, W.; Fletcher, L.; Tidswell, E.; O’Mahoney, P.; Buonanno, M.; Welch, D.; Adamson, C.S.; Brenner, D.J.; Noakes, C.; et al. Far-UVC (222 nm) efficiently inactivates an airborne pathogen in a room-sized chamber. Sci. Rep. 2022, 12, 4373. [Google Scholar] [CrossRef]
- Foschi, C.; Laghi, L.; Parolin, C.; Giordani, B.; Compri, M.; Cevenini, R.; Marangoni, A.; Vitali, B. Novel approaches for the taxonomic and metabolic characterization of lactobacilli: Integration of 16S rRNA gene sequencing with MALDI-TOF MS and 1H-NMR. PLoS ONE 2017, 12, e0172483. [Google Scholar] [CrossRef] [PubMed]
- Ouafi, M.; Dubos, F.; Engelman, I.; Lazrek, M.; Guigon, A.; Bocket, L.; Hober, D.; Alidjinou, E.K. Rapid syndromic testing for respiratory viral infections in children attending the emergency department during COVID-19 pandemic in Lille, France, 2021–2022. J. Clin. Virol. 2022, 153, 105221. [Google Scholar] [CrossRef]
- Choi, H.; Ahn, H.; Lee, R.; Cho, S.Y.; Lee, D.G. Bloodstream Infections in Patients with Hematologic Diseases: Causative Organisms and Factors Associated with Resistance. Infect. Chemother. 2022, 54, 340–352. [Google Scholar] [CrossRef]
- Burastero, G.J.; Orlando, G.; Santoro, A.; Menozzi, M.; Franceschini, E.; Bedini, A.; Cervo, A.; Faltoni, M.; Bacca, E.; Biagioni, E.; et al. Ceftazidime/Avibactam in Ventilator-Associated Pneumonia Due to Difficult-to-Treat Non-Fermenter Gram-Negative Bacteria in COVID-19 Patients: A Case Series and Review of the Literature. Antibiotics 2022, 11, 1007. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Doyle, T.B.; Hubler, C.M.; Collingsworth, T.D.; DeVries, S.; Mendes, R.E. The Plethora of Resistance Mechanisms in Pseudomonas aeruginosa: Transcriptome Analysis Reveals a Potential Role of Lipopolysaccharide Pathway Proteins to Novel β-lactam/β-lactamase Inhibitor Combinations. J. Glob. Antimicrob. Resist. 2022, 31, 72–79. [Google Scholar] [CrossRef]
- Akinduti, P.A.; Obafemi, Y.D.; Ugboko, H.; El-Ashker, M.; Akinnola, O.; Agunsoye, C.J.; Oladotun, A.; Phiri, B.S.J.; Oranusi, S.U. Emerging vancomycin-non susceptible coagulase negative Staphylococci associated with skin and soft tissue infections. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 31. [Google Scholar] [CrossRef] [PubMed]
- Badescu, B.; Buda, V.; Romanescu, M.; Lombrea, A.; Danciu, C.; Dalleur, O.; Dohou, A.M.; Dumitrascu, V.; Cretu, O.; Licker, M.; et al. Current State of Knowledge Regarding WHO Critical Priority Pathogens: Mechanisms of Resistance and Proposed Solutions through Candidates Such as Essential Oils. Plants 2022, 11, 1789. [Google Scholar] [CrossRef]
- Esmkhani, M.; Shams, S. Cutaneous infection due to Bacillus cereus: A case report. BMC Infect. Dis. 2022, 22, 393. [Google Scholar] [CrossRef]
- Foschi, C.; Zignoli, A.; Gaibani, P.; Vocale, C.; Rossini, G.; Lafratta, S.; Liberatore, A.; Turello, G.; Lazzarotto, T.; Ambretti, S. Respiratory bacterial co-infections in intensive care unit-hospitalized COVID-19 patients: Conventional culture vs BioFire FilmArray pneumonia Plus panel. J. Microbiol. Methods 2021, 186, 106259. [Google Scholar] [CrossRef]
- Buonanno, M.; Welch, D.; Shuryak, I.; Brenner, D.J. Far-UVC light (222 nm) efficiently and safely inactivates airborne human coronaviruses. Sci. Rep. 2020, 10, 10285, Erratum in Sci. Rep. 2021, 11, 19569. [Google Scholar] [CrossRef] [PubMed]
- Diab-El Schahawi, M.; Zingg, W.; Vos, M.; Humphreys, H.; Lopez-Cerero, L.; Fueszl, A.; Zahar, J.R.; Presterl, E.; ESCMID Study Group on Nosocomial Infections “The decontamination research working group”. Ultraviolet disinfection robots to improve hospital cleaning: Real promise or just a gimmick? Antimicrob. Resist. Infect. Control 2021, 10, 33. [Google Scholar] [CrossRef]
- Chiappa, F.; Frascella, B.; Vigezzi, G.P.; Moro, M.; Diamanti, L.; Gentile, L.; Lago, P.; Clementi, N.; Signorelli, C.; Mancini, N.; et al. The efficacy of ultraviolet light-emitting technology against coronaviruses: A systematic review. J. Hosp. Infect. 2021, 114, 63–78. [Google Scholar] [CrossRef]


{kind=link}
| Bacteria Identified in Preliminary Sampling (No Activity on the Device) | Bacteria Identified after Switching on the Sanitizer for 5 h | Bacteria Identified after Switching on the Sanitizer for 24 h |
|---|---|---|
| Bacillus cereus | - | - |
| Bacillus licheneformis | - | - |
| Micrococcus luteus | Micrococcus luteus | Micrococcus luteus |
| Staphylococcus capitis | - | - |
| Staphylococcus epidermidis | Staphylococcus epidermidis | Staphylococcus epidermidis |
| Staphylococcus haemolyticus | Staphylococcus haemolyticus | Staphylococcus haemolyticus |
| Staphylococcus hominis | Staphylococcus hominis | Staphylococcus hominis |
| Bacteria Identified in Preliminary Sampling (no Activity of the Device) | Bacteria Identified after Switching on the Sanitizer for 6 h |
|---|---|
| Acinetobacter lwoffii | Acinetobacter lwoffii |
| Bacillus badius | - |
| - | Bacillus megaterium |
| - | Bacillus simplex |
| Corynebacterium afermentans | - |
| - | Klebsiella pneumoniae |
| - | Kocuria rizhophila |
| Micrococcus lylae | - |
| Micrococcus luteus | Micrococcus luteus |
| Moraxella osloensis | Moraxella osloensis |
| Pseudomonas aeruginosa | - |
| Staphylococcus epidermidis | - |
| Staphylococcus haemolyticus | Staphylococcus haemolyticus |
| Staphylococcus hominis | Staphylococcus hominis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foschi, C.; Giorgi, B.; Ambretti, S.; Lazzarotto, T.; Violante, F.S. Real-Life Assessment of the Ability of an Ultraviolet C Lamp (SanificaAria 200, Beghelli) to Inactivate Airborne Microorganisms in a Healthcare Environment. Life 2023, 13, 1221. https://doi.org/10.3390/life13051221
Foschi C, Giorgi B, Ambretti S, Lazzarotto T, Violante FS. Real-Life Assessment of the Ability of an Ultraviolet C Lamp (SanificaAria 200, Beghelli) to Inactivate Airborne Microorganisms in a Healthcare Environment. Life. 2023; 13(5):1221. https://doi.org/10.3390/life13051221
Chicago/Turabian StyleFoschi, Claudio, Beatrice Giorgi, Simone Ambretti, Tiziana Lazzarotto, and Francesco Saverio Violante. 2023. "Real-Life Assessment of the Ability of an Ultraviolet C Lamp (SanificaAria 200, Beghelli) to Inactivate Airborne Microorganisms in a Healthcare Environment" Life 13, no. 5: 1221. https://doi.org/10.3390/life13051221