
Cancer Therapy-Related Cardiac Dysfunction in Patients Treated with a Combination of an Immune Checkpoint Inhibitor and Doxorubicin

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
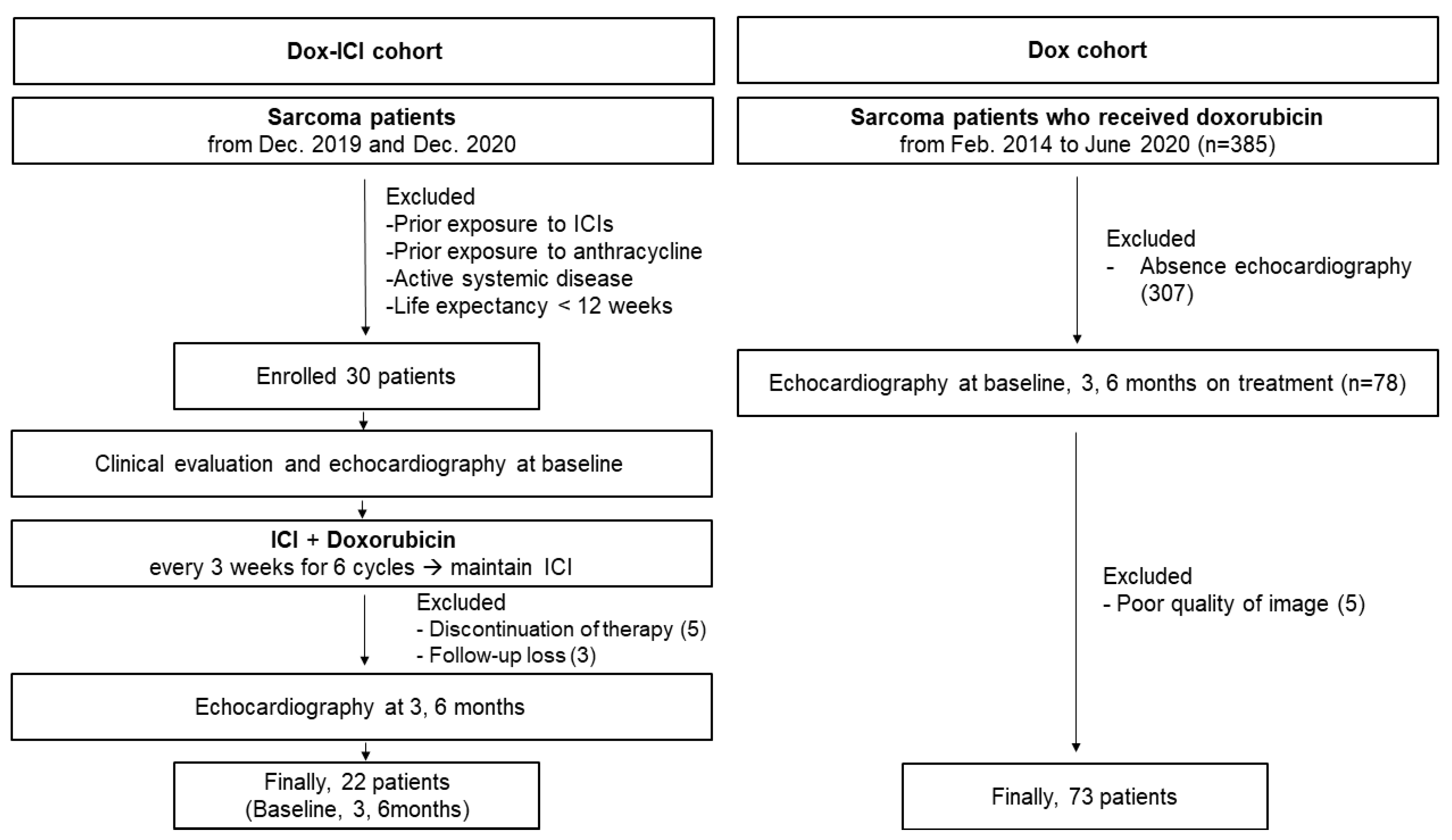
2.1. Study Population
2.2. 2D and Speckle Tracking Echocardiography
2.3. Echocardiography-Based Definition of Cancer Therapy-Related Cardiac Dysfunction
2.4. Statistical Analysis
3. Results
3.1. Patients and Demographics
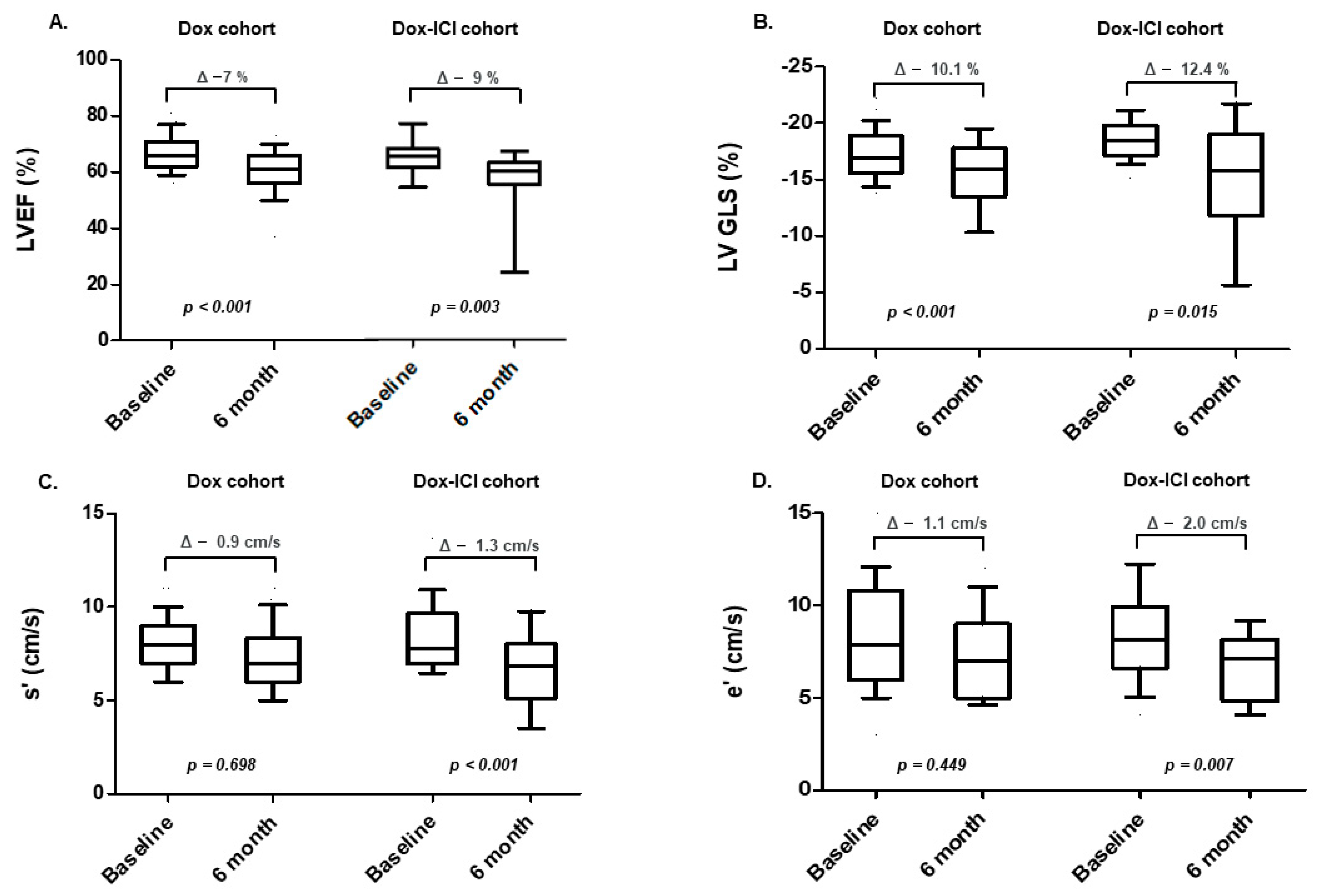
3.2. Echocardiographic Characteristics: Baseline and Serial Changes
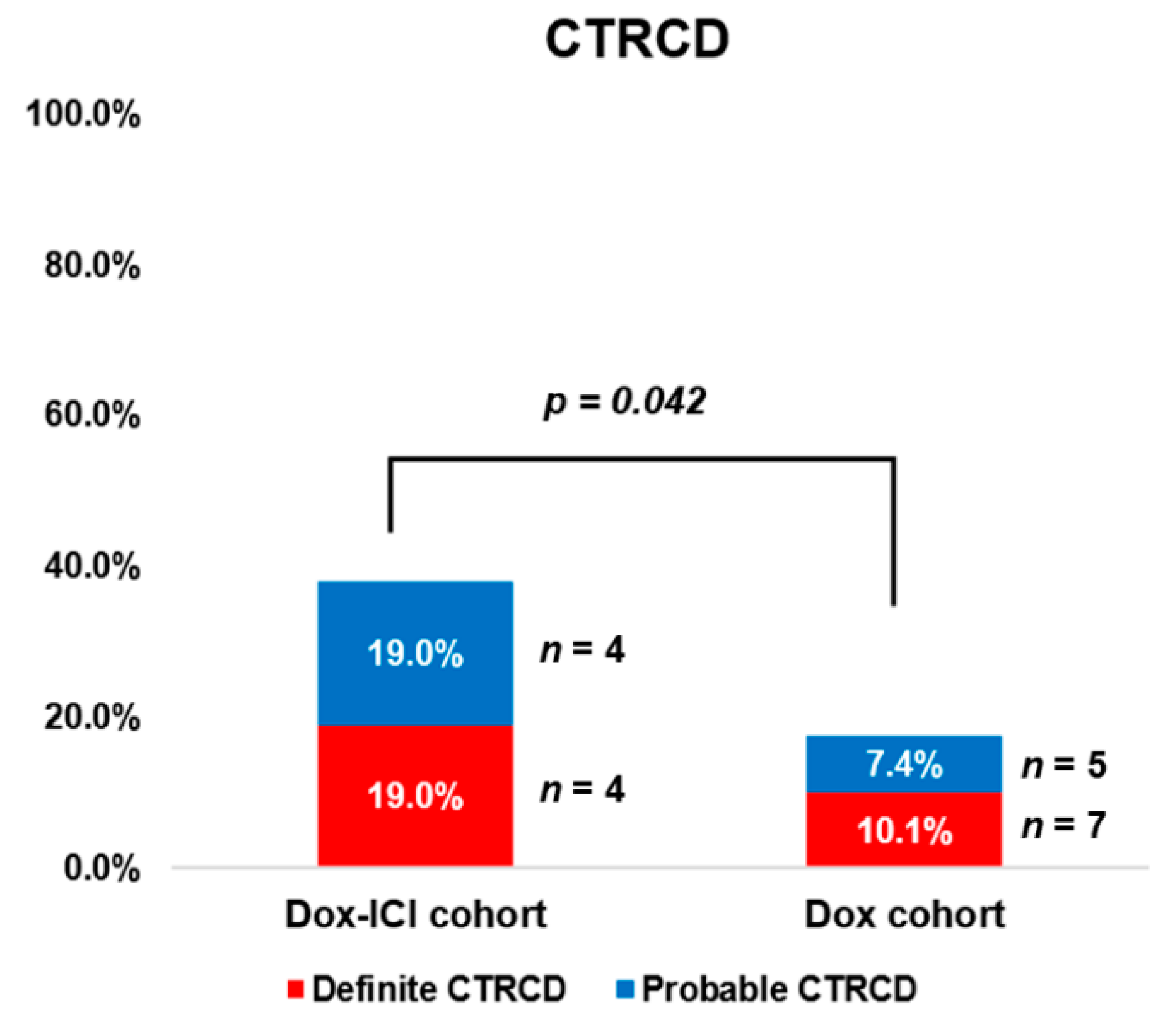
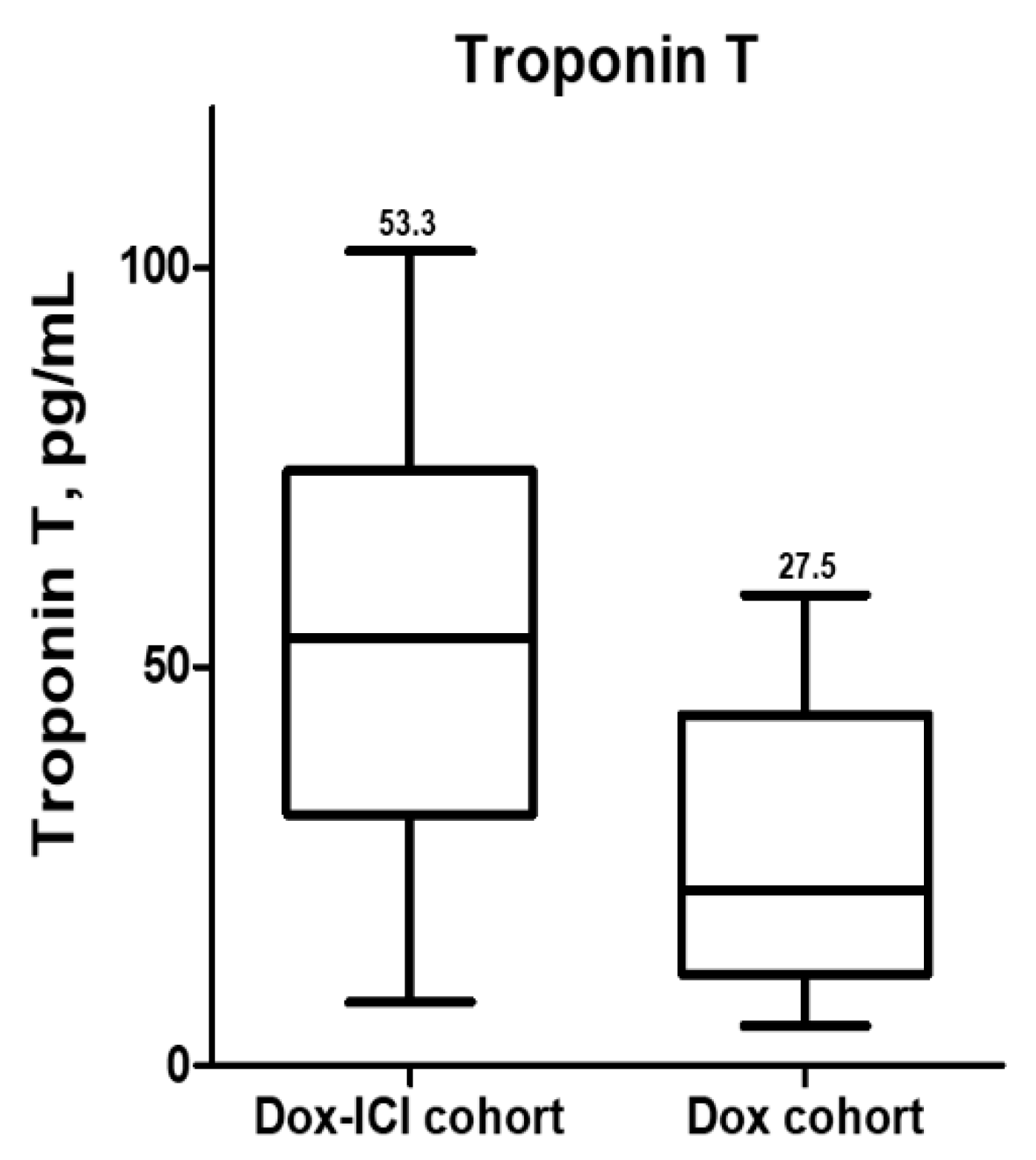
3.3. Cancer Therapy-Related Cardiac Dysfunction and Clinical Outcomes
3.4. Predictors of Cancer Therapy-Related Cardiac Dysfunction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICIs | Immune checkpoint inhibitors |
| LVGLS | Left ventricular global longitudinal strain |
| CTRCD | Cancer therapy-related cardiac dysfunction |
| LVEF | Left ventricular ejection fraction |
| TDI | Tissue Doppler imaging |
| ACIs | Angiotensin-converting enzyme inhibitors |
| ARBs | Angiotensin receptor blockers |
References
- Bramwell, V.H.; Anderson, D.; Charette, M.L. Doxorubicin-based chemotherapy for the palliative treatment of adult patients with locally advanced or metastatic soft-tissue sarcoma: A meta-analysis and clinical practice guideline. Sarcoma 2000, 4, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schoffski, P.; Blay, J.Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Jones, R.L.; Wagner, A.J.; Kawai, A.; Tamura, K.; Shahir, A.; Van Tine, B.A.; Martin-Broto, J.; Peterson, P.M.; Wright, J.; Tap, W.D. Prospective Evaluation of Doxorubicin Cardiotoxicity in Patients with Advanced Soft-tissue Sarcoma Treated in the ANNOUNCE Phase III Randomized Trial. Clin. Cancer Res. 2021, 27, 3861–3866. [Google Scholar] [CrossRef] [PubMed]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Mahoney, M.R.; Van Tine, B.A.; Atkins, J.; Milhem, M.M.; Jahagirdar, B.N.; Antonescu, C.R.; Horvath, E.; Tap, W.D.; Schwartz, G.K.; et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): Two open-label, non-comparative, randomised, phase 2 trials. Lancet Oncol. 2018, 19, 416–426. [Google Scholar] [CrossRef]
- Pollack, S.M.; Redman, M.W.; Baker, K.K.; Wagner, M.J.; Schroeder, B.A.; Loggers, E.T.; Trieselmann, K.; Copeland, V.C.; Zhang, S.; Black, G. Assessment of doxorubicin and pembrolizumab in patients with advanced anthracycline-naive sarcoma: A phase 1/2 nonrandomized clinical trial. JAMA Oncol. 2020, 6, 1778–1782. [Google Scholar] [CrossRef]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L. Fulminant myocarditis with combination immune checkpoint blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D. Myocarditis in patients treated with immune checkpoint inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Hu, J.-R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. [Google Scholar] [CrossRef] [Green Version]
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.; Moslehi, J.; Larkin, J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A. Clinical features, management, and outcomes of immune checkpoint inhibitor–related cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef]
- D’Souza, M.; Nielsen, D.; Svane, I.M.; Iversen, K.; Rasmussen, P.V.; Madelaire, C.; Fosbøl, E.; Køber, L.; Gustafsson, F.; Andersson, C. The risk of cardiac events in patients receiving immune checkpoint inhibitors: A nationwide Danish study. Eur. Heart J. 2021, 42, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Sondak, V.K.; McArthur, G.A. Adjuvant immunotherapy for cancer: The next step. Lancet Oncol. 2015, 16, 478–480. [Google Scholar] [CrossRef]
- Waheed, N.; Fradley, M.G.; DeRemer, D.L.; Mahmoud, A.; Shah, C.P.; Langaee, T.Y.; Lipori, G.P.; March, K.; Pepine, C.J.; Cooper-DeHoff, R.M. Newly diagnosed cardiovascular disease in patients treated with immune checkpoint inhibitors: A retrospective analysis of patients at an academic tertiary care center. Cardio-Oncology 2021, 7, 10. [Google Scholar] [CrossRef]
- Brouwer, C.A.; Postma, A.; Vonk, J.M.; Zwart, N.; van den Berg, M.P.; Bink-Boelkens, M.T.; Dolsma, W.V.; Smit, A.J.; de Vries, E.G.; Tissing, W.J.; et al. Systolic and diastolic dysfunction in long-term adult survivors of childhood cancer. Eur. J. Cancer 2011, 47, 2453–2462. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Infante, N.; Ramirez-Flores, Y.A.; Castillo, E.C.; Lozano, O.; Garcia-Rivas, G.; Torre-Amione, G. Cardiotoxicity associated with immune checkpoint inhibitor therapy: A meta-analysis. Eur. J. Heart Fail. 2021, 23, 1739–1747. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Amundsen, B.H.; Helle-Valle, T.; Edvardsen, T.; Torp, H.; Crosby, J.; Lyseggen, E.; Støylen, A.; Ihlen, H.; Lima, J.A.; Smiseth, O.A. Noninvasive myocardial strain measurement by speckle tracking echocardiography: Validation against sonomicrometry and tagged magnetic resonance imaging. J. Am. Coll. Cardiol. 2006, 47, 789–793. [Google Scholar] [CrossRef] [Green Version]
- Dobson, R.; Ghosh, A.K.; Ky, B.; Marwick, T.; Stout, M.; Harkness, A.; Steeds, R.; Robinson, S.; Oxborough, D.; Adlam, D. BSE and BCOS Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab. Cardio Oncol. 2021, 3, 1–16. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.-E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L. Fatal toxic effects associated with immune checkpoint inhibitors: A systematic review and meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drobni, Z.D.; Alvi, R.M.; Taron, J.; Zafar, A.; Murphy, S.P.; Rambarat, P.K.; Mosarla, R.C.; Lee, C.; Zlotoff, D.A.; Raghu, V.K. Association between immune checkpoint inhibitors with cardiovascular events and atherosclerotic plaque. Circulation 2020, 142, 2299–2311. [Google Scholar] [CrossRef] [PubMed]
- Kraigher-Krainer, E.; Shah, A.M.; Gupta, D.K.; Santos, A.; Claggett, B.; Pieske, B.; Zile, M.R.; Voors, A.A.; Lefkowitz, M.P.; Packer, M.; et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2014, 63, 447–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial strain imaging: How useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef] [Green Version]
- Thavendiranathan, P.; Poulin, F.; Lim, K.-D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll. Cardiol. 2014, 63, 2751–2768. [Google Scholar] [CrossRef] [Green Version]
- Oikonomou, E.K.; Kokkinidis, D.G.; Kampaktsis, P.N.; Amir, E.A.; Marwick, T.H.; Gupta, D.; Thavendiranathan, P. Assessment of prognostic value of left ventricular global longitudinal strain for early prediction of chemotherapy-induced cardiotoxicity: A systematic review and meta-analysis. JAMA Cardiol. 2019, 4, 1007–1018. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1063–1093. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef]
- Stoodley, P.W.; Richards, D.A.; Boyd, A.; Hui, R.; Harnett, P.R.; Meikle, S.R.; Clarke, J.L.; Thomas, L. Altered left ventricular longitudinal diastolic function correlates with reduced systolic function immediately after anthracycline chemotherapy. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 228–234. [Google Scholar] [CrossRef] [Green Version]
- Herman, E.H.; Zhang, J.; Lipshultz, S.E.; Rifai, N.; Chadwick, D.; Takeda, K.; Yu, Z.-X.; Ferrans, V.J. Correlation between serum levels of cardiac troponin-T and the severity of the chronic cardiomyopathy induced by doxorubicin. J. Clin. Oncol. 1999, 17, 2237. [Google Scholar] [CrossRef]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and brain natriuretic peptides for the prediction of cardiotoxicity in cancer patients: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilickap, S.; Barista, I.; Akgul, E.; Aytemir, K.; Aksoyek, S.; Aksoy, S.; Celik, I.; Kes, S.; Tekuzman, G. cTnT can be a useful marker for early detection of anthracycline cardiotoxicity. Ann. Oncol. 2005, 16, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Larkin, J.; Oya, M.; Thistlethwaite, F.; Martignoni, M.; Nathan, P.; Powles, T.; McDermott, D.; Robbins, P.B.; Chism, D.D. Preliminary results for avelumab plus axitinib as first-line therapy in patients with advanced clear-cell renal-cell carcinoma (JAVELIN Renal 100): An open-label, dose-finding and dose-expansion, phase 1b trial. Lancet Oncol. 2018, 19, 451–460. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unmatching | Matching * | ||||
|---|---|---|---|---|---|
| Dox-ICI Cohort (n = 22) | Dox Cohort (n = 73) | p Value | Dox Cohort (n = 22) | p Value † | |
| Age | 51 ± 14 | 53 ± 14 | 0.587 | 51 ± 14 | 0.985 |
| Male, n (%) | 14 (48.3) | 27 (39.1) | 0.402 | 14 (48.3) | 1.000 |
| Cardiovascular risk factors | |||||
| Hypertension, n (%) | 5 (17.2) | 16 (22.2) | 0.598 | 6 (20.7) | 0.783 |
| Diabetes, n (%) | 3 (10.3) | 7 (9.5) | 0.976 | 4 (13.8) | 0.687 |
| Dyslipidemia, n (%) | 2 (6.9) | 1 (1.3) | 0.153 | 0 (0) | 0.150 |
| Atrial fibrillation, n (%) | 1 (3.4) | 5 (6.8) | 0.474 | 3 (10.3) | 0.300 |
| Coronary artery disease, n (%) | 1 (3.4) | 1 (1.3) | 0.523 | 0 (0) | 0.313 |
| Chronic kidney disease, n (%) | 0 (0) | 12 (16.4) | 0.017 | 5 (17.2) | 0.019 |
| Baseline physical findings | 117 ± 11 | 113 ± 19 | 0.409 | 113 ± 19 | 0.409 |
| Systolic blood pressure, mmHg | 117 ± 11 | 113 ± 19 | 0.409 | 114 ± 19 | 0.395 |
| Diastolic blood pressure, mmHg | 71 ± 10 | 70 ± 17 | 0.841 | 69 ± 21 | 0.705 |
| BSA, kg/m2 | 1.67 ± 0.17 | 1.63 ± 0.22 | 0.472 | 1.63 ± 0.20 | 0.448 |
| Medication | |||||
| Beta blocker, n (%) | 1 (4.5) | 2 (2.7) | 0.667 | 1 (4.5) | 0.879 |
| ACE-I or ARB, n (%) | 3 (13.6) | 10 (13.6) | 0.469 | 5 (22.7) | 0.447 |
| Statin, n (%) | 5 (22.7) | 12 (16.4) | 0.145 | 6 (27.2) | 0.256 |
| Adriamycin cumulative dose, mg/m2 | 395 ± 49 | 400 ± 56 | 0.820 | 398 ± 55 | 0.954 |
| Unmatching | Matching * | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dox-ICI Cohort (n = 22) | Dox Cohort (n = 73) | Dox Cohort (n = 22) | |||||||
| Baseline | 6-Month | p Value | Baseline | 6-Month | p Value | Baseline | 6-Month | p Value | |
| LVEF, % | 65 ± 5 | 56 ± 8 | 0.003 | 66 ± 6 | 59 ± 6 | <0.001 | 66 ± 6 | 60 ± 9 | <0.001 |
| Change in LVEF, % | −9.3 ± 2.1 | −7.0 ± 1.3 | 0.376 | −6.9 ± 1.9 | 0.188 † | ||||
| (Absolute change) | |||||||||
| LVEDD, mm | 47 ± 3 | 45 ± 2 | 0.291 | 48 ± 3 | 48 ± 2 | 0.674 | 48 ± 3 | 48 ± 2 | 0.624 |
| LVESD, mm | 30 ± 2 | 31 ± 1 | 0.952 | 31 ± 3 | 32 ± 3 | 0.856 | 31 ± 3 | 33 ± 3 | 0.122 |
| LAVI, mL/m2 | 27.6 ± 1.3 | 27.5 ± 2.1 | 0.965 | 27.8 ± 11.0 | 28.4 ± 12.0 | 0.776 | 27.8 ± 11.0 | 28.8 ± 7.2 | 0.650 |
| E velocity, cm/s | 0.68 ± 0.16 | 0.58 ± 0.28 | 0.127 | 0.69 ± 0.16 | 0.65 ± 0.20 | 0.196 | 0.69 ± 0.16 | 0.64 ± 0.18 | 0.095 |
| A velocity, cm/s | 0.63 ± 0.24 | 0.51 ± 0.29 | 0.051 | 0.64 ± 0.16 | 0.67 ± 0.17 | 0.332 | 0.64 ± 0.16 | 0.67 ± 0.17 | 0.148 |
| S’, cm/s | 8.42 ± 2.06 | 6.15 ± 3.19 | <0.001 | 8.1 ± 1.5 | 7.2 ± 2.2 | 0.698 | 8.1 ± 1.5 | 7.2 ± 2.2 | 0.375 |
| e’, cm/s | 8.12 ± 2.39 | 6.07 ± 3.27 | 0.007 | 8.1 ± 2.7 | 7.0 ± 2.6 | 0.449 | 8.1 ± 2.7 | 7.1 ± 2.3 | 0.225 |
| a’, cm/s | 9.21 ± 3.30 | 6.89 ± 4.28 | 0.01 | 8.7 ± 1.8 | 8.1 ± 2.3 | 0.101 | 8.7 ± 1.8 | 8.1 ± 2.3 | 0.419 |
| E/e’ ratio | 8.76 ± 2.27 | 9.60 ± 2.27 | 0.602 | 9.1 ± 2.7 | 9.8 ± 4.1 | 0.209 | 9.1 ± 2.7 | 9.6 ± 2.9 | 0.589 |
| PASP, mmHg | 22 ± 9 | 27 ± 9 | 0.504 | 26 ± 7 | 28 ± 9 | 0.353 | 26 ± 7 | 28 ± 8 | 0.267 |
| LVGLS, % | −18.6 ± 1.9 | −15.3 ± 3.6 | 0.015 | −17.3 ± 2.3 | −15.4 ± 3.6 | <0.001 | −17.3 ± 2.3 | −15.6 ± 2.8 | <0.001 |
| Change in LVGLS, % | −12.4 ± −2.4 | −10.1 ± −1.9 | 0.392 | −10.0 ± −1.8 | 0.296 † | ||||
| (Relative change) | |||||||||
| CTRCD (n = 20) | Non-CTRCD (n = 75) | p Value | |
|---|---|---|---|
| Cardiovascular risk factors | |||
| Hypertension, n (%) | 8 (40.0) | 11 (15.3) | 0.029 |
| Diabetes, n (%) | 3 (15.0) | 8 (10.2) | 0.703 |
| Dyslipidemia, n (%) | 3 (15.0) | 1 (1.2) | 0.034 |
| Coronary artery disease, n (%) | 1 (5.0) | 1 (1.2) | 0.397 |
| Atrial fibrillation or atrial flutter, n (%) | 2 (10.0) | 4 (5.1) | 0.611 |
| Oncologic risk factor | |||
| Adriamycin cumulative dose, mg/m2 | 430 ± 133 | 394 ± 113 | 0.084 |
| Concomitant use of ICI | 8 (40.0) | 14 (18.7) | 0.044 |
| Baseline LV systolic function | |||
| LVEF, % | 67 ± 6 | 66 ± 6 | 0.408 |
| LVGLS, % | −18.0 ± 1.9 | −17.4 ± 3.2 | 0.296 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Cho, I.; You, S.-C.; Cha, M.-J.; Chang, J.-S.; Kim, W.D.; Go, K.-y.; Kim, D.-Y.; Seo, J.; Shim, C.-Y.; et al. Cancer Therapy-Related Cardiac Dysfunction in Patients Treated with a Combination of an Immune Checkpoint Inhibitor and Doxorubicin. Cancers 2022, 14, 2320. https://doi.org/10.3390/cancers14092320
Lee S-H, Cho I, You S-C, Cha M-J, Chang J-S, Kim WD, Go K-y, Kim D-Y, Seo J, Shim C-Y, et al. Cancer Therapy-Related Cardiac Dysfunction in Patients Treated with a Combination of an Immune Checkpoint Inhibitor and Doxorubicin. Cancers. 2022; 14(9):2320. https://doi.org/10.3390/cancers14092320
Chicago/Turabian StyleLee, Seon-Hwa, Iksung Cho, Seng-Chan You, Min-Jae Cha, Jee-Suk Chang, William D. Kim, Kyu-yong Go, Dae-Young Kim, Jiwon Seo, Chi-Young Shim, and et al. 2022. "Cancer Therapy-Related Cardiac Dysfunction in Patients Treated with a Combination of an Immune Checkpoint Inhibitor and Doxorubicin" Cancers 14, no. 9: 2320. https://doi.org/10.3390/cancers14092320