Predicting Peritoneal Dissemination of Gastric Cancer in the Era of Precision Medicine: Molecular Characterization and Biomarkers

Abstract
:1. Introduction
2. Diffuse Type Gastric Cancer from a Molecular Perspective
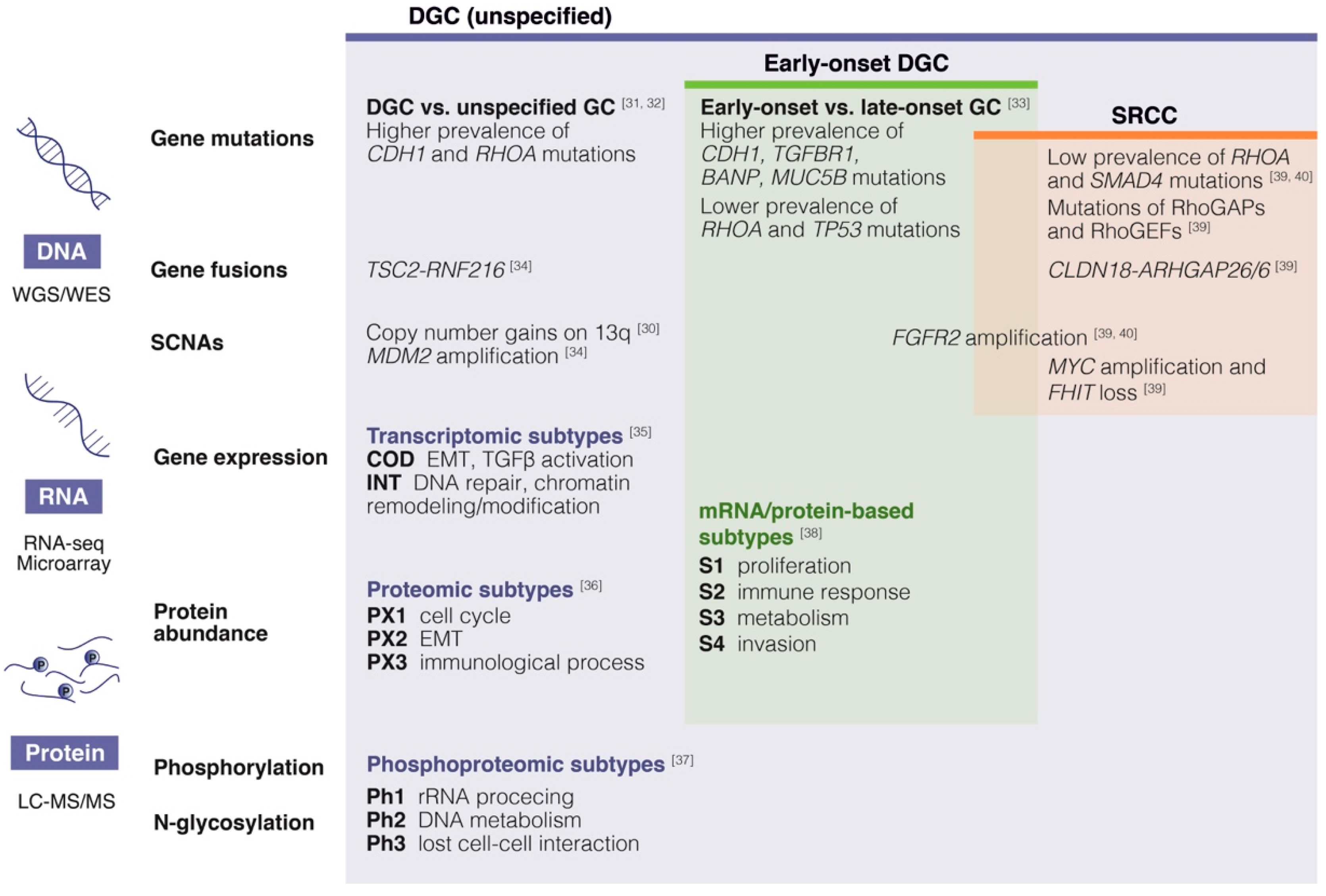
2.1. Multi-Omic Characterization of Diffuse Type Gastric Cancer
2.2. Early-Onset Diffuse Type Gastric Cancer
2.3. Gastric Signet Ring Cell Carcinoma
2.4. Molecular Features of Diffuse Type Gastric Cancer and Peritoneal Dissemination
3. Molecular Classifications of Gastric Cancer and Subsets with Peritoneal Dissemination Propensity
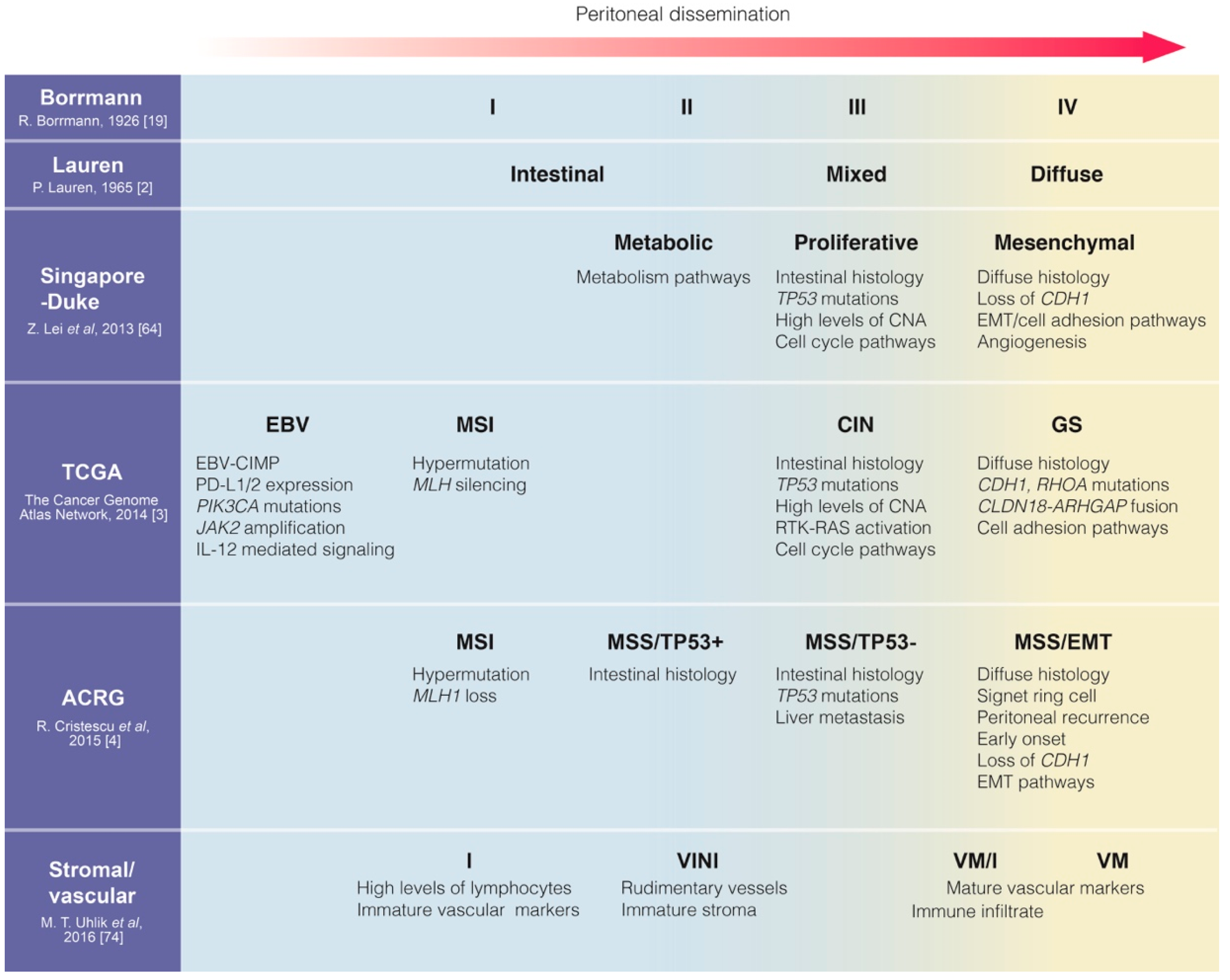
3.1. Expression Microarray-Based Classifications
3.2. The Cancer Genome Atlas (TCGA) and Other Genome-Based Classifications
3.3. Asian Cancer Research Group (ACRG) Classification
3.4. Tumor Microenvironment-Based Signatures
3.5. Molecular Profiling of Peritoneal Metastases or Malignant Ascites
3.6. Subsets Associated with Peritoneal Dissemination Propensity Across Multiple Classifications
4. Molecular Markers for Detection or Prediction of Peritoneal Dissemination
4.1. Serum Tumor Markers
4.2. Molecular Markers in Peritoneal Lavages
4.3. Molecular Markers in Primary Gastric Cancer Tissues
5. Conclusions and Future Perspective
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Lauren, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Chia, N.Y.; Tan, P. Molecular classification of gastric cancer. Ann. Oncol. 2016, 27, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Gheza, F.; Lotti, M.; Virzi, S.; Iusco, D.; Ghermandi, C.; Melotti, R.; Baiocchi, G.; Giulini, S.M.; Ansaloni, L.; et al. Peritoneal carcinomatosis. World J. Gastroenterol. 2013, 19, 6979–6994. [Google Scholar] [CrossRef]
- Ramos, R.F.; Scalon, F.M.; Scalon, M.M.; Dias, D.I. Staging laparoscopy in gastric cancer to detect peritoneal metastases: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1315–1321. [Google Scholar] [CrossRef]
- Allen, C.J.; Newhook, T.E.; Vreeland, T.J.; Das, P.; Minsky, B.D.; Blum, M.; Song, S.; Ajani, J.; Ikoma, N.; Mansfield, P.F.; et al. Yield of peritoneal cytology in staging patients with gastric and gastroesophageal cancer. J. Surg. Oncol. 2019, 120, 1350–1357. [Google Scholar] [CrossRef]
- Dong, D.; Tang, L.; Li, Z.Y.; Fang, M.J.; Gao, J.B.; Shan, X.H.; Ying, X.J.; Sun, Y.S.; Fu, J.; Wang, X.X.; et al. Development and validation of an individualized nomogram to identify occult peritoneal metastasis in patients with advanced gastric cancer. Ann. Oncol. 2019, 30, 431–438. [Google Scholar] [CrossRef]
- Kagawa, S.; Shigeyasu, K.; Ishida, M.; Watanabe, M.; Tazawa, H.; Nagasaka, T.; Shirakawa, Y.; Fujiwara, T. Molecular diagnosis and therapy for occult peritoneal metastasis in gastric cancer patients. World J. Gastroenterol. 2014, 20, 17796–17803. [Google Scholar] [CrossRef]
- Shiozaki, H.; Elimova, E.; Slack, R.S.; Chen, H.C.; Staerkel, G.A.; Sneige, N.; Shimodaira, Y.; Sagebiel, T.; Lee, J.H.; Bhutani, M.S.; et al. Prognosis of gastric adenocarcinoma patients with various burdens of peritoneal metastases. J. Surg. Oncol. 2016, 113, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.S.; Al-Adra, D.P.; Nagendran, J.; Campbell, S.; Shi, X.; Haase, E.; Schiller, D. Treatment of gastric cancer with peritoneal carcinomatosis by cytoreductive surgery and HIPEC: A systematic review of survival, mortality, and morbidity. J. Surg. Oncol. 2011, 104, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Badgwell, B.; Roy-Chowdhuri, S.; Chiang, Y.J.; Matamoros, A.; Blum, M.; Fournier, K.; Mansfield, P.; Ajani, J. Long-term survival in patients with metastatic gastric and gastroesophageal cancer treated with surgery. J. Surg. Oncol. 2015, 111, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Mizrak Kaya, D.; Nogueras-Gonzalez, G.M.; Harada, K.; Amlashi, F.G.; Roy-Chowdhuri, S.; Estrella, J.S.; Das, P.; Lee, J.H.; Weston, B.; Bhutani, M.S.; et al. Risk of peritoneal metastases in patients who had negative peritoneal staging and received therapy for localized gastric adenocarcinoma. J. Surg. Oncol. 2018, 117, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Chia, D.K.A.; So, J.B.Y. Recent Advances in Intra-peritoneal Chemotherapy for Gastric Cancer. J. Gastric Cancer 2020, 20, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Seyfried, F.; von Rahden, B.H.; Miras, A.D.; Gasser, M.; Maeder, U.; Kunzmann, V.; Germer, C.-T.; Pelz, J.O.W.; Kerscher, A.G. Incidence, time course and independent risk factors for metachronous peritoneal carcinomatosis of gastric origin–a longitudinal experience from a prospectively collected database of 1108 patients. BMC Cancer 2015, 15, e73. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Son, S.Y.; Lee, C.M.; Ahn, S.H.; Park, D.J.; Kim, H.H. Factors predicting peritoneal recurrence in advanced gastric cancer: Implication for adjuvant intraperitoneal chemotherapy. Gastric Cancer 2014, 17, 529–536. [Google Scholar] [CrossRef] [Green Version]
- D’Angelica, M.; Gonen, M.; Brennan, M.F.; Turnbull, A.D.; Bains, M.; Karpeh, M.S. Patterns of Initial Recurrence in Completely Resected Gastric Adenocarcinoma. Ann. Surg. 2004, 240, 808–816. [Google Scholar] [CrossRef]
- Borrmann, R. Geschwulste des Magens und des Duodenums. In Handbuch der Speziellen Pathologischen Anatomie und Histologie; Henke, F., Lubarsch, O., Eds.; Springer: Berlin/Heidelberg, Germany, 1926; Volume IV/I, pp. 812–1054. [Google Scholar]
- Henson, D.E.; Dittus, C.; Younes, M.; Nguyen, H.; Albores-Saavedra, J. Differential trends in the intestinal and diffuse types of gastric carcinoma in the United States, 1973–2000: Increase in the signet ring cell type. Arch. Pathol. Lab. Med. 2004, 128, 765–770. [Google Scholar]
- Lee, J.H.; Chang, K.K.; Yoon, C.; Tang, L.H.; Strong, V.E.; Yoon, S.S. Lauren Histologic Type Is the Most Important Factor Associated With Pattern of Recurrence Following Resection of Gastric Adenocarcinoma. Ann. Surg. 2018, 267, 105–113. [Google Scholar] [CrossRef]
- Luo, Y.; Gao, P.; Song, Y.; Sun, J.; Huang, X.; Zhao, J.; Ma, B.; Li, Y.; Wang, Z. Clinicopathologic characteristics and prognosis of Borrmann type IV gastric cancer: A meta-analysis. World J. Surg. Oncol. 2016, 14, e49. [Google Scholar] [CrossRef]
- Kanda, M.; Kodera, Y. Molecular mechanisms of peritoneal dissemination in gastric cancer. World J. Gastroenterol. 2016, 22, e6829. [Google Scholar] [CrossRef]
- Mikuła-Pietrasik, J.; Uruski, P.; Tykarski, A.; Książek, K. The peritoneal “soil” for a cancerous “seed”: A comprehensive review of the pathogenesis of intraperitoneal cancer metastases. Cell. Mol. Life Sci. 2017, 75, 509–525. [Google Scholar]
- Ceelen, W.P.; Bracke, M.E. Peritoneal minimal residual disease in colorectal cancer: Mechanisms, prevention, and treatment. Lancet Oncol. 2009, 10, 72–79. [Google Scholar] [CrossRef]
- Hu, B.; El Hajj, N.; Sittler, S.; Lammert, N.; Barnes, R.; Meloni-Ehrig, A. Gastric cancer: Classification, histology and application of molecular pathology. J. Gastrointest. Oncol. 2012, 3, 251–261. [Google Scholar] [PubMed]
- Chon, H.J.; Hyung, W.J.; Kim, C.; Park, S.; Kim, J.H.; Park, C.H.; Ahn, J.B.; Kim, H.; Chung, H.C.; Rha, S.Y.; et al. Differential Prognostic Implications of Gastric Signet Ring Cell Carcinoma: Stage Adjusted Analysis From a Single High-volume Center in Asia. Ann. Surg. 2017, 265, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Janjigian, Y.Y. Clinical impact of tumour biology in the management of gastroesophageal cancer. Nat. Rev. Clin. Oncol. 2016, 13, 348–360. [Google Scholar] [CrossRef]
- Rawicz-Pruszynski, K.; Mielko, J.; Pudlo, K.; Lisiecki, R.; Skoczylas, T.; Murawa, D.; Polkowski, W.P. Yield of staging laparoscopy in gastric cancer is influenced by Lauren histologic subtype. J. Surg. Oncol. 2019, 120, 1148–1153. [Google Scholar] [CrossRef]
- Wu, M.-S.; Chang, M.-C.; Huang, S.-P.; Tseng, C.-C.; Sheu, J.-C.; Lin, Y.-W.; Shun, C.-T.; Lin, M.-T.; Lin, J.-T. Correlation of histologic subtypes and replication error phenotype with comparative genomic hybridization in gastric cancer. Genes Chromosomes Cancer 2001, 30, 80–86. [Google Scholar] [CrossRef]
- Wang, K.; Yuen, S.T.; Xu, J.; Lee, S.P.; Yan, H.H.N.; Shi, S.T.; Siu, H.C.; Deng, S.; Chu, K.M.; Law, S.; et al. Whole-genome sequencing and comprehensive molecular profiling identify new driver mutations in gastric cancer. Nat. Genet. 2014, 46, 573–582. [Google Scholar] [CrossRef]
- Kakiuchi, M.; Nishizawa, T.; Ueda, H.; Gotoh, K.; Tanaka, A.; Hayashi, A.; Yamamoto, S.; Tatsuno, K.; Katoh, H.; Watanabe, Y.; et al. Recurrent gain-of-function mutations of RHOA in diffuse-type gastric carcinoma. Nat. Genet. 2014, 46, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Park, J.W.; Liu, Y.; Park, Y.S.; Kim, J.H.; Yang, H.; Um, H.; Ko, W.R.; Lee, B.I.; Kwon, S.Y.; et al. Sporadic Early-Onset Diffuse Gastric Cancers Have High Frequency of Somatic CDH1 Alterations, but Low Frequency of Somatic RHOA Mutations Compared With Late-Onset Cancers. Gastroenterology 2017, 153, 536–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-S.; Cho, Y.; Lee, G.; Lee, S.; Kim, Y.-W.; Jho, S.; Kim, H.-M.; Hong, S.-H.; Hwang, J.-A.; Kim, S.-Y.; et al. Genomic profile analysis of diffuse-type gastric cancers. Genome Biol. 2014, 15, R55. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-K.; Kim, H.-J.; Park, J.-L.; Heo, H.; Kim, S.-Y.; Lee, S.-I.; Song, K.-S.; Kim, W.-H.; Kim, Y.S. Identification of a molecular signature of prognostic subtypes in diffuse-type gastric cancer. Gastric Cancer 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, S.; Xia, X.; Ding, C.; Zhen, B.; Zhou, Q.; Feng, J.; Yuan, J.; Chen, R.; Li, Y.; Ge, Z.; et al. A proteomic landscape of diffuse-type gastric cancer. Nat. Commun. 2018, 9, e1012. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.; Yu, C.; Shi, J.; Huang, W.; Ge, S.; Liu, M.; Song, L.; Zhan, D.; Xia, X.; Liu, W.; et al. Phosphoproteomics Enables Molecular Subtyping and Nomination of Kinase Candidates for Individual Patients of Diffuse-Type Gastric Cancer. iScience 2019, 22, 44–57. [Google Scholar] [CrossRef] [Green Version]
- Mun, D.-G.; Bhin, J.; Kim, S.; Kim, H.; Jung, J.H.; Jung, Y.; Jang, Y.E.; Park, J.M.; Kim, H.; Jung, Y.; et al. Proteogenomic Characterization of Human Early-Onset Gastric Cancer. Cancer Cell 2019, 35, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Shu, Y.; Zhang, W.; Hou, Q.; Zhao, L.; Zhang, S.; Zhou, J.; Song, X.; Zhang, Y.; Jiang, D.; Chen, X.; et al. Prognostic significance of frequent CLDN18-ARHGAP26/6 fusion in gastric signet-ring cell cancer. Nat. Commun. 2018, 9, e2447. [Google Scholar] [CrossRef] [Green Version]
- Kwon, C.H.; Kim, Y.K.; Lee, S.; Kim, A.; Park, H.J.; Choi, Y.; Won, Y.J.; Park, D.Y.; Lauwers, G.Y. Gastric poorly cohesive carcinoma: A correlative study of mutational signatures and prognostic significance based on histopathological subtypes. Histopathology 2018, 72, 556–568. [Google Scholar] [CrossRef]
- Kim, K.-M.; Kwon, M.-S.; Hong, S.-J.; Min, K.-O.; Seo, E.-J.; Lee, K.-Y.; Choi, S.-W.; Rhyu, M.-G. Genetic classification of intestinal-type and diffuse-type gastric cancers based on chromosomal loss and microsatellite instability. Virchows Archiv. 2003, 443, 491–500. [Google Scholar] [CrossRef]
- Hong, S.J.; Jeon, E.J.; Oh, J.H.; Seo, E.J.; Choi, S.W.; Rhyu, M.G. The gene-reduction effect of chromosomal losses detected in gastric cancers. BMC Gastroenterol. 2010, 10, e138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, M.; Murrell, A.; Ito, Y.; Maia, A.T.; Hyland, S.; Oliveira, C.; Save, V.; Carneiro, F.; Paterson, A.L.; Grehan, N.; et al. Mechanisms and sequelae of E-cadherin silencing in hereditary diffuse gastric cancer. J. Pathol. 2008, 216, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wu, W.K.K.; Xing, R.; Wong, S.H.; Liu, Y.; Fang, X.; Zhang, Y.; Wang, M.; Wang, J.; Li, L.; et al. Distinct Subtypes of Gastric Cancer Defined by Molecular Characterization Include Novel Mutational Signatures with Prognostic Capability. Cancer Res. 2016, 76, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Ushiku, T.; Ishikawa, S.; Kakiuchi, M.; Tanaka, A.; Katoh, H.; Aburatani, H.; Lauwers, G.Y.; Fukayama, M. RHOA mutation in diffuse-type gastric cancer: A comparative clinicopathology analysis of 87 cases. Gastric Cancer 2016, 19, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.S.; Kim, K.-M.; Ting, J.C.; Yu, K.; Fu, J.; Liu, S.; Cristescu, R.; Nebozhyn, M.; Gong, L.; Yue, Y.G.; et al. Genomic landscape and genetic heterogeneity in gastric adenocarcinoma revealed by whole-genome sequencing. Nat. Commun. 2014, 5, 1–12. [Google Scholar] [CrossRef]
- Jansen, S.; Gosens, R.; Wieland, T.; Schmidt, M. Paving the Rho in cancer metastasis: Rho GTPases and beyond. Pharmacol. Ther. 2018, 183, 1–21. [Google Scholar] [CrossRef]
- Bautista, M.C.; Jiang, S.F.; Armstrong, M.A.; Postlethwaite, D.; Li, D. Impact of age on clinicopathological features and survival of patients with noncardia gastric adenocarcinoma. J. Gastric Cancer 2014, 14, 238–245. [Google Scholar] [CrossRef] [Green Version]
- Kong, X.; Wang, J.L.; Chen, H.M.; Fang, J.Y. Comparison of the clinicopathological characteristics of young and elderly patients with gastric carcinoma: A meta analysis. J. Surg. Oncol. 2012, 106, 346–352. [Google Scholar] [CrossRef]
- Taghavi, S.; Jayarajan, S.N.; Davey, A.; Willis, A.I. Prognostic significance of signet ring gastric cancer. J. Clin. Oncol. 2012, 30, 3493–3498. [Google Scholar] [CrossRef] [Green Version]
- Pernot, S. Signet-ring cell carcinoma of the stomach: Impact on prognosis and specific therapeutic challenge. World J. Gastroenterol. 2015, 21, e11428. [Google Scholar] [CrossRef] [PubMed]
- Piessen, G.; Messager, M.; Leteurtre, E.; Jean-Pierre, T.; Mariette, C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann. Surg. 2009, 250, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.-M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Corso, G.; Carvalho, J.; Marrelli, D.; Vindigni, C.; Carvalho, B.; Seruca, R.; Roviello, F.; Oliveira, C. Somatic mutations and deletions of the E-cadherin gene predict poor survival of patients with gastric cancer. J. Clin. Oncol. 2013, 31, 868–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, X.; Tang, Y.B.; Yuan, G.; Wang, Y.; Wang, J.; Yang, Y.; Chen, M. The prognostic value of E-cadherin in gastric cancer: A meta-analysis. Int. J. Cancer 2013, 132, 2589–2596. [Google Scholar] [CrossRef]
- Bijlsma, M.F.; Sadanandam, A.; Tan, P.; Vermeulen, L. Molecular subtypes in cancers of the gastrointestinal tract. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 333–342. [Google Scholar] [CrossRef]
- Tay, S.T.; Leong, S.H.; Yu, K.; Aggarwal, A.; Tan, S.Y.; Lee, C.H.; Wong, K.; Visvanathan, J.; Lim, D.; Wong, W.K.; et al. A combined comparative genomic hybridization and expression microarray analysis of gastric cancer reveals novel molecular subtypes. Cancer Res. 2003, 63, 3309–3316. [Google Scholar]
- Shah, M.A.; Khanin, R.; Tang, L.; Janjigian, Y.Y.; Klimstra, D.S.; Gerdes, H.; Kelsen, D.P. Molecular classification of gastric cancer: A new paradigm. Clin. Cancer Res. 2011, 17, 2693–2701. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.Y.; Lim, J.Y.; Cheong, J.H.; Park, Y.Y.; Yoon, S.L.; Kim, S.M.; Kim, S.B.; Kim, H.; Hong, S.W.; Park, Y.N.; et al. Gene Expression Signature-Based Prognostic Risk Score in Gastric Cancer. Clin. Cancer Res. 2011, 17, 1850–1857. [Google Scholar] [CrossRef] [Green Version]
- Motoori, M.; Takemasa, I.; Doki, Y.; Saito, S.; Miyata, H.; Takiguchi, S.; Fujiwara, Y.; Yasuda, T.; Yano, M.; Kurokawa, Y.; et al. Prediction of peritoneal metastasis in advanced gastric cancer by gene expression profiling of the primary site. Eur. J. Cancer 2006, 42, 1897–1903. [Google Scholar] [CrossRef]
- Takeno, A.; Takemasa, I.; Seno, S.; Yamasaki, M.; Motoori, M.; Miyata, H.; Nakajima, K.; Takiguchi, S.; Fujiwara, Y.; Nishida, T.; et al. Gene expression profile prospectively predicts peritoneal relapse after curative surgery of gastric cancer. Ann. Surg. Oncol. 2010, 17, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Tan, I.B.; Ivanova, T.; Lim, K.H.; Ong, C.W.; Deng, N.; Lee, J.; Tan, S.H.; Wu, J.; Lee, M.H.; Ooi, C.H.; et al. Intrinsic Subtypes of Gastric Cancer, Based on Gene Expression Pattern, Predict Survival and Respond Differently to Chemotherapy. Gastroenterology 2011, 141, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Lei, Z.; Tan, I.B.; Das, K.; Deng, N.; Zouridis, H.; Pattison, S.; Chua, C.; Feng, Z.; Guan, Y.K.; Ooi, C.H.; et al. Identification of molecular subtypes of gastric cancer with different responses to PI3-kinase inhibitors and 5-fluorouracil. Gastroenterology 2013, 145, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.H.; Hwang, J.E.; Jang, H.J.; Lee, H.S.; Oh, S.C.; Shim, J.J.; Lee, K.W.; Kim, E.H.; Yim, S.Y.; Lee, S.H.; et al. Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by The Cancer Genome Atlas Project. Clin. Cancer Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Sethi, N.S.; Hinoue, T.; Schneider, B.G.; Cherniack, A.D.; Sanchez-Vega, F.; Seoane, J.A.; Farshidfar, F.; Bowlby, R.; Islam, M.; et al. Comparative Molecular Analysis of Gastrointestinal Adenocarcinomas. Cancer Cell 2018, 33, 721–735. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Yang, D.; Li, X.; Sun, B.; Song, F.; Cao, W.; Brat, D.J.; Gao, Z.; Li, H.; Liang, H.; et al. Mutational landscape of gastric adenocarcinoma in Chinese: Implications for prognosis and therapy. Proc. Natl. Acad. Sci. USA 2015, 112, 1107–1112. [Google Scholar] [CrossRef] [Green Version]
- Serra, O.; Galán, M.; Ginesta, M.M.; Calvo, M.; Sala, N.; Salazar, R. Comparison and applicability of molecular classifications for gastric cancer. Cancer Treat. Rev. 2019, 77, 29–34. [Google Scholar] [CrossRef]
- Setia, N.; Agoston, A.T.; Han, H.S.; Mullen, J.T.; Duda, D.G.; Clark, J.W.; Deshpande, V.; Mino-Kenudson, M.; Srivastava, A.; Lennerz, J.K.; et al. A protein and mRNA expression-based classification of gastric cancer. Mod. Pathol. 2016, 29, 772–784. [Google Scholar] [CrossRef]
- Ahn, S.; Lee, S.J.; Kim, Y.; Kim, A.; Shin, N.; Choi, K.U.; Lee, C.H.; Huh, G.Y.; Kim, K.M.; Setia, N.; et al. High-throughput Protein and mRNA Expression-based Classification of Gastric Cancers Can Identify Clinically Distinct Subtypes, Concordant With Recent Molecular Classifications. Am. J. Surg. Pathol. 2017, 41, 106–115. [Google Scholar] [CrossRef]
- Pinto, M.P.; Cordova-Delgado, M.; Retamal, I.N.; Munoz-Medel, M.; Bravo, M.L.; Duran, D.; Villanueva, F.; Sanchez, C.; Acevedo, F.; Mondaca, S.; et al. A Molecular Stratification of Chilean Gastric Cancer Patients with Potential Clinical Applicability. Cancers (Basel) 2020, 12, 1863. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Grabsch, H.; Ivanova, T.; Tan, I.B.; Murray, J.; Ooi, C.H.; Wright, A.I.; West, N.P.; Hutchins, G.G.A.; Wu, J.; et al. Comprehensive genomic meta-analysis identifies intra-tumoural stroma as a predictor of survival in patients with gastric cancer. Gut 2013, 62, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- Uhlik, M.T.; Liu, J.; Falcon, B.L.; Iyer, S.; Stewart, J.; Celikkaya, H.; O’Mahony, M.; Sevinsky, C.; Lowes, C.; Douglass, L.; et al. Stromal-Based Signatures for the Classification of Gastric Cancer. Cancer Res. 2016, 76, 2573–2586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salati, M.; Orsi, G.; Smyth, E.; Aprile, G.; Beretta, G.; De Vita, F.; Di Bartolomeo, M.; Fanotto, V.; Lonardi, S.; Morano, F.; et al. Gastric cancer: Translating novels concepts into clinical practice. Cancer Treat. Rev. 2019, 79, e101889. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.J.; Gagnon-Bartsch, J.A.; Tan, I.B.; Earle, S.; Ruff, L.; Pettinger, K.; Ylstra, B.; van Grieken, N.; Rha, S.Y.; Chung, H.C.; et al. Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas. Gut 2015, 64, 1721–1731. [Google Scholar] [CrossRef]
- Park, C.; Cho, J.; Lee, J.; Kang, S.Y.; An, J.Y.; Choi, M.G.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S.; et al. Host immune response index in gastric cancer identified by comprehensive analyses of tumor immunity. OncoImmunology 2017, 6, e1356150. [Google Scholar] [CrossRef] [Green Version]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Ou Yang, T.H.; Porta-Pardo, E.; Gao, G.F.; Plaisier, C.L.; Eddy, J.A.; et al. The Immune Landscape of Cancer. Immunity 2018, 48, 812–830. [Google Scholar] [CrossRef] [Green Version]
- Pectasides, E.; Stachler, M.D.; Derks, S.; Liu, Y.; Maron, S.; Islam, M.; Alpert, L.; Kwak, H.; Kindler, H.; Polite, B.; et al. Genomic Heterogeneity as a Barrier to Precision Medicine in Gastroesophageal Adenocarcinoma. Cancer Discov. 2018, 8, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Qi, C.; Liu, X.; Zhang, C.; Gao, J.; Wu, Y.; Yang, J.; Zhao, Q.; Li, J.; Wang, X.; et al. Malignant ascites-derived exosomes promote peritoneal tumor cell dissemination and reveal a distinct miRNA signature in advanced gastric cancer. Cancer Lett. 2019, 457, 142–150. [Google Scholar] [CrossRef]
- Wang, R.; Song, S.; Harada, K.; Ghazanfari Amlashi, F.; Badgwell, B.; Pizzi, M.P.; Xu, Y.; Zhao, W.; Dong, X.; Jin, J.; et al. Multiplex profiling of peritoneal metastases from gastric adenocarcinoma identified novel targets and molecular subtypes that predict treatment response. Gut 2019. [Google Scholar] [CrossRef] [Green Version]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Jamel, S.; Markar, S.R.; Malietzis, G.; Acharya, A.; Athanasiou, T.; Hanna, G.B. Prognostic significance of peritoneal lavage cytology in staging gastric cancer: Systematic review and meta-analysis. Gastric Cancer 2018, 21, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Ikoma, N.; Blum, M.; Chiang, Y.J.; Estrella, J.S.; Roy-Chowdhuri, S.; Fournier, K.; Mansfield, P.; Ajani, J.A.; Badgwell, B.D. Yield of Staging Laparoscopy and Lavage Cytology for Radiologically Occult Peritoneal Carcinomatosis of Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 4332–4337. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, J.P.; Mezhir, J.J. The critical role of peritoneal cytology in the staging of gastric cancer: An evidence-based review. J. Surg. Oncol. 2014, 110, 291–297. [Google Scholar] [CrossRef]
- Mezhir, J.J.; Shah, M.A.; Jacks, L.M.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Positive peritoneal cytology in patients with gastric cancer: Natural history and outcome of 291 patients. Ann. Surg. Oncol. 2010, 17, 3173–3180. [Google Scholar] [CrossRef]
- Yasufuku, I.; Nunobe, S.; Ida, S.; Kumagai, K.; Ohashi, M.; Hiki, N.; Sano, T. Conversion therapy for peritoneal lavage cytology-positive type 4 and large type 3 gastric cancer patients selected as candidates for R0 resection by diagnostic staging laparoscopy. Gastric Cancer 2019. [Google Scholar] [CrossRef]
- Shimada, H.; Noie, T.; Ohashi, M.; Oba, K.; Takahashi, Y. Clinical significance of serum tumor markers for gastric cancer: A systematic review of literature by the Task Force of the Japanese Gastric Cancer Association. Gastric Cancer 2013, 17, 26–33. [Google Scholar] [CrossRef]
- Kodera, Y.; Yamamura, Y.; Torii, A.; Uesaka, K.; Hirai, T.; Yasui, K.; Morimoto, T.; Kato, T.; Kito, T. The prognostic value of preoperative serum levels of CEA and CA19-9 in patients with gastric cancer. Am. J. Gastroenterol 1996, 91, 49–53. [Google Scholar]
- Hwang, G.I.; Yoo, C.H.; Sohn, B.H.; Shin, J.H.; Park, Y.L.; Kim, H.D.; Kim, Y.S.; Han, W.K.; Pae, W.K. Predictive Value of Preoperative Serum CEA, CA19-9 and CA125 Levels for Peritoneal Metastasis in Patients with Gastric Carcinoma. Cancer Res. Treat. 2004, 36, e178. [Google Scholar] [CrossRef]
- Dalal, K.M.; Woo, Y.; Kelly, K.; Galanis, C.; Gonen, M.; Fong, Y.; Coit, D.G. Detection of micrometastases in peritoneal washings of gastric cancer patients by the reverse transcriptase polymerase chain reaction. Gastric Cancer 2008, 11, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, H.; Kodera, Y.; Yamamura, Y.; Ito, S.; Kato, T.; Ezaki, T.; Tatematsu, M. Rapid quantitative detection of carcinoembryonic antigen-expressing free tumor cells in the peritoneal cavity of gastric-cancer patients with real-time RT-PCR on the lightcycler. Int. J. Cancer 2000, 89, 411–417. [Google Scholar] [CrossRef]
- Kanetaka, K.; Ito, S.; Susumu, S.; Yoneda, A.; Fujita, F.; Takatsuki, M.; Kuroki, T.; Eguchi, S. Clinical significance of carcinoembryonic antigen in peritoneal lavage from patients with gastric cancer. Surgery 2013, 154, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Lin, S.R.; Lu, C.Y.; Chen, C.C.; Wu, D.C.; Chai, C.Y.; Chen, F.M.; Hsieh, J.S.; Huang, T.J. Gastric cancer cell detection in peritoneal lavage: RT-PCR for carcinoembryonic antigen transcripts versus the combined cytology with peritoneal carcinoembryonic antigen levels. Cancer Lett. 2005, 223, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kodera, Y.; Nakanishi, H.; Yamamura, Y.; Shimizu, Y.; Torii, A.; Hirai, T.; Yasui, K.; Morimoto, T.; Kato, T.; Kito, T.; et al. Prognostic value and clinical implications of disseminated cancer cells in the peritoneal cavity detected by reverse transcriptase-polymerase chain reaction and cytology. Int. J. Cancer 1998, 79, 429–433. [Google Scholar] [CrossRef]
- Nakanishi, H.; Kodera, Y.; Yamamura, Y.; Kuzuya, K.; Nakanishi, T.; Ezaki, T.; Tatematsu, M. Molecular diagnostic detection of free cancer cells in the peritoneal cavity of patients with gastrointestinal and gynecologic malignancies. Cancer Chemother Pharm. 1999, 43, 32–36. [Google Scholar] [CrossRef]
- Nakabayashi, K.; Uraoka, T.; Shibuya, M.; Matsuura, N.; Tsujimoto, M. Rapid detection of CEA mRNA in peritoneal washes using One-Step Nucleic acid Amplification (OSNA®) for gastric cancer patients. Clin. Chim. Acta 2015, 439, 137–142. [Google Scholar] [CrossRef]
- Yamamoto, M.; Baba, H.; Kakeji, Y.; Endo, K.; Ikeda, Y.; Toh, Y.; Kohnoe, S.; Okamura, T.; Maehara, Y. Prognostic Significance of Tumor Markers in Peritoneal Lavage in Advanced Gastric Cancer. Oncology 2004, 67, 19–26. [Google Scholar] [CrossRef]
- Huang, C.; Liu, Z.; Xiao, L.; Xia, Y.; Huang, J.; Luo, H.; Zong, Z.; Zhu, Z. Clinical Significance of Serum CA125, CA19-9, CA72-4, and Fibrinogen-to-Lymphocyte Ratio in Gastric Cancer With Peritoneal Dissemination. Front. Oncol. 2019, 9, e1159. [Google Scholar] [CrossRef] [Green Version]
- Emoto, S.; Ishigami, H.; Yamashita, H.; Yamaguchi, H.; Kaisaki, S.; Kitayama, J. Clinical significance of CA125 and CA72-4 in gastric cancer with peritoneal dissemination. Gastric Cancer 2011, 15, 154–161. [Google Scholar] [CrossRef]
- Nakata, B.; Chung, K.H.-Y.S.; Kato, Y.; Yamashita, Y.; Maeda, K.; Onoda, N.; Sawada, T.; Sowa, M. Serum CA 125 level as a predictor of peritoneal dissemination in patients with gastric carcinoma. Cancer 1998, 83, 2488–2492. [Google Scholar] [CrossRef]
- Ucar, E.; Semerci, E.; Ustun, H.; Yetim, T.; Huzmeli, C.; Gullu, M. Prognostic value of preoperative CEA, CA 19-9, CA 72-4, and AFP levels in gastric cancer. Adv. Ther. 2008, 25, 1075–1084. [Google Scholar] [CrossRef]
- Wang, T.; Wei, Y.; Tian, L.; Song, H.; Ma, Y.; Yao, Q.; Feng, M.; Wang, Y.; Gao, M.; Xue, Y. C-C motif chemokine ligand 5 (CCL5) levels in gastric cancer patient sera predict occult peritoneal metastasis and a poorer prognosis. Int. J. Surg. 2016, 32, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Kodera, Y.; Nakanishi, H.; Ito, S.; Yamamura, Y.; Fujiwara, M.; Koike, M.; Hibi, K.; Ito, K.; Tatematsu, M.; Nakao, A. Prognostic significance of intraperitoneal cancer cells in gastric carcinoma: Detection of cytokeratin 20 mRNA in peritoneal washes, in addition to detection of carcinoembryonic antigen. Gastric Cancer 2005, 8, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Katsuragi, K.; Yashiro, M.; Sawada, T.; Osaka, H.; Ohira, M.; Hirakawa, K. Prognostic impact of PCR-based identification of isolated tumour cells in the peritoneal lavage fluid of gastric cancer patients who underwent a curative R0 resection. Br. J. Cancer 2007, 97, 550–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takebayashi, K.; Murata, S.; Yamamoto, H.; Ishida, M.; Yamaguchi, T.; Kojima, M.; Shimizu, T.; Shiomi, H.; Sonoda, H.; Naka, S.; et al. Surgery-Induced Peritoneal Cancer Cells in Patients Who Have Undergone Curative Gastrectomy for Gastric Cancer. Ann. Surg. Oncol. 2014, 21, 1991–1997. [Google Scholar] [CrossRef]
- Sugita, Y.; Fujiwara, Y.; Taniguchi, H.; Mori, T.; Ishii, T.; Niwa, H.; Okada, Y.; Takiguchi, S.; Yasuda, T.; Yano, M.; et al. Quantitative molecular diagnosis of peritoneal lavage fluid for prediction of peritoneal recurrence in gastric cancer. Int. J. Oncol. 2003, 23, 1419–1423. [Google Scholar] [CrossRef]
- Miki, Y.; Yashiro, M.; Ando, K.; Okuno, T.; Kitayama, K.; Masuda, G.; Tamura, T.; Sakurai, K.; Toyokawa, T.; Kubo, N.; et al. Examination of cancer cells exposed to gastric serosa by serosal stamp cytology plus RT-PCR is useful for the identification of gastric cancer patients at high risk of peritoneal recurrence. Surg. Oncol. 2017, 26, 352–358. [Google Scholar] [CrossRef]
- Fujimura, T.; Ohta, T.; Kitagawa, H.; Fushida, S.; Nishimura, G.-I.; Yonemura, Y.; Elnemr, A.; Miwa, K.; Nakanuma, Y. Trypsinogen expression and early detection for peritoneal dissemination in gastric cancer. J. Surg. Oncol. 1998, 69, 71–75. [Google Scholar] [CrossRef]
- Nakanishi, K.; Kanda, M.; Umeda, S.; Tanaka, C.; Kobayashi, D.; Hayashi, M.; Yamada, S.; Kodera, Y. The levels of SYT13 and CEA mRNAs in peritoneal lavages predict the peritoneal recurrence of gastric cancer. Gastric Cancer 2019. [Google Scholar] [CrossRef]
- Kanda, M.; Shimizu, D.; Tanaka, H.; Tanaka, C.; Kobayashi, D.; Hayashi, M.; Takami, H.; Niwa, Y.; Yamada, S.; Fujii, T.; et al. Synaptotagmin XIII expression and peritoneal metastasis in gastric cancer. Br. J. Surg. 2018, 105, 1349–1358. [Google Scholar] [CrossRef]
- Da, M.-X.; Wu, X.-T.; Guo, T.-K.; Zhao, Z.-G.; Luo, T.; Qian, K.; Zhang, M.-M.; Wang, J. Clinical significance of telomerase activity in peritoneal lavage fluid from patients with gastric cancer and its relationship with cellular proliferation. World J. Gastroenterol. 2007, 13, e3122. [Google Scholar] [CrossRef] [PubMed]
- Mori, N.; Oka, M.; Hazama, S.; Iizuka, N.; Yamamoto, K.; Yoshino, S.; Tangoku, A.; Noma, T.; Hirose, K. Detection of telomerase activity in peritoneal lavage fluid from patients with gastric cancer using immunomagnetic beads. Br. J. Cancer 2000, 83, 1026–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Wu, H.; Zhang, S.; Yuan, H.; Cao, L. Clinical significance of telomerase activity in gastric carcinoma and peritoneal dissemination. J. Int. Med. Res. 2009, 37, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Kakeji, Y.; Maehara, Y.; Koga, T.; Shibahara, K.; Kabashima, A.; Tokunaga, E.; Sugimachi, K. Gastric cancer with high telomerase activity shows rapid development and invasiveness. Oncol. Rep. 2001. [Google Scholar] [CrossRef]
- Rosenberg, R.; Nekarda, H.; Bauer, P.; Schenck, U.; Hoefler, H.; Siewert, J.R. Free peritoneal tumour cells are an independent prognostic factor in curatively resected stage IB gastric carcinoma. Br. J. Surg 2006, 93, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Nekarda, H.; Gess, C.; Stark, M.; Mueller, J.D.; Fink, U.; Schenck, U.; Siewert, J.R. Immunocytochemically detected free peritoneal tumour cells (FPTC) are a strong prognostic factor in gastric carcinoma. Br. J. Cancer 1999, 79, 611–619. [Google Scholar] [CrossRef] [Green Version]
- Lorenzen, S.; Panzram, B.; Rosenberg, R.; Nekarda, H.; Becker, K.; Schenk, U.; Hofler, H.; Siewert, J.R.; Jager, D.; Ott, K. Prognostic significance of free peritoneal tumor cells in the peritoneal cavity before and after neoadjuvant chemotherapy in patients with gastric carcinoma undergoing potentially curative resection. Ann. Surg. Oncol. 2010, 17, 2733–2739. [Google Scholar] [CrossRef]
- Schauer, M.; Peiper, M.; Theisen, J.; Knoefel, W. Prognostic factors in patients with diffuse type gastric cancer (linitis plastica) after operative treatment. Eur. J. Med. Res. 2011, 16, 29–33. [Google Scholar] [CrossRef]
- Ushiku, H.; Yamashita, K.; Ema, A.; Minatani, N.; Kikuchi, M.; Kojo, K.; Yokoi, K.; Tanaka, T.; Nishizawa, N.; Ishii, S.; et al. DNA diagnosis of peritoneal fluid cytology test by CDO1 promoter DNA hypermethylation in gastric cancer. Gastric Cancer 2017, 20, 784–792. [Google Scholar] [CrossRef]
- Iida, T.; Iwahashi, M.; Katsuda, M.; Ishida, K.; Nakamori, M.; Nakamura, M.; Naka, T.; Ojima, T.; Ueda, K.; Hayata, K.; et al. Prognostic significance of IL-17 mRNA expression in peritoneal lavage in gastric cancer patients who underwent curative resection. Oncol. Rep. 2014, 31, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Sakakura, C.; Takemura, M.; Hagiwara, A.; Shimomura, K.; Miyagawa, K.; Nakashima, S.; Yoshikawa, T.; Takagi, T.; Kin, S.; Nakase, Y.; et al. Overexpression of dopa decarboxylase in peritoneal dissemination of gastric cancer and its potential as a novel marker for the detection of peritoneal micrometastases with real-time RT–PCR. Br. J. Cancer 2004, 90, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Yonemura, Y.; Fujimura, T.; Ninomiya, I.; Kim, B.S.; Bandou, E.; Sawa, T.; Kinoshita, K.; Endo, Y.; Sugiyama, K.; Sasaki, T. Prediction of peritoneal micrometastasis by peritoneal lavaged cytology and reverse transcriptase-polymerase chain reaction for matrix metalloproteinase-7 mRNA. Clin. Cancer Res. 2001, 7, 1647–1653. [Google Scholar]
- Li, Z.; Zhang, D.; Zhang, H.; Miao, Z.; Tang, Y.; Sun, G.; Dai, D. Prediction of peritoneal recurrence by the mRNA level of CEA and MMP-7 in peritoneal lavage of gastric cancer patients. Tumour Biol. 2014, 35, 3463–3470. [Google Scholar] [CrossRef]
- Zeng, R.; Li, B.; Huang, J.; Zhong, M.; Li, L.; Duan, C.; Zeng, S.; Huang, J.; Liu, W.; Lu, J.; et al. Lysophosphatidic Acid is a Biomarker for Peritoneal Carcinomatosis of Gastric Cancer and Correlates with Poor Prognosis. Genet. Test. Mol. Biomark. 2017, 21, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Suzuki, T.; Uozaki, H.; Nakanishi, H.; Ueda, T.; Matsuno, Y.; Kodera, Y.; Sakamoto, H.; Yamamoto, N.; Sasako, M.; et al. Detection of Minimal Gastric Cancer Cells in Peritoneal Washings by Focused Microarray Analysis with Multiple Markers: Clinical Implications. Ann. Surg. Oncol. 2007, 14, 1694–1702. [Google Scholar] [CrossRef] [PubMed]
- Ohzawa, H.; Saito, A.; Kumagai, Y.; Kimura, Y.; Yamaguchi, H.; Hosoya, Y.; Lefor, A.K.; Sata, N.; Kitayama, J. Reduced expression of exosomal miR29s in peritoneal fluid is a useful predictor of peritoneal recurrence after curative resection of gastric cancer with serosal involvement. Oncol. Rep. 2020, 43, 1081–1088. [Google Scholar]
- Hu, Q.; Masuda, T.; Sato, K.; Tobo, T.; Nambara, S.; Kidogami, S.; Hayashi, N.; Kuroda, Y.; Ito, S.; Eguchi, H.; et al. Identification of ARL4C as a Peritoneal Dissemination-Associated Gene and Its Clinical Significance in Gastric Cancer. Ann. Surg. Oncol. 2017, 25, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.G.; Nam, S.W.; Kim, T.Y.; Kim, Y.S.; Kim, C.J.; Park, J.Y.; Lee, J.H.; Kim, H.S.; Lee, J.W.; Park, C.H.; et al. Overexpression of S100A4 is closely related to the aggressiveness of gastric cancer. APMIS 2003, 111, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Ye, Z.Y.; Zhao, Z.S.; Tao, H.Q.; Chu, Y.Q. High-level expression of S100A4 correlates with lymph node metastasis and poor prognosis in patients with gastric cancer. Ann. Surg. Oncol. 2010, 17, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.J.; Park, S.; Kim, M.H.; Nam, C.M.; Kim, H.; Choi, Y.Y.; Jung, M.K.; Choi, H.J.; Rha, S.Y.; Chung, H.C. Mesothelin Expression Is a Predictive Factor for Peritoneal Recurrence in Curatively Resected Stage III Gastric Cancer. Oncologist 2019. [Google Scholar] [CrossRef] [Green Version]
- Kanda, M.; Shimizu, D.; Tanaka, H.; Tanaka, C.; Kobayashi, D.; Hayashi, M.; Iwata, N.; Niwa, Y.; Yamada, S.; Fujii, T.; et al. Significance of SYT8 For the Detection, Prediction, and Treatment of Peritoneal Metastasis From Gastric Cancer. Ann. Surg. 2018, 267, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Sawaki, K.; Kanda, M.; Miwa, T.; Umeda, S.; Tanaka, H.; Tanaka, C.; Kobayashi, D.; Suenaga, M.; Hattori, N.; Hayashi, M.; et al. Troponin I2 as a Specific Biomarker for Prediction of Peritoneal Metastasis in Gastric Cancer. Ann. Surg. Oncol. 2018, 25, 2083–2090. [Google Scholar] [CrossRef]
- Virgilio, E.; Giarnieri, E.; Giovagnoli, M.R.; Montagnini, M.; Proietti, A.; D’Urso, R.; Mercantini, P.; Valabrega, S.; Balducci, G.; Cavallini, M. Gastric Cancer Cells in Peritoneal Lavage Fluid: A Systematic Review Comparing Cytological with Molecular Detection for Diagnosis of Peritoneal Metastases and Prediction of Peritoneal Recurrences. Anticancer Res. 2018, 38, 1255–1262. [Google Scholar] [PubMed] [Green Version]
- Yamaguchi, H.; Satoh, Y.; Ishigami, H.; Kurihara, M.; Yatomi, Y.; Kitayama, J. Peritoneal Lavage CEA mRNA Levels Predict Conversion Gastrectomy Outcomes after Induction Chemotherapy with Intraperitoneal Paclitaxel in Gastric Cancer Patients with Peritoneal Metastasis. Ann. Surg. Oncol. 2017, 24, 3345–3352. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Shi, C.; Huang, X.; Zheng, J.; Zhu, Z.; Li, Q.; Qiu, S.; Huang, Z.; Zhuang, Z.; Wu, R.; et al. Molecular Profiles and Metastasis Markers in Chinese Patients with Gastric Carcinoma. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Thadi, A.; Khalili, M.; Morano, W.F.; Richard, S.D.; Katz, S.C.; Bowne, W.B. Early Investigations and Recent Advances in Intraperitoneal Immunotherapy for Peritoneal Metastasis. Vaccines (Basel) 2018, 6, 54. [Google Scholar] [CrossRef] [Green Version]
- Bebnowska, D.; Grywalska, E.; Niedzwiedzka-Rystwej, P.; Sosnowska-Pasiarska, B.; Smok-Kalwat, J.; Pasiarski, M.; Gozdz, S.; Rolinski, J.; Polkowski, W. CAR-T Cell Therapy-An Overview of Targets in Gastric Cancer. J. Clin. Med. 2020, 9, 1894. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Biomarker | Prognostic (Survival) | Diagnostic | Sample Type | Possible Assay Type for Biomarker Assessment | Reference |
|---|---|---|---|---|---|
| CEA | Positive | Positive | Serum, peritoneal lavage | IR, RT-PCR | [88,89,90,91,92,93,94,95,96,97,98] |
| CA12-5 | Positive | Positive | Serum, peritoneal lavage | IR | [90,99,100,101] |
| CA19-9 | Positive | Positive | Serum | IR | [88,89,99,102] |
| CA72-4 | Positive | Positive | Serum | IR | [88,99,102] |
| CCL5 | Positive | Positive | Serum, GC | IR, IHC | [103] |
| CK20, CEA | Positive | Positive | GC, Peritoneal lavage | RT-PCR | [104,105,106,107,108] |
| Trypsinogen-1 | TBD | Positive | GC, peritoneal lavage | IHC, RT-PCR | [109] |
| SYT13 | Positive | Positive | GC, peritoneal lavage | RT-PCR | [110,111] |
| Telomerase activity | TBD | Positive | GC, Peritoneal lavage | TRAP assay | [112,113,114,115] |
| Ber-EP4 | Positive | Positive | Peritoneal lavage | ICC | [116,117,118,119] |
| CDO1 gene promoter DNA methylation | Positive | Positive | Peritoneal lavage | quantitative methylation specific PCR | [120] |
| IL-17 | Positive | Positive | Peritoneal lavage | RT-PCR | [121] |
| Dopa decarboxylase | TBD | Positive | Peritoneal lavage | RT-PCR | [122] |
| MMP-7 | Positive | Positive | Peritoneal lavage | RT-PCR | [123,124] |
| Lysophosphatidic acid | Positive | Positive | Peritoneal lavage | RT-PCR | [125] |
| CEA, CK20, survivin and MUC2 | TBD | Positive | Peritoneal lavage | RT-PCR | [91] |
| CK20, FABP1, MUC2, TFF1 and MASPIN | Positive | TBD | Peritoneal lavage | ICC | [126] |
| Exosomal miR-29s | Positive | TBD | Peritoneal lavage | RT-PCR | [127] |
| ARL4C | Positive | Positive | GC | RT-PCR, IHC | [128] |
| S100A4 | Positive | Positive | GC | RT-PCR, IHC | [129,130] |
| Mesothelin | Positive | TBD | GC | IHC | [131] |
| SYT8 | Positive (PM-free survival) | Positive | GC | RT-PCR, IHC | [132] |
| Troponin I2 | Positive (PM-free survival) | Positive | GC | RT-PCR | [133] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Zhou, Q.; Wang, H.; Zhuo, W.; Ding, Y.; Lu, J.; Wu, G.; Xu, N.; Teng, L. Predicting Peritoneal Dissemination of Gastric Cancer in the Era of Precision Medicine: Molecular Characterization and Biomarkers. Cancers 2020, 12, 2236. https://doi.org/10.3390/cancers12082236
Chen Y, Zhou Q, Wang H, Zhuo W, Ding Y, Lu J, Wu G, Xu N, Teng L. Predicting Peritoneal Dissemination of Gastric Cancer in the Era of Precision Medicine: Molecular Characterization and Biomarkers. Cancers. 2020; 12(8):2236. https://doi.org/10.3390/cancers12082236
Chicago/Turabian StyleChen, Yanyan, Quan Zhou, Haiyong Wang, Wei Zhuo, Yongfeng Ding, Jun Lu, Guanghao Wu, Nong Xu, and Lisong Teng. 2020. "Predicting Peritoneal Dissemination of Gastric Cancer in the Era of Precision Medicine: Molecular Characterization and Biomarkers" Cancers 12, no. 8: 2236. https://doi.org/10.3390/cancers12082236