1. Introduction
The prevalence of overweight and obesity has risen substantially in the past three decades. A recent survey showed that the worldwide prevalence of overweight and obesity increased by 27.5% for adults and 47.1% for children between 1980 and 2013, with the number of overweight and obese individuals soaring from 857 million to 2.1 billion during the same period [
1]. Obesity is associated with a multitude of chronic medical conditions, including type 2 diabetes, heart disease, hypertension, stroke, and certain types of cancer [
2]. In 2010, overweight and obesity were estimated to have caused 3.4 million deaths, 4% of years of life lost, and 4% of disability-adjusted life-years worldwide [
3]. Given its substantial increase in prevalence and associated health risks, obesity has become a major global health challenge. It is influenced by various factors, including genetic predisposition, variations in nutrient intake, and behavioral and environmental factors [
4]. The important contribution of macronutrient intake to obesity has become better recognized [
5]. In addition, recent studies have suggested that certain micronutrients may also be associated with increased body fat accumulation [
6,
7,
8].
Selenium (Se) is a nutritionally essential trace element and naturally presents in many foods. Its biological effect is exerted via incorporation into selenoproteins, which play a critical role in reproduction, thyroid hormone metabolism, DNA synthesis, and protection from oxidative stress and inflammation [
9]. There is abundant evidence linking low Se status with the development of several chronic diseases, including cardiovascular disease [
10,
11], cancer [
12,
13], and diabetes [
14,
15,
16].
Some studies have suggested that Se may also inhibit adipocyte hypertrophy and adipogenesis [
17,
18]. Furthermore, biomarkers of Se nutrition status including serum Se levels as well as the activity of the important selenoprotein, glutathione peroxidase (GPx), may be associated with obesity [
19,
20,
21]. However, existing data were obtained mainly as byproducts from a few studies originally designed to study diabetes and cancer rather than obesity. In addition, the reported results were inconsistent. Obesity status in all studies was estimated by body mass index (BMI) or waist circumference (WC), which have limited accuracy in measuring body fat [
22]. Dual-energy X-ray absorptiometry (DXA) can accurately determine the quantity and distribution of body fat with a low margin of error [
22]. Moreover, many critical confounding factors potentially affecting both dietary Se intake and body composition have been poorly controlled. To date, no studies specifically designed to investigate the relationship between dietary Se intake and systematic measures of obesity have been completed.
Therefore, we designed the present study to investigate the relationship between dietary Se intake and a panel of body composition parameters, measured by DXA, in a large population-based study with systematic control of major confounding factors.
2. Subjects and Methods
2.1. Subjects
All participants were from the ongoing CODING (Complex Diseases in the Newfoundland population: Environment and Genetics) study [
22,
23,
24,
25,
26]. Eligibility for the CODING study was based on the following inclusion criteria: (1) ≥19 years of age; (2) at least a third generation Newfoundlander; (3) without serious metabolic, cardiovascular, or endocrine diseases; and (4) not pregnant at the time of the study. Ethics approval was obtained from the Health Research Ethics Authority, Memorial University, St. John’s, NL, Canada, with Project Identification Code #10.33 (latest date of approval: 21 January 2015). All subjects provided written and informed consent before participation in this study. Detailed information regarding the CODING Study was reported in our previously published papers [
22,
23,
24,
25,
26].
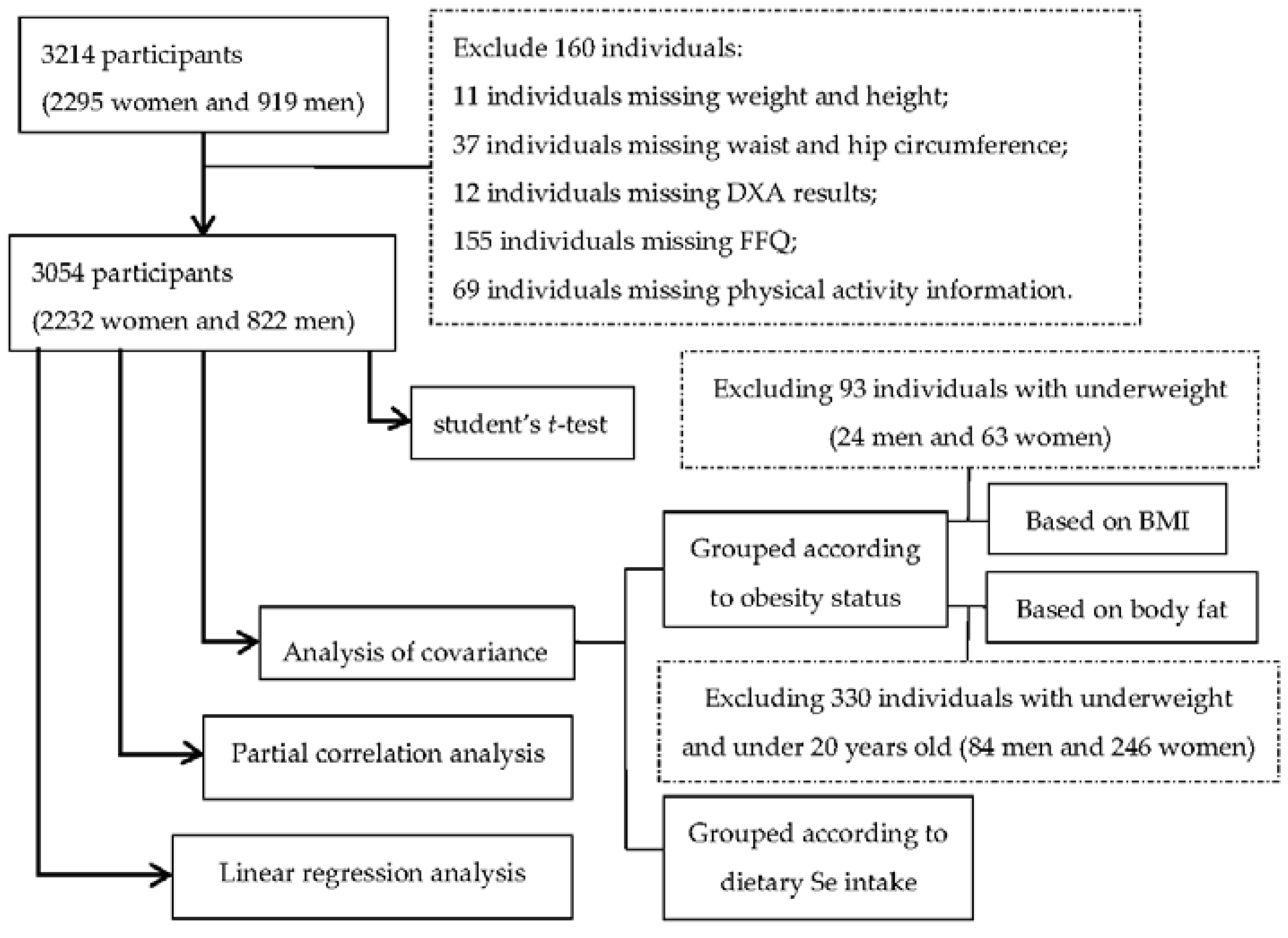
A total of 3214 participants including 2295 women and 919 men were initially included. Among them 160 individuals were excluded due to incomplete or missing data, including weight and height for 11 individuals, waist and hip circumference for 37 individuals, DXA results for 12 individuals, food frequency questionnaire (FFQ) for 155 individuals, and physical activity information for 69 individuals (
Figure 1).
Figure 1.
Flow-chart of subject selection for analyses.
Figure 1.
Flow-chart of subject selection for analyses.
2.2. Anthropometric Measurements
Anthropometrics were measured following a 12-h overnight fast. Trained personnel obtained anthropometric measurements for each subject using standard procedures. Standing height was measured using a fixed stadiometer (to the nearest 0.1 cm). After fully emptying their bladders, subjects wore standard hospital gowns for all weight measurements using a platform manual scale balance (Health O Meter, Bridgeview, IL, USA; nearest 0.1 kg). BMI (kg/m2) was calculated as weight in kilograms divided by height squared in meters. WC was measured at the midway point between the iliac crest and the lower rib, and hip by the maximum circumference over the buttocks below the iliac crest. Waist-hip ratio (WHR) was determined by dividing WC by hip circumference.
2.3. Body Composition Measurements
Body composition measurements, including total body fat percentage (BF%), trunk fat percentage (TF%), android fat percentage (AF%), and gynoid fat percentage (GF%), were taken in a supine position, utilizing DXA (Lunar Prodigy; GE Medical Systems, Madison, WI, USA) with the Lunar Prodigy software system, which has the capacity to distinguish each of these regions. The trunk fat region is measured from the top of the shoulders to the top of the iliac crest, the android fat region is represented by the distance from the top of the second lumbar vertebra to the top of the iliac crest, and the gynoid fat region extends down the iliac crest twice the height of the android area. The enCORE (Version 12.2, 2008, GE Medical Systems) software package was used for DXA data acquisition. Daily quality assurance was performed on the DXA scanner, and the typical coefficient of variation was 1.3% during the study period [
23,
24,
25,
26].
2.4. Dietary Assessment
Dietary intake for each participant was assessed by using a 124-item semi-quantitative Willett FFQ [
27], which is one of the most commonly used dietary questionnaires for large scale epidemiological studies [
28]. The Willett FFQ asks subjects to indicate the number of weekly servings of common food items consumed over the past 12 months. The FFQ was completed by each participant at the date of appointment. The NutriBase Clinical Nutrition Manager (version 8.2.0; CybersoftInc, Phoenix, AZ, USA) software package was used to convert weekly serving values into mean daily serving values to calculate the total daily intakes of calorie (kcal/day) and Se (μg/day) for each individual [
23,
25]. Dietary Se intake was expressed as per kilogram body weight (μg/kg/day).
2.5. Physical Activity Assessment and Other Information
Physical activity patterns were measured using the ARIC Baecke Questionnaire, which consists of a Work Index, Sports Index, and Leisure Time Activity Index [
23,
25]. In addition, all participants completed a self-administered screening questionnaire, which was used to collect information about their personal health history. Women completed an additional questionnaire regarding menstrual history and menopausal status (pre- or post-menopausal).
2.6. Data Analyses
All data are presented as mean ± standard error (SE). Calorie and dietary Se intake were log-transformed to normalize data distributions to perform effective statistical analysis. Anthropometrics, body composition, dietary intake and physical activity were compared between men and women using independent student’s t-test.
According to the criteria recommended by the World Health Organization [
29], obesity status was categorized based on BMI, as normal weight (18.5–24.9 kg/m
2), overweight (25.0–29.9 kg/m
2), or obese (≥30 kg/m
2). Obese subjects were further classified into three subgroup: obese class I (30.0–34.9 kg/m
2), obese class II (35.0–39.9 kg/m
2), and obese class III (≥40.0 kg/m
2). The number of underweight subjects (BMI < 18.5kg/m
2) was too small (
n = 93, men/women = 24/69) to perform meaningful statistical analysis, so they were excluded from the analysis (
Figure 1). Subjects were also divided into three groups based on body fat percentage according to age and gender specific criteria recommended by Bray [
30]. Underweight subjects were excluded from the analysis due to their small numbers, and subjects under 20 years of age were also excluded due to lack of available criteria for this age group (
Figure 1). Dietary Se intake was analyzed by analysis of variance and covariance controlling for age, total calorie intake and physical activity. Analyses on obesity measurements were performed when participants were divided into tertiles (low, medium, or high) based on dietary Se intake using analysis of variance and covariance controlling for age, total calorie intake and physical activity.
Partial correlation analysis controlling for age, total calorie intake, and physical activity was subsequently applied to determine the correlation between dietary Se intake and obesity measurements in both men and women, and also in obese groups separately. To overcome the possible influence of smoking, alcohol consumption, medication use, and menopausal status, participants were also divided into subgroups according to smoking status (yes or no), alcohol consumption (yes or no) and medication use (yes or no). Women were further divided into pre- or post-menopausal groups according to their menopausal status.
Finally, stepwise multiple linear regression analysis was used to evaluate the contribution of dietary Se intake to obesity among women or men. Weight, BMI, WC, WHR, TF%, AF%, GF%, and BF% were used as dependent variables and dietary Se intake, age, total calorie intake and physical activity were used as independent variables.
All statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). All tests were two-sided and a p < 0.05 was considered to be statistically significant.
4. Discussion
To the best of our knowledge, this is the first study specifically designed to examine the association between dietary Se intake and a full panel of obesity measurements with systematic control of major confounding factors in a large adult population. The most significant finding in the present study was that obesity and degree of obesity were associated with low dietary Se intake in the general adult population. Every 1 μg/kg/day increase in dietary Se intake corresponded to a 3%–6% decrease in body fat percentage.
To date, there is only one reported cross-sectional study evaluating the relationship between dietary Se intake and obesity in school children aged 8–13 years old [
32]. In that study, children with BMI >85th percentile had significantly lower dietary Se intake (μg/kg/day) than normal weight children, after adjusting for energy intake. The remaining studies evaluated the association with other biological samples rather than dietary Se intake. Data were extrapolated from nutrition surveys or studies designed to examine the relationship between Se and cardiovascular disease, diabetes or cancer. For example, data from the 1999 to 2004 US National Health and Nutrition Examination Survey (NHANES) showed that children at high risk of overweight were also at greater risk of dietary Se deficiency [
33]. In a survey from the NHANES 2003–2004, subjects were divided into quartiles based on serum selenium, and BMI decreased and dietary Se intake (μg/day) increased with increasing serum Se levels [
34]. A positive correlation between serum Se concentration and dietary Se intake (μg/day) was found, and a negative correlation between serum Se and BMI was reported [
32,
35]. Similar findings were revealed in a cancer study in Northern Italy [
36]. Additionally, an adverse association between anthropometric measurements and serum/plasma Se levels has been reported [
19,
20,
21,
37,
38,
39].
A variety of factors may affect body composition and dietary Se intake, including age, total dietary calorie intake and physical activity. Body composition, food choice and intake may change with age, making this an important confounding factor to be controlled for in analysis [
40]. Higher dietary calorie intake is a central risk factor for obesity, and is significantly correlated with dietary Se intake as well [
41]. This was observed in the present study (
r 0.13 to 0.27, not shown). Physical activity is likely one of the most important variables determining the amount of body fat [
42]. In addition, there are notable gender differences in the amount of body fat and fat distribution. On average, women have 12% more body fat than men in the Newfoundland population [
26]. Difference in food consumption also exists between men and women [
43]. Therefore, separate analyses were performed for men and women to eliminate the effect of gender on our results. In women, menopause results in profound hormonal changes, which may predispose to increased adiposity—a factor we also considered in our study [
44]. We found a similar correlation between dietary Se intake and body composition in both premenopausal and postmenopausal women. Smoking, alcohol consumption and medication use are potentially important covariates as well, since they may affect appetite and body weight regulation [
45,
46]. After separating the subjects according to these covariates, the association between dietary Se intake and body composition remained significant. It should be noted that the systematic control of major confounding factors in this study enabled us obtaining accurate and reliable findings.
The effect of dietary Se intake on body fat is supported by data from animal interventional experiments. Wang
et al. [
47] found that body weight significantly decreased and the ratio of adipose to body weight dropped when rats were treated with high doses of Se (200 μg/kg/day). This was due to enhanced lipolysis in adipose tissue and hepatic accumulation free fatty acids. Netto
et al. [
48] obtained a similar result. However, two small interventional studies in healthy human volunteers revealed contradictory findings [
49,
50]. In the study carried out by Hawkes
et al. [
49], body weight increased in the high Se group (297 μg/day) while weight decreased in the low Se group (14 μg/day) after 64 days of treatment, although energy intake was the same in both groups (5
vs. 6 in each group). In the study conducted by Navas-Carretero
et al. [
50], consumption of Se-enriched chicken (11 subjects) did not result in more weight loss than consumption of Se-non-enriched chicken (13 subjects). However caution must be exercised in interpreting these results, as the very small sample size may have contributed to this discrepancy.
The second major finding in our study is that the beneficial association between dietary Se intake and body fat is not only significant in normal and overweight subjects but also in obese individuals. This finding supports the theory that appropriate dietary Se supplementation may be useful in the battle against obesity. Se supplementation would be a simple and cost-efficient intervention for both overweight and obese individuals. It should be emphasized, however, that the low dietary Se intake in obese individuals may be a consequence of long-term consumption of high-fat and high-sugar foods, as well as more sugar-sweetened beverages [
51]. Such foods are typically low in Se content, and are negatively correlated with serum Se [
52].
At present, the mechanisms underlying this beneficial effect of dietary Se on body fat remain largely unclear. However, evidence linking Se with adipogenesis does exist. Some earlier studies have utilized Se in the differentiation of primary pig and rat preadipocytes, as well as chicken embryonic fibroblasts, suggesting that Se may have proadipogenic potential [
53,
54]. However, a recent study showed that Se also inhibits adipogenesis through reduction of mRNA expression of peroxisome proliferator-activated receptor-γ and fatty acid synthase, while activating expression of transforming growth factor-β [
18]. Furthermore, intra-peritoneal injections of sodium selenite reduce abdominal fat accumulation and adipocyte size in OLETF rats, supporting the anti-adipogenic role of Se
in vivo [
17].
In our study, dietary Se intake was expressed as μg/kg/day in all analyses. With substantial variations in body weight in the general human population, individuals of different body weight have different Se requirements. Therefore, one concern when Se is expressed as μg/day and large variations in body weight are not adjusted for in analysis is that results will be confounded. Consequently we included weight-based selenium intake (μg/kg/day) to eliminate this potential confounder. Furthermore, DXA measurement of body fat is more accurate than BMI and other field methods and best represents body adipose tissue with a low margin of error [
22]. Our use of DXA in the entire study contributed to the reliability of our findings.
Nevertheless, several possible limitations exist in the presented study because it is a population-based association study. The cross-sectional study design does not allow the determination of cause and effect. Secondly, the current version of DXA analysis software does not specifically measure visceral fat, and so any possible association between dietary Se intake and visceral fat could not be determined. Therefore, further research investigating the association between dietary Se and central adiposity is required. Dietary Se is not the only marker of Se nutritional status; serum Se, GPx activity, and selenoprotein
p are all important considerations. Further studies are needed to more closely evaluate their potential role—either alone or as a functional group if all measurements are available [
55,
56]. Finally, the FFQ is designed to assess habitual dietary intake by determining the frequency with which specific food items are consumed over a reference period. It is the most widely used dietary assessment method in large-scale epidemiological studies on macro- and micro-nutrient intakes. Moreover, the FFQ has been used to estimate dietary Se intake in previous studies [
57,
58,
59,
60]. However, it may not be as accurate for quantification of micronutrient intake, as compared with macronutrient intake [
61].

 ,
, 

{kind=link}