
The Role of Amino Acids in the Diagnosis, Risk Assessment, and Treatment of Breast Cancer: A Review



1
Biochemistry Research Laboratory, Omsk State Pedagogical University, 644099 Omsk, Russia
2
Department of Mathematics and Mathematics Teaching Methods, Omsk State Pedagogical University, 644043 Omsk, Russia
*
Author to whom correspondence should be addressed.
Curr. Issues Mol. Biol. 2023, 45(9), 7513-7537; https://doi.org/10.3390/cimb45090474
Submission received: 29 August 2023
/
Revised: 5 September 2023
/
Accepted: 12 September 2023
/
Published: 13 September 2023
(This article belongs to the Special Issue Advanced Molecular Solutions for Cancer Therapy)
Abstract
:This review summarizes the role of amino acids in the diagnosis, risk assessment, imaging, and treatment of breast cancer. It was shown that the content of individual amino acids changes in breast cancer by an average of 10–15% compared with healthy controls. For some amino acids (Thr, Arg, Met, and Ser), an increase in concentration is more often observed in breast cancer, and for others, a decrease is observed (Asp, Pro, Trp, and His). The accuracy of diagnostics using individual amino acids is low and increases when a number of amino acids are combined with each other or with other metabolites. Gln/Glu, Asp, Arg, Leu/Ile, Lys, and Orn have the greatest significance in assessing the risk of breast cancer. The variability in the amino acid composition of biological fluids was shown to depend on the breast cancer phenotype, as well as the age, race, and menopausal status of patients. In general, the analysis of changes in the amino acid metabolism in breast cancer is a promising strategy not only for diagnosis, but also for developing new therapeutic agents, monitoring the treatment process, correcting complications after treatment, and evaluating survival rates.
1. Introduction
Breast cancer (BC) remains the leading malignant neoplasm in women and the second leading cause of death from cancer among women worldwide [1,2]. Treatment for breast cancer has improved in recent years, but its high mortality remains a concern. Existing treatments for breast cancer often lead to intractable drug resistance. Therefore, the need for methods of early diagnosis and the identification of risk factors and groups are still relevant tasks. To solve these problems, scientists began to study the metabolic pathway in breast cancer. The connection between breast cancer and metabolic pathways may also lead to the discovery of new therapeutic possibilities and targets [3,4].
Recently, much attention has been paid to metabolomics as an effective tool for differentiating samples from patients with breast cancer from normal samples [5,6,7,8,9,10,11]. For example, a statistically significant difference in 24 metabolites in breast cancer compared with the control group was found by Dougan et al. [12], and a statistically significant difference in 78 metabolites was confirmed by Shen et al. [8]. Interestingly, the levels of metabolites are unique for different types of cancer, which could be a new way to classify tumors [13]. Jobard et al. identified nine metabolites to differentiate between metastatic and early breast cancer, although a separation of breast cancer phenotypes based on metabolomics is still controversial [14,15]. Several metabolomic studies of plasma/serum breast cancer have been performed, mainly aimed at distinguishing between the subtypes of breast cancer [16], metastatic breast cancer [8,14,17,18,19,20], recurrence [21,22], response to neoadjuvant chemotherapy [23,24], etc. An important part of the metabolomic profile, which makes it possible to discriminate between BC patients and healthy controls, is represented by amino acids. Amino acids in breast cancer are determined in the tissue [25,26,27], serum [7,28,29,30], plasma [6,31,32,33,34], saliva [35,36,37,38], and urine [39,40,41]. Amino acids not only play a vital role in the synthesis of biological molecules such as proteins in malignant cancer cells, but they are also important metabolites for immune cell activation and antitumor activity in the tumor microenvironment. Abnormal changes in the amino acid metabolism are closely associated with the onset and development of tumors and immunity [42]. An amino acid can supply sources of nitrogen and carbon for biosynthesis or satisfy the energy requirement for the rapid growth of tumor cells [43].
In this review, we focus on the role of amino acids in the diagnosis, risk assessment, imaging, and treatment of breast cancer.
2. Diagnostic Value of Determination of Amino Acids in Biological Fluids
2.1. Amino Acid Composition of Serum and Blood Plasma in Breast Cancer
The determination of the content of amino acids in serum and blood plasma was carried out in a large number of studies (Table 1).
For example, Kubota et al. showed that in breast cancer, the total content of amino acids (TAA) in plasma increases (3035 ± 118 vs. 2529 ± 115 nmol/mL), as do the contents of all major groups of amino acids: essential amino acids (EAAs), branched-chain amino acids (BCAAs), aromatic amino acids (AAAs), and gluconeogenic amino acids (GAAs) [44]. Similarly, a number of studies have also noted an increase in the amino acid content compared to healthy controls [50,61]. According to other data, in patients with breast cancer, a decrease in the plasma levels of branched-chain amino acids (BCAAs) was observed [57]. Lai et al. [62] showed that a decrease in the content of seven amino acids (Ala, His, Thr, Arg, Pro, Glu, and Gly) occurs more than six times more often than their increase. In this regard, it is noteworthy that these seven amino acids play more important roles than others during changes in the protein metabolism in cancer patients. In a review by Yang et al., an analysis of the most common biomarkers of breast cancer was carried out [63]. Based on clinical metabolic studies, Tyr and Ala shared the highest frequency, indicating that they may be sensitive metabolites in the diagnosis of breast cancer. Other amino acids are mentioned less frequently, and the frequency of occurrence decreases in the following order: Tyr (6/6), Ala (6/5), Glu (6/4), Val (4/6), Phe (5/4), Gln (4/5), Lys (3/6), Ile (4/4), His (3/4), Gly (4/2), Arg (3/3), Asn (4/2), Pro (3/3), Ser (5/1), Leu (2/4), Trp (1/5), Thr (2/3), Asp (3/1), Orn (2/2), and Cys (2/2). It should be noted that in different studies, the level of amino acids changes in different directions: the first digit corresponds to up-regulation, and the second digit corresponds to down-regulation [63]. Thus, the existing data from the literature provide conflicting information about the nature of changes in the content of amino acids in breast cancer.
In different studies, both the contents of individual amino acids and the complete amino acid profile of plasma and/or serum were evaluated. It has been shown, for example, that the arginine levels were significantly lower and the ornithine levels were significantly higher in breast cancer patients than in control patients [64]. Differences between breast cancer cases and controls were observed for the levels of Trp, Thr, Ala, Gly, Pro, Ile, Leu, and Val [34]. Miyagi et al. observed significant changes in the amino acid profiles between cancer patients and controls. They found that the concentrations of Thr, Pro, Ser, Gly, Ala, and Orn were significantly higher, but the concentrations of Gln, Trp, His, Phe, and Tyr were significantly lower compared to the control. Compared with the data from Lai et al., they found similarities in decreasing His and Gln levels and increasing Pro and Ala levels in breast cancer patients. Budczies et al. demonstrated that changes in the amino acid metabolism were associated with at least a 1.9-fold increase in 16 amino acids in breast cancer compared with healthy breast tissue [50,65].
The summarized results on the amino acid composition of serum/plasma in breast cancer compared with healthy controls are shown in Table 1.
To compare the change in the contents of individual amino acids in breast cancer according to different authors, we compared the relative contents of amino acids in relation to healthy controls (Table 2). It can be seen that a significant change in the concentration is rarely observed, for example, an increase in the contents of Arg [52,56], Thr [52], and Ser [33] by 2 times, a decrease in the content of Asp by 1.5 times [46,56], etc. In most cases, the change in concentration is up to 10–15% compared to the control. We calculated the average change in concentration and the interval of variation for each amino acid and plotted them on a diagram (Figure 1). Thus, it is possible to assess the nature of changes in the concentrations of individual amino acids in breast cancer.
It can be seen that for some amino acids (Thr, Arg, Met, and Ser), an increase in concentration is more often observed in breast cancer compared with a healthy control, and for other amino acids, a decrease is observed (Asp, Pro, Trp, and His) (Figure 1). However, in each case, to assess the change in the amino acid profile, it is necessary to take into account the characteristics of the sample due to the high heterogeneity of breast cancer.
The construction of the ROC curve makes it possible to assess the classification accuracy for separating BC patients from healthy controls. According to Park et al. [53], for Lys, His, Thr, and Trp, the area under the curve varies in the range of 0.527–0.583; for Leu/Ile, the area is 0.728; for Phe, the area is 0.838; and for 5-hydroxyproline, the area is 0.968 on the training set. However, in the test set for 5-hydroxyproline, the area under the curve decreases to 0.744. With the simultaneous evaluation of many metabolites, which include amino acids, the accuracy of diagnosis increases. Thus, An et al. [56] showed that with the simultaneous evaluation of 47 metabolites using the random forest method, AUC values of 0.998 were obtained. Jasby et al. [6], using 30 metabolites, showed that AUC = 0.89 (95% CI: 0.85–0.93), sensitivity = 0.80, and specificity = 0.75. Baranovicova et al. [57] showed that AUC > 0.91 for 10 metabolites, while only for the BCAAs, AUC = 0.733. Only for the combination of 10 amino acids, Han et al. [58] showed that AUC = 0.91. Thus, individual amino acids have a low diagnostic value for the detection of breast cancer, while combinations of a number of amino acids with each other or with other metabolites provide a higher accuracy. However, in each specific case, it is necessary to check the data obtained during the construction of the model on a test sample in order to obtain an objective idea of the diagnostic capabilities of the algorithm.
2.2. Features of the Amino Acid Composition of Serum/Plasma in Different Molecular Biological Subtypes of Breast Cancer
In a number of studies, special attention was paid to the influence of the molecular biological characteristics of breast cancer on the amino acid profile of blood serum/plasma. Thus, Ala had a significant difference between ER-positive and ER-negative breast cancer [16,66]. Fan Y. identified a panel of eight potential low-molecular-weight biomarkers for diagnosing breast cancer subtypes, which included three amino acids: Pro, Ala, and Val [16]. Elevated Pro levels (FC = 1.217, p = 0.007) may indicate the suppression of proline oxidase in the human growth factor receptor 2 (HER2) positive group [67]. Ala was the most significantly reduced metabolite (FC = 0.544, p < 0.001) in the ER-positive participants compared to the ER-negative group [66]. Val was significantly increased in the HER2-positive groups compared to the HER2-negative groups, but was markedly decreased in the ER-positive groups compared to the ER-negative groups. Val anomalies indicated a violation of energy supply in the HER2-positive (fold change = 1.187, p = 0.002) and ER-positive (fold change = 0.682, p < 0.001) patients. The authors emphasized the clinical predictive potential of the identified eight biomarkers for breast cancer subtypes. An average prediction accuracy of 88.5% (95% CI 83.3–93.7%) was obtained for the training set and an average prediction accuracy of 85.6% (95% CI 80.9–90.1%) was obtained for the test set.
Han et al. [58] studied TNBC (tumor control) as well as the non-malignant pathologies of mammary glands. Four amino acids (Phe, Tyr, Ser, and Arg) were found to be more common in the triple-negative breast cancer (TNBC) group, while six amino acids (Pro, Trp, Val, Thr, Ala, and His) were more common in the benign group. The sensitivity, specificity, and accuracy of the classification model for identifying healthy controls and patients with TNBC were 91%, 100%, and 95%, respectively. Shen et al. observed eight amino acids whose levels were significantly lower in patients with triple-negative breast cancer than in healthy controls (Asp, Ala, His, Tyr, Trp, Met, Arg, and Pro), and two amino acids whose levels were significantly lower in patients with ER+/PR+ breast cancer than healthy individuals (Ala and His) [8].
Baranovicova et al. [57] showed that the levels of circulating metabolites are not associated with breast cancer molecular subtypes (luminal A/luminal B), histological findings, or stage. According to the authors, in the early stage of breast cancer, patients have common metabolic fingerprints in blood plasma, regardless of the degree, stage, or molecular subtype of breast cancer. However, statistically significant correlations were found between the level of tumor proliferation marker Ki-67 and circulating metabolites: Ala, Tyr, Gln, His, and Pro [57].
A significant decrease in the Trp concentration was observed in the plasma of luminal A, triple-negative, and HER2-positive breast cancer compared with healthy controls [68].
2.3. Racial Characteristics of the Serum/Plasma Amino Acid Profile in Breast Cancer
Breast cancer is associated with marked metabolic changes. However, these metabolic shifts in tumors may differ between stages, subtypes, and race [8,69]. Racial differences may not only influence metabolite levels, but also modify associations between metabolites and breast cancer. Racial differences in the incidence of breast cancer are well documented [70,71,72]. Compared to Caucasian American (CA) women, African American (AA) women tend to develop more aggressive tumors that are characterized by an earlier age at diagnosis, a higher mitotic index, and a lower prevalence of ER/PR expression, and subsequently have a lower survival rate. It has been suggested that genetic predisposition plays a role in racial/ethnic disparity in breast cancer [73,74]. For example, Gieger et al. found that up to 12% of the observed dispersion of the metabolic homeostasis of the human body could be explained by genetic variants [75].
In a study by Shen et al., when stratified by race, the difference in the plasma amino acid composition between healthy and sick patients was more evident in the AA participants than in the CA participants [8]. However, due to the small sample size, no significant difference remained in either the AA or CA participants after adjusting for multiple comparisons [8]. A study by Cala et al. described the metabolic features in breast cancer in Latin woman of Hispanic origin [33].
Santaliz Casiano et al. found that amino acid levels are significantly lower in AA breast cancer patients than in healthy individuals [59]. The pathways associated with energy metabolism are glycolysis, amino acid metabolism, and the TCA cycle, which dominate in AA women with ER+ tumors, potentially indicating the aggressiveness of their tumors [76]. In AA individuals, metabolites associated with aminoacyl-tRNA biosynthesis, Arg metabolism, branched amino acid metabolism, and His metabolism were differently distributed in the plasma in individuals with breast cancer. It is known that tumor cells need amino acids both as alternative fuel and for DNA synthesis, building new blood vessels and supporting their rapid growth and proliferation. Amino acids provide metabolic intermediates for epigenetic regulation [77]. In particular, Met levels were found to be lower in plasma samples from AA women who had breast cancer. Met is a methyl group donor for methylation and is a major contributor to epigenetic regulation [78,79]. Systemic or cellular metabolic changes affect the epigenetic landscape, which is important for ERα activity and the response to clinical drugs [80,81]. In AA women, poverty rates are correlated with the hypermethylation of cancer-associated pathways, including the glucocorticoid receptor, p53, estrogen-dependent breast cancer signaling, and cell proliferation [82]. Therefore, hypermethylation is a possible biological mechanism that may explain the poorer outcomes in AA women with live-caused breast cancer in areas of low socioeconomic status.2.4. Serum/Plasma Amino Acids in Breast Cancer Risk Assessment.
Amino acids are most often positively associated with breast cancer risk, and among them are the branched-chain amino acids Val and Leu, as well as Lys, Arg, Phe, and Gln [83]. They are also positively associated with the risk of His as a necessary precursor of histamine, the release of which is an early event in inflammatory responses and is a regulator of cell proliferation [84].
The branched-chain amino acids (BCAAs) Leu, Val, and Ile are dietary essential amino acids and are important metabolites that are involved in cell signaling pathways and muscle protein synthesis [85]. Elevated plasma BCAA concentrations are strongly positively correlated with body mass index and insulin resistance and are markers of a dysfunctional metabolism [86]. In premenopause, elevated levels of circulating BCAAs have been associated with a lower risk of breast cancer (Table 3) [86]. In contrast, among postmenopausal women, elevated levels of circulating BCAAs have been associated with an increased risk of breast cancer [87].
Several studies have evaluated the effects of BCAAs on breast cancer risk with conflicting results, and only one study has assessed menopausal status [90,94,95]. A survival analysis showed that the expression of the catabolic BCAA gene is closely associated with long-term oncological outcomes [96]. High BCAA levels suppressed both tumor growth and breast cancer metastasis, demonstrating the potential benefits of increasing dietary BCAA intake during breast cancer therapy [97,98]. After stratification based on menopausal status, there was a significant inverse relationship between BCAA intake and the likelihood of postmenopausal breast cancer (RR = 0.22; 95% CI 0.13–0.39), although this significant association was not found in premenopausal breast cancer (RR = 2.57, 95% CI 0.51–12.73) [99].
Jobard et al. showed that in the premenopausal subgroup, breast cancer can be predicted by several risk-related metabolites, including His with moderate accuracy (AUC = 0.61, 95% CI: 0.49–0.73) (Table 3) [92]. Predictive power or significant metabolites have not been found in general or in postmenopausal women. Lecuyer et al. found high levels of Gln, Arg, Lys, and Val to be closely associated with a higher risk of BC [89]. Another study reported that higher levels of Gln/isoglutamine, Val/norvaline, Trp, and Phe were related to an increased risk of BC [95]. A study by Nagata et al. showed that the plasma levels of certain specific amino acids, such as Arg, Leu, Tyr, and Asp, were associated with endogenous sex hormone levels, sex-hormone-binding globulin (SHBG), or insulin-like growth factor (IGF-1), as determined by biomarkers of breast cancer risk [88].
Stevens et al. [93] found that Gln was associated with a reduced risk of breast cancer, as in studies involving pre- and postmenopausal women in EPIC [93], but other studies produced conflicting results. Gln was associated with an increased risk in the SU.VI.MAX [95] and E3N [92] cohorts, where the association was limited to premenopausal women. Mrowiec et al. [100] showed that the serum Asn concentration was significantly higher in late-detected breast cancer compared with early-detected breast cancer only in a subgroup of older women. The authors found that several metabolic pathways, including BCAA degradation and glutathione metabolism, differed between younger and older women with a cut-off point of 45 years. The overrepresentation of pathways associated with metabolites that differentiate early- and late-diagnosed cancer (His and Ala metabolism) was observed only in a subgroup of older women, which, once again, confirmed the age-related nature of the metabolic features associated with the risk of developing breast cancer. The results of His et al. [90] show that the concentration of amino acids in plasma is inversely related to the risk of breast cancer; however, these results contradict those of other studies, where, on the contrary, an increase in the concentration of amino acids contributed to an increase in the risk of breast cancer (Table 3).
Risi et al. conducted a study on the risk of breast cancer recurrence [101]. Higher levels of Phe and lower serum levels of Leu, Ile, Val, and His were shown to be associated with the presence of advanced breast cancer. Despite the fact that no statistically significant correlation was found between the levels of individual metabolites and the risk of recurrence in the entire cohort of breast cancer patients, Phe was significantly associated with advanced breast cancer that increased with breast cancer recurrence. However, the authors proposed a metabolomics model that demonstrated strong predictive power. Patients with a “high risk” had a significantly increased likelihood of disease recurrence compared to patients with a low-risk metabolomics fingerprint (HR = 3.42, 95% CI 1.58–7.37, p < 0.001). These results are consistent with those of other studies [102].
The AminoIndex Cancer Screening (AICS) technology has been described and used as a new cancer risk calculation method for early cancer diagnosis [34,49,103,104,105]. AICS (breast) detects breast cancer by detecting abnormal plasma concentrations of Thr, Ala, Orn, His, and Trp [106]. In breast cancer, the Thr, Ala, and Orn concentrations are elevated, while the His and Trp concentrations are reduced, and a multivariate analysis shows an overall accuracy of 88.2% [107].
Thus, it was shown that the risk of breast cancer is associated with the amino acid composition of blood plasma/serum; however, the patterns identified by the authors are closely related to the characteristics of the sample, menopausal status, and age. Nevertheless, according to most authors, Gln/Glu, Asp, Arg, Leu/Ile, Lys, and Orn have the greatest significance in assessing the risk of breast cancer.
3. Amino Acid Metabolism in Breast Cancer
3.1. Metabolic Features of Breast Cancer
The amino acid metabolism plays a critical role in the proliferation of breast cancer cells [108,109]. The intake and use of amino acids helps to support the growth of cancer cells [110,111,112]. A number of studies have shown that a decrease in the content of a number of amino acids may be the result of their excessive consumption or preferential use to support the uncontrolled growth of breast cancer cells [5,26,37,111,112,113,114].
The Glu/Gln, Ala, Asp, and Arg metabolisms were the most important biosynthetic pathways in breast cancer, suggesting extensive metabolic disturbances during breast cancer progression [115,116]. Huang S. et al. showed that the alanine, aspartate, and glutamate pathways are critical biological pathways for the early diagnosis of breast cancer [30]. Most of the metabolites in these three metabolic pathways were reduced in breast cancer patients compared to healthy controls. Thus, Ala promotes the proliferation of breast cancer cells, which indicates the potential role of Ala as a marker for cancer diagnosis [52]. The down-regulation of Gln indicated that Glu can accumulate in the body, which contributes to the development of breast cancer due to the increased proliferation of mammary epithelial cells [117] due to ATP production and nucleotide biosynthesis [118]. Moreover, Glu activation via glutaminolysis can maintain the citric acid cycle [119]. The metabolism of Gln is closely related to the process of providing energy to the cancer cell. Gln is transported into cancer cells by means of multiple transporters [116,120]. It was previously shown that the expressions of the Gln transporters ASCT2, SNAT1, SNAT2, and SNAT5 are increased in tumor tissue [121]. On the other hand, the inhibition of ASCT2 reduces the growth of TNBC [122]. It is known that the reductive metabolism of Gln supports tumor growth under conditions of hypoxia, mitochondrial dysfunction [123], and in an environment with a low nutrient content [124]. It was noted that Gln/Glu reversibility decreased in MCF-7 cells, indicating that breast cancer cells may be partially associated with irreversible glutaminase [125]. The Gln/Glu ratio can be used as a biomarker for the diagnosis of breast cancer [126]. The enzyme glutaminase I (GLS-I), which converts Gln to Glu via glutaminolysis, can be considered as a target for breast cancer therapy [127].
The change in the Gln level can be reflected in fluctuating levels of Ala and Asp due to the abnormal transport of ammonia. Higher histidine decarboxylase activity may lead to a decrease in the His levels [128], and low concentrations of His may be associated with increases in Asp and Glu, which can be converted to oxaloacetic and α-ketoglutaric acids, which are intermediates of the tricarboxylic acid cycle. Asp has been shown to be more sensitive to breast cancer [129]. Therefore, an increase in the use of Asp by BC cells can lead to a decrease in the levels of Asp and oxaloacetate in the blood. It is noteworthy that, as a transamination product of aspartic acid, Asp has an important effect on breast cancer metastasis [130].
The dysregulation of branched-chain amino acid (BCAA) metabolism, including Leu, Ile, and Val, has been reported to be associated with specific cancer phenotypes. BCAAs can inhibit tumor growth and metastasis [97], so changes in the BCAA levels can often reflect systemic changes in cancer patients compared to healthy controls [131]. Plasma Arg, Pro, and Trp metabolites decreased in BC patients [6]. Huang et al. [30] revealed a decrease in the Ser and Thr levels in the serum of patients with breast cancer. Harvie et al. showed that a Tyr deficiency can lead to the stunting of breast cancer cells [132], and the inhibition of tumor growth was confirmed with diets that were low in Phe and Tyr in an animal study [133]. It is known that sharp metabolic shifts in the levels of choline and Pro are characteristic of metastatic breast cancer [134]. Breast cancer has been shown to be highly dependent on Arg [6]. It has been shown to enhance the immune response, both innate and adaptive, with the administration of Arg supplements [135]. Conversely, a decrease in the dietary Asn intake or the suppression of asparagine synthetase reduced breast cancer metastasis [130].
Many authors agree that the concentration of Trp in the plasma and serum of breast cancer patients is reduced [26,28,113]. Previously, it was shown that Trp indirectly promotes the degradation of the extracellular matrix and the invasion of cancer cells [136]. Two major enzymes catalyze Trp into metabolites of the kynurenine (Kyn) pathway: indolamine 2,3 dioxygenase (IDO1) and tryptophan 2,3 dioxygenase (TDO2) [137]. Kyn activates the aryl hydrocarbon receptor, which promotes the evasion of the cancer immune response by increasing IL-10 and suppressing immune activation cells [138]. Thus, with IDO1/TDO2 overexpression, increased Trp catabolism can lead to a decrease in its serum concentration and an accumulation of Kyn metabolites [139].
Ser is transported into cells by means of ASCT1, which is highly expressed in breast cancer [140]. An increase in the rate of tumor cell proliferation depends on the presence of extracellular Ser. In an experiment with mice, it was shown that decreases in the Ser and Gly levels suppresses tumor growth and increases the lifespan [141]. It is interesting to note that, depending on the type of cancer, either Ser or Gly can contribute to the rapid proliferation of cancer cells [142].
Budhu A. et al. showed that a decrease in plasma Cys was inversely associated with an increase in Cys in breast cancer tissues [13], suggesting that breast cancer cells use more Cys. Cys is involved in the redox reaction of glutathione. With an increase in the concentration of Cys, oxidative damage and the production of free radicals also increase, which leads to gene mutation [143]. On the other hand, Cys can be considered as a substrate for the production of hydrogen sulfide, which stimulates cellular bioenergetics [144]. It has been established that the Cys-associated metabolic pathway of cysteinyl leukotrienes (CysLT) is also closely associated with cancer in enhancing the ability to survive and proliferate cancer cells [145].
3.2. Amino Acid Metabolism as a Target for Breast Cancer Imaging
Elevated levels of Met, Gln, Cys, Trp, Tyr, and other amino acids in tissues have been noted in many malignancies, including breast cancer [146]. Cancer cells with the up-regulation of amino acid metabolism stimulate the increased transport of amino acids into the cell [147]. The increased consumption of amino acids and the overexpression of amino acid transporters in malignant tumors make radiolabeled amino acids attractive imaging agents [114,148].
Multiple amino acid transporters have been demonstrated to be up-regulated in breast cancer families, including L-type amino acid transporter (LAT1), ASC transporter 2 (ASCT2), ATB0,+, SNAT1, and xc- [149,150]. LAT1 is required for the transport of large neutral amino acids and is overexpressed in many types of malignancies, including breast cancer [151]. The expression of ASCT2 also has prognostic associations in breast cancer [120]. The xc-system transporter, which mediates cysteine uptake, is up-regulated in some breast cancer tumors [152]. The two amino acid transporters SLC7A5 and SLC7A11 are considered essential for the growth of breast cancer cells in a cell-dependent manner [153].
Met is a naturally occurring large neutral amino acid that is readily labeled with the 11C radioactive isotope. 11C-methionine serves as a metabolic marker for Met uptake via L-type amino acid transporters. PET with 11C-methionine makes it possible to visualize primary and metastatic lesions, as well as to predict the response to breast cancer treatment [154]. Limitations of 11C-methionine include the ability to detect metastases only in the liver and bone marrow and its relatively short half-life (20 min). On the basis of Met, an MR contrast agent based on Met-MSN-Gd3+ was developed that targets methionine receptors, which are overexpressed in tumor cells (MSN—Mesoporous Silica Nanoparticles) [155,156].
Trans-1-amino-3-18F-fluorocyclobutanecarboxylic acid (anti-18F-FACBC, also known as 18F-fluciclovine) is a synthetic analogue of Leu, which is transported into the cell by the ASCT2 transporter with the additional involvement of LAT1 [157]. Uptake by cells is most similar to uptake of the natural amino acid Gln [158]. 18F-fluciclovine can visualize breast lesions [159,160], axillary lymph node metastases [161], and previously undetected extra-axillary nodular metastases [161,162]. Preclinical studies have demonstrated significant success with 18F-fluciclovine in detecting bone metastases.
(4S)-4-(3-[18F]fluoropropyl)-l-glutamate (BAY 94-9392, also known as [18F]FSPG), is a synthetic amino acid analogue of SLC7A11 [152,163]. Histological or molecular subtypes of breast cancer may affect 18F-FSPG uptake. 18F-5-fluoroaminosuberic acid, a synthetic amino acid substrate of SLC7A11, exhibited tumor uptake in three breast cancer cell lines (MDA-MB-231, MCF-7, and ZR-75-1), with the highest uptake observed in MDA-MB- 231, the TNBC cell line [164].
Several radioactively labeled Tyr analogues have been developed for tumor imaging, including L-[1–11C]tyrosine [165]. Technetium-labeled tyrosine analogs have also been synthesized in high yield and can distinguish malignant breast neoplasms from benign breast tissues [166]. O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) is a synthetic amino acid transported by SLC7A5 [167]. Animal experiments using rats and mice have shown that 18F-FET can distinguish between inflammation and malignancy [168,169] as well as in 75% of breast cancer patients.
In preclinical studies, several propanoic acid derivatives have demonstrated good tumor uptake in human breast cancer cells as well as mouse tumor xenografts [170]. 2-Amino-5-(4-[18F]fluorophenyl)pent-4-ynoic acid ([18F]FPhPA) is a synthetic amino acid that targets SLC1A5 and SLC7A5. A high uptake of the radiopharmaceutical [18F]FPhPA was detected in the mouse breast cancer cell line EMT6 by PET [171]. Trp analogs, primarily using L-type amino acid transport, have been developed by several research groups and have also been shown to be taken up by breast cancer cells in small animal studies [172]. An analogue of Leu, 5-[18F]fluoroleucine, was synthesized with primary transport via LAT1 [173]. Unlike 18F-fluciclovine, the absorption of 5-[18F]fluoroleucine gradually increases over time. The glutaminolysis pathway is very active in many malignancies, including triple-negative breast cancer. Preclinical work with the Gln analog [18F](2S,4R)4-fluoroglutamine demonstrated the ability of this indicator to track changes in the size of the cellular Gln pool and the glutaminolysis pathway after glutaminase inhibition [174].
Amino acid transporters can also be used to image tumors using single-photon emission computed tomography (SPECT). 3-[123I]-α-methyl-l-tyrosine (IMT) is an artificial amino acid that is transported through SLC7A5 [175] and is also a suitable metabolic indicator for SPECT in extracranial tumors, including breast cancer [176]. Using IMT SPECT, primary and metastatic breast cancer, as well as tumor regression after radiotherapy, were detected and were consistent with the results of the clinical assessment [175]. [99m]Tc-labeled diethylenetriaminepentaaceticacid (DTPA-bis)-methionine scintymammography has shown 96% sensitivity and a 96% positive predictive value for the detection of breast cancer [177], and therefore may be an alternative to conventional SPECT using non-specific mitochondrial uptake.
4. Amino Acids in Potential Strategies for the Treatment of Breast Cancer
One of the therapeutic approaches to cancer treatment is aimed at changing the metabolism of the tumor [178,179].
Some essential amino acids (EAAs)—Trp, His, Met, and branched-chain amino acids—are directly associated with tumor growth and treatment resistance [180,181,182,183]. EAAs provide important raw materials for protein synthesis, influence the biological behavior of cells, and induce therapeutic resistance in breast cancer cells. Strekalova et al. [184] found that Met plays a critical role in maintaining the self-renewal and survival of cancer stem cells. Met restriction reduced the population of cancer stem cells in TNBC. Saito et al. [185] showed that Leu not only promotes cell proliferation in ER-positive breast cancer, but also participates in the mechanism of resistance to tamoxifen. In addition, essential amino acids, as important nutrients, mediate the development of an immunosuppressive tumor microenvironment in breast cancer. For example, kynurenine, a product of Trp metabolism, can inhibit T cell proliferation and differentiation, leading to immune evasion and tumor progression in breast cancer [186]. Interestingly, both Trp and kynurenine were lower in plasma in breast cancer patients compared to controls, especially in women with estrogen-receptor-negative and advanced breast cancers [187]. These results show an intrinsic relationship between EAA metabolism and the immune microenvironment in breast cancer. Zhao et al. [188] found that the ratio of SLC7A5 to SLC7A8 (SSR) is significantly correlated with the level of EAA and the metabolic activity of EAA in breast cancer, and therefore, the SSR index can be used as a biomarker to assess the degree of metabolism of EAA in breast cancer. In addition, breast cancer patients with a high EAA metabolism had a shorter overall survival time, a higher PD-L1 expression, and higher T-regulatory cell infiltration, indicating that a high EAA metabolism was associated with a poor prognosis and immunosuppression in breast cancer.
Zhang, L. showed that the level of BCAA in the plasma and cancer tissues of BC patients was increased, which was accompanied by an increase in the expression of BCAA catabolism enzymes [189]. The stimulation of BCAA catabolism by modulating BCAT1 enhanced the growth and formation of colonies of breast cancer cells. BCAT1 promoted mitochondrial biogenesis and enhanced mitochondrial function by promoting ATP production and protection against oxidative stress by activating mTOR signaling, but not AMPK or SIRT1. The inhibition of mTOR by rapamycin neutralizes the role of BCAT1 in mitochondrial function and cancer cell growth.
For some cancer subtypes, such as TNBC, there is no specific therapy, resulting in a poor prognosis that is associated with invasion and metastasis.
Under physiological conditions, Gln is transported into cells by many transporters such as Ala, Ser, Cys-preferential transporter 2 (ASCT2, also known as SLC1A5), and L-type amino acid transporter 1 (LAT1, also known as SLC7A5). In TNBC, both ASCT2 and LAT1 are overexpressed [122,190]. Compared to other subtypes of breast cancer, TNBC is more Gln dependent and sensitive to glutaminolysis-targeted therapy due to glutaminase overexpression (GLS) [191,192], which is associated with high-grade metastatic breast cancer. Several small-molecule GLS inhibitors, such as CB-839, have been developed to combat the dysregulation of glutaminolysis [193]. Other combination therapies, such as the combination of GLS inhibition and bevacizumab (an anti-angiogenesis monoclonal antibody targeting VEGF), also show antitumor effects on TNBC [194]. Ginsenoside was described to effectively inhibit TNBC by suppressing Gln uptake and Glu production by down-regulating glutaminase 1 (GLS1) expression [195]. Ginsenoside treatment further reduced cellular ATP production, decreased amino acid utilization associated with Gln metabolism, and induced glutathione depletion and reactive oxygen species accumulation, which consequently triggered apoptosis in TNBC. Morotti et al. showed that the knockdown of the Gln transporter SLC38A2, which was identified as a highly expressed amino acid transporter in six breast cancer cell lines [196], reduced Gln uptake, inhibited cell growth, induced autophagy, and resulted in the production of reactive oxygen species in a subgroup of Gln-sensitive cell lines. A high expression of the SLC38A2 protein was associated with poor breast cancer survival in a large group of patients (p = 0.004), especially in TNBC (p = 0.02).
Increased Glu production by GLS may support the uptake of exogenous cystine via the cystine/glutamate antiporter xCT to maintain redox balance. As a clinically approved anti-inflammatory drug, sulfasalazine (SASP) was found to inhibit xCT activity and retard the growth of TNBC [197]. By immunizing mice with a DNA-based vaccine expressing the xCT protein, the cell surface immunotargeting of the xCT antigen effectively attenuated tumor growth and lung metastasis, and increased chemosensitivity to doxorubicin [198]. Additionally, virus-like particle immunotherapy was developed, which elicits a stronger humoral response against xCT [199].
In addition to Gln and Cys, TNBC cells are also somewhat dependent on the availability of several other amino acids such as Met, Asp, and Arg, suggesting that restricting these amino acids may have a therapeutic effect [200]. The depletion of either Met or Gln can increase the cell surface expression of the pro-apoptotic TNF-related apoptosis-inducing ligand receptor-2 (TRAIL-R2) and increase the sensitivity of TNBC cells to TRAIL-induced apoptosis [130,201]. Met deprivation in the diet increases cellular susceptibility to lexatumumab, an agonistic monoclonal antibody targeting TRAIL-R2, and reduces the rate of lung metastasis [202]. In addition, many tumor and stem cells depend on the biosynthesis of the universal methyl donor S-adenosylmethionine from the exogenous Met via methionine adenosyltransferase 2α (MAT2A) to maintain their epigenome [203,204]. A restriction on Met is enough to undermine the ability of TNBC to initiate a tumor, which is in part due to the impaired formation of S-adenosylmethionine. The combination of methionine restriction and the MAT2A inhibitor cycloleucine has a synergistic antitumor effect [184]. Under normal physiological conditions, the serum levels of Asp are lower than in the mammary gland, making Asp bioavailability a key regulator of circulating tumor cells and the metastatic potential of breast cancer. The restriction of Asp intake by the suppression of asparagine synthetase, treatment with L-asparaginase, or the restriction of Asp intake in the diet inhibits breast cancer metastasis [201]. The depletion of Arg by recombinant human arginase (rhArg) leads to the apoptosis of TNBC cells via reactive oxygen species and induces adaptive autophagy, while blocking the flow of autophagy via autophagy-targeting drugs enhances rhArg cytotoxicity [205]. The deprivation of Arg by L-arginase impairs tumor growth, leading to cell death [206]. Much attention has been paid to epigenetic modifications caused by enzymes of protein arginine methyltransferases, in which methylate Arg make a great contribution to the process of breast carcinogenesis and tumor suppression [207] and are targets for many types of cancer [208].
Leu uptake is predominantly mediated by the L-type amino acid transporter (LAT) family, a group of four Na+-independent transporters (LAT1, SLC7A5; LAT2, SLC7A8; LAT3, SLC43A1; and LAT4, SLC43A2) with an affinity for branched and neutral amino acid transporters [130]. Glutamine transport is largely mediated by Ala, Ser, and Cys-preferential transporter 2 (ASCT2; SLC1A5). The authors proposed using the ASCT2 inhibitor, benzylserine (BenSer), to doubly inhibit Gln [209] and Leu [210] uptake. It has been shown that a double inhibition with the pharmacological inhibitor BenSer can reduce the growth of breast cancer cells and limit the progression of the cell cycle.
Amino acid deprivation (AADT) is becoming a promising strategy for the development of new therapeutic agents against cancer [211]. The rapid growth of tumors leads to a decrease in the expression of certain enzymes, which leads to the auxotrophy of some specific amino acids. Amino acid depletion selectively inhibits tumor growth because normal cells can synthesize amino acids through their normal machinery. The enzymes used in AADT are primarily obtained from microbes due to their easy availability. Thus, the deprivation of Gln leads to a decrease in cell proliferation and cell death in breast cancer cell lines [212].
Endocrine therapy is the standard treatment for estrogen-receptor-positive (ER+) breast cancer, but 40% of women experience a recurrence of the disease during therapy. A general analysis of transcription in cells revealed a suppression of the neutral and basic amino acid transporter SLC6A14, which is regulated by the increased expression of miR-23b-3p, which leads to impaired amino acid metabolism [213]. This altered cellular amino acid metabolism is supported by autophagy activation and the increased import of acidic amino acids (Asp and Glu) mediated by the SLC1A2 transporter. Targeting these amino acid metabolic dependencies increases the sensitivity of cells to endocrine therapy.
Anticancer agents delivered to cancer cells often exhibit multidrug resistance due to a displacement of the agents. One way to solve this problem is to increase the accumulation of anticancer agents in cells with the help of amino acid transporters. Val-lapatinib and Tyr-lapatinib were newly synthesized by adding Val and Tyr fragments, respectively, to the parent anticancer agent lapatinib. Val-lapatinib and Tyr-lapatinib demonstrated enhanced anticancer activity compared to parental lapatinib in various cancer cell lines (MDA-MB-231 and MCF7) [214]. Both Val-lapatinib and Tyr-lapatinib, but not the parent lapatinib, inhibit glutamine transport in MDA-MB-231 and MCF7 cells, suggesting the involvement of amino acid transporters. Thus, amino acid transporters can be effective drug delivery targets to increase the uptake of anticancer agents, leading to one method of overcoming multidrug resistance in cancer cells.
Mello-Andrade et al. studied the effect of ruthenium(II) complexes associated with the amino acids methionine (RuMet) and tryptophan (RuTrp) on the induction of cell death, clonogenic survival, the inhibition of angiogenesis, and the migration of MDA-MB-231 cells [215]. The study also showed that RuMet and RuTrp complexes induce cell cycle arrest and the apoptosis of MDA-MB-231 cells, as evidenced by an increase in the number of annexin V-positive cells, p53 phosphorylation, caspase 3 activation, and poly(ADP-ribose) polymerase cleavage. RuMet and RuTrp complexes act directly on breast tumor cells, leading to cell death and suppressing their metastatic potential; this reveals the potential therapeutic effect of these drugs.
The use of various drugs based on platinum nanoparticles leads to a disruption of the amino acid metabolism, a disruption of tRNA aminoacylation, and protein synthesis [216]. Mitrevska et al. [217] analyzed the effect on amino acid metabolism in MDA-MB-231 cells upon treatment with cisplatin, PtNP-10, and PtNP-40, and revealed a marked contrast between the effects of cisplatin and PtNP. The results indicate a higher sensitivity of MDA-MB-231 cells to PtNP compared to cisplatin, since the increase in the number of amino acids was associated with the degree of insensitivity to various chemotherapeutic agents [217].
In general, combinations of anticancer drugs and amino acids can improve the intratumoral distribution of the active substance and increase its bioavailability. In particular, amino acid-based poly(ether urea ester) (AA-PEUU), as a nanocarrier for the systemic delivery of gamboginic acid, demonstrates the effectiveness of engineered AA-PEUU nanocarriers with custom structures and universal customization for the systemic delivery of therapeutics in the treatment of TNBC [218].
Plasma amino acid analysis can be used to monitor treatment progress. So, Minet-Quinard et al. [47] showed that the plasma levels of Ser and Glu returned to normal six months after the surgical removal of the tumor. Dunstan et al. [219] considered the changes in the amino acid homeostasis during radiation therapy. The urinary histidine and alanine levels were shown to be elevated prior to radiotherapy, while the Thr, Met, Ala, Ser, Asp, and Gln levels were higher after 5 weeks of radiotherapy. Many complications such as cachexia, anorexia, and fatigue occur in the treatment of problems associated with breast cancer, and many studies have considered the addition of amino acids with BCAAs [220] or a single amino acid or its derivative [221] to reduce the effects of treatment. Li et al. provided preliminary data to support the correction of the Trp metabolism for the treatment of neuropsychiatric symptoms [222].
Changes in the concentration of metabolites may also be useful in predicting the overall survival of patients with breast cancer. Thus, two metabolites differ significantly depending on the previous therapy: Met and Ser [223]. The blood Met levels were higher in the patients treated with anti-Her2 therapy, while the Ser levels were lower in the patients treated with endocrine therapy alone. Patients with TNBC were previously shown to have higher Ser levels, while patients with luminal cancer A, on the contrary, had low blood Ser concentrations [224], which is consistent with the therapy and Ser accumulation with anti-Her2 therapy [225]. In addition, Possemato et al. found an increased flux of Ser synthesis in patients with estrogen-negative breast cancer, which is also associated with a poor 5-year survival [226].
5. Conclusions
A fairly large number of studies have been devoted to the study of amino acid metabolism in breast cancer. At the same time, both the contents of individual amino acids and the combinations of amino acids with each other or with other metabolites determined in the course of obtaining the metabolomic profiles of biological fluids were determined. We have shown that for some amino acids (Thr, Arg, Met, and Ser) an increase in concentration is more often observed in breast cancer compared with a healthy control, and for other amino acids, there is a decrease (Asp, Pro, Trp, and His). However, the amino acid profile must be analyzed while taking into account the high heterogeneity of breast cancer, as well as age and race. The accuracy of the diagnosis using amino acids depends on the number of metabolites in the algorithm and varies from 52 to 98%. The contents of amino acids in biological fluids are used to assess the risk of breast cancer; however, the identified patterns are closely related to the characteristics of the sample, menopausal status, and age. According to most authors, Gln/Glu, Asp, Arg, Leu/Ile, Lys, and Orn have the greatest significance in assessing the risk of breast cancer. An analysis of the changes in the amino acid metabolism in breast cancer is a promising strategy for developing new therapeutic agents, monitoring the treatment process, correcting complications after treatment, and evaluating the survival rates. This, once again, emphasizes the high importance of research in this area.
Author Contributions
Conceptualization, L.V.B. and D.V.S.; methodology, L.V.B. and D.V.S.; software, I.A.G.; validation, L.V.B., I.A.G. and D.V.S.; formal analysis, I.A.G.; resources, L.V.B.; data curation, I.A.G. and D.V.S.; writing—original draft preparation, I.A.G. and D.V.S.; writing—review and editing, L.V.B.; visualization, I.A.G.; supervision, D.V.S.; project administration, L.V.B.; funding acquisition, L.V.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Russian Science Foundation, grant number 23-15-00188; https://rscf.ru/project/23-15-00188/, accessed on 13 September 2023.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zeng, H.; Fan, J.; Wang, F.; Xu, C.; Li, Y.; Tu, J.; Nephew, K.P.; Long, X. Glutamine metabolism in breast cancer and possible therapeutic targets. Biochem. Pharmacol. 2023, 210, 115464. [Google Scholar] [CrossRef]
- Jiao, Z.; Pan, Y.; Chen, F. The Metabolic Landscape of Breast Cancer and Its Therapeutic Implications. Mol. Diagn. Ther. 2023, 27, 349–369. [Google Scholar] [CrossRef] [PubMed]
- Jové, M.; Collado, R.; Quiles, J.L.; Ramírez-Tortosa, M.C.; Sol, J.; Ruiz-Sanjuan, M.; Fernandez, M.; de la Torre Cabrera, C.; Ramírez-Tortosa, C.; Granados-Principal, S.; et al. A plasma metabolomic signature discloses human breast cancer. Oncotarget 2017, 8, 19522–19533. [Google Scholar] [CrossRef]
- Jasbi, P.; Wang, D.; Cheng, S.L.; Fei, Q.; Cui, J.Y.; Liu, L.; Wei, Y.; Raftery, D.; Gu, H. Breast cancer detection using targeted plasma metabolomics. J. Chromatogr. B 2019, 1105, 26–37. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, X.; Chou, J.; Yu, J.; Yang, T.; Liu, L.; Zhang, F. Taurine, glutamic acid and ethylmalonic acid as important metabolites for detecting human breast cancer based on the targeted metabolomics. Cancer Biomarkers 2018, 23, 255–268. [Google Scholar] [CrossRef]
- Shen, J.; Yan, L.; Liu, S.; Ambrosone, C.B.; Zhao, H. Plasma metabolomic profiles in breast cancer patients and healthy controls: By race and tumor receptor subtypes. Transl. Oncol. 2013, 6, 757–765. [Google Scholar] [CrossRef]
- Da Cunha, P.A.; Nitusca, D.; Canto, L.M.D.; Varghese, R.S.; Ressom, H.W.; Willey, S.; Marian, C.; Haddad, B.R. Metabolomic Analysis of Plasma from Breast Cancer Patients Using Ultra-High Performance Liquid Chromatography Coupled with Mass Spectrometry: An Untargeted Study. Metabolites 2022, 12, 447. [Google Scholar] [CrossRef]
- Neagu, A.-N.; Whitham, D.; Bruno, P.; Morrissiey, H.; Darie, C.A.; Darie, C.C. Omics-Based Investigations of Breast Cancer. Molecules 2023, 28, 4768. [Google Scholar] [CrossRef]
- Wei, Y.; Jasbi, P.; Shi, X.; Turner, C.; Hrovat, J.; Liu, L.; Rabena, Y.; Porter, P.; Gu, H. Early Breast Cancer Detection Using Untargeted and Targeted Metabolomics. J. Proteome Res. 2021, 20, 3124–3133. [Google Scholar] [CrossRef]
- Dougan, M.M.; Li, Y.; Chu, L.W.; Haile, R.W.; Whittemore, A.S.; Han, S.S.; Moore, S.C.; Sampson, J.N.; Andrulis, I.L.; John, E.M.; et al. Metabolomic profiles in breast cancer: A pilot case-control study in the breast cancer family registry. BMC Cancer 2018, 18, 532. [Google Scholar] [CrossRef]
- Budhu, A.; Terunuma, A.; Zhang, G.; Hussain, S.P.; Ambs, S.; Wang, X.W. Metabolic profiles are principally different between cancers of the liver, pancreas and breast. Int. J. Biol. Sci. 2014, 10, 966–972. [Google Scholar] [CrossRef]
- Jobard, E.; Pontoizeau, C.; Blaise, B.J.; Bachelot, T.; Elena-Herrmann, B.; Trédan, O. A serum nuclear magnetic resonance-based metabolomic signature of advanced metastatic human breast cancer. Cancer Lett. 2014, 343, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Ambs, S. Metabolic Signatures of Human Breast Cancer. Mol. Cell. Oncol. 2015, 2, e992217. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Zhou, X.; Xia, T.S.; Chen, Z.; Li, J.; Liu, Q.; Alolga, R.N.; Chen, Y.; Lai, M.D.; Li, P.; et al. Human plasma metabolomics for identifying differential metabolites and predicting molecular subtypes of breast cancer. Oncotarget 2016, 7, 9925–9938. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Wang, Q.; Chen, G. Serum metabolomics analysis reveals changes in signaling lipids in breast cancer patients. Biomed. Chromatogr. 2016, 30, 42–47. [Google Scholar] [CrossRef]
- Gu, H.; Pan, Z.; Xi, B.; Asiago, V.; Musselman, B.; Raftery, D. Principal component directed partial least squares analysis for combining nuclear magnetic resonance and mass spectrometry data in metabolomics: Application to the detection of breast cancer. Anal. Chim. Acta 2011, 686, 57–63. [Google Scholar] [CrossRef]
- Oakman, C.; Tenori, L.; Claudino, W.M.; Cappadona, S.; Nepi, S.; Battaglia, A.; Bernini, P.; Zafarana, E.; Saccenti, E.; Fornier, M.; et al. Identification of a serum-detectable metabolomic fingerprint potentially correlated with the presence of micrometastatic disease in early breast cancer patients at varying risks of disease relapse by traditional prognostic methods. Ann. Oncol. 2011, 22, 1295–1301. [Google Scholar] [CrossRef]
- Tenori, L.; Oakman, C.; Claudino, W.M.; Bernini, P.; Cappadona, S.; Nepi, S.; Biganzoli, L.; Arbushites, M.C.; Luchinat, C.; Bertini, I.; et al. Exploration of serum metabolomic profiles and outcomes in women with metastatic breast cancer: A pilot study. Mol. Oncol. 2012, 6, 437–444. [Google Scholar] [CrossRef]
- Asiago, V.M.; Alvarado, L.Z.; Shanaiah, N.; Gowda, G.A.N.; Owusu-Sarfo, K.; Ballas, R.A.; Raftery, D. Early detection of recurrent breast cancer using metabolite profiling. Cancer Res. 2010, 70, 8309–8318. [Google Scholar] [CrossRef]
- Tenori, L.; Oakman, C.; Morris, P.G.; Gralka, E.; Turner, N.; Cappadona, S.; Fornier, M.; Hudis, C.; Norton, L.; Luchinat, C.; et al. Serum metabolomic profiles evaluated after surgery may identify patients with oestrogen receptor negative early breast cancer at increased risk of disease recurrence. Results from a retrospective study. Mol. Oncol. 2015, 9, 128–139. [Google Scholar] [CrossRef]
- Wei, S.; Liu, L.; Zhang, J.; Bowers, J.; Gowda, G.A.N.; Seeger, H.; Fehm, T.; Neubauer, H.J.; Vogel, U.; Clare, S.E.; et al. Metabolomics approach for predicting response to neoadjuvant chemotherapy for breast cancer. Mol. Oncol. 2013, 7, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Zapater-Moros, A.; Díaz-Beltrán, L.; Gámez-Pozo, A.; Trilla-Fuertes, L.; Lumbreras-Herrera, M.I.; López-Camacho, E.; González-Olmedo, C.; Espinosa, E.; Zamora, P.; Sánchez-Rovira, P.; et al. Metabolomics unravels subtype-specific characteristics related to neoadjuvant therapy response in breast cancer patients. Metabolomics 2023, 19, 60. [Google Scholar] [CrossRef] [PubMed]
- Torata, N.; Kubo, M.; Miura, D.; Ohuchida, K.; Mizuuchi, Y.; Fujimura, Y.; Hayakawa, E.; Kai, M.; Oda, Y.; Mizumoto, K.; et al. Visualizing energy charge in breast carcinoma tissues by MALDI mass-spectrometry imaging profiles of low-molecular-weight metabolites. Anticancer Res. 2018, 38, 4267–4272. [Google Scholar] [CrossRef] [PubMed]
- More, T.H.; RoyChoudhury, S.; Christie, J.; Taunk, K.; Mane, A.; Santra, M.K.; Chaudhury, K.; Rapole, S. Metabolomic alterations in invasive ductal carcinoma of breast: A comprehensive metabolomic study using tissue and serum samples. Oncotarget 2018, 9, 2678–2696. [Google Scholar] [CrossRef]
- Bathen, T.F.; Geurts, B.; Sitter, B.; Fjosne, H.E.; Lundgren, S.; Buydens, L.M.; Gribbestad, I.S.; Postma, G.; Giskeødegård, G.F. Feasibility of MR metabolomics for immediate analysis of resection margins during breast cancer surgery. PLoS ONE 2013, 8, e61578. [Google Scholar] [CrossRef]
- Eniu, D.T.; Romanciuc, F.; Moraru, C.; Goidescu, I.; Eniu, D.; Staicu, A.; Rachieriu, C.; Buiga, R.; Socaciu, C. The decrease of some serum free amino acids can predict breast cancer diagnosis and progression. Scand. J. Clin. Lab. Investig. 2019, 79, 17–24. [Google Scholar] [CrossRef]
- Zhou, J.; Wang, Y.; Zhang, X. Metabolomics studies on serum and urine of patients with breast cancer using 1H-NMR spectroscopy. Oncotarget 2017, 5. [Google Scholar] [CrossRef]
- Huang, S.; Chong, N.; Lewis, N.E.; Jia, W.; Xie, G.; Garmire, L.X. Novel personalized pathway-based metabolomics models reveal key metabolic pathways for breast cancer diagnosis. Genome Med. 2016, 8, 34. [Google Scholar] [CrossRef]
- Yuan, B.W.; Schafferer, S.; Tang, Q.Q.; Scheffler, M.; Nees, J.; Heil, J.; Schott, S.; Golatta, M.; Wallwiener, M.; Sohn, C.; et al. A plasma metabolite panel as biomarkers for early primary breast cancer detection. Int. J. Cancer 2019, 144, 2833–2842. [Google Scholar] [CrossRef]
- Suman, S.; Sharma, R.K.; Kumar, V.; Sinha, N.; Shukla, Y. Metabolic fingerprinting in breast cancer stages through (1)H NMR spectroscopy-based metabolomic analysis of plasma. J. Pharm. Biomed. Anal. 2018, 160, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Cala, M.P.; Aldana, J.; Medina, J.; Sanchez, J.; Guio, J.; Wist, J.; Meesters, R.J.W. Multiplatform plasma metabolic and lipid fingerprinting of breast cancer: A pilot control-case study in Colombian Hispanic women. PLoS ONE 2018, 13, e0190958. [Google Scholar] [CrossRef] [PubMed]
- Miyagi, Y.; Higashiyama, M.; Gochi, A.; Akaike, M.; Ishikawa, T.; Takeshi, M.; Saruki, N.; Bando, E.; Kimura, H.; Imamura, F.; et al. Plasma free amino acid profiling of five types of cancer patients and its application for early detection. PLoS ONE 2011, 6, e24143. [Google Scholar] [CrossRef] [PubMed]
- Murata, T.; Yanagisawa, T.; Kurihara, T.; Kaneko, M.; Ota, S.; Enomoto, A.; Tomita, M.; Sugimoto, M.; Sunamura, M.; Hayashida, T.; et al. Salivary metabolomics with alternative decision tree-based machine learning methods for breast cancer discrimination. Breast Cancer Res. Treat. 2019, 177, 591–601. [Google Scholar] [CrossRef]
- Zhong, L.; Cheng, F.; Lu, X.; Duan, Y.; Wang, X. Untargeted saliva metabonomics study of breast cancer based on ultra-performance liquid chromatography coupled to mass spectrometry with HILIC and RPLC separations. Talanta 2016, 158, 351–360. [Google Scholar] [CrossRef]
- Sugimoto, M.; Wong, D.T.; Hirayama, A.; Soga, T.; Tomita, M. Capillary electrophoresis mass spectrometry-based saliva metabolomics identified oral, breast and pancreatic cancer-specific profiles. Metabolomics 2010, 6, 78–95. [Google Scholar] [CrossRef]
- Bel’skaya, L.V.; Sarf, E.A.; Loginova, A.I. Diagnostic Value of Salivary Amino Acid Levels in Cancer. Metabolites 2023, 13, 950. [Google Scholar] [CrossRef]
- Cala, M.P.; Aldana, J.; Sanchez, J.; Guio, J.; Meesters, R.J.W. Urinary metabolite and lipid alterations in Colombian Hispanic women with breast cancer: A pilot study. J. Pharm. Biomed. Anal. 2018, 152, 234–241. [Google Scholar] [CrossRef]
- Slupsky, C.M.; Steed, H.; Wells, T.H.; Dabbs, K.; Schepansky, A.; Capstick, V.; Faught, W.; Sawyer, M.B. Urine metabolite analysis offers potential early diagnosis of ovarian and breast cancers. Clin. Cancer Res. 2010, 16, 5835–5841. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, R.; Song, Y.; He, J.; Sun, J.; Bai, J.; An, Z.; Dong, L.; Zhan, Q.; Abliz, Z. RRLC-MS/MS-based metabonomics combined with in-depth analysis of metabolic correlation network: Finding potential biomarkers for breast cancer. Analyst 2009, 134, 2003–2011. [Google Scholar] [CrossRef]
- Hussain, A.; Xie, L.; Deng, G.; Kang, X. Common alterations in plasma free amino acid profiles and gut microbiota-derived tryptophan metabolites of five types of cancer patients. Amino Acids 2023. [Google Scholar] [CrossRef]
- Liu, N.; Shi, F.; Yang, L.; Liao, W.; Cao, Y. Oncogenic viral infection and amino acid metabolism in cancer progression: Molecular insights and clinical implications. Biochim. Biophys. Acta (BBA)-Rev. Cancer 2022, 1877, 188724. [Google Scholar] [CrossRef]
- Kubota, A.; Meguid, M.M.; Hitch, D.C. Amino acid profiles correlate diagnostically with organ site in three kinds of malignant tumors. Cancer 1992, 69, 2343–2348. [Google Scholar] [CrossRef]
- Cascino, A.; Muscaritoli, M.; Cangiano, C.; Conversano, L.; Laviano, A.; Ariemma, S.; Meguid, M.M.; Rossi Fanelli, F. Plasma amino acid imbalance in patients with lung and breast cancer. Anticancer Res. 1995, 15, 507–510. [Google Scholar] [PubMed]
- Proenza, A.M.A.; Oliver, J.J.; Palou, A.A.; Roca, P.P. Breast and lung cancer are associated with a decrease in blood cell amino acid content. J. Nutr. Biochem. 2003, 14, 133–138. [Google Scholar] [CrossRef]
- Minet-Quinard, R.; Van Praagh, I.; Kwiatkowski, F.; Beaujon, G.; Feillel, V.; Beaufrère, B.; Bargnoux, P.J.; Cynober, L.; Vasson, M.P. Pre- and postoperative aminoacidemia in breast cancer: A study vs. matched healthy subjects. Cancer Investig. 2004, 22, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Vissers, Y.L.J.; Dejong, C.H.C.; Luiking, Y.C.; Fearon, K.C.H.; von Meyenfeldt, M.F.; Deutz, N.E.P. Plasma arginine concentrations are reduced in cancer patients: Evidence for arginine deficiency? Am. J. Clin. Nutr. 2005, 81, 1142–1146. [Google Scholar] [CrossRef]
- Okamoto, N.; Miyagi, Y.; Chiba, A.; Akaike, M.; Shiozawa, M.; Imaizumi, A.; Yamamoto, H.; Ando, T.; Yamakado, M.; Tochikubo, O. Diagnostic modeling with differences in plasma amino acid profiles between non-cachectic colorectal/breast cancer patients and healthy individuals. Int. J. Med. Med. Sci. 2009, 1, 1–8. [Google Scholar]
- Poschke, I.; Mao, Y.; Kiessling, R.; Boniface, J. Tumor-dependent increase of serum amino acid levels in breast cancer patients has diagnostic potential and correlates with molecular tumor subtypes. J. Transl. Med. 2013, 11, 290. [Google Scholar] [CrossRef]
- Barnes, T.; Bell, K.; DiSebastiano, K.M.; Vance, V.; Hanning, R.; Russell, C.; Dubin, J.A.; Bahl, M.; Califaretti, N.; Campbell, C.; et al. Plasma amino acid profiles of breast cancer patients early in the trajectory of the disease differ from healthy comparison groups. Appl. Physiol. Nutr. Metab. 2014, 39, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Chen, T.; Fu, S.; Sun, X.; Wang, L.; Lu, Y.; Ding, S.; Ruan, G.; Teng, L.; Wang, M. Perioperative dynamics and significance of amino acid profiles in patients with cancer. J. Transl. Med. 2015, 13, 35. [Google Scholar] [CrossRef]
- Park, J.; Shin, Y.; Kim, T.H.; Kim, D.-H.; Lee, A. Plasma metabolites as possible biomarkers for diagnosis of breast cancer. PLoS ONE 2019, 14, e0225129. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, M.; Men, Y.; Wang, W.; Zhang, W. Heavy metals interfere with plasma metabolites, including lipids and amino acids, in patients with breast cancer. Oncol. Lett. 2020, 19, 2925–2933. [Google Scholar] [CrossRef]
- Politi, C.; Fattuoni, C.; Serra, A.; Noto, A.; Loi, S.; Casanova, A.; Faa, G.; Ravarino, A.; Saba, L. Metabolomic analysis of plasma from breast tumour patients. A pilot study. J. Public Health Res. 2021, 10, 2304. [Google Scholar] [CrossRef]
- An, R.; Yu, H.; Wang, Y.; Lu, J.; Gao, Y.; Xie, X.; Zhang, J. Integrative analysis of plasma metabolomics and proteomics reveals the metabolic landscape of breast cancer. Cancer Metab. 2022, 10, 13. [Google Scholar] [CrossRef]
- Baranovicova, E.; Racay, P.; Zubor, P.; Smolar, M.; Kudelova, E.; Halasova, E.; Dvorska, D.; Dankova, Z. Circulating metabolites in the early stage of breast cancer were not related to cancer stage or subtypes but associated with ki67 level. Promising statistical discrimination from controls. Mol. Cell. Probes 2022, 66, 101862. [Google Scholar] [CrossRef]
- Han, X.; Li, D.; Wang, S.; Lin, Y.; Liu, Y.; Lin, L.; Qiao, L. Serum amino acids quantification by plasmonic colloidosome-coupled MALDI-TOF MS for triple-negative breast cancer diagnosis. Mater. Today Bio 2022, 17, 100486. [Google Scholar] [CrossRef] [PubMed]
- Santaliz-Casiano, A.; Mehta, D.; Danciu, O.C.; Patel, H.; Banks, L.; Zaidi, A.; Buckley, J.; Rauscher, G.H.; Schulte, L.; Weller, L.R.; et al. Identification of metabolic pathways contributing to ER+ breast cancer disparities using a machine-learning pipeline. Sci. Rep. 2023, 13, 12136. [Google Scholar] [CrossRef] [PubMed]
- Panigoro, S.S.; Kurniawan, A.; Ramadhan, R.; Sukartini, N.; Herqutanto, H.; Paramita, R.I.; Sandra, F. Amino Acid Profile of Luminal A and B Subtypes Breast Cancer. Indones. Biomed. J. 2023, 15, 194–295. [Google Scholar] [CrossRef]
- Morad, H.M.; Abou-Elzahab, M.M.; Aref, S.; EL-Sokkary, A.M.A. Diagnostic Value of 1H NMR-Based Metabolomics in Acute Lymphoblastic Leukemia, Acute Myeloid Leukemia, and Breast Cancer. ACS Omega 2022, 7, 8128–8140. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.S.; Lee, J.C.; Lee, P.H.; Wang, S.T.; Chen, W.J. Plasma free amino acid profile in cancer patients. Semin. Cancer Biol. 2005, 15, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wang, Y.; Cai, H.; Wang, S.; Shen, Y.; Ke, C. Application of metabolomics in the diagnosis of breast cancer: A systematic review. J. Cancer 2020, 11, 2540–2551. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Gao, Y.; Cao, Y.; Zhang, Y.; Xu, M.; Wang, Y.; Jing, Y.; Guo, S.; Jing, F.; Hu, X.; et al. Identification of arginine and its “Downstream” molecules as potential markers of breast cancer. IUBMB Life 2016, 68, 817–822. [Google Scholar] [CrossRef]
- Budczies, J.; Denkert, C.; Muller, B.M.; Brockmoller, S.F.; Klauschen, F.; Gyorffy, B.; Dietel, M.; Richter-Ehrenstein, C.; Marten, U.; Salek, R.M.; et al. Remodeling of central metabolism in invasive breast cancer compared to normal breast tissue—A GC-TOFMS based metabolomics study. BMC Genom. 2012, 13, 334. [Google Scholar] [CrossRef]
- Budczies, J.; Brockmöller, S.F.; Müller, B.M.; Barupal, D.K.; Richter-Ehrenstein, C.; Kleine-Tebbe, A.; Griffin, J.L.; Orešič, M.; Dietel, M.; Denkert, C.; et al. Comparative metabolomics of estrogen receptor positive and estrogen receptor negative breast cancer: Alterations in glutamine and beta-alanine metabolism. J. Proteom. 2013, 94, 279–288. [Google Scholar] [CrossRef]
- Togashi, Y.; Arao, T.; Kato, H.; Matsumoto, K.; Terashima, M.; Hayashi, H.; de Velasco, M.A.; Fujita, Y.; Kimura, H.; Yasuda, T. Frequent amplification of ORAOV1 gene in esophageal squamous cell cancer promotes an aggressive phenotype via proline metabolism and ROS production. Oncotarget 2014, 5, 2962. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Beltrán, L.; González-Olmedo, C.; Luque-Caro, N.; Díaz, C.; Martín-Blázquez, A.; Fernández-Navarro, M.; Ortega-Granados, A.L.; Gálvez-Montosa, F.; Vicente, F.; Pérez del Palacio, J.; et al. Human Plasma Metabolomics for Biomarker Discovery: Targeting the Molecular Subtypes in Breast Cancer. Cancers 2021, 13, 147. [Google Scholar] [CrossRef] [PubMed]
- Tayyari, F.; Gowda, G.A.N.; Olopade, O.F.; Berg, R.; Yang, H.H.; Lee, M.P.; Ngwa, W.F.; Mittal, S.K.; Raftery, D.; Mohammed, S.I. Metabolic profiles of triple-negative and luminal A breast cancer subtypes in African-American identify key metabolic differences. Oncotarget 2018, 9, 11677–11690. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Chen, Z.; Anderson, G.L.; Rohan, T.; Aragaki, A.; Lane, D.; Dolan, N.C.; Paskett, E.D.; McTiernan, A.; Hubbell, F.A.; et al. Ethnicity and breast cancer: Factors influencing differences in incidence and outcome. J. Natl. Cancer Inst. 2005, 97, 439–448. [Google Scholar] [CrossRef]
- Kwan, M.L.; Kushi, L.H.; Weltzien, E.; Maring, B.; Kutner, S.E.; Fulton, R.S.; Lee, M.M.; Ambrosone, C.B.; Caan, B.J. Epidemiology of breast cancer subtypes in two prospective cohort studies of breast cancer survivors. Breast Cancer Res. 2009, 11, R31. [Google Scholar] [CrossRef] [PubMed]
- Amirikia, K.C.; Mills, P.; Bush, J.; Newman, L.A. Higher population-based incidence rates of triple-negative breast cancer among young African-American women: Implications for breast cancer screening recommendations. Cancer 2011, 117, 2747–2753. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Antoniou, A.C.; Easton, D.F.; Garcia-Closas, M. Genetic susceptibility to breast cancer. Mol. Oncol. 2010, 4, 174–191. [Google Scholar] [CrossRef]
- Pharoah, P.D.P.; Antoniou, A.C.; Easton, D.F.; Ponder, B.A.J. Polygenes, risk prediction, and targeted prevention of breast cancer. N. Engl. J. Med. 2008, 358, 2796–2803. [Google Scholar] [CrossRef] [PubMed]
- Gieger, C.; Geistlinger, L.; Altmaier, E.; Hrabé de Angelis, M.; Kronenberg, F.; Meitinger, T.; Mewes, H.W.; Wichmann, H.E.; Weinberger, K.M.; Adamski, J.; et al. Genetics meets metabolomics: A genome-wide association study of metabolite profiles in human serum. PLoS Genet. 2008, 4, e1000282. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Shen, J.; Moore, S.C.; Ye, Y.; Wu, X.; Esteva, F.J.; Tripathy, D.; Chow, W.H. Breast cancer risk in relation to plasma metabolites among Hispanic and African American women. Breast Cancer Res. Treat. 2019, 176, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Huo, M.; Zhang, J.; Huang, W.; Wang, Y. Interplay among metabolism, epigenetic modifcations, and gene expression in cancer. Front. Cell Dev. Biol. 2021, 9, 793428. [Google Scholar] [CrossRef]
- Jones, P.A. Functions of DNA methylation: Islands, start sites, gene bodies and beyond. Nat. Rev. Genet. 2012, 13, 484–492. [Google Scholar] [CrossRef]
- Herman, J.G.; Baylin, S.B. Gene silencing in cancer in association with promoter hypermethylation. N. Engl. J. Med. 2003, 349, 2042–2054. [Google Scholar] [CrossRef]
- Garcia-Martinez, L.; Zhang, Y.; Nakata, Y.; Chan, H.L.; Morey, L. Epigenetic mechanisms in breast cancer therapy and resistance. Nat. Commun. 2021, 12, 1786. [Google Scholar] [CrossRef]
- Mogol, A.N.; Zuo, Q.; Yoo, J.Y.; Kaminsky, A.Z.; Imir, O.B.; Landesman, Y.; Walker, C.J.; Erdogan, Z.M. NAD+ metabolism generates a metabolic vulnerability in endocrine-resistant metastatic breast tumors in females. Endocrinology 2023, 164, bqad073. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.C.; Kadlubar, S.; Su, L.J.; Acheampong, D.; Rogers, L.J.; Runnells, G.; McElfish, P.A.; Schootman, M. County poverty levels infuence genome-wide DNA methylation profles in African American and European American women. Transl. Cancer Res. 2019, 8, 683–692. [Google Scholar] [CrossRef]
- Moore, S.C.; Playdon, M.C.; Sampson, J.N.; Hoover, R.N.; Trabert, B.; Matthews, C.E.; Ziegler, R.G. A metabolomics analysis of body mass index and postmenopausal breast cancer risk. J. Natl. Cancer Inst. 2018, 110, 588–597. [Google Scholar] [CrossRef]
- Medina, V.; Cricco, G.; Nunez, M.; Martin, G.; Mohamad, N.; Correa-Fiz, F.; Sanchez-Jimenez, F.; Bergoc, R.; Rivera, E.S. Histamine-mediated signaling processes in human malignant mammary cells. Cancer Biol. Ther. 2006, 11, 1462–1471. [Google Scholar] [CrossRef]
- Wolfe, R.R. Branched-chain amino acids and muscle protein synthesis in humans: Myth or reality? J. Int. Soc. Sports Nutr. 2017, 14, 30. [Google Scholar] [CrossRef]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Zeleznik, O.A.; Balasubramanian, R.; Ren, Y.; Tobias, D.K.; Rosner, B.A.; Peng, C.; Bever, A.M.; Frueh, L.; Jeanfavre, S.; Avila-Pacheco, J.; et al. Branched-Chain Amino Acids and Risk of Breast Cancer. JNCI Cancer Spectr. 2021, 5, pkab059. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Wada, K.; Tsuji, M.; Hayashi, M.; Takeda, N.; Yasuda, K. Plasma amino acid profiles are associated with biomarkers of breast cancer risk in premenopausal Japanese women. Cancer Causes Control 2014, 25, 143–149. [Google Scholar] [CrossRef]
- Lécuyer, L.; Victor Bala, A.; Deschasaux, M.; Bouchemal, N.; Nawfal Triba, M.; Vasson, M.P.; Rossary, A.; Demidem, A.; Galan, P.; Hercberg, S.; et al. NMR metabolomic signatures reveal predictive plasma metabolites associated with long-term risk of developing breast cancer. Int. J. Epidemiol. 2018, 47, 484–494. [Google Scholar] [CrossRef]
- His, M.; Viallon, V.; Dossus, L.; Gicquiau, A.; Achaintre, D.; Scalbert, A.; Ferrari, P.; Romieu, I.; Onland-Moret, N.C.; Weiderpass, E.; et al. Prospective analysis of circulating metabolites and breast cancer in EPIC. BMC Med. 2019, 17, 178. [Google Scholar] [CrossRef]
- Zhang, J.; Tao, B.; Chong, Y.; Ma, S.; Wu, G.; Zhu, H.; Zhao, Y.; Zhao, S.; Niu, M.; Zhang, S.; et al. Ornithine and breast cancer: A matched case-control study. Sci. Rep. 2020, 10, 15502. [Google Scholar] [CrossRef] [PubMed]
- Jobard, E.; Dossus, L.; Baglietto, L.; Fornili, M.; Lécuyer, L.; Mancini, F.R.; Gunter, M.J.; Trédan, O.; Boutron-Ruault, M.C.; Elena-Herrmann, B.; et al. Investigation of circulating metabolites associated with breast cancer risk by untargeted metabolomics: A case-control study nested within the French E3N cohort. Br. J. Cancer 2021, 124, 1734–1743. [Google Scholar] [CrossRef] [PubMed]
- Stevens, V.L.; Carter, B.D.; Jacobs, E.J.; McCullough, M.L.; Teras, L.R.; Wang, Y. A prospective case–cohort analysis of plasma metabolites and breast cancer risk. Breast Cancer Res. 2023, 25, 5. [Google Scholar] [CrossRef] [PubMed]
- Kühn, T.; Floegel, A.; Sookthai, D.; Johnson, T.; Rolle-Kampczyk, U.; Otto, W.; von Bergen, M.; Boeing, H.; Kaaks, R. Higher plasma levels of lysophosphatidylcholine 18:0 are related to a lower risk of common cancers in a prospective metabolomics study. BMC Med. 2016, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Lécuyer, L.; Dalle, C.; Lyan, B.; Demidem, A.; Rossary, A.; Vasson, M.P.; Petera, M.; Lagree, M.; Ferreira, T.; Centeno, D.; et al. Plasma metabolomic signatures associated with long-term breast cancer risk in the SU. VI. MAX prospective cohort. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1300–1307. [Google Scholar] [CrossRef]
- Jung, M.K.; Okekunle, A.P.; Lee, J.E.; Sung, M.K.; Lim, Y.J. Role of Branched-chain Amino Acid Metabolism in Tumor Development and Progression. J. Cancer Prev. 2021, 26, 237–243. [Google Scholar] [CrossRef]
- Chi, R.; Yao, C.; Chen, S.; Liu, Y.; He, Y.; Zhang, J.; Ellies, L.G.; Wu, X.; Zhao, Q.; Zhou, C.; et al. Elevated BCAA suppresses the development and metastasis of breast cancer. Front. Oncol. 2022, 12, 887257. [Google Scholar] [CrossRef]
- Tobias, D.K.; Chai, B.; Tamimi, R.M.; Manson, J.E.; Hu, F.B.; Willett, W.C.; Eliassen, A.H. Dietary Intake of Branched Chain Amino Acids and Breast Cancer Risk in the NHS and NHS II Prospective Cohorts. JNCI Cancer Spectr. 2021, 5, pkab032. [Google Scholar] [CrossRef]
- Nouri-Majd, S.; Salari-Moghaddam, A.; Benisi-Kohansal, S.; Azadbakht, L.; Esmaillzadeh, A. Dietary intake of branched-chain amino acids in relation to the risk of breast cancer. Breast Cancer 2022, 29, 993–1000. [Google Scholar] [CrossRef]
- Mrowiec, K.; Kurczyk, A.; Jelonek, K.; Debik, J.; Giskeødegård, G.F.; Bathen, T.F.; Widłak, P. Association of serum metabolome profile with the risk of breast cancer in participants of the HUNT2 study. Front. Oncol. 2023, 13, 1116806. [Google Scholar] [CrossRef]
- Risi, E.; Lisanti, C.; Vignoli, A.; Biagioni, C.; Paderi, A.; Cappadona, S.; Monte, F.D.; Moretti, E.; Sanna, G.; Livraghi, L.; et al. Risk assessment of disease recurrence in early breast cancer: A serum metabolomic study focused on elderly patients. Transl. Oncol. 2023, 27, 101585. [Google Scholar] [CrossRef]
- Hart, C.D.; Vignoli, A.; Tenori, L.; Uy, G.L.; Van To, T.; Adebamowo, C.; Hossain, S.M.; Biganzoli, L.; Risi, E.; Love, R.R.; et al. Serum Metabolomic Profiles Identify ER-Positive Early Breast Cancer Patients at Increased Risk of Disease Recurrence in a Multicenter Population. Clin. Cancer Res. 2017, 23, 1422–1431. [Google Scholar] [CrossRef]
- Yatabe, J.; Yatabe, M.S.; Ishibashi, K.; Nozawa, Y.; Sanada, H. Early detection of colon cancer by amino acid profiling using AminoIndex Technology: A case report. Diagn. Pathol. 2013, 8, 203. [Google Scholar] [CrossRef]
- Maeda, J.; Higashiyama, M.; Imaizumi, A.; Nakayama, T.; Yamamoto, H.; Daimon, T.; Yamakado, M.; Imamura, F.; Kodama, K. Possibility of multivariate function composed of plasma amino acid profiles as a novel screening index for non-small cell lung cancer: A case control study. BMC Cancer 2010, 10, 690. [Google Scholar] [CrossRef]
- Okamoto, N. Use of ‘AminoIndex Technology’ for cancer screening. Ningen Dock 2012, 26, 911–922. [Google Scholar]
- Jikuzono, T.; Ishibashi, O.; Kure, S.; Ohmae, Y.; Ohmae, T. Associations of AminoIndex Cancer Screening (Breast) Grade with Clinical and Laboratory Variables. J. Nippon Med. Sch. 2022, 89, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Miyagi, Y.; Chiba, A.; Shiozawa, M.; Akaike, M.; Imaizumi, A.; Ando, T.; Tochikubo, O. Multivariate discrimination functions composed with amino acid profiles (Amino Index®) as a novel diagnostic marker for breast and colon cancer. Cancer Prev. 2008, 6, 47–48. [Google Scholar] [CrossRef]
- Wei, Z.; Liu, X.; Cheng, C.; Yu, W.; Yi, P. Metabolism of Amino Acids in Cancer. Front. Cell Dev. Biol. 2020, 8, 603837. [Google Scholar] [CrossRef] [PubMed]
- Geck, R.C.; Toker, A. Nonessential amino acid metabolism in breast cancer. Adv. Biol. Regul. 2016, 62, 11–17. [Google Scholar] [CrossRef]
- Subramani, R.; Poudel, S.; Smith, K.D.; Estrada, A.; Lakshmanaswamy, R. Metabolomics of Breast Cancer: A Review. Metabolites 2022, 12, 643. [Google Scholar] [CrossRef]
- Willmann, L.; Schlimpert, M.; Halbach, S.; Erbes, T.; Stickeler, E.; Kammerer, B. Metabolic profiling of breast cancer: Differences in central metabolism between subtypes of breast cancer cell lines. J. Chromatogr B Anal. Technol. Biomed. Life Sci. 2015, 1000, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Wang, Y.; Alatrash, N.; Weatherly, C.A.; Roy, D.; MacDonnell, F.M.; Armstrong, D.W. Altered profiles and metabolism of land d-amino acids in cultured human breast cancer cells vs. non-tumorigenic human breast epithelial cells. J. Pharm. Biomed. Anal. 2019, 164, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Sun, T.; Cao, Y.; Gao, P.; Dong, J.; Fang, Y.; Fang, Z.; Sun, X.; Zhu, Z. A dried blood spot mass spectrometry metabolomic approach for rapid breast cancer detection. Onco Targets Ther. 2016, 9, 1389–1398. [Google Scholar] [PubMed]
- Jain, M.; Nilsson, R.; Sharma, S.; Madhusudhan, N.; Kitami, T.; Souza, A.L.; Kafri, R.; Kirschner, M.W.; Clish, C.B.; Mootha, V.K. Metabolite profiling identifies a key role for glycine in rapid cancer cell proliferation. Science 2012, 336, 1040–1044. [Google Scholar] [CrossRef]
- Craze, M.L.; Cheung, H.; Jewa, N.; Coimbra, N.D.M.; Soria, D.; El-Ansari, R.; Aleskandarany, M.A.; Wai Cheng, K.; Diez-Rodriguez, M.; Nolan, C.C.; et al. MYC regulation of glutamine-proline regulatory axis is key in luminal B breast cancer. Br. J. Cancer 2018, 118, 258–265. [Google Scholar] [CrossRef]
- Cha, Y.J.; Kim, E.S.; Koo, J.S. Amino Acid Transporters and Glutamine Metabolism in Breast Cancer. Int. J. Mol. Sci. 2018, 19, 907. [Google Scholar] [CrossRef]
- Coloff, J.L.; Murphy, J.P.; Braun, C.R.; Harris, I.S.; Shelton, L.M.; Kami, K.; Gygi, S.P.; Selfors, L.M.; Brugge, J.S. Differential glutamate metabolism in proliferating and quiescent mammary epithelial cells. Cell Metab. 2016, 23, 867–880. [Google Scholar] [CrossRef]
- El Ansari, R.; McIntyre, A.; Craze, M.L.; Ellis, I.O.; Rakha, E.A.; Green, A.R. Altered glutamine metabolism in breast cancer; subtype dependencies and alternative adaptations. Histopathology 2018, 72, 183–190. [Google Scholar] [CrossRef]
- Dowling, P.; Henry, M.; Meleady, P.; Clarke, C.; Gately, K.; O’Byrne, K.; Connolly, E.; Lynch, V.; Ballot, J.; Gullo, G.; et al. Metabolomic and proteomic analysis of breast cancer patient samples suggests that glutamate and 12-HETE in combination with CA15-3 may be useful biomarkers reflecting tumour burden. Metabolomics 2015, 11, 620–635. [Google Scholar] [CrossRef]
- Kandasamy, P.; Gyimesi, G.; Kanai, Y.; Hediger, M.A. Amino acid transporters revisited: New views in health and disease. Trends Biochem. Sci. 2018, 43, 752–789. [Google Scholar] [CrossRef]
- Bhutia, Y.D.; Babu, E.; Ramachandran, S.; Ganapathy, V. Amino Acid transporters in cancer and their relevance to “glutamine addiction”: Novel targets for the design of a new class of anticancer drugs. Cancer Res. 2015, 75, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- van Geldermalsen, M.; Wang, Q.; Nagarajah, R.; Marshall, A.D.; Thoeng, A.; Gao, D.; Ritchie, W.; Feng, Y.; Bailey, C.G.; Deng, N.; et al. ASCT2/SLC1A5 controls glutamine uptake and tumour growth in triple-negative basal-like breast cancer. Oncogene 2016, 35, 3201–3208. [Google Scholar] [CrossRef] [PubMed]
- Metallo, C.M.; Gameiro, P.A.; Bell, E.L.; Mattaini, K.R.; Yang, J.; Hiller, K.; Jewell, C.M.; Johnson, Z.R.; Irvine, D.J.; Guarente, L.; et al. Reductive glutamine metabolism by IDH1 mediates lipogenesis under hypoxia. Nature 2011, 481, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Le, A.; Lane, A.N.; Hamaker, M.; Bose, S.; Gouw, A.; Barbi, J.; Tsukamoto, T.; Rojas, C.J.; Slusher, B.S.; Zhang, H.; et al. Glucoseindependent glutamine metabolism via TCA cycling for proliferation and survival in B cells. Cell Metab. 2012, 15, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Meadows, A.L.; Kong, B.; Berdichevsky, M.; Roy, S.; Rosiva, R.; Blanch, H.W.; Clark, D.S. Metabolic and morphological differences between rapidly proliferating cancerous and normal breast epithelial cells. Biotechnol. Prog. 2008, 24, 334–341. [Google Scholar] [CrossRef]
- Budczies, J.; Pfitzner, B.M.; Györffy, B.; Winzer, K.-J.; Radke, C.; Dietel, M.; Fiehn, O.; Denkert, C. Glutamate enrichment as new diagnostic opportunity in breast cancer. Int. J. Cancer 2015, 136, 1619–1628. [Google Scholar] [CrossRef]
- Zhou, W.-X.; Chen, C.; Liu, X.-Q.; Li, Y.; Lin, Y.-L.; Wu, X.-T.; Kong, L.-Y.; Luo, J.-G. Discovery and optimization of withangulatin A derivatives as novel glutaminase 1 inhibitors for the treatment of triple-negative breast cancer. Eur. J. Med. Chem. 2021, 210, 112980. [Google Scholar] [CrossRef]
- Garcia-Caballero, M.; Neugebauer, E.; Campos, R.; Nunez de Castro, I.; Vara-Thorbeck, C. Increased histidine decarboxylase (HDC) activity in human colorectal cancer: Results of a study on ten patients. Agents Actions 1988, 23, 357–360. [Google Scholar] [CrossRef]
- Xie, G.; Zhou, B.; Zhao, A.; Qiu, Y.; Zhao, X.; Garmire, L.; Shvetsov, Y.B.; Yu, H.; Yen, Y.; Jia, W. Lowered circulating aspartate is a metabolic feature of human breast cancer. Oncotarget 2015, 6, 33369–33381. [Google Scholar] [CrossRef]
- Knott, S.R.V.; Wagenblast, E.; Khan, S.; Kim, S.Y.; Soto, M.; Wagner, M.; Turgeon, M.-O.; Fish, L.; Erard, N.; Gable, A.L.; et al. Asparagine bioavailability governs metastasis in a model of breast cancer. Nature 2018, 554, 378–381. [Google Scholar] [CrossRef]
- Sivanand, S.; Vander Heiden, M.G. Emerging roles for branched-chain amino acid metabolism in cancer. Cancer Cell 2020, 37, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Harvie, M.N.; Campbell, I.T.; Howell, A.; Thatcher, N. Acceptability and tolerance of a low tyrosine and phenylalanine diet in patients with advanced cancer—A pilot study. J. Hum. Nutr. Diet. 2002, 15, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Atoum, M.; Abdel-Fattah, M.; Nimer, N.; Abdel-Rahman, S.; Abdeldayem, S.A. Association of alanine-valine manganese superoxide dismutase gene polymorphism and microheterogeneity manganese superoxide dismutase activity in breast cancer and benign breast tissue. J. Breast Cancer 2012, 15, 157–161. [Google Scholar] [CrossRef]
- Nittoli, A.C.; Costantini, S.; Sorice, A.; Capone, F.; Ciarcia, R.; Marzocco, S.; Budillon, A.; Severino, L. Effects of α-zearalenol on the metabolome of two breast cancer cell lines by 1H-NMR approach. Metabolomics 2018, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Feng, Y.; Zhang, Y.; Zhu, X.; Jin, F. L-Arginine supplementation inhibits the growth of breast cancer by enhancing innate and adaptive immune responses mediated by suppression of MDSCs in vivo. BMC Cancer 2016, 16, 343. [Google Scholar] [CrossRef] [PubMed]
- Opitz, C.A.; Litzenburger, U.M.; Sahm, F.; Ott, M.; Tritschler, I.; Trump, S.; Schumacher, T.; Jestaedt, L.; Schrenk, D.; Weller, M.; et al. An endogenous tumour-promoting ligand of the human aryl hydrocarbon receptor. Nature 2011, 478, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Yue, L.; Shi, J.; Shao, M.; Wu, T. Role of IDO and TDO in Cancers and Related Diseases and the Therapeutic Implications. J. Cancer 2019, 10, 2771–2782. [Google Scholar] [CrossRef]
- Cheong, J.E.; Sun, L. Targeting the IDO1/TDO2–KYN–AhR Pathway for Cancer Immunotherapy—Challenges and Opportunities. Trends Pharmacol. Sci. 2018, 39, 307–325. [Google Scholar] [CrossRef]
- Platten, M.; Wick, W.; Van de Eynde, B.J. Tryptophan Catabolism in Cancer: Beyond IDO and Tryptophan Depletion. Cancer Res. 2012, 72, 5435–5440. [Google Scholar] [CrossRef]
- Pollari, S.; Käkönen, S.M.; Edgren, H.; Wolf, M.; Kohonen, P.; Sara, H.; Guise, T.; Nees, M.; Kallioniemi, O. Enhanced serine production by bone metastatic breast cancer cells stimulates osteoclastogenesis. Breast Cancer Res. Treat. 2011, 125, 421–430. [Google Scholar] [CrossRef]
- Maddocks, O.D.K.; Athineos, D.; Cheung, E.C.; Lee, P.; Zhang, T.; van den Broek, N.J.F.; Mackay, G.M.; Labuschagne, C.F.; Gay, D.; Kruiswijk, F.; et al. Modulating the therapeutic response of tumours to dietary serine and glycine starvation. Nature 2017, 544, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Vettore, L.; Westbrook, R.L.; Tennant, D.A. New aspects of amino acid metabolism in cancer. Br. J. Cancer 2020, 122, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Lee, I.M.; Song, Y.; Cook, N.R.; Selhub, J.; Manson, J.E.; Buring, J.E.; Zhang, S.M. Plasma homocysteine and cysteine and risk of breast cancer in women. Cancer Res. 2010, 70, 2397–2405. [Google Scholar] [CrossRef]
- Bonifácio, V.D.B.; Pereira, S.A.; Serpa, J.; Vicente, J.B. Cysteine metabolic circuitries: Druggable targets in cancer. Br. J. Cancer 2021, 124, 862–879. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.J.; Chang, W.A.; Chuang, C.H.; Wu, K.L.; Cheng, C.H.; Sheu, C.C.; Hsu, Y.L.; Hung, J.Y. Cysteinyl leukotriene pathway and cancer. Int. J. Mol. Sci. 2021, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Haukaas, T.H.; Euceda, L.R.; Giskeødegård, G.F.; Bathen, T.F. Metabolic Portraits of Breast Cancer by HR MAS MR Spectroscopy of Intact Tissue Samples. Metabolites 2017, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Cho, H.T.; Williams, L.; Zhu, A.; Liang, K.; Huang, K.; Wu, H.; Jiang, C.; Hong, S.; Crowe, R.; et al. Potential biomarker of L-type amino acid transporter 1 in breast cancer progression. Nucl. Med. Mol. Imaging 2011, 45, 93–102. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Schuster, D.M. Amino Acid Metabolism as a Target for Breast Cancer Imaging. PET Clin. 2018, 13, 437–444. [Google Scholar] [CrossRef]
- Hayashi, K.; Anzai, N. L-type amino acid transporter 1 as a target for inflammatory disease and cancer immunotherapy. J. Pharmacol. Sci. 2022, 148, 31–40. [Google Scholar] [CrossRef]
- Bhat, H.K.; Vadgama, J.V. Role of estrogen receptor in the regulation of estrogen induced amino acid transport of System A in breast cancer and other receptor positive tumor cells. Int. J. Mol. Med. 2002, 9, 271–279. [Google Scholar] [CrossRef]
- Shennan, D.B.; Thomson, J. Inhibition of system L (LAT1/CD98hc) reduces the growth of cultured human breast cancer cells. Oncol. Rep. 2008, 20, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.; Choi, C.M.; Ahn, S.H.; Lee, J.W.; Gong, G.; Ryu, J.S.; Oh, S.J.; Bacher-Stier, C.; Fels, L.; Koglin, N.; et al. Exploratory clinical trial of (4s)-4-(3-[18f]fluoropropyl)-l-glutamate for imaging xc-transporter using positron emission tomography in patients with non-small cell lung or breast cancer. Clin. Cancer Res. 2012, 18, 5427–5437. [Google Scholar] [CrossRef]
- Saito, Y.; Soga, T. Amino acid transporters as emerging therapeutic targets in cancer. Cancer Sci. 2021, 112, 2958–2965. [Google Scholar] [CrossRef] [PubMed]
- Lindholm, P.; Lapela, M.; Någren, K.; Lehikoinen, P.; Minn, H.; Jyrkkiö, S. Preliminary study of carbon-11 methionine PET in the evaluation of early response to therapy in advanced breast cancer. Nucl. Med. Commun. 2009, 30, 30–36. [Google Scholar] [CrossRef]
- Mehravi, B.; Ardestani, M.S.; Damercheli, M.; Soltanghoraee, H.; Ghanaldarlaki, N.; Alizadeh, A.M.; Oghabian, M.A.; Shirazi, M.S.; Mahernia, S.; Amanlou, M. Breast Cancer Cells Imaging by Targeting Methionine Transporters with Gadolinium-Based Nanoprobe. Mol. Imaging Biol. 2014, 16, 519–528. [Google Scholar] [CrossRef]
- Taylor, K.M.; Kim, J.S.; Rieter, W.J.; An, H.; Lin, W.; Lin, W. Mesoporous silica nanospheres as highly efficient MRI contrast agents. J. Am. Chem. Soc. 2008, 130, 2154–2155. [Google Scholar] [CrossRef]
- Okudaira, H.; Nakanishi, T.; Oka, S.; Kobayashi, M.; Tamagami, H.; Schuster, D.M.; Goodman, M.M.; Shirakami, Y.; Tamai, I.; Kawai, K. Kinetic analyses of trans-1-amino-3-[18F]fluorocyclobutanecarboxylic acid transport in Xenopus laevis oocytes expressing human ASCT2 and SNAT2. Nucl. Med. Biol. 2013, 40, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Okudaira, H.; Ono, M.; Schuster, D.M.; Goodman, M.M.; Kawai, K.; Shirakami, Y. Differences in transport mechanisms of trans-1-amino-3-[18F] fluorocyclobutanecarboxylic acid in inflammation, prostate cancer, and glioma cells: Comparison with L-[methyl-11C]methionine and 2-deoxy-2-[18F]fluoro-D-glucose. Mol. Imaging Biol. 2014, 16, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Tade, F.I.; Cohen, M.A.; Styblo, T.M.; Odewole, O.A.; Holbrook, A.I.; Newell, M.S.; Savir-Baruch, B.; Li, X.; Goodman, M.M.; Nye, J.A.; et al. Anti-3-18FFACBC (18F-Fluciclovine) PET/CT of breast cancer: An exploratory study. J. Nucl. Med. 2016, 57, 1357–1363. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Goldman, D.A.; Corben, A.; Lyashchenko, S.K.; Gönen, M.; Lewis, J.S.; Dickler, M. Prospective clinical trial of 18F-fluciclovine PET/CT for determining the response to neoadjuvant therapy in invasive ductal and invasive lobular breast cancers. J. Nucl. Med. 2017, 58, 1037–1042. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Goldman, D.A.; Gonen, M.; Pham, H.; Castillo, R.; Lyashchenko, S.K.; Lewis, J.S.; Dang, C. Initial results of a prospective clinical trial of 18f-fluciclovine pet/ct in newly diagnosed invasive ductal and invasive lobular breast cancers. J. Nucl. Med. 2016, 57, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Kanagawa, M.; Doi, Y.; Schuster, D.M.; Goodman, M.M.; Yoshimura, H. Fasting enhances the contrast of bone metastatic lesions in 18F-fluciclovine-PET: Preclinical study using a rat model of mixed osteolytic/osteoblastic bone metastases. Int. J. Mol. Sci. 2017, 18, 934. [Google Scholar] [CrossRef] [PubMed]
- Koglin, N.; Mueller, A.; Berndt, M.; Schmitt-Willich, H.; Toschi, L.; Stephens, A.W.; Gekeler, V.; Friebe, M.; Dinkelborg, L.M. Specific PET imaging of xC-transporter activity using a (1)(8)Flabeled glutamate derivative reveals a dominant pathway in tumor metabolism. Clin. Cancer Res. 2011, 17, 6000–6011. [Google Scholar] [CrossRef]
- Yang, H.; Jenni, S.; Colovic, M.; Merkens, H.; Poleschuk, C.; Rodrigo, I.; Miao, Q.; Johnson, B.F.; Rishel, M.J.; Sossi, V.; et al. (18)f-5-fluoroaminosuberic acid as a potential tracer to gauge oxidative stress in breast cancer models. J. Nucl. Med. 2017, 58, 367–373. [Google Scholar] [CrossRef]
- Kole, A.C.; Nieweg, O.E.; Pruim, J.; Paans, A.M.; Plukker, J.T.; Hoekstra, H.J.; Schraffordt Koops, H.; Vaalburg, W. Standardized uptake value and quantification of metabolism for breast cancer imaging with FDG and L-[1-11C]tyrosine PET. J. Nucl. Med. 1997, 38, 692–696. [Google Scholar] [PubMed]
- Kong, F.L.; Ali, M.S.; Rollo, A.; Smith, D.L.; Zhang, Y.; Yu, D.F.; Yang, D.J. Development of tyrosine-based radiotracer 99mTc-N4-Tyrosine for breast cancer imaging. J. Biomed. Biotechnol. 2012, 2012, 671708. [Google Scholar] [CrossRef]
- Kaim, A.H.; Weber, B.; Kurrer, M.O.; Westera, G.; Schweitzer, A.; Gottschalk, J.; von Schulthess, G.K.; Buck, A. (18)f-fdg and (18)f-fet uptake in experimental soft tissue infection. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Rau, F.C.; Weber, W.A.; Wester, H.J.; Herz, M.; Becker, I.; Kruger, A.; Schwaiger, M.; Senekowitsch-Schmidtke, R. O-(2-[(18)f]fluoroethyl)-l-tyrosine (fet): A tracer for differentiation of tumour from inflammation in murine lymph nodes. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 1039–1046. [Google Scholar] [CrossRef]
- Ren, W.; Liu, G.; Yin, J.; Tan, B.; Wu, G.; Bazer, F.W.; Peng, Y.; Yin, Y. Amino-acid transporters in t-cell activation and differentiation. Cell Death Dis. 2017, 8, e2655. [Google Scholar] [CrossRef]
- Yu, W.; McConathy, J.; Olson, J.J.; Goodman, M.M. System a amino acid transport-targeted brain and systemic tumor PET imaging agents 2-amino-3-[(18)F]fluoro-2-methylpropanoic acid and 3-[(18)F]fluoro-2-methyl2-(methylamino)propanoic acid. Nucl. Med. Biol. 2015, 42, 8–18. [Google Scholar] [CrossRef]
- Way, J.D.; Wang, M.; Hamann, I.; Wuest, M.; Wuest, F. Synthesis and evaluation of 2-amino-5-(4-[(18)f]fluorophenyl)pent-4-ynoic acid ([(18)f]fphpa): A novel (18)f-labeled amino acid for oncologic pet imaging. Nucl. Med. Biol. 2014, 41, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Michelhaugh, S.K.; Muzik, O.; Guastella, A.R.; Klinger, N.V.; Polin, L.A.; Cai, H.; Xin, Y.; Mangner, T.J.; Zhang, S.; Juhász, C.; et al. Assessment of tryptophan uptake and kinetics using 1-(2-18F-fluoroethyl)-l-tryptophan and alpha-11Cmethyl-l-tryptophan PET imaging in mice implanted with patient-derived brain tumor xenografts. J. Nucl. Med. 2017, 58, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Chin, B.B.; McDougald, D.; Weitzel, D.H.; Hawk, T.; Reiman, R.E.; Zalutsky, M.R.; Vaidyanathan, G. Synthesis and preliminary evaluation of 5-[18F]fluoroleucine. Curr. Radiopharm. 2017, 10, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Pantel, A.R.; Li, S.; Lieberman, B.P.; Ploessl, K.; Choi, H.; Blankemeyer, E.; Lee, H.; Kung, H.F.; Mach, R.H.; et al. [18F](2S,4R)4-fluoroglutamine PET detects glutamine pool size changes in triple-negative breast cancer in response to glutaminase inhibition. Cancer Res. 2017, 77, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Kopka, K.; Riemann, B.; Friedrich, M.; Winters, S.; Halfter, H.; Weckesser, M.; Stögbauer, F.; Bernd Ringelstein, E.; Schober, O. Characterization of 3-[123i]iodo-l-α-methyl tyrosine transport in astrocytes of neonatal rats. J. Neurochem. 2001, 76, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Jager, P.L.; Franssen, E.J.; Kool, W.; Szabo, B.G.; Hoekstra, H.J.; Groen, H.J.; de Vries, E.G.; van Imhoff, G.W.; Vaalburg, W.; Piers, D.A. Feasibility of tumor imaging using l-3-[iodine-123]-iodo-alpha-methyl-tyrosine in extracranial tumors. J. Nucl. Med. 1998, 39, 1736–1743. [Google Scholar]
- Sharma, S.; Singh, B.; Mishra, A.K.; Rathod, D.; Hazari, P.P.; Chuttani, K.; Chopra, S.; Singh, P.M.; Abrar, M.L.; Mittal, B.R.; et al. Lat-1 based primary breast cancer detection by [99m]tc-labeled dtpa-bis-methionine scintimammography: First results using indigenously developed single vial kit preparation. Cancer Biotherapy Radiopharm. 2014, 29, 283–288. [Google Scholar] [CrossRef]
- Brandon, F.; Ashley, S. Deberardinis RJ. Metabolic reprogramming and cancer progression. Science 2020, 368, eaaw5473. [Google Scholar]
- Chowdhry, S.; Zanca, C.; Rajkumar, U.; Koga, T.; Diao, Y.; Raviram, R.; Liu, F.; Turner, K.; Yang, H.; Brunk, E.; et al. NAD metabolic dependency in cancer is shaped by gene amplification and enhancer remodelling. Nature 2019, 569, 570–575. [Google Scholar] [CrossRef]
- Bian, Y.; Li, W.; Kremer, D.M.; Sajjakulnukit, P.; Li, S.; Crespo, J.; Nwosu, Z.C.; Zhang, L.; Czerwonka, A.; Pawłowska, A.; et al. Cancer SLC43A2 alters T cell methionine metabolism and histone methylation. Nature 2020, 585, 277–282. [Google Scholar] [CrossRef]
- Gao, X.; Sanderson, S.M.; Dai, Z.; Reid, M.A.; Cooper, D.E.; Lu, M.; Richie, J.P., Jr.; Ciccarella, A.; Calcagnotto, A.; Mikhael, P.G.; et al. Dietary methionine influences therapy in mouse cancer models and alters human metabolism. Nature 2019, 572, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Kanarek, N.; Keys, H.R.; Cantor, J.R.; Lewis, C.A.; Chan, S.H.; Kunchok, T.; Abu-Remaileh, M.; Freinkman, E.; Schweitzer, L.D.; Sabatini, D.M. Histidine catabolism is a major determinant of methotrexate sensitivity. Nature 2018, 559, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Sadik, A.; Somarribas Patterson, L.F.; Öztürk, S.; Mohapatra, S.R.; Panitz, V.; Secker, P.F.; Pfänder, P.; Loth, S.; Salem, H.; Prentzell, M.T.; et al. IL4I1 is a metabolic immune checkpoint that activates the AHR and promotes tumor progression. Cell 2020, 182, 1252–1270. [Google Scholar] [CrossRef] [PubMed]
- Strekalova, E.; Malin, D.; Weisenhorn, E.M.M.; Russell, J.D.; Hoelper, D.; Jain, A.; Coon, J.J.; Lewis, P.W.; Cryns, V.L. S-adenosylmethionine biosynthesis is a targetable metabolic vulnerability of cancer stem cells. Breast Cancer Res. Treat. 2019, 175, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Li, L.; Coyaud, E.; Luna, A.; Sander, C.; Raught, B.; Asara, J.M.; Brown, M.; Muthuswamy, S.K. LLGL2 rescues nutrient stress by promoting leucine uptake in ER+ breast cancer. Nature 2019, 569, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Li, C.F.; Kuo, C.C.; Tsai, K.K.; Hou, M.F.; Hung, W.C. Cancer/stroma interplay via cyclooxygenase-2 and indoleamine 2,3-dioxygenase promotes breast cancer progression. Breast Cancer Res. 2014, 16, 410. [Google Scholar] [CrossRef]
- Greene, L.I.; Bruno, T.C.; Christenson, J.L.; D’Alessandro, A.; Culp-Hill, R.; Torkko, K.; Borges, V.F.; Slansky, J.E.; Richer, J.K. A Role for Tryptophan-2,3-dioxygenase in CD8 T-cell Suppression and Evidence of Tryptophan Catabolism in Breast Cancer Patient Plasma. Mol. Cancer Res. 2019, 17, 131–139. [Google Scholar] [CrossRef]
- Zhao, Y.; Pu, C.; Liu, Z. Essential amino acids deprivation is a potential strategy for breast cancer treatment. Breast 2022, 62, 152–161. [Google Scholar] [CrossRef]
- Zhang, L.; Han, J. Branched-chain amino acid transaminase 1 (BCAT1) promotes the growth of breast cancer cells through improving mTOR-mediated mitochondrial biogenesis and function. Biochem. Biophys. Res. Commun. 2017, 486, 224–231. [Google Scholar] [CrossRef]
- El Ansari, R.; Craze, M.L.; Miligy, I.; Diez-Rodriguez, M.; Nolan, C.C.; Ellis, I.O.; Rakha, E.A.; Green, A.R. The amino acid transporter SLC7A5 confers a poor prognosis in the highly proliferative breast cancer subtypes and is a key therapeutic target in luminal B tumours. Breast Cancer Res. 2018, 20, 21. [Google Scholar] [CrossRef]
- Cao, M.D.; Lamichhane, S.; Lundgren, S.; Bofin, A.; Fjøsne, H.; Giskeødegård, G.F.; Bathen, T.F. Metabolic characterization of triple negative breast cancer. BMC Cancer 2014, 14, 941. [Google Scholar] [CrossRef]
- Lampa, M.; Arlt, H.; He, T.; Ospina, B.; Reeves, J.; Zhang, B.; Murtie, J.; Deng, G.; Barberis, C.; Hoffmann, D.; et al. Glutaminase is essential for the growth of triple-negative breast cancer cells with a deregulated glutamine metabolism pathway and its suppression synergizes with mTOR inhibition. PLoS ONE 2017, 12, e0185092. [Google Scholar] [CrossRef] [PubMed]
- Mates, J.M.; Campos-Sandoval, J.A.; Marquez, J. Glutaminase isoenzymes in the metabolic therapy of cancer. Biochim. Biophys. Acta Rev. Cancer 2018, 1870, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Stalnecker, C.; Zhang, C.; McDermott, L.A.; Iyer, P.; O’Neill, J.; Reimer, S.; Cerione, R.A.; Katt, W.P. Characterization of the interactions of potent allosteric inhibitors with glutaminase C, a key enzyme in cancer cell glutamine metabolism. J. Biol. Chem. 2018, 293, 3535–3545. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Fu, R.; Duan, Z.; Shen, S.; Zhu, C.; Fan, D. Ginsenoside CK induces apoptosis in triple-negative breast cancer cells by targeting glutamine metabolism. Biochem. Pharmacol. 2022, 202, 115101. [Google Scholar] [CrossRef]
- Morotti, M.; Zois, C.E.; El-Ansari, R.; Craze, M.L.; Rakha, E.A.; Fan, S.J.; Valli, A.; Haider, S.; Goberdhan, D.C.I.; Green, A.R.; et al. Increased expression of glutamine transporter SNAT2/SLC38A2 promotes glutamine dependence and oxidative stress resistance, and is associated with worse prognosis in triple-negative breast cancer. Br. J. Cancer 2021, 124, 494–505. [Google Scholar] [CrossRef]
- Timmerman, L.A.; Holton, T.; Yuneva, M.; Louie, R.J.; Padró, M.; Daemen, A.; Hu, M.; Chan, D.A.; Ethier, S.P.; van ‘t Veer, L.J.; et al. Glutamine sensitivity analysis identifies the xCT antiporter as a common triple-negative breast tumor therapeutic target. Cancer Cell 2013, 24, 450–465. [Google Scholar] [CrossRef]
- Lanzardo, S.; Conti, L.; Rooke, R.; Ruiu, R.; Accart, N.; Bolli, E.; Arigoni, M.; Macagno, M.; Barrera, G.; Pizzimenti, S.; et al. Immunotargeting of Antigen xCT Attenuates Stem-like Cell Behavior and Metastatic Progression in Breast Cancer. Cancer Res. 2016, 76, 62–72. [Google Scholar] [CrossRef]
- Bolli, E.; O’Rourke, J.P.; Conti, L.; Lanzardo, S.; Rolih, V.; Christen, J.M.; Barutello, G.; Forni, M.; Pericle, F.; Cavallo, F. A Virus-Like-Particle immunotherapy targeting Epitope-Specific anti-xCT expressed on cancer stem cell inhibits the progression of metastatic cancer in vivo. Oncoimmunology 2017, 7, e1408746. [Google Scholar] [CrossRef]
- Wang, Z.; Jiang, Q.; Dong, C. Metabolic reprogramming in triple-negative breast cancer. Cancer Biol. Med. 2020, 17, 44–59. [Google Scholar] [CrossRef]
- Strekalova, E.; Malin, D.; Good, D.M.; Cryns, V.L. Methionine deprivation induces a targetable vulnerability in triple-negative breast cancer cells by enhancing TRAIL receptor-2 expression. Clin. Cancer Res. 2015, 21, 2780–2791. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.; Kim, J.H.; Lee, E.; Jang, Y.J.; Son, J.E.; Kwon, J.Y.; Lim, T.G.; Kim, S.; Park, J.H.; Kim, J.E.; et al. Methionine deprivation suppresses triple-negative breast cancer metastasis in vitro and in vivo. Oncotarget 2016, 7, 67223–67234. [Google Scholar] [CrossRef] [PubMed]
- Borrego, S.L.; Fahrmann, J.; Datta, R.; Stringari, C.; Grapov, D.; Zeller, M.; Chen, Y.; Wang, P.; Baldi, P.; Gratton, E.; et al. Metabolic changes associated with methionine stress sensitivity in MDA-MB-468 breast cancer cells. Cancer Metab. 2016, 4, 9. [Google Scholar] [CrossRef]
- Wang, Z.; Yip, L.Y.; Lee, J.H.J.; Wu, Z.; Chew, H.Y.; Chong, P.K.W.; Teo, C.C.; Ang, H.Y.; Peh, K.L.E.; Yuan, J.; et al. Methionine is a metabolic dependency of tumor-initiating cells. Nat. Med. 2019, 25, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shi, X.; Li, Y.; Fan, J.; Zeng, X.; Xian, Z.; Wang, Z.; Sun, Y.; Wang, S.; Song, P.; et al. Blocking autophagy enhanced cytotoxicity induced by recombinant human arginase in triple-negative breast cancer cells. Cell Death Dis. 2014, 5, e1563. [Google Scholar] [CrossRef] [PubMed]
- Hassabo, A.A.; Abdelraof, M.; Allam, R.M. L-arginase from Streptomyces diastaticus MAM5 as a potential therapeutic agent in breast cancer: Purification, characterization, G1 phase arrest and autophagy induction. Int. J. Biol. Macromol. 2023, 224, 634–645. [Google Scholar] [CrossRef]
- Wang, S.M.; Dowhan, D.H.; Muscat, G.E.O. Epigenetic arginine methylation in breast cancer: Emerging therapeutic strategies. J. Mol. Endocrinol. 2019, 62, R223–R237. [Google Scholar] [CrossRef]
- Oh, T.G.; Wang, S.M.; Muscat, G.E. Therapeutic implications of epigenetic signaling in breast cancer. Endocrinology 2017, 158, 431–447. [Google Scholar] [CrossRef]
- Jeon, Y.J.; Khelifa, S.; Ratnikov, B.; Scott, D.A.; Feng, Y.; Parisi, F.; Ruller, C.; Lau, E.; Kim, H.; Brill, L.M.; et al. Regulation of glutamine carrier proteins by RNF5 determines breast Cancer response to ER stress-inducing chemotherapies. Cancer Cell 2015, 27, 354–369. [Google Scholar] [CrossRef]
- Broer, A.; Rahimi, F.; Broer, S. Deletion of amino acid transporter ASCT2 (SLC1A5) reveals an essential role for transporters SNAT1 (SLC38A1) and SNAT2 (SLC38A2) to sustain Glutaminolysis in Cancer cells. J. Biol. Chem. 2016, 291, 13194–13205. [Google Scholar] [CrossRef]
- Dhankhar, R.; Gupta, V.; Kumar, S.; Kapoor, R.K.; Gulati, P. Microbial enzymes for deprivation of amino acid metabolism in malignant cells: Biological strategy for cancer treatment. Appl. Microbiol. Biotechnol. 2020, 104, 2857–2869. [Google Scholar] [CrossRef] [PubMed]
- Gwangwa, M.V.; Joubert, A.M.; Visagie, M.H. Effects of glutamine deprivation on oxidative stress and cell survival in breast cell lines. Biol. Res. 2019, 52, 15. [Google Scholar] [CrossRef] [PubMed]
- Bacci, M.; Lorito, N.; Ippolito, L.; Ramazzotti, M.; Luti, S.; Romagnoli, S.; Parri, M.; Bianchini, F.; Cappellesso, F.; Virga, F.; et al. Reprogramming of Amino Acid Transporters to Support Aspartate and Glutamate Dependency Sustains Endocrine Resistance in Breast Cancer. Cell Rep. 2019, 28, 104–118. [Google Scholar] [CrossRef] [PubMed]
- Maeng, H.J.; Kim, E.S.; Chough, C.; Joung, M.; Lim, J.W.; Shim, C.K.; Shim, W.S. Addition of amino acid moieties to lapatinib increases the anti-cancer effect via amino acid transporters. Biopharm. Drug Dispos. 2014, 35, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Mello-Andrade, F.; Guedes, A.P.M.; Pires, W.C.; Velozo-Sá, V.S.; Delmond, K.A.; Mendes, D.; Molina, M.S.; Matuda, L.; de Sousa, M.A.M.; Melo-Reis, P.; et al. Ru(II)/amino acid complexes inhibit the progression of breast cancer cells through multiple mechanism-induced apoptosis. J. Inorg. Biochem. 2022, 226, 111625. [Google Scholar] [CrossRef]
- Yoo, H.C.; Han, J.M. Amino acid metabolism in cancer drug resistance. Cells 2022, 11, 140. [Google Scholar] [CrossRef]
- Mitrevska, K.; Rodrigo, M.A.M.; Cernei, N.; Michalkova, H.; Splichal, Z.; Hynek, D.; Zitka, O.; Heger, Z.; Kopel, P.; Adam, V.; et al. Chick chorioallantoic membrane (CAM) assay for the evaluation of the antitumor and antimetastatic activity of platinum-based drugs in association with the impact on the amino acid metabolism. Mater. Today Bio 2023, 19, 100570. [Google Scholar] [CrossRef]
- Ji, Y.; Li, J.; Xiao, S.; Kwan, H.Y.; Bian, Z.; Chu, C.C. Optimization of amino acid-based poly(ester urea urethane) nanoparticles for the systemic delivery of gambogic acid for treating triple negative breast cancer. Biomater. Sci. 2023, 11, 4370–4384. [Google Scholar] [CrossRef]
- Dunstan, R.H.; Sparkes, D.L.; Macdonald, M.M.; Roberts, T.K.; Wratten, C.; Kumar, M.B.; Baines, S.; Denham, J.W.; Gallagher, S.A.; Rothkirch, T. Altered amino acid homeostasis and the development of fatigue by breast cancer radiotherapy patients: A pilot study. Clin. Biochem. 2011, 44, 208–215. [Google Scholar] [CrossRef]
- Poon, R.T.P.; Yu, W.C.; Fan, S.T.; Wong, J. Long-term oral branched chain amino acids in patients undergoing chemoembolization for hepatocellular carcinoma: A randomized trial. Aliment. Pharmacol. Ther. 2004, 19, 779–788. [Google Scholar] [CrossRef]
- Gramignano, G.; Lusso, M.R.; Madeddu, C.; Massa, E.; Serpe, R.; Deiana, L.; Lamonica, G.; Dessì, M.; Spiga, C.; Astara, G.; et al. Efficacy of L-carnitine administration on fatigue, nutritional status, oxidative stress, and related quality of life in 12 advanced cancer patients undergoing anticancer therapy. Nutrition 2006, 22, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lockwood, M.B.; Schlaeger, J.M.; Liu, T.; Danciu, O.C.; Doorenbos, A.Z. Tryptophan and Kynurenine Pathway Metabolites and Psychoneurological Symptoms Among Breast Cancer Survivors. Pain Manag. Nurs. 2023, 24, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Nees, J.; Schafferer, S.; Yuan, B.; Tang, Q.; Scheffler, M.; Hartkopf, A.; Golatta, M.; Schneeweiß, A.; Burwinkel, B.; Wallwiener, M. How previous treatment changes the metabolomic profile in patients with metastatic breast cancer. Arch. Gynecol. Obstet. 2022, 306, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Jung, W.H.; Koo, J.S. Diferential expression of enzymes associated with serine/glycine metabolism in diferent breast cancer subtypes. PLoS ONE 2014, 9, e101004. [Google Scholar]
- Prokhorova, E.; Zobel, F.; Smith, R.; Zentout, S.; Gibbs-Seymour, I.; Schützenhofer, K.; Peters, A.; Groslambert, J.; Zorzini, V.; Agnew, T.; et al. Serine-linked PARP1 auto-modification controls PARP inhibitor response. Nat. Commun. 2021, 12, 4055. [Google Scholar] [CrossRef] [PubMed]
- Possemato, R.; Marks, K.M.; Shaul, Y.D.; Pacold, M.E.; Kim, D.; Birsoy, K.; Sethumadhavan, S.; Woo, H.K.; Jang, H.G.; Jha, A.K.; et al. Functional genomics reveal that the serine synthesis pathway is essential in breast cancer. Nature 2011, 476, 346–350. [Google Scholar] [CrossRef]
Figure 1.
Fold change BC/control (data were averaged over [7,8,28,33,34,44,46,47,48,49,51,52,53,56,57,60]).


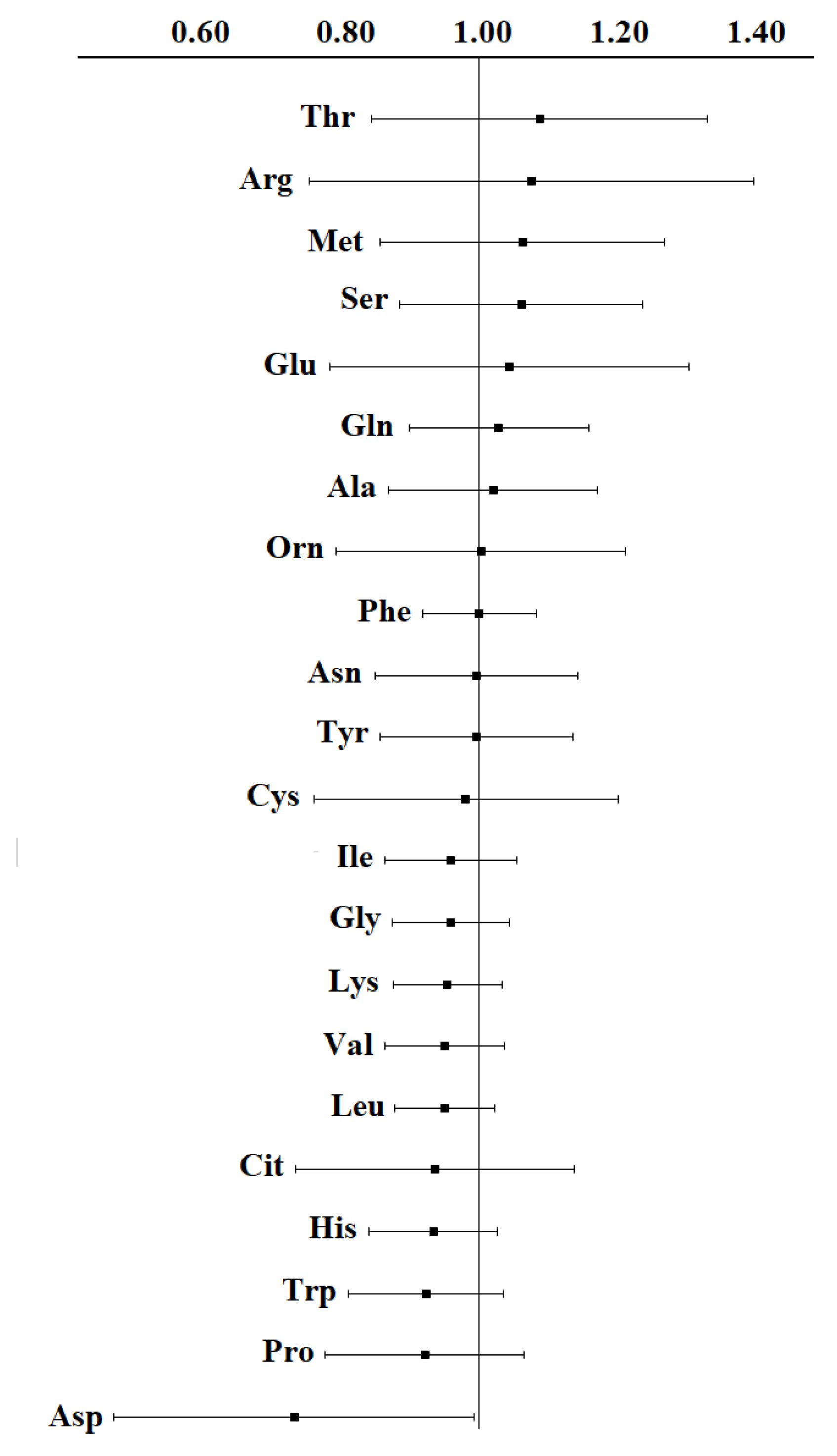{kind=link}
Table 1.
Basic studies of the amino acid composition of plasma/serum in breast cancer.
| No. | Author, Year | BC/Control | BC Stages | Method | Up-Regulated AAs | Down-Regulated AAs |
|---|---|---|---|---|---|---|
| 1 | Kubota A., 1992 [44] | 22/11 | St I + II—22 | AA analyzer | Ala, Arg, Thr | Cys, Gln |
| 2 | Cascino A., 1995 [45] | 33/28 | - | AA analyzer | Glu, Orn, Trp | - |
| 3 | Proenza A.M.A., 2003 [46] | 16/18 | St I—2, St II—5, St III—3, St IV—5, Unknown—1 | HPLC | Asn, Gln, Pro (Hydroxyproline) | Asp |
| 4 | Minet-Quinard R., 2004 [47] | 19/18 | T0—16%, T1—42%, T2—42% | AA analyzer | Ser, Glu, Orn | - |
| 5 | Vissers Y.L.J., 2005 [48] | 22/22 | St I—6, St II—7, St III—8 | HPLC | - | Arg |
| 6 | Okamoto N., 2009 [49] | 61/51 | St 0—8, St I—30, St II—18, St III–5 | HPLC–ESI–MS | Thr, Ser, Glu, Orn | Met, Ile, Phe, Arg |
| 7 | Miyagi Y., 2011 [34] | 196/976 | St II—95, St III—19, St IV—15, Unknown—5 | HPLC–ESI–MS | Thr, Pro, Ser, Gly, Ala, Orn | Gln, Trp, His, Phe, Tyr |
| 8 | Shen J., 2013 [8] | 60/60 | ER+/PR+—30, triple negative—30 African Americans and Caucasian Americans data sets | UPLC-MS/MS or GC-MS | - | Ala, His, Asp, Lys, Tyr, Trp, Met, Arg, Pro |
| 9 | Poschke I., 2013 [50] | 41/9 | - | HPLC | Glu, Ser, Gln, Ala, Val, Phe, Ile, Leu | - |
| 10 | Barnes T., 2014 [51] | 8/8 | St I + II—8 | HPLC | Ala, Asp, Gln, Lys, Met, Tyr | Arg, Gly, Pro, Ser, Ile, Val, Orn |
| 11 | Gu Y., 2015 [52] | 28/137 | St I—7, St II—18, St III—3 | AA analyzer | Thr, Arg | Asp, Gln, Gly, His |
| 12 | Jové M., 2017 [5] | 91/20 | St I—2, St IIA—40, St IIB—30, St IIIA—13, St IIIB—7 | ESI-Q-TOF MS/MS | - | Gln, Arg, Lys, Val |
| 13 | Wang X., 2018 [7] | 44/34 | - | UPLC-MS | Ala, Asp, Cys, Gly, Glu, Gln, His, Ile, Met, Pro, Phe, Ser, Tyr, Val | Arg |
| 14 | Jasbi P., 2018 [6] | 102/99 | St I—24, St II—42, St III—36 | UPLC-MS | Asp | Pro |
| 15 | Eniu D.T., 2018 [28] | 30/26 | St I—3, St II—17, St III—10 | HPLC-MS | - | Tyr, Arg, Ala, Ile, Trp, Leu |
| 16 | Cala M.P., 2018 [33] | 29/29 | St I—3, St II—15, St III—11 Colombian Hispanic data set | GC-MS | Val, Ala, Ile, Ser, Glu, 4-Hydroxyproline | - |
| 17 | Park J., 2019 [53] | 40/30 | St I—15, St II—15, St III—10 | HPLC-MS | 5-oxoproline, Phe, Ile + Leu | - |
| 18 | Li L., 2020 [54] | 105/35 | St I—65, St II—40 | NMR spectroscopy | Leu, Phe | Arg, Glu, Lys, Tyr, His |
| 19 | Politi C., 2021 [55] | 38/10 | - | GC-MS | Glu, Ile, Leu, Phe, Pro, Ser | Cys |
| 20 | An R., 2022 [56] | 75/20 | St I—31, St II—33, St III—11 | UPLC-MS | Gln, Arg | Glu, Asp, Cys |
| 21 | Baranovicova E., 2022 [57] | 50/46 | St I + II—50 | NMR spectroscopy | - | Leu, Ile, Val, Ala, His |
| 22 | Han X., 2022 [58] | 30/30 | ТНРМЖ | MALDI-TOF-MS | - | Ala, Ser, Pro, Val, Thr, His, Phe, Arg, Tyr, Trp |
| 23 | Santaliz-Casiano A., 2023 [59] | 103/150 | ER + breast cancer African American (AA) and non-Hispanic White (NHW) data sets | GC-MS | - | Arg (AA), His (AA), Met (AA) |
| 24 | Panigoro S.S., 2023 [60] | 29/28 | St I—13, St II—13, St III—3 | HPLC | Cys | Glu, His, Orn, Thr, Tyr, Val |
Note: HPLC—high performance liquid chromatography; GC-MS—gas chromatography coupled to a mass spectrometer; MALDI-TOF-MS—matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; HPLC-ESI-MS—high performance liquid chromatography–electrospray ionization-mass spectrometry; UPLC-MS—ultra-performance liquid chromatography coupled to a mass spectrometer; UPLC-QTOF-MS—ultra-performance liquid chromatography coupled with quadrupole/time-of-flight mass spectrometry; NMR—nuclear magnetic resonance spectroscopy.
Table 2.
Fold change BC/control according to different authors.
| Amino acid | Kubota, 1992 [44] | Proenza, 2003 [46] | Minet-Quinard, 2004 [47] | Vissers, 2005 [48] | Okamoto, 2009 [49] | Miyagi, 2011 [34] | Shen, 2013 [8] | Barnes, 2014 [51] | Gu, 2015 [52] | Wang, 2018 [7] | Eniu, 2018 [28] | Cala, 2018 [33] | Park, 2019 [53] | Baranovicova, 2022 [57] | An, 2022 [56] | Panigoro, 2023 [60] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ala | 1.96 | 0.93 | 1.11 | 0.94 | 1.06 | 1.08 | 0.82/0.80 * | 1.16 | 0.93 | 1.11 | 0.59 | 1.25 | 0.80 | 0.92 | 0.88 | |
| Arg | 1.33 | 0.86 | 0.84 | 0.98 | 0.90/0.86 | 0.91 | 1.78 | 0.81 | 0.32 | 2.35 | 0.99 | |||||
| Asn | 1.54 | 0.95 | 0.91 | 0.97 | 0.99 | 0.84/0.82 | 1.16 | 1.23 | 0.65 | 0.91 | ||||||
| Asp | 0.45 | 0.80 | 1.33 | 0.67 | 0.71 | 0.43 | ||||||||||
| Cys | 0.58 | 0.93/1.01 | 1.04 | 1.31 | 0.97 | 0.66 | 1.35 | |||||||||
| Gln | 0.73 | 1.16 | 1.05 | 0.92 | 1.00 | 0.97 | 0.94/1.00 | 1.08 | 1.53 | 0.77 | 1.21 | |||||
| Glu | 1.02 | 1.42 | 1.24 | 1.40 | 1.05/1.01 | 0.46 | 1.81 | 0.42 | 1.27 | 0.58 | 0.86 | |||||
| Gly | 0.94 | 1.01 | 1.08 | 1.12 | 0.90/0.91 | 0.91 | 0.90 | 1.16 | 0.68 | 0.94 | ||||||
| His | 1.08 | 1.04 | 1.17 | 1.04 | 0.95 | 0.97 | 0.88/0.91 | 0.87 | 1.20 | 0.61 | 0.99 | 0.63 | 0.93 | 0.75 | ||
| Ile | 0.94 | 1.00 | 0.93 | 0.85 | 1.02 | 0.93/0.94 | 0.72 | 0.93 | 1.11 | 0.55 | 1.21 | 1.32 | 0.82 | 1.12 | 0.96 | |
| Leu | 1.00 | 0.81 | 0.94 | 1.00 | 0.94/0.93 | 0.95 | 1.15 | 0.64 | 0.85 | 0.95 | 0.88 | |||||
| Lys | 1.04 | 1.07 | 1.02 | 0.99 | 1.03 | 0.91/0.86 | 1.19 | 0.92 | 0.98 | 0.62 | 0.94 | 0.84 | ||||
| Met | 1.01 | 1.04 | 0.87 | 0.93 | 0.99 | 0.88/0.87 | 1.08 | 1.05 | 2.02 | 0.67 | 1.36 | |||||
| Phe | 1.09 | 1.08 | 0.83 | 0.89 | 0.98 | 0.92/0.90 | 1.00 | 1.00 | 1.21 | 0.78 | 1.30 | 1.04 | ||||
| Pro | 1.07 | 0.85 | 0.97 | 1.12 | 0.85/0.87 | 0.95 | 0.51 | 1.19 | 0.59 | 1.17 | ||||||
| Ser | 1.01 | 1.13 | 1.11 | 1.10 | 1.04 | 0.92/0.89 | 0.86 | 0.98 | 1.14 | 0.79 | 2.10 | 0.87 | 0.93 | |||
| Thr | 1.48 | 1.01 | 0.94 | 0.92 | 1.07 | 1.08 | 0.89/0.94 | 2.46 | 1.00 | 0.63 | 1.08 | 0.93 | 0.82 | |||
| Trp | 0.82 | 0.93 | 0.94 | 0.94/0.88 | 1.02 | 0.61 | 1.15 | 1.02 | ||||||||
| Tyr | 0.98 | 1.09 | 0.89 | 0.92 | 0.96 | 0.92/0.80 | 1.55 | 1.07 | 1.20 | 0.56 | 1.24 | 0.78 | ||||
| Val | 0.93 | 1.02 | 0.79 | 1.01 | 1.01 | 0.95/0.94 | 0.90 | 0.93 | 1.15 | 0.68 | 1.36 | 0.85 | 0.96 | 0.79 | ||
| Cit | 1.23 | 0.97 | 0.90 | 1.01 | 0.47 | 1.04 | ||||||||||
| Orn | 1.28 | 1.07 | 1.47 | 0.65 | 1.25 | 1.12 | 0.98 | 0.53 | 0.68 |
Note: *—ER + PR+/TNBC.
Table 3.
Metabolites associated with breast cancer risk.
| No. | Author, Year | BC/Control | Subgroup | AAs | HR (95% CI) |
|---|---|---|---|---|---|
| 1 | Nagata C. et al., 2014 [88] | 350 | premenopausal | Arg, Leu, Tyr, Asp | - |
| 2 | Lécuyer L. et al., 2018 [89] | 206/396 | - | Val ↑ | 1.83 (1.15–2.92) |
| Gln ↑ | 1.61 (1.02–2.55) | ||||
| Lys + Creatine + Creatinine ↑ | 1.84 (1.19–2.85) | ||||
| Lys + Arg ↑ | 1.62 (1.05–2.48) | ||||
| 3 | His M. et al., 2019 [90] | 1624/1624 | - | Arg ↑ | 0.89 (0.80–0.99) |
| Asp ↑ | 0.87 (0.80–0.95) | ||||
| Gln ↑ | 0.91 (0.84–0.99) | ||||
| Gly ↑ | 0.90 (0.83–0.97) | ||||
| His ↑ | 0.91 (0.84–0.99) | ||||
| Lys ↑ | 0.90 (0.83–0.98) | ||||
| Thr ↑ | 0.92 (0.85–0.99) | ||||
| 4 | Zhang J. et al., 2020 [91] | 735/735 | - | Orn ↑ | 0.70 (0.53, 0.94) |
| 5 | Zeleznik O.A. et al., 2021 [87] | 1997/1997 | premenopausal | Ile ↑ | 0.86 (0.65–1.13) |
| postmenopausal | Ile ↑ | 1.63 (1.12–2.39) | |||
| 6 | Jobard E. et al., 2021 [92] | 791/791 | premenopausal | His ↑ | 1.70 (1.19–2.41) |
| Orn ↑ | 1.43 (1.06–1.95) | ||||
| Leu ↑ | 1.37 (1.01–1.86) | ||||
| Gln ↑ | 1.33 (1.00–1.78) | ||||
| Glu ↑ | 1.34 (1.00–1.79) | ||||
| 7 | Stevens V.L. et al., 2023 [93] | 1687/1983 | - | Ser ↓ | 0.89 (0.83–0.96) |
| Asp ↓ | 0.91 (0.84–0.97) | ||||
| Gln ↓ | 0.91 (0.85–0.98) |
Note: ↑—amino acid concentration in breast cancer increases; ↓—concentration decreases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bel’skaya, L.V.; Gundyrev, I.A.; Solomatin, D.V. The Role of Amino Acids in the Diagnosis, Risk Assessment, and Treatment of Breast Cancer: A Review. Curr. Issues Mol. Biol. 2023, 45, 7513-7537. https://doi.org/10.3390/cimb45090474
AMA Style
Bel’skaya LV, Gundyrev IA, Solomatin DV. The Role of Amino Acids in the Diagnosis, Risk Assessment, and Treatment of Breast Cancer: A Review. Current Issues in Molecular Biology. 2023; 45(9):7513-7537. https://doi.org/10.3390/cimb45090474
Chicago/Turabian StyleBel’skaya, Lyudmila V., Ivan A. Gundyrev, and Denis V. Solomatin. 2023. "The Role of Amino Acids in the Diagnosis, Risk Assessment, and Treatment of Breast Cancer: A Review" Current Issues in Molecular Biology 45, no. 9: 7513-7537. https://doi.org/10.3390/cimb45090474