
T-Cell Prolymphocytic Leukemia: Diagnosis, Pathogenesis, and Treatment
 , ,
, ,
Abstract
:1. Introduction
2. Clinical Presentation
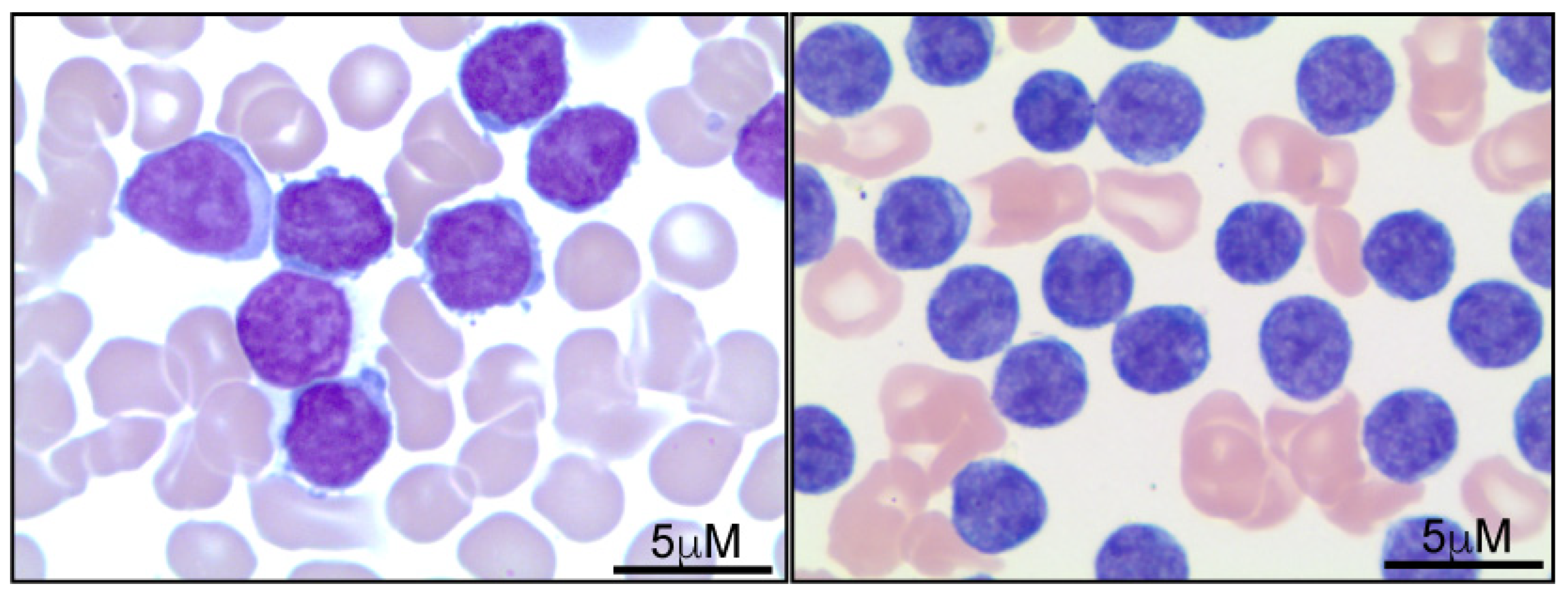
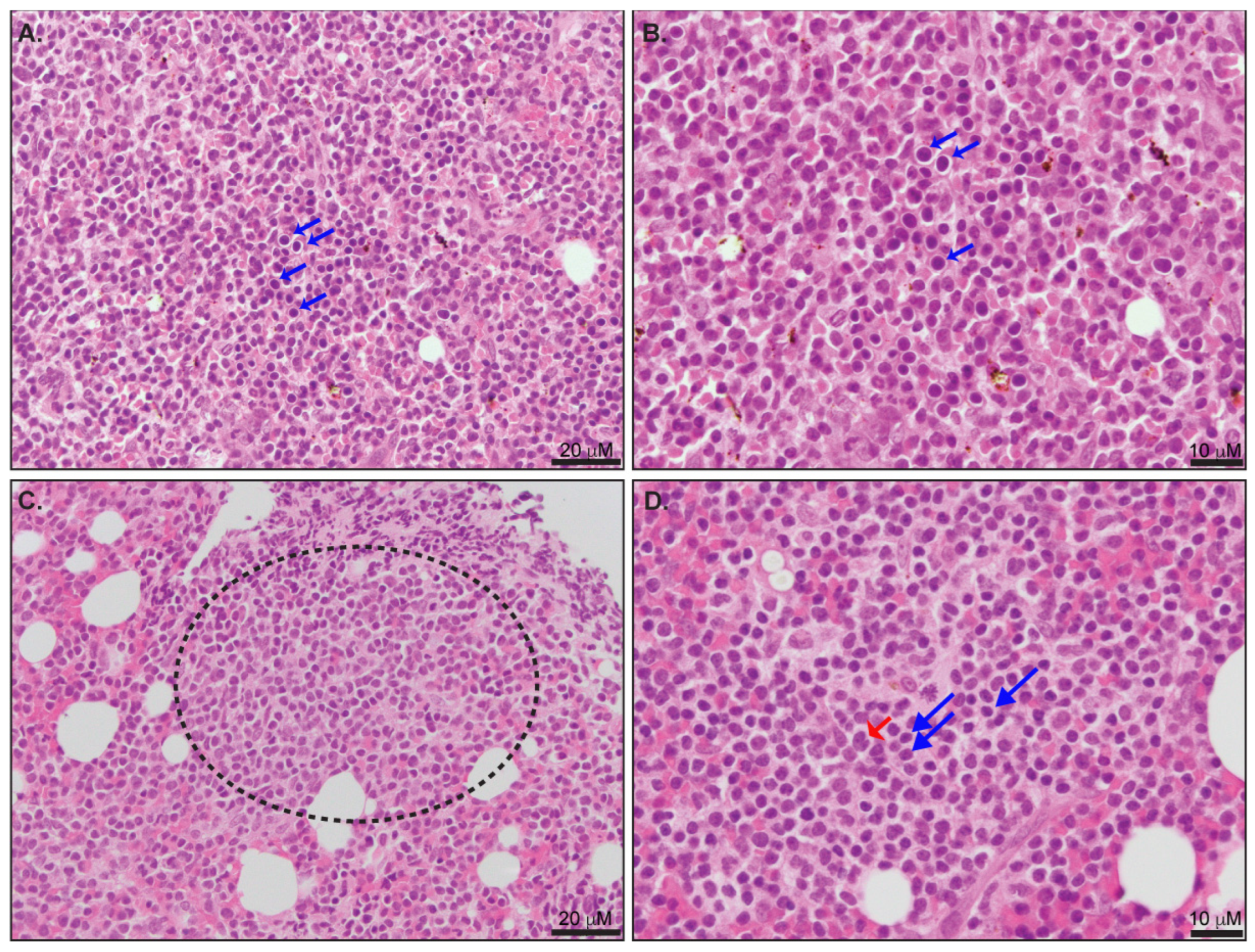
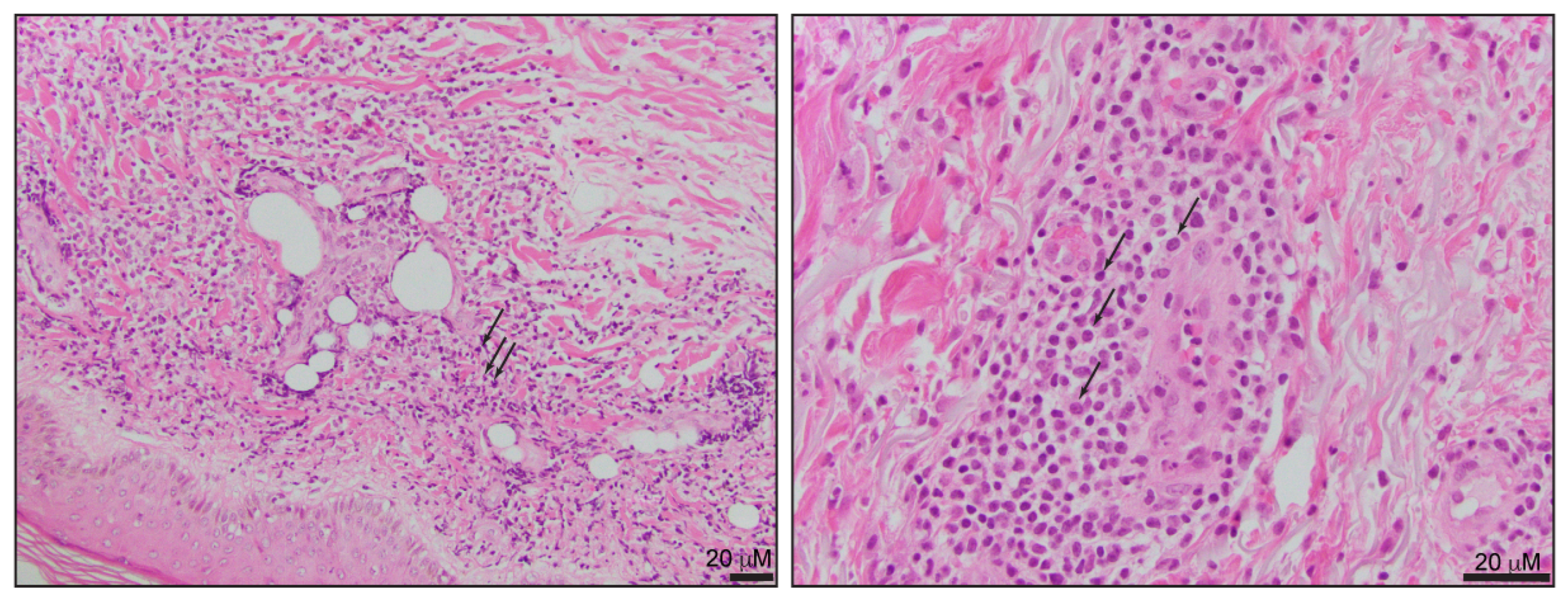
3. Diagnosis
4. Risk Stratification
5. Pathogenesis
6. Treatment
6.1. Conventional Cytotoxic Agents
6.2. Alemtuzumab
6.3. Stem Cell Transplantation
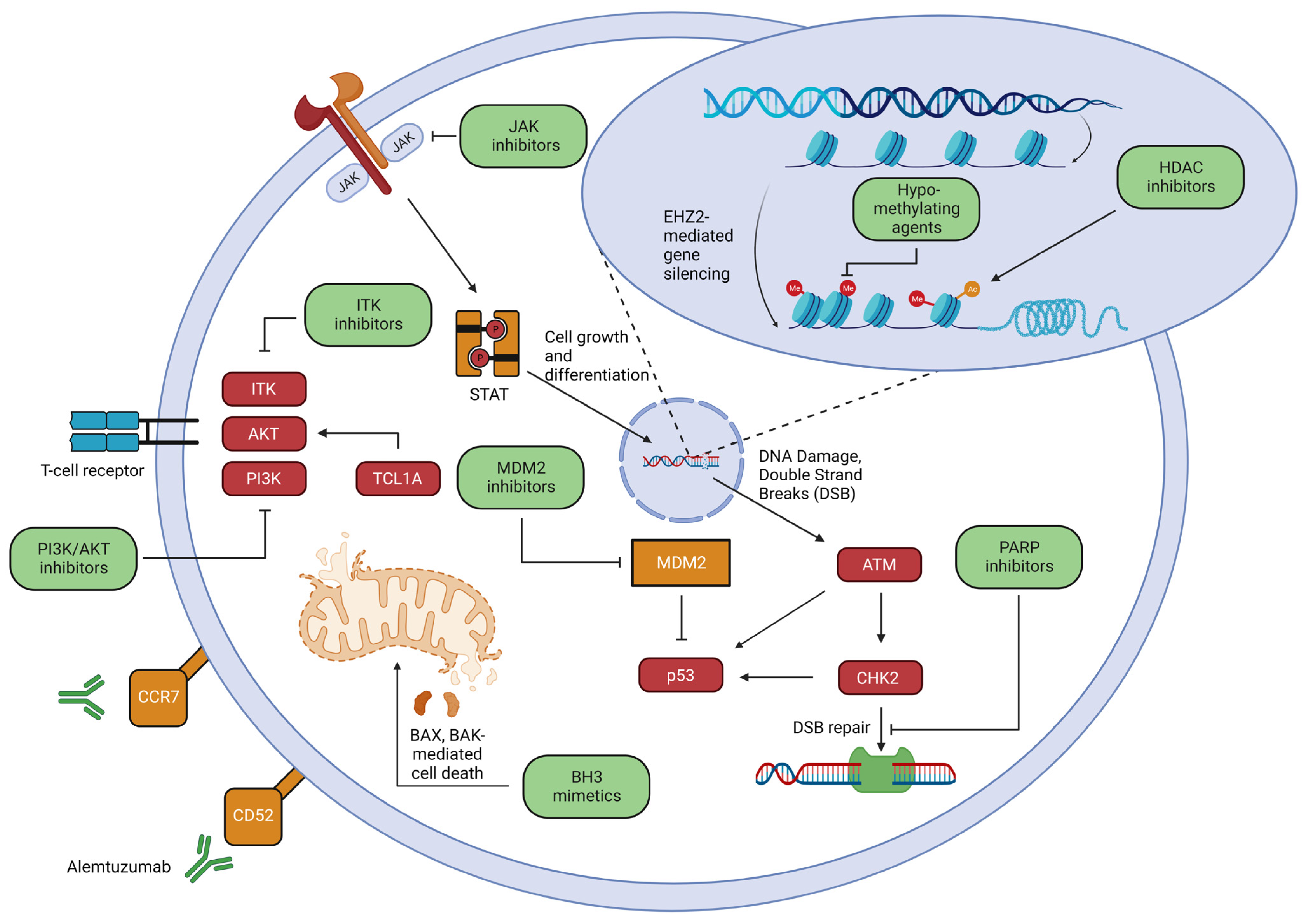
7. Novel Therapies and Future Therapeutic Strategies
7.1. MDM2 Inhibition
7.2. TCR Signaling
7.3. JAK/STAT Inhibition
7.4. BH3 Mimetics
7.5. Epigenetic Approaches
7.6. Monoclonal Antibodies: Moving beyond Alemtuzumab
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Catovsky, D.; Galetto, J.; Okos, A.; Galton, D.A.; Wiltshaw, E.; Stathopoulos, G. Prolymphocytic Leukaemia of B and T Cell Type. Lancet 1973, 2, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Herling, M.; Khoury, J.D.; Washington, L.T.; Duvic, M.; Keating, M.J.; Jones, D. A Systematic Approach to Diagnosis of Mature T-Cell Leukemias Reveals Heterogeneity among WHO Categories. Blood 2004, 104, 328–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staber, P.B.; Herling, M.; Bellido, M.; Jacobsen, E.D.; Davids, M.S.; Kadia, T.M.; Shustov, A.; Tournilhac, O.; Bachy, E.; Zaja, F.; et al. Consensus Criteria for Diagnosis, Staging, and Treatment Response Assessment of T-Cell Prolymphocytic Leukemia. Blood 2019, 134, 1132–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Lentzsch, S.; Gries, M.; Janz, M.; Bargou, R.; Dörken, B.; Mapara, M.Y. The International Consensus Classification of Mature Lymphoid Neoplasms: A Report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; de Oliveira Araujo, I.B.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th Edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Matutes, E.; Brito-Babapulle, V.; Swansbury, J.; Ellis, J.; Morilla, R.; Dearden, C.; Sempere, A.; Catovsky, D. Clinical and Laboratory Features of 78 Cases of T-Prolymphocytic Leukemia. Blood 1991, 78, 3269–3274. [Google Scholar] [CrossRef] [Green Version]
- Hoyer, J.D.; Ross, C.W.; Li, C.Y.; Witzig, T.E.; Gascoyne, R.D.; Dewald, G.W.; Hanson, C.A. True T-Cell Chronic Lymphocytic Leukemia: A Morphologic and Immunophenotypic Study of 25 Cases. Blood 1995, 86, 1163–1169. [Google Scholar] [CrossRef]
- Garand, R.; Goasguen, J.; Brizard, A.; Buisine, J.; Charpentier, A.; Claisse, J.F.; Duchayne, E.; Lagrange, M.; Segonds, C.; Troussard, X.; et al. Indolent Course as a Relatively Frequent Presentation in T-Prolymphocytic Leukaemia. Groupe Français d’Hématologie Cellulaire. Br. J. Haematol. 1998, 103, 488–494. [Google Scholar] [CrossRef]
- Jain, P.; Aoki, E.; Keating, M.; Wierda, W.G.; O’Brien, S.; Gonzalez, G.N.; Ferrajoli, A.; Jain, N.; Thompson, P.A.; Jabbour, E.; et al. Characteristics, Outcomes, Prognostic Factors and Treatment of Patients with T-Cell Prolymphocytic Leukemia (T-PLL). Ann. Oncol. 2017, 28, 1554–1559. [Google Scholar] [CrossRef]
- Suarez, F.; Mahlaoui, N.; Canioni, D.; Andriamanga, C.; Dubois d’Enghien, C.; Brousse, N.; Jais, J.-P.; Fischer, A.; Hermine, O.; Stoppa-Lyonnet, D. Incidence, Presentation, and Prognosis of Malignancies in Ataxia-Telangiectasia: A Report from the French National Registry of Primary Immune Deficiencies. J. Clin. Oncol. 2015, 33, 202–208. [Google Scholar] [CrossRef]
- Matutes, E.; Garcia Talavera, J.; O’Brien, M.; Catovsky, D. The Morphological Spectrum of T-Prolymphocytic Leukaemia. Br. J. Haematol. 1986, 64, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Jayakar, V.; Cheung, K.; Yebra-Fernandez, E.; Bain, B.J. The Distinctive Cytological Features of T-Cell Prolymphocytic Leukemia. Am. J. Hematol. 2017, 92, 830–832. [Google Scholar] [CrossRef]
- Ravandi, F.; O’Brien, S. Chronic Lymphoid Leukemias Other than Chronic Lymphocytic Leukemia: Diagnosis and Treatment. Mayo Clin. Proc. 2005, 80, 1660–1674. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; De Martinis, M.; Matutes, E.; Farahat, N.; Morilla, R.; Dyer, M.J.; Catovsky, D. Levels of Expression of CD52 in Normal and Leukemic B and T Cells: Correlation with in Vivo Therapeutic Responses to Campath-1H. Leuk. Res. 1998, 22, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, R.A. A Three-Signal Model of T-Cell Lymphoma Pathogenesis. Am. J. Hematol. 2016, 91, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanlari, M.; Ramos, J.C.; Sanchez, S.P.; Cho-Vega, J.H.; Amador, A.; Campuzano-Zuluaga, G.; Vega, F.; Chapman, J.R. Adult T-Cell Leukemia/Lymphoma Can Be Indistinguishable from Other More Common T-Cell Lymphomas. The University of Miami Experience with a Large Cohort of Cases. Mod. Pathol. 2018, 31, 1046–1063. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.-T.; Wang, D.; Luo, H.; Xiao, M.; Zhou, H.-S.; Liu, D.; Ling, S.-P.; Wang, N.; Hu, X.-L.; Luo, Y.; et al. Aggressive NK-Cell Leukemia: Clinical Subtypes, Molecular Features, and Treatment Outcomes. Blood Cancer J. 2017, 7, 660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virgilio, L.; Lazzeri, C.; Bichi, R.; Nibu, K.; Narducci, M.G.; Russo, G.; Rothstein, J.L.; Croce, C.M. Deregulated Expression of TCL1 Causes T Cell Leukemia in Mice. Proc. Natl. Acad. Sci. USA 1998, 95, 3885–3889. [Google Scholar] [CrossRef]
- Schrader, A.; Crispatzu, G.; Oberbeck, S.; Mayer, P.; Pützer, S.; von Jan, J.; Vasyutina, E.; Warner, K.; Weit, N.; Pflug, N.; et al. Actionable Perturbations of Damage Responses by TCL1/ATM and Epigenetic Lesions Form the Basis of T-PLL. Nat. Commun. 2018, 9, 697. [Google Scholar] [CrossRef] [Green Version]
- Lamy, T.; Moignet, A.; Loughran, T.P. LGL Leukemia: From Pathogenesis to Treatment. Blood 2017, 129, 1082–1094. [Google Scholar] [CrossRef] [Green Version]
- Jerez, A.; Clemente, M.J.; Makishima, H.; Koskela, H.; Leblanc, F.; Peng Ng, K.; Olson, T.; Przychodzen, B.; Afable, M.; Gomez-Segui, I.; et al. STAT3 Mutations Unify the Pathogenesis of Chronic Lymphoproliferative Disorders of NK Cells and T-Cell Large Granular Lymphocyte Leukemia. Blood 2012, 120, 3048–3057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohgami, R.S.; Ohgami, J.K.; Pereira, I.T.; Gitana, G.; Zehnder, J.L.; Arber, D.A. Refining the Diagnosis of T-Cell Large Granular Lymphocytic Leukemia by Combining Distinct Patterns of Antigen Expression with T-Cell Clonality Studies. Leukemia 2011, 25, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Iwanaga, M.; Yasunaga, J.-I.; Nagata, Y.; Kitanaka, A.; Kameda, T.; Yoshimitsu, M.; Shiraishi, Y.; Sato-Otsubo, A.; Sanada, M.; et al. Prognostic Relevance of Integrated Genetic Profiling in Adult T-Cell Leukemia/Lymphoma. Blood 2018, 131, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Kogure, Y.; Kameda, T.; Koya, J.; Yoshimitsu, M.; Nosaka, K.; Yasunaga, J.-I.; Imaizumi, Y.; Watanabe, M.; Saito, Y.; Ito, Y.; et al. Whole-Genome Landscape of Adult T-Cell Leukemia/Lymphoma. Blood 2022, 139, 967–982. [Google Scholar] [CrossRef]
- Korgavkar, K.; Xiong, M.; Weinstock, M. Changing Incidence Trends of Cutaneous T-Cell Lymphoma. JAMA Dermatol. 2013, 149, 1295–1299. [Google Scholar] [CrossRef] [Green Version]
- Pulitzer, M.P.; Horna, P.; Almeida, J. Sézary Syndrome and Mycosis Fungoides: An Overview, Including the Role of Immunophenotyping. Cytom. B Clin. Cytom. 2021, 100, 132–138. [Google Scholar] [CrossRef]
- Hristov, A.C.; Tejasvi, T.; Wilcox, R.A. Mycosis Fungoides and Sézary Syndrome: 2019 Update on Diagnosis, Risk-Stratification, and Management. Am. J. Hematol. 2019, 94, 1027–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Hussein, S.; Medeiros, L.J.; Khoury, J.D. Aggressive NK Cell Leukemia: Current State of the Art. Cancers 2020, 12, 2900. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Li, S.; Medeiros, L.J.; Sun, T. TCL-1-Positive Hematogones in a Patient with T-Cell Prolymphocytic Leukemia after Therapy. Hum. Pathol. 2017, 65, 175–179. [Google Scholar] [CrossRef]
- Hsi, A.C.; Robirds, D.H.; Luo, J.; Kreisel, F.H.; Frater, J.L.; Nguyen, T.T. T-Cell Prolymphocytic Leukemia Frequently Shows Cutaneous Involvement and Is Associated with Gains of MYC, Loss of ATM, and TCL1A Rearrangement. Am. J. Surg. Pathol. 2014, 38, 1468–1483. [Google Scholar] [CrossRef]
- Herling, M.; Valbuena, J.R.; Jones, D.; Medeiros, L.J. Skin Involvement in T-Cell Prolymphocytic Leukemia. J. Am. Acad. Dermatol. 2007, 57, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Valbuena, J.R.; Herling, M.; Admirand, J.H.; Padula, A.; Jones, D.; Medeiros, L.J. T-Cell Prolymphocytic Leukemia Involving Extramedullary Sites. Am. J. Clin. Pathol. 2005, 123, 456–464. [Google Scholar] [CrossRef]
- Nahmod, K.A.; Thakral, B.; Aakash, F.N.U.; Iyer, S.P.; Medeiros, L.J.; Quesada, A.E. From the Archives of MD Anderson Cancer Center: Aleukemic T-Prolymphocytic Leukemia, a Rare Presentation and Review of the Literature. Ann. Diagn. Pathol. 2023, 62, 152077. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, K.; Miyoshi, H.; Yanagida, E.; Yoshida, N.; Kiyasu, J.; Kozai, Y.; Morikita, T.; Kato, T.; Suzushima, H.; Tamura, S.; et al. Comparison of Clinicopathological Characteristics between T-Cell Prolymphocytic Leukemia and Peripheral T-Cell Lymphoma, Not Otherwise Specified. Eur. J. Haematol. 2017, 98, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Herling, M.; Patel, K.A.; Teitell, M.A.; Konopleva, M.; Ravandi, F.; Kobayashi, R.; Jones, D. High TCL1 Expression and Intact T-Cell Receptor Signaling Define a Hyperproliferative Subset of T-Cell Prolymphocytic Leukemia. Blood 2008, 111, 328–337. [Google Scholar] [CrossRef]
- Hu, Z.; Medeiros, L.J.; Fang, L.; Sun, Y.; Tang, Z.; Tang, G.; Sun, T.; Quesada, A.E.; Hu, S.; Wang, S.A.; et al. Prognostic Significance of Cytogenetic Abnormalities in T-Cell Prolymphocytic Leukemia. Am. J. Hematol. 2017, 92, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, P.; Cieslak, A.; Bernhart, S.H.; Toprak, U.H.; Wagener, R.; López, C.; Wiehle, L.; Bens, S.; Altmüller, J.; Franitza, M.; et al. Reconstruction of Rearranged T-Cell Receptor Loci by Whole Genome and Transcriptome Sequencing Gives Insights into the Initial Steps of T-Cell Prolymphocytic Leukemia. Genes Chromosomes Cancer 2020, 59, 261–267. [Google Scholar] [CrossRef]
- Stengel, A.; Kern, W.; Zenger, M.; Perglerová, K.; Schnittger, S.; Haferlach, T.; Haferlach, C. Genetic Characterization of T-PLL Reveals Two Major Biologic Subgroups and JAK3 Mutations as Prognostic Marker. Genes Chromosomes Cancer 2016, 55, 82–94. [Google Scholar] [CrossRef]
- Dürig, J.; Bug, S.; Klein-Hitpass, L.; Boes, T.; Jöns, T.; Martin-Subero, J.I.; Harder, L.; Baudis, M.; Dührsen, U.; Siebert, R. Combined Single Nucleotide Polymorphism-Based Genomic Mapping and Global Gene Expression Profiling Identifies Novel Chromosomal Imbalances, Mechanisms and Candidate Genes Important in the Pathogenesis of T-Cell Prolymphocytic Leukemia with Inv(14)(Q11q32). Leukemia 2007, 21, 2153–2163. [Google Scholar] [CrossRef] [Green Version]
- Mikhaylenko, N.; Wahnschaffe, L.; Herling, M.; Roeder, I.; Seifert, M. Computational Gene Expression Analysis Reveals Distinct Molecular Subgroups of T-Cell Prolymphocytic Leukemia. PLoS ONE 2022, 17, e0274463. [Google Scholar] [CrossRef]
- Oberbeck, S.; Schrader, A.; Warner, K.; Jungherz, D.; Crispatzu, G.; von Jan, J.; Chmielewski, M.; Ianevski, A.; Diebner, H.H.; Mayer, P.; et al. Noncanonical Effector Functions of the T-Memory-like T-PLL Cell Are Shaped by Cooperative TCL1A and TCR Signaling. Blood 2020, 136, 2786–2802. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; Stachelscheid, J.; Bley, N.; Oberbeck, S.; Otte, M.; Müller, T.A.; Wahnschaffe, L.; Glaß, M.; Ommer, K.; Franitza, M.; et al. Noncanonical Function of AGO2 Augments T-Cell Receptor Signaling in T-Cell Prolymphocytic Leukemia. Cancer Res. 2022, 82, 1818–1831. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Dong, S.; Strattan, E.; Ren, L.; Butchar, J.P.; Thornton, K.; Mishra, A.; Porcu, P.; Bradshaw, J.M.; Bisconte, A.; et al. Targeting Interleukin-2-Inducible T-Cell Kinase (ITK) and Resting Lymphocyte Kinase (RLK) Using a Novel Covalent Inhibitor PRN694. J. Biol. Chem. 2015, 290, 5960–5978. [Google Scholar] [CrossRef]
- Wang, T.; Lu, Y.; Polk, A.; Chowdhury, P.; Murga-Zamalloa, C.; Fujiwara, H.; Suemori, K.; Beyersdorf, N.; Hristov, A.C.; Lim, M.S.; et al. T-Cell Receptor Signaling Activates an ITK/NF-ΚB/GATA-3 Axis in T-Cell Lymphomas Facilitating Resistance to Chemotherapy. Clin. Cancer Res. 2017, 23, 2506–2515. [Google Scholar] [CrossRef] [Green Version]
- Geng, X.; Wang, C.; Gao, X.; Chowdhury, P.; Weiss, J.; Villegas, J.A.; Saed, B.; Perera, T.; Hu, Y.; Reneau, J.; et al. GATA-3 Is a Proto-Oncogene in T-Cell Lymphoproliferative Neoplasms. Blood Cancer J. 2022, 12, 149. [Google Scholar] [CrossRef] [PubMed]
- Wahnschaffe, L.; Braun, T.; Timonen, S.; Giri, A.K.; Schrader, A.; Wagle, P.; Almusa, H.; Johansson, P.; Bellanger, D.; López, C.; et al. JAK/STAT-Activating Genomic Alterations Are a Hallmark of T-PLL. Cancers 2019, 11, 1833. [Google Scholar] [CrossRef] [Green Version]
- Andersson, E.I.; Pützer, S.; Yadav, B.; Dufva, O.; Khan, S.; He, L.; Sellner, L.; Schrader, A.; Crispatzu, G.; Oleś, M.; et al. Discovery of Novel Drug Sensitivities in T-PLL by High-Throughput Ex Vivo Drug Testing and Mutation Profiling. Leukemia 2018, 32, 774–787. [Google Scholar] [CrossRef]
- Moskowitz, A.J.; Ghione, P.; Jacobsen, E.; Ruan, J.; Schatz, J.H.; Noor, S.; Myskowski, P.; Vardhana, S.; Ganesan, N.; Hancock, H.; et al. A Phase 2 Biomarker-Driven Study of Ruxolitinib Demonstrates Effectiveness of JAK/STAT Targeting in T-Cell Lymphomas. Blood 2021, 138, 2828–2837. [Google Scholar] [CrossRef]
- Dearden, C. How I Treat Prolymphocytic Leukemia. Blood 2012, 120, 538–551. [Google Scholar] [CrossRef] [Green Version]
- Dearden, C.E.; Khot, A.; Else, M.; Hamblin, M.; Grand, E.; Roy, A.; Hewamana, S.; Matutes, E.; Catovsky, D. Alemtuzumab Therapy in T-Cell Prolymphocytic Leukemia: Comparing Efficacy in a Series Treated Intravenously and a Study Piloting the Subcutaneous Route. Blood 2011, 118, 5799–5802. [Google Scholar] [CrossRef] [Green Version]
- Keating, M.J.; Cazin, B.; Coutré, S.; Birhiray, R.; Kovacsovics, T.; Langer, W.; Leber, B.; Maughan, T.; Rai, K.; Tjønnfjord, G.; et al. Campath-1H Treatment of T-Cell Prolymphocytic Leukemia in Patients for Whom at Least One Prior Chemotherapy Regimen Has Failed. J. Clin. Oncol. 2002, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Dearden, C.E.; Matutes, E.; Cazin, B.; Tjønnfjord, G.E.; Parreira, A.; Nomdedeu, B.; Leoni, P.; Clark, F.J.; Radia, D.; Rassam, S.M.; et al. High Remission Rate in T-Cell Prolymphocytic Leukemia with CAMPATH-1H. Blood 2001, 98, 1721–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbaux, C.; Genet, P.; Bouabdallah, K.; Pignon, J.-M.; Debarri, H.; Guidez, S.; Betrian, S.; Leleu, X.; Facon, T.; Morschhauser, F.; et al. Bendamustine Is Effective in T-Cell Prolymphocytic Leukaemia. Br. J. Haematol. 2015, 168, 916–919. [Google Scholar] [CrossRef] [PubMed]
- Ravandi, F.; Aribi, A.; O’Brien, S.; Faderl, S.; Jones, D.; Ferrajoli, A.; Huang, X.; York, S.; Pierce, S.; Wierda, W.; et al. Phase II Study of Alemtuzumab in Combination with Pentostatin in Patients with T-Cell Neoplasms. J. Clin. Oncol. 2009, 27, 5425–5430. [Google Scholar] [CrossRef] [Green Version]
- Hopfinger, G.; Busch, R.; Pflug, N.; Weit, N.; Westermann, A.; Fink, A.-M.; Cramer, P.; Reinart, N.; Winkler, D.; Fingerle-Rowson, G.; et al. Sequential Chemoimmunotherapy of Fludarabine, Mitoxantrone, and Cyclophosphamide Induction Followed by Alemtuzumab Consolidation Is Effective in T-Cell Prolymphocytic Leukemia. Cancer 2013, 119, 2258–2267. [Google Scholar] [CrossRef]
- Mercieca, J.; Matutes, E.; Dearden, C.; MacLennan, K.; Catovsky, D. The Role of Pentostatin in the Treatment of T-Cell Malignancies: Analysis of Response Rate in 145 Patients According to Disease Subtype. J. Clin. Oncol. 1994, 12, 2588–2593. [Google Scholar] [CrossRef]
- Johansson, P.; Klein-Hitpass, L.; Choidas, A.; Habenberger, P.; Mahboubi, B.; Kim, B.; Bergmann, A.; Scholtysik, R.; Brauser, M.; Lollies, A.; et al. SAMHD1 Is Recurrently Mutated in T-Cell Prolymphocytic Leukemia. Blood Cancer J. 2018, 8, 11. [Google Scholar] [CrossRef] [Green Version]
- Schneider, C.; Oellerich, T.; Baldauf, H.-M.; Schwarz, S.-M.; Thomas, D.; Flick, R.; Bohnenberger, H.; Kaderali, L.; Stegmann, L.; Cremer, A.; et al. SAMHD1 Is a Biomarker for Cytarabine Response and a Therapeutic Target in Acute Myeloid Leukemia. Nat. Med. 2017, 23, 250–255. [Google Scholar] [CrossRef]
- Pflug, N.; Cramer, P.; Robrecht, S.; Bahlo, J.; Westermann, A.; Fink, A.-M.; Schrader, A.; Mayer, P.; Oberbeck, S.; Seiler, T.; et al. New Lessons Learned in T-PLL: Results from a Prospective Phase-II Trial with Fludarabine-Mitoxantrone-Cyclophosphamide-Alemtuzumab Induction Followed by Alemtuzumab Maintenance. Leuk. Lymphoma 2019, 60, 649–657. [Google Scholar] [CrossRef]
- Martin, S.I.; Marty, F.M.; Fiumara, K.; Treon, S.P.; Gribben, J.G.; Baden, L.R. Infectious Complications Associated with Alemtuzumab Use for Lymphoproliferative Disorders. Clin. Infect. Dis. 2006, 43, 16–24. [Google Scholar] [CrossRef]
- Pawson, R.; Dyer, M.J.; Barge, R.; Matutes, E.; Thornton, P.D.; Emmett, E.; Kluin-Nelemans, J.C.; Fibbe, W.E.; Willemze, R.; Catovsky, D. Treatment of T-Cell Prolymphocytic Leukemia with Human CD52 Antibody. J. Clin. Oncol. 1997, 15, 2667–2672. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.; Klein-Hitpass, L.; Röth, A.; Möllmann, M.; Reinhardt, H.C.; Dührsen, U.; Dürig, J. Mutations in PIGA Cause a CD52-/GPI-Anchor-Deficient Phenotype Complicating Alemtuzumab Treatment in T-Cell Prolymphocytic Leukemia. Eur. J. Haematol. 2020, 105, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Tuset, E.; Matutes, E.; Brito-Babapulle, V.; Morilla, R.; Catovsky, D. Immunophenotype Changes and Loss of CD52 Expression in Two Patients with Relapsed T-Cell Prolymphocytic Leukaemia. Leuk. Lymphoma 2001, 42, 1379–1383. [Google Scholar] [CrossRef]
- Alsawah, F.; Benitez, L.; Choi, S.; Marini, B.; Perissinotti, A.; Skyles, A.; Burke, P.; Pettit, K.; Crouch, A.; Fox, H.; et al. Intrathecal Alemtuzumab: A Potential Treatment of Refractory Leptomeningeal T-Cell Prolymphocytic Leukemia. Blood Adv. 2019, 3, 3333–3336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varadarajan, I.; Ballen, K. Advances in Cellular Therapy for T-Cell Prolymphocytic Leukemia. Front. Oncol. 2022, 12, 781479. [Google Scholar] [CrossRef] [PubMed]
- Murthy, H.S.; Ahn, K.W.; Estrada-Merly, N.; Alkhateeb, H.B.; Bal, S.; Kharfan-Dabaja, M.A.; Dholaria, B.; Foss, F.; Gowda, L.; Jagadeesh, D.; et al. Outcomes of Allogeneic Hematopoietic Cell Transplantation in T Cell Prolymphocytic Leukemia: A Contemporary Analysis from the Center for International Blood and Marrow Transplant Research. Transplant. Cell. Ther. 2022, 28, 187.e1–187.e10. [Google Scholar] [CrossRef]
- Krishnan, B.; Else, M.; Tjonnfjord, G.E.; Cazin, B.; Carney, D.; Carter, J.; Ketterer, N.; Catovsky, D.; Ethell, M.; Matutes, E.; et al. Stem Cell Transplantation after Alemtuzumab in T-Cell Prolymphocytic Leukaemia Results in Longer Survival than after Alemtuzumab Alone: A Multicentre Retrospective Study. Br. J. Haematol. 2010, 149, 907–910. [Google Scholar] [CrossRef]
- Wiktor-Jedrzejczak, W.; Drozd-Sokolowska, J.; Eikema, D.J.; Hoek, J.; Potter, M.; Wulf, G.; Sellner, L.; Ljungman, P.; Chevallier, P.; Volin, L.; et al. EBMT Prospective Observational Study on Allogeneic Hematopoietic Stem Cell Transplantation in T-Prolymphocytic Leukemia (T-PLL). Bone Marrow Transplant. 2019, 54, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, T.; Beguin, Y.; Tabrizi, R.; Nguyen, S.; Blaise, D.; Deconinck, E.; Redjoul, R.; Cornillon, J.; Guillerm, G.; Contentin, N.; et al. Allogeneic Hematopoietic Stem Cell Transplantation for T-Prolymphocytic Leukemia: A Report from the French Society for Stem Cell Transplantation (SFGM-TC). Eur. J. Haematol. 2015, 94, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Dholaria, B.R.; Ayala, E.; Sokol, L.; Nishihori, T.; Chavez, J.C.; Hussaini, M.; Kumar, A.; Kharfan-Dabaja, M.A. Allogeneic Hematopoietic Cell Transplantation in T-Cell Prolymphocytic Leukemia: A Single-Center Experience. Leuk. Res. 2018, 67, 1–5. [Google Scholar] [CrossRef]
- Yamasaki, S.; Nitta, H.; Kondo, E.; Uchida, N.; Miyazaki, T.; Ishiyama, K.; Kiyota, M.; Matsuoka, H.; Ichinohe, T.; Fukuda, T.; et al. Effect of Allogeneic Hematopoietic Cell Transplantation for Patients with T-Prolymphocytic Leukemia: A Retrospective Study from the Adult Lymphoma Working Group of the Japan Society for Hematopoietic Cell Transplantation. Ann. Hematol. 2019, 98, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; Dechow, A.; Friedrich, G.; Seifert, M.; Stachelscheid, J.; Herling, M. Advanced Pathogenetic Concepts in T-Cell Prolymphocytic Leukemia and Their Translational Impact. Front. Oncol. 2021, 11, 775363. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; von Jan, J.; Wahnschaffe, L.; Herling, M. Advances and Perspectives in the Treatment of T-PLL. Curr. Hematol. Malig. Rep. 2020, 15, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Arteaga, A.; Margolskee, E.; Wei, M.T.; van Besien, K.; Inghirami, G.; Horwitz, S. Combined Use of Tofacitinib (Pan-JAK Inhibitor) and Ruxolitinib (a JAK1/2 Inhibitor) for Refractory T-Cell Prolymphocytic Leukemia (T-PLL) with a JAK3 Mutation. Leuk. Lymphoma 2019, 60, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Weston, V.J.; Oldreive, C.E.; Skowronska, A.; Oscier, D.G.; Pratt, G.; Dyer, M.J.S.; Smith, G.; Powell, J.E.; Rudzki, Z.; Kearns, P.; et al. The PARP Inhibitor Olaparib Induces Significant Killing of ATM-Deficient Lymphoid Tumor Cells in Vitro and in Vivo. Blood 2010, 116, 4578–4587. [Google Scholar] [CrossRef] [Green Version]
- Boidol, B.; Kornauth, C.; van der Kouwe, E.; Prutsch, N.; Kazianka, L.; Gültekin, S.; Hoermann, G.; Mayerhoefer, M.E.; Hopfinger, G.; Hauswirth, A.; et al. First-in-Human Response of BCL-2 Inhibitor Venetoclax in T-Cell Prolymphocytic Leukemia. Blood 2017, 130, 2499–2503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornauth, C.; Herbaux, C.; Boidol, B.; Guillemette, C.; Caron, P.; Mayerhöfer, M.E.; Poulain, S.; Tournilhac, O.; Pemovska, T.; Chong, S.J.F.; et al. Rationale for the Combination of Venetoclax and Ibrutinib in T-Prolymphocytic Leukemia. Haematologica 2021, 106, 2251–2256. [Google Scholar] [CrossRef]
- Herbaux, C.; Kornauth, C.; Poulain, S.; Chong, S.J.F.; Collins, M.C.; Valentin, R.; Hackett, L.; Tournilhac, O.; Lemonnier, F.; Dupuis, J.; et al. BH3 Profiling Identifies Ruxolitinib as a Promising Partner for Venetoclax to Treat T-Cell Prolymphocytic Leukemia. Blood 2021, 137, 3495–3506. [Google Scholar] [CrossRef]
- Herbaux, C.; Poulain, S.; Roos-Weil, D.; Bay, J.-O.; Guillermin, Y.; Lemonnier, F.; Laribi, K.; Visanica, S.; Moreaux, J.; Gonzalez, H.; et al. Preliminary Study of Ruxolitinib and Venetoclax for Treatment of Patients with T-Cell Prolymphocytic Leukemia Refractory to, or Ineligible for Alemtuzumab. Blood 2021, 138, 1201. [Google Scholar] [CrossRef]
- Hampel, P.J.; Parikh, S.A.; Call, T.G.; Shah, M.V.; Bennani, N.N.; Al-Kali, A.; Rabe, K.G.; Wang, Y.; Muchtar, E.; Leis, J.F.; et al. Venetoclax Treatment of Patients with Relapsed T-Cell Prolymphocytic Leukemia. Blood Cancer J. 2021, 11, 47. [Google Scholar] [CrossRef]
- Hasanali, Z.S.; Saroya, B.S.; Stuart, A.; Shimko, S.; Evans, J.; Vinod Shah, M.; Sharma, K.; Leshchenko, V.V.; Parekh, S.; Loughran, T.P.; et al. Epigenetic Therapy Overcomes Treatment Resistance in T Cell Prolymphocytic Leukemia. Sci. Transl. Med. 2015, 7, 293ra102. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.Y.; Yoshida, N.; Christie, A.L.; Ghandi, M.; Dharia, N.V.; Dempster, J.; Murakami, M.; Shigemori, K.; Morrow, S.N.; Van Scoyk, A.; et al. Targetable Vulnerabilities in T- and NK-Cell Lymphomas Identified through Preclinical Models. Nat. Commun. 2018, 9, 2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratt, G.; Yap, C.; Oldreive, C.; Slade, D.; Bishop, R.; Griffiths, M.; Dyer, M.J.S.; Fegan, C.; Oscier, D.; Pettitt, A.; et al. A Multi-Centre Phase I Trial of the PARP Inhibitor Olaparib in Patients with Relapsed Chronic Lymphocytic Leukaemia, T-Prolymphocytic Leukaemia or Mantle Cell Lymphoma. Br. J. Haematol. 2018, 182, 429–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreotti, A.H.; Schwartzberg, P.L.; Joseph, R.E.; Berg, L.J. T-Cell Signaling Regulated by the Tec Family Kinase, Itk. Cold Spring Harb Perspect. Biol. 2010, 2, a002287. [Google Scholar] [CrossRef] [Green Version]
- Waldmann, T.A. JAK/STAT Pathway Directed Therapy of T-Cell Leukemia/Lymphoma: Inspired by Functional and Structural Genomics. Mol. Cell. Endocrinol. 2017, 451, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Rajala, H.L.M.; Eldfors, S.; Kuusanmäki, H.; van Adrichem, A.J.; Olson, T.; Lagström, S.; Andersson, E.I.; Jerez, A.; Clemente, M.J.; Yan, Y.; et al. Discovery of Somatic STAT5b Mutations in Large Granular Lymphocytic Leukemia. Blood 2013, 121, 4541–4550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, F.; Davis, M.C.; McColl, K.S.; Distelhorst, C.W. Bcl-2 Differentially Regulates Ca2+ Signals According to the Strength of T Cell Receptor Activation. J. Cell Biol. 2006, 172, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Vardhana, S.; Moskowitz, A.J.; Porcu, P.; Dogan, A.; Dubovsky, J.A.; Matasar, M.J.; Zhang, Z.; Younes, A.; Horwitz, S.M. Pilot Trial of Ibrutinib in Patients with Relapsed or Refractory T-Cell Lymphoma. Blood Adv. 2018, 2, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Anshabo, A.T.; Milne, R.; Wang, S.; Albrecht, H. CDK9: A Comprehensive Review of Its Biology, and Its Role as a Potential Target for Anti-Cancer Agents. Front. Oncol. 2021, 11, 678559. [Google Scholar] [CrossRef]
- Bacon, C.W.; D’Orso, I. CDK9: A Signaling Hub for Transcriptional Control. Transcription 2019, 10, 57–75. [Google Scholar] [CrossRef] [Green Version]
- Johansson, P.; Dierichs, L.; Klein-Hitpass, L.; Bergmann, A.K.; Möllmann, M.; Menninger, S.; Habenberger, P.; Klebl, B.; Siveke, J.T.; Dührsen, U.; et al. Anti-Leukemic Effect of CDK9 Inhibition in T-Cell Prolymphocytic Leukemia. Ther. Adv. Hematol. 2020, 11, 2040620720933761. [Google Scholar] [CrossRef] [PubMed]
- Cidado, J.; Boiko, S.; Proia, T.; Ferguson, D.; Criscione, S.W.; San Martin, M.; Pop-Damkov, P.; Su, N.; Roamio Franklin, V.N.; Sekhar Reddy Chilamakuri, C.; et al. AZD4573 Is a Highly Selective CDK9 Inhibitor That Suppresses MCL-1 and Induces Apoptosis in Hematologic Cancer Cells. Clin. Cancer Res. 2020, 26, 922–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.-H.; Lujambio, A.; Zuber, J.; Tschaharganeh, D.F.; Doran, M.G.; Evans, M.J.; Kitzing, T.; Zhu, N.; de Stanchina, E.; Sawyers, C.L.; et al. CDK9-Mediated Transcription Elongation Is Required for MYC Addiction in Hepatocellular Carcinoma. Genes Dev. 2014, 28, 1800–1814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Y.; Zhao, W.; Chen, Y.; Zhao, Y.; Gu, W. Acetylation Is Indispensable for P53 Activation. Cell 2008, 133, 612–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toutah, K.; Nawar, N.; Timonen, S.; Sorger, H.; Raouf, Y.S.; Bukhari, S.; von Jan, J.; Ianevski, A.; Gawel, J.M.; Olaoye, O.O.; et al. Development of HDAC Inhibitors Exhibiting Therapeutic Potential in T-Cell Prolymphocytic Leukemia. J. Med. Chem. 2021, 64, 8486–8509. [Google Scholar] [CrossRef]
- Kiel, M.J.; Velusamy, T.; Rolland, D.; Sahasrabuddhe, A.A.; Chung, F.; Bailey, N.G.; Schrader, A.; Li, B.; Li, J.Z.; Ozel, A.B.; et al. Integrated Genomic Sequencing Reveals Mutational Landscape of T-Cell Prolymphocytic Leukemia. Blood 2014, 124, 1460–1472. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Li, B.; Lin, B.; Lee, P.T.; Chung, T.-H.; Tan, J.; Bi, C.; Lee, X.T.; Selvarajan, V.; Ng, S.-B.; et al. EZH2 Phosphorylation by JAK3 Mediates a Switch to Noncanonical Function in Natural Killer/T-Cell Lymphoma. Blood 2016, 128, 948–958. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Mateos, C.; Fuentes, P.; Schrader, A.; Juárez-Sánchez, R.; Loscertales, J.; Mateu-Albero, T.; Vega-Piris, L.; Espartero-Santos, M.; Marcos-Jimenez, A.; Sánchez-López, B.A.; et al. CCR7 as a Novel Therapeutic Target in T-Cell PROLYMPHOCYTIC Leukemia. Biomark. Res. 2020, 8, 54. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T-PLL [6,7,11,18,19] | T-LGL [20,21,22] | ATLL [16,23,24] | NK-Cell LGL [21] | Sézary Syndrome [25,26,27] | Aggressive NK-Cell Leukemia [17,28] | |
|---|---|---|---|---|---|---|
| Epidemiology | The incidence in Western countries is 2 per 1,000,000 people per year. T-PLL accounts for about 2% of mature leukemias. | Accounts for 2% to 5% of chronic lymphoproliferative disorders. The overall incidence is 0.72 per 1,000,000 people per year. | More common in parts of the world that are endemic for HTLV-1, including Japan, the Caribbean, and Central and South America. The global estimation of new cases is approximately 3000 per year. | Accounts for less than 5% of LGL disorders, is predominantly observed in Asia, and tends to affect individuals of younger age. | The annual incidence rate of SS is 1 per 10 million per year. SS represents 3% of all cutaneous lymphomas. | A very rare disease, predominantly in Asia. Median age 37 years (range 10–78). More frequent in males than females (male-to-female ratio: 1.3:1). |
| White Blood Cell Count (WBC) | Most patients present with extreme lymphoctosis (≥100,000/µL). | 1.6–49.1 × 109/L (median count 5.5 × 109/L) | Acute type: 3.9–296 × 109/L (median count 88 × 109/L). Chronic type: 10.4–17 × 109/L (median count 17 × 109/L). Lymphomatous type: 1.1–45.3 × 109/L (median count 7.5 × 109/L). | Similar WBCs as in T-LGL. Blood LGL count of >700/μL. | The median white blood cell count is 21 × 109/L. The Sézary cell count is ≥1000 cells/μL. | WBC count in aggressive NK-cell leukemia varies widely and can be high, with a median count of 2.80 × 109/L (range, 0.29–57 × 109/L). |
| Histology | Three morphologic variants have been recognized (see Section 3). | Neoplastic cells cannot be differentiated cytologically from normal reactive cytotoxic lymphocytes. | In the acute type, neoplastic cells feature hyperchromatic nuclear chromatin and deeply lobulated nuclear contours: “flower cells”. In the chronic type, the neoplastic cells show subtle cytological atypia. | The histological features of NK-cell LGL are indistinguishable from those of T-LGL. | Atypical lymphocytes with cerebriform nuclei that are larger than normal lymphocytes and have hyperchromatic nuclei. These features are not specific, as similar morphological features can be observed in reactive lymphocytes in autoimmune disorders. | Neoplastic cells are medium to large, with moderate amounts of basophilic agranular cytoplasm, highly irregular nuclear contours, and a distinct open chromatin pattern with visible nucleoli. |
| Phenotype | Usually CD3+. CD4+ and CD8− is most common, however co-expression of CD4 and CD8 is also observed. | CD3+, CD16+, CD27−, CD28−, CD45R0−, CD45RA+, and CD57+. Ta/b > Tg/d. CD8+ > CD4+. CD94 is positive in 20% of CD8+ and in 2% of CD4+ cases. | Preserved expression of pan-T-cell markers (CD2, CD3, CD4, CD5) with strong expression of CD25 and FoxP3, and frequent loss of CD7. | Characterized by CD2+, sCD3−, CD3e+, TCRa/b−, CD4−, CD8+, CD16+, and CD56+. Expression of CD94 is detected in more than 95% of the cases. KIR expression is detected in 53% of cases. | Usually CD3+, CD4+ and CD8−. The aberrant loss of pan-T-cell antigens, including CD2, CD3, CD4, CD5, CD7, and/or CD26 is frequently seen. | Characterized by the expression of CD2, cytoplasmic CD3, CD7, CD16, and CD56, while the expression of surface CD3 is negative. Expression of CD94 is detected in more than 95% of cases. |
| Molecular features | TCL1A overexpression, combined with loss of ATM appears unique to T-PLL (see Section 5). | Activating mutations in genes such as STAT3-STAT5b, and NFKB are common. | Most cases exhibit intricate cytogenetic abnormalities that result from the detrimental impact of the viral-encoded TAX. Recurrent loss-of-function mutations in CIC/ATXN1 complex are detected in up to 50% of cases. | Mutations in STAT3 are observed in less than 10% of the cases, and STAT5b mutations are not detected. | Commonly altered genes in Sézary syndrome include ZEB1, STAT5B, FAS, ARID1A, CDKN2A, and TP53. | Activating mutations in JAK-STAT pathway genes, particularly STAT3 and STAT5B are detected. Mutations in tumor suppressor genes, such as TP53 are frequent. |
| Clinical features | Generally presents with extreme lymphocytosis, anemia and thrombocytopenia in the 6th to 7th decade of life. | At the time of diagnosis, approximately one-third of patients are asymptomatic. The initial presentation is typically associated with cytopenias (anemia or neutropenia). | Caused by HTLV-1 infection. The acute and chronic types usually present with leukemia, hepatosplenomegaly, and hypercalcemia. The lymphomatous type does not exhibit leukocytosis or hepatosplenomegaly. | Characterized by a chronic and indolent clinical course, that is similar to T-LGL. The 10-year survival rate is around 70%. | Characterized by erythroderma with severe pruritus and generalized lymphadenopathy. | Patients typically present with fever, hepatosplenomegaly, hemophagocytic lymphohistiocytosis and hyperferritinemia. |
| Major Criteria |
|---|
| 1. >5 × 109/L cells of T-PLL phenotype in peripheral blood or bone marrow |
| 2. T-cell clonality (by polymerase chain reaction for T-cell receptor beta or gamma, or by flow cytometry) 3. Abnormalities of 14q32 or expression of TCL1A/B or MTCP1 |
| Minor Criteria |
| 1. Abnormalities of chromosome 11 (11q22.3, ATM) |
| 2. Abnormalities of chromosome 8 [idic(8)(p11), t(8;8), or trisomy 8(q)] chromosome 5, 12, 13, or 22 |
| 3. Complex karyotype |
| 4. Involvement of T-PLL specific site (e.g., splenomegaly or pleural effusions) |
| References | Regimen | Disease Status | n | ORR | CR | Median PFS (Months) | Median OS (Months) |
|---|---|---|---|---|---|---|---|
| [9,50,51,52] | IV alemtuzumab ** | Frontline | 80 | 85 | 71 | 11 | 15 |
| Salvage | 183 | 57 | 50 | 5 | 11.3 | ||
| [50] | Subcutaneous alemtuzumab | Frontline | 9 | 33 | 33 | - | - |
| [53] | Bendamustine | Frontline | 6 | 67 | 33 | 2 | 7 |
| Salvage | 9 | 44 | 11 | 0 | 3 | ||
| [9,54] | IV alemtuzumab and pentostatin ** | Frontline | 13 | 82 | 73 | 4.3 | 10.4 |
| Salvage | 18 | 70 | 59 | 5.2 | 6.4 | ||
| [55] | IV alemtuzumab and FMC | Frontline | 16 | 92 | 48 | 11.5 | 17.1 |
| Salvage | 9 | ||||||
| [56] | Pentostatin | Salvage | 55 | 45 | 9 | 6 | 9 |
| Reference | n | CR (%) at allo-HSCT | PR (%) at allo-HSCT | OS | Relapse Rate |
|---|---|---|---|---|---|
| [68] | 37 | 60% | 27% | 4-year OS: 42% | 38% at 4 years |
| [69] | 27 | 51% | 37% | 3-year OS: 36% | 47% at 3 years |
| [70] | 11 | 81% | 9% | 4-year OS: 56% | 21% at 4 years |
| [71] | 20 | 30% | 5% | 3-year OS: 39.8% | 69.6% at 3 years |
| [66] | 266 | 56% | 30% | 4-year OS: 30% | 41.9% at 4 years |
| Reference | Regimen | Disease Status | Study Type | n | Result |
|---|---|---|---|---|---|
| [74] | Tofacitinib and ruxolitinib | Salvage | Case Report | 1 | Patient had 10 months of partial response followed by eventual progression |
| [75] | Olaparib | Salvage | Phase I clinical trial | 2 | Patient A: treated for 133 days w/disease progression. Patient B withdrew after 14 days given dose limiting toxicity |
| [76] | Venetoclax | Salvage | Case Report | 2 | Patient A: partial response however died with fulminant sepsis 18 days after treatment initiation. Patient B: partial response, at 131 days on venetoclax, disease relapse |
| [77] | Venetoclax and ibrutinib | Salvage | Case Report | 2 | Patient A: treated for 40 days. Course was complicated by influenza A infection and patient transitioned to comfort care. Patient B: treated for 80 days; however, patient died of bacterial pneumonia. |
| [78] | Venetoclax and ruxolitinib | Salvage | Case Report | 2 | Patient A: 10 months of partial response. Patient B: progression on day 127 following therapy, then lost to follow-up. |
| [78] | Venetoclax and romidepsin | Salvage | Case Report | 1 | Partial response ongoing, 9 months, at time of publication of case. |
| [79] | Venetoclax and ruxolitinib | Salvage (n = 14) Frontline (n = 1) | Multicenter retrospective study | 15 | ORR 73% (all were partial response), median PFS 1.8 months in wild-type JAK/STAT vs. 5.6 months in mutated JAK/STAT pathway ‡ |
| [80] | Venetoclax; 5 patients received bendamustine | Salvage | Single-center retrospective study | 9 | Disease control rate 56% (best response was PR in 4 and stable disease in 1) |
| [81] | Alemtuzumab and cladribine, some received vorinostat, romidepsin, and brentuximab | Salvage (n = 6) Frontline (n = 2) | Single-center prospective study | 8 | ORR 100% (88% CR, 12% PR), median OS 25.7 months, 38% were alive at time of publication. |
| NCT03873493 | Venetoclax and Ibrutinib | Salvage | Phase II Clinical Trial | 14 | ORR 7.1%, median PFS 2.7 months |
| NCT01186640 | FMC-subcutaneous alemtuzumab induction followed by alemtuzumab | Salvage (n = 4) Frontline (n = 12) | Phase II Clinical Trial | 16 | ORR 68.8% (31.3% CR, 37.5% PR), median OS 16.7 months, median PFS 11.2 months |
| NCT04496349 | APG-115 (MDM2 inhibitor) +/− APG-2575 (Bcl-2 inhibitor) | Salvage | Phase II Clinical Trial | 36 † | Recruiting; estimated study completion date: 31 May 2024 |
| NCT03989466 | Alemtuzumab and Itacitinib (JAK1 inhibitor) | Frontline or salvage | Phase I Clinical Trial | 15 † | Recruiting; estimated study completion date: 21 December 2023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutierrez, M.; Bladek, P.; Goksu, B.; Murga-Zamalloa, C.; Bixby, D.; Wilcox, R. T-Cell Prolymphocytic Leukemia: Diagnosis, Pathogenesis, and Treatment. Int. J. Mol. Sci. 2023, 24, 12106. https://doi.org/10.3390/ijms241512106
Gutierrez M, Bladek P, Goksu B, Murga-Zamalloa C, Bixby D, Wilcox R. T-Cell Prolymphocytic Leukemia: Diagnosis, Pathogenesis, and Treatment. International Journal of Molecular Sciences. 2023; 24(15):12106. https://doi.org/10.3390/ijms241512106
Chicago/Turabian StyleGutierrez, Marc, Patrick Bladek, Busra Goksu, Carlos Murga-Zamalloa, Dale Bixby, and Ryan Wilcox. 2023. "T-Cell Prolymphocytic Leukemia: Diagnosis, Pathogenesis, and Treatment" International Journal of Molecular Sciences 24, no. 15: 12106. https://doi.org/10.3390/ijms241512106