Background
The history of hip resurfacing arthroplasties (HRA) exhibits an impeccable marriage between engineering and surgery. This article aims to review the key moments of historical importance in the development of today’s HRAs as well as showcasing HRA designs currently being developed and trialled. By identifying the challenges faced over the last few decades, specific solutions can be sought which will translate into improved implant performance, patient related outcome measures (PROMs) and revision rates.
Aims
Lessons learnt over the last century have shaped modern resurfacing implants currently in use and inspired the development of new HRAs. The objective of this article is to review the most significant moments in the history of HRA surgery and their relevance to current implants. We review key outcomes from joint registry studies and how this influences patient selection.
Methods
A scoping review of the literature was completed using a defined search strategy to identify key articles relevant to the history of hip resurfacing. The following online databases were accessed to identify articles: PubMed, Google Scholar, and MEDLINE. Additionally, Clinicaltrials.gov and the ISRCTN registry, were searched to identify ongoing clinical trials.
Exclusion criteria included letters, commentaries and studies identified as being poorly designed and of a low level of evidence (levels 4 and 5). Articles published from January 1920 to March 2023, in the English language, were included. Selected articles were then critically appraised by the authors and their references were screened for any additional articles which met the stated criteria.
1920s: Ivory and Glass HRA
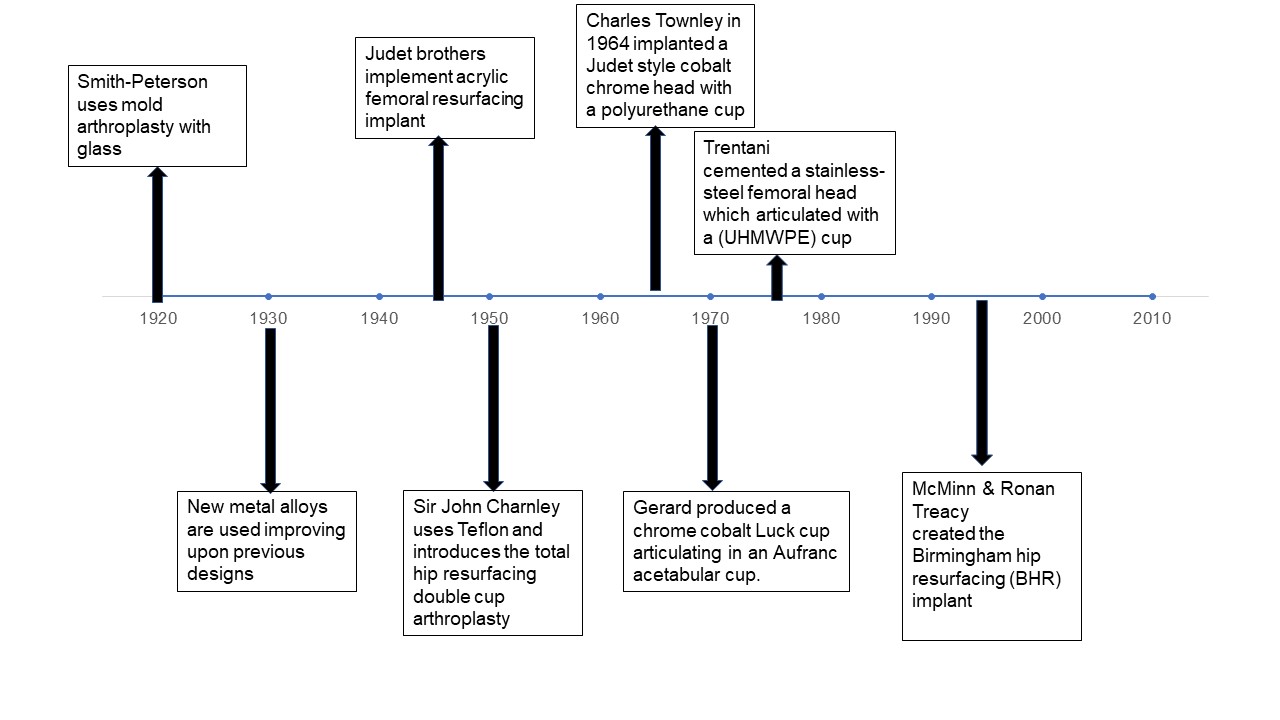
In 1926, Hey Grove delivered the Bradshaw lecture entitled “Contribution to Hip Reconstructive Surgery” at the Royal College of Surgeons.1 In his lecture, he introduced the world to an ivory hip resurfacing arthroplasty and his vision of a pegged implant. In the same period, Smith-Peterson devised the mold arthroplasty of the hip, manufactured from glass. The original design was a ball-shaped, hollow hemisphere of glass that could fit over the femoral head of the hip joint. The objective was to stimulate cartilage regeneration on both sides of the glass joint. Smith-Peterson intended to remove the glass after the restoration of the cartilage. Although glass was biocompatible and provided a smooth surface for motion, it could not withstand physiological weight-bearing stress and failed predictably. Over the years, Smith-Peterson continued to use different types of glass with improved material properties to overcome its shortcomings.1,2
1930s-40s: Cup and Double Cup Arthroplasties
During the 1930s several breakthroughs in metallurgy resulted in the development of new alloys. This led to attempts to incorporate these innovations into new prostheses. During this period, the Mold arthroplasty was considered one of the most popular prostheses with Sir John Charnley implanting it, however outcomes in terms of gait, material performance and implant survival were unpredictable and poor.2–8
Building upon this work, the Judet brothers introduced an acrylic femoral resurfacing implant in 1946. This design would become a trademark design for subsequent generations of femoral components due to its characteristic stem. Although the Judet hip yielded favourable early results, it led to a significant osteolytic reaction, acetabular erosion, and implant failure.9
The first to introduce the total hip resurfacing double cup arthroplasty was Sir John Charnley, using Teflon (polytetrafluoroethylene) as the primary material. Due to its low coefficient of friction, Charnley believed this could be likened to a ‘synthetic articular cartilage’ however this failed catastrophically due to the Teflon wear debris and ultimately, this acted as the catalyst for the development of the highly successful Charnley low friction total hip arthroplasty (THA) over the coming decades.10–12
1960s: Metal on Metal Resurfacing Arthroplasty
Endeavouring to improve on the early failures, Charles Townley in 1964 implanted a Judet style cobalt chrome head with a polyurethane cup. Early failures of the cup were secondary to significant osteolysis and so this was substituted for polyethylene. Unfortunately, this still demonstrated a high failure rate and was considered inferior to Charnley’s low friction THA which was setting the standard in hip surgery.12,13
Following this, Muller and Boltzy developed their own metal-on-metal HRA. The design involved a cobalt chrome head which articulated with pads on the interior aspect of a cup. Although this method provided good early results, they altered their original design to a metal on polyethene prostheses in 1968 however a 50% early reoperation rate led them to reconsider their decision.14–16
Gerard, in 1970, produced a paired cup arthroplasty consisting of cobalt chrome for the femoral head and acetabulum. This design used a Luck cup articulating in an Aufranc acetabular cup. The primary objective of this design was to maximise the range of motion within the metal components with the acetabular component remaining unfixed to the acetabulum and free to move. A polyethylene cup was introduced as a bearing for the acetabular cup in 1972 however this technique was largely abandoned by 1975 due to reports accelerated wear and osteolysis.17,18
These early attempts at resurfacing had high failure rates secondary to the use of unproven materials, poorly designed implants, and inadequate fixation strategies and surgical techniques. The next generation of implants focused on using improved materials and enhanced fixation strategies to improve survivorship.
1970s-80s: Learning from the past
In 1971 Trentani et al instigated what is often regarded as the next chapter in the history of HRA. He cemented a stainless-steel femoral head which articulated with an acetabular ultra-high molecular weight polyethylene (UHMWPE) cup. The implant itself was considered a landmark in the history of hip resurfacing and consisted of a femoral component with a polished stainless steel two third spherical shape with a 4 mm long load-bearing skirt. This was designed to reduce the risk of femoral neck fracture which was a major cause for revision along with loosening by enhancing physiological stress transfer/loading of the medial calcar. The design included coarse concentric grooves on the inner surface of the component to enhance cement fixation. Additionally, Trentani et al were meticulous in their description of their surgical technique and the importance of avoiding damaged to the femoral neck.
Ultimately, he reported a 12% failure rate at 6 years in his series of 70 patients. This was a significant improvement compared to previous reported outcomes for HRAs and emphasised the importance of implant design and surgical technique.19 Attempts to replicate these outcomes were made in Japan with Furuya et al, however a significant revision rate of 58% was reported and attributed to a higher degree of acetabular dysplasia in the Japanese cohort of patients.20
Freeman, in 1972, developed the Imperial College London Hospital (ICLH) hip resurfacing implant in the biomechanics laboratory. It consisted of a high-density polyethene femoral head coupled with a cobalt chrome acetabular cup.21 In 1974 he altered the design to accommodate for a cobalt chrome femoral head and high-density polyethene cup. These implants showed a 21% failure rate, primarily due to aseptic loosening at follow-up of up to 6 years.21
Other notable contributions in this period came from Harlan Amstutz, who developed the total hip articular replacement using eccentric internal shells (THARIES). This implant was the first to require the chamfered cylinder-shaped cuts to the femoral head; now the standard femoral preparation method in modern resurfacing implants.. Although Amstutz reported a high revision rate of 59% at ten years primarily due to aseptic loosening, he noted that males with larger femoral head sizes had the best implant survivorship which was comparable to generationally matched THAs.22,23 Amstutz reported that he considered loosening in his series to be due to poor fixation with cement and so developed press-fit components in the 1980s. These showed similar rates of loosening and it was not until the pathophysiology of aseptic loosening was better understood, could this be improved.22,24
Upon reviewing the outcomes of the key studies during this period it is clear that the combination of a hard on soft bearing couple with a large bearing surface caused high frictional torque, increased volumetric wear and osteolysis which was a major factor in the loosening of these prostheses. At this point, HRA was being largely abandoned in favour of the low friction THA and research was being focussed to refining the THA. (Figure 1)

1990s: Resurrection of HRA
Overall, hip resurfacing was unfavoured by clinicians until the 1990s, when key individuals resurrected its use. These include Derek McMinn, Wagner and Amstutz. During this period, a greater understanding of polyethene wear debris was spreading throughout the orthopaedic community.16,25 In parallel to this, there was an appreciation for the reported success of some of the first metal-on-metal articulations (e.g. the Muller and McKee-Farrar prostheses). Bernhard Weber was the first to develop a metal-on-metal THA; the Metasul bearing system which became widely used throughout Europe.26–30 Wagner introduced a high carbon cobalt chrome Molybdenum bearing with a press-fit design achieved through a grit-blasted titanium coating at the bone implant interfaces.29 Despite the increasing enthusiasm, early outcomes were unsatisfactory, with 5/35 (14.3%) patients requiring revision of the Metasul HRA for loosening in 4 patients and a single patient suffering a femoral neck fracture. for one patient at a mean follow-up of 20 months. Within this initial cohort, a significant proportion of patients were female patients with a history of dysplasia which may have contributed to their early failure.29
Concurrently, McMinn was developing a metal-on-metal resurfacing hip. The implant design consisted of a press-fit cobalt chrome femoral component and a press-fit acetabular shell with a central peg and anti-rotation fins. Unfortunately, at 54 months follow-up, there was an 8.6% revision rate, with long term survival at 16 years of 63.6%.31 McMinn modified the design by incorporating hydroxyapatite (HA) at the implant bone interface; despite this, the 15-year data only demonstrated 66.7% survival.31,32 Subsequently, further modifications to the design were made which involved cement fixation of both components. Similarly, these demonstrated poor revision rates and led to the trial of a hybrid configuration. The final evolution comprised of a cemented femoral component with an uncemented acetabulum coated with HA in addition to incorporating splines to enhance stability. The change proved to be a success, with 10-year survival at 96%.32,33 Unfortunately, the manufacturer altered the heated treatment process during manufacture of the implant which resulted in significant implant failure.32 This led to McMinn collaborating with Ronan Treacy to create the Birmingham hip resurfacing (BHR) implant. Thereafter, a 92% survivorship at ten years was reported in multiple studies and joint registries, which ushered in the modern era of hip resurfacing.33–38
2000s – Modern Day: Clinical Outcome Data
The turn of the millennium saw Amstutz further develop his HRA in the United States. The Conserve Plus had a 10-year survival of 88.5%.39 Following these successes and evolutions of HRAs, a number of manufacturers entered the market and produced their own HRAs (e.g. the ASR by Depuy and the Durom prosthesis by Zimmer). Unfortunately, enthusiasm for HRAs once again diminished due to registry data showing the ASR 10-year revision rate approached 45%.40–42 This led to the recall of the ASR and attention to be directed towards the aetiological reasons for the poor implant survivorship. It became clear that subtle design differences varying from the established BHR resulted in significantly different clinical outcomes. The ASR had a sub-hemispheric shape with a 151-degree arc compared to the successful BHRs’ arc of 162 degrees. There was also a smaller radial clearance between the femoral head and cup which led to limited lubrication in the ASR, seizing of the cup and allowed for the articular contact patch to move to the rim of the cup.43,44 This led to edge loading, significant wear, and metal ion release. This affect was exaggerated in smaller sized components (allowing the wear patch to reach the rim even if implanted at less than 45 degrees of inclination) and those with an acetabular inclination angle of >55 degrees.38,42–44 Following this, most manufacturers withdrew their HRAs. However, the more established BHR and Conserve Plus remain on the market and have subsequently had large, single surgeon series 10-year outcomes reported. Matharu et al reported a 96.3% survival in a cohort of 447 BHRs at 10 years and Girard et al reported a 98.7% 10 year survival in 962 Conserve Plus HRAs.45,46
How does hip resurfacing compare to total hip arthroplasty?
There is significant debate in the orthopaedic community regarding the optimal surgical strategy when treating young patients with end-stage hip degeneration. A number of studies suggest that both HRA and THA can yield comparable outcomes in terms of pain resolution, return to sport, and restoration of physiological hip biomechanics.47–49
A recent study by LeBrun et al compared the patient reported outcome measures (PROMs) and revision rates of these procedures in 101 patients aged 35 or younger.50 Of these patients, 76 underwent HRA and 33 underwent a primary THA. Within five years, 9% (n=3) of patients in the THA group required revision due to complications such as instability (n=1), squeaking (n=1) or ceramic liner fracture (n=1), whereas no patients in the HRA group were revised.50 Both HRA and THA resulted in significant improvements in PROMs, including the University of California, Los Angeles Activity (UCLAA) score (74% increase in both groups), modified Harris Hip score (HHS) (64% increase in HRA vs. 66% increase in THA), and Hip Dysfunction and Osteoarthritis Outcome Scores for Joint Replacement (49% increase in both groups).50 Despite lower preoperative and postoperative PROMs in the THA group, the absolute improvements in these measures did not differ significantly between the two groups. The researchers concluded that both HRA and THA can be suitable surgical options for young patients.47,50
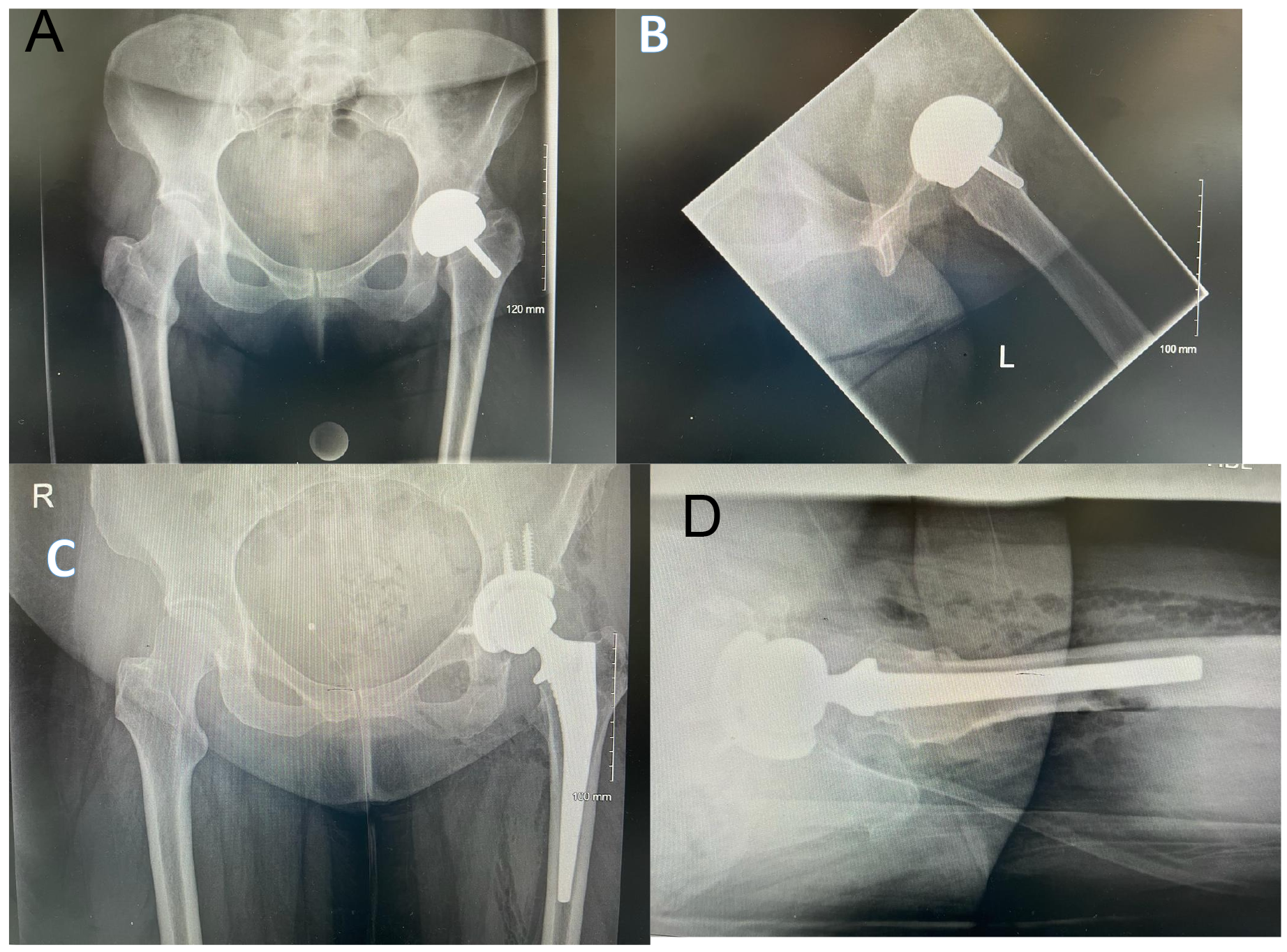
Other authors have drawn similar conclusions. Rueckl et al conducted a prospective case control study to investigate the return to sport and function after HRA (n = 40) and THA (n = 40).47 Patients were matched based on age, body mass index (BMI) and pre-operative University of California Arthroplasty Score (UCLA). A telephone questionnaire was completed assessing general health and sports activities in THA patients (n=40) and HRA patients (n=40) matched based on pre-operative University of California Arthroplasty Score (UCLA), body mass index (BMI). The mean follow-up period was 56 months (range 24-87 months).47 The results indicated that the HRA group had significantly higher scores in the High-activity arthroplasty score (HAAS) (14.9 vs. 12.9, p<0.001), Lower extremity activity scale (LEAS) (15.9 vs. 14.1, p<0.001), the Hip cycle score (HCS) (44.7 vs. 35.7, p=0.037) and the Impact score (IS) (40.9 vs. 29.6, p<0.002) versus the THA group. Despite this, no significant differences were identified in the hip disability and osteoarthritis outcome score (HOOS) and the Pain numeric rating scale.47 The authors of this study concluded that HRA allowed for young male patients to achieve higher activity levels after HRA compared to a primary THA.47,50,51 This may be further supported by gait analysis studies which report a more physiological gait compared to THAs.52 However, Costa et al in Oxford completed a randomized control trial to compare hip function and quality of life over a 5 year period in young patients randomised to undergo a primary THA or HRA.53 At 12 months postoperatively the mean Oxford Hip Score (OHS) was 40.4 (95% confidence interval 37.9 to 42.9) in the HRA group and 38.2 (35.3 to 41.0) in the THA group.53 The mean HHS score was 88.4 (84.4 to 92.4) in the resurfacing group and 82.3 (77.2 to 87.5) in the total arthroplasty group.53 These results indicated no statistical difference in functional outcomes (Oxford hip scores and Harris Hip scores) between the two procedures at 12 months.47,50,51,53 Additionally 78% of the participants provided mid-term data at 5 years post-operatively and confirmed that these original results persisted.54 It is reasonable to consider that these studies do not demonstrate inferiority of the HRA to the THA which is of value when considering treatment options with patients. (Figure 2)

Van Der Straeten and the International Hip Resurfacing Group analysed 11,382 HRAs from 13 countries. They reported implant survivorship, reasons for revision, clinical scores and metal ion levels for patients with metal on metal implants.51 At 22 years, the cumulative Kaplan-Meier survivorship rate in patients younger than 50 years was 88.9% (95% Confidence Interval (CI): 88.3–89.5%) in 11,382 HRAs. Notably, men had a higher implant survivorship rate of 99% at 10 years and 92.5% at 21 years, while women had lower rates at 90% and 81.3%, respectively.51 The most common reasons for revision were implant loosening and adverse local tissue reactions and the overall revision rate was 3.6%. Patients with osteoarthritis had the highest survivorship rates (95% CI, 92.1–93.3% at 22 years), while dysplastic hips had the poorest (78.3%; 95% CI, 76.5–80.1% at 20 years, p<0.001).51 Additionally, the authors noted that HRA implant survivorship compared favourably to THA in under 50 years old at 10 years (96% in males undergoing an HRA versus 89% in males undergoing a THA as reported by the Swedish joint registry).This implies that one should consider HRA when counselling young active patients.50,51,55
Who is the ideal patient?
The ideal patient cohort that would benefit most from this prosthesis has not been fully defined however a number of poor prognostic variables have helped inform patient selection. The available data from the Australian NJR reported that males under 55 years of age have greater implant survivorship than females with a revision rate under 6.5% versus 19.1%. The reasons for this remain debated in the literature however it has been suggested that reduced femoral head sizes and factors such as decreased bone mineral density occurring more commonly in the female population could be responsible.40,41 These findings are echoed by the international hip resurfacing group who reported a 99% and 92.5% implant survivorship at 10 and 21 years postoperatively. Female patients had a 10 year implant survivorship of 90% and 81.3% implant survivorship at 21 years.51
Patients with a femoral head size under 44 millimetres (mm) had a 13.8% revision rate. This revision rate decreased as femoral head sizes increased (head sizes of 50-54mm reported a revision rate at seven years of 3.7%, head sizes > 55mm reported a revision rate of 2.2%).41,42 There are multiple possible reasons for this however, older designed HRAs consisted of a femoral peg with constant dimensions. Therefore, if implanting this into smaller-sized femoral necks the peg could account for a greater proportion of the native femoral neck-to-implant construct volume and any remaining bone in the neck would potentially suffer from stress shielding increasing the risk of a fracture occurring.37,39,42
The quality of the bone bed has a significant impact on patient selection. This is best demonstrated in the series by Matharu et al of 447 hips at a mean follow-up of 10 years.45 The revision rate in patients with rheumatoid arthritis and those with avascular necrosis was 9.5% and 7.5% respectively. The lowest revision rate occurred in patients with primary osteoarthritis (3%).45 Therefore, it is vital to consider the quality of the bone bed prior to considering an HRA.
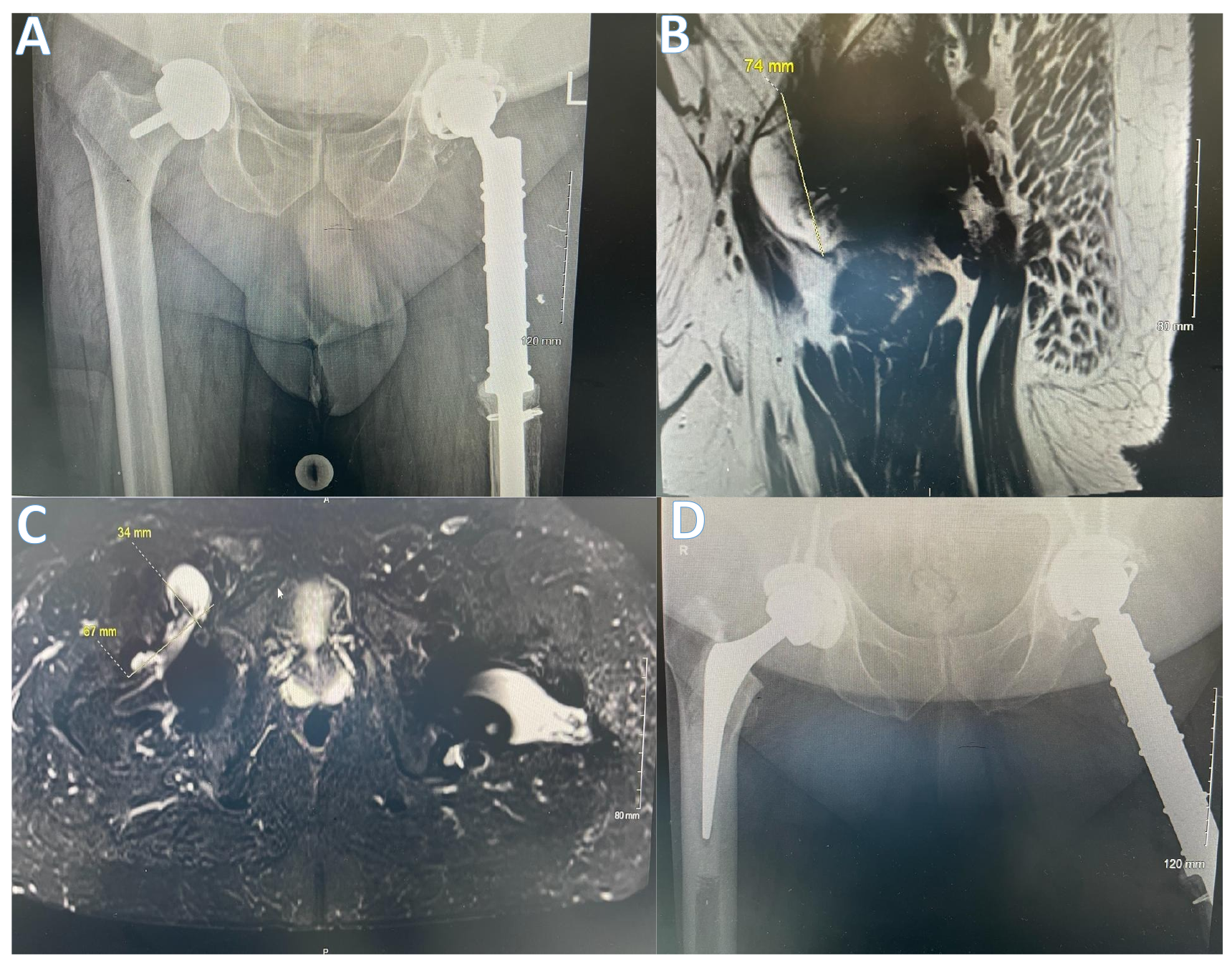
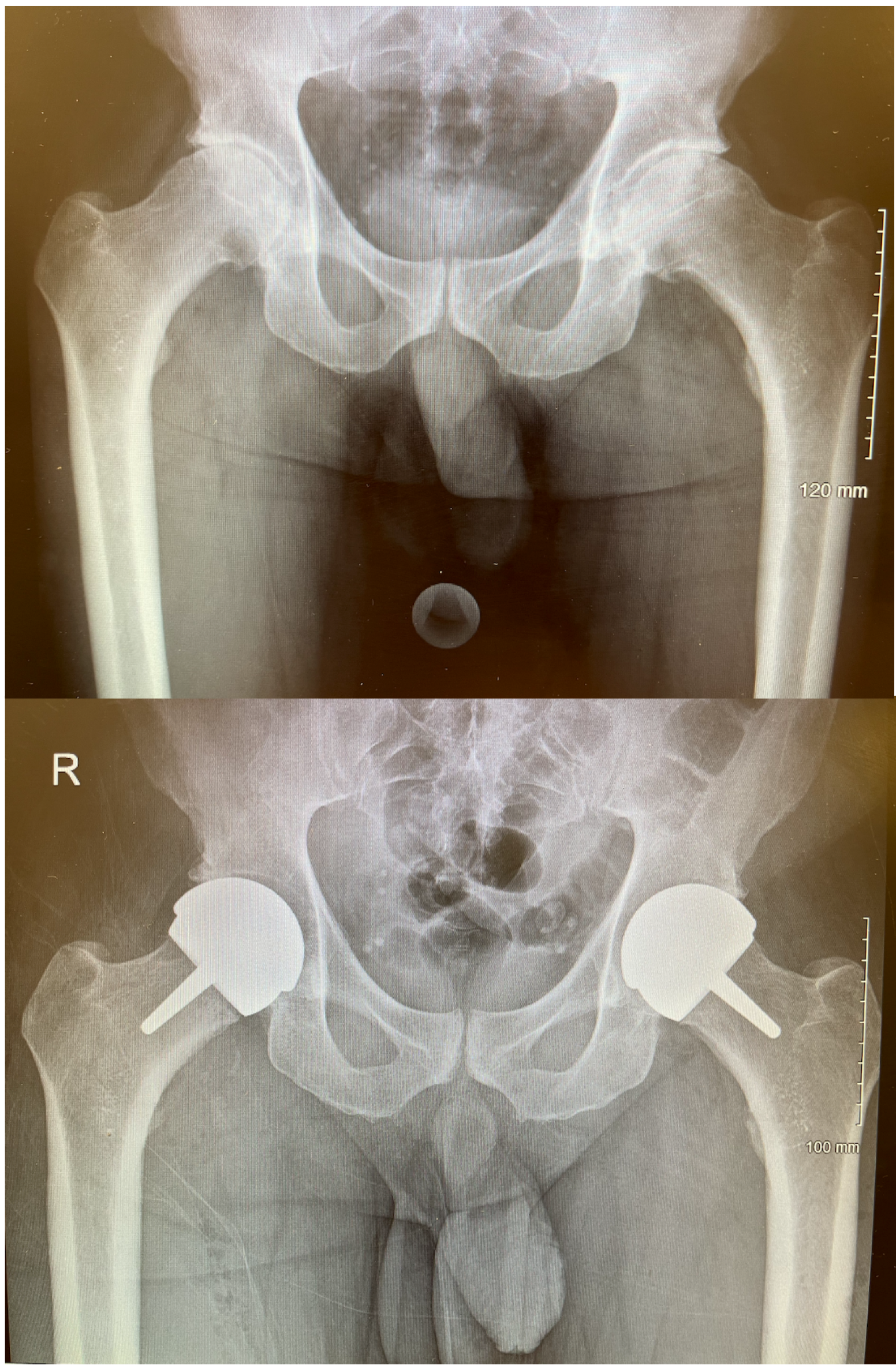
In addition, patients with developmental dysplasia of the hip (DDH) are generally considered unsuitable for HRA. This cohort of patients’ anatomy involves abnormal femoral and acetabular morphology such as increased anteversion, as well as a shallow, dysplastic, and more inclined acetabulum therefore, making it more challenging to optimise the position of the cup and avoid edge loading. The Australian NJR has reported a 20.3% revision rate in DDH patients undergoing HRAs over a ten-year period; in comparison, patients with osteoarthritis (OA) as a primary diagnosis had a 9.3% revision rate. It is worth noting that when a cup is implanted >10 degrees away from the ideal 45-degree inclination, the risk of metal-on-metal pseudotumour is tripled.43 (Figure 3) Therefore, the ideal candidate for consideration for a HRA is a male aged under 55 years with primary osteoarthritis and an adequately sized femoral head in the absence of a history of DDH, avascular necrosis or inflammatory arthritis (Figure 4).


Future prospects
The history of HRAs has demonstrated the impact of technological innovations on implant survival. Although, HRAs have become infrequently performed procedures in the United Kingdom, one must appreciate the importance of preserving bone stock when treating young, active patients who would very likely require multiple revisions in their lifetime. Preserving the femoral neck during HRA allows for easy conversion to a THA. Additionally, in the presence of a well-positioned and fixed acetabular component, one can revise the femur and incorporate a bipolar femoral head. Revision of a primary THA carries greater risk and much longer rehabilitation/recovery periods than undergoing a primary THA and this must be considered when planning treatment for patients across their lifespan.56,57 HRAs allow for large femoral heads which translates into an increase in jump distances and the safe range of motion compared to THAs. The UK NJR reports the rate of revision for dislocation following HRA versus THA as 0.27 per 1000 prosthesis years versus 0.84 per 1000 prosthesis years.58
In light of the recall of a number of implants and the concern regarding adverse reactions to metal debris, there has been interest in the development of ceramic-on-ceramic and metal-on-polyethylene HRAs (59–65). Additionally, current generation ceramics demonstrate a number of advantages which has increased their appeal. These include: resistance to chemical reactions in physiological conditions, bio-inertness, excellent wear properties and high fracture strength and toughness compared to previous generations.45,59 Manufacturers have now incorporated lateral fall simulation impact tests to ensure the absence of fracture or visible damage, as well as high velocity car crash impaction test which have confirmed the suitability of modern ceramic materials for prosthesis design.59,60
An additional advantage is the potential for reduced bacterial adhesion as demonstrated in in-vitro studies however, a reduction in periprosthetic joint infection remains controversial thought Pitto et al noted a lower risk of revision for deep infection in ceramic on ceramic THAs over a 15 year period in their registry based study.61 Currently, there are two ‘Medicines and Healthcare products Regulatory Agency’ approved (MHRA) ceramic-on-ceramic HRA ongoing clinical trials. These are the H1® (Embody Ltd.) and the ReCerf® (MatOrtho Ltd.) and their outcomes are yet to be published (59–61). Other groups have focused their efforts on developing metal-on-polyethylene HRAs though wear has been a concern. The cross-linking of polyethylene has seen a major reduction in the wear vulnerability of these bearings as demonstrated by wear simulator HRA studies which demonstrate a 93% reduction in wear compared to conventional polyethylene.62 Further studies using computed tomographic scans and clinical retrievals have also demonstrated low wear in vivo and have recommended highly cross-linked polyethylene as an alternative bearing options to reduce metal ion-related sequalae.62–65 Treacy et al has recently developed a monobloc highly cross linked polyethylene acetabulum which articulates with a cobalt-chrome femoral head. They reported no impending revisions in the short term and long term data is currently being collected.65 Pritchett has recently reported his series of 190 HRAs using a cementless acetabular cup and a 3.8mm highly cross-linked polyethylene liner with 97% implant survivorship at a mean follow-up of 8.5 years.64 It is hoped that incorporating new bearing materials may improve implant survivorship and allow for greater consideration of HRAs when treating young, active patients.
Competing interests
The authors declare that they do not have any competing interests.
Funding
The authors did not receive any funding for this article.
Ethical Approval
This was not required for this article.
Authors’ contributions
T Al-Jabri: Designed the article layout, drafted, edited, and approved the manuscript.
M Ridha: drafted and edited the manuscript.
A Arif: edited and approved the manuscript
RA McCulloch: helped design the layout, edited and approved the manuscript.
C Jayadev: edited and approved the manuscript.
M Habad: edited and approved the manuscript.
D Kosuge: edited and approved the manuscript.
B Kayani: edited and approved the manuscript.
J Donaldson: edited and approved the manuscript.
JA Skinner: edited and approved the manuscript.
Acknowledgments
Not applicable.
Consent for publication
Not applicable.