
Put your head phones in and experience what it is like to have auditory hallucinations
- Schizophrenia is a type of psychosis, a severe mental disorder in which thoughts and emotions are so impaired that contact is lost with external reality.
- Schizophrenia is the most common psychotic disorder, affecting about 1% of the population.
- Predominantly the illness affects younger people and 75% of sufferers will first experience the onset of schizophrenia between the ages of 16 and 25.
- Someone with schizophrenia would characteristically experience delusions (a belief in something that is not, nor could be, true) and hallucinations (experiencing stimuli that are not present).
- There are many symptoms of the disorder, although not every patient displays all the symptoms.
This video was produced by a sixth form student and I think it takes a really empathetic approach in breaking down the stereotypes of the disorder, whilst also raising awareness.
Movies that showcase schizophrenia


Memory Strategy – SHADED
Speech Poverty
Hallucinations
Avolition
Delusions
Emotional Flattening
Disorganised/Catatonic behaviour
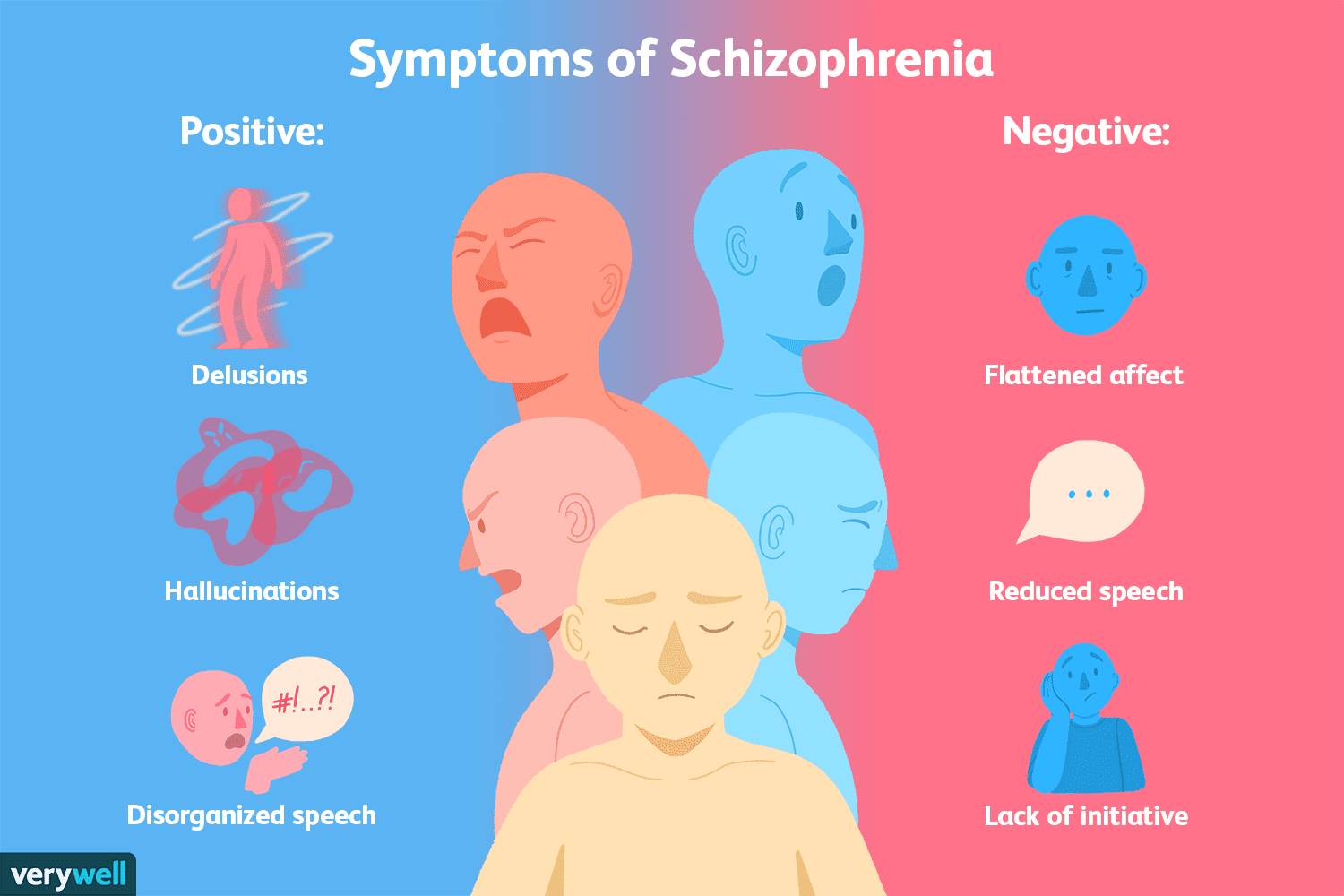
Positive Symptoms: Something extra e.g. a behaviour or biological reaction that you didn’t have before.
- Delusions – beliefs that conflict with reality
- Disorganised or Catatonic behaviour e.g. bizarre and inappropriate outbursts or movements
- Hallucinations – auditory or visual
- Disorganised speech is classed a a POSITIVE SYMPTOM in the DSM-5. This is because they focus on speech becoming incoherent due to swift changes in topics and sentences that don’t appear to connect.

Negative Symptoms: These reflect a reduction or loss of normal function.
- Speech poverty – a rambling of sentences that are difficult to understand, because there is a reduction in the quality of speech- Seen as a NEGATIVE SYMPTOM with the ICD-10 as it is a reduction in the amount and quality of speech.
- Avolition/Apathy: inability to initiate in goal-directed behaviour e.g. poor hygiene, inability to work, lack of energy
- Emotional flattening – reduction in range and intensity of emotional expression, voice tone, eye contact and body language. Also a loss of interest in pleasure in all or almost all activities
Diagnosis and Classification of Schizophrenia
In order to make a diagnosis of schizophrenia, a clinician would use a diagnostic manual such as the DSM-5 (Diagnostic Statistical Manual of mental health) is a classification and description of over 200 mental disorders, grouped in terms of their common features/symptoms. DSM is mostly used in the US. Europe mainly uses the ICD (International Classification of Diseases) which was developed by World Health Organisation (WHO). The way that the DSM-5 and ICD classify schizophrenia differ slightly.
Classification of Schizophrenia according to the DSM-5:
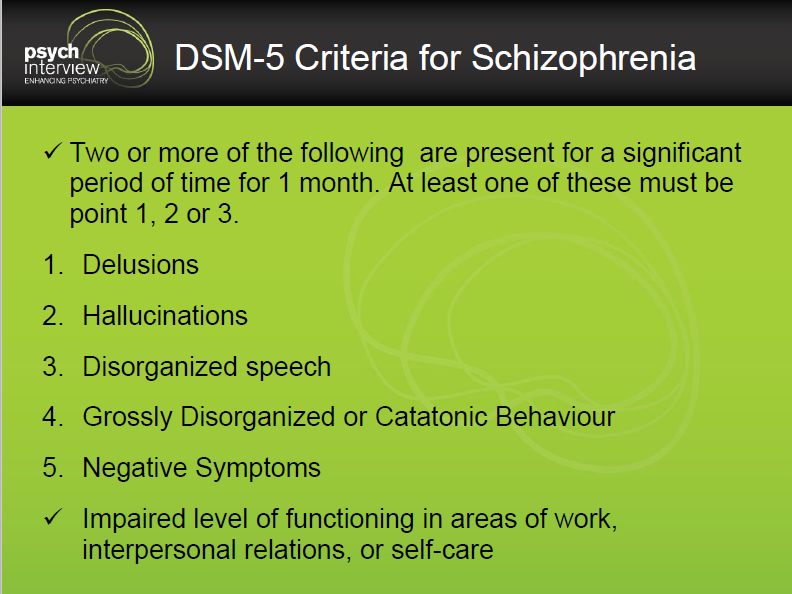
IMPORTANT TO NOTE: Disorganised speech is classed a a POSITIVE SYMPTOM in the DSM-5. This is because they focus on speech becomes incoherent due to swift changes in topics and sentences that don’t appear to connect.
Classification of Schizophrenia according to the ICD-10
At least one of A OR two of B, in both categories the individual must experience the symptoms for most of the time over the course of 1 month.
A:
- Delusions
- Hallucinations voices
- Thought broadcasting (believing that their thoughts can be heard by other people)
B:
- Hallucinations in other formats e.g. visual, olfactory (smell) tactile (touch) etc.
- Speech poverty – seen as a negative symptom as it is a reduction in the amount and quality of speech.
- Catatonic behaviour,
- Negative symptoms e.g. avolition
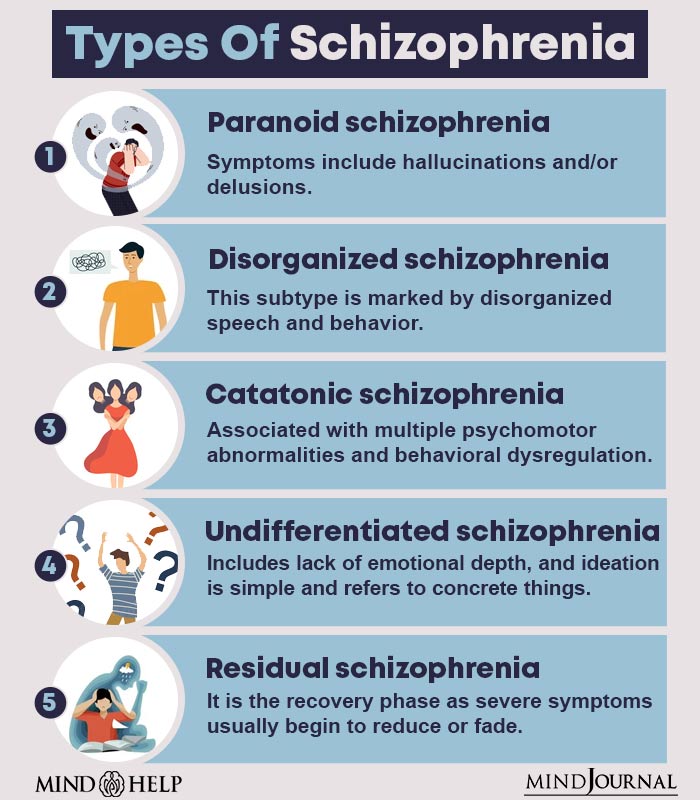
The ICD-10 criteria are also used to classify a patient with subtypes of schizophrenia based on his or her prominent symptoms at presentation. For example, paranoid schizophrenia has prominent symptoms of paranoid delusions accompanied by auditory hallucinations. You do not need to know all of these for your exams, but it is worth learning one or 2 examples so that you can use this as an evaluation point.
You can access the ICD-10 online with this link: https://icd.who.int/browse10/2016/en
Evaluation:
As a reminder it is important to distinguish between reliability and validity when evaluating the classification and diagnosis of schizophrenia.
- Classification systems such as DSM are greatly weakened if they are not reliable. Reliability refers to the consistency of a classification system such as DSM. Does every psychiatrist diagnose patients in a consistent way?
- Validity refers to the extent that a diagnosis represents something that is real and distinct from other disorders. E.g. is schizophrenia really what the patient has? Have they been diagnosed with the correct disorder?
All of the following evaluation points are really important for you to know for the exam because each of the following are names on the specification: CO-MORBIDITY, CULTURAL BIAS, SYMPTOM OVERLAP AND GENDER BIAS. This means you could get get a specific question in these key terms and points.
Co-morbidity: refers to having more than one disorder that exists alongside a primary diagnosis. For example, a person could have both schizophrenia and a personality disorder. However, co-morbidity becomes an issue when psychiatrists are not able to accurately tell the difference between the two conditions. This could lead to an individual being given one diagnosis that is inaccurate, instead of being diagnosed with two disorders, which would be more accurate.
Gender bias in diagnosis: this is when patients can display the same symptoms, but receive different diagnoses because of their gender. For example being diagnosed with autism is generally biased towards males.
Symptom overlap: can lead to inaccurate diagnosis due to other conditions having similar, or the same symptoms e.g. both schizophrenia and bipolar involve positive symptoms such as delusions and avolition.
Cultural bias in diagnosis: this is when patients can display the same symptoms but receive different diagnoses because of their ethnic background; i.e. a patient’s ethnicity makes it more or less likely that they will be diagnosed with schizophrenia.
Reliability and Validity:
- Whaley (2004) suggests that cultural bias is the main reason for the different rates of schizophrenia found when diagnosing black and white Americans. Black Americans are diagnosed with schizophrenia more than white Americans as doctors do not judge their culture norms accurately and misinterpret symptoms (e.g. auditory hallucinations) due to their cultural differences with the patient. This means that cultural bias hinders the validity and accuracy when diagnosing schizophrenia.
- Gender bias – Loring and Powell (1988) selected 290 male and female psychiatrists to read cases studies of patients’ behaviour and make a judgement on these people using standardised diagnostic criteria (e.g. DSM). When the patients were described as ‘male’ or no info about gender was given, 56% of psychiatrists have a schizophrenia diagnosis. When patients were described as ‘female’, only 20% were given a diagnosis of schizophrenia. Interestingly, the gender bias was not as evident among the female psychiatrists, suggesting that diagnosis is influenced not only by gender of the patient but also the gender of the clinician.
- Symptom overlap – Furthermore, symptom overlap can lead to an inaccurate diagnosis. For example, some symptoms of bipolar are similar and overlap with schizophrenia. For example, if a patient is displaying symptoms such as inflated self-esteem, this could easily be confused as a delusion, psychomotor agitation could be confused with catatonic behaviour, depressed mood and energy could be seen as avolition.
- Co-morbidity – refers to the extent that 2 or more conditions can occur at the same time. Psychiatric co-morbidities are common among patients with schizophrenia. These include substance abuse, anxiety and symptoms of depression. Buckley et al (2009) found that 50% of patients with schizophrenia also have a diagnosis of depression and 47% of schizophrenic patients also have a diagnosis substance abuse. This could lead to someone only being provided one diagnosis, when they should have 2 separate diagnoses. Another issue is that because 2 conditions are co-existing, this could lead to misdiagnosis because the collection of symptoms that are presented, may confuse psychiatrists and they could diagnose the patient with an incorrect disorder.
- Validity – The DSM-5 is lead by research. For example, It incorporates the latest findings in neuro-imaging and genetics for each disorder along with gender and cultural considerations. New disorders have been added or adapted to fit in with clinical practice and research. For example, changes in DSM-5 included the reconceptualization of Asperger syndrome from a distinct disorder to an autism spectrum disorder, also the elimination of subtypes of schizophrenia. As a consequence of this continued adaptation, this helps to make diagnosis as accurate as possible
- Reliability – The differences in ICD-10 and DSM-5 will lead to inconsistent diagnoses. For example, if an individual was displaying catatonic behaviour and negative symptoms, they would be diagnosed with schizophrenia under the ICD criteria, but they would not receive a diagnosis of schizophrenia under DSM-5. Therefore, if psychiatrists are using different diagnostic criteria, this will lead to inconsistent diagnoses.
- Rosenhan (1973): This study showed that psychiatrists did not diagnose schizophrenia consistently across different hospitals. 11 patients were diagnosed with schizophrenia and 1 was diagnosed with manic depression. This may seem like a small issue, however, if this is considered on a mass scale, this would suggest that a large number of institutions are not ensuring that diagnoses are consistent. Consequently this reduces the validity of diagnoses because this inconsistency leads to some patients receiving accurate diagnoses, but others with inaccurate. Furthermore, this inaccuracy could also lead to incorrect treatments as a consequence!
The video below is a very biased video about reliability issues. None the less, it gives you some insight into the inconsistency of diagnosis.
Watch the following clip to see first hand some of the issues with reliability and validity. Rosenhan (1973) conducted a study which illustrated just how poor psychiatrists were at accurately diagnosing whether someone had schizophrenia.
Rosenhan (1973) 8 pseudo patients who were unwashed and ungroomed, went into 12 different hospitals and said that they could hear voices saying empty, hollow and thud. 11 patients were admitted to the hospital with a diagnosis of schizophrenia, and 1 patient was admitted with a diagnosis of manic-depression. Once admitted, the pseudo patients acted normally, said they were fine, the voices had gone. Staff never detected their sanity, even when their reports uniformly indicated that the pseudo patients were “friendly”, “cooperative” and “did not exhibit abnormal behaviour”. The average hospital stay was 19 days. All pseudo patients were discharged with diagnosis of schizophrenia ‘inremission’.
Extension – If you really want to show the examiners that you know your stuff, you could use these types of validity 😉
- Aetiological validity: the extent to which the cause of the disorder is the same for each sufferer.
- Descriptive validity: the extent to which individuals diagnosed with the same disorder are similar.
- Predictive validity: the extent to which the diagnostic categories predict the course and outcome of treatment accurately.
