Interviews
Emer Kelly, Fitriana Mawardi, and Kiley Whalen share perspectives in multidisciplinary healthcare

Contraceptive Use Among Females with HIV
1
emjreviews.com Article
Flagship Journal Spring 2024 Volume 9.1
Follow-Up Care Models Post-cancer Treatment Editor's Pick
4 Editorial Board 7 Welcome 9 Foreword Congress Feature 10 Non-Factor Therapies: Reflections on Current Clinical Practice Helena Bradbury Poster Review 13 Sparsentan, a Dual Endothelin Type A and Angiotensin II Subtype 1 Receptor Antagonist for the Treatment of Immunoglobulin A Nephropathy: Latest Trial Results, Pharmacokinetic Considerations, and Binding Profile Interviews 22 Transitioning Patients From Second- to First-Line Prophylaxis in Hereditary Angioedema 28 Emer Kelly 31 Fitriana Mawardi 35 Kiley Whalen Infographic 38 Reviewing Advances in Bone Health Contents 2 T Area ● Month 2023 ● Creative Commons Attribution-Non Commercial 4.0 EMJ ● March 2023 ● Creative Commons Attribution-Non Commercial 4.0
Articles
40 Editor's Pick: Patients’ Preferences for Models of Follow-Up Care During or After Initial Cancer Treatment in Greece: Development of the Qualitative Phase, and Protocol for a Discrete Choice Experiment
Stamuli et al.
51 Prevalence and Factors Associated with Contraceptive Use Among Females Living with HIV at Moi Teaching and Referral Hospital, Eldoret, Kenya
Sawe et al.
59 Renal Replacement Therapy During Liver Transplant Surgery
Sekar et al.
68 Staphylococcus aureus Bacteremia in Patients with Chronic Kidney Disease: Single-Centre Data from Pakistan
Moin et al.
77 Coexistence of Sickle Cell Thalassaemia with Overlapping Syndrome: A Case Report of Systemic Lupus Erythematosus and Autoimmune Hepatitis
Sawlani et al.
87 Impact of Surgical Treatment on Quality of Life of Patients with Early-Stage Cervical Cancer: A Case Study of Two Referral Hospitals in Kenya
Moseti et al.
96 Immunoglobin D Multiple Myeloma: A Single Centre Experience
Narayanan et al.
106 Membranous Nephropathy and Pulmonary Tuberculosis: An Uncommon Combination: Case Report
Bhuwania et al.
111 Post-endoscopic Retrograde Cholangiopancreatography Air Leak Syndrome: An Overview of Current Perspectives
Zameer et al.
118 Liver Elastography for the Detection of MethotrexateInduced Liver Injury: A Retrospective Study
Brotherton et al.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 3 Attribution-Non March EMJ
Editorial Board
Editor-in-Chief
Prof Markus Peck-Radosavljevic Klinikum Klagenfurt am Wörthersee, Austria
Editorial Board
Dr Pierfrancesco Agostoni St. Antonius Hospital, the Netherlands
Dr Fernando Alfonso Hospital Universitario de La Princesa, Spain
Dr Emanuele Angelucci IRCCS Ospedale Policlinico, San Martino, Italy
Dr George Anifandis University of Thessaly, Greece
Dr Riccardo Autorino Virginia Commonwealth University, USA
Prof Ahmad Awada Jules Bordet Institute, Belgium
Prof Sorin T. Barbu “Iuliu Hațieganu” University of Medicine & Pharmacy, Romania
Dr Mátyás Benyó University of Debrecen, Hungary
Prof Andrew Bush Imperial College London, UK
Dr Abdullah Erdem Canda Yildirim Beyazit University, Türkiye
Prof Ian Chikanza Harley Street Clinic, UK
Dr Hassan Galadari United Arab Emirates University, United Arab Emirates
Dr Amir Hamzah Abdul Latiff Pantai Hospital, Malaysia
Dr Lorenz Räber Bern University Hospital, Switzerland
Prof Lászlo Vécsei University of Szeged, Hungary
4 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Aims and Scope
EMJ, the flagship journal of the EMJ portfolio, is an openaccess, peer-reviewed eJournal, committed to elevating the quality of healthcare globally by publishing high-quality medical content across the 18 clinical areas covered in our portfolio. The journal is published quarterly and showcases the latest developments across these clinical areas.
EMJ publishes peer-reviewed research papers, review articles, and case reports across all therapy areas of the EMJ portfolio. In addition, the journal publishes features and opinion pieces create a discussion around key topics in the field and broaden readers’ professional interests. The journal also features interviews with leading experts in various clinical disciplines.
The journal covers advances within the pharmaceutical arena by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in EMJ undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the EMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of EMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-associated content authored by the EMJ Editorial staff undergoes internal quality control checks. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls
into any of the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
Launch Date: 2016
Frequency: Quarterly
Online ISSN: 2397-6764
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (EAHAD 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Greece, the location of work for the primary author of Editor's Pick.
Front cover and contents photograph: Sounion, Greece © NPershaj / stock.adobe.com
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 5

EMJ Podcasts The EMJ Podcast aims to provoke conversations around the latest trends and innovations in healthcare, provide engaging and educational content for healthcare professionals, and hosts conversations with physician entrepreneur, Jonathan Sackier. Listen today www.emjreviews.com
Welcome letter
Editor
Evgenia Koutsouki
Editorial Managers
Anaya Malik, Darcy Richards
Copy Editors
Noémie Fouarge, Kirsty Hewitt
Editorial Co-ordinators
Abigail Craig, Natasha Meunier-McVey
Editorial Assistants
Victoria Antoniou, Helena Bradbury, Ada Enesco, Evan Kimber
Design Manager
Stacey Rivers
Senior Designer
Roy Ikoroha Designers
Steven Paul, Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Head of Sales
Robert Hancox
Director of Performance
Keith Moule
Chief Operating Officer
Dan Scott
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Dear Readers,

Evgenia Koutsouki
Editor
With great satisfaction, I welcome you to the first EMJ flagship issue of 2024. We are delighted to begin the year with this culmination of insightful content, showcasing a selection of articles and interviews, with a special focus on multidisciplinary healthcare. This journal spans several therapeutic areas, and there are highlights within these pages to educate and inform a wide range of healthcare professionals.
The haematologists amongst you will enjoy the articles which bring forward new perspectives on multiple myeloma and sickle cell thalassaemia. Alongside these is a feature that explores non-factor replacement therapy for bleeding disorders, based on a symposium at the annual European Association for Haemophilia and Allied Disorders (EAHAD) meeting.
Three interviews with thought leaders are also included in this issue, each discussing important aspects of multidisciplinary care. Spanning obstructive pulmonary disease to disaster preparedness, these are sure to spotlight important factors to consider when delivering care.
The Editor’s pick for this release is a compelling research article by Stamuli et al., which outlines patient preferences in the follow-up care of survivors of cancer, aiming to use patient-centred care models and preferences to improve support.
Thank you to all of our amazing contributors, and to the supportive Editorial Board that maintains the high standards of content we are pleased to share in this issue. Alongside this, thanks to our reviewers, who also consistently play a pivotal role in ensuring the articles we publish are of an esteemed quality. I hope you enjoy reading!
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 7
Stay up to date with new advancements across European healthcare Visit EMJ for our comprehensive collection of peerreviewed research articles, latest interviews, and features across a range of therapeutic disciplines. Visit EMJ www.emjreviews.com
Foreword

Dear Colleagues,
Welcome to the latest issue of EMJ, exploring the importance of multidisciplinary healthcare. This theme is discussed in depth across a diverse range of topics, including cervical cancer, post-endoscopic retrograde cholangiopancreatography air leak syndrome, and the use of liver elastography for methotrexate-induced liver injury, amongst others.
Notably, my Editor’s Pick for this issue is the article entitled ‘Patients’ Preferences for Models of Follow-Up Care During or After Initial Cancer Treatment in Greece: Development of the Qualitative Phase, and Protocol for a Discrete Choice Experiment’. It offers insightful findings from a recent discrete choice experiment, emphasising the importance of patient-centred care approaches.
Additionally, within this issue is an article that investigates the clinical features of Staphylococcus aureus bacteraemia among
patients with chronic kidney disease, highlighting the prevalence of hospital-acquired infections. In another article, the detection potential of elastography for methotrexate-induced liver fibrosis is assessed, giving promise to alternative non-invasive diagnostic techniques.
The first EMJ issue of 2024 also showcases case reports on the association between pulmonary tuberculosis and membranous nephropathy, and the incidence of post-endoscopic retrograde cholangiopancreatography air leak syndrome. Observations like these can elevate clinical understanding of diseases, directly improving patient care as a result. Insightful interviews were also conducted with Fitriana Mawardi, Emer Kelly, and Kiley Whalen.
I would like to extend thanks to all the authors, reviewers, interviewees, and Editorial Board members for their continued dedicated commitment to EMJ. I hope this issue proves to be an illuminating and informative read for all healthcare professionals.
 Prof Lászlo Vécsei
Prof Lászlo Vécsei
Head of Neuroscience Research Group, Department of Neurology, University of Szeged, Hungary
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 9
Non-Factor Therapies: Reflections on Current Clinical Practice
Authors: Helena Bradbury, EMJ, London, UK
Citation: EMJ. 2024;9[1]:10-12. https://doi.org/10.33590/emj/CPRD5899.
The 17th Annual Congress of the European Association for Haemophilia and Allied Disorders (EAHAD) took place on 6th–9th February 2024 in Frankfurt, Germany. In a comprehensive and interactive session, healthcare experts and patients gathered to discuss current approaches in clinical practice. The session was chaired by Jan Blatny, University Hospital Brno, Czechia; and Niamh O’Connell, The National Coagulation Centre, St James’s Hospital, Dublin, Ireland.
ALLIED HEALTHCARE PROFESSIONALS’ DAY
Nanda Uitslager, University Medical Center Utrecht, the Netherlands, opened the session by providing an overview of the Allied Healthcare Professions (AHP) Day. Comprising nurses, physiotherapists, and psychologists, this event was a collaborative effort to celebrate and recognise the remarkable work of the healthcare workforce, as well as highlight current challenges in haemophilia treatment. A joint midday session on non-factor therapies was held, with the aim to better understand the experiences of healthcare professionals (HCP) and patients with this line of treatment.
Common blood disorders, such as haemophilia, are caused by a lack of integral clotting proteins like Factor VIII and Factor IX in haemophilia A and B, respectively. Factor replacement therapy combats this by replenishing the clotting agent in question, through intravenous infusion. Whilst the safety and efficacy has proven successful, there is a considerable associated treatment and disease burden, impacting the patient’s quality of life, and prompting HCPs to call for treatment alternatives. The bleeding rate, for example, remains high for those receiving prophylaxis, and intravenous drug
administration several times a week can be demanding on patients.
Conversely, non-replacement therapies target the coagulation cascade, boosting the haemostatic potential by mimicking coagulation factors, or by reducing naturally occurring inhibitors, known as factor mimetics and rebalancing agents, respectively. As administration is given subcutaneously, the treatment burden is also reduced. Differences in treatment and disease burden between factor versus non-factor-based replacement therapy was discussed in-depth within the AHP joint session.
SETTING THE SCENE: THE DIFFERENCE BETWEEN CHOOSING FOR YOURSELF AND RECOMMENDING
Ilaria Cutica, University of Milan, Italy, highlighted the unique challenges in making treatment decisions for oneself, and on behalf of someone else, and provided comprehensive guidance for each circumstance. For both caregivers and HCPs, she emphasised the importance of information, with greater treatment knowledge corresponding to improved engagement, trust, and communication from the patient.
"This event was a collaborative effort to celebrate and recognise the remarkable work of the healthcare workforce."
10 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● EAHAD 2024
The influence of personal factors, such as beliefs, desires, cognitive bias, and risk perception in decision-making, was subsequently explored. When seeking to recognise potential conflicts of interest, Cutica explained that one might not necessarily agree with a patient’s values or beliefs, but it is paramount that these factors are acknowledged, and incorporated within the decision-making process.
"Caregiver figures often exhibit greater risk perception than paediatric patients."
Finally, she drew on shared decision-making, which HCPs use when making decisions on behalf of a patient. In this collaborative approach, the treatment options are firstly relayed to the patients, with potential adverse risks and reported successes listed. A discussion then follows, in which any patient queries or questions are addressed. As noted by Cutica, the latter stage also serves as an opportunity for the HCP to better understand the patient as a person, allowing the provision of more tailored recommendations.
PANEL DISCUSSION ON TREATMENT CHOICES: MULTIDISCIPLINARY SUPPORT FOR DECISION-MAKING
A panel session followed, in which questions were posed to the audience, voted on, and the answers discussed amongst the panellists. The panel consisted of patient David Flanagan; Marie Katzerova, University Children’s Hospital, Brno; Niamh O’Connell; Mary Kavanagh, Children’s Health Ireland (CHI), Crumlin, Ireland; Ilaria Cutica; and Jan Blatny.
The first question focused on the decisionmaking process, and whether it changes when the perspective shifts from that of patient to caregiver. With 69% of the votes, ‘No’ was the predominant answer. Providing a patient and HCP perspective, respectively, Flanagan and O’Connell agreed that caregiver figures often exhibit greater risk perception than paediatric patients, acknowledging the natural worry parents may feel for their children. Offering a nurse’s viewpoint, Kavanagh stated that the requirement for information may be higher, as the caregiver adopts a responsibility to understand all risks on behalf of the child.

Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 11 EAHAD 2024 ● Congress Feature

The precise role of HCPs within the decisionmaking process was then questioned. A majority (85%) felt it was ‘to describe the treatment options and discuss the potential benefits and risks before coming to an agreed decision’, a view shared amongst the panellists. Few agreed with the remaining statements, suggesting leaving the decision entirely to the patient, or providing a direct recommendation. Opening the discussion further, the panellists explored several scenarios, such as a conflict of interest between caregiver and patient, and providing treatment information when limited literature exists.
Finally, with recent advances in treatment options for patients with haemophilia, the importance of the multidisciplinary approach was reviewed. This aims to optimise patient management and outcomes by supplying patients with a range of medical personnel, such as haematologists, physiotherapists, psychosocial support, dental care, and surgery.
In agreement with the majority (76%), Flanagan felt that multidisciplinary treatment was more important in haemophilia treatment, raising the point that as the availability and quality of treatment options improve, patients may live longer, and thus require wider holistic care as new, unforeseen complications may arise.
CONCLUSION
With greater implementation of non-factor replacement therapy in clinical practice for bleeding disorders, it is ever more necessary for reflections like this to occur. The discussion called for continued collaboration between patients and HCPs, and multidisciplinary care for haemophilia. The panel offered a comprehensive view of the considerations at play when making medical decisions, highlighting risk perception, cognitive bias, and personal beliefs, amongst others. ●
12 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● EAHAD 2024
Sparsentan, a Dual Endothelin Type A and Angiotensin II Subtype 1 Receptor Antagonist for the Treatment of Immunoglobulin A Nephropathy: Latest Trial Results, Pharmacokinetic Considerations, and Binding Profile
This presentation took place at the American Society of Nephrology (ASN) Kidney Week 2023, held on 2nᵈ–5ᵗʰ November in Philadelphia, Pennsylvania, USA
Presenters: Brad Rovin,1 Bruce Hendry,2 Chee Kay Cheung3,4
1. Division of Nephrology, Ohio State University Wexner Medical Center, Columbus, USA
2. Travere Therapeutics, Inc., San Diego, California, USA
3. University of Leicester, UK
4. Leicester General Hospital, UK

Disclosure:
Rovin reports consulting fees from Alexion Pharmaceuticals, Alpine Pharma, BioCryst Pharmaceuticals, Calliditas Therapeutics, Novartis, Q32 Bio, Omeros, Otsuka Pharmaceuticals, Travere Therapeutics, Inc., and Vera Therapeutics; and has a leadership role at NephroNet, Lupus ABC/LRA, and Lupus Foundation of America. Hendry is an employee of Travere Therapeutics, Inc.; and has equity or other financial interest in Travere Therapeutics, Inc. Cheung repots consulting fees from George Clinical, and Vera Therapeutics; honoraria from Stada; research funding from GSK and Travere Therapeutics, Inc.; advisory boards for Calliditas, CSL Vifor, and Novartis; steering committee/DSMC for CSL Vifor, Alpine Immune Sciences, and Roche; and travel support from Otsuka, and Chinook Therapeutics.
Acknowledgements: Writing assistance was provided by Eleanor Roberts, Beeline Science Communications Ltd, London, UK.
Disclaimer: The opinions expressed in this article are not necessarily those of CSL Vifor.
Support: Publication of this feature was supported and reviewed by CSL Vifor, and reviewed by Travere Therapeutics.
Keywords: Angiotensin, endothelin, glomerulonephritis, optimised supportive care, pharmacodynamics, pharmacokinetics, proteinuria, receptor occupancy.
Citation: EMJ. 2024;9[1]:13-21. DOI/10.33590/emj/11000020. https://doi.org/10.33590/emj/11000020.
13
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 13 Poster Review
Meeting Summary
Immunoglobulin A nephropathy (IgAN) is one of the most common forms of primary glomerulonephritis. In some patients, it can progress rapidly, leading to proteinuria, kidney failure, and death. Standard of care is traditionally with an angiotensin converting enzyme inhibitor (ACEi), or an angiotensin II (Ang II) receptor blocker (ARB). More recently, drugs targeting both endothelin 1 (ET-1) and Ang II receptors have been developed, as overactivation of such is implicated in IgAN. Sparsentan is a dual ET Type A (ETAR) and Ang II subtype 1 receptor (AT1R) antagonist. The PROTECT study compared sparsentan with the ARB irbesartan, in patients with IgAN and with proteinuria of ≥1 g/day despite stable dose of ACEi/ARB for ≥90 days. Data presented at the 2023 American Society of Nephrology (ASN) Kidney Week showed that use of sparsentan led to sustained (>110 weeks) decreases in proteinuria, and a significantly greater preservation of kidney function, compared with irbesartan. The ongoing SPARTAN study is investigating the use of sparsentan in recently diagnosed, treatment-naïve patients with IgAN. Preliminary data in 12 patients showed rapid and sustained proteinuria reductions, with little change from baseline in estimated glomerular filtration rate (eGFR), body weight, or total body water mean at Week 36. In both studies, sparsentan was generally well-tolerated with, in PROTECT, a comparable safety profile to irbesartan. Data presented at the congress also showed that sparsentan consistently occupies AT1R at levels exceeding ETAR occupancy. This balance is hypothesised to contribute to sparsentan’s limited risk of fluid retention.
Introduction
The immune complex-mediated glomerular disease IgAN is a predominant cause of primary glomerulonephritis,1-4 especially in males,5 with an incidence of 0.2–5.7 per 100,000 persons per year.2,3 IgAN is most commonly diagnosed in patients between 20–40 years of age.2,6,7 Initial presentation of IgAN can range from generally asymptomatic microscopic haematuria, to high levels of proteinuria, and from slow to rapid progression, to kidney decline and death.1,8 Analysis of 2,299 adults with IgAN from the UK National Registry of Rare Kidney Diseases (RaDaR) database found an estimated 5-year survival rate of 0.71 (95% confidence interval [CI]: 0.69–0.73) and 20-year survival rate of 0.28 (95% CI: 0.25–0.31).9
IgAN initially develops due to high circulating levels of galactose-deficient IgA1,10 which can occur following a mucosal infection, and is due to an inherited abnormality in some.11,12 Autoantigens can develop to galactose-deficient IgA1 and, in complex, these can be deposited in glomerular mesangium, leading to mesangial cell activation and ET-1 and Ang II overexpression, complement pathway activation, and inflammatory component secretion, proteinuria, glomerular injury, kidney
inflammation, tubulointerstitial scarring, and fibrosis.1,12-14 ET-1 has a wide role in kidney function, including in fluid, sodium, and reninangiotensin-aldosterone system homeostasis, as well as glomerular arteriolar and vascular tone regulation.15 Increased ET-1 renal expression is predictive of rapid IgAN progression,16 with sustained ETAR activation shown in progressive IgAN, associated with proteinuria, tubulointerstitial inflammation, and fibrosis.17 Ang II, via AT1R, has a role in intraglomerular pressure and cell growth, as well as in renal inflammation, vascular dysfunction, tubulointerstitial fibrosis, and proteinuria development.18,19 It can also stimulate renal release of, and enhanced vasoconstriction by, ET-1.18,20
IgAN treatment is key to slowing progression and increasing survival.21 According to the Kidney Disease Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group, for patients with proteinuria >0.5 g/day, initial therapy is the highest tolerated dose of an ACEi or ARB. Optimised supportive care may include blood pressure management, strategies to reduce cardiovascular risks, and lifestyle modifications. For patients with proteinuria >0.75–1.00 g/day despite ≥90 days optimised supportive care, immunosuppressive drugs may be utilised, and/
14 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Poster Review
or patients may consider entering into a clinical trial, where appropriate. Treatment-emerged toxicity risks with immunosuppressive drugs must be considered in patients with eGFR <30 mL/ min/1.73 m2, diabetes, a BMI >30 kg/m2, latent infections, secondary disease, uncontrolled psychiatric illness, severe osteoporosis, or active peptic ulceration.21
Sparsentan for the Treatment of IgAN
Analysis of the RaDaR data showed that, for patients with IgAN, higher proteinuria was significantly associated with worse kidney survival.9 As such, treatment includes drugs that can lower proteinuria.21 One such therapy is sparsentan, a novel, non-immunosuppressive, single-molecule, dual ETAR and AT1R antagonist (DEARA).18 This drug received a European Medicines Agency (EMA) orphan designation for IgAN,22 and accelerated approval by the U.S. Food and Drug Administration (FDA).23 Sparsentan’s action as a DEARA is key to its role in controlling IgAN.18
The PROTECT Study for Sparsentan
Sparsentan received accelerated FDA approval23 based on interim results from the double-blind, randomised PROTECT study (NCT03763850), which included the AT1R-only antagonist irbesartan as an active comparator.24 PROTECT included adults (≥18 years old) with biopsyproven IgAN and, at screening, proteinuria of ≥1 g/day, and eGFR ≥30 mL/min/1.73 m2 Participants were on stable, maximally tolerated ACEi or ARB doses for ≥12 weeks prior to screening. The double-blind treatment period was 110 weeks, with the primary efficacy endpoint of change in urinary protein-tocreatinine ratio (UPCR) from baseline to Week 36. After 110 weeks, there was a 4-week study drug withdrawal period, and resumption of optimised supportive care.24
In total, 404 participants were randomised and treated with either sparsentan (200 mg/day initially, titrated to 400 mg/day from Week 3; n=202) or irbesartan (150 mg/day initially, titrated to 300 mg/day from Week 3; n=202). For both
drugs, these are the maximum label doses.25,26 All participants discontinued ACEi/ARB treatment 1 day prior to study start. For the majority of participants, the study drug target dose was reached (sparsentan 95%, irbesartan 97%), with 17% of participants taking sparsentan and 11% taking irbesartan requiring dose reduction after reaching target. By Week 110, 19 participants discontinued sparsentan due to an adverse event (AE), and five due to participant decision. For irbesartan, 18 discontinued due to an AE, and 28 due to physician or participant decision.27
Mean age (±standard deviation [SD]) was similar between groups (sparsentan 46.6 years [±12.8] versus irbesartan 45.4 [±12.1] years), with both groups having a mean time of initial biopsy to informed consent of 4 years. Both groups had more males (sparsentan 69%, irbesartan 71%) than females, in line with epidemiology findings.5 The majority were White (sparsentan 64%, irbesartan 70%), or Asian (sparsentan 33%, irbesartan 24%). Groups had similar median (interquartile ranges) urine protein excretion values (sparsentan 1.8 g/day [1.2−2.9] versus irbesartan 1.8 g/day [1.3−2.6]), and mean eGFR (sparsentan 56.8 [±24.3] mL/ min/1.73 m2 versus irbesartan 57.1 [±23.6] mL/ min/1.73 m2), as well as similar blood pressure levels and haematuria occurrence.27,28
Results from the Phase III PROTECT Trial
Brad Rovin
In PROTECT,28 sparsentan significantly reduced UPCR by 49.8% from baseline to Week 36, compared with 15.1% for irbesartan (p<0.0001).29 As presented by Brad Rovin, Ohio State University Wexner Medical Center, Columbus, USA, and recently published, this reduction was sustained at Week 110 (Figure 1) when reductions from baseline were 42.8% with sparsentan, and 4.4% with irbesartan.27,28 A greater proportion of the sparsentan group (31%), compared with the irbesartan group (11%), achieved complete remission (<0.3 g/day; relative risk: 2.5 [95% CI: 1.6–4.1]).28
To ascertain whether changes in proteinuria translated into kidney function benefits, eGFR was
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 15 Poster Review
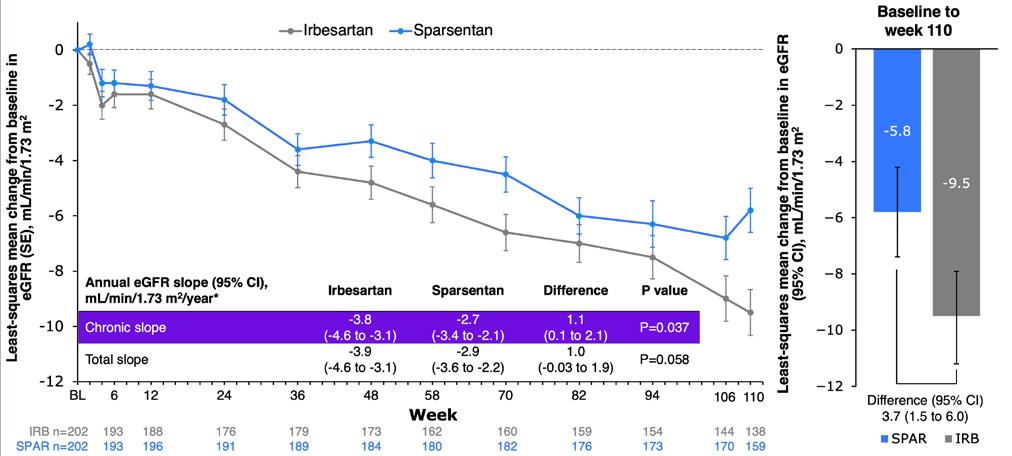
*Analysis includes eGFR data for patients on treatment; off-treatment and missing data imputed using the multiple imputation procedure.
CI: confidence intervals; eGFR: estimated glomerular filtration rate; SE: standard error.
also tracked over 110 weeks, with overall decline shown to be consistently lower with sparsentan than with irbesartan (Figure 1).27,28 A significant difference, favouring sparsentan, was shown in chronic slope (Weeks 6−110; p=0.037), with difference in total slope (Day 1−Week 110) narrowly missing significance (p=0.058; Figure 1).28
Subgroup analyses of annualised change in eGFR by baseline eGFR (<60 or ≥60 mL/min/1.73 m2) or proteinuria (≤1.75 or >1.75 g/day) using the chronic or total slope demonstrated consistent treatment effects across disease severity. Sensitivity analyses of annualised change in eGFR (chronic or total slope models) included either the intentionto-treat population (all eGFR measurements to study end), or discounted eGFR measurements after initiation of rescue immunosuppression for renal disease (3% with sparsentan, 8% with irbesartan).28 These analyses also showed differences in favour of sparsentan. An additional finding was that 9% of the sparsentan group and 13% of the irbesartan group had a confirmed 40% reduction in eGFR, kidney failure, or death, with a relative risk for this composite kidney failure endpoint of 0.68 (95% CI: 0.4–1.2).27,28
Over 110 weeks, 93% of the sparsentan group and 88% of the irbesartan group reported a treatment-emergent AE (TEAE). The most common was COVID-19, followed by hyperkalaemia, peripheral oedema, dizziness, headache, hypotension, and hypertension. Percentages for each were similar between groups. There was a low, comparable incidence of elevated liver enzymes, and there were no cases of drug-induced liver injury. TEAEs led to treatment discontinuation in 10% of the sparsentan group and 9% of the irbesartan group. There was one TEAE leading to death, in the irbesartan group.27,28
Rovin concluded that the clinical benefit of sparsentan with regard to significant, rapid, and sustained proteinuria was confirmed by findings of significant differences in chronic eGFR slope between treatments, which they proposed to be an accurate measurement of the long-term nephroprotective effect of sparsentan and irbesartan. Sparsentan was generally welltolerated, and the safety profile was comparable to irbesartan.27,28
16 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Poster Review
Figure 1: Change from baseline in estimated glomerular filtration rate.28
Sparsentan Receptor Occupancy Modelling, Clinical Actions, and Safety Implications
Bruce Hendry
Two other findings in the PROTECT study were minimal changes in body weight in either group, and a low incidence of peripheral oedema (15% of the sparsentan group, 12% of the irbesartan group). Among participants with no oedema at baseline, 1% treated with sparsentan developed moderate oedema, and 1% treated with irbesartan developed severe oedema. New diuretic use was prescribed in 24% of the sparsentan group and 27% of the irbesartan group. No events of oedema led to sparsentan discontinuation, and there was no treatment-related fluid retention or heart failure.27 “These observations,” said Bruce Hendry, Travere Therapeutics, Inc., San Diego, California, USA, “are consistent with a benign safety profile of sparsentan in regard to fluid status.”
Hendry hypothesised that the action of sparsentan on maintaining normal fluid balance may be related to properties as a DEARA. IgAN mouse models show that blocking ETAR can lead to significant decreases in proteinuria and glomerulonephritis.31,32 However, use of drugs that target ETAR alone can lead to fluid retention, which, in some patients, has led to heart failure and hospitalisation.33 Conversely, AT1R antagonists can lead to decreased sodium retention and promote fluid excretion.34 Hence, with regard to fluid levels, the AT1R antagonist in sparsentan is proposed to balance the actions of the ETAR antagonist.19,29,35
To examine the relationship between the clinical actions of sparsentan in IgAN, and its molecular, pharmacological properties, radioligand binding assays were used to determine 24-hour receptor affinities (inhibitory constant [Ki]) of sparsentan for ETAR, ETBR, AT1R, and AT2R, with population pharmacokinetic (PK) modelling used to derive 24-hour PK and receptor occupancy profiles. This utilised data from PROTECT participants.30
Steady-state PK parameters of sparsentan (Figure 2) included minimum/maximum plasma concentrations of 1,266/5,936 ng/mL, a halflife of 9.6 hours, and an area under the curve of 80,000 ng.h/mL. Receptor affinity (Ki) of
sparsentan was highest for AT1R (0.36 nmol/L) and ETAR (12.8 nmol/L), and much lower for AT2R (190 nmol/L) and ETBR (6,582 nmol/L). Protein binding was 99%. “The data show that sparsentan creates a fully occupied AT1R throughout the 24 hours, at >0.95% occupancy,” said Hendry, “and substantial occupancy of the ETAR, varying between 60% and 90% that, importantly, is always less than AT1R occupancy. Occupancy of the ETBR is very low, <2%, and therefore, the selectivity for ETAR versus ETBR plays out as a clear effect in the clinical setting” (Figure 2).30 “When a drug solely targets ETAR, on top of AT1R blockade,” said Hendry, “periods of relatively unaccompanied ETAR antagonism may occur, representing a risk for fluid retention. If AT1R consistently exceeds ETAR antagonism, as seen with sparsentan, risk appears to be minimised or avoided.” The data shown here, continued Hendry, “are consistent with this hypothesis.” In summary, said Hendry, the results here “could partly explain the fluid retention seen with ETAR antagonists and the minimal changes in fluid status seen with sparsentan.”30
Sparsentan as First-Line Treatment for Incident Patients with IgA Nephropathy: Preliminary Findings from the SPARTAN Trial
Chee Kay Cheung
In the RaDaR data analysis, survival rate was lowest, and mean eGFR slopes greatest, in patients with proteinuria ≥1.76 g/g. This was vice versa in those with proteinuria <0.44 g/g.9 As such, the actions of sparsentan on lowering proteinuria and eGFR slope shown above may, over time, lead to greater survival benefit.30 However, in PROTECT, the average time between diagnosis of IgAN and age at initial biopsy was around 4 years, with nearly one-third of participants receiving an ACEi or ARB at time of enrolment.27
Sparsentan’s rapid, sustained reduction in proteinuria, with corresponding nephroprotective properties,27,28 means it may be appropriate for newly diagnosed patients. The ongoing SPARTAN study (NCT04663204), a Phase II, open-label, single-arm trial, is investigating the safety, efficacy, and mechanistic actions of sparsentan as first-line therapy for patients with IgAN.37
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 17 Poster Review
A) AT1R and ETAR. B) ETAR and ETBR.30
*PK data are based on population PK model prediction for a patient with IgAN.
AT1R: angiotensin II receptor type 1; ETAR: endothelin receptor type A; ETBR: endothelin receptor type B; h: hours; IgAN: immunoglobulin A nephropathy; PK: pharmacokinetics.
Participants receive sparsentan 200 mg for the first 2 weeks, up-titrated to 400 mg, which they receive until Week 110, followed by a 4-week off treatment period. Key eligibility criteria include age ≥18 years, biopsy-proven diagnosis of IgAN within ≤6 months, proteinuria ≥0.5 g/day, eGFR ≥30 mL/min/1.73 m2, and no ACEIs/ARBs within ≤12 months. Key endpoints are change from baseline in proteinuria, eGFR, and blood pressure; complete remission of proteinuria (<0.3 g/day); and safety.37
Chee Kay Cheung, University of Leicester, UK, reported preliminary clinical findings to Week 36 of SPARTAN for 12 participants, seven of whom
were male (58.3%), 10 (83.3%) were White, and the mean age at informed consent was 35.8 years (±12.2). At data cutoff (September 26th 2023), seven participants had received sparsentan for 36 weeks, three for 12 weeks, and two for 6 weeks.36 At baseline, median (interquartile range) urine protein excretion rate was 1.4 g/day (0.6–3.2), and median UPCR was 1.3 g/g (0.4–1.7).36 Similar to PROTECT findings,27 following sparsentan initiation, UPCR decreased rapidly by Week 4, with reductions sustained over 36 weeks (Figure 3).36 Cheung reported how, “at baseline, four patients had protein excretion >2 g/day, three of which had proteinuria reductions of more than 75% during
Time (h) 10,000 9,000 8,000 7,000 6,000 5,000 4,000 3,000 2,000 1,000 0 3 6 9 12 15 18 21 24 100 75 50 25 0 ETAR occupancy Sparsentan PK Time (h) AT1R occupancy 10,000 9,000 8,000 7,000 6,000 5,000 4,000 3,000 2,000 1,000 0 3 6 9 12 15 18 21 24 100 75 50 25 0 Sparsentan PK
A B 18 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Poster Review
Figure 2: Sparsentan steady-state concentration (left axis)* and receptor occupancies (right axis) over 24 hours following administration of a single 400 mg oral dose in PROTECT.
treatment. Overall, 67% achieved complete remission of proteinuria at any timepoint during the first 36 weeks.”
Also shown in this analysis were relatively stable eGFR levels (baseline mean: 70.2 mL/min/1.732 [±25.0]) over 36 weeks.36 Mean systolic/ diastolic blood pressure (125 [±10]/78 [±10] at baseline) decreased slightly until Week 4, but then remained stable (mean 114/70 at Week 36, SD not reported). Mean office and ambulatory 24-hour blood pressures also showed a systolic/ diastolic decrease from baseline to Week 6: −12 mmHg (±8)/−7 mmHg (±8), −13 mmHg (±13)/−10 mmHg (±9), respectively. At baseline, mean BMI was 27.5 kg/m2 (±7.2), and weight was 83.1 kg (±24.7). The latter fluctuated mildly over 36 weeks, with mean changes ranging from −0.3 kg (±0.7) to 0.8 kg (±3.0). Total body water mean was 47.1 L (±7.4) at baseline. At Weeks 6, 12, and 14, this decreased slightly by −2.0 L (±7.2), −1.9 L (±7.9), and −3.6 L (±9.1), respectively.36 One participant discontinued after 6 weeks’ treatment due to hypotension. There were three serious AEs, none of which were treatment-related.36
Cheung concluded that “as first-line treatment in patients newly diagnosed with IgAN, sparsentan led to a rapid and sustained reduction in proteinuria and control of blood pressure, and was generally well-tolerated. Body weight was
maintained, with no evidence of fluid retention.”36 These initial findings are similar to those shown in PROTECT.27 Of note, this was a treatmentnaïve population.36 As higher proteinuria levels at diagnosis and over time are associated with worse survival and kidney failure outcomes,9 lowering proteinuria early following diagnosis could contribute to better outcomes.
Conclusion
IgAN can, in some patients, progress rapidly to kidney failure or death; hence, effective treatment is key to preserving kidney function and sustain survival.1,8,38 The strong antiproteinuric effects of sparsentan shown in PROTECT27 and SPARTAN36 arise, according to Hendry, from the properties of sparsentan as a DEARA.35,39 There is also evidence to suggest that minimal to no rates of clinically relevant fluid retention observed with sparsentan may be due to consistent occupancy of AT1R at levels always exceeding ETAR occupancy.27,30,36 The PROTECT27 and SPARTAN36 trials show the utility of sparsentan in both treatment-experienced and treatment-naïve patients, with regard to both sustained proteinuria decreases and renal protection. Sparsentan was generally safe and well-tolerated.
Week -100 -80 -60 -40 -30 0 0 4 n=10 -62.6% -58.4% -71.0% -75.5% -81.0% n=12 n=10 n=7 n=7 6 12 24 36
SE: standard error; UPCR: urine protein-to-creatinine ratio.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 19 Poster Review
Figure 3: Proteinuria change (urine protein-to-creatinine ratio) from baseline.
References
1. Lai KN et al. IgA nephropathy. Nat Rev Dis Primers. 2016;2:16001.
2. Nair R, Walker PD. Is IgA nephropathy the commonest primary glomerulopathy among young adults in the USA? Kidney Int. 2006;69(8):1455-8.
3. McGrogan A et al. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transplant. 2011;26(2):414-30.
4. Kwon CS et al. A systematic literature review of the epidemiology, healthrelated quality of life impact, and economic burden of immunoglobulin a nephropathy. J Health Econ Outcomes Res. 2021;8(2):36-45.
5. O'Shaughnessy MM et al. Glomerular disease frequencies by race, sex and region: results from the International Kidney Biopsy Survey. Nephrol Dial Transplant. 2018;33(4):661-9.
6. Le W et al. Long-term renal survival and related risk factors in patients with IgA nephropathy: results from a cohort of 1155 cases in a Chinese adult population. Nephrol Dial Transplant. 2012;27(4):1479-85.
7. Selewski DT et al. Clinical characteristics and treatment patterns of children and adults with IgA nephropathy or IgA vasculitis: Findings from the CureGN study. Kidney Int Rep. 2018;3(6):1373-84.
8. Jarrick S et al. Mortality in IgA nephropathy: a nationwide population-based cohort study. J Am Soc Nephrol. 2019;30(5):86676.
9. Pitcher D et al. Long-term outcomes in IgA nephropathy. Clin J Am Soc Nephrol. 2023;18(6):72738.
10. Knoppova B et al. Pathogenesis of IgA nephropathy: current understanding and implications for development of diseasespecific treatment. J Clin Med. 2021;10(19):4501.
11. Kiryluk K et al. Aberrant glycosylation of IgA1 is inherited in both pediatric IgA nephropathy and Henoch-Schönlein purpura nephritis. Kidney Int. 2011;80(1):79-87.
12. Magistroni R et al. New developments in the genetics, pathogenesis, and therapy of
IgA nephropathy. Kidney Int. 2015;88(5):974-89.
13. Boyd JK et al. An update on the pathogenesis and treatment of IgA nephropathy. Kidney Int. 2012;81(9):833-43.
14. Suzuki H, Novak J. IgA glycosylation and immune complex formation in IgAN. Semin Immunopathol. 2021;43(5):669-78.
15. Jandeleit-Dahm KA, Watson AM. The endothelin system and endothelin receptor antagonists. Curr Opin Nephrol Hypertens. 2012;21(1):66-71.
16. Tycová I et al. Molecular profiling in IgA nephropathy and focal and segmental glomerulosclerosis. Physiol Res. 2018;67(1):93-105.
17. Kohan DE et al. Targeting the endothelin A receptor in IgA nephropathy. Kidney Int Rep. 2023;8(11):2198-210.
18. Komers R, Plotkin H. Dual inhibition of renin-angiotensin-aldosterone system and endothelin-1 in treatment of chronic kidney disease. Am J Physiol Regul Integr Comp Physiol. 2016;310(10):R87784.
19. Trachtman H et al. Sparsentan. Dual angiotensin II AT1 receptor blocker and endothelin ETA receptor antagonist, treatment of focal segmental glomerulosclerosis, treatment of IgA nephropathy. Drugs Future. 2020;45(2):79-98.
20. Lin YJ et al. Angiotensin II enhances endothelin-1-induced vasoconstriction through upregulating endothelin type A receptor. Biochem Biophys Res Commun. 2014;451(2):263-9.
21. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4s):S1-276.
22. European Medicines Agency (EMA). Orphan designation for the treatment of primary IgA nephropathy. 2020. Available at: https://www.ema.europa.eu/ en/medicines/human/orphandesignations/eu-3-20-2345. Last accessed: 21 December 2023.
23. Travere Therapeutics. Travere therapeutics announces FDA accelerated approval of FILSPARI™ (sparsentan), the first and only non-immunosuppressive therapy for the reduction of
proteinuria in IgA nephropathy. 2023. Available at: https://www. globenewswire.com/en/newsrelease/2023/02/17/2610963/0/ en/Travere-TherapeuticsAnnounces-FDA-AcceleratedApproval-of-FILSPARI-sparsentanthe-First-and-Only-Nonimmunosuppressive-Therapy-forthe-Reduction-of-Proteinuriain-IgA-Nephropathy.html. Last accessed: 21 December 2023.
24. Travere Therapeutics, Inc. A study of the effect and safety of sparsentan in the treatment of patients with IgA nephropathy (PROTECT). NCT03762850. https://clinicaltrials.gov/study/ NCT03762850.
25. Travere Therapeutics. Filspari (sparsentan) prescribing information. Available at: https://www.accessdata. fda.gov/drugsatfda_docs/ label/2023/216403s000lbl.pdf. Last accessed: 21 December 2023.
26. European Medicines Agency (EMA). Irbesartan summary of product characteristics. Available at: https://www.ema.europa.eu/en/ documents/product-information/ irbesartan-teva-epar-productinformation_en.pdf. Last accessed: 21 December 2023.
27. Rovin BH et al. Efficacy and safety of sparsentan versus irbesartan in patients with IgA nephropathy (PROTECT): 2-year results from a randomised, activecontrolled, phase 3 trial. Lancet. 2023;402(10417):2077-90.
28. Rovin B et al. Pivotal results of the phase 3 PROTECT trial of sparsentan vs irbesartan in patients with immunoglobulin A nephropathy. Abstract FR-OR109. ASN Kidney Week 2-5 November, 2023.
29. Heerspink HJL et al. Sparsentan in patients with IgA nephropathy: a prespecified interim analysis from a randomised, double-blind, active-controlled clinical trial. Lancet. 2023;401(10388):1584-94.
30. Hendry B et al. Sparsentan receptor occupancy modeling, clinical actions, and safety. Abstract SA-PO276. ASN Kidney Week 2-5 November, 2023.
31. Nakamura T et al. Effect of a specific endothelin receptor A antagonist on glomerulonephritis of ddY mice with IgA nephropathy. Nephron. 1996;72(3):454-60.
32. King A et al. POS-378 Selective ETA antagonist atrasentan,
20 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Poster Review
rapidly reduces albuminuria and downregulates intra-renal pro-inflammatory and profibrotic transcriptional networks in the GDDY mouse model of spontaneous IgA nephropathy. Kidney Int Rep. 2021;6(4):S164.
33. Mann JF et al. Avosentan for overt diabetic nephropathy. J Am Soc Nephrol. 2010;21(3):527-35.
34. Navar LG et al. Renal responses to AT1 receptor blockade. Am J Hypertens. 2000;13(1 Pt 2):45s-54s.
35. Kowala MC et al. Novel dual
action AT1 and ETA receptor antagonists reduce blood pressure in experimental hypertension. J Pharmacol Exp Ther. 2004;309(1):275-84.
36. Cheung CK et al. Sparsentan as first-line treatment of incident patients with IgA nephropathy: Preliminary findings from the SPARTAN trial. Abstract SA-PO901. ASN Kidney Week 2–5 November, 2023.
37. University of Leicester; Travere Therapeutics, Inc. A study of the safety and activity of
sparsentan for the treatment of incident patients with immunoglobulin a nephropathy (SPARTAN). NCT04663204. https://clinicaltrials.gov/study/ NCT04663204.
38. Barratt J et al. Natural history of IgA nephropathy: analysis of a UK national RaDaR IgA nephropathy cohort. Abstract PO1577. ASN Kidney Week, 2-4 November, 2021.
39. Trachtman H. Emerging drugs for treatment of focal segmental glomerulosclerosis. Expert Opin Emerg Drugs. 2020;25(3):367-75.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 21 Poster Review FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Transitioning Patients From Second- to First-Line Prophylaxis in Hereditary Angioedema
Interviewees:
Padmalal Gurugama,1 David Launay2-5
1. Clinical Immunology and Allergy, Cambridge University Hospitals NHS Foundation Trust, UK
2. Institute for Translational Research in Inflammation, University of Lille, France
3. Institut national de la santé et de la recherche médicale (Inserm), Lille, France
4. Department of Internal Medicine and Immunology, Centre Hospitalier Universitaire (CHU) de Lille, France
5. National Reference Centre for Angioedema, Kinine (CREAK), Lille, France
Disclosure:
Acknowledgements:
Gurugama has received consultation fees from BioCryst and Kalvista Pharmaceuticals; and educational sponsorship from ALK, CSL, Pharming, and Takeda. Launay has received honoraria and meeting support from Behring, Biocryst, CSL, and Takeda.
Medical writing assistance provided by Caroline E. Cross, Reading, UK. Prescribing Information (PI) for BioCryst products mentioned in this article: Orladeyo▼ (berotralstat) can be found here. Always consult local prescribing information in country of practice as information may vary.
Disclaimer: The opinions expressed in this article belong solely to the named interviewees.
Support: The publication of this article was funded by BioCryst, who selected the interviewees and have reviewed the article.
Keywords:
Attenuated androgens (AA), berotralstat, guidelines, hereditary angioedema (HAE), long-term prophylaxis (LTP), quality of life (QoL), switching, transition.
Citation: EMJ. 2024;9[1]:22-27. DOI/10.33590/emj/10307646. https://doi.org/10.33590/emj/10307646.
Interview Summary
Modern targeted prophylaxis is recommended for patients with hereditary angioedema (HAE), but many remain on attenuated androgens. EMJ spoke to two HAE experts who explain how they help patients to make the switch.
INTRODUCTION
HAE is a rare genetic condition that affects approximately one in 50,000 people worldwide. Patients experience unpredictable episodes of cutaneous or submucosal oedema in different parts of the body, which can be life-threatening
when affecting the upper respiratory tract.1 Attacks can occur without warning, and can also be triggered by a variety of factors including stress, infections, injury, and surgery.1 The unpredictable periodicity and intensity of attacks can significantly impair individuals’ quality of life (QoL).1
22 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview
Most cases of HAE are caused by mutations in the SERPING1 gene that encodes the C1esterase inhibitor (C1-INH) protein.2 The mutations result in a reduction or dysfunction in C1-INH protein (HAE-C1-INH type 1 and HAEC1-INH type 2, respectively).2 Such mutations affect the kinin-kallikrein pathway and lead to overproduction of bradykinin, with increased vascular permeability and oedema.2
In the past decade, specific, targeted medicines for treatment of HAE attacks, and for longterm prophylaxis (LTP) to prevent attacks, have been licenced, and are now recommended in international guidelines.1 This follows decades when the only medicines available to treat HAE were non-specific compounds such as attenuated androgens (AA), which can cause debilitating side effects, and are unlicenced in many European countries.1,3
Recently available agents, including kallikrein inhibitors, such as oral berotralstat and subcutaneous lanadelumab, are transforming the way HAE can be managed, by making it possible for targeted prophylaxis to be the mainstay of their treatment.1 However, a significant proportion of patients throughout Europe and the USA are still prescribed AAs, which are not recommended as first-line prophylaxis in the guidelines.1,4-8
To find out why this is the case, and to understand what can be done to ensure more patients can access first-line prophylactics, EMJ interviewed David Launay, Department of Internal Medicine and Immunology, Hospital Centre, University of Lille, France; and Padmalal Gurugama, Clinical Immunology and Allergy, Cambridge University Hospitals NHS Foundation Trust, UK, who are both experts managing patients with HAE in specialist centres.
Both specialists are increasingly seeing patients with HAE who are keen to transition from AAs to kallikrein inhibitors. This article discusses the value of clear guidelines for treatment and management of HAE, and highlights the different approaches used to switch patients’ medications. It also provides insights that demonstrate a need for consensus among clinicians on how best to manage the transition away from AAs.
THE VALUE OF GUIDELINES FOR HEREDITARY ANGIOEDEMA MANAGEMENT
The 2021 International World Allergy Organization (WAO)/European Academy of Allergy and Clinical Immunology (EAACI) Guidelines for HAE management1 recommend long-term prophylaxis to reduce the risk of HAE attacks.1 Three medications are now licenced as firstline prophylactics: plasma-derived C1-INH and lanadelumab, which are administered subcutaneously biweekly; and berotralstat, which is an oral medication taken daily.1 Berotralstat and lanadelumab act by inhibiting the action of kallikrein by different mechanisms.1
“Prior to the guidelines,1 we were treating patients to control the number of attacks. Now the bar is set higher, and we aim to control attacks, and also to normalise their QoL. It is an important strategic change,” Launay explained.
Gurugama and Launay agree that the guidelines provide clear treatment algorithms that can be applied to all patients, in accordance with a medicine’s licencing.1 The guidelines give clinicians the confidence to talk to patients about how medication can reduce the overall burden of disease. “At all our clinics, we first ask patients to complete the Angioedema Control Test (AECT) and QoL questionnaires, recommended in the guidelines,”1 Launay said. It provides a robust way to check how well an individual’s disease is controlled, and is a good starting point for discussions about new medications.
The guidelines clearly state that AAs should only be used as second-line treatments, as they are non-specific, and have potential short- and long-term side effects,1 including an increased risk of comorbidities such as hypertension, hypercholesterolaemia, and diabetes.9 However, despite the recommendations for first-line targeted treatments, a significant number of existing patients with HAE across Europe are still being prescribed AAs.4-7 Gurugama and Launay agree that this is, at least partly, because AAs are less costly, and clinicians and patients are very familiar with these medicines. Gurugama said: “We have a cohort of more than 100 patients at our tertiary clinic, and many of them have been taking AAs for 20–30 years.” It can be difficult to convince people to change their medications.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 23 Interview
Both specialists find the guidelines helpful when starting conversations with their patients about newly licenced and recommended treatments. The evidence-based guidelines also provide a good basis for discussions with patients currently taking AAs, who might be encouraged to transition to first-line prophylaxis.
However, according to Gurugama, who has 30–40 patients who still take the AA danazol, there is reluctance from some patients to transition away from AAs, as their disease is relatively well controlled with danazol.
“Many patients who continue on AAs such as danazol are on relatively low doses, and do not experience tangible side-effects,” he explained. “Patients who still have attacks despite higher dose AAs are more open to a discussion about transitioning to first-line LTPs.”
An additional consideration for Gurugama is that, in the UK, prescribing practices are informed by the National Institute for Health and Care Excellence (NICE) guidelines.10 The NICE guidelines state that if a patient has two or more attacks per week, lanadelumab or C1-INH should be prescribed.10 If the patient has two or more attacks per month, berotralstat should be given.10 “However, these recommendations do not consider patients whose attacks are already being controlled with danazol,” Gurugama pointed out. This is also the case for the EAACI guidelines.1
Although all newly diagnosed patients receive first-line LTPs, according to Gurugama, there is an ongoing debate among some clinicians about the cost of newer targeted therapies versus attenuated androgens, which are relatively inexpensive, and can help to control attacks. This argument can be a barrier to moving patients onto firstline recommended treatments.
Launay believes the value of consensus guidelines goes beyond treatments. “The guidelines also remind us that we should talk to the patient about the overall burden of disease on their lives, rather than just the number of attacks,” he said. “This can help inform the best course of action in terms of prophylaxis,” Launay added.
CHOOSING FIRST-LINE LONG-TERM PROPHYLAXIS
There is good clinical evidence that first-line LTPs improve patient QoL.11,12 This aligns with Launay’s experience: “I see more and more patients asking for LTP because they know people with HAE that are on first-line LTPs who experience improved QoL, and they want to have that improvement in their QoL too.”
“We have several first-line LTP options, administered via different routes, and this is an advantage for patients, as they have a choice,” added Launay, who believes reducing anxiety through shared decision-making is an important part of managing HAE.
Gurugama described a recent case in their clinic. The individual was on danazol, but had not been to clinic for more than 2 years. Gurugama was able to inform the patient of new treatment options and, as a result, the individual is now transitioning to a first-line LTP.
Recent surveys of people with HAE indicate that many patients find their treatment burdensome, and would prefer to take medicines with a more convenient route of administration,13 and a majority would prefer to take an oral medication, rather than medicine administered via the intravenous or subcutaneous route.13 The convenience of an oral medication may be a factor in patients starting on LTPs.14
In Launay’s and Gurugama’s experience, the frequency of doses can also influence patient choice. “Some people are uncomfortable selfadministering a subcutaneous dose,” said Launay, but others prefer to accept the burden of injectable administration, because they can take the medicine biweekly or monthly, rather than daily, making them less likely to forget. “Others may be concerned that they will forget the treatment if it is taken only once a month, so prefer a daily oral treatment,” Launay added.
ATTENUATED ANDROGEN WITHDRAWAL STRATEGIES: WHAT WORKS?
Although international guidelines for HAE management make clear recommendations
24 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview
on first-line treatments and prophylaxis, they do not provide clear guidance for transitioning patients from second- to first-line prophylactic medications. This is a gap that Launay and Gurugama think could be filled with further studies and real-world data analysis, and this is starting to happen.15,16
A recent survey of 12 physicians, carried out alongside a review of the endocrine literature,15 highlighted a range of approaches to androgen withdrawal. The authors conclude that there is unlikely to be a ‘one size fits all’ approach that works in every case. Many factors, such as age, gender, and coexisting conditions, can affect how an individual will respond to androgen withdrawal, both in terms of increases in attack rate, and also other adverse effects such as fatigue and mood changes, including anxiety and depression.15
“We are constantly asking ourselves ‘what is the best strategy for transitioning patients from androgens to first-line LTPs?’,” Launay said. “It is an important question, because we have a lot of patients who are taking androgens.” Launay follows approximately 200 patients at his centre and, to date, approximately 20 have transitioned successfully from androgens to first-line LTPs.
Overlapping Androgens and First-Line Long-Term Prophylaxis Before Androgen Withdrawal
When a patient decides to transition away from AAs, Launay starts them on first-line LTP while they are still taking androgens: “The medicines are effective, but do not start to work immediately. In my experience, there is a period of time before we see an effect. After that time, if the patient’s disease is controlled, the androgens are withdrawn as quickly as possible.” (Figure 1A)
Launay accepts that there may be other strategies that are useful, but reiterates that this one works: “I have not seen side effects with this approach of overlapping the medications.”
In particular, Launay is concerned about the psychological impacts for patients of experiencing an increase in attacks during the transition, and wants to avoid this, where possible: “If I stop the androgen before, or on the day I start a new treatment, the patient can experience more attacks, and this may lead them to falsely conclude that the recently introduced treatment is not working.”
Tapering
Overlap
Tapering
Overlap
Androgens dose Washout Start first-line LTP
Tapering with washout period Tapering after initiation of firstline LTP
Androgens dose
LTP
of attacks but lower androgen withdrawal symptom risk
of attacks minimised and any androgen withdrawal symptoms are not interpreted as LTP side effects
Start first-line
Risk
Risk
Initiate first-line LTP while tapering
Androgens dose
attacks reduced, and any androgen withdrawal
are not
Overlap Start first-line LTP Risk of
symptoms
interpreted as LTP side effects
Androgens dose Washout Start first-line LTP
with washout period Tapering after initiation of firstline LTP Androgens dose
of attacks but lower androgen withdrawal symptom risk
of attacks minimised and any androgen withdrawal symptoms are not interpreted as LTP side effects
Start first-line LTP Risk
Risk
Initiate first-line LTP while tapering
Androgens dose
attacks reduced, and any androgen withdrawal symptoms are not
Overlap Start first-line LTP Risk of
interpreted as LTP side effects
Androgens dose Washout Start first-line LTP
with washout period Tapering after initiation of firstline LTP
Androgens dose
LTP
of attacks but lower androgen withdrawal symptom risk
of attacks minimised and any androgen withdrawal symptoms are not interpreted as LTP side
Overlap Start first-line
Risk
Risk
effects
Initiate first-line LTP while tapering
Androgens dose
LTP
reduced, and any androgen withdrawal
are
side effects
Overlap Start first-line
Risk of attacks
symptoms
not interpreted as LTP
LTP: long-term prophylaxis.
B
C Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 25 Interview
Figure 1: Possible options for transitioning to first-line long-term prophylaxis from androgens.
A
Tapered Androgen Withdrawal With or Without Overlap with First-Line Long-Term Prophylaxis
Many clinicians, including Gurugama, have concerns about withdrawing androgens rapidly.15 Gurugama, who has a cohort of 30–40 patients on low-dose danazol, recommends a tapered withdrawal of AAs over a 3–4 month period (Figure 1B), with close monitoring to check for adverse effects, such as liver function abnormalities.15 Gurugama discusses the treatment plan in detail with the patient in advance, and ensures they are aware that they may experience an increase in attacks, but that they will have access to on-demand treatment to control them as soon as they arise.
“It is important the patient is aware that they may have a temporary increase in the number of attacks as androgens are withdrawn,” Gurugama said. “Patients have a good picture of what might happen and have on-demand treatment at home to provide a safety net if they experience early signs of an attack.” He added: “If my patient was on 700 mg danazol a week, I would reduce the dose by 100 mg per week. I have not seen any adverse effects using this approach.”
Also, Gurugama said, patients know that HAE is a life-long condition, and the transition away from a medication that can cause long term side-effects is important. The period when they might experience an increase in symptoms is relatively short.
Gurugama agrees that there may be some occasions where overlap with a first-line prophylactic makes sense (Figure 1B and 1C). For example, if a patient is taking AAs and still has one or two attacks per month, overlapping with berotralstat should be considered. “We believe that berotralstat has no marked effect on liver function,” Gurugama continued, but it would be good to have clinical data for overlap with lowdose danazol.
ENCOURAGING MORE PEOPLE TO TRANSITION FROM SECOND- TO FIRST-LINE PROPHYLACTICS
The number of patients transitioning away from AAs is likely to increase dramatically in the short term, according to Launay. “Older patients are starting to get side-effects, cardiovascular
disease, and other comorbidities, which were not apparent when they were younger,” explained Launay.
However, some existing patients may not be eligible for first-line LTPs, particularly in the UK. Gurugama has observed that, in a few cases, patients in their 60s and 70s remain attack-free when androgens are withdrawn: “In these cases, we can only recommend on-demand treatment, as these patients don’t meet the criteria set by NICE for treatment with first-line LTPs.10 Like many colleagues, I would like to see the NICE guidelines changed so we can prescribe firstline LTPs to all patients, as and when they are needed, because if these older individuals do go on to have further attacks, they will likely want to go back onto danazol.”
There is clear evidence from clinical trials and real-world data that licenced LTPs are more efficacious and better tolerated than AAs,1,17 and this is reassuring for patients, encouraging them to switch treatments.
To help minimise anxiety during the transition, Launay’s patients are monitored with a monthly phone call and a 3-month follow-up visit. For Launay, this close monitoring and management of the patient is critical for successful transition: “During the first weeks, patients may experience side effects and attacks, so we need to reassure them that these will diminish. It is important for them to adhere to the treatment, both in short term and long term.”
CONCLUSION
Launay and Gurugama agree better guidelines are needed to give patients and clinicians more confidence on how to transition away from AAs. Different clinicians have different experiences and it is important these are shared across the clinical community.15 “The lack of consensus on how to transition can be a reason for clinicians to avoid switching patients from second- to firstline prophylactics, because they do not know how best to do this,” Launay said.
He went on to emphasise the point, saying: “Should we recommend withdrawal or overlap? If androgen tapering works, how long should it take? When and how do we stop? We need good data.”
26 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview
In addition, Launay believes guidelines that are specific for different treatments would be helpful. “It may be that a different transitioning strategy should be applied, depending on whether the patient is switching to oral or subcutaneous prophylactic medication,” Launay explained.
Gurugama agreed and concluded: “Clinicians want to provide long-term recommended prophylaxis to most of their patients. The medications are available, and we should be able to apply best practice strategies, and use them.”
Adverse events should be reported. Reporting forms and information for the United Kingdom can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to BioCryst UK Ltd on +44 (0)203 8850789 or email medinfoeurope@biocryst.com
References
1. Maurer M et al. The international WAO/EAACI guideline for the management of hereditary angioedema-the 2021 revision and update. Allergy. 2022;77(7):196190.
2. Santacroce R et al. The genetics of hereditary angioedema: a review. J Clin Med. 2021;10(9):2023.
3. Bork K et al. Benefits and risks of danazol in hereditary angioedema: a long-term survey of 118 patients. Ann Allergy Asthma Immunol. 2008;100(2):153-61.
4. Bouillet L et al. Long-term prophylaxis in hereditary angioedema management: current practices in France and unmet needs. Allergy Asthma Proc. 2022;43(5):406-12.
5. Van der Poorten MM et al. Hereditary angioedema (HAE) in Belgium: results from a national survey. Front Allergy. 2023;4:1143897.
6. Varandas C et al. Hereditary angioedema: 24 years of experience in a Portuguese reference center. Eur Ann Allergy Clin Immunol. 2022;DOI:10.23822/ EurAnnACI.1764-1489.278.
7. Yong PFK et al. A national survey of hereditary angioedema and acquired C1 inhibitor deficiency in the United Kingdom. J Allergy Clin Immunol Pract. 2023;11(8):247683.
8. Mendivil J et al. A multicenter chart review of patient characteristics, treatment, and outcomes in hereditary angioedema: unmet need for more effective long-term prophylaxis. Allergy Asthma Clin Immunol. 2023;19(1):48.
9. Zanichelli A. Comorbidities in angioedema due to C1-inhibitor deficiency: an Italian survey. J Allergy Clin Immunol Pract. 2024;S2213-2198(24)00003-5.
10. National Institute for Health and Care Excellence (NICE). Berotralstat for preventing recurrent attacks of hereditary angioedema. 2021. Available at: https://www.nice.org.uk/guidance/ ta738. Last accessed: 17 January 2024.
11. Lumry WR et al.; HELP Study Investigators. Impact of lanadelumab on health-related quality of life in patients with hereditary angioedema in the HELP study. Allergy. 2021;76(4):1188-98.
12. Johnson F et al. A retrospective
analysis of long-term prophylaxis with berotralstat in patients with hereditary angioedema and acquired C1-inhibitor deficiencyreal-world data. Clin Rev Allergy Immunol. 2023;65(3):354-64.
13. Radojicic C et al. Patient perspectives on the treatment burden of injectable medication for hereditary angioedema. Allergy Asthma Proc. 2021;42(3):S4-10.
14. Geba D et al. Hereditary angioedema patients would prefer newer-generation oral prophylaxis. J Drug Assess. 2021;10(1):51-6.
15. Johnston DT et al. Androgen use in hereditary angioedema: a critical appraisal and approaches to transitioning from androgens to other therapies. Allergy Asthma Proc. 2021;42(1):22-9.
16. Lumry WR et al. An expert panel’s review on patients with hereditary angioedema switching from attenuated androgens to oral prophylactic therapy. Allergy Asthma Proc. 2024;45(1):44-9.
17. Ahuja M et al. Berotralstat for the prophylaxis of hereditary angioedema - real-world evidence data from the United Kingdom. Allergy. 2023;78(5):1380-3.
EU.HAE.00018
Date of preparation: March 2024
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 27 Interview
Q1
Interviews
Emer Kelly, Fitriana Mawardi, and Kiley Whalen shared their perspectives on the importance of multidisciplinary healthcare, exploring its importance in disaster preparedness, COPD, and Ehlers–Danlos syndrome.

Emer Kelly
Respiratory Consultant and General Physician, St. Vincent’s University Hospital, Dublin, Ireland
Citation: EMJ. 2024;9[1]:28-30. DOI/10.33590/emj/11000035. https://doi.org/10.33590/emj/11000035.
What sparked your initial interest in respiratory health, and led you to pursue a career in this specialty?
I had asthma as a child, so I have experienced breathlessness firsthand. The real urgency of this symptom inspired me to understand it better, and to understand the diseases that cause it. The need to help patients with respiratory symptoms drives me every day.
Q2
Having trained in both Ireland and the USA, what do you believe you have gained from these experiences, and how have they filtered into your daily practice?
I have been privileged to work in these two health services. During my training in the USA, at the Harvard Pulmonary and Critical Care Fellowship, I had the opportunity to work in world-renowned centres, and see the expanding frontier of medical progress. It was also interesting to see the challenges of paying for this care. In Ireland, as in many European countries, we also face the challenge of meeting
healthcare needs in a more socialised medicine setting. In my daily practice, I am driven to have patients receive the healthcare they need, and to make sure this is valued in society.
Q3 Could you explain the impacts of a multidisciplinary approach to healthcare, and the benefits for both patients and physicians?
One of my favourite parts of my role in caring for patients with chronic obstructive pulmonary disorder (COPD), is working with the multidisciplinary team to reach this goal. Patients value the holistic approach greatly, and I think the doctor often plays a more minor role in the care. I continue to learn from the nurses, physiotherapists, and other members of the team on a daily basis. I think the strength of this approach is best seen in the pulmonary rehabilitation setting. This is a highlight in my work. As physicians, we are often the person a patient needs when they are very unwell, but it is so great to be involved in keeping a patient as well as they can be, instead of waiting for a crisis.
Interview
28 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
"It is so great to be involved in keeping a patient as well as they can be, instead of waiting for a crisis."
Q4
What were the key takeaways from your recent publication, ‘Caring for Patients with Advanced COPD: Beyond the Inhalers’?
This was a review article to summarise the multifaceted approach to help patients with advanced COPD. Key points of this paper included that O2 therapy reduces mortality in patients with COPD with severe hypoxaemic respiratory failure; non-invasive ventilation is of benefit in some patients, as it can improve admission-free survival in stable hypercapnic patients, or persistently hypercapnic patients post-acute exacerbation of COPD; and physiotherapy and rehabilitation approaches can address dyspnoea management, and improve exercise tolerance. Furthermore, consideration of lung volume reduction via surgical or bronchoscopic approaches is appropriate for patients within set criteria; lung transplantation assessment is appropriate for a subgroup of patients, although mortality benefit is not demonstrated; and symptom management with a palliative approach can run alongside the other treatments.
Q5
What do you believe is the most significant reasoning behind the importance of multidisciplinary care for COPD, and how has this research been received upon implementation into practice?
I think it is the recognition that our drugs and medical therapies are only part of the solution to optimal care, and that engaging with each individual patient, and understanding their individual needs, is paramount. Even when we have effective therapies, the coaching on how to take the medication, techniques on using inhalers, and confidence that the medication is right for them, come from an effective multidisciplinary team approach. The multifaceted approach also helps to address symptoms in daily life.
I have received positive feedback in relation to this article, and it has served as a valuable resource to those involved in COPD care. It has also served to improve collaboration with others who are researching within this field. On a practical level, it has helped us to establish pathways for referral for lung volume reduction interventions and transplant on a local level.
The focus on palliative care has led to collaborations with community-, hospital-, and hospice-based services. We were a major recruiting centre for the BETTER-B trial,

Interview
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 29
partnering with the Cicely Saunders Institute at King’s College Hospital, London, UK, which was a randomised controlled trial investigating the use of mirtazapine for dyspnoea in advanced lung disease. Randomised controlled trials are not very common in palliative care, and the clinical/ symptom need would argue for more such trials. Setting up our COPD patient registry puts us in a better position to have patients with COPD help to push forward progress in their disease.
Q6
Looking to the future, where can we expect to see your research focuses lie in the coming years?
I think there is great hope for the future care of patients with COPD. There are areas for further research and service development within advanced COPD. More widespread support for O2 therapy and non-invasive ventilation follow-up care may help with appropriate prescription and therapy compliance, to optimise this expensive resource for each patient. Studies are needed to clarify which patient cohorts may benefit from referral to transplant, rather than lung volume reduction options. Within the area of lung transplant, work continues on donor organ preservation methods and reconditioning of lungs, and a more focused approach is now being adopted with respect to the area of personalised medicine in immunosuppression treatments. Results are to come through from ongoing trials in the area of pharmacological management of dyspnoea. It has been exciting to be involved in trials in palliating the symptom of dyspnoea. Ongoing collaboration with palliative care colleagues, in combination with further training in this skillset for pulmonary specialists, is likely to improve symptom management care for these patients.
Q7
As an eLearning Resources Director of the European Respiratory Society (ERS), what do you believe are the benefits eLearning can provide to clinical care?
I think eLearning can remove barriers to further learning in many settings. At the ERS, we are a European society with a global outlook. The expansion of online resources, and support for lower- and middle-income nations to have access to learning resources, will hopefully empower physicians working all over the world to optimally manage their respiratory patients within the resources available, and to fight to improve these resources.
"At the ERS, we are a European society with a global outlook."
Barriers to learning can exist in many other settings. Healthcare workers with busy lives professionally and at home are now able to access up-to-the-minute resources on their terms, and on their schedule. It has been a great privilege to work with my ERS colleagues to push this forward over the last few years.
Q8
Are there any innovations in the field of respiratory health that you are particularly excited to see translated into practice?
I am excited to see patients with COPD moving into the spotlight, in terms of clinical trials and innovations. This patient group has not been prioritised enough over the years. I have enjoyed working with my wonderful patients in setting up a research registry, and am motivated by their willingness to participate, and move things forward for themselves, and for other patients, into the future. ●
Interview
30 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0

Fitriana Mawardi
Director of Health Clinic, Red Cross Indonesia of Yogyakarta; Executive Manager, Community and Family Healthcare with Inter-Professional Education (CFHC-IPE) Department, Yogyakarta; Member, The Network: Towards Unity for Health (TUFH); Member, World Organization of Family Doctors (WONCA); Family Physician, Junior Lecturer in Faculty of Medicine, Public Health and Nursing, Gadjah Mada University, Yogyakarta, Java, Indonesia
EMJ. 2024;9[1]:31-34. DOI/10.33590/emj/10302931.
Q1Citation:
https://doi.org/10.33590/emj/10302931.
Could you begin by telling us what attracted you to specialise in family medicine and primary healthcare?
I am interested in family medicine and primary healthcare because primary healthcare is the first gatekeeper in the community. Primary healthcare ensures that people receive quality, comprehensive care, ranging from promotion and prevention, to treatment, rehabilitation, and palliative care, which takes place as closely as is feasible to people’s everyday environment.
Primary healthcare is the most inclusive, equitable, cost-effective, and efficient approach to enhance people’s physical and mental health, as well as their social wellbeing.
The main role of primary healthcare is to provide continuous and comprehensive care to the patients. The patient can also be made aware of various social welfare and public health services initiated by the concerned governing bodies, and other organisations. The other major role of a primary healthcare centre is to offer quality health and social services to underprivileged sections of society. As for the benefits to community members, primary healthcare offers the first point of professional care to patients, by incorporating a proactive approach that utilises several preventative measures, manages chronic disease, and promotes self-care. Primary healthcare also provides increased accessibility to advanced healthcare within the community, which results in excellent health outcomes, and prevents delays.
Furthermore, family physicians play a crucial role in various aspects of healthcare. We are often the primary providers of early diagnosis and pharmacotherapy in the care and management of patients, and we provide ongoing comprehensive care, manage treatment-related side effects, and offer follow-up care. Family physicians can strengthen primary healthcare by providing skilled primary care, supporting ongoing training for other healthcare providers, developing relationships with specialists, and engaging communities as partners in healthcare delivery. The comprehensive role of this specialty attracted me to pursuing a specialisation in family medicine and primary healthcare.
Q2Your research is largely focused on the importance of collaborative approaches in primary healthcare and family healthcare. Could you tell our readers about the effects of a multidisciplinary model on patient outcomes?
Collaboration-based care will help to achieve the triple aims of healthcare: better patient experience, better health outcomes, and lower costs. Health workers are expected to provide services that can deal with the complexity of health issues, eliminate fragmentation, and collaborate to meet health needs. The primary care multidisciplinary approach appears to lead to lower healthcare utilisation, reduced sick leave, improved depression, increased social activity, reduced medication use, and reduced disability. We believe that multidisciplinary research in primary care should build on
Interview
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 31
"Health services based on interprofessional collaboration among health service providers are essential to deal with complex health problems."
this already established model of clinical teamwork, and should seek to include the full range of healthcare workers delivering primary care services. Involvement of patients in a multidisciplinary research team, as opposed to just being subjects in research, is a concept that is starting to be recognised as very important.
The Institute of Medicine (IOM), which was founded in 1970 under the charter of the National Academy of Sciences (NAS) in the USA to address the concerns of medicine and healthcare, recommends that all health workers collaborate when conducting the management of a patient. Interprofessional collaborative practice (IPCP) occurs when two or more health workers learn from each other, to improve collaboration and service quality. It is hoped that health workers will realise that practical co-operation can improve the quality of health services. The World Health Organization (WHO) realises that IPCP is an innovative strategy, which plays a vital role in dealing with global health problems. IPCP is considered capable of strengthening the health system, and improving the quality of health services. Health workers are expected to be able to have IPCP competencies to be implemented in providing health services.
Q3Have you been confronted with any challenges or misconceptions towards the multidisciplinary model, and could you explain the rationale behind these?
Health services based on interprofessional collaboration among health service providers are essential to deal with complex health problems. However, this is in contrast to the reality in the field, especially within primary health services, where the difficulty of access to health management in a collaborative, interprofessional manner is one of the shortcomings in terms of service support in primary health.
For example, in Indonesia, through the Ministry of Health, several steps have been implemented in primary services to improve the health of the elderly, including the Elderly Friendly Health
Center in all primary healthcare in Indonesia; the Elderly Empowerment Programme; and the Plenary Assessment of Geriatric Patients (P3G). The Elderly Friendly Health Center is a primary healthcare centre, with health workers who have knowledge and training in geriatrics, and who have the infrastructure to accommodate the needs of the elderly. The Elderly Empowerment Programme is a programme that aims to empower the elderly to be able to improve their family health status, so that the potential for them to be able to work and be efficient can be optimised. P3G is an interdisciplinary diagnostic process to determine problems in elderly patients. Geriatrics evaluations and assessment, in terms of the collaboration of health workers, are still not implemented, especially in primary health services.
Some studies also show that the challenges of multidisciplinary care in primary care include a deficit of content and practice in primary care training, variations in training between courses and universities, and the need for permanent education actions and meetings in daily work. Other challenges include inadequate staffing, insufficient education, the lack of financial compensation, low motivation, and lack of time. The implementation of care pathways in primary care also faces barriers, including inadequate staffing, insufficient education, lack of financial compensation, low motivation, and lack of time; and facilitators, including adequate skills and knowledge through training activities for health professionals, and good multidisciplinary communication.
Q4You are a member of The Network: Towards Unity for Health (TUFH) and the World Organization of Family Doctors (WONCA), both of which advocate for equitable global health. Could you explain the impact of these organisations, and the work that they are doing to achieve this mission?
TUFH brings together a diversity of thought, experience, and technical/financial resources. Members of TUFH include various healthcare
Interview
32 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
providers, so our members can challenge the status quo, push boundaries, learn from others (mentors), launch healthy vibrant initiatives, and then share best practices and learnings, on a local, regional, and global scale. The TUFH community is an interprofessional, multicultural, and global hub on social accountability. TUFH is open to all institutions and individuals who have a passion for global equitable health. The TUFH conduct routine events, such as symposiums, workshops, and international conference-related collaborative practice.
The mission of WONCA is to improve the quality of life of all people of the world, through defining and promoting its values, including respect for universal human rights and gender equity, and by fostering high standards of care in general practice and family medicine. To achieve their mission, WONCA promote personal, comprehensive, and continuing care for the individual and the family in the context of the community and society; promote equity through the equitable treatment, inclusion, and meaningful advancement of all groups of people, particularly females and girls, in the context of all healthcare and other societal initiatives; encourage and support the development of academic organisations of general practitioners
and family physicians; provide a forum for the exchange of knowledge and information between member organisations, general practitioners, and family physicians; and represent the policies and the educational, research, and service provision activities of general practitioners and family physicians to other world organisations and forums concerned with health and medical care.
WONCA represents, and acts as an advocate for, its constituent members at an international level, where it interacts with world bodies such as the WHO, with whom it has official relations as a non-governmental organisation, and is engaged in a number of collaborative projects.
WONCA also give the award for the family doctor across the world through the Montegut Global Scholar Award. The Montegut Global Scholars Program was established by the American Board of Family Medicine Foundation (ABFM-F) in 2010. The ABFM is a member of the American Board of Medical Specialties (ABMS), and the ABFM-F is a supporting organisation of the ABFM. Its primary mission is to support the ABFM’s research and scholarly activities. I was one of the awardees of the Montegut Global Scholars Program in 2019, and presented my awardee speech at the WONCA Asia Pacific Regional Conference in Kyoto, Japan.
"It is important for communities and all global partners to be more prepared by taking action before disasters occur."

Interview
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 33
Q5
You co-authored a paper in 2020 entitled ‘Strengthening Primary Health Care: Emergency and Disaster Preparedness in Community with Multidisciplinary Approach’. Could you give an overview of the main findings of this paper?
The increasing number of disasters and communities affected, coupled with the threats from climate change, has drawn not only national but also international attention to the risks of disasters, and what can be done about them. Therefore, it is important for communities and all global partners to be more prepared by taking action before disasters occur through disaster risk reduction, including the efforts of emergency preparedness, as well as through disaster response and recovery. To meet the emergency public health needs in any population, there is no other option than strengthening the primary health care system. For this goal, practitioners from various professions can work together, and share an affinity in synthesising knowledge and bridging gaps across functional areas. These include the disaster risk assessment and preparedness, involving several disciplines, for limiting human and material damage. This primary healthcare strategy, with a multidisciplinary approach, is the best possible method in developing improved approaches for disaster risk reduction and emergency preparedness, by improving health emergency management plans and protocols.
Q6
How do you believe the multidisciplinary approach outlined in your paper contributes to enhancing emergency and disaster preparedness in community healthcare settings?
In this study, we show that the integration of disaster management in primary healthcare
is needed, by making it an essential part of the disaster response system. It is vital to start providing disaster management training for primary healthcare staff, and to develop a comprehensive, as well as co-ordinated, approach with all other sectors. In this paper, we show the importance of primary healthcare in disaster preparedness.
Q7
Given the evolving nature of healthcare and emergencies, do you foresee any updates or revisions to the strategies outlined in your paper, and if yes, what aspects might need further exploration?
Based on our study, the aspect that needs further exploration is the competencies of primary healthcare related to disaster preparedness. The listed competencies for first-level healthcare providers can be broadly categorised into three domains: disaster and emergency preparedness, early warning, and response system; patient care and mass casualty management; and resource (human and material) management and eviction. The implementation of collaborative practice in disaster preparedness need to be implemented in primary healthcare.
Q8
As a researcher and practitioner in the field of family medicine and primary care, where do you see your focus lie in the coming years?
In the future, my focuses are related to emergency and disaster preparedness, especially for vulnerable groups including the elderly, children, and pregnant people. ●

Interview
34 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0

Kiley Whalen
Physician Assistant, Adirondack Rehabilitation Medicine; Master of Science in Physician Assistant Studies at the Center for Physician Assistant Studies, Albany Medical College; Previous Restorative Justice in Academic Medicine (RJAM) Facilitator, Albany Medical College, New York, USA
Citation: EMJ. 2024;9[1]:35-37. DOI/10.33590/emj/10309888. https://doi.org/10.33590/emj/10309888.
Q1What sparked your initial interest in healthcare, and led you to pursue a career focused on rehabilitation and Ehlers–Danlos syndrome (EDS)?
I became interested in healthcare at a very young age. I saw it as the perfect marriage between science, art, and, most importantly, the ability to help improve the lives of others. My earliest exposure was as a hospital volunteer at the age of 13. As time went on, my interest and involvement in healthcare increased. This allowed me to spend time as a junior emergency medicine technician, pharmacy technician, medical assistant, and reproductive health educator on a volunteer trip in Uganda.
My interest in EDS started shortly after I was diagnosed with the syndrome in high school. This is what I attribute to allowing me to find my true passion for healthcare. I was able to see, on a very personal level, what a difference good healthcare can make in the lives of patients.
I chose to focus my career on rehabilitation, because its philosophy is about improving the quality of life of others. I think that, in a lot of cases, society is hyperfocused on curing disease, which is, of course, important; however, I would argue that working with patients to improve their quality of life, even when we cannot ‘cure’ them, is equally important. Rehabilitation also allows me to spend time treating others with EDS and other hypermobility syndromes, along with various other disorders.
Q2As a physician assistant, you are directly exposed to the direct impacts of chronic illnesses when caring for patients. Could you tell us about the benefits of employing a multidisciplinary approach in your field, and how this has impacted patients?
I truly believe that the best outcomes for patients are achieved when a multidisciplinary approach is used. Ideally, you have a team of physicians, occupational therapists, physical therapists, nurses, social workers, pharmacists, and mental health providers, and, if your country has them, providers such as nurse practitioners or physician assistants and associates. This team works together to ensure patients have the best care. Not all facilities have access to this; for example, in my case, I often have to take the time out of my day to contact a patient’s other healthcare providers and therapists to discuss their observations and plans. My patients often do best when we have multiple providers providing input regarding treatment plans. Simply put, more minds are better than one.
"I truly believe that the best outcomes for patients are achieved when a multidisciplinary approach is used."
With regard to patients with EDS and rehabilitation, I am often referring them to physical therapy, occupational therapy, behavioural therapy to assist with coping and pain management techniques, and working with pharmacists for medication management. All of these different approaches tend to have a synergistic effect together.
Interview
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 35
Q3
Regarding your recent publication, ‘Multidisciplinary Approach to Treating Chronic Pain in Patients with Ehlers–Danlos Syndrome: Critically Appraised Topic’, could you explain what led you to write this piece?
As discussed above, I have a personal tie to EDS. I remember being frustrated at the lack of research and recommendations for the syndrome. Often, I would see papers recommending the use of a multidisciplinary approach in treating the disorder, but there was not a good definition of what a multidisciplinary approach was. I had hoped to be able to come up with a better definition of what a multidisciplinary approach was within this paper. While more research is certainly needed, I will continue to focus my research in this area.
Q4 What do you believe is the most significant reasoning behind the importance of multidisciplinary care in EDS?
Because the pathology of pain in EDS is not well established, we lack targeted treatment for pain in the disorder. Unfortunately, this can mean that one single treatment may not be effective, and often, it requires the use of various modalities to treat the pain. Because of this, various approaches need to be taken, such as physical therapies, occupational therapies, assistive devices, medications, and cognitive behavioural therapy. These can all be useful, and work best when used in conjunction with one another.
"Because the pathology of pain in EDS is not well established, we lack targeted treatment for pain in the disorder."
Q5 Since publication, how has your research been received, and have you observed implementation of the research within clinical practice?
I believe the research has been well received. I have personally used the research within my own clinical practice. I hope that, as time goes on, more people will devote their time to studying EDS and hypermobility syndromes. There is still so much to learn about the disorders. We truly have only see the tip of the iceberg when it comes to these disorders.
Q6 Have there been any challenges to the implementation of the multidisciplinary approach in your field, and how have these been overcome?
Time is a large constraint. Healthcare in the USA, as I am sure is the case in many other parts of the world, is strained. Patients often have long waiting times, and providers are often pressured to see people in a short amount of time, due to both financial reasons, and in an effort to reduce waiting times for patients. Having good support staff to assist in decreasing provider burden, to allow them to spend time conversing with other

Interview
36 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0

"Movement from a hierarchical healthcare system with physicians at the head of the system, to a collaborative one, is already occurring."
providers, and allowing them to spend more time with patients, is huge.
Movement from a hierarchical healthcare system with physicians at the head of the system, to a collaborative one, is already occurring, and I believe it will only improve care. Each specialty and provider has a unique perspective and role. The more easily different providers can communicate, the better patient outcomes will be. Electronic medical records have helped with this, but they are far from perfect. Often, nothing can replace a phone call or, in an ideal world, inperson discussions with other providers.
Access to care is a significant issue. Many of my patients must dictate their care based on insurance coverage and cost. Waiting times and distance to specialists can both be issues to access. In my patients with mobility issues, which is a significant portion of the patients I treat as a rehabilitation provider, leaving the house can be difficult, let alone getting to medical appointments. These are complex issues, which I will not pretend to have all of the answers to.
Q7 You have a special interest in Restorative Justice in Academic Medicine. Could you explain the mission behind this programme, and its importance in the field of healthcare?
Restorative Justice in Academic Medicine helps to improve communication and engagement among healthcare providers, students, and
educators to discuss difficult topics. It was developed and modelled after First Nation restorative justice practices. It allows participants to have open discussions, and to brainstorm ways to improve society and our communities in direct ways, instead of alienating others who may not hold the same perspective or opinion about a topic. It allows participants to discuss difficult topics openly and without judgement, and to reach common ground and goals. It is my hope that more medical schools and medical institutions implement restorative justice practices to bring their communities together for the common good. Some examples of discussion topics I have had the privilege to facilitate and partake in have included healthcare and disability, intersex healthcare, and social determinants of health, among many others.
Q8
Looking to the future, is there a direction you intend to focus your subsequent research efforts in?
I would love to be able to further expand my research on EDS, and as genetic research improves, there will be more targeted treatments for EDS. The opportunity to partake in clinical research and/or case studies would be very exciting to me. I think right now is such an exciting time to research EDS, given current medical advancements. ●
Interview
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 37
Reviewing Advances in Bone Health
The Bone Health Forum
The Bone Health Forum is a sponsored standalone event that unites top experts from the JAPAC region.
Three osteoporosis experts each presented recent publications providing:
1.
New insights and novel approaches in bone health
2.
Real-world evidence and clinical insights
3.
Insights from basic and translational researchin special populations
1. Advances in Osteoporosis Management:
Peter Ebeling, Monash University, Melbourne, Australia
Antagonising microRNA-19a/b augments action and restores bone mass in osteoporosis
• Anti-microRNA-19a/b may enhance drug efficacy, as a novel osteoporosis therapy by promoting and reducing resorption
WNT modulating gene silencers as a gene osteoporosis, bone fracture, and critical bone defects2
• Bone-targeted adeno-associated viruses deliver and/or sclerostin to osteoblast cells, enhancing WNT/β-catenin signalling
• Potential treatment for osteoporosis, bone critical-sized bone defects
2. Real-world Management of Osteoporosis: Latest Evidence and Clinical Insights
Hua Yue, Shanghai Jiao Tong University School
Effects of zoledronate on bone mineral bone turnover after long-term denosumab observations in a real-world setting5
• Rebound bone loss plateaus after 4–6 years treatment, regardless of subsequent zoledronate therapy frequency
Baseline serum P1NP level is associated increase in hip BMD seen with romosozumab in previously untreated females with osteoporosis
• A baseline P1NP level of >53.7 µg/L is associated increased hip BMD following romosozumab
Economic evaluation of four treatment postmenopausal patients with osteoporosis fracture in mainland China: a cost-effectiveness
• Among patients who are postmenopausal a recent fracture, stratified treatment based more cost-effective than conventional pills
References:
1. Taipaleenmäki H et al. Antagonizing microRNA-19a/b augments PTH anabolic action and restores bone mass in osteoporosis in mice. EMBO Mol Med. 2022;14(11):e13617.
2. Oh W-T et al. WNT-modulating gene silencers as a gene therapy for osteoporosis, bone fracture, and critical-sized bone defects. Mol Ther. 2023;31(2):435-53.
3. Kim J et al. UBAP2 plays a role in bone homeostasis through the regulation of osteoblastogenesis and osteoclastogenesis. Nat Commun. 2023;14(1):3668.
4. Liang H et al. Relationships between sclerostin and morphometric vertebral fractures, bone mineral density, and bone microarchitecture in postmenopausal women. Arch Osteoporos. 2023;18(1):57.
5. Everts-Graber J et al. Effects of zoledronate on bone mineral density and bone turnover after long-term denosumab therapy: observations in a real-world setting. Bone. 2022;163:116498.
6. Kashii M et al. Baseline serum PINP level is associated with the increase in hip bone mineral density seen with romosozumab treatment in previously untreated women with osteoporosis. 2023;34(3):563-72.
7. Tian L et al. Economic evaluation of four treatment strategies for postmenopausal patients with osteoporosis and a recent fracture in mainland China: a cost-effectiveness analysis. Arch Osteoporos.
8. Eastell R et al. Diabetes mellitus and the benefit of antiresorptive therapy on fracture risk. J Bone Miner Res. 2022;37(11):2121-31.
9. Saito T et al. One-year romosozumab treatment followed by one-year denosumab treatment for osteoporosis in patients on hemodialysis: an observational study. Calcif Tissue Int. 2023;112(1):34-44.
10. Agarwal S et al. Teriparatide followed by denosumab in premenopausal idiopathic osteoporosis: bone microstructure and strength by HR-pQCT. J Bone Miner Res. 2023;38(1):35-47.
Key: BMD: bone mineral density; BHF: Bone Health Forum; CKD: chronic kidney disease; DPP-4: dipeptidyl-peptidase 4; HR-pQCT: high-resolution peripheral quantitative CT; JAPAC: Japan and Asia-Pacific; thyroid hormone; P1NP: procollagen type 1 N propeptide; RNA: ribose nucleic acid; SHN3: Schnurri-3; UBAP2: ubiquitin-associated protein 2; WNT: wingless and Int-1.
The publication of this infographic was supported by Amgen.
Citation: EMJ. 2024;9[1]:38-39. DOI/10.33590/emj/10305848. https://doi.org/10.33590/emj/10305848.
Management: Insights from Recent Basic and Translational Research
Australia
augments PTH anabolic osteoporosis mice1
efficacy, or serve promoting bone formation
gene therapy for critical sized deliver SHN3 enhancing fracture healing, and
Osteoporosis:
School of Medicine, China
density and denosumab therapy:
years of denosumab zoledronate with the romosozumab treatment osteoporosis 6
associated with ≥3% romosozumab treatment
strategies for osteoporosis and a recent cost-effectiveness analysis7
and osteoporotic with based on fracture risk is
2023;18(1):57.
Osteoporos Int.
Osteoporos. 2023;18(1):100.
2023;112(1):34-44.
UBAP2 plays a role in bone homeostasis through the regulation of osteoblastogenesis and osteoclastgenesis3
• Newly identified gene, UBAP2, regulates bone remodelling
• Serum UBAP2 levels may aid osteoporosis diagnosis
Relationships between sclerostin and morphometric vertebral fractures, bone mineral density, and bone microarchitecture in postmenopausal females4
• High serum sclerostin levels in postmenopausal females were paradoxically linked to improved bone microarchitecture, BMD, and bone strength
• No association between serum sclerostin and the prevalence of morphometric vertebral fractures
3. Bone Health in Special Populations: New Insights and Novel Approaches
Toshio Matsumoto, Tokushima University, Japan
Diabetes and the benefits of antiresorptive therapy on fracture risk8
• Denosumab:
1) Improves insulin sensitivity by reducing inflammatory cytokines and DPP-4
2) Reduces the incidence of Type 2 diabetes in patients with osteoporosis in line with other antiresorptive treatments
One-year romosozumab treatment followed by 1-year denosumab treatment for osteoporosis in patients on haemodialysis: an observational study9
• Romosozumab followed by denosumab effectively increases BMD in patients with CKD without dose adjustment
Teriparatide followed by denosumab in premenopausal idiopathic osteoporosis: bone microstructure and strength by HR-pQCT 10
• Teriparatide followed by denosumab enhances trabecular microstructure, increases cortical area, and improves bone strength, but raises cortical porosity
• The BHF had ~100 live attendees, with content available on demand via the BHF platform; this was a unique moment to share some of the recent advances in bone health
• 100% of attendees strongly agreed that the meeting will impact their clinical practice*
Information Asia-Pacific; PTH: para-
Meeting
Footnote: * Data on file Click here to download
Patients’ Preferences for Models of Follow-Up Care During or After Initial Cancer Treatment in Greece: Development of the Qualitative Phase, and Protocol for a Discrete Choice Experiment
Editor's Pick
This article outlines a study protocol to investigate patient preferences for posttreatment care models for survivors of cancer in Greece. Follow-up care models are an essential part of the patient’s journey, and provide a support network, as well as offering a way to assess the safety and effectiveness of treatments, and to monitor signs of recurrence or metastasis. Here, the authors provide valuable patient insights, as well as outlining the protocol for future dissemination into practice.
Prof Lászlo Vécsei Head of Neuroscience Research Group, Department of Neurology, University of Szeged, Hungary
Authors:

*Eugena Stamuli,1 Maria Papageorgiou,2 Varvara Baroutsou3
1. HES Choices, Athens, Greece
2. K.E.F.I. Cancer Patients Association, Athens, Greece
3. Consultant in Internal Medicine & Pharmaceutical Medicine, Athens, Greece
*Correspondence to eugena.stamuli@heschoices.com
Disclosure: The authors have declared no conflicts of interest. The study received approval from the Governing Committee of the KEFI Association, and adheres to its internal ethical guidelines. All participants will receive comprehensive study information through a participant information section of the survey. They will be explicitly asked for their informed consent to participate in the research.
Acknowledgements: The authors extend heartfelt thanks to the members of the KEFI association's management team for their valuable support and contributions to this study. We are particularly grateful to Zoe Grammatoglou and Elisavet Psilopoulou for their insightful comments, support, and direction, which significantly enhanced the study's design and quality.
Received: 03.11.23
Accepted: 05.02.24
Keywords: Cancer care models, cancer survivors, discrete choice experiment, Greece, patient preferences.
Citation: EMJ. 2024;[9]1:40-50. DOI/10.33590/emj/10307189. https://doi.org/10.33590/emj/10307189.
40 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Abstract
Cancer survivors face a range of physical symptoms, emotional and practical difficulties, and late and long-term effects of treatment. Follow-up care aims to monitor the effectiveness and safety of treatments, and detect recurrence or metastasis. However, survivorship care extends beyond clinical aspects, and should include all forms of necessary support, such as psychological, informational, and practical assistance. The European Cancer Patient's Bill of Rights emphasises patient-centred care, and the right to access information, receive personalised care, participate in decision-making, and receive psychological and social support. There are national plans for cancer care in place in Greece, and it is essential to acknowledge patient preferences and the acceptability of emerging plans for the ever-expanding population of survivors of cancer.
A discrete choice experiment (DCE) will be conducted to identify and quantify the preferences of Greek patients with cancer towards a care model that reflects the current state of cancer care, while also providing valuable insights into what patients consider important. By understanding patients' preferences, the study aims to identify areas for improvement, and contribute to the development of more patient-centred care models in Greece. This study will mark the first systematic measurement and quantification of preferences of patients with cancer in the Greek context.
This paper presents the development of the qualitative phase of the DCE, which focused on identifying the characteristics that are both important and relevant to patients with cancer. Further, it outlines the protocol for the subsequent stages of the study, which involve the DCE experimental design, the data collection, and analysis and dissemination of the findings.
Key Points
1. This study will explore cancer survivor preferences in Greece, informing patient-centred care models and policy decisions for improving post-treatment support.
2. A discrete choice experiment is in development to identify preferences of patients with cancer for follow-up care models, offering insights important for enhancing survivorship care in Greece.
3. Health policymakers and clinicians must recognise the importance of patient preferences in survivorship care. Tailoring follow-up models to align with patient needs and preferences can optimise outcomes and promote patient-centred cancer care.
INTRODUCTION
After being diagnosed with cancer, patients embark on a journey that involves ongoing treatments, and regular visits to healthcare providers. During the initial treatment, and following its completion, the main focus of follow-up care is to monitor the effectiveness and safety of the treatments received, and to detect any recurrence or metastasis of the disease.1 Survivors of cancer, whether
considered disease-free or not, often experience late and long-term effects of treatment, a range of physical symptoms, and emotional and practical difficulties.2 Hence, it is widely recognised that care models for survivors of cancer should extend beyond the clinical aspects of care, and include all forms of necessary support, such as psychological, informational, and practical assistance to patients, with a focus on their overall experience and outcomes.3
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 41 Article
According to the European Society for Medical Oncology (ESMO)’s patient guide on survivorship,4 survivorship care encompasses the health and physical, psychological, social, and economic issues that affect people after initial cancer treatment has ended. Survivorship care includes issues related to aftercare; managing delayed side effects of treatment; improving quality of life; and psychological and emotional health. The objective of aftercare is to improve the survival, manage physical symptoms and psychosocial effects, and enhance the quality of life for cancer survivors.
As early as 2014, the European Cancer Patient’s Bill of Rights was published5 by the European Cancer Concord (ECC), a coalition of cancer organisations, patient groups, and healthcare professionals. The Bill of Rights outlines a comprehensive set of fundamental rights that aim to highlight the importance of patient-centred care, and to encourage healthcare providers and policymakers to prioritise the needs and rights of patients with cancer. It includes the right to access information about their diagnosis, treatment, and follow-up care; the right to receive personalised care, and to participate in decision-making about their treatment; the right to be treated by a multidisciplinary team of healthcare professionals; and the right to receive psychological and social support.
The rights of patients with cancer, as described above, have been endorsed by organisations across Europe, such as cancer organisations, patient groups, healthcare professional associations, and governments, including the Greek government. National plans to tackle issues of cancer care are in place in Greece.6,7 As the field of cancer care continues to evolve in Greece, it is crucial to acknowledge the significance of patient preferences, and to consider the acceptability of emerging plans of follow-up care for the expanding population of survivors of cancer. It is essential to ensure that any plans for cancer care align with patients’ preferences, needs, and lifestyles, to promote optimal adherence and outcomes.
This paper presents the qualitative phase, and the protocol for the subsequent stages of a DCE that will be conducted with the aim to identify the preferences of Greek patients with cancer regarding a cancer care model’s
key characteristics. To the best of the authors’ knowledge, this will be the first study in Greece to systematically measure and quantify patients’ preferences, offering valuable insights into what patients consider important. By understanding patients’ preferences, the study can identify areas for improving cancer care in Greece, and contribute to more patient-centred models. It aims to identify preferred attributes and quantify trade-offs made by patients in their cancer care decisions.
Importantly, the findings of this study can provide valuable insights for decision-makers in designing cancer care models and facilities. By understanding patient preferences, decisionmakers can tailor healthcare system provisions to better meet the needs and expectations of patients with cancer. This, in turn, can lead to improved outcomes in cancer care, the optimisation of resource allocation, and the reduction of healthcare disparities.
METHODS
This study will utilise a DCE to capture patients’ preferences for the attributes of a cancer care model. The DCEs involve presenting participants with a series of hypothetical choices between different alternatives that are described by a set of attributes.8 By varying the levels of the attributes, researchers can assess the relative importance of each attribute to respondents, and the trade-offs they are willing to make between them. The results of a DCE provide a quantitative measure of the importance of each attribute, and can inform policy decisions, resource allocation, and the development of new interventions that align with patients’ preferences.9
DCEs have been used extensively in health economics and outcomes research, particularly in the context of healthcare decision-making.10 They have been employed to assess patient preferences for different treatments, health states, and healthcare services, as well as to evaluate the impact of different factors on healthcare decision-making, such as cost, efficacy, and side effects.11 DCEs have been shown to be a reliable and valid method for eliciting preferences, with high levels of test-retest reliability and construct validity.12 Compared with traditional rating and ranking
42 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
methods for eliciting preferences in healthcare, DCEs have been found to be more efficient and provide more information about the relative importance of attributes than traditional methods, making them a preferred method for preference elicitation in healthcare research.13
Typically, the development of the DCE survey involves several stages, to ensure that the DCE is developed correctly, and that the data collected are reliable and valid. Figure 1 depicts the steps required for developing a DCE.
Formulation of the Research Question
This study was commissioned by the Association of Oncological Patients (KEFI) in Greece,14 an organisation that supports patients with cancer in managing their illness effectively. KEFI offers practical and administrative assistance to ensure that patients with cancer can access the necessary care and support. The association’s mission is to improve quality of life by offering support to navigate the complex healthcare system.
The research question is relevant to the current developments in the healthcare sector in Greece, specifically regarding cancer care. The aim of the study is to capture the preferences of patients
with cancer regarding the various characteristics of cancer care in Greece. By exploring patients’ preferences, the study seeks to identify areas for improvement in cancer care, and to ensure that patient-centred care is being delivered. Ultimately, the study aims to contribute to the enhancement of cancer care services in Greece by providing valuable insights into the needs and preferences of patients, and this was established with consultation with the Governing Committee of KEFI.
Selection Of Attributes And Respective Levels
To identify the attributes and respective levels for this DCE, two distinctive but complementary, research methods were followed: targeted literature reviews (TLR) and focus group interviews (FGI), with the patients-members of KEFI.
Targeted Literature Reviews
The aim of the TLR was to create a comprehensive list of potential descriptors for cancer survivor care, along with specific characteristics. To achieve this, separate literature searches (Search 1, 2, and 3) were conducted. The separate searches were
1
2
3 4 5 6
Formulation of the research question
Selection of attributes and respective levels
Design of the survey
Piloting and improvement of the survey instrument
Data collection
Analysis and reporting
Figure 1: Process for developing a discrete choice experiment.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 43 Article
conducted in a complementary way, i.e., to be able to identify various aspects of cancer care models via a variety of sources.
Search 1 focused on identifying published papers that described cancer care models in Greece. The study will take place in Greece; hence, this was considered the starting point, and is essential to develop the list of potential attributes for the DCE. Search 2 aimed to identify cancer care models in countries other than Greece. The intention was to enrich the list of potential services for survivors of cancer by identifying services provided in other countries but not in Greece. Since the DCE is based on hypothetical scenarios, it provides the opportunity to capture patients’ preferences for attributes of the services that could potentially be available in the Greek healthcare setting. It was anticipated that the number of identified records for this review would be very large; hence, for this part of the review, the focus was on identifying only systematic or meta-systematic reviews. Search 3 aimed to identify methodologically relevant literature, i.e., DCEs conducted on the same topic, which would assist with the attribute selection.
The literature search resulted in a list of domains that included topics such as healthcare practitioners’ level of expertise; method of contact; location and frequency of follow-up visits; waiting time for booking an appointment, as well as waiting time during the appointment; and the existence of additional supportive or educational activities. While not exhaustive, this list played a pivotal role in shaping the topics for the FGI. Its purpose was to provide a starting point for participants to delve into their thoughts and opinions on the key aspects of cancer care that held the most significance for them.
Focus Group Interview with PatientMembers of KEFI
For the FGI, members of KEFI were recruited. Initially, all members were informed, via email or text message, about the upcoming study, which would involve conducting an FGI. Members were notified with the following message:
"For the first time in Greece, at the initiative of KEFI, a study is being conducted with the aim of eliciting the quantitative preferences of cancer
patients for models of care following their initial treatment. We invite you at the premises of our association to participate in the first phase of the study, where there will be a discussion on the needs of the Greek cancer patient. Our association will use the findings of the study to initiate necessary actions to inform and mobilise healthcare policymakers to design better, patient-centred health policies that consider patients’ preferences."
Approximately 30 members responded to the invitation, showing interest in the study, and willingness to participate in the FGI. On the day of the FGI, 15 members attended the event. Hence, for the FGI, the convenience sampling of 15 participants was deemed appropriate.
After the welcome, introduction, and completion of the consent form, the focus group co-ordinator provided participants with an overview of the focus group’s objectives, and the planned steps. The results of the TLRs were presented, serving as the groundwork for the subsequent focus group discussion. Subsequently, the participants were divided into two groups to discuss the characteristics of a care model that they would ideally like to see implemented in Greece, drawing from their personal experiences and their journeys with their illness. The two groups were moderated by two researchers specially trained in conducting FGIs. Participants were explicitly informed that the list of components served as a reference, and they were encouraged to share and discuss issues based on their unique perspectives, experiences, and preferences for the model of care after the initial treatment. The discussion was conducted using open-ended questions, intentionally without any predetermined order, and, most importantly, without the focus group moderators expressing a position, or influencing the participants’ responses. This approach was designed to facilitate impartial and unrestrained discussions, allowing participants to freely articulate their perspectives and insights. The process was guided by the co-ordinators’ neutrality and objective stance, enabling focus group participants to thoughtfully explore the critical parameters of a care model without coordinators’ intervention.
Each of the two groups, following the process described above, produced a distinct list of
44 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
themes (attributes) characterising a desirable cancer care model. These lists were then merged, and further discussed in the next stage of the FGI, where all the participants agreed on a final list of characteristics (presented in Table 1). All characteristics are deemed to be suitable for the DCE on the basis of three criteria: relevance to the research question, relevance to the decision context, and whether attributes are related to one another.9
Following the identification of characteristics, the participants were asked to rank them by order of importance via an online voting system, where Google forms were utilised. The objective of this task was to determine the top five to seven attributes that could be utilised in the DCE. According to the existing literature on DCEs, the average number of attributes in published studies is estimated to be 5.74 (standard deviation: 1.98), with a minimum of two and a maximum of 12.15 Therefore, adhering to common practice in DCE development, the authors considered a range of five to seven attributes to be satisfactory, ensuring that the DCE would not impose excessive cognitive demands on the respondents.16 The seven top ranked attributes are presented in the last column of Table 1
The findings of the FGI were further discussed with the Governing Committee of KEFI in a final stage of the qualitative part of the study, where a definitive list of attributes was created to develop the DCE survey (Table 2). The levels for each attribute were informed by a literature review applicable to the Greek context, and qualitative interviews with the Governing Committee of KEFI. Out-of-pocket costs to patients were additionally included, as this was deemed important due to the healthcare market dynamics in Greece, which involves a mix of private and social insurance coverage. In this context, it is common for patients to incur routine out-ofpocket medical expenses for procedures and/ or medical tests. Additionally, by incorporating out-of-pocket costs as an attribute, it allows the authors to use it as a standardised measure to evaluate the trade-offs that respondents make when assessing various attributes of a cancer care model.
Design of the Survey
Following the identification of attributes, the next step involves the experimental design for the DCE. Given the large number of profiles resulting from the combination of attributes and levels (2^[2]×4^4=1024 profiles), which result in 523,776 possible choice sets, a full factorial design is not feasible. Instead, an efficient experimental design will be constructed using the relevant macros in the SAS® statistical software (SAS, Cary, North Carolina, USA).17 Efficient experimental designs in the context of choice modelling refer to designs that optimise the precision of estimated parameters, while minimising the number of choice questions or choice sets presented to participants.18 The goal is to gather the maximum amount of information with a minimal number of choice tasks, reducing participant burden, and saving resources. Additionally, to serve this aim, a blocked design might be adopted.
In addition to the DCE questionnaire, the survey will include questions covering four main domains:
• Sociodemographic data on age, gender, education, occupation, and income, to provide context and possibility for subgroup analysis.
• Disease-related data on the type of cancer and time since diagnosis, to account for variations in preferences.
• Cancer care in Greece, enquiring about treatment options, access to healthcare services, provider interactions, and challenges, to understand the current state of cancer care in Greece.
• The EuroQol19 EQ-5D-5L questionnaire to allow for the assessment of the respondents’ current health state, across five dimensions (mobility, self-care, usual activities, paindiscomfort, and anxiety-depression). The EQ-5D-5L questionnaire is a standardised instrument designed to assess health-related quality of life. It is widely used in health research, clinical studies, and health economics.
Through these additional questions, the survey aims to collect a comprehensive dataset, beyond
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 45 Article
the DCE choices, which allows for a nuanced analysis of participants’ preferences concerning their sociodemographic characteristics, diseaserelated factors, healthcare experiences, and current health status. It provides a richer context for interpreting DCE results in the context of cancer care in Greece.
Piloting and Improvement of the Survey Instrument
The final survey instrument will be piloted with a small sample from KEFI members (approximately 25–30), who represent this study’s target population. This step is crucial to ensure the survey’s validity, reliability, and clarity. During the pilot phase, participants’ feedback on their understanding of the questions, and any
Characteristics Description Seven top ranked attributes via voting 1 Level of expertise of the healthcare provider Describes the level of specialisation of the doctor (e.g., pathologist, oncologist, nurse, surgeon, radiologist) 1 2 Method of contacting the health care provider Face-to-face meeting, by phone, video call 2 3 Visit location Hospital, doctor's office, patient's home, rehabilitation centres 4 Distance of the visit appointment It describes how far the patient will have to travel to see the healthcare provider 6 5 Frequency of visits Monthly, every 3 months, every 6 months 7 6 Waiting time during the Appointment Describes the length of time the patient waits outside the doctor's office 7 Waiting time to book an Appointment Describes how soon the patient can make an appointment with the healthcare provider (1 week, 2 weeks, 1 month, longer) 4 8 Supportive activities Activities that aim at patient education, information provision, nutritional advice, psychological support, pain clinic, adverse event management, social worker 5 9 Cost to the patient Costs for either paying for the appointments and test, or for the patient's travel 10 Holistic monitoring/ comorbidities Describes the ability to monitor the patient for the full range of health problems (comorbidities) 3 11 Waiting time for tests How quickly the patient can have all the tests and examinations prescribed by their doctor 12 Patients’ digital records Existence of a digital records, accessible to all healthcare providers who follow patients 13 Ease of access (availability) How direct and timely is the patient's communication with the doctor 14 Quality of service To what extent the services provided are governed by quality (patient information, courtesy, empathy)
care
Table 1: List of characteristics for a model of cancer
as produced by the focus group.
Article 46 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Attribute
1. Holistic Monitoring of the patient and decisionmaking for their care: how the patient is monitored for the full range of health problems during treatment and afterwards (e.g., thromboprophylaxis, comorbidities, and other emergencies)
2. Waiting time to book an appointment
3. Supportive activities, such as:
• Comprehensive patient education for treatment and aftercare
• Information on the management of treatment side effects
• Nutritional advice
• Psychological support/social worker
4. Distance of the centre where the medical visit will take place from the patient's residence
Levels
• Individually by the oncologist
• Collective decisions are made, with the participation of other specialties (e.g., radiation therapist, oncologist , pathologist, cardiologist, etc.)
• 1 week
• 2 weeks
• 1 month
• 3 months
• Yes
• No
5. Frequency of regular visits
6. Cost to the patient per year. It concerns any expenses incurred related to the illness (e.g., travel expenses, parking, meals, accommodation; if required, expenses for examinations that are not reimbursed by the EOPYY; costs of the patient's participation in the examinations, etc.) and is deducted from the annual family budget.
EOPPY: National Organization for Health Care Services.
• 30 minutes
• 1–2 hours
• Half a day
• More than a day
Every
• 3 months
• 6 months
• 9 months
• 12 months
• 500 EUR
• 1,000 EUR
• 1,500 EUR
• 2,000 EUR
Table 2: Final list of attributes and levels included in the discrete choice experiment.
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 47
challenges they encounter while completing the survey, will be gathered and analysed. In addition, the length of the survey and the time required for participants to complete it will be tested. Long surveys may lead to respondent fatigue, and a higher likelihood of incomplete or rushed responses. The piloting of the survey will lead to iterative improvement, as the survey instrument will be revised accordingly, based on the pilot test findings and participant feedback. Once the revisions are made, the final survey instrument will be deployed.
Data Collection
The survey will be conducted online, allowing respondents to complete it at their convenience via a web browser. This approach offers flexibility and convenience, enabling participants to complete the survey from any location with Internet access. The administrative team of KEFI will play a central role in recruiting participants, members of KEFI, or other associations in Greece set up for patients with cancer, for the survey. The primary criterion for participation is that respondents have been, or are currently, patients with cancer. No additional inclusion criteria will be applied to ensure an adequate number of responses.
Before beginning the survey, participants will be presented with a patient information sheet detailing the study’s purpose, procedures, confidentiality, and their rights as participants. They will then be asked to provide informed consent before proceeding with the survey.
The determination of the final sample size for a DCE considers various factors specific to the design itself. These factors include the number
of attributes, the range of attribute levels, the number of choice scenarios, the number of alternatives within each choice set, and the influence of prior parameters.20 Prior DCEs conducted in this field show a variability in the number of respondents, as well as the number of attributes that were used in the DCE: 185 respondents for a DCE with six attributes,21 668 respondents for a DCE with eight attributes,22 722 respondents for a DCE with five attributes,23 and 331 respondents for a DCE with five attributes.24 In this study, the final number of respondents required for the study will depend on the final experimental design.
Data Analysis, Reporting, and Dissemination
DCE data analysis typically involves regression modelling within a random utility framework. The random utility model is a commonly used approach in DCE analysis, and is based on the Lancaster theory of consumer demand.25,26 This framework assumes that individuals make trade-offs when making decisions, and choose the option that provides the greatest utility, determined by the attributes associated with the product or service. The utility of each alternative can be decomposed into systematic (observable) and random (unobservable) components (Figure 2).27 The systematic component represents the part of utility that can be explained by the attributes and their levels. It is typically modelled using regression techniques, such as the conditional logit, mixed logit, or latent class models. These models estimate the relationship between the attributes and the choice probabilities, allowing for the calculation of attribute importance, and the assessment of trade-offs. The random
U_ijt= V_ijt+ ε_ijt ,j=1,…,J
Where (U) utility of individual (i) conditional on alternative (j) in choice situation (t) is decomposable into an explainable or systematic component (Vijt) and a non-explainable or random component (εijt).
Article 48 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Figure 2: Equation.
component represents unobserved factors or individual-specific heterogeneity that affects the decision-making process. It is assumed to follow a specific distribution, such as the extreme value distribution, in the case of the conditional logit model.28 This component captures idiosyncratic preferences, taste variations, and random errors in decision-making.
Based on the above, the analysis will start with a multinomial logit model,29 which is commonly used in the analysis of DCE data. The model estimates the parameters that quantify the relative importance of the different attributes in influencing the choice probabilities. Further, other extensions of this model,30 such as the random parameters logit model or the mixed logit model, and latent class models, will be explored to capture individual heterogeneity, and account for preference variation across the sample. These models relax the assumption of identical preferences across individuals, and allow for more flexible estimation of preference heterogeneity.
Measures of goodness of fit, such as loglikelihood, McFadden’s R squared, Ben-AkivaLerman; and information criteria, like Akaike information criterion and Bayesian information criterion, will be used to determine the final parsimonious model in the context of choice modelling.
The study results will be disseminated via national and international scientific and health policy-related conferences to the academic community, policymakers, and the general public. It is envisaged that a manuscript will be published in a peer-reviewed journal.
SUMMARY
This study reports on the development of the qualitative phase of a DCE, and describes a
References
1. Kattlove H, Winn RJ. Ongoing care of patients after primary treatment for their cancer. CA Cancer J Clin. 2003;53(3):172-96.
2. Firkins J et al. Quality of life in “chronic” cancer survivors: a meta-analysis. J Cancer Surviv. 2020;14(4):504-17.
comprehensive protocol for the subsequent phases of the study. The utilisation of the DCE approach in the authors’ study holds promise for capturing the patient preferences regarding models of care for survivors of cancer in Greece, aligning with the global paradigm shift towards patient-centric care models. The findings of the study will enhance healthcare policymakers’ and clinicians’ understanding of patients’ needs and preferences, and subsequently develop strategies for the improvement of care for patients with cancer. The utilisation of a DCE reflects the broader trend of employing DCEs in healthcare decision-making, contributing to the growing literature on eliciting patient preferences.11
The aim of the qualitative phase of the study was to identify the attributes and levels which will be utilised in the experimental design of the DCE. A rigorous qualitative approach, which involved literature reviews, qualitative interviews, and FGI, was employed. Further, the large number of attributes which resulted from the FGI was scaled down to a manageable number by a rating exercise. This systematic combination of methods enhances the study’s quality and validity.12 Nonetheless, this study faces methodological limitations inherent in all DCEs. For instance, the utilisation of convenience sample for the FGI may be perceived as a potential source of bias, as the participants may not fully represent the diversity of perspectives within the broader population.
The DCE will be completed by a broad and diverse sample of individuals who have undergone, or are undergoing, cancer treatment. The study will provide insights into the patients’ trade-offs for the different attributes of cancer care, aiding policymakers in understanding the preferences of patients. These study findings will be placed in the context with existing research on how patients prefer post-cancer care, to gain a broader perspective of the general preferences for their care.
3. American Society of Clinical Oncology (ASCO). Survivorship: during and after treatment. 2016. Available at: https://www.cancer. net/survivorship/during-andafter-treatment. Last accessed: 3 February 2023.
4. European Society for Medical Oncology (ESMO). Patient guide on survivorship. 2017. Available at:
https://www.esmo.org/content/ download/117593/2061518/1/ ESMO-Patient-Guide-Survivorship. pdf. Last accessed: 3 November 2023.
5. Lawler M et al. A catalyst for change: the European cancer Patient's Bill of Rights. Oncologist. 2014;19(3):217-24.
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 49
6. European Partnership Action Against Cancer (EPAAC). Greece national cancer plan 2011-2015. Available at: http://www.epaac.eu/ from_heidi_wiki/Greece_-_National_ Cancer_Plan_2011-2015,_Greek. pdf. Last accessed: 3 November 2023.
7. Greek Ministry of Health. National action plan for public health 2021-2025. Available at: https:// www.moh.gov.gr/articles/health/ domes-kai-draseis-gia-thn-ygeia/ ethnika-sxedia-drashs/8776ethniko-sxedio-drashs-gia-thdhmosia-ygeia-2021-2025?fdl= 20523. Last accessed: 3 November 2023.
8. Ryan M et al., Using discrete choice experiments to value health and health care (2007) Volume 11, Luxembourg: Springer Science & Business Media.
9. Jackson Y et al. The evolving role of patient preference studies in health-care decision-making, from clinical drug development to clinical care management. Expert Rev Pharmacoecon Outcomes Res. 2019;19(4):383-96.
10. Clark MD et al. Discrete choice experiments in health economics: a review of the literature. PharmacoEconomics. 2014;32(9):883-902.
11. de Bekker-Grob et al. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145-72.
12. Bridges JF et al. Conjoint analysis applications in health-a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403-13.
13. Ryan M et al. Eliciting public
preferences for healthcare: a systematic review of techniques. Health Technol Assess. 2001;5(5):1-186.
14. KEFI of Athens. Homepage. Available at: https://www. anticancerath.gr/. Last accessed: 3 November 2023.
15. Trapero-Bertran M et al. What attributes should be included in a discrete choice experiment related to health technologies? A systematic literature review. PLoS One. 2019;14(7):e0219905.
16. Marshall D et al. Conjoint analysis applications in health-how are studies being designed and reported? An update on current practice in the published literature between 2005 and 2008. Patient. 2010;3:249-56.
17. SAS Software. Homepage. Available at: https://www.sas.com/ en_us/home.html. Last accessed: 3 November 2023.
18. Reed Johnson F et al. Constructing experimental designs for discretechoice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3-13.
19. EuroQol. EQ-5D-5L questionnaire. Available at: https://euroqol.org/ information-and-support/euroqolinstruments/eq-5d-5l/. Last accessed: 5 January 2024.
20. Assele SY et al. Sample size selection for discrete choice experiments using design features. J Choice Model. 2023;49:100436.
21. Wong SF et al. A discrete choice experiment to examine the preferences of patients with cancer and their willingness to pay for different types of health
care appointments. J Natl Compr Cancer Netw. 2016;14(3):311-9.
22. Murchie P et al. Determining cancer survivors' preferences to inform new models of follow-up care. Br J Cancer. 2016;115(12):1495-503.
23. Bessen T et al. What sort of followup services would Australian breast cancer survivors prefer if we could no longer offer long-term specialist-based care? A discrete choice experiment. Br J Cancer. 2014;110(4):859-67.
24. Merel LK et al. Follow-up after treatment for breast cancer: One strategy fits all? An investigation of patient preferences using a discrete choice experiment. Acta Oncologica. 2010;49(3):328-37.
25. Lancaster K. A new approach to consumer theory. J Polit Econ. 1966;74:132-57.
26. Lancaster K et al., Consumer demand: a new approach (1971), New York: Columbia University Press.
27. Louviere JJ et al. Stated choice methods: analysis and applications. 2000;DOI:10.1017/ CBO9780511753831.008.
28. McFadden D, “Conditional logit analysis of qualitative choice behaviour,” Zarembka P (ed.), Frontiers in Econometrics (1974), New York: Academic Press, pp.105-42.
29. Train KE, Discrete Choice Methods with Simulation (2009) 1ˢᵗ edition, Cambridge: Cambridge University Press.
30. Hensher DA et al., Applied Choice Analysis: A Primer (2005) 1ˢᵗ edition, Cambridge: Cambridge University Press.
Article 50 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Prevalence and Factors Associated with Contraceptive Use Among Females Living with HIV at Moi Teaching and Referral Hospital, Eldoret, Kenya
Authors:
*Sheila Sawe,1 Edwin Were,1 Winfred Mwangi,1 Jack Odunga1
1. Department of Reproductive Health, Moi University School of Medicine, Eldoret, Kenya
*Correspondence to sheilasawe@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 30.01.23
Accepted: 15.01.24
Keywords: Contraceptive use, females living with HIV (FLHIV), HIV, Moi Teaching and Referral Hospital (MTRH).
Citation: EMJ. 2024;[9]1:51-58. DOI/10.33590/emj/10301577. https://doi.org/10.33590/emj/10301577.
Abstract
Objective: To assess the prevalence of, and the factors associated with, contraceptive use among females living with HIV at Moi Teaching and Referral Hospital, Eldoret, Kenya.

Methods: A cross-sectional study with a sample including a total of 375 females living with HIV aged 15–49 years undergoing follow-up. Data were collected using a semi-structured questionnaire. Bivariate and multivariate analysis was done to check for association and predictors of contraceptive use.
Results: The contraceptive prevalence rate was 64%. Factors associated with contraceptive utilisation included parity (crude odds ratio [COR]: 2.33; 95% confidence interval [CI]: 1.22–4.45; P=0.010), marital status (COR: 1.75; 95% CI: 1.04–2.97; P=0.036), and availability of information on the side effects of the contraception methods (COR: 29.93; 95% CI: 14.26–70.58; P=0.001).
Multivariate analysis showed a significant association between contraceptive use and whether information on the side effects of the current contraception method was provided (adjusted OR: 34.98; 95% CI: 16.72–83.33; P=0.001).The odds of meeting the contraceptive needs of females living with HIV was 34 times higher among females who had information on side effects of the contraceptives than their counterparts who had no information.
Conclusions: The contraceptive prevalence rate was 64% among females living with HIV, higher than latest national value of 61%. Females living with HIV had a high unmet need for contraceptive use at 28.4%. Key factors associated with contraceptive utilisation included awareness of side effects.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 51 Article
Key Points
1. The contraceptive prevalence rate among females living with HIV at Moi Teaching and Referral Hospital, Eldoret, Kenya, was 64%, higher than the national rate of 61%; yet, there is significant unmet need for contraceptive use.
2. Multivariate analysis revealed a significant association between contraceptive use, and the provision of information on the side effects of current contraception methods.
3. Counselling on the side effects of the various contraceptive methods should be emphasised, in order to empower females to make informed choices which limit discontinuation.
BACKGROUND
HIV is an epidemic in Kenya. Females living with HIV (FLHIV) have an eight-fold increased risk of a pregnancy-related death compared to females without the infection.1 This has necessitated multidisciplinary efforts in its management and control to reduce both disease progression and burden. A major weak link in this control is the prevention of mother-to-child transmission (MTCT) among infected females who are still sexually active. An estimated overall MTCT rate of 11% is very significant, and the elimination of MTCT therefore remains a key goal of Kenya’s HIV epidemic response.2
Contraceptive services for females who are HIV-positive are one of the four cornerstones of a comprehensive programme for prevention of MTCT of HIV, thereby reducing paediatric HIV infection, and are vital to meeting sexual and reproductive health needs of females who are HIV-positive.
There has been a growing trend in the contraception prevalence rate in Kenya, from 32% in 2003 to 53% in 2014, with unmet contraceptive need standing at 18% of currently married females, with 9% in need of spacing and 8% in need of limiting. A total of 31% of family planning (FP) users discontinue use of a method within 12 months of starting its use. Side effects and health concerns (11%) are the main reason for discontinuation.3
Females with unmet need are those who are fecund and sexually active, but are not using any method of contraception, and report not wanting any more children, or wanting to delay the next child.
Studies conducted on unmet contraceptive needs among FLHIV in Kenya and in Africa show mixed results, indicating differences in study settings that may influence contraceptive use. Therefore, despite the great overall progress toward increased uptake of FP, there is unmet need for consistent contraceptive use among FLHIV in Kenya.
Facilitators to contraceptive needs were not incorporated in the study of Amo-Adjei et al.,4 which the current study sought to incorporate, in addition to barriers, unmet needs, and the contraceptive prevalence rate. A review of the existing literature presented above shows that knowledge gaps exist on prevalence rate, factors associated with contraceptive use, and unmet contraceptive needs among FLHIV.
Despite pregnancy intentions being low, contraceptive use among FLHIV has been low and associated with high unmet need and consequences. However, general population contraceptive prevalence has increased, and unmet need has decreased over the last decade.3 Though a lot has been done in this field of FP and FLHIV, results have been mixed, indicating regional disparities and even disparities within countries, hence the need for local data.
In this study, the authors assess contraceptive use and factors associated with use among FLHIV in a major referral comprehensive care centre.
52 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
STUDY OBJECTIVE
The authors’ aim was to assess the prevalence and the factors associated with contraceptive use among FLHIV at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya.
METHODOLOGY
Study Design
This was a cross-sectional study conducted at the Academic Model for Providing Access To Healthcare (AMPATH) Centre in Eldoret.
Study Population
This study targeted females between 15–49 years of age, who were living with HIV and registered at the AMPATH programme in 2019. The major role of AMPATH is to provide clinical healthcare to the general population on diseases that are affecting them, particularly targeting communicable diseases.
Sampling Procedure
Systematic sampling was adopted as the preferred sampling technique to meet the computed sample size of 377. To obtain the sampling interval (k), the calculated sample size was divided by the total population, giving a sampling interval of 18. The study sampled every 18th potential participant as per the triage register. After the first participant was recruited, there was an interval of 18 participants until the required sample size was achieved.
Data Collection Procedure and Quality Assurance
Data collection was done from the AMPATH Centre by the principal investigator and research assistants who were nurses that had been trained in data collection by the principal investigator. This was done in order to limit stigma that may arise from patients not being conversant with the investigator. Data collection was done using an electronic version of the questionnaire that was designed using EpiData Entry Software (EpiData, Odense, Denmark). Checks and balances were included
in the design of the questionnaire, such that automatic pop-up alerts were activated in case wrong data were erroneously entered in a particular field. The checks also limited the participants as per the inclusion criteria, hence a candidate who did not meet the bare minimum was automatically rejected. When the last entry in the questionnaire was made, the computer prompted to save the recorded data. This limited errors associated with transfer of data during data entry.
Data Management and Analysis
The contraceptive prevalence rate among females of reproductive age living with HIV in MTRH was calculated as the percent of married females of reproductive age who were using (or whose partner was using) a contraceptive method at the time of our study. The authors included modern contraceptive methods
Inferential Analysis
A statistical model that takes into account the nominal scale of the response variable was considered for modelling the association between the dependent and independent variables. A multinomial logistic regression model was adopted as the statistical model of choice in this study. Simple and multiple forms of this model yield unadjusted and adjusted odds ratios as measure of association between the variables. The group of mothers who were not using contraceptives at all were considered as the preferred reference group for the independent variables during analysis. All the analyses were done at 95% significance level in R Studio Version 1.2.1335 statistical software (Posit, Boston, Massachusetts, USA).
Ethical Considerations
Ethical approval was sought and approved from the Institutional Research and Ethics Committee (IREC) of MTRH, and from AMPATH. Informed written consent and assent was obtained before carrying out the study from each sampled participant. Privacy and confidentiality was ensured by obtaining consent from participants in a private room.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 53 Article
RESULTS
Socio-demographic Characteristics of the Study Participants
In this study, the authors recruited 375 females aged 15–45 years with a mean age of 34.8 years (standard deviation: 7.5). Of these, 100 (26.7%), 153 (40.8%), 80 (21.3%), and 42 (11.2 %) participants were single, married, separated, or widowed, respectively. The majority of the study participants (334; 89.1%) had sexual partners. A total of 131 (34.9%), 13 (36.0%), and 88 (24.0%) had attained primary, secondary, and tertiary education, respectively. Moreover, 87 (23.2%), 148 (39.4%), and 138 (36.8%) participants were either employed, selfemployed, or unemployed, respectively. Most participants in the study were Christians (365; 97.3%).
Contraceptive Prevalence Rate Among Females Living with HIV in MTRH
Of the 375 participants, 240 were on a modern contraceptive method, giving a contraceptive prevalence rate of 64%, while 135 (36.0%) were not using any contraceptive methods.
Male and female condoms were used by 76 (20.6%) participants, sub-dermal implants were used by 72 (19.2%) participants, while oral contraceptives were used by seven (1.8%) of the participants. A total of 68 (18.0%) participants used injections, while four (1.0%) used emergency contraceptive pills. Sterilisation was adopted by three (0.8%) of the participants, and intra-uterine devices were used by 14 (3.7%).
Sources of Information on Contraception Methods
In reference to the source from which the participants heard about contraceptives and FP, 30 (8.0%) got information from radio or television, 18 (4.8%) from newspapers, 20 (5.3%) from the internet, 321 (85.6%) from healthcare providers, and 106 (28.3%) obtained it from friends and relatives. A total of 135 (91.2%) attended antenatal care during their last pregnancy, where 124 (83.8%) said contraceptive methods were discussed.
Barriers to Contraceptive Use Among Females Living with HIV in MTRH
In total, 265 (70.7%) participants had encountered challenges in accessing contraceptives. Of those, 16 (4.3%) thought that nulliparity had partly contributed to their challenge, since they had the desire to have more children. Four (1.5%) stated that they had been denied FP access because of their age. A total of 18 (6.8%) reported that their challenge arose from their lack of knowledge on modern methods of contraception.
Side effects featured in the form of participant’s personal experiences, and what they had heard from other sources. More than half (144; 54.3%) said that the fear of side effects associated with the FP methods that they had experienced was also a contributing factor. A total of 79 (29.8%) of the participants said that what they had heard about side effects of contraceptives was a challenge, hence making it hard for them to use contraceptives.
In respect to cost, six (2.3%) and five (1.9%) of the participants cited inability to afford the cost of consultation and contraception, respectively. Couple counselling also featured as a challenge, whereby 14 (5.3%) participants reported that their husband or male partners were never involved in discussions on FP methods. Moreover, 42 (15.8 %) participants admitted that traditional beliefs in their community had prevented them from using contraceptives. The participants, however, did not specify any of the cultural beliefs (Table 1).
Challenges with Dual Method of Contraception
In relation to challenges, 258 (68.8%) participants acknowledged that they were facing some challenges in the use of dual methods recommended for prevention of sexually transmitted infections, while 117 (31.2%) had no challenges.
Inconsistent use of condoms was reported by 184 (49.1%) participants. This was followed closely by partner’s negative attitude towards condom use, reported by 123 (32.8%) participants.
54 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Discontinuation
More than half (267; 71.2%) of the participants had once discontinued a contraceptive method within the first year of contraceptive use. Out of 267 participants, 118 (44.2%) reported side effects as a reason for the discontinuation. A total of 77 (28.8 %) subjects desired to get pregnant. In relation to health challenges, 32 (12.0%) participants reported that their health challenges had led to the discontinuation of contraceptive use. Method failure marked by pregnancy while on contraceptive was acknowledged by 40 out of 267 participants (15%).
Facilitators to Choice of Contraceptive Use
When asked about what could be done to improve the use of contraceptives, the study participants reported the main facilitators of FP use were increased awareness on the availability of FP methods at 99.2%, and the knowledge of the side effects of contraceptive use at 94.9%
Inferential Statistics on the Association Between Contraceptive Use and Independent Variables
Bivariate analysis showed a significant association between contraceptive use with parity (crude odds ratio [COR]: 2.33; 95% confidence interval [CI]: 1.22–4.45; p=0.010), marital status (COR: 1.75; 95% CI: 1.04–2.97; p=0.036), and availability of information on the side effects of the current contraception methods (COR: 29.93; 95% CI: 14.26–70.58; P=0.001).
Other variables, like awareness on the availability of contraceptive methods, travelling distance, transport cost, age, employment status, and education, were not significantly related to contraceptive use (Table 2).
Multivariate analysis showed a significant association between contraceptive use and availability of information on the side effects of the contraception methods (adjusted OR: 34.98; 95% CI: 16.72–83.33; P=0.001). Parity and marital status both became non-significant in the multivariate analysis.
Challenge Category n=265 (%) Because I have no child (nulliparity). Yes 16 (6.0) I have been denied family planning because of my age. Yes 4 (1.5) Participant’s perception on barriers to contraceptive use. Yes 18 (6.8) Because I fear the side effects associated with the methods from what I have experienced. Yes 144 (54.3) Because I fear the side effects associated with the methods from what I have heard about. Yes 79 (29.8) Because I could not afford the consultation fees required at the clinic. Yes 6 (2.3) Because I could not afford the cost of the contraception I wanted. Yes 5 (1.9) Because my husband/male partner was not involved in family planning methods discussion. Yes 14 (5.3) Do traditional beliefs in your community prevent you from using contraceptives? Yes 42 (15.8) Table
Barriers
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 55 Article
1:
to contraceptive use among females living with HIV in Moi Teaching and Referral Hospital, Eldoret,
Kenya.
Contraceptive use Variable No (n %) Yes (n %) N=135 N=240 P Awareness on the availability No 1 (0.7) 2 (0.8) Yes 134 (99.3) 238 (99.2) 0.834 Travelling shorter distance No 129 (95.6) 233 (97.1) Yes 6 (4.4) 7 (2.9) 0.301 Affordable cost of transport No 130 (96.3) 232 (96.7) Yes 5 (3.7) 8 (3.8) 0.422 Information on the side effects of the current contraception method No 126 (93.3) 76 (31.7) Yes 9 (6.7) 164 (98.3) 0.001 Age (mean, SD) 34.3 (8.6) 35.1 (6.9) 0.339 Parity Nulliparous 23 (17.0) 21 (8.8) Reference Uniparous 18 (13.3) 25 (10.4) 0.332 Multiparous 89 (65.9) 189 (78.8) 0.010 Employment status Employed 29 (21.5) 60 (25.0) Reference Self-employed 53 (39.3) 95 (39.6) 0.613 Unemployed 53 (39.3) 85 (35.4) 0.373 Education None 7 (5.2) 15 (6.3) Reference Primary 51 (37.8) 80 (33.3) 0.525 Secondary 46 (34.1) 88 (36.7) 0.817 Tertiary 31 (23.0) 57 (23.8) 0.763 Marital status Single 43 (31.9) 57 (23.8) Reference Married 46 (34.1) 107 (44.6) 0.036 Separated 26 (19.3) 54 (22.5) 0.151 Widowed 20 (14.8) 22 (15.7) 0.613
56 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Table 2: Bivariate association between contraceptive use among females living with HIV and selected variables.
SD: standard deviation.
The odds of meeting the contraceptive needs of FLHIV was 34 times higher among females who had information on side effects of the contraceptives than their counterparts who had no information (Table 3).
DISCUSSION
Contraceptive Prevalence Rate among Females Living with HIV in MTRH
Of the 375 participants, 240 were on a modern contraceptive method, giving a contraceptive prevalence rate of 64%.
The increase in contraceptive prevalence rate that has been reported recently is probably in both FLHIV, as well as in the general population. The authors stipulate that recent efforts to integrate FP in HIV services may have resulted in better counselling, which may have resulted in increased uptake, and possibly less discontinuation rates.
In terms of popular contraceptive methods, the authors found most females were using the male condom. This is consistent with the Kenya Family Planning report 2020, which showed that condoms were the most used form of contraceptive.5
The authors results are in contrast with a study done by Mumbo et al.,6 which found the prevalence rate of contraceptive utilisation to be 79% among the study participants in a study done in Kwale, Kenya.6 Similar results were reported by Adesola et al.7 in Nigeria, who found a contraceptive prevalence rate of 67.7% among FLHIV, and Chibwesha et al.8 in Zambia, where the contraceptive prevalence rate was 69% among FLHIV.
From the bivariate analysis, there was a significant association between marital status, parity, information on the side effects of contraceptives, and contraceptive utilisation. More married females used the FP method than single females, but this was not statistically significant. This could have been caused by the sample size, and the distribution of numbers on the marital status variable.
According to the Kenya Demographic and Health Survey,3 contraceptive use was higher among sexually active, unmarried females (60.9%) than
among married females (53.2%). There may be autonomy in decision-making for single females and those not in union as compared to those in a union.9
Facilitators and Barriers to Contraceptive Use Among Females Living with HIV in MTRH
Knowledge about contraceptives side effects
There was a statistically significant association with information on the side effects of the current contraception method at multivariable analysis. The odds of meeting the contraceptive needs of FLHIV was 34 times higher in females who had information on side effects of the contraceptives, compared with their counterparts who had no information. These findings compare with a study by Ryan et al.,10 which showed that knowledge of contraceptive methods was an important predictor of use, associated at logistic regression knowledge with 33% (OR: 1.33) increased odds of using contraceptives.10
The effect of counselling on contraception use is quite important in the correction of myths and misconceptions related to contraception use, creating awareness of the various contraception options for FLHIV to make their preferred choices of FP methods, and in addressing other FP related barriers.
CONCLUSIONS AND RECOMMENDATION
Conclusions
The authors found a contraceptive prevalence rate of 64%, which is higher than the latest national value of 61%, which is a good thing for this facility. The unmet need for FP for FLHIV was 28.4% higher than the African average of 24.2%. This percentage is high, and needs to be reduced by providing contraceptives and health education. Fear of the side effects was the main barrier or discontinuation factor for contraceptive use. The male condom was the most commonly used method of contraception; however, the majority also reported inconsistent use. The authors encourage the use of male condoms, since it is the most readily available means of contraception, with no known side effects.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 57 Article
Recommendations
The authors recommend that health professionals should encourage reproductive choices of females who are HIV-positive by increasing counselling and appropriate contraception provision at the time of HIV diagnosis, and during follow-up. Counselling on the side effects of the various contraceptive methods should be taken into account, especially at the time of giving these options, so that females are aware, and therefore make informed choice that limit discontinuation.
References
1. Calvert C. et al. The contribution of HIV to pregnancy-related mortality: a systematic review and metaanalysis. Aids 2013;27(10):1631-9.
2. Kumar P et al. Augmenting progress on the elimination of vertical transmissions of HIV in India: insights from Spectrum-based HIV burden estimations. PLOS Glob Public Health. 2023;3(8):e0002270.
3. The World Bank. Demographic and health survey 2014. 2019. Available at: https://microdata.worldbank. org/index.php/catalog/2544#study_ desc1684336809542. Last accessed: 1 January 2024.
4. Amo-Adjei J et al. Fertility intentions and the adoption of long-acting
Study Limitations
Study limitations include that consistent and correct use in regard to the different contraceptive methods was not taken into consideration. Considering that the interviews took place at the clinic facility, there is also a possibility that the findings do not reflect what is happening at the community level.
and permanent contraception (LAPM) among women: evidence from Western Kenya. BMC Womens Health. 2019;19(1):26.
5. Ministry of Health (MOH). (2020). National family planning guidelines for service providers (6th Edition). 2020. Available at: https:// tciurbanhealth.org/wp-content/ uploads/2019/04/Kenya-NationalFamily-Planning-Guidelines-6thEdition-for-Print.pdf. Last accessed: 1 January 2024.
6. Mumbo E et al. Unmet need for contraception use among HIV positive women in Kwale county, Kenya. Afr J Health Sci. 2021;34(6):767-78.
7. Adesola AF et al. contraceptive use
among women living with HIV and AIDS receiving care at secondary and tertiary health care facilities in Ibadan, Nigeria. Am J Clin Exp Med. 2017;5(6):218-23.
8. Chibwesha CJ et al. Modern contraceptive and dual method use among HIV infected women in Lusaka, Zambia. Inf Dis Obstet Gynecol. 2011;2011:261453.
9. Sedgh G et al. Unmet need for contraception in developing countries: examining women’s reasons for not using a method. Guttmaker Inst. 2016.
10. Ryan S et al. Knowledge, perceptions, and motivations for contraception. Youth & Society. 2007;39(2):182-208.
Variable Unadjusted OR (95% CI) Adjusted OR (95% CI) P value Information on
Yes 29.93 (14.26–70.58) 34.98 (16.72–83.33) 0.001 No Reference Reference Parity Nulliparous Reference Reference Uniparous 1.52 (0.65–3.58) 2.01 (0.62–6.63) 0.245 Multiparous 2.33 (1.22–4.45) 2.56 (0.72–9.65) 0.153 Marital status Single Reference Married 1.75 (1.04–2.97) 0.77 (0.30–1.91) 0.569 Separated 1.57 (0.85–2.91) 0.85 (0.32–2.20) 0.739 Widowed 0.83 (0.40–1.72) 0.52 (0.17–1.55) 0.244 CI: confidence interval; OR: odds ratio.
the side effects of the current contraception method
Table 3: Multivariate logistic regression after adjusting for confounding variables.
58 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Renal Replacement Therapy During Liver Transplant Surgery
Authors:
*Arjun Sekar,1 Aswanth Reddy,2 Pulkit Gandhi,1 Vijay Raj3
1. Rochester General Hospital, New York, USA
2. Mercy Clinic, Fort Smith, Arkansas, USA
3. Conway Medical Center, South Carolina, USA
*Correspondence to arjun_sekar@hotmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 05.10.23
Accepted: 15.02.24
Keywords: Liver transplant (LT), renal replacement therapy (RRT), reperfusion syndrome.
Citation: EMJ. 2024;9[1]:59-67. DOI/10.33590/emj/11000030. https://doi.org/10.33590/emj/11000030.
Abstract
Liver transplant is the treatment available for eligible patients with end-stage liver cirrhosis. Acute kidney injury and electrolyte abnormalities are associated with liver disease and can be exacerbated by surgery. Intraoperative renal replacement therapy has been tried in some large centres. The authors discuss the physiological changes and complications during liver transplant surgery, and review literature on the safety, feasibility, benefits, and drawbacks of intraoperative renal replacement therapy during liver transplant surgery.
Key Points
1. Renal insufficiency in liver cirrhosis portends a poor prognosis. Liver transplant is the only treatment for end-stage liver disease, and the surgery is complex, with major disturbances in acid-base and electrolyte status.
2. Intraoperative renal replacement therapy can be an option to optimise acid-base and electrolyte status during liver transplant.
3. This review discusses the limited data of intraoperative renal replacement therapy during liver transplant, and reviews the challenges, benefits, and adverse events described.
INTRODUCTION
End-stage liver disease (ESLD) represents a nonreversible, advanced stage of cirrhosis, where the hepatic architecture is distorted and nodular. It is one of the top 10 causes of death in the USA, and common causes include alcohol abuse and viral infections.
The complications in patients with acute fulminant hepatic failure and ESLD range from bleeding, infections, and malnutrition, to multiorgan failure. Acute kidney injury (AKI) is common (50–58%) in hospitalised patients with cirrhosis.1 It can be precipitated by gastrointestinal bleeding, angiotensinconverting enzyme inhibitors, large volume paracentesis, and infection. Types of AKI include
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 59 Article
acute tubular necrosis, glomerular pathologies (cryoglobulinaemia, secondary IgA, etc.), and hepatorenal syndrome (HRS). AKI portends a poor prognosis, with one analysis showing a combined mortality rate of 67%, with 1-month mortality at 58%, and 54–79% at 1 year.2
ESLD is a condition that is increasing in prevalence, and has very high morbidity and mortality. Even without complications, the median survival is approximately 2 years.3 Liver transplantation (LT) remains the best treatment option for eligible patients. AKI before LT worsens the prognosis (50% mortality).4 The need for renal replacement therapy (RRT) pre- or post-LT is associated with more than a two-fold increase in risk of death.5 For those undergoing LT, AKI is present in 15–20% on admission, and this number can increase as they wait for LT.6
Eligible patients with ESLD who are dialysis dependent beyond 8 weeks (about 2 months) are considered for simultaneous liver-kidney transplant.7 The pre-, intra-, and postoperative management of LT surgery is challenging, and requires close monitoring of electrolytes, volume status, and acid-base homeostasis.
A recent article6 reviewed the physiological changes in liver cirrhosis, and how intraoperative RRT could impact this. This article does denote the limitations in data, with limited to no controls in available literature. The authors’ review further expands on this, and also analyses data from multiple studies regarding the safety, feasibility, and practical challenges of intraoperative RRT.
This is important, as LT surgery is associated with high morbidity and mortality, some of which are related to complications from AKI and electrolyte disturbances.
INDICATIONS FOR RENAL REPLACEMENT THERAPY IN HEPATORENAL SYNDROME
Dialysis is offered to patients with HRS who are candidates for LT.8 The indications to start RRT are like the general indications for RRT. HRS needing dialysis is associated with a poor prognosis.9 RRT can be a bridge to transplant in those on the waitlist, and those undergoing evaluation for eligibility.
Given the complex physiological changes during LT surgery, some centres are utilising RRT perioperatively (including intraoperatively) in patients with kidney disease.
At present, there is no clear consensus or guideline regarding dialysis initiation.
Continuous renal replacement (CRRT) is the modality that is mostly used.
Entwined Organ Failure and Physiological Changes in Cirrhosis
An understanding of these physiological changes helps us better understand the complications that can arise intraoperatively, and the potential role of RRT in mitigating these complications (Figure 1).
Impact of end-stage liver disease on cardiovascular and pulmonary circulation
Splanchnic vasodilation due to liver cirrhosis leads to decreased systemic vascular resistance, causing relative hypotension.10 A possible mechanism is ‘leakage’ of endogenous mediators (nitric oxide, IL-6, and TNF-α) from the portal circulation into the systemic circulation, because of impaired hepatic metabolism. Further, increased catecholamines in cirrhosis can cause tachycardia and reduced cardiac afterload.11
Simultaneously, systemic vasodilation causes intrapulmonary vasodilation and portopulmonary hypertension.12 This can lead to ventilationperfusion mismatch. The physiologically volume-compliant right ventricle dilates from the elevated right-sided pressure.13 Overall, cirrhosis can lead to right and left heart strain.
Impact on kidneys
Splanchnic vasodilatation leads to effective arterial intravascular volume depletion, activating the renin angiotensin aldosterone system and sympathetic pathways, resulting in renal vasoconstriction and decrease in glomerular filtration rate (GFR).14 As a compensatory mechanism, sodium reabsorption and passive fluid retention, reduced oncotic pressure, and non-osmotic release of vasopressin leads to increased extracellular water accumulation. Fluid retention and azotaemia can lead to cerebral oedema and intracranial hypertension.15 In many instances of cirrhosis, renal vasoconstriction and
60 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article


fluid shifts can lead to cumulative nephrotoxicity, and eventually interstitial fibrosis and need for RRT.
IMPACT OF SURGERY ON HOMEOSTASIS
Orthotopic LT surgery is a complex procedure that involves transplanting a donor liver to the recipient post-native hepatectomy. With associated AKI, there could be severe electrolyte and acid-base disturbances.
The surgery poses a substantial risk of developing de novo AKI from renal venous congestion (from clamping the inferior vena cava [IVC] and major veins) and ischaemic injury. Metabolic derangements can worsen intraoperatively if renal function is compromised.
Liver Transplantation Surgery and Hyponatraemia
Hyponatraemia is a common electrolyte abnormality seen in ESLD,16 and is associated with worse mortality in CKD.17 Sodium levels can rise due to improved liver function post-


transplant. The anaesthesiologist can attempt to avoid substantial changes in sodium levels, but this might not always be possible because of the need for intravenous fluids and blood products. Rapid sodium correction can lead to osmotic demyelination syndrome.18
A study conducted by Romanovsky et al.,19 in LT, showed increased neurological deficits (p=0.006) if the 24-hour post-transplant correction was more than 10 mmol/L.
The goal before LT should be to improve the sodium level to avoid substantial changes intraoperatively. Hypotonic solutions for carrier fluids or volume resuscitation can be used to avoid overcorrection.18
Liver Transplantation Surgery and Metabolic Acidosis
Lactic acidosis is common, and is associated with increased mortality in LT.20 The liver is an important organ in the ‘clearance’ of lactate. In states of hypoperfusion coupled with decreased clearance in liver dysfunction, this can be severe. Renal dysfunction further worsens metabolic acidosis due to losses of bicarbonate from the tubules and loss of renal buffer.
Figure 1: Entwined organ failure in liver cirrhosis.
blood flow
retention
blood flow
aldosterone system
Hepatorenal
syndrome Portal
Splenomegaly Cirrhosis Sodium
Renal
Renin-angiotensin-
Splanchnic vasodilation
Decreased arterial blood volume
Peripheral vasodilation
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 61 Article
Leakage
of endogenous mediators Nitric oxide IL-6 TNF-α
AKI: acute kidney injury; CRRT: continuous renal replacement therapy; CVVH: continuous veno-venous haemofiltration; CVVHDF: continuous veno-venous haemodiafiltration; N/A: not applicable; OLT: orthotopic liver transplant; SLK: simultaneous liver kidney.
Under physiological conditions, the kidney is the second most efficient organ in removing/ metabolising lactate.21 Studies have suggested that the kidney can be responsible for 20–30% removal of an exogenous load of lactate.22 A lot of the ‘removal’ of lactate by the kidney is by uptake and metabolism of lactate, rather than by urinary excretion.23 If there is metabolic acidosis, renal uptake of lactate increases despite a reduction in renal blood flow.24
Bicarbonate
in anuric AKI and lactic acidosis is unlikely to be beneficial, with the potential risk of volume overload. In addition,
high volumes of parental bicarbonate can cause a paradoxical intracellular acidosis by increasing the concentration of dissolved CO2.25 Intracellular acidosis can decrease cardiac contractility.26
Intraoperative bicarbonate is not effective in lactic acidosis.27 RRT with bicarbonate-based dialysis baths can reduce acidosis, as per one study.28
Liver Transplantation Surgery and Portopulmonary Hypertension
Pulmonary artery hypertension associated with
Study Modality Preoperative Intraoperative Postoperative Mortality Length of stay Comments Douthitt et al.42 CVVHDF 5 9 9 75% survival 1 year Longer (30 days) 100% alive at 1 month Lamattina et al.43 CVVH N/A 14/21 N/A 86% CVVH versus 71% N/A Patients with AKI Townsend et al.9 CRRT 26/636 41/636 32/636 75% survival 1 year N/A Renal recovery 100% of dialysis Mitra et al.44 Haemodialysis N/A 155 OLT & 83 SLK N/A 80% survival at 1 year N/A 99% dialysis free Kobori et al.45 CVVH N/A 6 SLK N/A 100% survival at 1 year N/A N/A Inception study41 CRRT 22/32 N/A N/A Similar survival at 1 year for RRT versus no RRT N/A N/A Kościelska et al.46 Haemodialysis N/A 93/1,033 N/A Postoperative outcomes not looked at N/A Dialysis was safe
therapy
Table 1: Summary of studies on perioperative renal replacement therapy in liver transplantation.
62 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Hyperkalaemia
Rapid correction possible Correction is slower
Metabolic acidosis N/A N/A
Ultrafiltration
Hyponatraemia
Cerebral oedema
Staffing needs
More prone for hypotension UF 10–13 mL/kg/hr
Cardiac stability better preserved44 Up to 300 mL/hr only
Overcorrection risk is higher? Slower correction of sodium47
Risk is higher48,49
Dialysis nurse required
Less risk
Might not require dedicated dialysis staff
HRS: hepatorenal syndrome; N/A: not applicable; RRT: renal replacement therapy.
portal hypertension is called portopulmonary hypertension. All patients who are candidates for LT should be screened for portopulmonary hypertension by transthoracic echocardiography. Those with right ventricular systolic pressures greater than 45 mmHg should undergo right heart catheterisation.29 Mean pulmonary artery pressure greater than 35 mmHg is associated with increased operative risk, and should be treated prior to LT.30
Anaesthesia for LT has dramatically changed in the past three decades. As high-risk patients became candidates for LT, the risk for intraoperative complications has also increased. With the new MELD-NA scoring system, more patients with hyponatraemia are likely to be transplanted due to incorporation of the serum sodium in scoring. The risk of central pontine myelinolysis if serum sodium is corrected too rapidly is increased.31
All these variables, in conjunction with the use of more marginal organs, can result in more challenging management from an anaesthesia standpoint. Each stage during LT surgery incorporates its own set of challenges, and deep understanding of the physiologic derangements that each stage represents will decrease morbidity and mortality.
THREE STAGES OF SURGERY
Pre-anhepatic Stage
This stage starts from the surgical incision, and ends with freeing the native (diseased) liver from the vascular access by clamping the inferior vena cava (IVC), hepatic artery, and hepatic portal vein. Bleeding is common at this stage of surgery, and sometimes, massive transfusions are needed.
Surgical techniques currently used for LT include the conventional caval reconstruction technique. Conventional caval reconstruction involves recipient hepatectomy, including the retro-hepatic vena cava. This technique will cause occlusion of the vena cava and portal vein.32 This will result in a severe reduction in preload to the right heart during the anhepatic phase. Overcompensation with aggressive volume expansion can become detrimental, as this volume will return the circulation after unclamping. Hypervolaemia can lead to venous congestion and poor function in the newly transplanted graft. Second, the piggyback technique involves hepatectomy with preservation of native retro-hepatic vena cava. This technique also has a few shortcomings, which include outflow obstruction, specifically in the hepatic venous cuff anastomosis.33 Haemodynamics are usually more stable than with a full clamp.
RRT in HRS Intermittent RRT Continuous RRT
Table 2: Advantages and disadvantages of intermittent and continous modalities during surgery.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 63 Article
The application of veno-venous bypass is still justifiable in certain patient populations.34 With this technique, venous blood from the IVC and femoral vein is returned into the internal jugular vein using extracorporeal veno-venous cannulas and a centrifugal pump. This practice is decreasing due to lack of clinical evidence to support its use.35
Anhepatic Stage
The anhepatic stage begins with the occlusion of blood supply to the native liver (clamping the IVC), and ends with reperfusion of the new graft. Decreased blood flow below the diaphragm (from clamping the IVC) can cause worsening of metabolic acidosis.
In this phase, the new graft is anastomosed. Coagulopathy, hyperkalaemia, and acidemia are common, as the liver is rendered metabolically ineffective. The patient should be metabolically optimised by the anaesthesiologist to set up the stage for the reperfusion phase.36
Neohepatic Stage
This phase starts with reperfusion of the donor liver. As the IVC is ‘open’, venous blood will return to the right heart, with subsequent improvement in cardiac output. However, this improvement in haemodynamics will come at a cost. After the portal vein is open, acidotic and hyperkalaemic blood from below the clamp and from the graft itself will return to the right heart.31 In addition, toxins that have been accumulating in the enteric system while the portal vein is clamped, will be reintroduced into the general circulation.37 Severe hypotension upon unclamping is called reperfusion syndrome and can happen in up to 12.1–31.6% of patients.38-40 This can improve with the administration of calcium chloride, bicarbonate, and vasopressors.31
ROLE OF CONTINOUS RENAL REPLACEMENT THERAPY DURING LIVER TRANSPLANT
Risk factors for AKI during surgery include a full caval clamp, long anhepatic time, or prolonged hypotension. A selected group of patients with volume overload, hyperkalaemia, hyponatraemia, or preoperative AKI may benefit from the use of
CRRT that can be started in the operating room or after arrival to the intensive care unit.31 RRT in AKI can not only control electrolytes and acid-base status, but can also avoid positive fluid balance, which is associated with adverse outcomes in critically ill patients.
CRRT provides enhanced haemodynamic tolerance, sustained acid-base, and azotaemia control. The premise on the use of intraoperative CRRT in LT is based on the rationale that patients with impaired kidney function will poorly tolerate fluid shifts and metabolic disturbances during the intraoperative period. The use of intraoperative CRRT has been proven safe with no significant difference in complications, compared with patients that underwent a classic approach (Table 1).41
From these studies, the authors can conclude that perioperative (including intraoperative) RRT is feasible and safe, with outcomes that were not significantly worse than in those who did not need it. The modality most used was CRRT, except one study, which used intermittent dialysis.
There are risks and benefits of each modality of RRT. Table 2 briefly summarises the advantages and disadvantages of intermittent and continuous modalities of dialysis.
Liver Transplant
In 2023, 10,660 LTs were done in the USA, as per UNOS data.50
Benefits of Preoperative CRRT in Liver Transplant
RRT can correct electrolyte and acid-base abnormalities, and optimise volume status by ultrafiltration in the setting of fluid overload.
Benefits and Challenges of Continuous Renal Replacement Therapy Intraoperatively
As previously described, it is possible intraoperatively to develop acidemia, hyperkalaemia, rapid correction of hyponatraemia. RRT can help prevent this or at least limit the severity of these electrolyte and acid-base issues.
64 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Bleeding is common during surgery, and the need for blood transfusions (sometimes massive transfusions) is common.51 This can lead to significantly lowered filling pressures. Volume expansion should be a balance between maintaining a low central venous pressure and maintaining adequate cardiac filling pressures in the setting of ongoing blood loss.
Clotting of dialysis filters is an amplified complication of CRRT here, because of decreased anticoagulation use, due to high bleeding risk with heparin. Citrate-based anticoagulation should be used with caution in liver disease, due to unpredictable metabolic clearance.52 Citrate accumulation can also occur when the rate of citrate metabolism exceeds hepatic metabolism, leading to metabolic alkalosis.53
In one study,54 citrate-based anticoagulation was done in patients with liver disease with close monitoring of acid-base parameters. They identified that a prothrombin time ≤26% and a serum lactate level ≥3.4 mmol/L was useful for predicting citrate accumulation. A reduced dose of citrate infusion might be warranted in liver disease.
Methods to offset circuit clotting
Methods to offset circuit clotting include: flushing the extracorporeal circuit with normal saline every 30–60 minutes; use of rostacyclin as anticoagulation in the extracorporeal circuit;55 and use of serine protease inhibitors nafamostat mesylate and kallikrein.56
Intermittent Haemodialysis During Liver Transplant Surgery
Most of the studies in Table 1 used CRRT during surgery. Life-threatening hyperkalaemia or acidosis that develops intraoperatively can be corrected by haemodialysis more rapidly.
The study by Mitra et al.45 noted 1-year survival of 80% in patients who had intraoperative haemodialysis. The concern with intermittent dialysis is hypotension and neurological complications from rapid solute shifts and hypotension.
This study showed that intraoperative haemodialysis is possible, though it must be noted that unstable patients were on CRRT before surgery in that study. In patients with an arteriovenous fistula, sustained low efficiency dialysis can be a safe option to avoid dialysis catheter-related infections. Sustained low efficiency dialysis can also be a safer alternative to intermittent haemodialysis intraoperatively.
Assessing Renal Recovery Post-op
AKI is a common complication post-LT.57 Some of the risk factors associated with post-LT AKI are unique from other medical and surgical causes of AKI.58 These include hepatic reperfusion injury and marginal graft use.59 Assessment of renal recovery could be hampered if liver function is impaired, as creatinine-based estimated GFR can be overestimated in liver dysfunction.60 AKI based on urine output or cystatin-based measurements can be more accurate to assess renal solute clearance.61
One study showed renal recovery of AKI post-LT was 33% among those who had an estimated GFR <30 mL/min (MDRD6).62
CONCLUSION
ESLD is associated with high mortality. LT is the definitive treatment and is a complex surgery. The risk of renal dysfunction with liver cirrhosis during the surgery is high. Perioperative RRT could help correct or prevent some of the electrolyte and acid-base abnormalities encountered during surgery.
There are challenges with RRT during LT, but the authors reviewed studies that have shown that it is safe, feasible, and with potential benefits. This would require interdisciplinary co-ordination and expertise, but the benefits include less complications, better outcomes, and possibly even decreased length of stay. Defined protocols for implementing intraoperative RRT should include vascular access, modality of RRT, timing of initiation (how soon during surgery), and anticoagulation.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 65 Article
References
1. Nadim MK, Garcia-Tsao G. Acute kidney injury in patients with cirrhosis. N Engl J Med. 2023;388(8):733-45.
2. Fede G et al. Renal failure and cirrhosis: a systematic review of mortality and prognosis. J Hepatol. 2012;56(4):810-8.
3. D'Amico G et al. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217-31.
4. Mendoza A et al. Liver transplantation for fulminant hepatic failure: importance of renal failure. Transpl Int. 1997;10:55-60.
5. Sethi A et al. Kidney function and mortality post-liver transplant in the Model for End-Stage Liver Disease era. Int J Nephrol Renovasc Dis. 2011;4:139-44.
6. Bohorquez H et al. Intraoperative renal replacement therapy in orthotopic liver transplantation. Adv Kidney Dis Health. 2023;30(4):378-86.
7. Ruiz R et al. Long-term analysis of combined liver and kidney transplantation at a single center. Arch Surg. 2006;141(8):735-41.
8. Gonwa TA et al. Continued influence of preoperative renal function on outcome of orthotopic liver transplant (OLTX) in the US: where will MELD lead us? Am J Transplant. 2006;6(11):2651-9.
9. Townsend DR et al. Intraoperative renal support during liver transplant. Liver Transplant. 2009;15(1):73-8.
10. Kotin P, Hall EM. “Cardiac” or congestive cirrhosis of the liver. Am J Pathol. 1951;27:561-71.
11. Møller S et al. Pathophysiological basis of pharmacotherapy in the hepatorenal syndrome. Scand J Gastroenterol. 2005;40(5):491500.
12. Hemprich U et al. Respiratory failure and hypoxemia in the cirrhotic patient including hepatopulmonary syndrome. Curr Opin Anesthesiol. 2010;23(2):1338.
13. Ramsay M. Portopulmonary hypertension and right heart failure in patients with cirrhosis. Curr Opin Anesthesiol. 2010;23(2):145-50.
14. Melzer J, Brentjens TE. Renal failure in patients with cirrhosis: hepatorenal syndrome and renal support strategies. Curr Opin
Anesthesiol. 2010;23(2):139-44.
15. Hoetzel A et al. Anesthetic considerations for the patient with liver disease. Curr Opin Anesthesiol. 2012;25(3):340-7.
16. Leise MD et al. Effect of the pretransplant serum sodium concentration on outcomes following liver transplantation. Liver Transpl. 2014;20(6):687-97.
17. Hassanein M et al. Dysnatremias, mortality, and kidney failure in CKD: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Kidney Med. 2022;4(12):100554.
18. Verbeek TA et al. Hyponatremia and liver transplantation: a narrative review. J Cardiothorac Vasc Anesth. 2021;DOI:10.1053/j. jvca.2021.05.027.
19. Romanovsky A et al. Serum sodium shift in hyponatremic patients undergoing liver transplantation: a retrospective cohort study. Ren Fail. 2015;37(1):37-44.
20. Jipa LN et al. The interrelation between arterial lactate levels and postoperative outcome following liver transplantation. Rom J Anaesth Intensive Care. 2014;21(2):106-12.
21. Yudkin J, Cohen RD. The contribution of the kidney to the removal of a lactic acid load under normal and acidotic conditions in the conscious rat. Clin Sci Mol Med. 1975;48(2):121-31.
22. Leal-Pinto E et al. Metabolism of lactate by the intact functioning kidney of the dog. Am J Physiol. 1973;224(6):1463-7.
23. Bellomo R. Bench-to-bedside review: lactate and the kidney. Crit Care. 2002;6(4):322-6.
24. Dawson AG. Contribution of pH sensitive metabolic processes to pH homeostasis in isolated rat kidney tubules. Biochim Biophys Acta. 1977;499(1):85-98.
25. Shapiro JI et al. Brain pH responses to sodium bicarbonate and carbicarb during systemic acidosis. Am J Physiol. 1989;256(5 Pt 2):H1316-21.
26. Cingolani HE et al. Depression of human myocardial contractility with "respiratory" and "metabolic" acidosis. Surgery. 1975;77(3):42732.
27. Cooper DJ et al. Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled
clinical study. Ann Intern Med. 1990;112(7):492-8.
28. Hilton PJ et al. Bicarbonate-based haemofiltration in the management of acute renal failure with lactic acidosis. QJM. 1998;91(4):279-83.
29. Akhtar S. Preoperative evaluation of geriatric patients undergoing liver transplantation. Curr Opin Anaesthesiol. 2022;35(1):96-104.
30. Savale L, Manes A. Pulmonary arterial hypertension populations of special interest: portopulmonary hypertension and pulmonary arterial hypertension associated with congenital heart disease. Eur Heart J. 2019;21(Suppl K):37-45.
31. Adelmann D et al. Anesthesia for liver transplantation. Anesthesiol Clin. 2017;35(3):491-508.
32. Tzakis A et al. Orthotopic liver transplantation with preservation of the inferior vena cava. Ann Surg. 1989;210(5):649-52.
33. Nishida S et al. Piggyback technique in adult orthotopic liver transplantation: an analysis of 1067 liver transplants at a single center. HPB (Oxford). 2006;8(3):182-8.
34. Fonouni H et al. The need for venovenous bypass in liver transplantation. HPB (Oxford). 2008;10(3):196-203.
35. Gurusamy KS et al. Venovenous bypass versus none for liver transplantation. Cochrane Database Syst Rev. 2011;(3):CD007712.
36. Dalal A. Anesthesia for liver transplantation. Transplant Rev (Orlando). 2016;30(1):51-60.
37. Jeong SM. Postreperfusion syndrome during liver transplantation. Korean J Anesthesiol. 2015;68(6):527-39.
38. Aggarwal S et al. Postreperfusion syndrome: cardiovascular collapse following hepatic reperfusion during liver transplantation. Transplant Proc. 1987;19(4 Suppl 3):54-5.
39. Bukowicka B et al. The occurrence of postreperfusion syndrome in orthotopic liver transplantation and its significance in terms of complications and shortterm survival. Ann Transplant. 2011;16(2):26-30.
40. Fukazawa K et al. Hemodynamic recovery following postreperfusion syndrome in liver transplantation. J Cardiothorac Vasc Anesth. 2014;28(4):1006-14.
66 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
41. Karvellas CJ et al. Intraoperative continuous renal replacement therapy during liver transplantation: a pilot randomized-controlled trial (INCEPTION). Can J Anesth. 2019;66(10):1151-61.
42. Douthitt L et al. Perioperative use of continuous renal replacement therapy for orthotopic liver transplantation. Transplant Proc. 2012;44(5):1314-7.
43. LaMattina JC et al. Intraoperative continuous veno-venous hemofiltration facilitates surgery in liver transplant patients with acute renal failure. Transplant Proc. 2015;47(6):1901-4.
44. Nadim Mitra K et al. Intraoperative hemodialysis during liver transplantation: a decade of experience. Liver Transpl. 2014;20(7):756-64.
45. Fehervari I et al. Mitigation of cytokine storm by intraoperative use of renal replacement therapy during combined liver-kidney transplantation. Transplant Proc. 2010;42(6):2353-6.
46. Kościelska M et al. Intraoperative dialysis during liver transplantation. Transplant Proc. 2020;52(8):24548.
47. Larner AJ et al. Correction of severe hyponatraemia by continuous arteriovenous haemofiltration before liver transplantation. BMJ. 1988;297(6662):1514-5.
48. Davenport A et al. Continuous arteriovenous haemofiltration
in patients with hepatic encephalopathy and renal failure. Br Med J. 1987;295(6605):1028.
49. Arieff AI. Dialysis disequilibrium syndrome: current concepts on pathogenesis and prevention. Kidney Int. 1994;45(3):629-35.
50. Organ Procurement and Transplantation Network (OPTN). National data. Available at: https:// optn.transplant.hrsa.gov/data/viewdata-reports/national-data/#. Last accessed: 6 March 2024.
51. Ramos E et al. Intraoperative red blood cell transfusion in liver transplantation: influence on patient outcome, prediction of requirements, and measures to reduce them. Liver Transpl. 2003;9(12):1320-7.
52. Apsner R et al. Impairment of citrate metabolism in acute hepatic failure. Wien Klin Wochenschr. 1997;109(4):123-7.
53. Mehta RL et al. Regional citrate anticoagulation for continuous arteriovenous hemodialysis in critically ill patients. Kidney Int. 1990;38(5):976-81.
54. Schultheiß C et al. Continuous venovenous hemodialysis with regional citrate anticoagulation in patients with liver failure: a prospective observational study. Critical Care. 2012;16(4):R162.
55. Davenport A et al. Comparison of the use of standard heparin and prostacyclin anticoagulation in spontaneous and pump driven
extracorporeal circuits in patients with combined acute renal and hepatic failure. Nephron. 1994;66(4):431-7.
56. Davenport A. Continuous renal replacement therapies in patients with liver disease. Semin Dial. 2009;22(2):169-72.
57. Mokdad AA et al. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysis. BMC medicine. 2014;12(1):145.
58. Lee HC et al. Prediction of acute kidney injury after liver transplantation: machine learning approaches vs. logistic regression model. J Clin Med. 2018;7(11):428.
59. Pérez GS et al. Central pontine myelinolysis in a liver transplant recipient. Medicina Intensiva. 2004;28(2):83-5.
60. Beben T, Rifkin DE. GFR estimating equations and liver disease. Adv Chronic Kidney Dis. 2015;22(5):337-42.
61. Mindikoglu AL et al. Performance of chronic kidney disease epidemiology collaboration creatinine‐cystatin C equation for estimating kidney function in cirrhosis. Hepatology. 2014;59(4):1532-42.
62. Singal AK et al. Biomarkers of renal injury in cirrhosis: association with acute kidney injury and recovery after liver transplantation. Nephron. 2018;138(1):1-12.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 67 Article FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Staphylococcus aureus Bacteraemia in Patients with Chronic Kidney Disease: Single-Centre Data from Pakistan
Authors:
Disclosure:
*Safia Moin,1 Bina Salman,1 Aasim Ahmad1
1. The Kidney Centre Postgraduate Training Institute, Karachi, Pakistan
*Correspondence to saphiaowais@gmail.com
The authors have declared no conflicts of interest.
Received: 14.09.23
Accepted: 22.01.24
Keywords:
Methicillin-resistant Staphylococcus aureus (MRSA), methicillinsensitive Staphylococcus aureus (MSSA), Staphylococcus aureus bacteraemia (SAB).
Citation: EMJ. 2024;9[1]:68-76. DOI/10.33590/emj/10304613. https://doi.org/10.33590/emj/10304613.
Abstract
Background: Infection, especially Staphylococcus aureus bacteraemia (SAB), increases morbidity and mortality in patients with chronic kidney disease (CKD), particularly those who are dialysis-dependent. This study describes the clinical features of SAB amongst patients with CKD.
Method: The authors planned a retrospective observational study of adult patients with CKD and SAB from January 2021–June 2022. Microbiology laboratory data and hospital medical records were reviewed. All detailed clinical data, including baseline characteristics, source of infection, management, methicillin susceptibility of S. aureus isolates, and outcome, were collected. The association between baseline characteristics, source of infection, management, and outcome of patients, was examined.
Results: The authors included 49 patients in their study. Methicillin-resistant S. aureus was more prevalent (35 out of 49; 71.4%) than methicillin-sensitive S. aureus (14 out of 49; 28.6%). Central venous catheter was the most common source of infection (38 out of 49; 77.6%). Most patients recovered (26 out of 49; 53.1%), while 12 (24.5%) were referred to other hospitals. Four patients expired. Methicillin-resistant S. aureus bacteraemia had higher mortality than methicillinsensitive S. aureus bacteraemia. Central line-associated bloodstream infections showed higher mortality than other sources of infection, although due to a small sample size, this difference could not be proven statistically. SAB showed significant association with patient outcomes. The central venous catheter could not be removed in three of four expired patients (p=0.018).
Conclusion: SAB is a serious but preventable nosocomial infection in patients with CKD who are dependent on dialysis. Strict infection prevention measures are needed to prevent hospital-acquired infections in these patients.
68 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Key Points
1. Staphylococcus aureus bacteraemia is the most common cause of infection in patients with chronic kidney disease who are dialysis-dependent. This paper adds to the existing data from Pakistan.
2. This article describes the association between baseline characteristics, the source of infection, management of, and outcomes of patients with S. aureus bacteraemia. Methicillin-resistant S. aureus bacteraemia had higher mortality than methicillin-sensitive S. aureus bacteraemia. Central lineassociated bloodstream infection showed higher mortality than other sources of infection.
3. S. aureus bacteraemia is a serious but preventable nosocomial infection in patients with CKD who are dialysis-dependent. Strict infection prevention measures are needed to prevent hospital-acquired infections in these patients.
INTRODUCTION
Patients with chronic kidney disease (CKD), especially those on chronic haemodialysis (HD), have a higher incidence of nosocomial infection than non-dialysis-dependent patients who are hospitalised, due to repeated exposure to the healthcare environment. Mortality from all causes in patients on dialysis treatment is 6.5–7.9 times higher than that of the general population. In patients ≥65 years of age, mortality from infection is two times higher than that in a population of the same age with other comorbidities, such as diabetes, neoplasms, or congestive heart failure.1-3 The risk and incidence of infection increases with catheter use for vascular access.4,5 Staphylococcus aureus bacteraemia (SAB) is a leading cause of infection in these patients.6,7
S. aureus (SA) is a part of normal skin flora, and is the most common cause of bacteraemia in patients who are dependent on HD. Repeated hospital exposure, intravascular catheter use, invasive procedures, skin barrier disruption, and impaired renal function increase the risk of SAB in these patients.8 SAB has many complications, as well as increased morbidity and mortality.9 It is associated with severe, often fatal complications, such as endocarditis, osteomyelitis, septic arthritis, empyema thoracis, pneumonia, and meningitis, despite relevant antibiotic treatment.10 Methicillin-resistant S. aureus (MRSA) bacteraemia has a higher risk of mortality than methicillin-sensitive S. aureus (MSSA) bacteraemia.11
The authors’ institution, The Kidney Centre Postgraduate Training Institute, Karachi, Pakistan, is a not-for-profit specialised hospital, which provides care to patients with kidney disease. It is mainly a renal disease centre, with a large dialysis unit. Around 200 dialysis sessions take place per day at the institute. Multiple patients are awaiting renal transplant, and they need access for dialysis, usually through an arteriovenous fistula (AVF), which takes at least a few weeks to mature. During this period, dialysis is carried out via central venous catheters (CVC).12 Central line-associated blood stream infection (CLABSI), especially with SA, is a very commonly encountered hospital-acquired infection in these patients. Previous studies from Pakistan show that there is a high burden of SA infection, especially with MRSA, in this patient group.13,14 There are limited reports on the clinical features and outcomes of SAB in patients with CKD in Pakistan. More local data are required to see the current burden of infection, especially with a preventable cause like SAB, in this patient group; this will highlight the importance of preventing infections, especially SAB. This study describes the clinical features of SAB among patients with CKD at a tertiary care renal centre.
METHODS
The authors carried out a retrospective observational study of patients with SAB from January 2021–June 2022. All patients with SAB who were registered at The Kidney Centre Postgraduate Training Institute were
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 69 Article
included in the study; this included all admitted patients, those routinely receiving dialysis at the institution, and those who presented to the emergency room. The authors excluded all non-registered patients, and all cases with bacteraemia with other organisms. Exemption was obtained from the ethical review committee of the institute (ref. no. 152-IDC102022[EXEMPTION]).
Microbiology laboratory data and hospital medical records were reviewed. All detailed clinical data, including baseline characteristics, source of infection, management, methicillin susceptibility of SA isolates, and outcome, were collected. Association between baseline characteristics, source of infection, management, and outcome of patients was examined.
STATISTICAL ANALYSIS
The data were analysed using IBM SPSS Statistics version 26.0 (IBM, Armonk, New York, USA). Mean with standard deviation was evaluated for continuous variables, while frequency with percentage was calculated for categorical data. Association among the following variables was observed with the patient outcome, using the chi-squared test: methicillin susceptibility of SA; source of infection; type and site of line; central line management; and treatment. A p value of ≤0.05 was considered significant.
RESULTS
The authors included 49 patients in this study, with a female to male ratio of 1.00:1.58, and a mean age of 51.0±18.4 years (minimum: 9 years; maximum: 91 years). Hypertension (36 out of 49; 61.2%) and diabetes (27 out of 49; 55.1%) were the most prevalent comorbidities. Diabetic nephropathy was the major known cause of CKD (10 out of 49; 20.4%; Table 1A).
MRSA was more prevalent (35 out of 49; 71.4%) than MSSA (14 out of 49; 28.6%). CVC was the most common source of infection (38 out of 49; 77.6%). Most of the CVCs were temporary (22 out of 49; 44.9%). Internal jugular (28 out of 49; 57.1%) was the most common line insertion site. In most cases, vancomycin was the drug of
choice (34 out of 49; 69.4%; Table 1B). Most patients recovered (26 out of 49; 53.1%), while 12 (24.5%) were referred to other hospitals (Figure 1).
Three (75.0%) of four expired patients were male, although this was statistically insignificant (p=0.064). All four patients who died had hypertension, and three (75.0%) were also diabetic, but this was also statistically insignificant. Since the authors’ institute is a specialised hospital for renal diseases, and does not offer treatment for COVID-19 infection, almost all patients who tested positive were referred to COVID-19 care facilities. One patient who tested positive expired (Table 2A).
MRSA bacteraemia had a higher mortality rate than MSSA bacteraemia. Similarly, CLABSI showed higher mortality than the other sources of infection, although due to a small sample size, this difference could not be proven statistically (Table 2B).
The management of SAB showed a significant association with patient outcomes. The CVC could not be removed in three of four expired patients due to non-availability of venous access for dialysis (p=0.018; Table 2C).
DISCUSSION
SAB is a leading cause of infection in patients with CKD who are dialysis-dependent, due to vascular access and repeated hospital exposures. According to a report by the Centers for Disease Control and Prevention (CDC), patients who were dialysis-dependent were 100 times more likely to have an SAB than adults not on dialysis.15 This can be prevented by appropriate infection prevention and control strategies.
Though a lot of international data are available, as a first step, it is important to know the burden of this infection in the authors’ patient population. They retrospectively observed the clinical features of patients with CKD and SAB at a tertiary specialised hospital for renal care. CVC was the major source of SAB in their patients, and MRSA dominated MSSA. Most of the patients were empirically started on meropenem and vancomycin, with the continuation of vancomycin and discontinuation of meropenem after the
Article 70 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
finalisation of cultures. Timely source removal and appropriate antibiotic use were associated with survival.
SAB causes higher morbidity and mortality rates in patients with CKD, especially those who are dialysis-dependent, as compared to patients without CKD. Cheon et al.16 compared the clinical outcomes associated with SAB in patients with and without CKD. High Sequential Organ Failure
Assessment (SOFA) score and proportion of administration of inappropriate antibiotics were associated with CKD.16 In a cross-sectional study from Rawalpindi, Pakistan, Jamil et al.17 determined the prevalence of bacteraemia in patients with CKD, particularly those on dialysis, and those with renal transplants. They reported the frequency of SAB among patients with CKD and on haemodialysis to be 15%.17 MRSA prevalence was detected to be 2%.
Mean±Standard Deviation (n; %) Total=59 Age (years) 51±18.4 Sex Male 30 (61.2) Female 19 (38.8) Comorbidities Anaemia 5 (10.2) Atherosclerosis 3 (6.1) Benign prostatic hyperplasia 1 (2.0) Carcinoma breast 1 (2.0) Cerebrovascular accident 2 (4.1) COVID-19 6 (12.2) Dermatitis 1 (2.0) Diabetes 27 (55.1) Diabetic retinopathy 3 (6.1) Hypertension 36 (73.5) Ischaemic heart disease 11 (22.4) Other lower respiratory tract infection 9 (18.4) Prostate neoplasia 1 (2.0) Subclavian steal syndrome 1 (2.0) Transient ischaemic attack 1 (2.0) Septic arthritis 3 (6.1) Autoimmune polycystic kidney disease 1 (2.0) Cause of chronic kidney disease Diabetes 10 (20.4) Hypertension 5 (10.2) Glomerulonephritis 3 (6.1) Lupus 1 (2.0) Nephrolithiasis 7 (14.3) Nonspecific causes of chronic kidney disease 19 (38.8) Other obstructive uropathy 3 (6.1)
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 71
Table 1A: Baseline characteristics of patients.
Haemodialysis vascular access, particularly when using a CVC, increases the risk of SAB and sepsis compared to AVF.12,18,19 Long-term CVC is associated with serious complications, such as CLABSI.20 In a previous study from the authors’ institute, Qureshi et al.12 concluded that out of a total of 429 non-tunneled catheters, 50 (17%) were removed due to CLABSI. In these findings, MRSA was the most common organism responsible.12 The authors’ findings are consistent with this. CLABSI (38 out of 49; 77.6%) was the major source of infection in the studied cohort, with a predominance of MRSA (35 out of 49; 71.4%).
In a similar study from Pakistan, Shahnila et al.13 described the clinical presentation of SAB, and outcomes from a tertiary care hospital. SAB increases morbidity and mortality in patients with CKD. Haemodialysis and CVCs were the major risk factors of SAB. Similar to the authors’
findings, out of 92 patients, 81 (88%) had MRSA, and 11 (12%) MSSA. MRSA bacteraemia presented with more complications.13
MRSA bacteraemia possesses a higher risk of mortality compared to MSSA bacteraemia.11 Of the authors’ four patients who expired, three had MRSA bacteraemia. Multiple studies from Pakistan have previously reported the increasing frequency of emerging resistance to methicillin in SA.14,21,22 In a descriptive study in Rawalpindi, Ali et al.14 recovered 100 (42.01%) MRSA samples from 238 SA isolates, in different clinical samples.
SAB has increased the mortality rate in patients with COVID-19.23 The authors had six patients with both SAB and COVID-19. Five of these were referred to COVID-19 care facilities. One patient with MRSA bacteraemia and COVID-19 expired, as a result of an AVF infection.
Methicillin susceptibility of Staphylococcus aureus Methicillin-resistant Staphylococcus aureus 35 (71.4) Methicillin-sensitive Staphylococcus aureus 14 (28.6) Source of infection Central line 38 (77.6) Arteriovenous fistula infection 7 (14.3) Surgical site infection 3 (6.1) Urosepsis 1 (2.0) Type of line Temporary 22 (57.9) Permacath 16 (42.1) Site of line Internal jugular 28 (73.6) Femoral 10 (26.3) Line management Central line removed 26 (68.4) Central line salvaged 11 (28.9) Lock therapy 1 (2.6) Treatment Vancomycin 34 (69.4) Meropenem 7 (14.3) Piperacillin-tazobactam 2 (4.1) Meropenem+clindamycin 1 (2.0) Cefoperazone-sulbactam 1 (2.0) None 4 (8.2)
Article 72 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Table 1B: Clinical parameters of patients (n; %).
LAMA:
left against medical advice.
Baseline Parameters Patient Outcomes P value Recovered Referred Left against medical advice Expired Gender Male 15 (57.7) 5 (41.7) 7 (100.0) 3 (75.0) 0.064 Female 11 (42.3) 7 (58.3) 0 (0.0) 1 (25.0) Age ≤40 years 8 (30.8) 3 (25.0) 1 (14.3) 2 (50.0) 0.383 41–60 years 13 (50.0) 4 (33.3) 4 (57.1) 0 (0.0) >60 years 5 (19.2) 5 (41.7) 29 (28.6) 2 (50.0) Hypertension Yes 18 (69.2) 9 (75.0) 5 (71.4) 4 (100.0) 0.813 No 8 (30.8) 3 (25.0) 2 (28.6) 0 (0.0) Diabetes Yes 13 (50.0) 8 (66.7) 3 (42.9) 3 (75.0) 0.631 No 13 (50.0) 4 (33.3) 4 (57.1) 1 (25.0) Ischaemic heart disease Yes 5 (19.2) 3 (25.0) 2 (28.6) 1 (25.0) 0.908 No 21 (80.8) 9 (75.0) 5 (71.4) 3 (75.0) COVID-19 Yes 0 (0.0) 5 (41.7) 0 (0.0) 1 (25.0) 0.002 No 26 (100.0) 7 (58.3) 7 (100.0) 3 (75.0)
0 Recovered 26/53 Referred 12/24 LAMA 7/14 Expired 4/8 5 10 15 20 25 30 Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 73
Figure 1: Patient outcomes.
Table 2A: Association between baseline characteristics and patient outcomes (n; %).
Despite timely treatment with vancomycin, the patient succumbed.
The clinical presentation of SAB might differ from previous patients with SAB. Changes in the characteristics of the patient population, as well as clinical and molecular epidemiology of SAB in patients receiving maintenance HD, and in the clones causing SAB, may contribute to increased morbidity and mortality.24,25
The small sample size is the major limitation of the authors’ study, and means that statistical significance could not be proven in many of their findings. The authors were unable to follow their patients for SAB complications. Despite this, their research supports that SAB led to increased
morbidity and mortality in their institution’s patients with CKD who are dialysis-dependent.
Preventive measures need to be prioritised. Catheter locks should be considered when the CVC needs to be salvaged. There needs to be a focus on improving infection prevention protocols. An appropriate staff-to-patient ratio with strict infection prevention measures is needed to prevent SAB in patients undergoing dialysis. MRSA decolonisation can be an option to decrease the chances of SAB in those who are colonised.19 Better antimicrobial surveillance is needed to decrease emerging antimicrobial resistance. To prevent SAB, the first step can be detecting CKD in its early stages to prevent or delay the need for dialysis, including methods
parameters Patient Outcomes P value Recovered
Type of Staphylococcus aureus Methicillinresistant Staphylococcus aureus 20 (76.9) 9 (75.0) 3 (42.9) 3 (75.0) 0.364 Methicillinsensitive Staphylococcus aureus 6 (23.1) 3 (25.0) 4 (57.1) 1 (25.0) Source of Infection Central lineassociated bloodstream infection 23 (88.5) 8 (66.7) 4 (57.1) 3 (75.0) 0.219 Arteriovenous fistula infection 1 (3.8) 3 (25.0) 2 (28.6) 1 (25.0) Surgical site infection 1 (3.8) 1 (8.3) 1 (14.3) 0 (0.0) Urosepsis 1 (3.8) 0 (0.0) 0 (0.0) 0 (0.0) Type of Line Temporary 13 (50.0) 5 (41.7) 2 (28.6) 2 (50.0) 0.571 Permacath 10 (38.5) 3 (25.0) 2 (28.6) 1 (25.0) None 3 (11.5) 4 (33.3) 3 (42.9) 1 (25.0) Site of Line Internal jugular 18 (69.2) 4 (33.3) 3 (42.9) 3 (75.0) 0.221 Femoral 5 (19.2) 4 (33.3) 19 (14.3) 0 (0.0) None 3 (16.5) 4 (33.3) 3 (43.9) 1 (25.0)
Infection
Referred Left against medical advice Expired
Article 74 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Table 2B: Association between infection variables and outcome of the patients (n; %).
N/A: not applicable.
to manage diabetes and high blood pressure, as well as providing education on treatment options among all patients, particularly those at greatest risk, to slow the progression of CKD.15
CONCLUSION
SAB is a serious but preventable nosocomial infection in patients with CKD who are dialysisdependent. Strict infection prevention measures are needed to prevent hospital-acquired infections in these patients.
References
1. U.S. Department of Health and Human Services. United States Renal Data System (USRDS). 2013. Available at: https://health.gov/ healthypeople/objectives-anddata/data-sources-and-methods/ data-sources/united-states-renaldata-system-usrds. Last accessed: 7 February 2024.
2. Mohamed H et al. Determinants and outcomes of access-related bloodstream infections among Irish haemodialysis patients; a cohort study. BMC Nephrol. 2019;20(1):68.
3. Fram D et al. Risk factors for bloodstream infection in patients at a Brazilian hemodialysis center: a case-control study. BMC Infect Dis. 2015;15:158.
4. D’Agata EM et al. Hospitalacquired infections among chronic hemodialysis patients. Am J Kidney Dis. 2000;35(6):1083-8.
5. Lata C et al. Catheter-related bloodstream infection in endstage kidney disease: a Canadian narrative review. Can J Kidney Health Dis. 2016;3:24.
Variables of Management Patient Outcomes P value Recovered Referred Left against medical advice Expired Central Line Management Central line removed 18 (73.1) 3 (25.0) 3 (42.9) 1 (25.0) 0.018 Central line salvaged 6 (23.1) 9 (75.0) 4 (57.1) 3 (75.0) Lock therapy 1 (3.8) 0 (0.0) 0 (0.0) 0 (0.0) Treatment Vancomycin 25 (96.2) 3 (25.0) 3 (42.9) 3 (75.0) <0.001 Meropenem 0 (0.0) N/A 3 (42.9) 1 (25.0) Piperacillintazobactam 0 (0.0) 2 (16.7) 0 (0.0) 0 (0.0) Meropenem+ clindamycin 1 (3.8) 0 (0.0) 0 (0.0) 0 (0.0) Cefoperazonesulbactam 0 (0.0) 1 (8.3) 0 (0.0) 0 (0.0) None 0 (0.0) 3 (25.0) 1 (14.3) 0 (0.0) Type of Line Temporary 13 (50.0) 5 (41.7) 2 (28.6) 2 (50.0) 0.571 Permacath 10 (38.5) 3 (25.0) 2 (28.6) 1 (25.0) None 3 (11.5) 4 (33.3) 3 (42.9) 1 (25.0) Site of Line Internal jugular 18 (69.2) 4 (33.3) 3 (42.9) 3 (75.0) 0.221 Femoral 5 (19.2) 4 (33.3) 19 (14.3) 0 (0.0) None 3 (16.5) 4 (33.3) 3 (43.9) 1 (25.0)
Table 2C: Association between variables of management and patient outcomes (n; %).
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 75
6. Kumbar L, Yee J. Current concepts in hemodialysis vascular access infections. Adv Chronic Kidney Dis. 2019.26(1):16-22.
7. Rojas-Moreno CA et al. Catheterrelated bloodstream infections in patients on emergent hemodialysis. Infect Control Hosp Epidemiol. 2016;37(3):301-5.
8. Chaudry MS et al. Increased risk of Staphylococcus aureus bacteremia in hemodialysis-a nationwide study. Hemodial Int. 2019;23(2):230-8.
9. Kim YS et al. Higher risk for allcause mortality of Staphylococcus aureus bacteremia in patients with non-dialysis dependent chronic kidney disease. Infect Chemother. 2020;52(1):82-92.
10. Nielsen LH et al. Risk and prognosis of Staphylococcus aureus bacteremia among individuals with and without end-stage renal disease: a Danish, populationbased cohort study. BMC Infect Dis. 2015;15:6.
11. Reed SD et al. Costs and outcomes among hemodialysis-dependent patients with methicillin-resistant or methicillin-susceptible Staphylococcus aureus bacteremia. Infect Control Hosp Epidemiol. 2005;26(2):175-83.
12. Qureshi R et al. Reasons for removal of non-tunneled double lumen catheters in incident dialysis patients. J Coll Physicians Surg Pak. 2018;28(4):284-7.
13. Javaid S et al. Clinical features and outcome of Staphylococcus aureus bacteremia from a tertiary care hospital in Pakistan. Infect Dis J Pak. 2022;31(3):89-95.
14. Ali AM et al. Nosocomial infections due to methicillin resistant Staphylococcus aureus in hospitalized patients. Pak J Med Sci. 2007;23(4):593-6.
15. Centers for Disease Control and Prevention (CDC). Black and Hispanic patients on dialysis have higher rates of staph bloodstream infections. Available at: https:// www.cdc.gov/media/releases/2023/ s0206-vs-staph-infection.html. Last accessed: 28 December 2023.
16. Cheon S et al. Outcomes of staphylococcus aureus bacteremia in patients with chronic kidney disease versus without chronic kidney disease. Infect Dis Ther. 2019;7(2):398.
17. Jamil B et al. Bacteremia: prevalence and antimicrobial resistance profiling in chronic kidney diseases and renal transplant patients. J Pak Med Assoc. 2016;66(6):705-9.
18. Piraino B. Staphylococcus aureus infections in dialysis patients: focus on prevention. ASAIO J. 2000;46(6):S13-7.
19. Scheuch M et al. Staphylococcus aureus colonization in hemodialysis patients: a prospective 25 months observational study. BMC Nephrol. 2019;20(1):153.
20. Alby-Laurent F et al. Salvage strategy for long-term central venous catheter-associated Staphylococcus aureus infections in children. Front Pediatr. 2019;6:427.
21. Ahmed K et al. Methicillin resistant Staphylococcus aureus prevalence amongst community versus hospital acquired skin and soft tissue infections. Infect Dis J Pak. 2007;16(1):14-6.
22. Ajmal AN et al. Nosocomial methicillin resistant Staphylococcus aureus frequency in a tertiary care hospital, Lahore, Pakistan. Biomedica. 2009;25(2):97-100.
23. Cusumano JA et al. Staphylococcus aureus bacteremia in patients infected with COVID-19: a case series. Open Forum Infect Dis. 2020;7(11):ofaa518.
24. Souli M et al. Changing characteristics of Staphylococcus aureus bacteremia: results from a 21-year, prospective, longitudinal study. Clin Infect Dis. 2019;69(11):1868-77.
25. Sinclair MR et al. Staphylococcus aureus bacteremia among patients receiving maintenance hemodialysis: trends in clinical characteristics and outcomes. Am J Kidney Dis. 2022;79(3):393-403.e1.
Article 76 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Coexistence of Sickle Cell Thalassaemia with Overlapping Syndrome: A Case Report of Systemic Lupus Erythematosus and Autoimmune Hepatitis
Authors:
*Anjlee Sawlani,1 Rida Masood,1 Jai Kumar,2 Kartaar Saahil3
1. Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan
2. Wayne State University School of Medicine, Detroit, USA
3. Jinnah Sindh Medical University, Karachi, Pakistan
*Correspondence to anjleesawlani56@gmail.com

Disclosure: The authors have declared no conflicts of interest. In accordance with the policies and guidelines of Dow University of Health Sciences, formal Institutional Review Board (IRB) approval is not required for case reports. However, all ethical considerations and principles were followed. Patient privacy and confidentiality were rigorously maintained. Written informed consent was obtained from the patient for publication of this case report and accompanying images. The informed consent form was translated to ensure that the patient and patient’s family, without proficiency in English, fully understood its content and implications. The authors have chosen not to share supporting data associated with this case report. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Sawlani drafted and wrote the entire manuscript, including literature review, case presentation, and conclusions, and conducted data analysis and interpretation of clinical findings. Masood provided clinical care for the patient, conducted follow-up assessments, and contributed to the acquisition of clinical data.
Received: 02.10.23
Accepted: 08.01.24
Citation: EMJ. 2024;9[1]:77-86. DOI/10.33590/emj/11000015. https://doi.org/10.33590/emj/11000015.
Keywords: Autoimmune hepatitis, overlapping syndrome, sickle cell thalassaemia, systemic lupus erythematosus (SLE).
Abstract
This case report highlights a rare and unique occurrence: the simultaneous presence of sickle cell thalassaemia and overlapping syndrome, which involves systemic lupus erythematosus and autoimmune hepatitis. The coexistence of sickle cell disease with overlapping syndrome is exceptionally rare, with only a few documented cases in the literature, one of which involves sickle cell β-thalassaemia. Significantly, this case enhances understanding of the intricate relationship among these conditions, and offers valuable perspectives on how to clinically manage them. The authors present the case of a young male in his early 20s, who presented with haemolytic anaemia, jaundice, joint pain, and hepatomegaly. Extensive laboratory investigations, including serological markers, haemoglobin electrophoresis, and liver function tests, confirmed the coexistence of sickle cell thalassaemia,
Article
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 77
systemic lupus erythematosus, and autoimmune hepatitis. The treatment included O2 therapy, hydration, hydroxyurea, and antibiotics. After 4–5 days, the patient showed improvement, and at discharge, hydroxyurea and folic acid were continued. Significantly, considering the complex medical history of the patient, a decision was made to include a carefully considered, low-dose steroid regimen. The choice of a maintenance dose over an induction therapy was specifically made to mitigate potential complications, particularly the risk of vaso-occlusive crises in patients with sickle cell disease. This case report contributes to the understanding of concurrent manifestation of these complex conditions, and emphasises the importance of a comprehensive approach, early diagnosis, and timely management, to optimise patient outcomes in such intricate overlapping syndromes.
Key Points
1. Importance of recognising overlapping symptoms: this case report emphasises the critical role of physicians in identifying overlapping symptoms, particularly in patients with sickle cell thalassaemia. Recognising the coexistence of autoimmune illnesses is critical for early management and improved patient outcomes.
2. Intricate interplay between sickle cell disease and autoimmunity: the case report discusses the complex relationship between sickle cell disease and autoimmune illnesses, emphasising the elevated risk and clinical implications. Elevated antinuclear antibody levels, possible problems from hydroxyurea, and the nuanced use of steroids highlight the various issues in managing these individuals.
3. Diagnostic complexity and a call for research: the case report emphasises the challenges in diagnosing concurrent autoimmune diseases in patients with sickle cell, due to overlapping clinical characteristics. Comprehensive assessments are required, and the article calls for more research to uncover the underlying processes. This approach seeks to improve diagnosis accuracy, and enable more effective treatment solutions.
INTRODUCTION
Sickle cell disease (SCD) is a genetic condition caused by mutations in the haemoglobin (Hb) gene, resulting in various complications. One specific form of SCD is sickle cell thalassaemia, which occurs by inheriting both sickle cell and thalassaemia traits.1,2 SCD encompasses several other variants, including sickle cell trait, sickle cell anaemia, and sickle cell Hb-C disease, each with distinct characteristics.3,4 Systemic lupus erythematosus (SLE) is a complex autoimmune disease characterised by autoantibodies binding to tissues, forming immune complexes, and causing damage across various organs, leading to chronic inflammation.5 The disease is more prevalent in females, with a female-to-male ratio of 9:1.6 This condition arises when the immune system mistakenly targets healthy cells and tissues, leading to a diverse array of symptoms, including joint pain, fever, fatigue, skin rashes, and potential damage to vital organs, such as the
kidneys, heart, and lungs.7 Autoimmune hepatitis is a chronic liver disease in which the immune system mistakenly attacks liver cells, leading to inflammation and potential damage.8
While SCD has been extensively studied, conditions such as sickle cell thalassaemia and autoimmune disorders that overlap with it remain relatively rare, with only a limited number of reported cases, including a scarcity of sickle cell β-thalassaemia cases.2,8 Although sickle cell thalassaemia and SLE are distinct medical conditions with different underlying pathophysiological mechanisms, they can present with overlapping symptoms, such as anaemia, fever, joint pain, arthritis, and chronic inflammation.1,9 This overlap in clinical manifestations can often lead to difficulties and delays in the diagnosis of SLE in patients with SCD.3 Furthermore, individuals with SCD have compromised activation of the alternate complement pathway, making them more
78 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
susceptible to infections, and potentially prone to autoimmune disorders.4,9 Patients with SCD may also experience hepatic crises due to red blood cell sickling, leading to hepatomegaly, elevated liver enzyme levels (serum transaminases), or cholestasis.10 Liver issues in these patients can result from various factors, including hepatic sequestration, viral hepatitis from blood transfusions, haemosiderosis (iron accumulation in the liver), gallstones, or unrelated medical conditions.10,11 However, an exceedingly rare association has been observed between sickle cell thalassaemia and autoimmune hepatitis, with only a handful of published cases documented.8,11
In this case report, the authors present a case of the coexistence of SLE and autoimmune hepatitis in a male patient with sickle cell thalassaemia. The occurrence of this uncommon overlapping syndrome highlights the complexities involved in diagnosing and managing these distinct conditions, emphasising the need for careful consideration and evaluation.
CASE PRESENTATION
Patient Information
In this case report, the authors present the admission of a male in his early 20s from the rural interior Sindh region of Pakistan. The patient exhibited symptoms over a 3-day period, including yellowing of the sclera, darkening of urine, pale stools, itching, fever, and joint pain. Notably, there were no known comorbidities, or a family history of similar conditions.
Clinical Findings
During the physical examination, the patient had a normal body temperature of 36.7 °C, blood pressure of 110/70 mmHg, and a heart rate of 88 beats/min. He showed signs of anaemia, moderate jaundice, an elevated jugular venous pressure, a facial rash, a receding hairline, and an enlarged liver located 2 cm below the right costal margin, with sharp margins, firm consistency, and no tenderness. He had pain on pressure in the long bones, and knee arthritis with normal joint movements. This patient previously had a similar episode of eye yellowing, and received red blood cell transfusions a few years ago. In the last year, he experienced a recurrence, which necessitated
four units of packed red blood cell transfusion and a bone marrow biopsy. He did not use any routine medications, such as antimalarial prophylaxis, steroids, or pain relievers.
Diagnostic Assessment
Extensive investigations revealed findings contributing to the patient’s differential diagnosis. The malaria panel revealed positive results for both the malarial parasite test and the malarial parasite immunochromatographic test, confirming the presence of Plasmodium vivax. Blood test results showed normocytic anaemia (Hb: 5.8 g/dL) with a corrected reticulocyte count of 2.53%, hyperleukocytosis (leukocyte count: 37,000 cells/mm³), and a platelet count of 156,000 cells/mm³. The peripheral film showed the malarial vivax trophozoites and gametocytes, along with anisocytosis, poikilocytosis, polychromasia, target cells, fragmented red blood cells, nucleated red blood cells, and sickle cells. Additionally, the sickling test was positive, indicating sickle cell thalassaemia. Hb electrophoresis further confirmed this diagnosis, with Hb S at 95.6% and Hb A2 at 4.40%. The diagnostic evaluation of the patient revealed significant findings indicative of SLE.
Immunological investigations demonstrated a positive antinuclear antibody (ANA) titre of 1/2,560, with a coarse speckled pattern. The anti-double-stranded DNA antibody was elevated at 30.8, indicating the presence of antibodies against double-stranded DNA. Further positive results included SS-A/Ro antibodies at 50.11, and while serum C3 levels were low, C4 and CH50 levels, as well as thyroid and renal functions, were all within acceptable limits. The elevated levels of inflammatory markers, such as C-reactive protein (88.3 mg/dL), erythrocyte sedimentation rate (30 mm/hour), ferritin (20,000 ng/mL), and lactate dehydrogenase (1,168 U/L), further suggested an active inflammatory process, consistent with SLE. The diagnostic workup also revealed evidence supporting a diagnosis of autoimmune hepatitis. The immune laboratory tests showed a positive ANA, with a coarse speckled pattern at a titre of 1/2,560, indicative of autoimmune involvement. Additionally, anti-smooth muscle antibodies tested positive. Serum IgG levels were elevated at 28.74 g/L, surpassing the normal reference range of 6.12–16.16 g/L. Liver function tests displayed total bilirubin elevated at 9.5 mg/
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 79 Article
dL, direct bilirubin at 6.0 mg/dL, and indirect bilirubin at 3.5 mg/dL, suggesting a pattern of hyperbilirubinaemia indicative of hepatic dysfunction. Transaminases were significantly elevated, with aspartate aminotransferase at 244 IU/L, and alanine transaminase at 129 IU/L, surpassing the normal reference ranges. Alkaline phosphatase was elevated at 158 IU/L, and serum γ-glutamyl transferase was elevated at 193 IU/L, indicating cytolysis and cholestasis (Table 1).
Chest radiography and echocardiography results were normal. Abdominal ultrasonography revealed an enlarged liver with a span of 15.7 cm, smooth margins, and altered echotexture. Rheumatoid factor, anti-U1-ribonucleoprotein antibodies, anti-SS-B/La antibodies, anti-Smith antibodies, anti-Scl-70 antibodies, and anticyclic citrullinated peptide antibodies were all negative, as was viral serology. Tests for anti-phospholipid and anti-thyroid peroxidase antibodies were negative. The results of the Coombs test and glucose-6-phosphate dehydrogenase test were negative.
In the bone marrow biopsy conducted 1 year ago, all three primary cell lines were observed. Notably, there was a slight increase in the production of red blood cells, which displayed a typical maturation process. The myelopoiesis, responsible for white blood cell formation, exhibited a balanced ratio of 1:2. The percentage of blast cells (immature blood cells) was less than 4%, while plasma cells constituted 2% of the total cell population. Furthermore, the biopsy identified the presence of megakaryocytes (involved in platelet production), and featured prominent eosinophilic precursors (immature eosinophils, a specific type of white blood cell).
On the second day of hospital admission, the patient complained of relative constipation followed by abdominal distension and discomfort. Upon examination, the abdomen was tense and tender, with fullness around the umbilicus, and decreased gut sounds were noted upon auscultation. In addition, during a digital rectal examination, ballooning of the rectum was observed. Considering the possibility of acute abdominal obstruction, urgent abdominal X-ray and ultrasound were performed. The imaging studies shown in Figure 1A and 1B revealed multiple air-fluid levels and dilated bowel loops on the left side of the abdomen, indicating
the presence of an obstruction. Furthermore, peristaltic movements of the bowel were observed to be sluggish on ultrasound. Due to the severity of the condition, the surgical team was consulted. In addition to the abdominal symptoms, the patient developed a high spiking fever and a continuously rising total leukocyte count. The patient was in a sickle crisis, which explained the presenting symptoms of constipation, abdominal distention, and fever. A CT scan was planned; however, it had to be deferred due to the patient’s declining medical condition at the time. Subsequently, following the receipt of laboratory results, a liver biopsy was proposed as a means to establish a conclusive diagnosis of autoimmune hepatitis. Regrettably, the patient declined to provide consent for the liver biopsy procedure.
During the patient’s follow-up appointment, a 24-hour urinary protein-to-creatinine ratio test was performed, and the results fell within the established normal range, affirming normal renal function without evidence of autoimmune-related complications. Notably, spot urine parameters, including a protein concentration of 46 mg/dL and creatinine level within reference ranges, supported this finding. The spot urine proteinto-creatinine ratio of 0.6 g/gCr, above the threshold of 0.2 g/gCr, further confirmed the absence of significant renal issues. The results provide valuable insights into effective kidney filtration and regulation of protein excretion. It is important to note that an elevated spot urinary protein-to-creatinine ratio, as observed previously, can be influenced by factors such as infection, dehydration, stress, and specific dietary choices. These normal findings contribute to a comprehensive assessment, reassuring the absence of autoimmune-related renal complications. Ongoing monitoring was advised for continued care.
Therapeutic Intervention
The treatment regimen encompassed a multifaceted approach to manage the sickle crisis. O2 therapy was provided to enhance O2 saturation, intravenous fluids were administered to maintain proper fluid balance, and hydroxyurea was initiated at a daily dose of 500 mg for its disease-modifying properties. The patient received periodic packed red blood cell transfusions to address diminishing
80 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Malaria Panel: Both the malarial parasite test and the malarial parasite immunochromatographic test confirmed the presence of Plasmodium vivax.
Complete Blood Picture
Peripheral Blood Film
Malarial vivax trophozoites and gametocytes, anisocytosis, poikilocytosis, polychromasia, target cells, fragmented RBCs, nucleated RBCs, and sickle cells seen. Occasional Howell–Jolly bodies. Sickle Cell Thalassaemia Haemoglobin
Sickling test
SLE Markers Immune laboratory tests
Inflammatory Markers
Laboratory Test Patient Laboratory Values Normal Reference Range
Haemoglobin 5.8 g/dL Male: 12.3–16.6 g/dL Female: 12.1–15.1 g/dL Haematocrit 17.1% Male: 40–54% Female: 36–48% WBC count 37×109/L 4.8–11.3×109/L Platelets 156×109/L 154–433×109/L Corrected reticulocyte count 2.53% 0.50–2.50%
Electrophoresis Haemoglobin A2 4.40% <3% of the total haemoglobin Haemoglobin S 95.6%
Positive
ANA 1/2,560 (pattern: coarse speckled) 1/40–1/60 Anti-dsDNA 30.8 <20 IU/mL=NEGATIVE 20–25 IU/mL=EQUIVOCAL ≥25 IU/mL=POSITIVE Complement C3 0.5 g/L 0.9–1.8 g/L Complement C4 0.25 g/L 0.12–0.36 g/L Urea Creatinine Electrolytes Sodium 142 mEq/L 135–145 mEq/l Calcium 9.4 mg/dL 8.6–10.3 mg/dL Creatinine 1.2 mg/dL Male: 0.7–1.3 mg/dL Female: 0.6–1.1 mg/dL Potassium 4.3 mEq/L 3.5–5.2 mEq/L Urinary Protein-to-Creatinine Spot urine protein 46 mg/dL 0–10 mg/dL Spot urine creatinine 68 mg/dL Male: 20–320 mg/dL Female: 20–275 mg/dL 24hr Urinary Protein-to-Creatinine Ratio Spot urine P/C ratio 0.6 g/gCr <0.2 g/gCr
Immune laboratory tests Reference range
Ferritin 20,000 ng/mL Male: 12–300 ng/mL Female: 12–150 ng/mL
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 81 Article
Table 1: Patient blood panel.
Table 1 continued.
ANA: antinuclear antibody; ALP: alkaline phosphatase; ALT: alanine transaminase; ASMA: anti-smooth muscle antibody; AST: aspartate aminotransferase; CRP: C-reactive protein; C/S: culture and sensitivity; dsDNA: double-stranded DNA; ESR: erythrocyte sedimentation rate; HBsAg: hepatitis B surface antigen; HCV: hepatitis C virus; LDH: lactate dehydrogenase; RBC: red blood cell; serum γ-GT: serum γ-glutamyl transferase; SLE: systemic lupus erythematosus; TSH: thyroid-stimulating hormone;
WBC:
blood cell.
white
CRP 88.3 mg/dL 0.3–1.0 mg/dL ESR 30 mm/hr Male: ≤15 mm/hr Female: ≤20 mm/hr. LDH 1,168 IU/L 140–280 IU/L Serum procalcitonin 3.54 ng/mL <0.1 ng/mL Thyroid Function Test Serum free T4 1.57 ng/dL 0.8–1.6 ng/dL Serum free T3 2.22 pg/mL 2.0–4.4 pg/mL TSH 11.2 IU/mL 0.35–5.5 IU/mL Autoimmune Hepatitis Markers ANA 1/2,560 (pattern: coarse speckled) 1/40–1/60 ASMA POSITIVE Serum IgG levels 28.74 g/L 6.12–16.16 g/L Liver Function Test Total bilirubin 9.5 mg/dL 0.1–1.2 mg/dL Serum direct bilirubin 6.0 mg/dL Less than 0.3 mg/dL Serum indirect bilirubin 3.5 mg/dL 0.1–0.8 mg/dL AST 244 IU/L 8–33 IU/L ALT 129 IU/L 7–55 IU/L ALP 158 IU/L 44–147 IU/L Serum γ-GT 193 IU/L 5–40 IU/L Viral Markers Anti-HCV Non-reactive HBsAg Non-reactive HB core (total) Non-reactive HIV Non-reactive Culture Reports Blood C/S test No growth Urine C/S test No growth 82 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
haemoglobin levels, but no phlebotomy was performed. Furthermore, the patient was prescribed meropenem 1 g intravenously three times daily to address potential infections, and a course of Gen-M (120 mg intravenously) was administered for the treatment of malaria. In light of the presence of other autoimmune diseases, and a decline in complement levels indicative of a disease flare-up, the patient was started on a low-dose steroid regimen, ranging from 10–20 mg per day, followed by a tapering schedule. The decision to incorporate steroids into the treatment plan was carefully considered, taking into account the patient’s intricate medical history. However, in an effort to mitigate potential complications, particularly the risk of vaso-occlusive crises in patients with SCD, a maintenance dose of steroids was chosen over an induction therapy. Importantly, no immunosuppressive agents were introduced during the course of treatment. This careful

choice was made to keep a careful balance in taking care of the different parts of the patient’s health, without adding extra factors that might influence the authors’ understanding of the treatment results.
Follow-up and Outcomes
Following the 4–5-day treatment period, the patient showed substantial improvement in symptoms. Pain became less severe and less frequent, the fever resolved, and relief from constipation and abdominal distention was observed. Upon discharge, the patient’s treatment plan included the continuation of hydroxyurea and folic acid, along with a tapering dosage schedule of steroids. Despite the initial challenges, the patient’s recovery was uneventful, with no observed complications or recurrence of symptoms after treatment.
 These figures present anteroposterior projection abdominal X-ray images taken in the supine position. The images reveal multiple air-fluid levels and dilated bowel loops on the left side of the abdomen, indicating the presence of an obstruction.
These figures present anteroposterior projection abdominal X-ray images taken in the supine position. The images reveal multiple air-fluid levels and dilated bowel loops on the left side of the abdomen, indicating the presence of an obstruction.
B A Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 83 Article
Figure 1: Patient abdominal X-ray.
DISCUSSION
This case report provides a comprehensive analysis of a male patient concurrently diagnosed with sickle cell thalassaemia, SLE, and autoimmune hepatitis. It sheds light on the intricate interplay between these conditions, prompting crucial considerations for further exploration.1,3 When patients with sickle cell thalassaemia exhibit unusual clinical characteristics or multi-organ involvement, clinicians must consider overlapping syndromes.2,9
While the exact mechanisms responsible for these interactions are not fully understood, it is hypothesised that individuals with these interactions may possess an aberrant alternate pathway within their complement system, potentially heightening their vulnerability to autoimmune disease development.4,9 Another hypothesis posits that individuals afflicted with this condition may have an immune system that does not function optimally. This immune dysfunction may be attributed to factors such as diminished spleen function, disruptions within the complement pathway, and compromised processes of opsonisation and phagocytosis, contributing to the pathogenesis. As a consequence, the effective clearance of immune complexes may be compromised. It has been suggested that there is suspicion of SLE in a patient with SCD.12 The clinical suspicion is supported by the finding that patients with SCD tend to have higher ANA titres than the general population.13
In addition, it is hypothesised that SLE is the most commonly reported autoimmune disorder in SCD.3,13,14 The coexistence of SCD and autoimmune hepatitis is also uncommon, with only a few documented cases in the literature. Autopsy studies suggest a prevalence of cirrhosis ranging from 16–29% in patients with sickle cell anaemia. The main contributing factor for liver disease in individuals with SCD is receiving multiple blood transfusions, which is associated with infections such as hepatitis B virus (HBV) and hepatitis C virus, along with the accumulation of excessive iron in the liver.15,16 In an important study, it was observed that children who got the HBV vaccine had a significant drop in HBV infections for 3–5 years after getting vaccinated. This highlights the effectiveness of the vaccination in reducing the incidence of HBV among at-risk groups, emphasising the
positive impact of timely vaccination measures in preventing infections.17 Considering the heightened risk, the patient was also counselled to undergo HBV vaccination during subsequent follow-up appointments. Nevertheless, the presence of ANA positivity at a titre of 1/160 may indicate the potential existence of concurrent autoimmune hepatitis as a plausible explanation for liver damage.16
Managing the presence of both autoimmune diseases and SCD is a challenging task. Decisions regarding overlap syndromes should be carefully made under specialised guidance to optimise outcomes and minimise risks, especially in individuals with SCD.18 Hydroxyurea, a frequently used treatment for SCD, plays a pivotal role in reducing the frequency and severity of complications associated with SCD, including painful events, preservation of splenic function, and attenuation of sickle-related organ damage.19 This drug suppresses the production of autoantibodies, potentially concealing early autoimmune disease.20 As a matter of fact, corticosteroids are an appealing treatment for severe SCD complication, because they are inexpensive, readily available, and exhibit strong anti-inflammatory effects.21
In this particular situation, a decision was made to refrain from using full-dose steroids, despite their known anti-inflammatory properties. This decision was made by evidence suggesting an elevated risk of vaso-occlusive crises and subsequent hospitalisation in patients with SCD who undergo steroid treatment.22 Several studies suggest that treatments, such as those targeting TNF, may offer potential benefits for autoimmune diseases associated with SCD.23 Immunosuppressive and anti-inflammatory medications have the potential to cause kidney and liver damage, which could be exacerbated by complications related to SCD. They also heighten the susceptibility to infections.24 The commencement of such therapies should be a subject of consultation at specialised centres, and calls for vigilant oversight.25 Given the overlapping clinical features and the high prevalence of positive ANA in individuals with SCD, clinicians encounter significant challenges in accurately identifying coexisting autoimmune disorders.4 A delay in diagnosis contributes to elevated morbidity and mortality associated with both autoimmune diseases and SCD.25
84 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
This case report underscores the pressing need for further research to deepen the understanding of the pathophysiology, natural history, and optimal treatment approaches for overlapping syndrome and sickle cell thalassaemia. In addition, the necessity of a multidisciplinary approach, encompassing medical specialists such as haematologists, rheumatologists, and nephrologists, is imperative due to the involvement of multiple organ systems in these coexisting conditions. Effective treatment demands the collective expertise of these specialised medical professionals. Continued investigation is imperative to advance patient care and outcomes in this complex clinical scenario.
CONCLUSION
High Index of Suspicion for Overlapping Syndromes
This report illustrates the unique occurrence of concomitant manifestation of sickle cell thalassaemia with SLE and autoimmune hepatitis, representing a complex and intriguing overlapping syndrome. Clinicians should be alert for signs of competing conditions while treating patients with sickle cell thalassaemia with unusual symptoms, or significant organ dysfunction. The coexistence of these illnesses highlights the importance of investigating any additional problems.
Sickle Cell Disease and Autoimmune Diseases
Patients with SCD are more likely to develop autoimmune disorders. Elevated ANA levels in these patients may raise clinical concerns about conditions such as SLE, prompting more research into the underlying processes and unusual complement pathways.
Hydroxyurea and Autoimmune Disorders
Hydroxyurea, a drug commonly used for the treatment of SCD, suppresses the production of
autoantibodies, and may mask the early signs and symptoms of autoimmune conditions. Healthcare workers should be aware of this effect.
Use of Steroids in Sickle Cell Disease
Due to the increased risk of vaso-occlusive crises and hospital admissions associated with their use, the choice to use steroids in patients with SCD is frequently avoided, even though they possess recognised anti-inflammatory properties.
Challenges in Identifying Coexisting Autoimmune Disorders
The similarity in clinical features and high frequency of patients with SCD who are ANApositive make it difficult for clinicians to diagnose between concurrent autoimmune diseases. The diagnostic journey for this patient involved comprehensive laboratory investigations, serological markers, and imaging studies to confirm the presence of these overlapping disorders. To understand the underlying mechanisms causing the coexistence of these rare illnesses, and to investigate other management strategies, more research is required. Increased awareness and knowledge of such overlapping syndromes will contribute to improved diagnosis, treatment, and overall care for patients facing similar challenges.
Patient Perspective
Living with multiple illnesses can be incredibly challenging. Some days, you experience intense pain and constant fatigue, making it hard to make plans due to the unpredictability of getting sick. Frequent doctor visits become a routine. However, despite the hardships, you grow stronger, and learn to cherish the positive moments in life. It is a journey filled with numerous obstacles, ultimately shaping you into a more resilient individual.
Note: This perspective was originally shared by the patient in another language and has been translated by the doctor for reference.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 85 Article
References
1. Robazzi TC et al. [Coexisting systemic lupus erythematosus and sickle cell disease: case report and literature review]. Rev Bras Reumatol. 2015;55(1):68-74. (In Portuguese).
2. Kaloterakis A et al. Sickle cell/ β0-thalassemia and systemic lupus erythematosus. Lupus. 1999;8(9):778-9.
3. Maamar M et al. Systemic lupus erythematosus associated with sickle-cell disease: a case report and literature review. J Med Case Rep. 2012;6:366.
4. Das DS, Sahoo D. Coevality of systemic lupus erythematosus with sickle cell trait: a not so uncommon entity. Cureus. 2020;12(8):e10119.
5. Rajanna AH et al. A case of male SLE: an unusual presentation. Int J Adv Res. 2023;11(1):1462-5.
6. Sibarani H, Zubir Z. Systemic lupus erythematosus in a male patient. IOP Sci. 2018;125:012158.
7. do Socorro Teixeira Moreira Almeida M et al. Male systemic lupus erythematosus, an overlooked diagnosis. Clin Pract. 2011;1(4):e103.
8. Khartade PB et al. An uncommon presentation of autoimmune hepatitis in a child with thalassemia trait. Cureus. 2023;15(5):e38964.
9. Warrier RP et al. Hemoglobin sickle cell disease and systemic lupus erythematosus. J Natl Med Assoc. 1984;76(10):1030-1.
10. Banerjee S, DeBaun MR. Hepatic
manifestations of sickle cell disease. UptoDate. 2023. Available at: https://medilib.ir/uptodate/ show/3589. Last accessed: 1 January 2024.
11. Lykavieris P et al. Autoimmune liver disease in three children with sickle cell disease. J Pediatr Gastroenterol Nutr. 2006;42(1):104-8.
12. Minocha V, Rana F. Lupus nephritis in a patient with sickle cell disease. Case Rep Hematol. 2013;2013:907950.
13. Toly-Ndour C et al. High titers of autoantibodies in patients with sickle-cell disease. J Rheumatol. 2011;38(2):302-9.
14. Baethge BA et al. Antinuclear antibodies in sickle cell disease. Acta Haematol. 1990;84(4):186-9.
15. Samuel SS, Jain N, Sickle Cell Hepatopathy [Internet] (2022) Treasure Island: StatPearls Publishing. Available at: https:// www.ncbi.nlm.nih.gov/books/ NBK574502/. Last accessed: 1 January 2024.
16. Santi L et al. Liver cirrhosis in a patient with sickle cell trait (Hb Sβ thalassemia) without other known causes of hepatic disease. Case Rep Gastroenterol. 2009;3(3):2759.
17. al-Fawaz I, Ramia S. Decline in hepatitis B infection in sickle cell anaemia and beta thalassaemia major. Arch Dis Child. 1993;69(5):594-6.
18. Couillard S et al. Steroid treatment in children with sickle-cell disease. Haematologica. 2007;92(3):425-6.
19. Agrawal RK et al. Hydroxyurea in sickle cell disease: drug review. Indian J Hematol Blood Transfus. 2014;30(2):91-6.
20. Piccin A et al. Autoimmune disease and sickle cell anaemia: 'Intersecting pathways and differential diagnosis'. Br J Haematol. 2022;197(5):518-28.
21. Lanzkron S, Pecker L. Pain without gain: steroids and sickle crisis. Blood. 2022;139(26):3678-9.
22. Stein BL. Risks of steroid use in patients with sickle cell disease. NEJM J Watch. 2022. Available at: https://www.jwatch.org/ na55121/2022/07/11/risks-steroiduse-patients-with-sickle-celldisease. Last accessed: 1 January 2024.
23. Solovey A et al. Interference with TNFα using long-term etanercept in s+santilles sickle transgenic mice ameliorates abnormal endothelial activation, vasoocclusion, and pulmonary hypertension including its pulmonary arterial wall remodeling. Blood. 2013;122(21):728.
24. Michel M et al. Characteristics and outcome of connective tissue diseases in patients with sickle-cell disease: report of 30 cases. Semin Arthritis Rheum. 2008;38(3):22840.
25. Li-Thiao-Te V et al. Coexistent sickle-cell anemia and autoimmune disease in eight children: pitfalls and challenges. Pediatr Rheumatol Online J. 2018;16(1):5.
86 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Impact of Surgical Treatment on Quality of Life of Patients with Early-Stage Cervical Cancer: A Case Study of Two Referral Hospitals in Kenya
Authors:
*Ghalib Moseti,1 Omenge Orango,1 Benjamin Elly Odongo,1 Peter Itsura,1 Jack Odunga1
1. Moi University School of Medicine, Eldoret, Kenya *Correspondence to gmosetiocharo@gmail.com
Disclosure: The authors have declared no conflicts of interest. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements: Moseti designed, collected data, analysed, and interpreted the data, and wrote the manuscript. Orango and Odongo analysed and interpreted the data. Odunga analysed data and contributed to writing the manuscript. All authors read and approved the final manuscript.
Received: 04.03.22
Accepted: 29.01.24
Keywords: Cervical cancer, Kenyatta National Hospital (KNH), Moi Teaching and Referral Hospital (MTRH), quality of life (QoL), surgery.
Citation: EMJ. 2024;9[1]:87-95. DOI/10.33590/emj/10306929. https://doi.org/10.33590/emj/10306929.
Abstract
Objective: To determine the impact of surgical treatment on quality of life (QoL) of patients with early-stage cervical cancer at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya, and Kenyatta National Hospital (KNH), Nairobi, Kenya.
Methods: A cohort study conducted among 71 patients undergoing surgery for surgically amenable cervical cancer stage. Consecutive sampling of females was used to recruit participants. Participants were followed up for 3 months post-operatively. Descriptive statistics was used to describe the study participants. Bivariate analysis was used to assess the relationship between dependent and independent variables, and p value ≤0.05 was considered to be statistically significant.
Results: Nearly two-thirds (63.5%) of the females had a parity of four or more, 69 (97.2%) did not have a family history of cervical cancer, and 57 (80.3%) were negative on HIV test. Most females (47.9%) had Stage IB2 cervical cancer, followed by those with Stage IB1, seen in 28 (39.4%) of the females enrolled. There were statistically significant differences in pain/discomfort (p=0.028) and anxiety/ depression (p=0.028). Patients aged 20–35 years had a two-fold increased likelihood (adjusted odds ratio: 2.44; 95% confidence interval: 1.30–3.10; p=0.011) of reporting better QoL scores compared to older females. The lower the cervical cancer stage (Stage IA2), the higher the likelihood for improved QoL following surgical management of cervical cancer (adjusted odds ratio: 5.69; 95% confidence interval: 3.55–6.89; p=0.001).
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 87 Article
Conclusion: This study reports that being aged 20–35 years old and having a lower stage cervical cancer increased the likelihood of a good QoL outcome following surgical management of cervical cancer.
Key Points
1. Because of the high disease burden associated with cervical cancer, there is a need to determine whether the current early intervention of radical hysterectomy improves the patient's quality of life (QoL).
2. The QoL among patients with early-stage cervical cancer after surgery was generally good, indicating an overall improvement of QoL, especially with regard to pain/discomfort and anxiety/depression.
3. There should be more attention and clinical focus in the tertiary facilities of low and middle income countries, offered to patients with cervical cancer who are >35 years, and with Stage IB and above, to improve their QoL by focusing more on addressing their pain/discomfort and anxiety/depression, through a multidisciplinary approach in these patients’ care.
BACKGROUND
Cervical cancer is established as a major cause of morbidity and mortality among females globally.1 In Kenya, and other countries with developing economies within sub-Saharan Africa, it is the second most prevalent cancer after breast cancer among females.2 Because of this huge disease burden, the majority of the females affected are still in their reproductive age, and this raises concerns about their resultant quality of life (QoL). The great disease burden is further compounded by the high prevalence of HIV infections in these countries. Because of the many early detection programmes, such as the see and treat strategy introduced in Kenya and other sub-Saharan African countries, females with cervical cancer are now identified early, and prescribed radical hysterectomy for their surgically amenable cervical cancer.2 However, this procedure is associated with the complete resection of the uterus, parametrium (round, broad, cardinal, and uterosacral ligaments), cervix, upper one-third to one-half of the vagina, and bilateral pelvic lymph nodes.3 The removal of the ovaries and fallopian tube is an integral part of the radical hysterectomy. The ovaries will be removed in post-menopausal females and transpositioned in pre-menopausal females who may require radiotherapy later on. This may interfere with their perception of wellbeing, especially in the aspect of fertility and childbearing ability, and psychosexual health and wellbeing.4
Complications, such as longer operation time, pain, and side effects of lymph node dissection, like lymphoedema, which reduces the QOL of females who have undergone radical hysterectomy, could influence both the physical (pain, discomfort, low energy and fatigue, sleep disturbance, and medication dependency) and psychological (anxiety and depression) domains.5 Most of the studies conducted in many developing countries have focused on the prevalence and disease burden of cervical cancer, with a few focusing on early screening and interventions for the disease. However, very few published studies have focused on the resultant QoL among females who undergo radical hysterectomy as an intervention for surgically amenable early-stage cervical cancer. This study therefore aims to determine the QoL of these females by assessing both the physical and psychological domains at two national referral and teaching hospitals in Kenya. Because of this huge disease burden, major concerns on the QoL, resulting from both the disease itself and treatment modalities, have been raised.
Most studies done in other populations on the impact of treatment for cancer of the cervix on QoL, evaluated females in all stages of the disease, and included all treatment modalities. This study, therefore, set out to determine the major indicators of QoL among patients with surgically amenable cervical cancer, who had undergone radical hysterectomy at two major national hospitals in Kenya.
88 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
The objective of this study was to determine the impact of surgical treatment on QoL of patients with early-stage cervical cancer at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya, and Kenyatta National Hospital (KNH), Nairobi, Kenya.
METHODS
Study Design
This was a prospective cohort study conducted among females with a surgically amenable stage of cervical cancer, and scheduled for radical hysterectomy.
Study Area
The study was carried out at two national hospitals in Kenya, MTRH in Eldoret and KNH in Nairobi. This study was carried out for a period of 17 months from October 2019–February 2021, with each participant followed for 12 weeks after radical hysterectomy to assess the person’s perception of their QoL.
Study Procedure
Females who presented with a histologically confirmed diagnosis of cervical cancer at the gynae-oncology units of both KNH and MTRH were recruited into the study. Appropriate laboratory and radiological investigations, such as a complete blood count, abdominopelvic CT scan, chest X-ray, and renal function test, were done.
Based on their medical history and clinical signs, the International Federation of Gynecology and Obstetrics (FIGO) criteria were used to stage the patients with newly diagnosed cervical cancer. Those who met the criteria of Stage IB2 and below were recruited into the study. After consenting, an interviewer administered a questionnaire that included the EQ-5D-5L to collect participants’ clinical and reproductive characteristics, as well as assessing their QoL prior to surgery. After radical hysterectomy, the participants were followed up after 3 months to determine their post-surgical QoL.
Data Management and Analysis
Data were collected using a structured questionnaire where both participants’
information and QoL score (pre- and posthysterectomy) were documented. The questionnaire was administered by medically trained research assistants to single out patients before and after surgery.
Descriptive results were computed, and presented in the form of tables for the participants’ sociodemographic characteristics, cervical cancer stage, treatment factors (surgery), and impact of treatment on QoL.
Inferential statistical analysis using bivariate analysis with the Pearson's χ2 test was adopted to compare the difference in participants’ sociodemographic characteristics and QoL indicators, where a p value of ≤0.05 was considered to be statistically significant.
Ethical Considerations
The MTRH Institutional Research and Ethics Committee and KNH Institutional Research Board reviewed and approved the conduct of this study, and no data collection took place prior to approval.
RESULTS
Sociodemographic Characteristics of Study Participants
A total of 71 participants were recruited into the study. The mean age of the participants was 47.94 years, and most of the participants were aged between 40–50 years old. The youngest was 26 years old, and the eldest 68 years old.
The majority of the participants were married (87.3%), while 7.0% were either single or divorced. A total of 39 (54.9%) had no education or primary education, with 22.5% having secondary education, and the same percentage (22.5%) having tertiary education. Most of the interviewed participants (52.1%) were unemployed, 16.9% were in formal employment, and the remaining 31.0% were running their own businesses or participating in other economic activities, such as farming. Thirty-nine (54.9%) had health insurance. Most of the patients (56.4%) were from the KNH study site. There were no patients lost to follow-up or death during the 12-month study period.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 89 Article
The sociodemographic characteristics are presented in Table 1.
The study conducted a bivariate comparison between participants’ sociodemographic characteristics and QoL improvement. Females aged 21–35 years were significantly (p=0.011) more likely to improve, compared to the older counterparts aged 35 years or higher. Females with a tertiary level of education significantly (p=0.004) reported an improvement in their QoL, compared to those with a secondary and primary level of education. Similarly, formally employed females were significantly (p=0.012) more likely to report an improvement in their QoL, compared to those who were either unemployed or in self-employment.
Clinical Characteristics of the Study Participants
The clinical characteristics of the study participants are shown in Table 2
The study further compared whether there was any statistically significant association between the participants’ clinical characteristics and QoL improvement. Females with Stage IA2 were more likely to report a significant (p=0.001) improvement in their QoL, compared to those presenting with all the other early clinical stages of cervical cancer.
Quality of Life of Patients Diagnosed with Cancer of Cervix Pre- and Post-surgical Treatment
A descriptive analysis using the EQ-5D-5L dimensions showed a positive improvement in the QoL score before and after radical hysterectomy on all five dimensions. This was further stratified into five levels: Level 1 (no problems), Level 2 (slight problems), Level 3 (moderate problems), Level 4 (severe problems), and Level 5 (unable to do anything).
The mobility level of patients significantly improved after surgery, as depicted in Table 3
A total of 65 out of 71 of the patients were at Level 1 (91.5%) after surgery, which was a good indicator, as opposed to only 45.1% before, meaning more than half of the participants at a percentage of 54.9% had a poor score (Levels 2–5) prior to surgery.
Descriptive
Comparison of
Number
of
Patients in EQ-5D-5L Before and After Surgery in Aspect of Self-Care
In the aspect of self-care, a total of 70 (98.6%) participants were able to take care of themselves without any assistance, as opposed to only 38 participants prior to surgery (53.5%). Therefore, 46.5% of participants had problems with taking care of themselves; however, this percentage comes down to only 1.4% post-operatively, representing improvement.
Descriptive Comparison of Number of Patients in EQ-5D-5L Before and After Surgery in Aspect of Usual Activities
In total, 84.0% of participants had no problems conducting their usual activities after surgery; however, only 22.5% of participants were at the same level pre-operatively. This indicates that 81.5% of participants had problems conducting their usual activities prior to surgery, while that percentage significantly reduced to 15.5% post-operatively.
Descriptive Comparison of Number of Patients in EQ-5D-5L Before and After Surgery in Aspect of Pain/Discomfort
In the domain of pain/discomfort, only 4.2% of participants had no problems with pain or discomfort, meaning that 95.8% of participants had problems, or complained of pain or discomfort, prior to operation. However, postoperatively, 47.9% of participants had no problems with pain or discomfort, while 52.1% still reported or complained of pain or discomfort 12 weeks post-operatively.
Descriptive Comparison of Number of Patients in EQ-5D-5L Before and After Surgery in Aspect of Anxiety/Depression
In the domain of anxiety or depression prior to surgery, 15.5% of participants did not report pain or anxiety, while 84.5% of the participants had problems, or complained of anxiety or depression. Post-operatively, only 60.6% had no problems, or reported no anxiety or depression, meaning that 39.4% of participants still had problems with anxiety and depression.
90 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
N/A: not applicable.
Therefore, a descriptive analysis of the authors’ results using the EQ-5D-5L dimensions showed a positive improvement between the two time periods. The health state and QoL of the
interviewed patients was better after surgery with regard to mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
Variable N Frequency (n) Percent (%) P value Age <20 0 0.0 N/A 21–35 71 9 12.7 0.011 >35 62 87.3 Reference Marital Status Single 5 7.0 0.702 Married 71 66 93.0 0.062 Education None/Primary 71 39 54.9 0.245 Secondary 16 22.5 Reference Tertiary 16 22.5 0.004 Occupation 71 Unemployed 37 52.1 Reference Formal employment 12 16.9 0.012 Business 22 31.0 0.103 Health Insurance 71 No 32 45.1 Reference Yes 39 54.9 0.460 Residence Uasin Gishu 7 9.9 0.101 Outside Uasin Gishu 24 33.8 Reference Nairobi 21 29.6 0.312 Outside Nairobi 19 26.8 0.112
Table 1: Participants’ sociodemographic characteristics (N=71).
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 91 Article
N/A: not applicable.
The statistically significant sociodemographic and clinical characteristics of the study participants were then fitted into a logistic regression model, where females aged 21–35 years had a two-fold (adjusted odds ratio [AOR]: 2.44; 95% confidence interval [CI]: 1.30–3.10) increased likelihood of reporting an improvement in their QoL compared to their compatriots older than 35 years. Similarly, females with Stage IA2
reported a nearly six-fold (AOR: 5.69; 95% CI: 3.55–6.89) improvement in their QoL outcomes across all five domains assessed, compared to their colleagues with other early stages of cervical cancer. However, after adjusting for the confounders, level of education and being formally employed did not significantly increase the likelihood of better QoL scores (Table 3).
Variable N Frequency (n) Percent (%) P value Parity 1 4 5.6 0.303 2–3 71 22 30.9 Reference ≥4 45 63.5 0.782 Family history of cervical cancer No 69 97.2 0.478 Yes 71 2 2.8 Reference History of smoking No 71 71 100 N/A Yes 0 0 HIV Status 71 Negative 57 80.3 Reference Positive 14 19.7 0.521 Cervical cancer stage 71 Stage IA1 2 2.8 0.845 Stage IA2 7 9.9 0.001 Stage IB1 28 39.4 Reference Stage IB2 34 47.9 0.058
Table 2: Clinical characteristics of patients with early-stage cervical cancer.
92 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
DISCUSSION
Sociodemographic and Clinical Characteristics of Patients Who Underwent Surgery for Early-Stage Cervical Cancer
This study evaluated the QoL among patients with cervical cancer, and its relationship to sociodemographic and clinical variables. Findings from the study established that age, level of education, and occupation influenced the QoL of patients with cervical cancer in the studied settings. The study also established a significant association between the stages of cervical cancer and QoL scores.
Having completed secondary education or higher positively influenced QoL of the patients. Therefore, patients who had primary or no education were the more likely to have a low QoL score, and thus seemed to require more attention and focus from caregivers.
This was consistent with findings of Twahir et al.,2 which reported that patients with higher levels of education were more likely to achieve a better QoL than their counterparts with a lower level of education. The authors’ findings were also supported in a study done in Ethiopia on the QoL in patients with gynaecological cancer who had undergone surgery, which also found
an AOR of 4.33 of better QoL in patients with post-secondary education; patients with postsecondary education had a four times better chance of having a good QoL score than their counterparts with primary or no education.
However, these results contrasted with findings from a study that reported higher physical and overall QoL scores among patients with lower levels of education.6,7 This difference could be due to the different coping methods and social support they obtained from family and friends.
Patients who had completed secondary and tertiary levels of education had higher total QoL scores compared to those with lower levels of education. Low levels of education have been associated with decreased awareness of the disease. This often contributes to a large number of females being less likely to be screened early for their cancers, which makes them increasingly present to health facilities in the late stages of their cancers, leading to poor prognosis, hence low QoL scores. These findings are consistent with those by Araya et al.8 reporting higher QoL scores with higher levels of education, while lower levels of education were associated with lower QoL scores in two other studies.
The patients’ occupation was significantly associated with QoL. The formally employed had higher QoL scores compared to their unemployed
Variable (N=71) Pre-operation Post-operation P value Mean (SD) Mean (SD) Mobility 14.2 (12.7) 35.5 (41.7) 0.068 Self-care 17.7 (14.7) 35.5(48.8) 0.095 Usual activities 13.0 (12.9) 35.5 (34.6) 0.088 Pain/discomfort 14.2 (16.5) 23.6 (12.3) 0.028 Anxiety/depression 14.2 (9.44) 23.6 (16.7) 0.028 Your health today 47.32 (8.9) 80.85 (10.0) <0.001 SD: standard deviation.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 93 Article
Table 3: Bivariate association of EQ-5D-5L scores pre- and post-radical hysterectomy.
counterparts. Formal employment is associated with adequate social support based on high income earnings. This finding was consistent with that of Araya et al.8 among patients with cancer, where those with higher levels of employment had higher QoL.
The patients who were formally or self-employed had higher QoL scores compared to those who had no source of income. This finding was consistent with other studies that have reported a significant association between income and overall QoL.
Patients aged 21–35 years had higher QoL scores compared to the older patients. This was consistent with the findings of Chan et al.,9 but contrasted findings from a study by Goker et al.,7 who reported higher physical and overall QoL scores among older Turkish patients with gynaecological cancer.
Patients with Stage IA2 had better QoL scores than those with Stage IB1 and above. This finding was consistent with that of another study,7 where patients who had early-stage cancer had better health status, role function, and social wellbeing than those with advanced cancers. The observed difference could be attributed to good prognosis following early diagnosis and pathogenesis. Normally, females with early-stage ovarian cancer tended to have good prognosis following surgical treatment.
From the regression analysis, age and cervical cancer stage were found to be independent predictors of QoL among patients with cervical cancer in this study. This finding was consistent with those of other studies,7 which identified age, cancer stage, and level of education as predictors of QoL among patients with cancer.
Quality of Life of Patients Diagnosed with Cervical Cancer Pre- and Postsurgical Treatment of Surgically Amenable Stage
This study determined that the majority of the study participants improved in all the five indicators on their QoL. Specifically, nearly all participants were able to move (91.5%), take care of themselves (98.6%), and perform usual activities (84.5%) without any difficulty. However, less than half (47.9%) of the females enrolled did not experience any pain or
discomfort, and 60.6% did not report anxiety or depression symptoms.
Previous studies have indicated variability in the participants’ perception to mobility, self-care, and ability to perform usual activities, and this is often affected by the place a participant resides, their occupation, and number of individuals living in their household.10 For instance, participants living in a bungalow or groundfloor of a multistorey building will report less mobility challenges, compared to those living in mansions or higher floors within a multistorey building. The findings of this study match those reported in Indonesia,11 where 77.0% of females enrolled did not experience any difficulties with mobility, 83.9% were able to perform self-care activities without any problem, and two-thirds (66.7%) performed their usual activities with ease. More than half of the participants enrolled in the Indonesian study11 experienced moderateto-severe problems in their assessment of pain or discomfort, as well as anxiety or depression. It is easier for participants to express pain or discomfort, as well as anxiety, compared to other QoL indicators, such as self-care and usual activities; these are easily confounded by the nature of self-care and usual activity a participant is involved in. Furthermore, the assessment of the first three QoL indicators (mobility, self-care, and usual activities) is not significantly affected by the assessment tool (whether it is EQ-5D-3L or EQ-5D-5L), as was demonstrated in a Polish general population, and a sample of patients with cancer in Korea.12
The mean values for pre- and post-radical hysterectomy QoL indicators have also been demonstrated to differ based on the assessment tools. In a Dutch retrospective study,13 the mean total EQ-5D utility post-radical hysterectomy score of 81.4 (±24.4) was nearly half that reported in the current study. This could be attributed to the differences in the study designs adopted by these two studies, one being retrospective and the other prospective; differences in the study duration; and QoL assessment questionnaire. It may also be due to sociocultural differences, as this has previously been shown to affect the efficacy of questionnaires. This creates the need for the massive adoption of a universal QoL assessment tool for patients with cervical cancer undergoing radical hysterectomy.
94 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
CONCLUSION
The QoL among patients with early-stage cervical cancer after surgery was generally good, indicative of overall improvement of QoL.
References
1. Cecilia NC et al. Global burden of cervical cancer: a literature review. Int J Public Health. 2017;4(2):10-8.
2. Twahir M et al. Real-world challenges for patients with breast cancer in sub-Saharan Africa: a retrospective observational study of access to care in Ghana, Kenya and Nigeria. BMJ Open. 2021;11(3):e041900.
3. Mann Jr WJ. Radical hysterectomy. 2023. Available at: https://www. uptodate.com/contents/radicalhysterectomy. Last accessed: 1 January 2024.
4. Jalal K et al. Changes in ovarian volume, function and vascularity following hysterectomy. Popul Sci. 2010;2010(35):1-18.
5. Jaszkul KM et al. Global impact of lymphedema on quality of life and society. Eur J Plast Surg. 2023;46(6):1-13.
Specifically, with regard to pain/discomfort and anxiety/depression, there appears to be an improvement in QOL scores post-surgery for early cancer.
6. Chen H et al. A 5-gene DNA methylation signature is a promising prognostic biomarker for early-stage cervical cancer. J Obstetr Gynaecol. 2021;42(2):32732.
7. Goker A et al. Quality of life in women with gynecologic cancer in Turkey. Asian Pac J Cancer Prev. 2011;12(11):3121-8.
8. Araya LT et al. Health-related quality of life and associated factors among cervical cancer patients at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia. Health Qual Life Outcomes. 2020;18(1):72.
9. Chan KY et al. Quality of life for Hong Kong Chinese patients with advanced gynecological cancers in the palliative phase of care: a cross-sectional study. J Palliat Care. 2012;28(4):259-66.
10. Mahendra INB. The characteristic of cervical cancer patients who
underwent a radical hysterectomy at Sanglah Hospital Denpasar in 2015. Bali Med J. 2016;5(1):237-9.
11. Adama O et al. Indications and prognosis of the hysterectomy operation in the obstetrics and gynecology department at the University Teaching Hospital of Ouagadougou (UTH-YO), Burkina Faso. Open J Obstet Gynecol. 2017;7(13):1239-46.
12. Kim SI et al. Impact of laparoscopic radical hysterectomy on survival outcome in patients with FIGO stage IB cervical cancer: a matching study of two institutional hospitals in Korea. Gynecol Oncol. 2019;155(1):75-82.
13. Herdman M et al. Development and preliminary testing of the new fivelevel version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-36.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 95 Article FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Immunoglobin D Multiple Myeloma: A Single Centre Experience
Authors:
Disclosure:
*Geetha Narayanan,1 Abhilash Menon,1 Sugeeth M.T.,1 Sherry Abraham,1 Krishnan Unni,1 Sreejith G. Nair1
1. Department of Medical Oncology, Regional Cancer Centre, Thiruvananthapuram, India
*Correspondence to geenarayanan@yahoo.com
The authors have declared no conflicts of interest. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.
Received: 09.07.23
Accepted: 04.01.24
Keywords: IgD, immunoglobulin, multiple myeloma (MM).
Citation: EMJ. 2024;9[1]:96-105. DOI/10.33590/emj/11000013. https://doi.org/10.33590/emj/11000013.
Abstract
Background: Immunoglobulin D (IgD) myeloma is an uncommon subtype of multiple myeloma that accounts for 1–2% of all myeloma cases. IgD myeloma is often associated with a high incidence of renal insufficiency, hypercalcaemia, extraosseous disease, amyloidosis, and Bence–Jones proteinuria.
Materials and Methods: The authors discuss the clinical presentation and treatment results of 12 cases of IgD myeloma, treated at a single centre.
Results: The study included nine males and three females, with a median age of 48.5 years. All had lytic bone lesions, eight had anaemia, five had renal impairment, three had hypercalcaemia, three had features of amyloidosis, and one had polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes syndrome. On immunofixation electrophoresis, 10 patients had IgD λ subtype, and two had IgD κ. Urine Bence–Jones protein was positive for five patients. Eleven patients received bortezomib-based chemotherapy. Three patients achieved complete response, two had a very good partial response, two achieved partial response,three progressed, and one discontinued treatment. At 2 years, six patients were alive (50%). Median overall survival of the series was 21 months (range: 1–80 months).
Conclusion: IgD myeloma is an uncommon subtype of myeloma associated with a high incidence of hypercalcaemia, renal insufficiency, extraosseous lesions, amyloidosis, and Bence–Jones proteinuria. IgD λ disease is more frequent, unlike other subtypes of IgD myeloma. Management is similar to other myeloma types, but with poorer outcomes.
96 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Key Points
1. Immunoglobulin D (IgD) myeloma is a rare subtype of multiple myeloma, which accounts for less than 2% of all myelomas. It is often associated with a high incidence of renal failure, hypercalcaemia, extraosseous disease, amyloidosis, Bence–Jones proteinuria, and a small or absent M spike. Patients with IgD myeloma have a poor outcome compared to other subtypes.
2. This study describes the clinical presentations, laboratory findings, treatment received, and outcome of 12 patients with IgD multiple myeloma, treated in a tertiary cancer centre. A literature review of clinical characteristics, and treatment outcome of studies in IgD myeloma published in literature, is also included.
3. IgD myeloma affects relatively younger males, and presents in advanced International Staging System (ISS) stage. IgD λ disease is more frequent, unlike other subtypes of myeloma. Since IgD levels are generally very low in the serum, it may escape detection. Treatment of IgD myeloma is similar to other subtypes of myeloma. Bortezomib-based chemotherapy is an effective regimen.
INTRODUCTION
Multiple myeloma (MM) is a disease characterised by the clonal expansion of malignant plasma cells in the marrow, leading to anaemia, hypercalcaemia, bone lesions, and renal dysfunction. MM accounts for approximately 10% of haematologic malignancies, and 1% of all cancers.1 MM can be of various types, involving different isotypes of immunoglobin (Ig) heavy chains and light chains. IgG, IgA, and light chain myelomas are the most prevalent, comprising 52%, 21%, and 16% of MM cases, respectively. Together, they constitute 90% of all MM cases. Other MM types are IgD, IgE, IgM, and non-secretory types.2,3
IgD myeloma is a rare subtype of MM, accounting for <2% of all myelomas.4-6 It is often associated with a high incidence of renal failure, hypercalcaemia, extraosseous disease, amyloidosis, and Bence–Jones proteinuria.7-9
As the secretion of IgD is low in the serum, it is difficult to confirm the presence of monoclonal protein IgD by serum protein electrophoresis or immunofixation electrophoresis.10 Patients with IgD myeloma have a poor outcome compared to other subtypes, with a median survival of 13–21 months.11,12 Despite its aggressive course, recent advances in the treatment of MM have improved patient outcomes in IgD myeloma.
In this report, the authors present the results of a retrospective analysis of 12 cases of IgD myeloma, treated at a tertiary cancer centre.
OBJECTIVES
The objective was to study the clinical presentations, treatment, and survival of patients with IgD myeloma treated in a single centre.
MATERIALS AND METHODS
This is a retrospective study conducted at a tertiary cancer centre, in the Department of Medical Oncology, Regional Cancer Centre, Thiruvananthapuram, India, on 12 patients diagnosed with IgD myeloma during a 5-year period, from January 2015–December 2019. The details of clinical presentation, diagnosis, treatment, and survival were noted from medical records. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.
TREATMENT PROTOCOL
The standard treatment for MM included systemic chemotherapy with the proteasome inhibitor bortezomib, along with other
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 97 Article
drugs, or a combination of lenalidomide and dexamethasone, as induction. This was followed by bortezomib or lenalidomide maintenance chemotherapy. The patient response was assessed at regular intervals during induction and maintenance therapy. Radiotherapy was considered for patients with spinal cord compression, and for pain relief.
STATISTICAL METHODS
The baseline patient characteristics, diagnosis, treatment details, and response assessment were analysed using descriptive statistics, including frequency, percentage, median, range, and mean. Overall survival (OS) was calculated from the date of initial diagnosis to the date of death from any cause, or last follow-up visit. Progression-free survival (PFS) was calculated from the initiation of chemotherapy until disease progression.
RESULTS
Among 1,240 patients with MM seen between 2015–2019 at the authors’ centre, 12 patients were diagnosed with IgD myeloma, with an incidence of 0.96%. The median age was 48.5 years (range: 34.0–67.0 years). There were nine males and three females. Eight patients presented with bone pain, and three patients presented with features of amyloid deposits. One patient had features of polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes (POEMS) syndrome. Among the 12 cases, all had lytic bone lesions, eight had anaemia (haemoglobin <10 g/dL), five had renal impairment (serum creatinine >2 mg/ dL), and three had hypercalcaemia (>11.5 mg/ dL). The median duration of symptoms was 8 weeks (range: 4–24 weeks). The baseline characteristics of all patients are summarised in Table 1.
Mean haemoglobin was 10.13 g/dL (standard deviation [SD]: 2.12 g/dL). Two patients had thrombocytopenia. Mean albumin was 4.05 g/ dL (SD: 0.47 g/dL), and β2 microglobulin was 8.40 mcg/mL (SD: 4.72 mcg/mL). The albumin/ globulin ratio was reversed in four patients.
According to the International Staging System (ISS), three patients had Stage I MM, one patient
had Stage II, and eight patients had Stage III. Median serum lactate dehydrogenase was 223 IU/L (range: 142–710 IU/L [normal range: 120–246 IU/L]). Six patients had a prominent M-band of >1 g/dL, with a median M-spike of 1 g/dL (range: 0.34–3.6 g/dL). On immunofixation electrophoresis, 10 patients had IgD λ subtype, and two had IgD κ. On free light chain assay, the median serum κ was 23.5 mg/L (range: 8.8–5,395.0 mg/L) and serum λ was 1,765.1 mg/L (range: 11.8–6,935.0 mg/L). The ratio of involved to uninvolved free light chain was >100 in seven patients. The median 24-hour urine protein was 2,000 mg (range 147–4,095 mg). Urine Bence–Jones protein was positive in five patients. Urine electrophoresis was available in 10 patients, of whom eight showed a band in the γ-globulin region. Cytogenetics risk stratification was not done, since the facility was not available in the authors’ centre.
Six patients received induction with bortezomib, lenalidomide, and dexamethasone; two patients with bortezomib, cyclophosphamide, and dexamethasone; and three with bortezomib and dexamethasone. One patient died before treatment initiation. Two patients received radiation at a dose of 20 Gy/5# for spinal cord compression, and four patients received palliative radiation at a dose of 8 Gy/1# to symptomatic bone lesions. Response assessment was done according to the International Myeloma Working Group (IMWG) response assessment criteria. Complete response was achieved in three patients, two patients had very good partial response (VgPR), two achieved partial response, and three progressed. In one case, response could not be assessed, since the patient defaulted after the first cycle. Patients who achieved at least VgPR received maintenance with bortezomib (n=4) and lenalidomide (n=1). Three patients relapsed during maintenance. All patients who relapsed or progressed received salvage chemotherapy with carfilzomib, pomalidomide, lenalidomide, or thalidomide-based regimens. Following salvage chemotherapy, one patient achieved complete response, one achieved VgPR, and all others had persistent disease. At 2 years, six patients were alive (50%). Median OS of the series was 21 months (range: 1–80 months; Table 2).
Article 98 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
ISS: international staging system; LDH: lactate dehydrogenase; N/A: not applicable; POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy and skin changes.
DISCUSSION
IgD myeloma was first described by Rowe and Fahey in 1965.13 Since then, studies have reported a prevalence of IgD myeloma of 1–2% among all myeloma cases.2,7,14,15 In patients <40 years, the incidence of IgD myeloma is 6%.16 The incidence in the present study was 0.96%. IgD myeloma affects relatively younger males, with an average age of 59 years (54–65 years).3,11,17 The median age in the present study was 48.5
years, which is younger than previously reported. In a recent study, IgD myeloma accounted for 4.3% of all myeloma cases, with a median age of 57.5%.18 Given the rarity of the disease, large studies on IgD myeloma are limited. Selene et al.19 conducted a systematic review of the clinical presentation, management, and prognostic factors of 166 patients with IgD MM.
The clinical features of IgD myeloma are similar to other types of myelomas. However, IgD MM
Patient Number Age in Years/Sex Presenting Symptom Hypercalcaemia Renal impairment Anaemia Lytic bone lesions (CRAB) Extramedullary Involvement LDH (IU/L) β2 Microglobulin (mcg/mL) M-protein (g/dL) IgD Subtype ISS Stage 1 48/M Left hip pain C- R+ A+ B+ N/A 710 11.40 N/A IgD λ III 2 48/M Back pain C- R- A- B+ N/A 188 2.70 2.23 IgD κ I 3 61/M Back pain C- R- A+ B+ N/A 223 11.20 3.60 IgD λ III 4 47/M Body pain; fatigue C- R+ A+ B+ N/A 248 11.60 1.46 IgD λ III 5 38/F Submandibular swelling C- R- A- B+ Amyloid deposit in neck 180 4.60 0.34 IgD κ II 6 67/M Fatigue; loss of weight C- R- A+ B+ Splenomegaly; generalised lymphadenopathy; POEMS 577 10.70 0.61 IgD λ III 7 47/M Dyspnoea; abdominal distension C- R- A+ B+ Cardiac amyloidosis 326 5.60 1.79 IgD λ III 8 49/M Back pain C+ R+ A+ B+ N/A 615 18.00 1.25 IgD λ III 9 51/M Back pain C+ R+ A- B+ Lymphadenopathy 200 11.10 0.81 IgD λ III 10 34/F Swelling forehead C- R- A+ B+ N/A 142 8.10 0.50 IgD λ III 11 62/M Back pain C+ R+ A- B+ N/A N/A 3.00 1.00 IgD λ I
58/F Swelling
C- R- A+ B+ Amyloid deposits in the tongue and heart 180 2.90 0.40 IgD λ I
12
tongue; palpitations
Article
Table 1: Summary of clinical presentation and diagnosis of 12 patients with immunoglobin D myeloma.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 99
CR: complete response; KCd: carfilzomib+cyclophosphamide+dexamethasone; Kd: carfilzomib+dexamethasone; KRd: carfilzomib+lenalidomide+dexamethasone; Mp: melphalan+prednisolone; N/A: not applicable; PCd: pomalidomide+cyclophosphamide+dexamethasone; Pd: pomalidomide+dexamethasone; PFS: progression-free survival; PR: partial response; Rd: lenalidomide+dexamethasone; RVd: nortezomib+lenalidomide+dexamethasone; Td: thalidomide+dexamethasone; VAd: vincristine+adriamycin+dexamethasone; VCd: bortezomib+cyclophosphamide+dexamethasone; Vd: bortezomib+dexamethasone; VgPR: very good partial response.
has been found to involve relatively younger patients, and is characterised by extramedullary disease, osteolytic bone lesions, amyloidosis, hypercalcaemia, renal failure, Bence–Jones proteinuria, and a small or absent M-spike.3,7,14,15,20 These patients usually present in the advanced ISS stage as well.
Renal failure and Bence–Jones proteinuria are significantly higher with IgD myeloma compared to other subtypes, with renal failure present in 20–40% of patients at the time of diagnosis.11,21 Renal injury may be caused by light chain cast nephropathy, or due to direct toxicity by intracellular crystals.22,23 A recent study on risk factors of renal damage and prognosis in IgD
Patient Number Induction Regimen Response MaintMaintenance PFS (months) Salvage Current Status Overall survival (months) 1 RVd CR Lenalidomide 11 Td Alive and no evidence of disease 80 2 RVd CR Bortezomib 31 N/A Alive and on bortezomib maintemaintenance 31 3 RVd VgPR Bortezomib 24 N/A Alive and on bortezomib maintenance 24 4 Vd PR N/A 5 N/A Defaulted after 6th cycle 5 5 RVd N/A N/A 2 N/A Defaulted after 1st cycle 2 6 Vd Progression N/A 10 KCd Progressed and died 14 7 VCd PR N/A 11 N/A Progressed and died 11 8 VCd VgPR Bortezomib 14 Rd Progressed and died 36 9 RVd Progression N/A 8 PCd Progressed and died 18 10 RVd CR Bortezomib 16 KRd Progressed and died 25 11 Vd Progression N/A 4 Rd, VAd, Pd, Kd, Mp Progressed and died 29 12 N/A N/A N/A N/A N/A Died before the start of treatment 1
Article 100 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Table 2: Summary of treatment details of 12 patients with immunoglobin D myeloma.
myeloma reported that 55.3% of patients with IgD myeloma had renal damage as a complication, and that β2 microglobulin was an independent risk factor for renal damage. The median OS of the renal impairment group was significantly shorter than the non-renal impairment group.24 Bence–Jones proteinuria was reported in about 71% of IgD myeloma cases, in contrast to 35% of IgG, and 20% of IgA myeloma.3
Extramedullary disease is seen in 19–63% of patients with MM, the commonly involved sites being the chest wall, respiratory tract, gastrointestinal tract, skin, lymph nodes, and, rarely, testes.19,25 Amyloid light chain amyloidosis mostly affecting the heart is a common complication of IgD myeloma, seen in 19% of cases.3 In the present study, among 12 patients, three had amyloidosis, three had hypercalcaemia, and five had renal impairment.
In a recent study on the clinical features and prognosis of IgD myeloma, the first clinical manifestations were fatigue, bone pain, renal impairment, anaemia in 70.0% of cases, bone lesions in 60.0% of cases, renal impairment in 40.0% of cases, and hypercalcaemia in 51.4% of cases. 1q21 amplification was noted in 50% of cases, extramedullary disease occurred in 20% of cases, and 90% of patients had λ light chain disease.18
IgD-secreting plasma cells originate from somatic hypermutation of the IgD region of germinal centre B cells.19,25 In contrast to other subtypes of myeloma, there is a predominance of λ light chain in IgD myeloma (70–90%), compared to κ light chain (3–4%).26,27 An increased survival has also been reported in patients with λ subtype.5 In the present study, 80% of the light chain was λ. Recently, detection of cytoplasmic IgD by flow cytometry was identified as a sensitive way to diagnose IgD myeloma.28
Cytogenetic changes have an important role in the pathogenesis of myeloma. High risk chromosomal changes in IgD myeloma are reported to range from 33–53%.17 Complex karyotype has been reported in 21% of patients, of which 90% had TP53 gene deletion or 1q21 amplification, which is considered to be one of the poor prognostic factors in IgD myeloma.29,30 IgD levels in serum are generally very low, and may escape detection, leading to the
misdiagnosis of IgD myeloma as non-secretory myeloma.19 The role of N-glycan biomarkers in the diagnosis and prognosis of IgD myeloma has also been studied.31 Egan et al.32 reported on interphase fluorescence in situ hybridisation from 29 cases of IgD myeloma. They showed a decreased OS in patients aged ≥70 years, and better outcomes in those with κ light chain restriction. Patients who were CD56-positive had longer survival than those lacking CD56.32
Agbuduwe et al.33 compared the clinical characteristics and outcomes of patients with IgD myeloma from UK Phase III clinical trials, before 2002 and after 2002. IgD myeloma comprised 1.6% and 1.2% of the two groups, respectively. It was associated with male predominance, low level of paraproteins, and λ light chains. The frequency of high-risk cytogenetics was similar compared to other types. The recent trials showed a higher response rate and median OS compared to those prior to 2002.33
Liu et al.34 carried out a multicentre retrospective study to evaluate the prevalence, clinical features, and prognosis of IgD myeloma, and to develop and validate a prognostic model, including 356 patients with IgD myeloma from 14 centres in the Asian Myeloma Network (AMN). IgD myeloma represented 2.0–8.8% of all patients with myeloma. The clinical characteristics of IgD myeloma were compared with 712 nonIgD myeloma patients. IgD myeloma was more common in males, younger patients, and patients who had advanced revised-ISS Stage III, hypercalcaemia, elevated creatinine levels, and elevated lactate dehydrogenase. A total of 40.6% of patients had abnormal karyotypes, and the frequency of chromosomal translocation t(11;14) was significantly higher than in non-IgD subtypes. However, the cytogenetic abnormalities did not have an impact on survival.34
Treatment of IgD myeloma is similar to other subtypes of myeloma. Although the survival of patients with IgD myeloma is shorter compared to other subtypes, the outcome of IgD myeloma is improving with the use of novel agents and autologous transplantation.35,36 The median survival of patients with IgD myeloma who received traditional chemotherapy was <2 years.9 Novel agents have improved the survival in these patients.5,17 Studies comparing bortezomib-based regimens with non-bortezomib-based regimens
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 101
showed higher PFS and OS with bortezomibbased treatments.17
Blade et al.7 reported a median OS of 21 months, with 3-year and 5-year survival of 26% and 21%, respectively. In the AMN study, the median OS was 36.5 months. Patients who received immunomodulatory drugs had better OS, and patients who underwent autologous stem cell transplant (ASCT) had a median OS of 45.7 months.34 Kim et al.37 reported on 75 patients with IgD myeloma from the Korean Myeloma Registry. In the current study, all patients received bortezomib-based treatment, 50% of patients were alive at 2 years, and the median OS was 21 months. Table 3 gives a summary of clinical characteristics and outcomes of salient studies in IgD myeloma published in literature, and compared with the present study.
New generation agents pomalidomide, proteasome inhibitors carfilzomib and ixazomib, histone deacetylase inhibitors panobinostat and vorinostat, and monoclonal antibodies daratumumab and elotuzumab, may be promising in the treatment of IgD myeloma, but have not yet been verified in clinical trials. Studies comparing the outcomes following chemotherapy versus ASCT showed significant survival benefit in patients treated with ASCT.12,14,15 The use of high-dose chemotherapy followed by ASCT increased OS and PFS by 63% and 69%, respectively, compared to patients treated with conventional chemotherapy.38 However, a comparison of the outcome of patients with IgD myeloma who underwent ASCT with patients with non-IgD myeloma did not show any significant difference in PFS and OS.39 Venetoclax, a Bcl-2 inhibitor, might provide a new option for patients with t(11:14) translocation
in view of the increased expression of BCL-2 in patients with IgD myeloma.34 Recently, sensitive quantitative IgD assays were shown to increase the PFS prediction accuracy in IgD myeloma.40 The relevant clinical role of laboratory in the detection of this rare disease was also highlighted by Intra et al.41
This study has some limitations. The authors do not have data on non-IgD myeloma from their institute; hence they are unable to compare the results of IgD and non-IgD myeloma. They are also unable to risk stratify based on cytogenetics, since the data were not available.
CONCLUSION
IgD myeloma is a rare subtype of MM, associated with a high incidence of renal failure, hypercalcaemia, extraosseous disease, amyloidosis, and Bence–Jones proteinuria. IgD λ disease is more frequent, unlike other subtypes of MM. Since IgD levels are generally very low in the serum, it may escape detection, and may lead to misdiagnosis as non-secretory myeloma. Immunofixation electrophoresis is very helpful in making the diagnosis, as in the authors’ case. Treatment is similar to other myeloma subtypes. Bortezomib-based chemotherapy is an effective treatment , with 50% of patients alive at 2 years. The outcome of IgD myeloma has improved, with the use of newer drugs, and with ASCT. More studies with a larger number of patients are needed to help understand the biology, and improve the outcome, of this rare myeloma subtype.
Article 102 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
1 Jin Liu 202134 356 56.0 years M: 241 F: 115
2 Selene 201919 166 54.5: 65.0 years M: 104 F: 62
λ: 88.8% κ: 11.2%
Anaemia: 64.9%
RI: 38.5%
HC 23.9%
EM: 19.1%
λ: 136 κ: 30
Anaemia: 69.8%
Bone pain: 55.9%
RI: 63%
EM: 28.3%
HC: 9%
BJP: 64.5%
Amyloid: 3.5%
Infection: 47.1%
I: 70 II: 64 III: 222
n = 147 I: 21 II: 36 III: 90
N/A t(11:14): 29.2% >50% plasma cells: 149
>5 µg/mL: 62% Abnormal: 41/56
>40% plasma cells: 95.6%
ORR: 88.8% MOS: 36.5 MOS for ASCT: 45.7
RR: 83.9% MOS 9–62
ASCT: 37
Novel agents MOS: 23
Conventional MOS: 14
3 Qian Zhao 201930 13 52.0 years M: 8 F: 5
4 Wang 201617 68 56.5 years M: 44 F: 24
λ: 12 κ: 1
Bone lesion: 76.9%
RI: 69.2%
EM: 15.4%
HC: 23.1%
Amyloid: 30.8%
λ: 55 κ: 13
Bone pain: 48.6%
RI: 27.9%
EM: 5.9%
Anaemia:
64.7%
HC: 4.4%
Amyloid: 2.9%
Pleural
effusion: 10.3%
III: 13 (100%) >5 µg/mL: 13 12 N/A Median PFS: 10 MOS: 22.9
5 Djidjik 20153 17 60.0 years M: 12 F: 5
6 Pisani 201238 17 55.0 years M: 11 F: 6
λ: 65% κ: 35%
Anaemia: 93%
Bone pain:
75%
RI: 82%
Amyloid: 6%
HC: 37%
BJP: 71%
λ: 11 κ: 6
Bone lesion:
82%
RI: 47%
EM: 0%
BJP: 70%
HC: 1%
Amyloid: 1%
I: 5 II: 24 III: 39
Median: 6.96 20/38 49.5% plasma cells
III: 100% Median: 4.5 ng/mL N/A N/A
ORR: 89.7% MOS: 24
PFS: 15.5
3-year OS: 69%
3-year PFS: 43%
5-year OS: 45%
5-year PFS: 13%
MS: 9 2-year survival: 12%
I: 7 II: 2 III: 5 UK: 3
>5 µg/mL: 29% 6 30% plasma cells
Chemotherapy MOS: 34
Median PFS: 18
ASCT (n=11)
ORR: 90% MOS and PFS not reached
and Sex (n)
Subtype
Features
Table 3: Summary of clinical characteristics and outcomes of studies in immunoglobin D myeloma, published in literature.
Reference Number of Patients Median Age
Light Chain
Clinical
ISS Stage (n) β2 microglobulin Cytogenetics Bone Marrow Plasma Cell Outcome and MOS (months)
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 103
Table 3
continued.
Reference
Number of
7 Kim 201137 75 57.0 years
M: 50
F: 25
8 Manish Sharma 201039
15 with ASCT 51.0 years M: 13 F: 2
9 Bladé 19947 53 60.0 years
M: 33
F: 20
10 Present study 12 48.5 years M: 9
F: 3
λ: 67 (89%)
Bone lesion: 94%
RI: 53%
HC: 27%
EM : 10.7%
κ: 67%
RI: 40%
EM: 20%
HC: 30%
λ: 60%
κ: 38%
Indeterminate: 2%
λ: 10 κ: 2
Bone pain: 72%
BJP: 96%
RI: 33%
HC: 22%
EM: 19%
Amyloid: 19%
Bone lesion: 100%
Anaemia: 66%
RI: 42%
BJP: 42%
HC: 25%
Amyloid:
25%
POEMS: 8.3%
I: 6 II: 20 III: 48
I: 3 II: 3 III: 4 UK: 5
Median: 8 mg/dL >5.5 mg/ dL: 65%
References
1. Siegel R et al. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11-30.
2. Kyle RA et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
3. Djidjik R et al. IgD multiple myeloma: clinical, biological features and prognostic value of the serum free light chain assay. Pathol Biol (Paris). 2015;63(4-5):210-4.
4. Bladé J, Kyle RA. Nonsecretory myeloma, immunoglobulin D myeloma, and plasma cell leukemia.
Plasma
26 >50%
plasma cells: 52%
Outcome and MOS (months)
ORR: 81%
MOS: 18.5
Median PFS: 10
ASCT (n=34)
MOS: 30
>3.5 mg/ dL: 40% 7 N/A ASCT ORR: 86%
II or III: 46% >6 ng/mL: 31% N/A >40%
plasma cells: 45%
Hematol Oncol Clin North Am. 1999;13(6):1259-72.
5. Ongoren S et al. IgD Multiple myeloma, descriptive report of eight cases, single centre experience. Clin Lymphoma Myeloma Leuk. 2015;15 (Suppl 3):e313.
6. Pandey S, Kyle RA. Unusual myelomas: a review of IgD and IgE variants. Oncology (Williston Park). 2013;27(8):798-803.
7. Bladé J et al. Immunoglobulin D multiple myeloma: presenting features, response to therapy, and survival in a series of 53 cases. J Clin Oncol. 1994;12(11):2398-404.
3-year PFS: 38%
3-year OS: 64%
ORR: 58%
MOS: 21 3-year OS: 36%
5-year OS: 21%
8. Sinclair D. IgD myeloma: clinical, biological and laboratory features. Clin Lab. 2002;48(11-12):617-22.
9. Lu J et al. Clinical features and treatment outcome in newly diagnosed Chinese patients with multiple myeloma: results of a multicenter analysis. Blood Cancer J. 2014;4(8):e239.
10. Li Y, Cai Z. Clinical characteristics and survival of patients with IgD multiple myeloma. Blood Sci. 2021;3(2):57-58.
11. Zagouri F et al.; Greek Myeloma Study Group. Immunoglobulin D myeloma: clinical features and outcome in the era of novel agents.
8.4 µg/mL N/A N/A MOS: 21 2-year OS: 50% Article 104 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
Patients Median Age and Sex (n)
ASCT: autologous stem cell transplantation; BJP: Bence–Jones protein; EM: extramedullary; F: female; HC: hypercalcaemia; ISS: International Staging System; M: male; MOS: median overall survival; N/A: not applicable; ORR: overall response rate; OS: overall survival; PFS: progression-free survival; POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes; RI: renal insufficiency. Chain Subtype
Light
Clinical Features ISS Stage (n)
β2 microglobulin Cytogenetics Bone Marrow
Cell
I: 3 II: 1 III: 8
Eur J Haematol. 2014;92(4):308-12.
12. Wechalekar A et al. IgD multiple myeloma--a clinical profile and outcome with chemotherapy and autologous stem cell transplantation. Ann Hematol. 2005;84(2):115-7.
13. Rowe DS, Fahey JL. A new class of human immunoglobulins. I. A unique myeloma protein. J Exp Med. 1965;121(1):171-84.
14. Morris C et al.; Myeloma Subcommittee of Chronic Leukaemia Working Party of EBMT. Efficacy and outcome of autologous transplantation in rare myelomas. Haematologica. 2010;95(12):212633.
15. Reece DE et al. Outcome of patients with IgD and IgM multiple myeloma undergoing autologous hematopoietic stem cell transplantation: a retrospective CIBMTR study. Clin Lymphoma Myeloma Leuk. 2010;10(6):458-63.
16. Bladé J et al. Presenting features and prognosis in 72 patients with multiple myeloma who were younger than 40 years. Br J Haematol. 1996;93(2):345-51.
17. Wang GR et al. Immunoglobulin D multiple myeloma: disease profile, therapeutic response, and survival. Acta Haematol. 2016;136(3):140-6.
18. Gao XY et al. Clinical characteristics and survival analysis of patients with IgD multiple myeloma. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2021;29(2):547-52.
19. Selene II et al. Presentation patterns, diagnostic markers, management strategies, and outcomes of IgD multiple myeloma: a systematic review of literature. Cureus. 2019;11(2):e4011.
20. Modi J et al. Immunoglobulin D multiple myeloma with rapidly progressing renal failure. J Clin Med Res. 2015;7(8):653-5.
21. Rabrenović V et al. Kidney failure as an unusual initial presentation of biclonal gammopathy (IgD multiple myeloma associated with light chain
disease)-a case report. Vojnosanit Pregl. 2015;72(2):196-9.
22. Gao L et al. Non-secreting multiple myeloma switches to IgD of lamda type: a case report and review of literature. Int J Clin Exp Med. 2015;8(9):16984-90.
23. Lescoat A et al. Demonstration of the cause of acute renal failure in a case of IgD multiple myeloma. Br J Haematol. 2015;168(2):162.
24. Yan G et al. Renal insufficiency predicts worse prognosis in newly diagnosed IgD multiple myeloma patients. Front Oncol. 2022;12:1012889.
25. Sharma A et al. An extremely rare manifestation of multiple myeloma: an Immunoglobulin D secreting testicular plasmacytoma. Cureus. 2017;9(6):e1400.
26. Yang W et al. IgD-λ multiple myeloma accompanying with elevated AFP level: a case report and literature review. Int J Clin Exp Med. 2018;11(5):5176-180.
27. Laribi K, Lemaire P. IgD κ multiple myeloma and myelodysplastic syndrome. Blood. 2017;129(15):2203.
28. Wang W et al. Detection of intracellular IgD using flow cytometry could be a novel and supplementary method to diagnose IgD multiple myeloma. BMC Cancer. 2018;18(1):650.
29. Li YY et al. [Clinical characteristics analyses of 27 cases of immunoglobin D multiple myeloma]. Zhonghua Xue Ye Xue Za Zhi. 2017;38(10):893-5. (In Chinese).
30. Zhao Q et al. Poor outcomes of immunoglobulin D multiple myeloma patients in the era of novel agents: a single-center experience. Cancer Commun (Lond). 2019;39(1):51.
31. Chen J et al. N-glycosylation of serum proteins for the assessment of patients with IgD multiple myeloma. BMC Cancer. 2017;17(1):881.
32. Egan PA et al. IgD multiple myeloma:
biology, diagnosis, and treatment. Leuk Lymphoma. 2022;63(14): 3433-7.
33. Agbuduwe C et al. Clinical characteristics and outcomes of IgD myeloma: experience across UK national trials. Blood Adv. 2022;6(17):5113-23.
34. Liu J et al. Clinical features and survival outcomes in IgD myeloma: a study by Asia Myeloma Network (AMN). Leukemia. 2021;35(6): 1797-802.
35. Chen L et al. Clinical characteristics and prognosis of immunoglobulin D myeloma in the novel agent era. Ann Hematol. 2019;98(4):963-70.
36. Kang J et al. Efficacy and survival outcome associated with the use of novel agents and autologous stem cell transplantation in cases of immunoglobulin D multiple myeloma in Korea. Acta Haematol. 2018;139(3):185-92.
37. Kim MK et al.; Korean Multiple Myeloma Working Party. Immunoglobulin D multiple myeloma: response to therapy, survival, and prognostic factors in 75 patients. Ann Oncol. 2011;22(2):411-6.
38. Pisani F et al.; Multiple Myeloma GIMEMA-Latium Region Working Group, Italy. IgD multiple myeloma a descriptive report of 17 cases: survival and response to therapy. J Exp Clin Cancer Res. 2012;31(1):17.
39. Sharma M et al. The outcome of IgD myeloma after autologous hematopoietic stem cell transplantation is similar to other Ig subtypes. Am J Hematol. 2010;85(7):502-4.
40. Liu J et al. Sensitive quantitative IgD assay increases progression-free survival prediction accuracy in IgD plasma cell myeloma. Leukemia. 2023;37(2):497-9.
41. Intra J et al. IgD multiple myeloma: the relevant clinical role of laboratory in the detection of rare plasma cell neoplasms. Am J Med Sci. 2022; 364(4):505-7.
Article Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 105 FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Membranous Nephropathy and Pulmonary Tuberculosis: An Uncommon Combination: Case Report
Authors:
Disclosure:
*Puneet Bhuwania,1 Aniket Mule,2 Sanggita Checker2
1. Department of Nephrology, Wockhardt Hospitals, Mira Bhayandar, Maharashtra, India
2. Department of Medicine, Wockhardt Hospitals, Mira Bhayandar, Maharashtra, India
*Correspondence to punit101.pb@gmail.com
The authors have declared no conflicts of interest. Consent has been taken from the patient about publication of his condition in the journal.
Received: 09.02.23
Accepted: 15.01.24
Keywords: Glomerulonephritis (GN), membranous nephropathy, tuberculosis (TB).
Citation: EMJ. 2024;9[1]:106-110. DOI/10.33590/emj/11000011. https://doi.org/10.33590/emj/11000011.
Abstract
It is imperative to evaluate for secondary causes of membranous glomerulonephritis, from infections such as hepatitis B and C, viruses and parasites, autoimmune diseases like systemic lupus erythematosus, and other neoplasms. Tuberculosis associated with membranous glomerulonephritis is rare. The authors report a case of microbiologically proven pulmonary tuberculosis and membranous nephropathy occurring concurrently in the same patient. Antitubercular therapy alone was sufficient to cause improvement in the patient. Tuberculosis should be recognised as a potentially treatable infectious cause of secondary membranous nephropathy.
Key Points
1. A thorough evaluation always has to be done to rule out secondary causes of membranous nephropathy.
2. Tuberculosis affects the kidney insidiously, and is often misdiagnosed as primary glomerulonephritis.
3. Therapy can effectively mitigate both tuberculosis and the associated glomerulonephritis.
INTRODUCTION
Mycobacterium tuberculosis causing glomerulonephritis (GN) is a rare occurrence,1 and its association has been seldom reported.2
On account of its non-specific and atypical manifestations, tuberculosis-associated GN (TB-GN) becomes an unusual diagnosis. The usual presentation is oedema, proteinuria, haematuria, and varying degrees of kidney
Case Report 106 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0
dysfunction, which resemble symptoms of primary GN, thus, often leading to a misdiagnosis of primary GN rather than TB-GN. Deterioration of renal function and the spread of TB are potentially life-threatening complications, which occur if patients are treated with glucocorticoids or/and other immunosuppressive agents. Here, the index case the authors report is of a 20-year-old male with membranous nephropathy (MN) secondary to pulmonary tuberculosis (consent given).
CASE REPORT
The index case was brought to Wockhardt Hospitals, Mira Bhayandar, Maharashtra, India, in altered sensorium, and short duration (of about 1 week) history of fever and lower extremity oedema. The patient did not complain of cough with or without expectoration, or give history of weight loss. On further physical examination, a blood pressure of 90/60 mmHg,
pallor, and bilateral pitting pedal oedema were found.
No palpable lymphadenopathy, skin rash, or focal neurologic deficit were documented. Laboratory analyses yielded the following findings: mild anaemia, normal white blood cell count, and mild thrombocytopenia; normal serum creatinine; urine sediment was active, i.e. 4+ protein, 10–12 red blood cells, 6–8 white blood cells per high-power field, urine protein creatinine ratio of 7.83, and a serum albumin of 1.4g/dl; transaminitis and serositis (pleural effusion and ascites). Neuroimaging studies were normal. Cerebrospinal fluid revealed five cells per high-power field (lymphocyte predominance). Viral markers like hepatitis B or C, anti-streptolysin O, auto-immune workup (antinuclear antibodies and rheumatoid factor), anti-PLA2R antibody, and complement levels, along with serum and urine immunofixation electrophoresis and tumour markers, were all negative (Table 1). Cultures were sterile. Ultrasonography of the kidneys revealed the
protein, 10–12 RBC/HPF, 6–8 WBC/HPF
Anti-streptolysin
ANA: antinuclear antibodies; HPF: high-power field; RBC: red blood cell; WBC: white blood cell.
Laboratory parameters Values (units) Haemoglobin 10 g/dL Total leucocyte count 6,000 cells /mm3 Platelet count 120,000 /mm3 Erythrocyte sedimentation rate 75 mm/hr Serum albumin 1.4 g/dL Serum creatinine 0.7 mg/dL
routine 4+
Urine protein creatinine ratio 7.83 mg/mg Total cholesterol 250 mg/dL HIV, hepatitis B, anti-hepatitis C antibody Negative Anti-PLA2R antibody <2 RU/mL Rheumatoid factor <10 IU/mL
ANA (immunofluorescence) Negative
three levels 125 mg/dL
Urine
Serum
Complement:
O titres Negative
Case Report Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 107
Table 1: Laboratory values: initial.
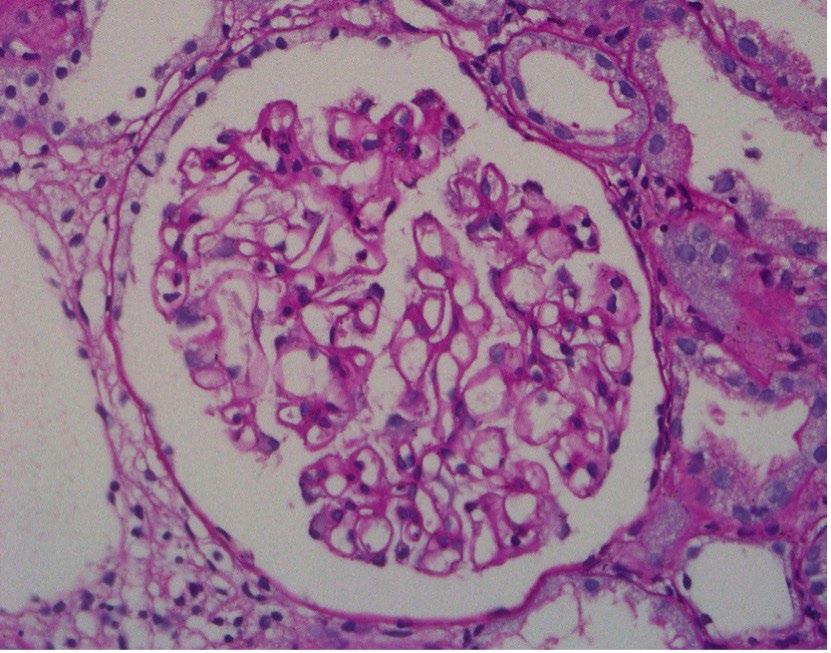
normal diameters with good corticomedullary differentiation, which subsequently led to the diagnosis of acute GN.
Initially, the patient was given supportive therapy and treated with lines of a non-specific viral aetiology. Once his platelet counts stabilised, a kidney biopsy was carried out. Light microscopy examination of the specimen revealed 34 mildly enlarged normocellular glomeruli with irregular thickening of basement membranes (Figure 1), with silver staining showing thickened glomerular basement membranes, with small spikes and tubules showing prominent zones of injury. The arterioles were unremarkable, and there was absence of granuloma in the renal tissue sample. Immunofluorescence revealed positive IgG staining along the glomerular capillary wall (Figure 2), with similar staining intensity of κ and λ light chains. The glomeruli did not stain for IgM, IgA, C3, C1q, IgG4, or PLA2R, and Congo red stain was negative. MN was the pathological diagnosis contemplated on the basis of the biopsy. To explore secondary causes of MN, the patient was evaluated but to no avail; hence, patient was started on angiotensin receptor blockers, and discharged in afebrile state.
One week later, the patient again became febrile and developed hypotension; hence, angiotensin receptor blockers were stopped and he underwent PET-CT scan. This revealed a sub-lobar consolidation with cavity formation, especially in the left lower lobe; the presence of metabolically active mediastinal, subcarinal, and bilateral hilar lymph nodes with necrosis (Figure 3); and thrombo-emboli in the left upper and right lower lobe pulmonary arteries. Therefore, to confirm the aetiology, the authors also carried out bronchoalveolar lavage (BAL), which revealed M. tuberculosis by GeneXpert® (Cepheid®, Sunnyvale, California, USA; seminested Real time PCR).
The index case was initiated on a four-drug anti-tuberculosis regimen, encompassing isoniazid (H), rifampicin (R), ethambutol (E), and pyrazinamide (Z). However, the patient subsequently developed drug-induced hepatitis; hence, his drug regimen was optimised to levofloxacin (L), H, R, and E for the initial 2 months, followed by H, R, and E for the subsequent 4 months, along with oral anti-coagulation targeting a PT-INR of around 2.5. After 2 months of treatment, the patient’s urinary protein creatinine ratio reduced to 0.5, and serum albumin increased to 3.5 g/dL.
Figure 1: Periodic Acid Schiff stain showing glomerular basement membrane thickening (400x).
108 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report

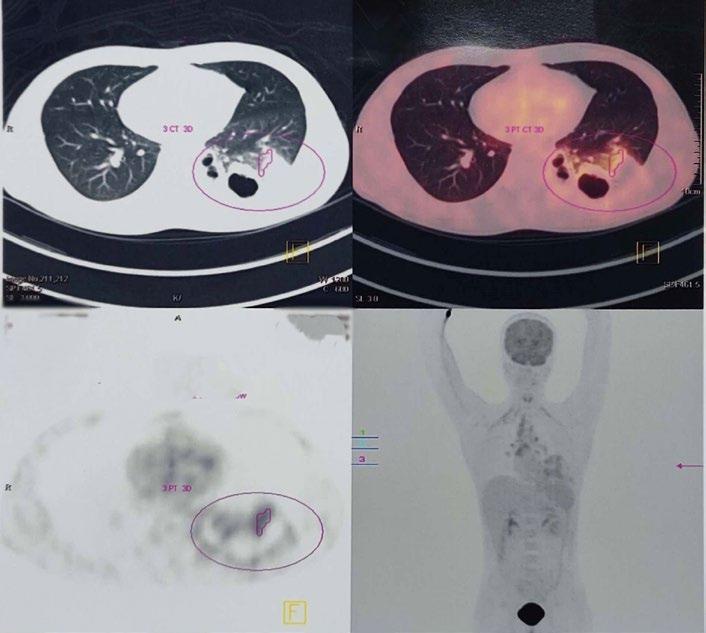 Figure 2: Immunofluorescence stain showing irregular IgG deposition (400x).
Figure 2: Immunofluorescence stain showing irregular IgG deposition (400x).
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 109 Case Report
Figure 3: PET-CT scan showing sub-lobar consolidation with cavity formation and presence of metabolically active mediastinal, subcarinal, and bilateral hilar lymph nodes with necrosis.
DISCUSSION
As per the information currently available, membranous pattern of glomerular injury is unique in a patient with TB, and, so far, has been seldomly documented in the literature. Based on the available clinical data and investigations, secondary causes like medication use, neoplasms, autoimmune diseases, and viral hepatitis were all winnowed out. A clue to suspect TB was offered by the abnormal findings of PET-CT and non-resolving fever. Hence, a final diagnosis of TB leading to the development of MN was considered, based on the positive BAL sample’s detection of M. tuberculosis by PCR method, and the index case’s favourable response to anti-TB treatment, which, in turn, demonstrates the cause-and-effect relationship between TB and the glomerular injury. GN associated with TB often tends to complicate the treatment in terms of the sequence and modality of therapeutic options, i.e., anti-TB drugs and/or immuno-suppressive agents. The latest available information has revealed GNs of various forms which are associated tuberculosis to show inconsistent responses to several available treatment options.3 Anti-tuberculosis drugs reduce the antigen load, which in turn reduces immune complex formation, all by decreasing the mycobacterial load from circulation.4
In the index case, the authors’ patient presented with nephrotic syndrome, and normal kidney function tests, but was found to have active M. tuberculosis in BAL; hence, immunosuppression was not considered. Treatment for tuberculosis itself provided favourable results by causing amelioration of proteinuria and symptoms; hence, the aetiologic link was further strengthened. Solak et al.1 identified 15 cases of GN associated with TB. Of these, six cases of IgA nephropathy were noted: four of crescentic GN; two mesangioproliferative; and one each of collapsing GN, mesangio-capillary GN and membranous GN.1 A case of MN and TB has also been published in Japanese literature, but it was a diagnosis of renal TB.5
CONCLUSIONS
To summarise, based on the authors’ index case, several points need to be emphasised.
Firstly, a thorough evaluation should be done in MN to rule out secondary cause, especially in patients at either end of the age spectrum. Secondly, TB affects the kidney insidiously, and is often diagnosed as de novo or primary GN due to its indistinct manifestations. Thirdly, therapy for treatment of TB can effectively mitigate both TB and the associated GN. Lastly, prior to commencement of any therapy, kidney biopsy acts as an important tool in securing a precise diagnosis.
References
1. Solak Y et al Glomerulonephritis associated with tuberculosis: a case report and literature review. Kaohsiung J Med Sci. 2013;29(6):337-42.
2. Kanaji N et al. Membranous glomerulonephritis associated with Mycobacterium shimoidei
pulmonary infection. Am J Case Rep. 2013;14:543-7.
3. Waikhom R et al. Rapidly progressive glomerulonephritis in tuberculosis. Saudi J Kidney Dis Transpl 2014;25(4):872-5.
4. Keven K et al A case of pulmonary tuberculosis associated with IgA
nephropathy. Int J Tuberc Lung Dis. 2004;8(10):1274-5.
5. Suzuki Y et al. [A case of nephrotic syndrome with membranous nephropathy and renal tuberculous granuloma]. Nihon Naika Gakkai Zasshi. 1989;78:1181-6. (In Japanese).
110 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Post-endoscopic Retrograde
Cholangiopancreatography Air Leak Syndrome: An Overview of Current Perspectives
Authors:
*Sheharyar Zameer,1 Kashmala Safdar,1 Huma Ahmed Khan,1 Umer Anwar,1 Fatima Sohail,1 Rasikh Maqsood1
1. Fauji Foundation Hospital, Rawalpindi, Pakistan *Correspondence to sheriyar55@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 30.09.23
Accepted: 31.01.24
Keywords: Air embolism, pneumomediastinum, pneumoperitoneum, pneumothorax, subcutaneous emphysema.
Citation: EMJ. 2024;9[1]:111-117. DOI/10.33590/emj/10305274. https://doi.org/10.33590/emj/10305274.
Abstract

Post-endoscopic retrograde cholangiopancreatography (ERCP) air leak (PEAL) syndrome is a rare complication that includes pneumothorax, pneumomediastinum, pneumoperitoneum, air embolism, and subcutaneous emphysema. A 71-year-old female diagnosed with mild acute biliary pancreatitis, who underwent ERCP for stone retrieval developed neck, chest, and abdominal pain, as well as swelling of the neck, along with crepitus all along the neck and face. CT scan showed pneumoperitoneum, pneumomediastinum, and subcutaneous emphysema. The patient was diagnosed as a case of PEAL syndrome, and was managed conservatively. She ultimately underwent an uneventful cholecystectomy with peroperative stone retrieval. PEAL syndrome, albeit rare, can be a potentially life-threatening complication following ERCP, which requires continuous monitoring. It may be managed conservatively, endoscopically, or surgically.
Key Points
1. Post-endoscopic retrograde cholangiopancreatography (ERCP) air leak (PEAL) syndrome is any of the various combinations of pneumothorax, pneumomediastinum, pneumoperitoneum, air embolism, and subcutaneous emphysema occurring secondary to injury during ERCP.
2. Although rare, it is one of the life-threatening complications of ERCP that is often overlooked and misunderstood.
3. Management of post-ERCP air leak syndrome is mainly based on conservation treatment; however, a select few require surgical intervention for correction.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 111 Article
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) includes specialised techniques, such as sphincterotomy, balloon dilation, nasobiliary drainage, and stent placement. This makes it more challenging than oesophagogastroduodenoscopy, and gives rise to a unique set of complications, such as pancreatitis, cholangitis, gastrointestinal bleeding, and perforation.1 The rarest of these complications is perforation, with an incidence of 0.6–0.8%, which can lead to conditions ranging from post-ERCP air leak (PEAL) syndrome to peritonitis.1,2
PEAL syndrome encompasses a range of clinical manifestations attributed to iatrogenic perforation of the duodenum, ampulla, or biliary tree after ERCP, potentially resulting in pneumoperitoneum, pneumomediastinum, pneumothorax, air embolism, or subcutaneous emphysema.1-3 It is important to note that pneumobilia is not considered a part of PEAL syndrome.4 In this context, the authors present a case of PEAL syndrome, which, to their knowledge, is the first case report of its kind from Pakistan. The study introduces the term of PEAL syndrome, and outlines recommendations, along with managerial principles for the treatment of this complication. Informed written consent was taken from the patient regarding the use of images and publication of the case.
CASE DESCRIPTION
A 71-year-old female of South Asian origin presented to the surgical outpatient department with an acute history of abdominal pain associated with nausea and vomiting for 3 days. She had moderately severe, dull, intermittent epigastric pain radiating to the back. Her past medical history was unremarkable, and she did not have any relevant history of drug use or genetic disorders.
On examination, she was vitally stable, with a pulse rate of 77 bpm, blood pressure of 110/75 mmHg, respiratory rate of 15 breaths per minute, temperature of 98 °F, and SpO2 of 99% at room air. She was thin and lean, and her systemic examination was unremarkable. An abdominal ultrasound showed a well-distended gallbladder
with multiple echogenic calculi (the largest measuring 0.8 cm). Incidentally, two echogenic calculi (the largest measuring 1.1 cm) were seen in the common bile duct, causing proximal dilation to 1.3 cm. Her serum amylase was significantly elevated at 756 U/L. The rest of her investigations were within normal limits, and her Ranson’s score was calculated to be less than three.
She was diagnosed with acute biliary pancreatitis of the mild category, and was managed conservatively with adjusted doses of ketorolac, ondansetron, and omeprazole. An ERCP was planned by the Gastroenterology team for stone retrieval. During ERCP, cannulation of the major papilla was attempted with the standard guidewire technique. However, it could not be done successfully, even after multiple attempts. The head endoscopist took the decision to proceed with a needle knife papillotomy to gain access; however, cannulation could still not be done successfully, and the procedure was abandoned. The Gastroenterology team rescheduled the ERCP procedure to try again after a certain time.
The patient had an uneventful initial recovery; however, on the first post-procedure day, she reported pain in her neck, chest, and abdomen, along with lethargy. On examination, she had gross distension of the neck with the presence of crepitus all around the neck and on both cheeks. Her chest X-ray showed pneumomediastinum and pneumoperitoneum, as shown in Figure 1.
She underwent an urgent CT scan of the chest and abdomen under controlled conditions. It showed subcutaneous emphysema, pneumomediastinum, and pneumoperitoneum with no obvious site of perforation, as shown in Figure 2. The patient was shifted to the High Dependency Unit, and was managed conservatively with continuous monitoring and symptomatic treatment. She was started on an adjusted dose of cefuroxime (750 mg IV every 8 hours for 7 days). She was initially kept nil per os, and a nasogastric tube was kept in place. With no progressive clinical deterioration, the nasogastric tube was removed and she was allowed to ingest liquids and then semi-solids orally after 48 hours. She received maintenance fluids during this period; however, she was not started on total parenteral nutrition. By the fourth post-procedure day, she was allowed a soft diet.
112 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
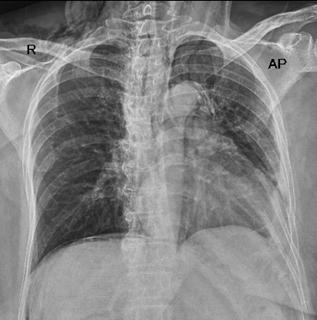
 Figure 1: Chest X-ray showing pneumomediastinum and pneumoperitoneum.
Figure 1: Chest X-ray showing pneumomediastinum and pneumoperitoneum.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 113 Article
Figure 2: CT Scan showing pneumomediastinum (A), pneumoperitoneum (B), and subcutaneous emphysema (C).
Type Injury Management
I Lateral or medial duodenal wall perforation, endoscope-related
II Perivaterian perforation, sphincterotomy-related
III Ductal or duodenal perforation due to endoscopic instruments
IV Guidewire-related perforation with presence of retroperitoneal air alone
By the seventh post-procedure day, she had complete resolution of symptoms, and her amylase spontaneously normalised. On account of her improvement, her rescheduled ERCP was called off, and she was discharged with regular follow-ups. She was readmitted 6 weeks later and underwent an uneventful cholecystectomy with stone retrieval from the biliary ducts.
DISCUSSION
During ERCP, perforations may occur in the duodenum via stents; in the ampulla via sphincterotomy; or in the biliary channels via guidewires, stents, and balloons. Mortality rates have been reported to be as high as 34.4% (with an average of 0.3–3.5%).1,2 Multiple risk factors have been identified, including patient factors, such as senility, female sex, and hypertension; disease factors, such as sphincter of Oddi dysfunction, juxtapapillary duodenal diverticula, biliary strictures, papillary stenosis, Billroth II reconstruction, and pre-cut sphincterotomy; and technical factors, such as difficult cannulation, an unskilled endoscopist, and prolonged procedure time.5,6
It is postulated that there are two major mechanisms as to how the air traverses during PEAL syndrome. The first is that air enters the retroperitoneal space after an interruption in the duodenal barrier, tracking the deep fascial places from the retroperitoneal space to peritoneum,
Typically requires immediate surgery
Most seal spontaneously within 48–72 hours, but about 30% will require surgery
Most seal spontaneously with conservative management, with or without stent placement
Mostly treated conservatively
mediastinum, and subcutaneous tissue, which are contiguous with the diaphragmatic hiatus and major thoracic airways. The second states that air passes to the right pararenal spaces, from where it reaches the diaphragmatic hiatus, leading to pneumomediastinum, pneumothorax, and cervical subcutaneous emphysema.7
A widely used classification system for ERCPrelated perforations is the Stapfer classification, as shown in Table 1.7,8 However, it is not commonly used in clinical practice, due to its focus on the location and severity of perforation. For this reason, alternative classifications have been proposed that take into account the instrument causing the perforation.2
The European Society of Gastrointestinal Endoscopy (ESGE) reports causes of post-ERCP perforation as endoscopic sphincterotomy (56%), guidewire manipulation (23%), stricture dilation (4%), and stent insertion/migration (3%).9
Clinical manifestations of ERCP-related perforations include epigastric or generalised abdominal pain associated with non-specific complaints, like nausea, vomiting, and dyspepsia. Depending on the degree of perforation, the subsequent development of PEAL syndrome may have additional features.5,6
The ESGE recommends an early contrast study during ERCP or CT scan, to assess for perforation in high degree of suspicion.4,9
Table 1: Srapfer et al.7 classification of iatrogenic perforation during endoscopic retrograde cholangiopancreatography.
114 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Treatment of the perforation itself includes conservative, endoscopic, and surgical options. Conservative treatment involves parenteral nutrition (for malnourished individuals, if feeding is not resumed in 7 days), antibiotics, nasogastric/nasoduodenal drainage, and symptomatic relief.9 Endoscopic options include using endoscopic clips alone for perforations <1 cm, or combined endoclips and endoloops, combined endoclips and double endoscopic band ligations, and endoscopic device closures for perforations >1 cm. Other options include vacuum therapy, tulip-bundle, metallic stenting, purse-string sutures, and fibrin glue.2,5,6 The most commonly employed tool, however, is to divert fluids from the perforation site via stenting.9
Surgery is required in approximately one-quarter of the cases. Surgical options typically include Graham patch repair or primary repair, and are offered to patients developing chemical peritonitis, purulent peritonitis, larger peritoneal collections, major contrast medium leak, unresolved problems like retained hardware that cannot be solved nonsurgically, or if the condition does not improve with conservative/endoscopic management.7,9 Once indicated, early surgery is preferred over delayed surgery due to increase in morbidity.6
The ESGE recommendations also mention the implementation of a written policy regarding management of iatrogenic perforations, reporting endoscopically identified perforation and early utilisation of CT scan in high index of suspicion.9
PEAL syndrome comprises five components, each with its own set of management principles: pneumothorax, pneumomediastinum, pneumoperitoneum, air embolism, and subcutaneous emphysema.4,6
Development of pneumothorax after ERCP may present with tachypnoea, respiratory distress, tracheal deviation, and hypoxia.10 It is typically on the right side, but may be bilateral.7 Diagnosis can be made clinically or through a chest X-ray or CT scan of the chest. Usual management involves supportive care of the airway, breathing, and circulation with continuous monitoring. Patients are placed in a position where they are comfortable, typically reverse Trendelenburg. In cases of tension pneumothorax or clinical deterioration, decompression via an intercostal drain is indicated.10
Post-ERCP pneumomediastinum, pneumoperitoneum, and subcutaneous emphysema typically do not require treatment, since the air is gradually absorbed. However, hyperbaric O2 therapy may expedite the process.8,11 Periocular subcutaneous oedema requires close monitoring for pressure effects on the orbit manifested by proptosis, raised intraocular pressure, or worsening of vision. In any of these symptoms, a decision may be warranted to perform emergency orbital decompression via lateral canthotomy/ cantholysis, needle decompression, or by decompression.11
Air embolism is an even rarer component of PEAL syndrome that can be fatal, and should be considered in patients with sudden clinical deterioration during, or immediately after, the procedure. Diagnosis may involve the use of precordial Doppler ultrasound and transoesophageal echocardiogram. Treatment mainly consists of supportive measures, including airway, breathing, and circulation management. Fluid resuscitation and vasopressors have been shown to improve cardiac output, while hyperbaric O2 therapy is initiated in suspected cerebral air embolism.3 A detailed algorithm for management is displayed in Figure 3.
PATIENT’S PERSPECTIVE
The patient reported that she initially felt very traumatised by the whole scenario, as her whole face, neck, chest, and the rest of her body were swollen. She further said she thought she could never look at herself again, but the doctors reassured her that everything was in control, and they were right. Slowly, things got better and she went back to the way she was.
CONCLUSIONS
PEAL syndrome is a rare complication of ERCP that is potentially life-threatening. Most components of PEAL syndrome are managed via supportive care, with most patients managed conservatively. However, a subset of patients will require endoscopic or surgical interventions to treat the underlying perforation.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 115 Article
Pulseless
Start ACLS protocol
Sudden clinical deterioration during or immediately after ERCP
Venous embolism
Shift to Trendelenburg position and aspirate from CVC
Adapted from Lanke et al.3
Diagnosis made on CXR; brain, chest, and abdomen CT; brain MRI; TOE; and precordial USG Gas embolism
Pulse detected; however, unstable
Secure airway, breathing, and circulation. Start hyperbaric O2, fluids, and vasopressors
Arterial embolism
Shift to supine position and maintain hyperbaric O2 therapy
ACLS: advanced cardiovascular life support; CVC: central venous catheter; CXR: chest X-ray; ERCP: endoscopic retrograde cholangiopancreatography; TOE: transoesophageal echocardiogram; USG: ultrasonography.
References
1. Cirocchi R et al. A systematic review of the management and outcome of ERCP related duodenal perforations using a standardized classification system. Surgeon. 2017;15(6):379-87.
2. Zhu G et al. Recent advances in prevention and management of endoscopic retrograde
cholangiopancreatography-related duodenal perforation. Wideochir Inne Tech Maloinwazyjne. 2021;16(1):19-29.
3. Lanke G, Adler DG. Gas embolism during endoscopic retrograde cholangiopancreatography: diagnosis and management. Ann Gastroenterol. 2019;32(2):156-67.
4. Manoharan D et al. Complications of endoscopic retrograde cholangiopancreatography: an imaging review. Abdom Radiol. 2019;44:2205-16.
5. Jiménez-Cubedo E et al. Review of duodenal perforations after endoscopic retrograde cholangiopancreatography in
Figure 3: Algorithm for management of post-endoscopic retrograde cholangiopancreatography air embolism.
116 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Hospital Puerta de Hierro from 1999 to 2014. Rev Esp Enferm Dig. 2018;110:515-9.
6. Weiser R et al. Management of endoscopic retrograde cholangiopancreatographyrelated perforations: experience of a tertiary center. Surgery. 2017;161(4):920-9.
7. Jha AK et al. Post‐endoscopic retrograde cholangiopancreatography pneumothorax: report of two cases and literature review. JGH Open.
2018;2(6):329-32.
8. Stapfer M et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy. Ann Surg. 2000;232(2):191-8.
9. Paspatis GA et al. Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement. Endoscopy. 2014;46(8):693-711.
10. Madani S et al. Bilateral pneumothorax: the cause of hypoxia during endoscopic retrograde cholangiopancreatography. Caspian J Intern Med. 2021;12(Suppl 2):426-30.
11. Lekha T et al. Periorbital and mediastinal emphysema after upper gastrointestinal endoscopy: case report of a rare complication. J Ophthalmic Vis Res. 2017;12(3):345-7.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 117 Article FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Liver Elastography for the Detection of Methotrexate-Induced Liver Injury: A Retrospective Study
Authors:
*Tim Brotherton,1 Maya Mahmoud,1 Sam Burton,1 Kamran Qureshi2
1. Department of Internal Medicine, SSM Health Saint Louis University Hospital, Missouri, USA
2. Department of Gastroenterology/Hepatology Division, SSM Health Saint Louis University Hospital, Missouri, USA

*Correspondence to timothy.brotherton@slucare.ssmhealth.com
Disclosure: The authors have declared no conflicts of interest.
Received: 22.10.23
Accepted: 05.02.24
Keywords: FibroScan®, fibrosis, liver, methotrexate (MTX), transient elastography (TE).
Citation: EMJ. 2024;9[1]:118-125. DOI/10.33590/emj/10304060. https://doi.org/10.33590/emj/10304060.
Abstract
Background: Liver biopsy, the gold standard for monitoring of methotrexateinduced liver injury, is associated with significant morbidity and mortality. Transient elastography (TE) has been used as a non-invasive alternative to detect liver stiffness.
Aim: To assess the utility of TE in detecting liver fibrosis in patients with methotrexate use.
Methods: A retrospective chart review was performed for 35 patients referred to the liver clinic for evaluation of suspected methotrexate-induced liver injury. Demographic, clinical, histopathological, and elastographic data were collected and interpreted. Liver stiffness measurement (LSM) and controlled attenuation parameter were recorded from TE results.
Results: Thirty-five patients with a mean age of 58 years, including 23 females (66%), were included. The median LSM by TE was 10.8 kPa and the median controlled attenuation parameter was 303 dB/m. A total of 12 out of 35 patients (34%) had evidence of clinical and pathological advanced fibrosis. Using a cutoff elastography value of 10 kPa, the TE yielded 92% sensitivity and 93% negative predictive value for ruling out methotrexate-induced advanced liver fibrosis. Using a higher LSM cut-off point of kPa ≥15.0, specificity was calculated at 87% and positive predictive value at 80%. Area under the receiver operating characteristic curve was 0.80 (95% confidence interval).
Conclusion: FibroScan® (Echosens, Paris, France) has a high sensitivity and specificity for kPa 10 and 15, respectively, for detecting advanced liver fibrosis in patients on methotrexate.
118 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Key Points
1. Despite its efficacy, long-term methotrexate therapy can lead to liver injury characterised by elevation in hepatic aminotransferases, steatosis, fibrosis, and rarely, cirrhosis.
2. FibroScan, a non-invasive test using transient elastography, estimates liver fibrosis and steatosis by measuring liver stiffness and controlled attenuation parameter.
3. The study underscores the importance of larger, prospective studies to validate the utility of FibroScan in managing methotrexate-induced liver injury, and potentially reducing the need for invasive liver biopsies.
INTRODUCTION
Methotrexate (MTX), an antimetabolite, has a multifarious mechanism of action that most notably includes folate antagonism, effects on adenosine signalling, and modulation of many other cellular proteins and pathways, that overall results in an anti-inflammatory effect.1 MTX is used in rheumatologic disorders (e.g., rheumatoid arthritis), dermatologic conditions (e.g., psoriasis), inflammatory bowel disease, and a multitude of other diseases.
Elevation in hepatic aminotransferases is a well-illustrated side effect of MTX therapy. In patients on low-to-moderate dose long-term MTX, aminotransferase elevation occurs in 15–50% of patients, but is typically mild and self-limiting.2 Long-term therapy can also result in steatosis, fibrosis, and rarely, cirrhosis.2 The mechanism of liver injury is believed to be due to inhibition of DNA and RNA synthesis, causing cellular arrest.2 The mechanism of MTXinduced liver fibrosis is postulated to be due to hepatic accumulation of MTX metabolites, leading to excessive homocysteine generation, oxidative stress, inflammation, and ultimately the activation of hepatic stellate cells forming myofibroblasts and resultant fibrosis.2,3 Structural damage in rat livers exposed to MTX include sinusoidal dilatation, inflammatory cell infiltration, congestion, and hydropic degeneration.4
FibroScan® (Echosens, Paris, France), or transient elastography (TE), is a test used to noninvasively estimate the degree of liver fibrosis and steatosis.5 The test consists of an ultrasound transducer mounted on a vibrator. Vibrations are transmitted to hepatic tissue with propagation of an elastic shear wave.6 The velocity of the shear
wave is subsequently measured and expressed in kilopascals (kPa). The kPa corresponds to liver stiffness as sound waves travel faster in media with greater elasticity.7-9 Thus, kPa represents the liver stiffness measurement (LSM). Hepatic steatosis is represented by the controlled attenuation parameter (CAP). The CAP is measured by energy loss as the sound wave passes through the medium, and is expressed in dB/m.10,11
A cross-sectional study by Lertnawapan et al.12 in 2018 found an association between cumulative MTX intake in patients with rheumatoid arthritis and hepatic fibrosis measurement by FibroScan.12 It also showed a statistically significant association with BMI, fatty liver, and alanine transaminase levels. Large prospective studies have previously been conducted in patients with non-alcoholic fatty liver disease to establish cut-offs for the LSM and CAP, corresponding to fibrosis stage and steatosis grade, respectively.13-15 These studies compare FibroScan findings with biopsy proven fibrosis stage and/or steatosis grade. Optimal cut-off points are devised typically through the use of receiver operating characteristics (ROC) curves.
However, the accuracy of FibroScan in measuring MTX-induced fibrosis has not been completely established. The aim of this study is to evaluate the utility of FibroScan in predicting advanced liver fibrosis in patients with a history of MTX use.
METHODS
The authors performed a retrospective study of patients referred to the hepatology clinic at
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 119 Article
Saint Louis University Hospital, Missouri, USA, between 2016–2021, for estimation of liver disease related to MTX use. The hepatology service utilised FibroScan as an initial noninvasive test to screen for presence of advanced liver disease in the setting of chronic MTX use. Patients with a known history of nonalcoholic fatty liver disease, chronic hepatitis B or hepatitis C, or current alcohol use were excluded. This study (IRB #31760) was approved by the institutional review board of Saint Louis University Hospital, Missouri, USA under Exempt Category 4 and was conducted under the Declaration of Helsinki.
Chart review was performed and data regarding sex; ethnicity; BMI; FibroScan results, including LSM (kPa), and CAP (dB/m); liver biopsy results; and signs of clinical cirrhosis were recorded. The authors also collected data regarding outcomes, including follow-up FibroScans, need for transplant, development of hepatocellular carcinoma, and mortality.
LSM cut-off values of more than 15.0 on TE were used to diagnose advanced fibrosis, whereas a cut-off of <10.0 was used to indicate low probability of advanced fibrosis.12,14 Liver fibrosis staging was performed according to Metavir classification.16 Patients with F3 or F4 were considered to have ‘advanced fibrosis’. Patients without a liver biopsy who had a clinical diagnosis of cirrhosis were also considered to have ‘advanced fibrosis’.
STATISTICAL ANALYSIS
Data were presented as number (percentage) or median (minimum–maximum), as indicated. The ROC curve, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated using SPSS version 27.0 (IBM, Armonk, New York, USA) in order to assess diagnostic accuracy of TE against histopathology. Area under the ROC (AUROC) of 1.0 represents an excellent test; however, AUROC of ≤0.5 indicates a worthless test.17 Categorical variables were compared between groups using Fisher’s exact test. P<0.05 was considered statistically significant.
RESULTS
The authors identified 35 patients with a history of MTX use who underwent FibroScan to screen for possible MTX-induced liver injury. One patient had a prior history of alcohol use disorder that was in remission at the time of FibroScan. Of this sample, 23 (66%) were female. The median age was 63 years (range: 32–74 years) and median BMI was 32.1 (range: 20.6–46.3). MTX was used by patients to treat rheumatologic or dermatologic diseases in 26 patients (74%), and haematologic diseases in nine patients (26%). Rheumatologic/dermatologic indications included rheumatoid arthritis in 15 patients (58%), psoriasis or psoriatic arthritis in seven (27%), scleroderma in two patients (8%), and one case for each of atopic dermatitis and inclusion body myositis. Haematologic indications were lymphoma/leukaemia in four patients (45%), myelodysplastic syndrome in three patients (33%), and myelofibrosis in two (22%). LSM ranged from 3.8–74.8 kPa with a median of 10.8. CAP ranged from 118–400 dB/m. Twenty-seven of the patients (77%) underwent a liver biopsy. Of those, nine patients (33%) had advanced liver fibrosis on biopsy. Of the eight patients who did not undergo biopsy, three had a clinical diagnosis of cirrhosis. Thus, 12 of the 35 patients (34%) were considered to have advanced liver fibrosis based on clinical and histopathological data. Table 1 shows a summary of the demographic, clinical, TE, and histopathologic results of the study cohort.
A total of 14 patients had LSM values of less than 10.0 kPa on TE. Of those patients, only one was found to have advanced liver disease confirmed by biopsy. Figure 1 shows the scatterplot of LSM values for patients with confirmed non-advanced and advanced liver fibrosis, respectively. Sensitivity of FibroScan for ruling out advanced fibrosis when kPa is <10.0 was calculated to be 92% and NPV was 93%. These data can be found in Table 2. Table 3 shows that for LSM cut-off value of 15.0 or greater, 10 total patients were identified. Of those patients, seven were found to have advanced fibrosis according to METAVIR classification. Specificity of FibroScan for ruling in advanced fibrosis when kPa is ≥15.0 was calculated to be 87%, while PPV was 80%. Evaluation of these data using a ROC curve showed an area under the curve of 0.80 (Figure 2).
120 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Indication for MTX use
Feature Rheumatologic or Dermatologic Haematologic Total Total number of patients (N) 26 9 35 Female Sex 19 4 23 Age, years (Median) 61 (32–74) 65 (51–73) 63 (32–74) BMI, kg/m2 (Median) 32.6 (20.6–46.3) 26.4 (21.5–37.9) 32.1 (20.6–46.3) LSM, kPa (Median) 10.5 (3.8–64.9) 11.0 (5.9–74.8) 10.8 (3.8–74.8) CAP, dB/m (Median) 313 (121–400) 259 (118–400) 303 (118–400) Underwent biopsy 19 8 27 Advanced fibrosis on biopsy 6 3 9 Clinical diagnosis of cirrhosis 3 0 3 Histopathology/Clinical Non-advanced liver disease Advanced liver disease LSM <10.0 kPa 13 1 LSM ≥10.0 kPa 10 11 CAP: controlled attenuation parameter; LSM: liver stiffness measurement; MTX: methotrexate.
LSM: liver stiffness measurement.
Table 1: Demographic, clinical, elastographic, and histopathological data of the authors’ population.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 121 Article
Table 2: Clinical/histopathological advanced liver disease and liver stiffness measurement of 10 kPa.
Individual value plot of liver stiffness measurement in kPa
Individual value plot of liver stiffness (excludes outliers)
Histopathology/Clinical Non-advanced liver disease Advanced liver disease LSM ≥15.0 kPa 3 7 LSM <15.0 kPa 20 5 LSM:
liver stiffness measurement.
Non-advanced fibrosis Non-advanced fibrosis kPa kPa 0 0 40 40 10 10 50 50 20 20 60 60 30 30 70 70 80 80 Advanced fibrosis Advanced fibrosis
Table 3: Clinical/histopathological advanced liver disease and liver stiffness measurement of 15 kPa.
Figure 1: Scatter-plot diagram showing the distribution of liver stiffness values (kPa) between advanced and non-advanced fibrosis confirmed clinically or by histopathology.
122 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Treatment with MTX was continued after evaluation for MTX-induced liver injury in six out of 35 patients. Of these, five had reassuring biopsy results (score of F0, F1, and F2) and one had a low LSM value of 4.6 kPa. Elastography was performed in two out of six of the patients continued on MTX, and showed stable kPa. MTX was initially stopped then restarted in three patients, after repeat TE showed improvement of LSM values. A follow-up FibroScan was performed in eight out of 35 patients and showed stable LSM values in six patients, and worsening LSM in two patients, even after stopping the MTX. Six out of the 35 were deceased, none of them developed hepatocellular carcinoma, and none received liver transplant.
DISCUSSION
The use of MTX is associated with increased risk of liver fibrosis and cirrhosis.18,19 Given the inherent risk of liver biopsy with associated increased morbidity and mortality,20,21 noninvasive techniques have been used to assess for liver fibrosis. TE has been adopted as a routine
investigation technique for monitoring of liver injury in patients treated with MTX.3 Elastography can help measure liver stiffness through LSM and predict the degree of steatosis through CAP. Prior studies have shown mixed results in the sensitivity and specificity of FibroScan to detect advanced fibrosis, compared to histopathology. The authors’ study was conducted to add to the available data on the performance of FibroScan in this population.
Although low LSM cut-off values have been previously adopted in literature,22,23 other guidelines recommend the use of higher cutoffs, since elastography has high sensitivity and specificity when used to detect cirrhosis rather than lower stages of liver fibrosis.3,24,25 Hence, the authors used kPa cut-off of <10 kPa to rule out advanced chronic liver disease, kPa between 10–15 to suggest possible advanced disease, and LSM >15 kPa to be highly suggestive of advanced liver disease. In this cohort, the median LSM was 10.8 kPa and 33% of the cohort had advanced liver disease based on clinical and histopathological evidence. This percentage of advanced disease is in accordance with results
ROC curve Sensitivity 0.0 0.0 0.2 0.4 0.6 0.8 1.0 0.8 0.2 0.4 1.0 0.6
Figure 2: Receiver operating characteristic curve for prediction of advanced liver fibrosis based on kPa measurements.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 123 Article
Diagonal segments are produced by ties. ROC: receiver operating characteristic.
from a recent review showing that 0–33% of patients on MTX can develop significant hepatic fibrosis.3
The authors’ study showed a sensitivity of 92% and NPV of 93% in ruling out advanced liver fibrosis with kPa <10.0. Furthermore, the sensitivity and NPV were 100% for a kPa of <7.0. The high sensitivity in ruling out advanced fibrosis indicates FibroScan is a useful screening test for patients at risk of MTX-induced fibrosis. This was supported by a smaller study by Bray et al.,26 which used a kPa cut-off of 7.1, for which the sensitivity was 100% in detecting liver fibrosis.26 However, two studies by Berends et al.27 of 24 patients, and another by Rongngern et al.23 of 45 patients, used a cutoff of 7.1 kPa, and found sensitivity to be 50% for detecting ≥F2 liver fibrosis.22,27 Importantly, the authors’ study measured the ability of FibroScan to detect ≥F3 liver fibrosis. Thus, the higher sensitivity than the latter two studies is likely, due in part to the fact FibroScan can more readily detect a more advanced form of liver disease.3,25 In addition, it is important to mention that the latter studies were performed on patients with psoriasis who commonly have higher incidence of metabolic syndrome, and obesity is a common cause for failure of elastography.28
Using a higher LSM cut-off point of kPa ≥15, the authors’ specificity was calculated at 87% and PPV at 80%. The AUROC was 0.80 (95% confidence interval). These findings indicate a reasonable ability of FibroScan to rule in advanced fibrosis in our population, though they were not as significant as the sensitivity and NPV. These results are in accordance with Berends et al.,27 who showed that TE has 88% specificity for detection of ≥F2. On the contrary, a recent prospective cross-sectional
References
1. Bedoui Y et al. Methotrexate an old drug with new tricks. Int J Mol Sci. 2019;20(20):5023.
2. National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox: clinical and research information on drug-induced liver injury. Methotrexate [Internet] (2020) Bethesda: National Institute of Diabetes and Digestive and Kidney Diseases. Available from: https://www.ncbi.nlm.nih.
study demonstrated a low predictive ability of elastography to identify fibrosis with an AUROC of 0.41.22
The authors’ literature review showed that guidelines regarding the use of MTX following the identification of MTX-induced liver injury are scarce. In their cohort, they were able to restart MTX in a total of nine out of 35 patients. All nine patients had low kPa on elastography and/or F0, F1, or F2 fibrosis stages on histopathology. Results for follow-up FibroScans were available in two cases showing stable kPa after restarting MTX. Larger and prospective studies are needed to help establish standardised guidelines for continuation of MTX in such settings.
The authors’ study has several limitations, including being retrospective and having a small sample size. While the authors did exclude patients with other more common aetiologies of liver fibrosis (viral hepatitis, active alcohol use, diagnosis of non-alcoholic fatty liver disease), any patient with another covert aetiology of fibrosis would introduce confounding into the population. Additional limitations included lack of biopsy in eight of the patients, and lack of available data on cumulative doses of MTX.
In conclusion, the authors’ retrospective study shows that FibroScan has high sensitivity and specificity for kPa 10 and 15, respectively, for detecting advanced liver fibrosis in patients on MTX. Higher powered studies, and ideally prospective studies, are needed to validate these findings in the context of mixed results among the available small studies. Verification of the utility of FibroScan can increase the confidence in which we interpret non-invasive findings for this population and potentially avoid unnecessary liver biopsies.
gov/books/NBK548219/. Last accessed: 1 February 2023.
3. Cheng HS, Rademaker M. Monitoring methotrexate-induced liver fibrosis in patients with psoriasis: utility of transient elastography. Psoriasis (Auckl). 2018;8:21-9.
4. Akbulut S et al. Cytoprotective effects of amifostine, ascorbic acid and N-acetylcysteine against methotrexate-induced hepatotoxicity in rats. World J
Gastroenterol. 2014;20(29):1015865.
5. Wong VW, Chan HL. Transient elastography. J Gastroenterol Hepatol. 2010;25(11):1726-31.
6. Vergniol J, de Ledinghen V. [Transient elastography (FibroScan): a new tool in hepatology]. Presse Med. 2009;38(10):1516-25. (In French).
7. Sandrin L et al. Transient elastography: a new noninvasive method for assessment of hepatic
124 EMJ ● March 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
fibrosis. Ultrasound Med Biol. 2003;29(12):1705-13.
8. Jung KS, Kim SU. Clinical applications of transient elastography. Clin Mol Hepatol. 2012;18(2):163-73.
9. Castera L. Transient elastography and other noninvasive tests to assess hepatic fibrosis in patients with viral hepatitis. J Viral Hepat. 2009;16(5):300-14.
10. Ozturk A et al. Principles of ultrasound elastography. Abdom Radiol (NY). 2018;43(4):773-85.
11. Sasso M et al. Controlled attenuation parameter (CAP): a novel VCTE guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med Biol. 2010;36(11):1825-35.
12. Lertnawapan R et al. Association between cumulative methotrexate dose, non-invasive scoring system and hepatic fibrosis detected by Fibroscan in rheumatoid arthritis patients receiving methotrexate. Int J Rheum Dis. 2019;22(2):21421.
13. Siddiqui MS et al. Vibrationcontrolled transient elastography to assess fibrosis and steatosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2019;17(1):156-63.
14. Park CC et al. Magnetic resonance elastography vs transient elastography in detection of fibrosis and noninvasive measurement of steatosis in patients with biopsy-
proven nonalcoholic fatty liver disease. Gastroenterology. 2017;152(3):598-607.
15. Tapper EB et al. The performance of vibration controlled transient elastography in a US cohort of patients with nonalcoholic fatty liver disease. Am J Gastroenterol. 2016;111(5):677-84.
16. Castera L et al. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48(5):835-47.
17. Park SH et al. Receiver operating characteristic (ROC) curve: practical review for radiologists. Korean J Radiol. 2004;5(1):11-8.
18. Dahl MG. Methotrexate and the liver. Br J Dermatol. 1969;81(6):465-7.
19. Carneiro SC et al. Methotrexate and liver function: a study of 13 psoriasis cases treated with different cumulative dosages. J Eur Acad Dermatol Venereol. 2008;22(1):25-9.
20. Kremer JM et al. Methotrexate for rheumatoid arthritis. Suggested guidelines for monitoring liver toxicity. American College of Rheumatology. Arthritis Rheum. 1994;37(3):316-28.
21. Howlett DC et al. Findings of the UK national audit evaluating image-guided or image-assisted liver biopsy. Part II. Minor and major complications and procedure-related mortality. Radiology. 2013;266(1):226-35.
22. Khandpur S et al. Ultrasound liver elastography for the detection of liver fibrosis in patients with psoriasis and reactive arthritis on long-term methotrexate therapy:
a cross-sectional study. Indian J Dermatol Venereol Leprol. 2020;86(5):508-14.
23. Rongngern P et al. Diagnostic performance of transient elastography for detection of methotrexate-induced liver injury using Roenigk classification in Asian patients with psoriasis: a retrospective study. Arch Dermatol Res. 2017;309(5):403-8.
24. Ferraioli G, Roccarina D. Update on the role of elastography in liver disease. Therap Adv Gastroenterol. 2022;15:17562848221140657.
25. European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH clinical practice guidelines: non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237-64.
26. Bray AP et al. Liver fibrosis screening for patients with psoriasis taking methotrexate: a cross-sectional study comparing transient elastography and liver biopsy. Br J Dermatol. 2012;166(5):1125-7.
27. Berends MA et al. Biochemical and biophysical assessment of MTXinduced liver fibrosis in psoriasis patients: fibrotest predicts the presence and Fibroscan predicts the absence of significant liver fibrosis. Liver Int. 2007;27(5):63945.
28. Garg H et al. Utility of transient elastography (fibroscan) and impact of bariatric surgery on nonalcoholic fatty liver disease (NAFLD) in morbidly obese patients. Surg Obes Relat Dis. 2018;14(1):81-91.
Creative Commons Attribution-Non Commercial 4.0 ● March 2024 ● EMJ 125 Article FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM

Receive our free newsletters and alerts Get the latest updates on all our upcoming journals and receive first-class insights into ground-breaking news and advancements in medicine across multiple therapeutic areas. www.emjreviews.com Join our mailing list
